
Abstract
Introduction
The incidence of depression among healthcare providers is higher compared to that of other occupations. 1 Clinical depression is a predictor of morbidity and mortality and accounts for the greatest contribution to disability of all mental health disorders.2-4 The overall pooled prevalence of depression in resident physicians is 28.8%. 5 Depression in medical students and residents has been studied in depth, revealing increased rates of depressive symptoms leading to decreased academic performance and increased risk for medication errors compared to their non-depressed colleagues.5-7 The major reasons for depression among medical residents include workload, work inefficiency, lack of autonomy and meaning in work, and work-home conflict.5-7
Pharmacy residents too face a heavy workload and experience a great weight of expectation and responsibility. 8 Thus, pharmacy residents may also suffer from symptoms of depression, stress, and anxiety. Publications regarding this topic have focused on establishing the occurrence of depressive symptoms and high stress among pharmacy residents, and have outlined rates of these symptoms.8-10 Residency-specific factors related to depressive symptoms include lack of support from directors and/or preceptors, ineffective teaching methods, unclear expectations, unstructured programs, not having a full day off each week, working over 40 hours per week, and practicing in an inpatient setting. 11 Current literature focuses on the viewpoint of pharmacy residents regarding their symptoms and potential contributing factors; however, data is lacking regarding the awareness of these issues by residency program directors (RPDs), and available resources or viable solutions to address the problem.8-11 RPDs work closely with residents and may have an understanding of the various aspects of residency that may be leading to depressive symptoms, or have offered resources or solutions to help address the problem. They may potentially serve as the first-line resource for the resident if these symptoms occur. Therefore, RPDs are in an ideal position to provide further insight into this topic. However, there are no studies inquiring into the RPDs’ points of view, or identifying and implementing possible solutions. Additionally, research shows lack of support from RPDs as an important factor in development of depressive symptoms amongst residents. 11 Therefore, devising solutions first requires a complete understanding of the problem from all stakeholders, including RPDs, who can help identify potential factors, as well as propose solutions. With a lack of literature in this context, the goal of this study is to understand the scope of this issue using a qualitative methodology, which will help in getting a rich description of the issue.
The primary outcomes of this study are to understand the RPD viewpoints about potential contributing factors for depressive symptoms in pharmacy residents, determine current resources available, and outline possible solutions to decrease the burden of depressive symptoms amongst pharmacy residents from the viewpoint of RPDs.
Methods
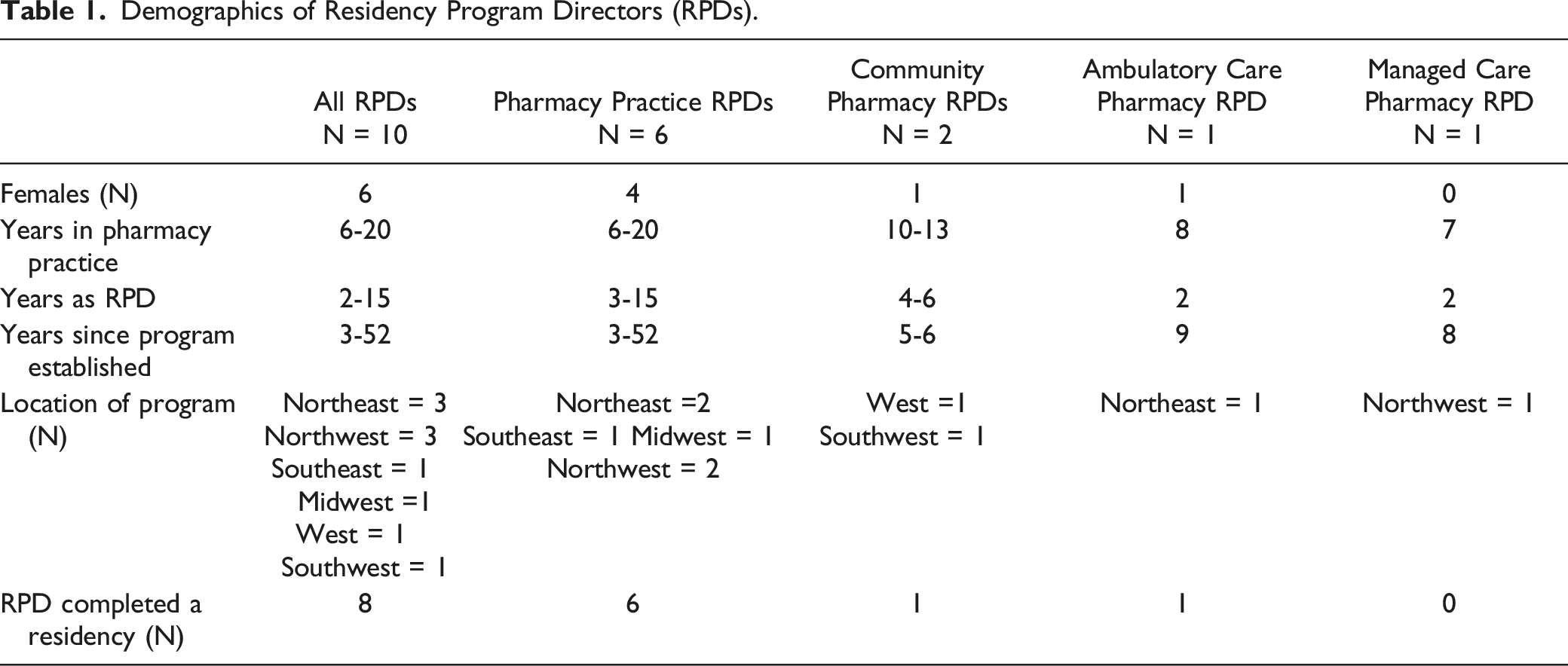
The study utilized a qualitative research design with semi-structured one-on-one interviews with RPDs. A list of 2500 PGY1 and PGY2 residency programs in the United States was retrieved from the American Society of Health-System Pharmacists (ASHP) in 2017. This list was randomly narrowed down to 20 RPDs to represent diversity in location and type of residency program. Since it was a homogenous population, the authors decided to interview ten RPDs to ensure data saturation would be achieved.12,13 Among the ten RPDs, it was decided to have six RPDs from PGY1 pharmacy practice, two from ambulatory care, one from managed care, and one from community pharmacy practice to match the proportion of the various residencies available in the US.
