
Abstract
Introduction
Diabetic ketoacidosis (DKA) is a life threatening emergency in patients with type 1 and type 2 diabetes defined by hyperglycemia, metabolic acidosis, and ketonemia. This metabolic emergency is driven by an absolute insulin deficiency and upregulation of counter regulatory hormones triggered by acute illness, trauma, or medication use or non-adherence. 1 DKA accounts for 500,000 hospital days and $5.1 billion annually in the United States with an increasing incidence over the past decade.1,2
Insulin is the mainstay of treatment in DKA with an American Diabetes Association (ADA) position statement recommending that patients either be started on an insulin infusion of .14 units/kg/h or administered a .1 units/kg bolus dose of insulin followed by a continuous infusion of .1 units/kg/h. 1 Despite the recommendation for an initial bolus of insulin and a theoretical benefit in overcoming insulin resistance in DKA, the data to support this practice are limited.1,3,4 Specifically, previous studies have failed to show a benefit of an initial insulin bolus in reducing time to resolution of DKA or shortening length of stay.5-7
In addition to lack of demonstrated benefits with using an initial insulin bolus, there are concerns regarding the safety of this practice due to potential risk of causing hypoglycemia and hypokalemia. Furthermore, the use of an initial insulin bolus has been recommended against in high risk patients such as pediatrics and those with end stage renal disease (ESRD) based on the potential to cause overly rapid blood glucose (BG) correction leading to cerebral edema and hypoglycemia respectively.8-10 The safety of an initial insulin bolus has been evaluated in the general DKA population without clear evidence of harm compared to infusion alone.5-7 Goyal et al. evaluated rates of hypoglycemia in patients receiving an initial insulin bolus compared to an insulin infusion alone and found an increased rate of hypoglycemia (6.4% vs 1.3%, P = .12) that was not statistically significant. This study also failed to find a reduction in time to DKA resolution or hospital discharge. 6
Hypoglycemia is only one complication with the potential to interfere with the treatment of DKA. Hypokalemia due to excretion of potassium secondary to diuresis and intracellular shifting of potassium with high doses of insulin can lead to significant morbidity and interruptions in treatment.1,11 Brown et al. found a numerically higher incidence of hypokalemia in patients not given a bolus compared to those who received an initial insulin bolus (16% vs 29%, P = .65) although this study evaluated patients throughout their entire hospitalization which may not be indicative of the effect of the insulin bolus. 7 Complications associated with the management of DKA are well documented however the contribution of an initial insulin bolus to the development of hypokalemia and hypoglycemia has not been adequately evaluated.
The purpose of this study is to evaluate the overall safety of an initial insulin bolus in the treatment of DKA compared to an insulin infusion alone in terms of rate of hypoglycemia, hypokalemia, and interruption in insulin infusion while also evaluating the impact on resolution of DKA and length of intensive care unit (ICU) and hospital length of stay with either strategy.
Materials and Methods
This was a retrospective, single-center, observational study comparing patients presenting to the emergency department (ED) in DKA between September 1, 2019 and August 31, 2020 being treated with either an initial insulin bolus followed by a continuous insulin infusion or an insulin infusion without an initial bolus. Patients were eligible for inclusion if they were at least 18 years of age, presented to the ED, and met the clinical criteria for DKA including the presence of hyperglycemia (BG >250 mg/dL), ketonemia as determined by measured beta-hydroxybutyrate concentration, and metabolic acidosis as determined by anion gap calculated from initial basic metabolic panel. In our ED, DKA is treated based on an order-set and protocol to guide fluid resuscitation, electrolyte repletion, and insulin titration. Patients are generally started on insulin infusions at .1 units/kg/h with the addition of an initial insulin bolus or alteration from recommended initial insulin dose at the physician’s discretion. An insulin bolus was defined as a dose of intravenous (IV) regular insulin or subcutaneous (SC) regular insulin or rapid acting insulin analogs prior to starting a continuous IV administration of regular insulin. Subcutaneous administration was included as patients occasionally receive an initial insulin dose prior to a full set of lab values being available to determine whether patient is in DKA and in need of an IV insulin infusion. While SC insulin may have delayed onset compared to IV administration, SC insulin has been used in the treatment of DKA and would be expected to have an appreciable effect on the treatment time for DKA as well as safety parameters, such as blood glucose and potassium, evaluated in this study. Electrolytes are monitored every 4 to 6 hours and repleted at the discretion of the physician. Insulin is titrated by nursing staff based on an electronic health record-based calculator to maintain a steady reduction in glucose of 50-75 mg/dL/h by recommending 20% increases or decreases in insulin infusion rate. Supplemental dextrose boluses are available for all patients as standing orders to be administered as needed for BG <70 mg/dL and dextrose containing fluids available once patient glucose is < 250 mg/dL while still needing to be on an insulin infusion. Patients on insulin infusions are managed in the ED and ICU setting with insulin infusion transitioned to SC by the physician once metabolic acidosis, ketonemia, and hyperglycemia have resolved.
