
Abstract
Keywords
Background
Non-teaching community hospitals account for the majority of hospitals in the country, however they are under-represented in the stewardship literature.1-3 The community hospital antimicrobial stewardship literature that does exist mostly involves teaching community hospitals.3-7 The extent of antimicrobial stewardship program (ASP) implementation in community hospitals differs due to staffing and resource disparities, including financial limitations. 8 According to the CDC National Healthcare Safety Network (NHSN) in 2015, hospitals <200 beds vs >200 beds met all 7 “core elements” of antibiotic stewardship 49% vs 66%, respectively, but hospital teaching status was not assessed.9,10 Due to limited resources, smaller hospitals are also less likely to meet the pharmacy expertise “core element”. 9 Pharmacy faculty members, typically full-time employees at their respective university vs a paid hospital employee, are an available resource that provide a clinical service in exchange for precepting pharmacy students at the hospital. Community teaching hospitals have shown that the incorporation of advanced pharmacy practice experience (APPE) students, pharmacy residents, and infectious disease (ID)-trained pharmacists into ASP is beneficial.4-6 The addition of an ID-trained pharmacist faculty member and APPE students to a non-teaching community hospitals is a unique opportunity to expand ASP services at their institution, but there is a lack of literature available.11-14
Recently, Mount Sinai Queens (MSQ), a non-teaching urban community hospital, had an ID-trained, board-certified pharmacist faculty member from a local pharmacy school join the ASP team. MSQ has a typical daily census of 140-150 adult inpatients with no pediatric inpatient services. The emergency department has 70 beds and services both pediatrics and adults, and all traumas are transferred to another hospital in the health-system. The ID pharmacist faculty member precepts APPE students on 3 to 4, 5-week rotations per year. Prior to joining, MSQ predominantly had a prior authorization run stewardship program, where certain restricted antimicrobials required an ID-consult. The MSQ antimicrobial stewardship team consists of an ID physician lead of stewardship and infection control, two private ID physicians, a part-time (1 day per week) ID pharmacist from the Mount Sinai main campus, an infection control nurse, and a centralized microbiology team. The ID pharmacist faculty expanded the ASP to provide prospective audit and feedback services. We hypothesize that the addition of APPE students working with the ID pharmacist faculty can benefit an ASP at a non-teaching community hospital.
Methods
This was a single-center, retrospective chart review comparing antimicrobial stewardship interventions by an ID pharmacist faculty with and without APPE students from a local pharmacy school. Interventions were assessed for the first year the ID pharmacist faculty joined the antimicrobial stewardship team (January 16, 2020 to January 16, 2021), in accordance with The Icahn School of Medicine Institutional Review Board. All research was performed retrospectively, thus informed consent was not required. During the study period four APPE rotations occurred: three lasted the planned 26 business days and one only 18 business days, due to the start of the COVID-19 pandemic. The total number of business days with students vs without students, while accounting for vacation time was 96 vs 104 days, respectively. Each rotation had two to three APPE students. All APPE students were from the same private teaching university, which has about 200 students per graduating class. All APPE students were in their final year of pharmacy school. The first APPE student rotation also started on January 16, 2020.