An email was sent to the 20 randomly selected RPDs in May 2019, with a reminder email one week later, which yielded one interview with a pharmacy practice RPD. Another 50 RPDs were randomly selected in July 2019 and an email was sent to them, with a reminder one week later, which yielded three additional pharmacy practice RPD interviews. A third email with a reminder was sent to an additional 50 randomly selected RPDs by the end of July 2019, which did not yield any interviews. One hundred additional RPDs were randomly selected and emailed in September 2019, which yielded one additional interview with a pharmacy practice RPD. Another 100 RPDs were randomly selected and emailed a request at the end of September 2019, leading to three additional interviews (one pharmacy practice and two community practice RPDs). Since the email recruiting strategy was not able to engage any RPDs from ambulatory care or managed care, a snowball sampling technique was used to identify two additional RPDs (one each from ambulatory care and managed care). All emails sent incentivized participation by provision of a $50.00 gift card.
RPDs were invited to participate in a 45-60 minute semi-structured interview focusing on current and past residents from their respective programs. An interview guide (Appendix 1) was created by the authors based on three major domains in line with this study’s aims to identify: 1) potential factors leading to depressive symptoms, 2) current resources allocated, and 3) possible solutions identified by the RPDs to reduce the depressive symptoms. For the first domain, the interview questions focused on whether RPDs were aware of this phenomenon, whether the depressive symptoms observed were a recent development, and identification of any potential reasons for depressive symptoms. For the second domain, the questions focused on the current systems and policies in place, or resources allocated to prevent or mitigate depressive symptoms amongst residents. The third domain focused on identifying possible solutions from the RPDs’ perspective. Demographic questions included number of years in the RPD role, number of years practicing as a pharmacist, and whether the RPDs had completed a residency. Demographic information collected from the participants was summarized using descriptive statistics. Each interview was semi-scripted, and all participants were asked the same questions; however, the interviewer could follow-up with additional questions or ask for clarification based on the participant’s response. The study was reviewed and certified as exempt by the Investigational Review Board at Roseman University.
Inductive approaches were used in data collection and analysis. All interviews were conducted by the primary investigator (PI) using telephone. 14 All interviews were audio recorded, transcribed into a Microsoft Word document via a qualitative data transcription and analysis software (NVivo), and de-identified by the interviewer. The PI compared the transcribed documents with the audio recordings of the interviews to ensure transcription accuracy. The PI, along with two co-investigators, manually and independently analyzed data to achieve data immersion, create initial codes, make notes, and add additional codes with repeated reading, resulting in either editing the older codes or creating newer codes.
Codes were further analyzed to find similarities so they could then be grouped under sub-categories and then larger categories. Themes were formed based on the relationship between categories. The investigators discussed findings and discrepancies to agree upon thematic interpretations of the transcripts. Original transcripts were referenced as necessary, until a consensus was reached on the interpretations of the transcripts.
Results
Demographics of Residency Program Directors (RPDs).
Theme 1, codes, and representative quotes from analysis of transcribed interviews.
Theme 2, codes, and representative quotes from analysis of transcribed interviews.
Theme 3, codes, and representative quotes from analysis of transcribed interviews.