Patients were excluded from this study if they were less than 18 years of age, pregnant, or ESRD on hemodialysis (HD) as bolus dose is not recommended in these populations, had an initial elevated potassium (K+ >5.5 mEq/L) that would necessitate a bolus dose of insulin for hyperkalemia, or those treated with an insulin infusion for a diagnosis other than DKA such as hyperosmolar hyperglycemic syndrome. Patients were identified based on receiving insulin infusions in the ED within the study period and eligibility was further determined through manual chart review. Patient protected health information was secured in a password protected database.
The primary outcome of this study was a composite of complications associated with insulin therapy occurring within eight hours of starting the insulin infusion. Complications included in the composite were hypoglycemia defined as BG <70 mg/dL, hypokalemia defined as K+ ≤3.3 mEq/L, and interruption in insulin infusion within eight hours of initiating the insulin infusion. Interruption in insulin infusion was included to account for patients with impending hypoglycemia or hypokalemia leading to insulin being held as an interruption in insulin therapy would potentially delay DKA resolution. The composite primary outcome was evaluated up to eight hours from initiation of the insulin bolus or infusion to ensure that the complications evaluated would be related to the use or lack of use of an initial insulin bolus rather than continued DKA management. Eight hours was selected as the time point for the primary outcome to provide two sets of lab values with which to evaluate for hypokalemia based on our institutional protocol of checking labs every four hours in these patients. Secondary outcomes included each of the individual above complications as well as time to resolution of DKA defined as anion gap <15 mEq/L and BG <250 mg/dL, which match the institutional protocol for transitioning patients off the insulin infusion. Time to discontinuation of insulin infusion, time to discharge from the ICU, and time to discharge from the hospital were also evaluated as secondary outcomes.
Non-normally distributed continuous data including time to resolution, discontinuation of insulin infusion, discharge from ICU, and discharge from hospital were analyzed using Wilcoxon-Rank Sum test and nominal data including baseline characteristics, primary outcome, and individual complications were analyzed by Chi-square tests except for incidence of hypoglycemia which was analyzed using Fisher’s exact test based on low incidence.