Interventions were performed by prospective audit and feedback and patients were identified using positive blood culture reports via the clinical surveillance program, Vigilanz, and drug-specific reports via the electronic medical record, Epic. The pharmacist faculty alone performed interventions 2 days a week with a primary focus on positive blood cultures and patients on vancomycin due to high usage at the institution. Comparatively, APPE students performed interventions 5 days a week, with a primary focus on patients on vancomycin and ceftriaxone, since they are the most commonly-used non-restricted antibiotics. The pharmacist faculty continued to review positive blood culture patients while APPE students were on rotation and assigned those patients to students as the students progressed through rotation. Both the pharmacist faculty and APPE students’ typical hours were 8:30
An Epic report was used to collect details about interventions. Options for intervention type included add therapy, additional lab monitoring, allergy review, alternative agent recommended, broaden therapy, discontinuation of therapy, dose increase, dose decrease, drug information, intravenous (IV) to by mouth (PO) switch, pharmacokinetic (PK) monitoring, recommend culture, recommend ID consult, and streamline therapy. Any intervention that did not apply to one of these intervention types were classified as other. Additional lab monitoring was defined as any lab value except drug levels, which were considered PK monitoring. Prior to the ID pharmacist faculty joining the team antimicrobial pharmacokinetic monitoring and dose adjustments were performed by the ID physician. Drug information was defined as any additional literature/information that was shared with the provider to confirm therapy. Intervention documentation accuracy was verified via manual chart review by two PharmD students, which were then reviewed by the ID pharmacist faculty. A single intervention that was tagged to two antimicrobials were manually reviewed and separated into two interventions. Provider responses were categorized as accepted, rejected or not applicable if the antibiotic was discontinued or the clinical picture of the patient changed. Interventions were only considered accepted if the exact recommendation was followed. The patient location at time of intervention was categorized as medical floor, step-down, intensive care unit, emergency department, or outpatient. Outpatient interventions were defined if the intervention date was post-discharge and were predominantly positive blood culture follow-up by the ID pharmacist faculty. The presence of APPE students on rotation was defined based on the dates of rotation. The length of stay was calculated utilizing admission and discharge times.
Presence of an ID consult, and the order date and time of the antimicrobial intervened upon were obtained via manual chart extraction. If more than one order was present for the antimicrobial intervened upon, the older order time was utilized, unless the gap between orders was greater than 48 hours then the more recent order time was used. The time from antimicrobial order to intervention was then calculated. Antimicrobials intervened upon were categorized by class based on National Healthcare Safety Network (NHSN) antimicrobial use and resistance (AUR) module criteria. 15 We utilized NHSN criteria to align with current antimicrobial stewardship practices for tracking antimicrobial usage. Antimicrobials not included in NHSN criteria were classified as other. The top four antimicrobials utilized were separated out from the designated NHSN antimicrobial class. Antimicrobials were also categorized as restricted or non-restricted, as all restricted antimicrobials at MSQ require prior authorization via an ID consult from an ID physician. Restricted antimicrobials include amikacin, aztreonam, carbapenems, caspofungin, cefepime, ceftaroline, daptomycin, IV fluoroquinolones, IV fluconazole, linezolid, piperacillin/tazobactam, and voriconazole.
The primary endpoints were the rate of intervention, and the intervention acceptance rate, with and without APPE students on rotation. The intervention rate was calculated based on the number of working days for each group. Working days excluded weekends, holidays and vacation time taken by the ID pharmacist faculty. Secondary endpoints included the difference in the time from antimicrobial order to intervention and length of stay, as well as comparison of acceptance rates stratified by intervention type or the type of antimicrobial intervened upon with and without APPE students. Intervention responses classified as “not applicable” and interventions performed on outpatients were excluded from analyses of acceptance rates, as outpatient interventions were primarily blood culture follow-up and only performed by the ID pharmacist.
Differences between interventions by the ID pharmacist faculty with and without APPE students were assessed by chi-square or Fisher’s exact test for categorical variables and t-test for parametric continuous variables or Wilcoxon rank sum test for non-parametric continuous variables. A P-value < .05 was considered statistically significant. Analyses were conducted using R (version x64 4.0.3; R Foundation for Statistical Computing, Vienna, Austria). All data can be shared upon request.