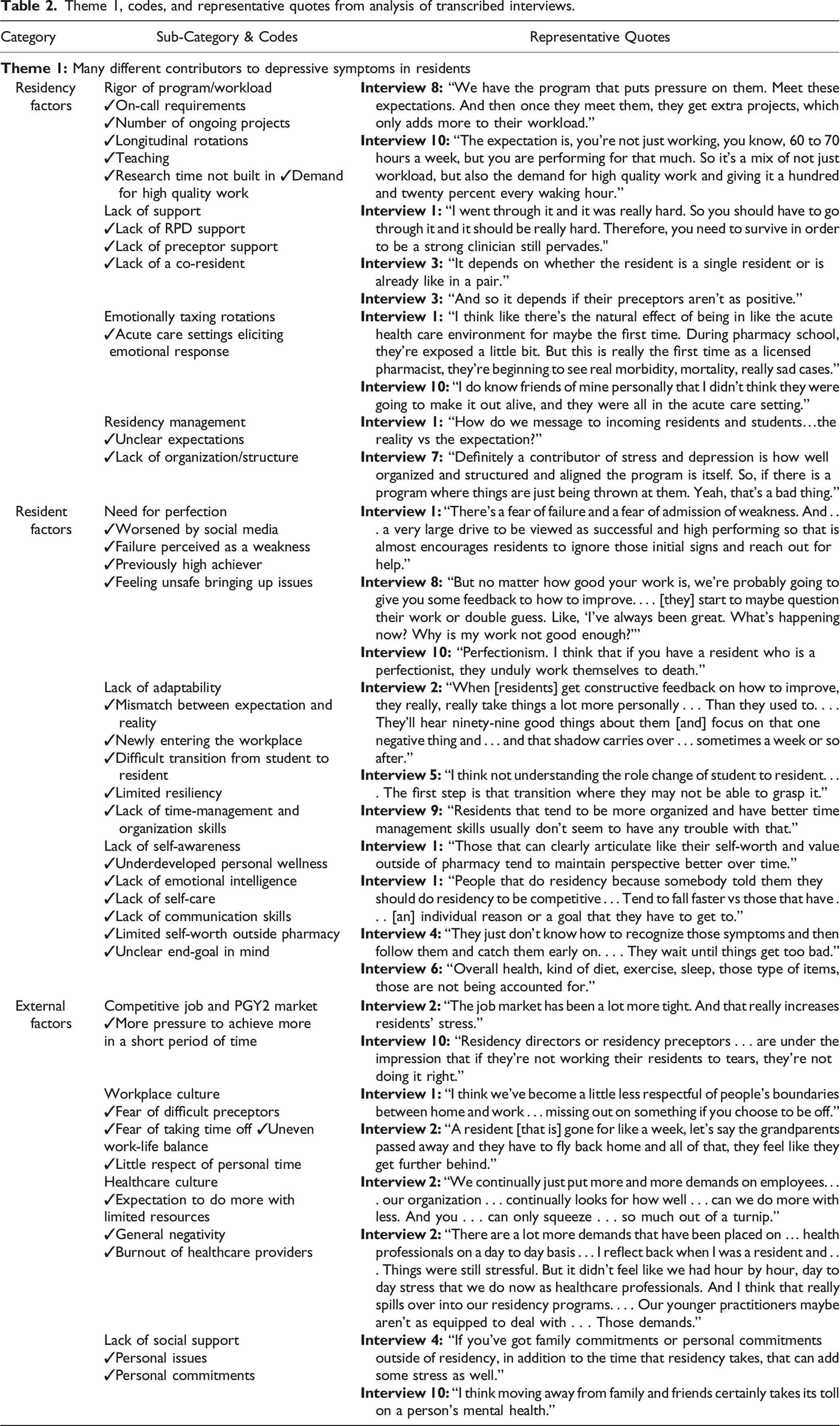
Theme 1: Many different Contributors to Depressive Symptoms in Residents (Table 2)
The major categories within this theme were residency related factors, resident specific factors, and external factors. All RPDs agreed that the rigor of the residency year exacerbated by workload and demand for high-quality work was a significant factor. After completing patient care responsibilities during work hours, residents are required to work on ongoing projects, teaching, research requirements, etc., and are expected to produce high quality work. Additionally, lack of support from RPDs, preceptors, or co-residents, and at times not having a co-resident were mentioned as potential contributors to depressive symptoms in residents. Four RPDs mentioned that emotionally taxing rotations, especially in the acute care setting or if the resident had not previously encountered that setting, could elicit strong negative emotional responses. Finally, poor residency management, leading to unclear expectations for the residents, could lead to depressive symptoms.
Although RPDs agreed that residency was challenging, a few felt that workload was manageable and had not increased in recent years. Half of the RPDs commented on resident-specific factors which may worsen depressive symptoms, including a need for perfection, which may be intensified by social media and from receiving limited constructive feedback in the past. Residents may feel unsafe bringing up emotional concerns to RPDs due to a potential need to be perceived as high achieving or viewing asking for help as a weakness. RPDs commented on the difficult transition from student to resident as a result of the discord between expectation and reality of residency, as well as the lack of time management skills. RPDs consistently agreed that residents who lacked self-awareness related to self-care, communication skills, etc. struggled more during a challenging residency compared to those residents with more developed skills in these areas and emotional intelligence.
Finally, external factors including limited availability of PGY2 opportunities and a competitive job market both place an additional burden on residents to achieve more in a short period of time. Both workplace and healthcare cultures place additional weight on the residents. Difficult preceptors with little respect for the residents’ personal time, as well as a general expectation of healthcare providers, including pharmacists, to achieve more with limited resources creates a pattern of negativity and may lead to depressive symptoms. In this environment, residents may avoid taking time off due to fear of falling behind, which could worsen work-life balance. External factors also included lack of social support for the resident, where personal commitments took time and energy away from residency workload, compounding depressive symptoms.