This project was formally determined to be quality improvement, not human subject research, and was therefore not overseen by the Institutional Review Board per institutional policy. The protocol was accepted by the institution’s Chief Quality Determination Reviewer. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Results
Between September 1, 2019 and August 31, 2020, 271 patients were identified as being started on an insulin infusion with 167 patients meeting inclusion criteria. Reasons for exclusion are listed in Figure 1 with the majority of patients excluded for elevated initial potassium (n = 41), history of ESRD on HD (n = 14), and insulin infusion treating an alternative diagnosis to DKA (n = 45). Flow Chart of Inclusion and Exclusion Criteria. DKA – diabetic ketoacidosis, ED – emergency department, ESRD – end-stage renal disease, HD – hemodialysis, K+ - potassium.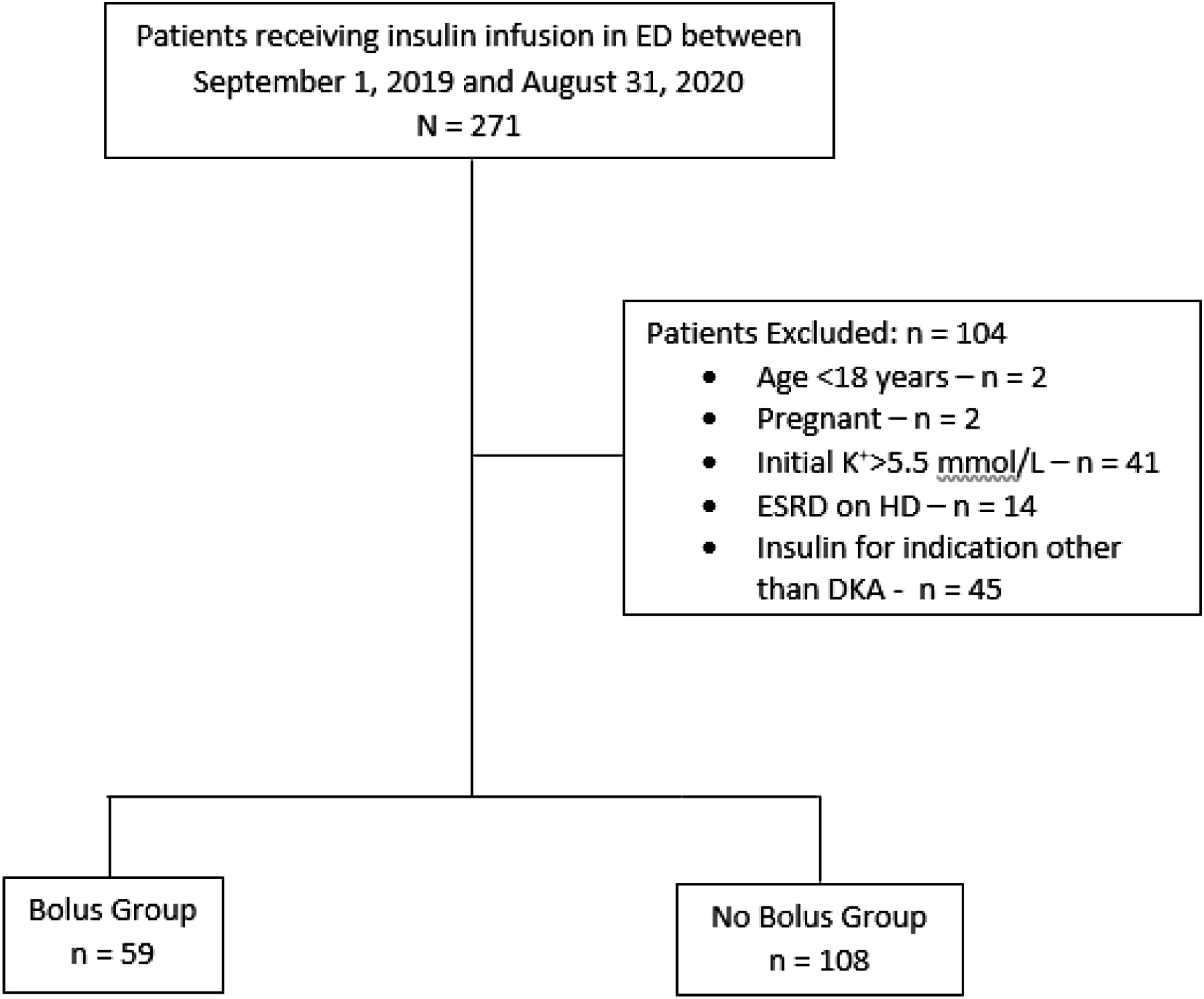
Baseline Characteristics.