Results
A total of 739 antimicrobial stewardship interventions were made during the first year the ID pharmacist faculty joined the stewardship team. There were 428 interventions with APPE students on rotation vs 311 without them. The number of weekly interventions by the ID pharmacist faculty with and without students are displayed in Figure 1. Students were present for a total of 96 working days compared to a total of 104 working days with only the ID pharmacist faculty present. The rate of intervention per working day for the ID pharmacist faculty with and without APPE students was 4.46 vs 2.99, respectively. No interventions occurred during August due to the ID pharmacist faculty’s vacation time. The student interventions were divided among 10 APPE students. Antimicrobial stewardship interventions from January 2020 to January 2021.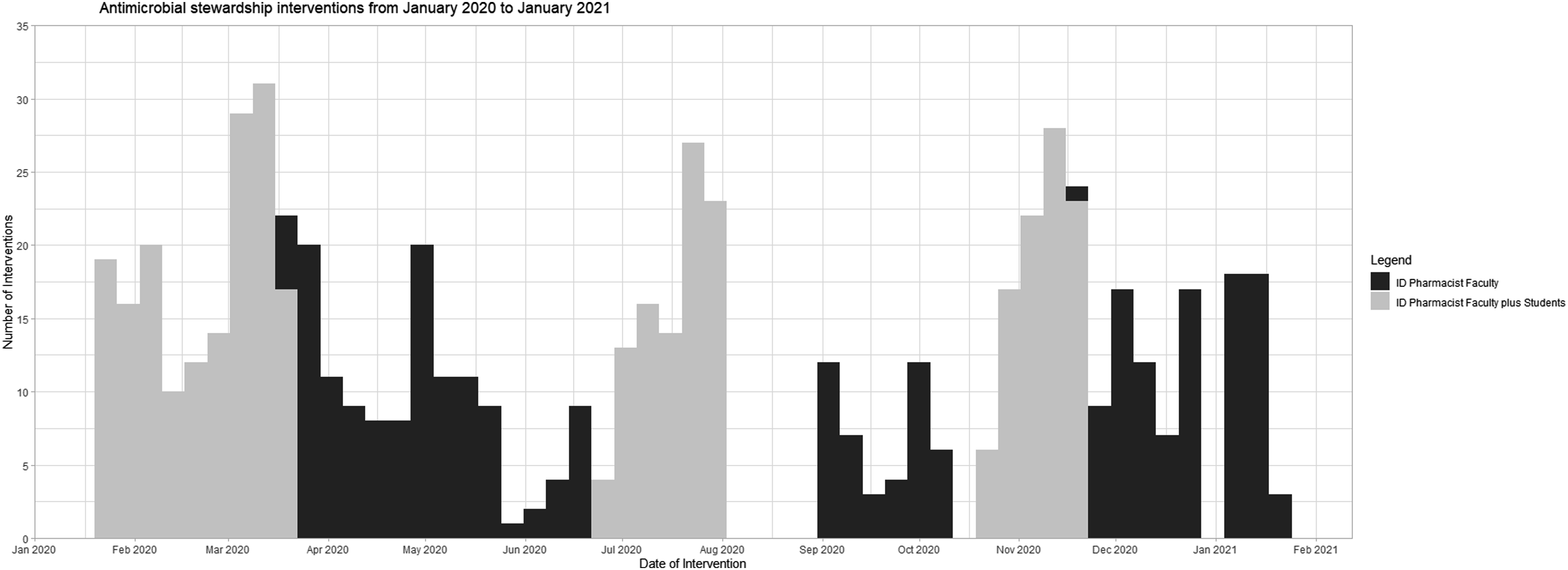
Antimicrobial Stewardship Interventions.