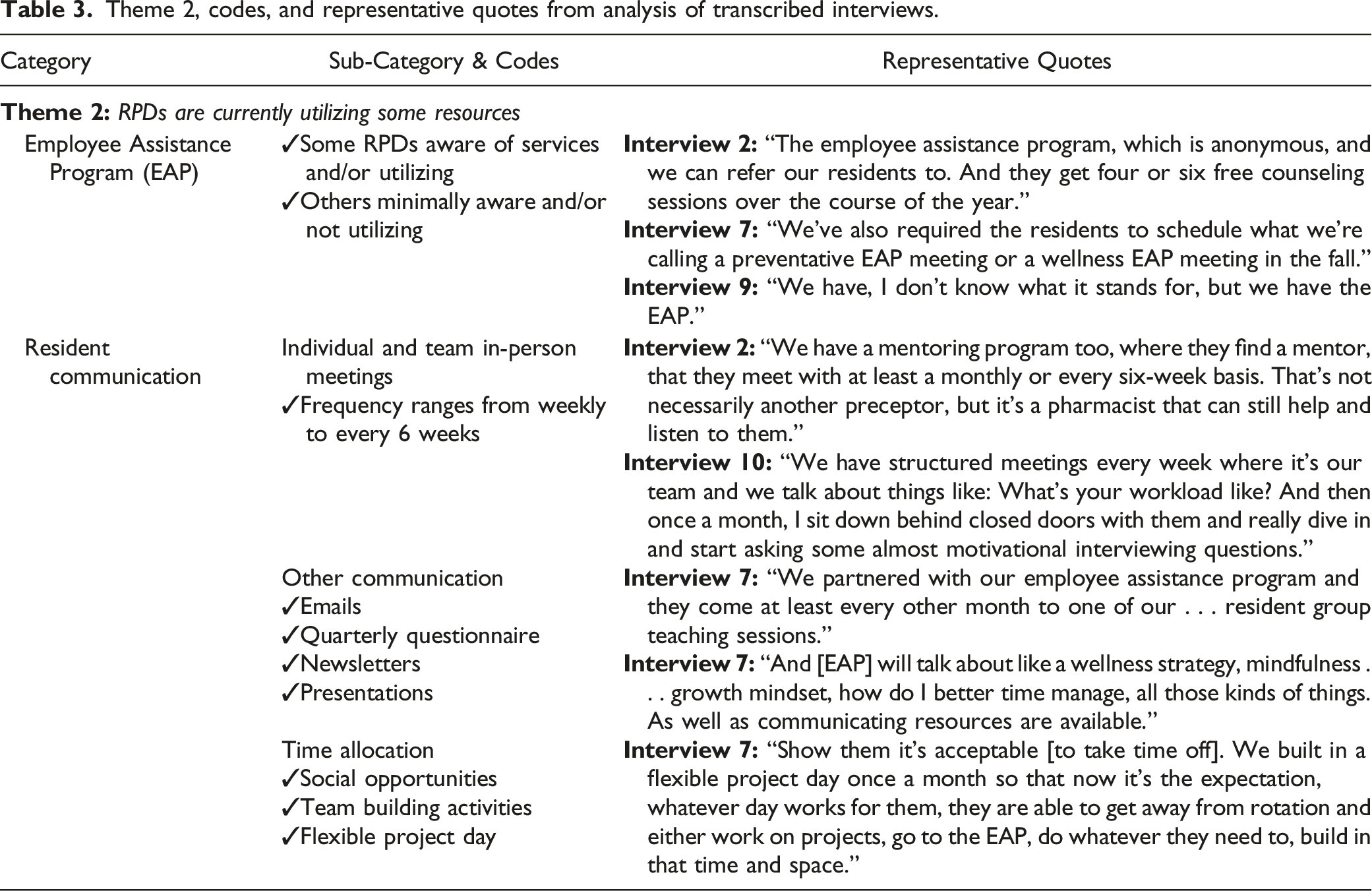
Theme 2: RPDs Are Currently Utilizing Some Resources (Table 3)
RPDs have implemented some strategies to help prevent or mitigate depressive symptoms. Nine RPDs mentioned having, and three of them reported utilizing, the employee assistance program (EAP) offered by their healthcare system to different extents. The services offered by the EAP ranged from monthly discussions to communicate resources available to residents, to individual counseling sessions. Half of the RPDs have already incorporated wellness strategies into the residency year. One strategy employed by the RPDs to help residents included enhanced and more structured communication via both group and individual meetings with residents, ranging from weekly to every six weeks. Topics included transparent discussions related to contributors to depressive symptoms and stress, the transition from student to resident, personal and professional adjustment, improving grit, what to expect from residency, establishing self-care practices, etc. RPDs also used other forms of communication including emails, newsletters, and group presentations to potentially improve resident wellness. Some RPDs had a dedicated time when all residents were off resident duties to allow for social opportunities and team building activities. Additionally, one RPD mentioned that residents appreciated being given a flexible project day once per month to allow time for self-care.