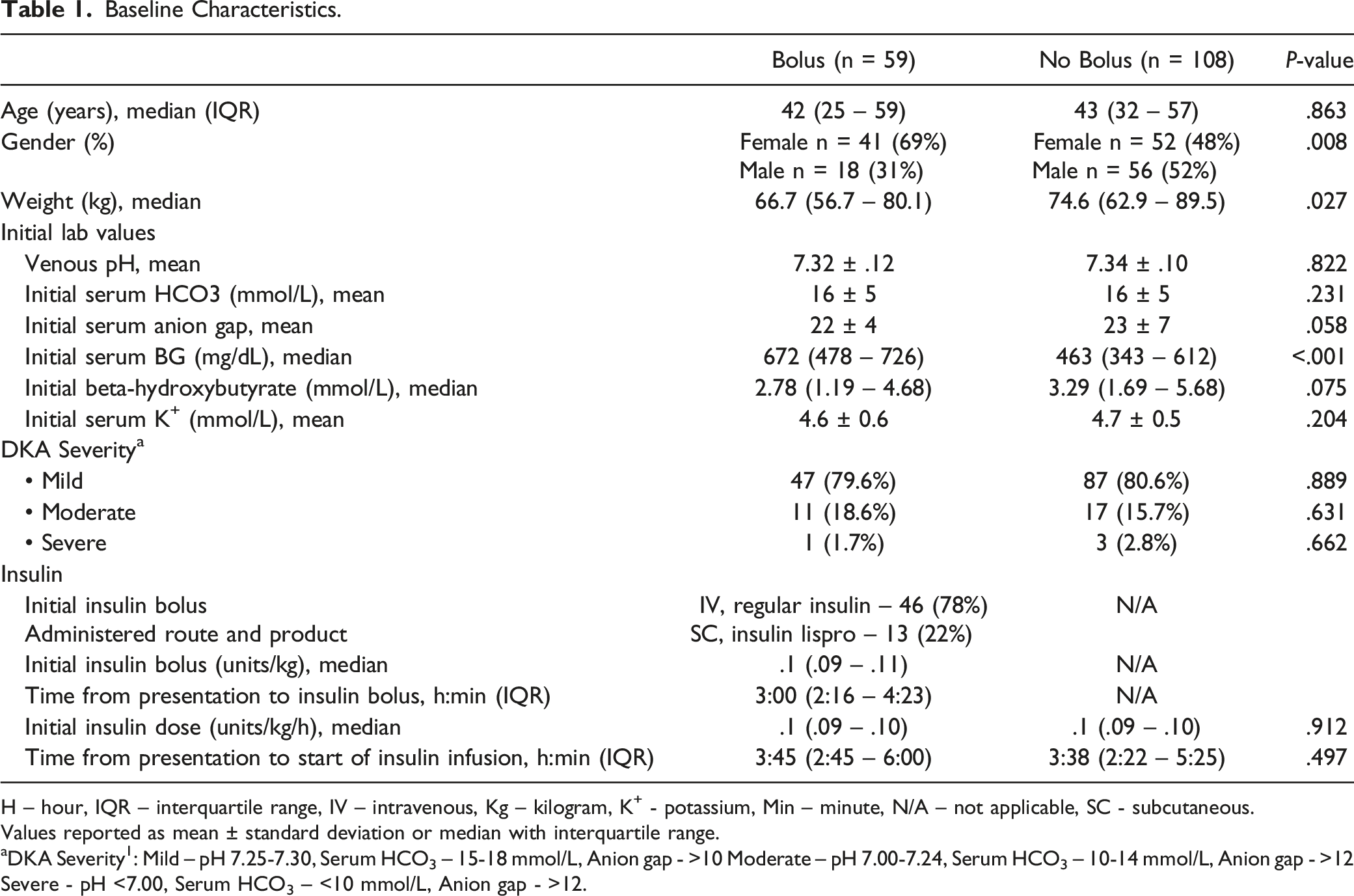
H – hour, IQR – interquartile range, IV – intravenous, Kg – kilogram, K+ - potassium, Min – minute, N/A – not applicable, SC - subcutaneous.
Values reported as mean ± standard deviation or median with interquartile range.
aDKA Severity 1 : Mild – pH 7.25-7.30, Serum HCO3 – 15-18 mmol/L, Anion gap - >10 Moderate – pH 7.00-7.24, Serum HCO3 – 10-14 mmol/L, Anion gap - >12 Severe - pH <7.00, Serum HCO3 – <10 mmol/L, Anion gap - >12.
Results.