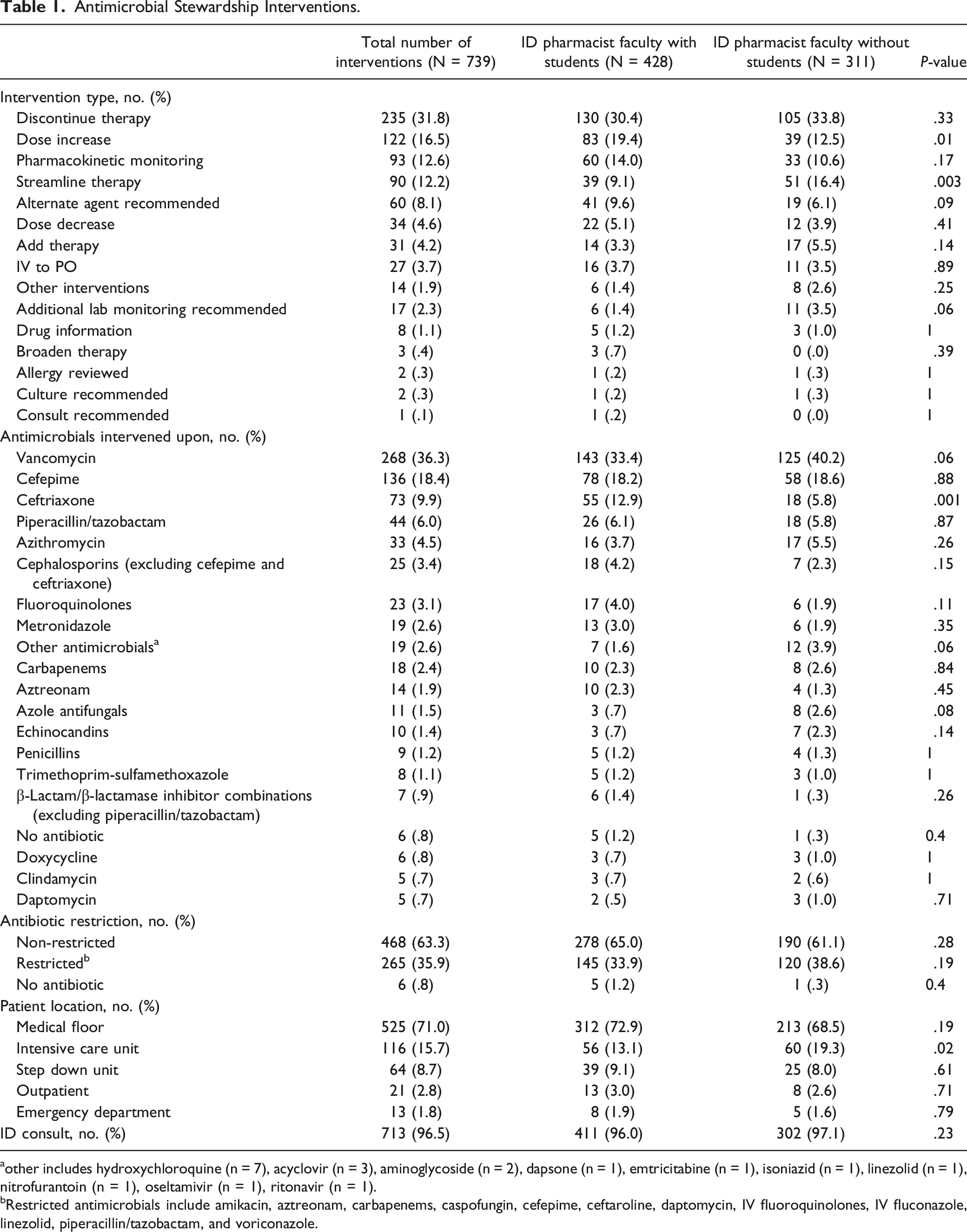
other includes hydroxychloroquine (n = 7), acyclovir (n = 3), aminoglycoside (n = 2), dapsone (n = 1), emtricitabine (n = 1), isoniazid (n = 1), linezolid (n = 1), nitrofurantoin (n = 1), oseltamivir (n = 1), ritonavir (n = 1).
Restricted antimicrobials include amikacin, aztreonam, carbapenems, caspofungin, cefepime, ceftaroline, daptomycin, IV fluoroquinolones, IV fluconazole, linezolid, piperacillin/tazobactam, and voriconazole.