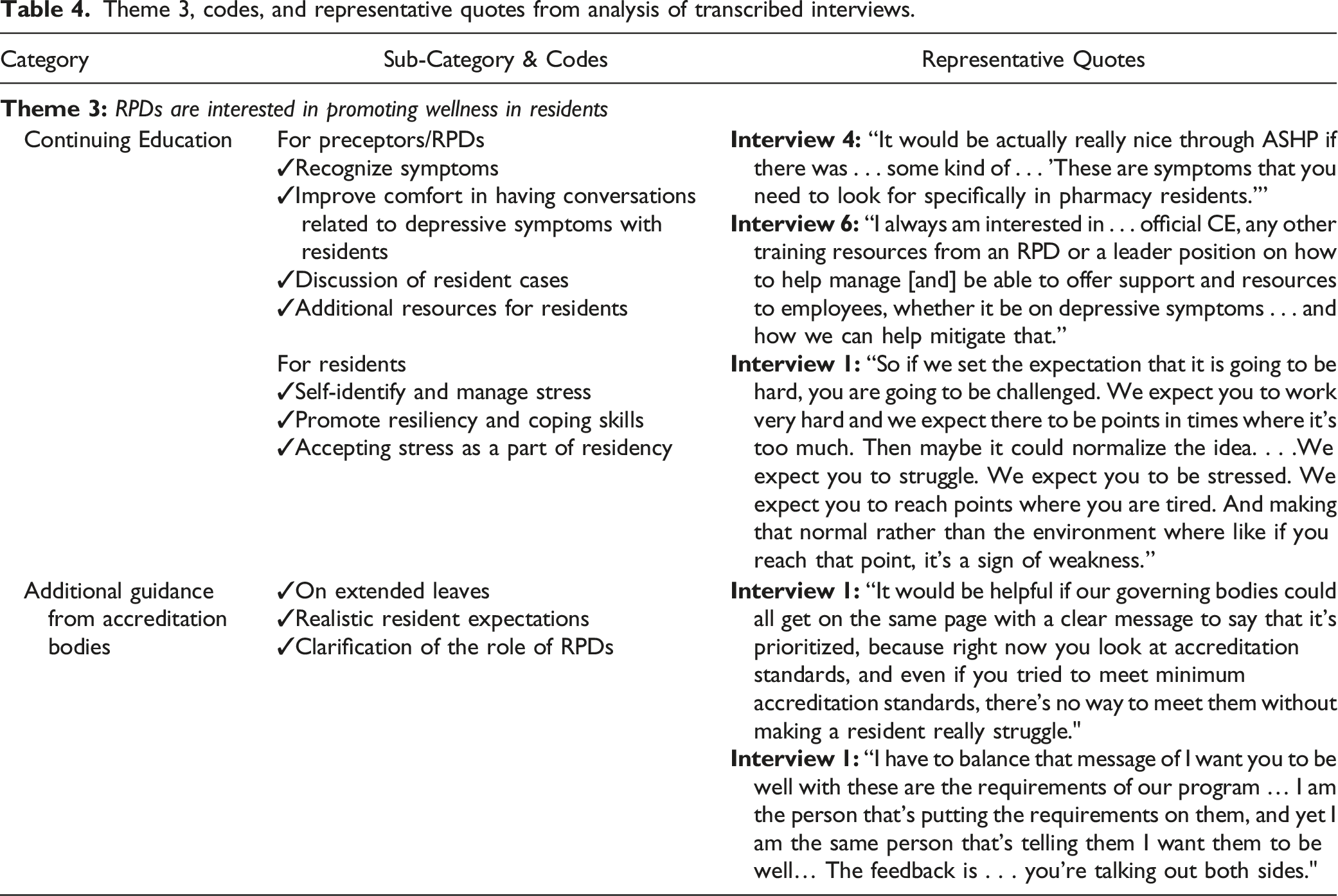
Theme 3: RPDs Are Interested in Promoting Wellness in Residents (Table 4)
RPDs were interested in promoting wellness in residents but they recognized that they did not quite know how to achieve that. Most RPDs requested additional continuing education (CE) opportunities for themselves, other preceptors, and residents in regards to this topic. The CE for RPDs and preceptors would focus on recognizing symptoms, improving their comfort when approaching this sensitive topic, and becoming familiar with resources, other than the EAP, to provide to residents. RPDs also felt that training residents to self-identify symptoms and to learn how to better manage stress, but at the same time accepting that stress is part of residency, would help to improve depressive symptoms. One RPD also identified that having a forum with other RPDs to discuss resident cases and how they were resolved would be beneficial. Finally, RPDs emphasized the need for more guidance from accreditation bodies, such as ASHP, regarding clearer policies on extended resident leave, and clarification regarding the role of RPDs in overall resident wellness. Multiple RPDs also stressed the importance of having a national conversation regarding what residents can realistically achieve in one year without neglecting their wellness.