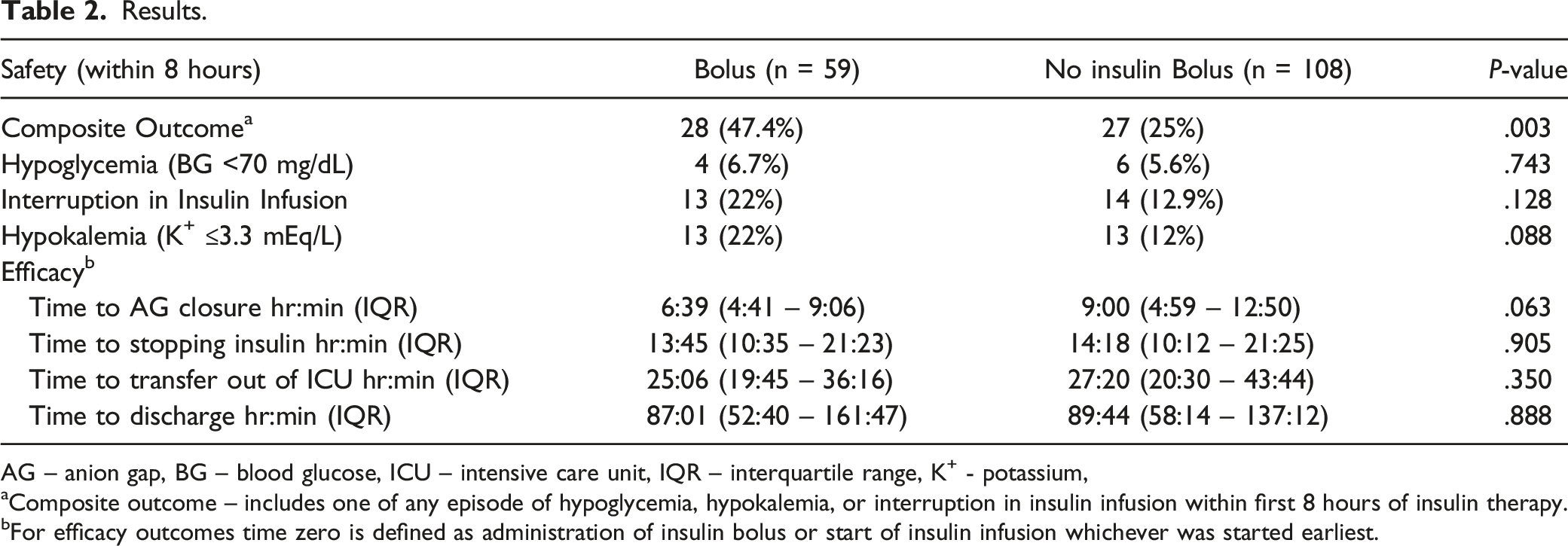
AG – anion gap, BG – blood glucose, ICU – intensive care unit, IQR – interquartile range, K+ - potassium,
aComposite outcome – includes one of any episode of hypoglycemia, hypokalemia, or interruption in insulin infusion within first 8 hours of insulin therapy.
bFor efficacy outcomes time zero is defined as administration of insulin bolus or start of insulin infusion whichever was started earliest.
Patients who received an initial insulin bolus were shown to have more rapid correction in their anion gap and resolution in their DKA (6:39 vs 9:00, P = .063) although this finding was not statistically significant. This more rapid correction in DKA did not lead to a significant difference in time on the insulin infusion (13:45 vs 14:18, P = .905), time to ICU discharge (25:06 vs 27:20, P = .350), or time to hospital discharge (87:01 vs 89:44, P = .888) (Table 2).
Discussion
Insulin is a cornerstone of treatment in DKA; however, despite decades of experience with using insulin for this indication, controversy remains regarding most appropriate dosing and administration. The ADA position statement on DKA recommends using an initial insulin bolus followed by a continuous insulin infusion as an option for the initial management of DKA yet this recommendation lacks clinical evidence to support it. 1 The basis for this recommendation stems from a theoretical benefit of higher insulin doses being able to overcome insulin resistance that standard infusion doses cannot, as well as potential for faster resolution of DKA, less time in intensive care, and more rapid discharge.1,3,4 In addition to proposed benefits of an initial insulin bolus there are also recognized complications including hypoglycemia, hypokalemia, and necessary interruptions in insulin therapy.6-9 This study adds to the body of literature questioning the continued practice of an initial insulin bolus in the treatment of DKA while also evaluating potential harms and complications an initial insulin bolus can cause early on in the treatment of this population.