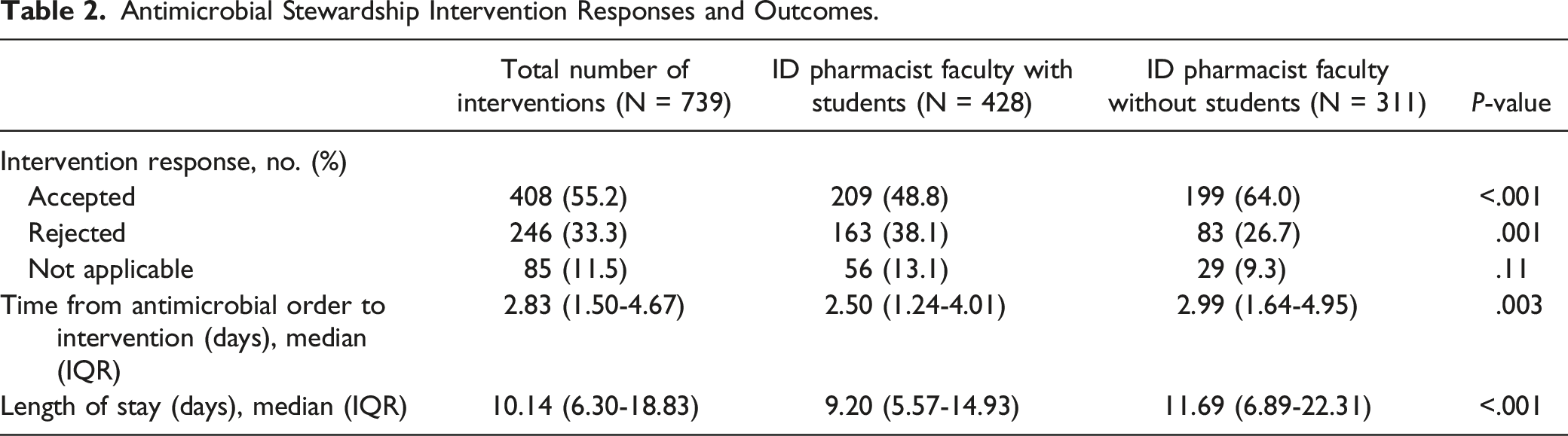
Antimicrobial Stewardship Intervention Responses and Outcomes.
Antimicrobial Stewardship Intervention Acceptance Rates by Intervention Type and Antimicrobial Intervened Upon. a
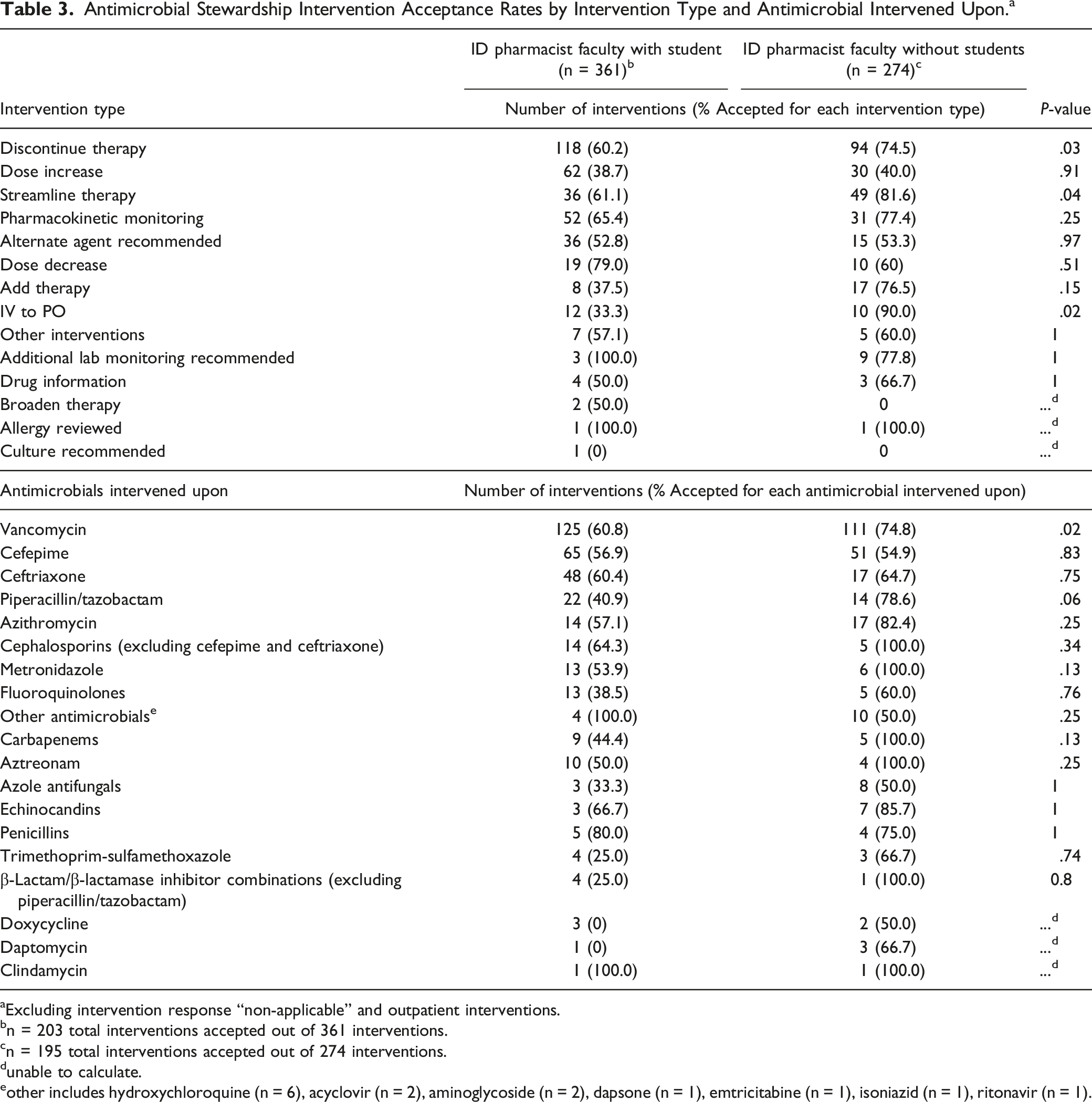
Excluding intervention response “non-applicable” and outpatient interventions.
n = 203 total interventions accepted out of 361 interventions.
n = 195 total interventions accepted out of 274 interventions.
unable to calculate.
other includes hydroxychloroquine (n = 6), acyclovir (n = 2), aminoglycoside (n = 2), dapsone (n = 1), emtricitabine (n = 1), isoniazid (n = 1), ritonavir (n = 1).
Discussion
We describe the impact of an ID pharmacist faculty member with and without APPE students on an antimicrobial stewardship team at a non-teaching community hospital. After one year with this expanded service, over 700 interventions were made, with more interventions being completed while students were on rotation. Pharmacist faculty members are usually not at their hospital sites full-time due to other college obligations, and at our institution they are only available 2 days a week for stewardship services. However, APPE students are present 5 days a week for stewardship services, which allows the faculty member to spread their 2 days of service over 5 days by reviewing all of the students’ recommendations with them daily and approving all interventions before they are made to the clinical teams. The extended service a faculty member with APPE students can provide is an excellent opportunity for facilities, including non-teaching community hospitals, to expand their stewardship services.
Previous studies describing stewardship initiatives for community hospitals should be interpreted while keeping in mind there are multiple definitions for both the terms “community hospital” and “non-teaching” hospital.16-18 We considered MSQ a non-teaching community hospital, per Becker’s Hospital Review, since MSQ is less than 550 beds and has “minimal” teaching programs.