Discussion
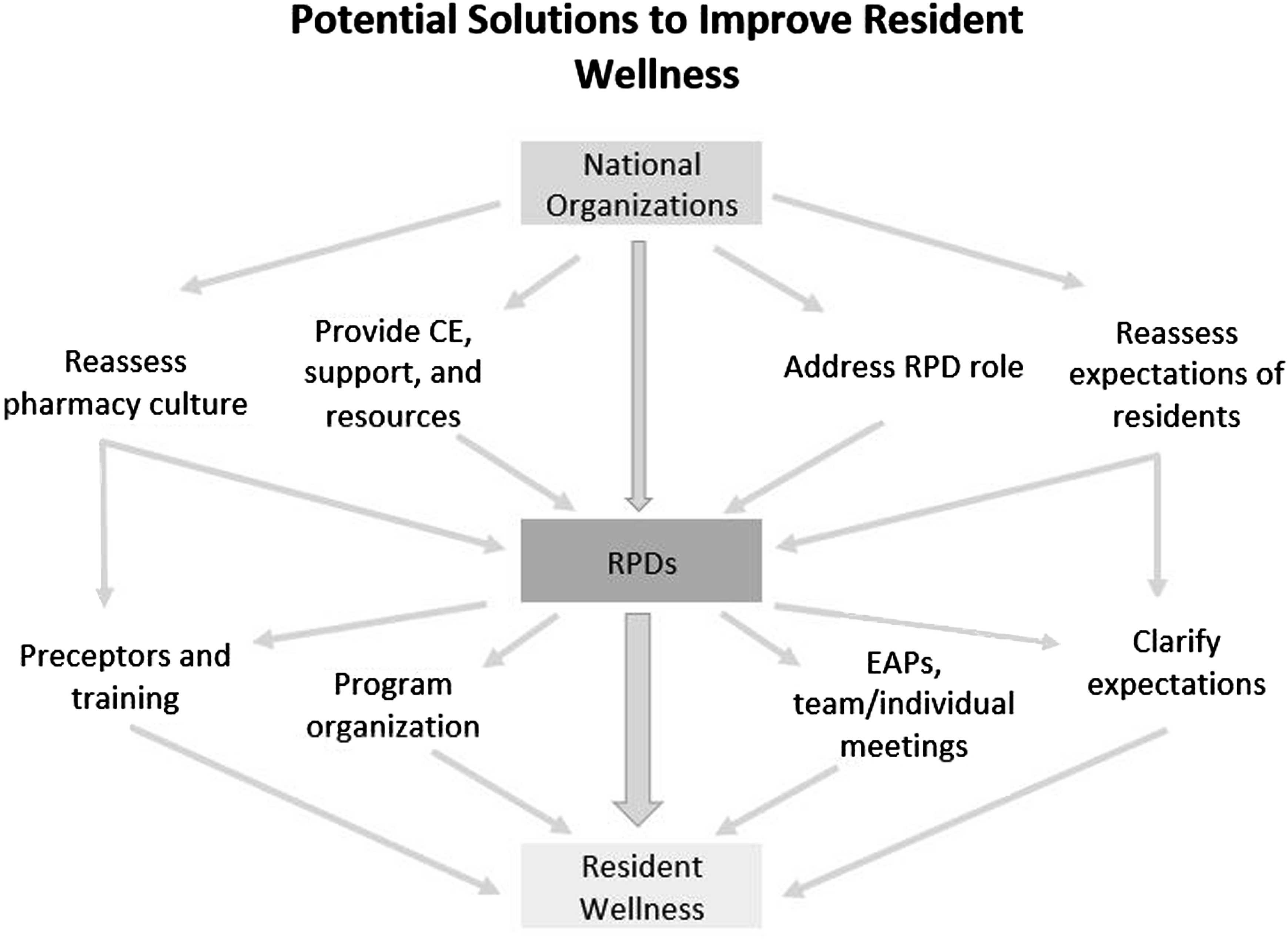
The results of this research demonstrated that RPDs recognize depressive symptoms among residents and multiple stakeholders are potentially contributing to these, including national organizations, individual residency programs (RPDs and supporting preceptors), and residents themselves (Figure 1). As such, each group shares responsibility for helping to prevent or mitigate these risks to promote overall resident wellness (Figure 2). The major source of support for the RPDs is support systems available through human resources, which they currently use at varying levels. Results indicate that none of the RPDs are completely confident about the resources used in handling these issues. When asked for solutions, there was consensus about the various stakeholders coming together to resolve the problem. Perspectives of RPDs regarding influences on resident wellness. Potential solutions to improve resident wellness.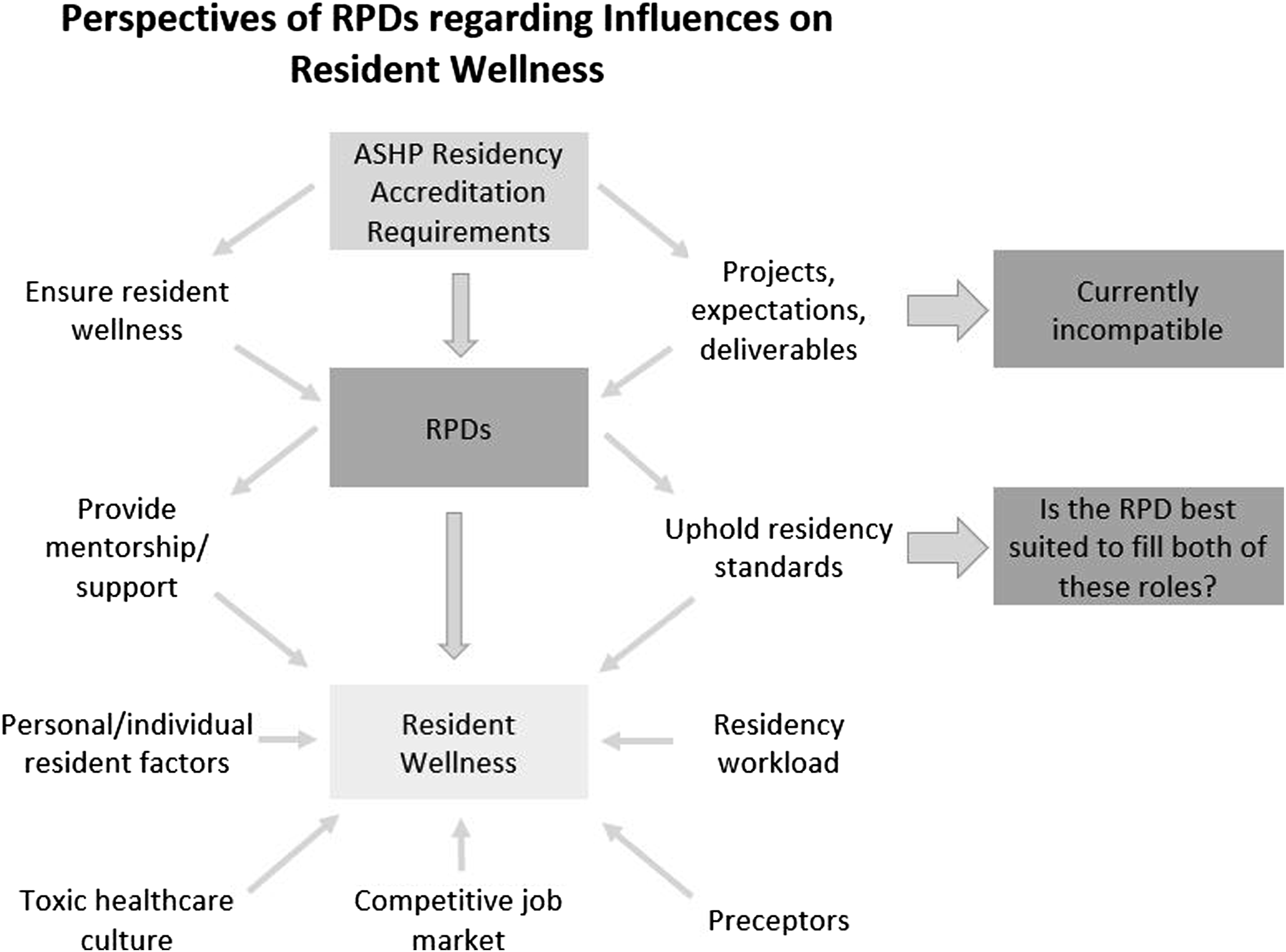
Role of National Organizations/Accreditation Bodies and Residency Programs in Reassessing Expectations of Residents
As RPDs are the bridge between residents and residency requirements outlined by accreditation bodies, they can help to implement change, while working collaboratively with both groups. Workload and the normalization of work-related stress were perceived as the most significant factors leading to depressive symptoms in pharmacy residents. Some mitigation strategies, also available through the ASHP webpage focus on well-being and resiliency, help address residency and personal resident factors, but they do not directly resolve the issue of workload. 15 Although RPDs agreed residencies should challenge the resident to achieve three to five years of clinical experience in one year, they also felt this expectation did not align with the recommendations to achieve wellness, both set by accreditation bodies.15-17 RPDs found it challenging to have conversations with residents about maintaining work-life balance when they were imposing work requirements and deadlines. RPDs stated that a national conversation regarding what can realistically be achieved in one residency year must be led by accreditation bodies to bridge the gap of reality vs expectations and maintain wellness in residents’ professional careers (Figure 2). This will then help RPDs to clearly identify these responsibilities for the residents. To highlight this, a recent commentary by Potter and Cadiz called on AACP to improve our working knowledge of evidence-based strategies to improve resident well-being. 16
Role of Residency Programs in Addressing Program Organization and Management