This study provides evidence that, within the initial eight hours of treatment, an insulin bolus given with a continuous insulin infusion leads to significantly more hypoglycemia, hypokalemia, and interruptions in therapy compared to an insulin infusion alone. Previous studies have found conflicting results when evaluating potential harms associated with an initial insulin bolus.5-7 Goyal et al. evaluated the safety and efficacy of an initial insulin bolus in the treatment of DKA and found a numerically higher rate of hypoglycemia (6.4% vs 1.3%, P = .12) that was not statistically significant, likely due to low overall incidence and a small sample size. 6 Brown et al. similarly evaluated the safety of efficacy of an initial insulin bolus and found no significant difference in rates of hypoglycemia (2% vs 7%, P = .64) or hypokalemia (16% vs 29%, P = .65). However, hypoglycemia and hypokalemia were considered throughout the hospitalization which may be indicative of continued management of DKA rather than a specific effect of an initial bolus. 7 Whereas these previous studies focused on a single complication of insulin 6 or the complication rate throughout the hospitalization 7 we believe our study captures the true incidence of complications associated with an initial insulin bolus by considering a variety of potential issues as well as focusing our evaluation only during the initial eight hours of therapy when the insulin bolus would be expected to be contributing most to these complications.
Although limited as a retrospective study, our data is in line with previous evidence failing to demonstrate a benefit of an initial bolus on reducing time to resolution of DKA, time in the ICU, or time to discharge. Kitabchi et. al. found that while an initial insulin bolus achieved therapeutic insulin concentrations faster than no bolus, this difference was not significant after 60 minutes nor was the faster time to therapeutic insulin concentration associated with improved time to resolution of DKA. 5 Goyal et. al. and Brown et. al. similarly failed to show a reduction in overall length of stay comparing patients receiving an insulin bolus to those being managed with an infusion alone.6,7 Our study did indicate a small reduction in time to resolution of DKA of approximately two and a half hours. Due to the retrospective nature of this study it is unclear if this reduction represents true clinical benefit of an initial insulin bolus or a product of when the follow up lab values were evaluated. These results carried forward through time on insulin, time in ICU, and time to discharge; however, these reductions cannot be considered statistically or clinically significant. The lack of clinical benefit of an initial insulin bolus can be attributed to the fact that DKA requires a prolonged treatment beyond the effects of a single insulin dose and time to resolution of DKA may be impacted more through continued management and titration of insulin, fluids, and electrolytes.
Limitations
One limitation of this study was the non-randomized cohort design. Group assignments were determined by physician preference which may have introduced confounding into the treatment assignments. While the two groups were well matched in baseline characteristics, this confounding can be seen in the significantly higher initial BG values of the bolus insulin group. The retrospective study design also limited our ability to accurately evaluate endpoints such as hypoglycemia, hypokalemia, and time to resolution of DKA as our determination of these values and time points were based on when labs were drawn which may have led to omission of hypoglycemic or hypokalemic episodes or delays in recognition of DKA resolution. The majority of our patient population was considered to have mild DKA which limits our ability to make conclusions on the role of an initial insulin bolus in more severe DKA populations. Further studies are needed to specifically evaluate the associated benefits and complications of these populations. Finally, deviations from the DKA protocol in terms of insulin titration, fluid administration, and electrolyte replacement were not captured in this study and may have contributed to increased complications in one or both groups. The impact of protocol deviations on safety endpoints was limited in our evaluation by only evaluating the initial eight hours of therapy. Protocol deviations may still have occurred during the treatment course and impacted time to discontinuation of insulin infusion, transferring out of the ICU, and discharge from the hospital however would be expected to have occurred similarly in both groups.
Conclusion
In this study, the administration of an insulin bolus plus a continuous insulin infusion was associated with an increase in hypoglycemia, hypokalemia, and interruption in insulin therapy within the initial eight hours of therapy compared to starting an insulin infusion alone and did not lead to faster resolution of DKA in our population. Further randomized controlled trials are needed to evaluate whether there is a benefit of an initial insulin bolus in any subset of DKA patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.