Our reported overall intervention acceptance rate of 55.2% was lower than previously reported acceptance rates in the literature at community hospitals.4,12,13 A 545-bed community teaching hospital antimicrobial stewardship team that included APPE students, reported 554 interventions over a two year period (January 1, 2006 to December 31, 2007) with a 68.4% acceptance rate. 4 Recommendations were made verbally via rounds 3 days a week with an ID physician who would then write the recommendations in the medical record. 4 Similarly, a 155-bed non-teaching community hospital had an intervention acceptance rate of 73.9% after the first year of stewardship implementation. 12 Interventions were performed by rotating non-ID trained pharmacists and were reviewed on weekdays with a contract private ID physician. 12 All recommendations were made as a note in the medical record or a call to the ordering physician. 12 Our lower intervention rate may be due to use of secure chat instead of verbal recommendations. Since our institution is non-teaching, there are no rounding services for infectious disease or antimicrobial stewardship, and the ID pharmacist and students operate independently from the private ID physicians. It has previously been demonstrated that verbal stewardship recommendations significantly improve acceptance rates compared to notes in the medical record. 19 Our acceptance rate was also higher by the ID pharmacist faculty without students compared to with students. The ID provider’s lack of experience with the rotating students may have contributed. A qualitative interview of 134 Veteran Health Administration and 20 Intermountain Healthcare system hospitals assessing stewardship implementation, identified provider familiarity with the individual making the recommendation as a key to intervention acceptance. 20 As a result of our findings, we have made a point to ensure providers that all student interventions are first discussed with the ID pharmacist faculty. We also plan to formally introduce the APPE students to the ID provider to improve familiarity, as well as verbally discuss interventions with the ID consult physician as this has previously been shown to be more successful.
Despite APPE students’ lower acceptance rates, the students were able to provide more interventions than the pharmacist faculty alone and thus had a higher overall number of accepted interventions. The students also were able to intervene half a day earlier on antibiotic orders and were associated with a decreased length of stay. Similarly, a 41-bed non-teaching, long-term acute hospital added a 6-week ID APPE elective rotation where the APPE students performed prospective audit and feedback and met with their ID pharmacist and clinical pharmacist daily to develop recommendations. 11 The authors identified a trend towards decreasing length of stay (28.6 vs 31.4 days, P = .164) compared to two years prior to APPE student implementation. 11 Our shared observation of a decreased length of stay is limited by a lack of patient level data that may be confounding the outcome. Future studies are warranted to examine if there is a direct impact of antimicrobial stewardship in small non-teaching community hospitals on length of stay.
We also observed differences in the types of interventions as well as antimicrobials intervened upon by the ID pharmacist faculty with and without APPE students. The students more frequently recommended dose increases, which may be due to the fact that they are able to more closely monitor renal function on a daily basis compared to the ID pharmacist faculty that only provides service 2 days a week. We also observed that the ID pharmacist faculty performed more streamline therapy interventions without APPE students, which may be due to the pharmacist faculty’s focus on patients with positive blood cultures whose therapy can be streamlined when susceptibilities return. We saw that the students performed more interventions on patients receiving ceftriaxone, which is anticipated since the ID pharmacist faculty did not run ceftriaxone reports when students were not on rotation. We also anticipate that piperacillin/tazobactam and cefepime were top antimicrobials intervened upon even though they were targeted for review as they are commonly prescribed in conjunction with vancomycin.
Our study was limited by the retrospective design and that this was the first time for our institution to have a faculty member as well as APPE students. It was also particularly challenging to continue to implement a new stewardship service during the COVID-19 pandemic, which began during the third month of the ID pharmacist faculty joining the antimicrobial stewardship team. Additionally, we found that students were able to intervene on antimicrobials more quickly than the ID faculty member alone but this finding may be affected by interventions not being entered in real time. Further research is warranted to determine if the addition of APPE students impacts patient outcomes. Finally, our institution’s ID faculty member is a tenure-track faculty and therefore has fewer APPE student rotations as compared to non-tenure clinical faculty.
Conclusion
Due to resource limitations, non-teaching community hospitals often lack an employed ID-trained pharmacist. An ID-trained pharmacist faculty member with the addition of the APPE students offers non-teaching institutions a unique opportunity to expand their antimicrobial stewardship program. We found that the addition of APPE students increased the number of stewardship interventions, and was associated with decreased time from antimicrobial order to intervention as well as patient length of stay.
Footnotes
Acknowledgments
The information provided in this manuscript are those of the authors and do not necessarily reflect the position or policy of Mount Sinai Hospital System, or Mount Sinai Queens. We would like to thank Sara Farooqi and Lana Zaki for their assistance in preliminary data collection, and all APPE students for their participation on the antimicrobial stewardship team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.