Poor residency management unintentionally increases workload, as residents are left to assume what their responsibilities, which may be different than the expectations of the preceptor or RPD. This observation is consistent with published literature on residents’ views. 11 Although RPDs took some ownership in setting clear expectations of the residents, they also mentioned that residents themselves need to have a better understanding of their role and workload to better adapt to the transition from student to resident. RPDs also placed some onus on schools and colleges of pharmacy to better educate students regarding what to expect during a residency, developing proper time-management skills, and to find internal motivation with a clear end goal for pursuing a residency beyond becoming professionally competitive for jobs.
Role of Residency Programs in Supporting Residents Professionally and Personally, and Creating Opportunities for Continuing Education for Both Themselves and Residents
Previous research among residents demonstrated RPD and preceptor support as a major protective factor against depressive symptoms. 11 RPDs in this study also agreed that support from RPDs and preceptors in the form of recognizing the importance of and providing opportunities for work-life balance could decrease depressive symptoms. RPDs and preceptors can support residents in addressing emotional burdens, such as the need for perfection, lack of adaptability, and self-awareness. Most RPDs in this study had already implemented solutions, such as utilizing EAP services and improving communication with residents through individual or team meetings; however, the extent of enhanced communication and EAP services utilized varied widely amongst programs. RPDs also emphasized the need for resources other than EAP to address the situation. They agreed additional continuing education training, as provided by national organizations, to recognize symptoms, improving comfort in having conversations related to depressive symptoms, and any additional resources to provide to residents, would assist them in providing residents a more well-rounded experience. These observations match with the ASHP guidance document for the PGY1 residencies in which residency programs are asked to provide preceptors and staff education on burnout syndrome, and mitigation resources and strategies. 17
Interestingly, most RPDs felt they needed help recognizing symptoms themselves to reach out to the residents. Continuing education for residents themselves could help them achieve better self-care and recognize their symptoms. Medical literature has also suggested a need for medical education curricula to teach early-career physicians to recognize signs and symptoms of depression and seek help, or having residency programs implement interventions to promote resiliency and wellbeing.18-21 Another study from medical residents’ perspectives on supporting wellness helped identify several solutions including increasing awareness and removing stigmatization. 19 One program implemented resident-led initiatives to improve residents’ on-call experience, increase social activities, support preventative care, and promote wellness education. 21 When reassessing burnout one year after implementation, they saw a statistically significant reduction in overall resident burnout. 22 Implementation of some of these strategies in pharmacy education and residencies may also help to promote overall wellness.
Role of National Organizations/Accreditation Bodies in Clarifying the Role of RPDs and Reassessing Overall Pharmacy Culture
Although additional training was deemed to be necessary, RPDs also emphasized the importance of balancing their role in helping residents with their role as a supervisor with influence over the residents’ careers. They needed clarification regarding their role, and where their support should end and the resident should be further assessed by a mental health specialist. Therefore, accreditation bodies could help provide additional guidance on how RPDs can keep expectations to achieve the residency outcomes balanced with residents’ mental health needs.
Aside from workload expectations set nationally, other external factors that could lead to depressive symptoms included workplace and healthcare culture. RPDs mentioned difficult or negative preceptors having an impact on residents. Research in medical residents has shown that negativity from preceptors towards residents creates an environment that is not conducive to learning.23,24 Residencies are intended to enhance learning and patient-care skills, and the effectiveness of post-graduate education may be stymied by reductions in aptitude due to depression. With the high number of pharmacy graduates, limited number of residency positions, and a very competitive job market, residents are expected to always perform at their highest level to showcase their capabilities. This high expectation to succeed comes at the cost of personal time and commitments and pervades the pharmacy profession as a whole. As part of healthcare culture, there is a general expectation to do more with fewer resources, which is affecting pharmacists and being trickled down to residents (Figure 1). Research has shown that this leads to burnout in pharmacists, and residents are also at risk either during or after residency.25-28 These factors highlight the need for additional preceptor training to address negativity but also a more national conversation regarding not only residencies, but also pharmacy practice. Changes in practice culture will filter down through RPDs and preceptors, ultimately influencing resident wellness (Figure 2).
Limitations
This is the first study that examined the viewpoint of RPDs regarding depressive symptoms among pharmacy residents; however, the study is not without limitations. The small sample size of ten RPDs may not reflect the viewpoints of all RPDs across the country. In previous studies, it has been shown that 12 interviews typically suffice to understand perceptions and experiences among a group. 13 However, in this study, after 10 interviews, no new themes emerged. The results from this study could be used to develop a questionnaire that can be used to survey RPDs nationally. Around 350 RPDs were contacted to identify ten volunteers which required several modifications to the search strategy, despite the provision of a $50.00 gift card for their time. Even then, a snowball sampling technique had to be utilized to engage RPDs from ambulatory care and managed care residencies, which may have introduced selection bias of more engaged and knowledgeable RPDs. This could be due to the workload of RPDs themselves prohibiting time to conduct the interview. On the other hand, it is also possible RPDs did not place importance on this topic or did not feel comfortable having this vulnerable conversation. In addition, the RPDs working with PGY2 residents too may have had a different opinion or perspective. However, this data was not collected. Finally, the study provides RPDs’ perspectives of depressive symptoms in residents. The use of depressive symptoms as the metric during the interviews was based on the quality of the available literature regarding wellbeing in pharmacy residents. While a plethora of data exists specifically addressing depression in medical residents, data in pharmacy residents uses various metrics, including stress, anxiety, and burnout in addition to depressive symptoms or self-reported depression.5,6,8-11 The most recent and robust data in pharmacy residents uses depressive symptoms as a measurement of wellbeing, in contrast to even more recent studies in the pharmacy profession as a whole which use burnout.8,11,25-28 The inconsistencies in metric use regarding wellness in the literature may obfuscate the scope of the issue in pharmacy residents. Furthermore, the incidence of depression may be under-reported if residents don’t feel comfortable sharing experience with their RPDs. Therefore, RPDs may not be able to speak to the complete experience of the residents. However, the results from the study help establish that RPDs recognize that a problem does exist and outlines some resources currently utilized and future solutions to bring more awareness to the issues.
Conclusion
This qualitative study highlights multiple factors that could lead to depressive symptoms in residents, the most significant of which are workload and normalizing stress. The study emphasized the role RPDs can play in helping to manage resident workload by creating a structured residency year with clear expectations. Other supporting factors from RPDs can be communication, adaptability, and connecting with residents. Although RPDs are crucial stakeholders in providing a successful residency experience, a national conversation is needed to determine what residents can achieve within one year of residency training while maintaining wellness, as well as clarification of the role of the RPD in these issues. The accreditation agencies, academic societies, and residency sites should also be willing to invest in the RPDs and residents by providing resources and tools to recognize and mitigate depressive symptoms in residents in a timely manner to prevent future burnout.
Footnotes
Acknowledgement
This research was supported by an intramural grant from Roseman University of Health Sciences, College of Pharmacy. The authors would like to thank Anna Ferri, MLIS, Research and Learning Librarian at Roseman University, and Dr. Courtney Scott, PharmD, PGY1 pharmacy practice resident at Valley Hospital in Las Vegas, NV for their assistance in creating the figures for this manuscript.