
Abstract
Introduction
Trauma remains one of the most common reasons for emergency department (ED) visits, with 25% of all visits being injury-related. 1 Among those admitted after trauma, untreated pain remains a concern among both patients and providers. Inadequate control of constant and intermittent pain is associated with increased morbidity, hospital length of stay, and health care costs.2,3 While approximately 20% of trauma patients report pre-injury opioid use, prescribing in the opioid-naïve patient brings forth new concerns for abuse, misuse and dependence.4,5 Furthermore, in-hospital opioid prescribing for acute pain and failure to discontinue at discharge may inadvertently lead to chronic opioid use. 6
Trends in opioid prescribing have fluctuated over the last two decades. 7 Opioid prescribing at ED discharge has decreased (2010-2017, 14.6% vs 2006-2011, 19.0% to 21.5%), although hospital opioid prescribing at discharge remains high, particularly after trauma. 8 A study by Chaudhary and colleagues 9 found the incidence of hospital opioid prescribing at discharge after traumatic injury to be 54.3%. Despite decreases in opioid prescribing following implementation of safe prescribing practices, the incidence of drug overdose deaths in the United States exceeds 100,000 annually.10-15 In 2019, over 70% of drug overdose deaths involved an opioid and nearly three-quarters of opioid-involved overdose deaths involved a synthetic opioid. One-fifth of patients who receive their first opioid prescription will receive additional opioid prescriptions thereafter. 16
The American College of Surgeons Best Practice Guidelines for Acute Pain Management in Trauma Patients recommends multimodal analgesia. 17 While implementation of non-pharmacologic strategies (e.g., temperature therapy, massage therapy, immobilization) is important, patients often require pharmacologic agents. Non-opioid analgesics such as acetaminophen (APAP) and nonsteroidal anti-inflammatory drugs (NSAIDs) should be prescribed for most patients unless contraindicated. In select patients, alternative or adjunctive non-opioid analgesics (e.g., skeletal muscle relaxants, N-methyl D-aspartate (NMDA) antagonists, gabapentinoids) may reduce pain severity and decrease opioids requirements. 18 When non-pharmacologic and non-opioid analgesics are insufficient, opioids remain the mainstay for the treatment of trauma-related pain. Among those requiring opioids, multimodal analgesia is crucial to reduce opioid requirements. A 2020 study by Harvin et al, 19 compared two multimodal pain regimens in trauma patients. Those who received the multimodal analgesic strategies for trauma patients (MAST), had lower median morphine milligram equivalents (MME) per day [34(15-61) vs 48 (22-74, P < .001] and fewer opioids prescribed at discharge (62% vs 67%; P = .029). In an earlier study by Hamrick et al, 20 similar results were seen when evaluated the effect of implementing a multimodal pain management order set. This study found a statistically significant reduction in oral morphine equivalents in the post-implementation group [125.6(45.0- 415.0) vs 481.5(174.8-881.3) mg, P < .001].
Efforts to reduce in-hospital and discharge opioid prescribing remain a focus for health care institutions. St. Joseph’s Health developed the Alternative to Opioids Program (ALTOSM), a comprehensive evidence-based multimodal opioid-sparing approach to pain management in January 2016. 21 The program launched as an ED initiative and included multidisciplinary training of pharmacists, nurses, and physicians. The purpose of this program was to provide an opioid-sparing algorithm for acute pain management to providers and encourage use of non-opioid or alternative analgesics (e.g., soft tissue injections, joint injections, and ultrasound-guided regional anesthesia). Following implementation of ALTOSM, a 50% reduction in ED opioid and 82% reduction in ED opioid prescribing at discharge was observed. 22 While ALTOSM effectively reduced ED opioid use, its effects on hospital opioid prescribing at discharge are unknown. The purpose of this study was to determine if a hospital-wide ALTOSM program reduced opioid prescribing in hospital and upon discharge after trauma.
Methods
This was an institutional review board approved single-center, retrospective cohort of patients ≥18 years old admitted for ≥24 hours admitted with a primary diagnosis of traumatic injury between August 1, 2018 and October 30, 2019. Patients with a history of alcohol use disorder or polysubstance abuse, chronic opioid use, and mortality prior to hospital discharge were excluded. Alcohol use disorder was defined as documented use (i.e., patient report, positive blood alcohol level on admission >10 mg/dL) or history of use (i.e., documented in electronic medical record, previous positive blood alcohol level). Polysubstance abuse was defined as documented use (i.e., patient report, positive urine toxicology screen on admission) or history of use (i.e., documented in electronic medical record, previous positive urine toxicology screen). A seven-panel urine toxicology screen assessed for the presence of amphetamines, barbiturates, benzodiazepines, tetrahydrocannabinol, cocaine, opiate, and phencyclidine. Chronic opioid use was defined as current use (i.e., patient reported currently prescribed opioids for chronic pain, opioids in prescription fill history or admission/discharge medication reconciliations within the last 6 months) or history of use (i.e., chronic use of opioids or documented use of opioids in electronic medical record).
ALTOSM was launched at St. Joseph’s Health in January 2016. Until July 1, 2019, ALTOSM was used solely in the ED to reduce opioid prescribing in the ED and at ED discharge. Thus, admissions prior to July 1, 2019 represent the control group (Pre-ALTO). Admission after July 1, 2019 therefore represent the hospital-wide ALTOSM program (Post-ALTO). Admitted trauma patients included those requiring general floor and intensive care unit management. General floor admissions were managed by the trauma service. All critically ill patients were admitted to a combined Surgical/Trauma/Neurological ICU and managed by the ICU team. Eligible patients were identified using the institution’s trauma registry. Electronic medical records were reviewed for exclusion criteria. Past medical history was obtained using admission history, documentation from prior hospitalizations, and the diagnosis and problem list within the electronic medical record.
Patient demographics and the following were collected: injury type, injury mechanism, initial Injury Severity Score (ISS), Charlson Comorbidity Index (CCI), need for surgery, intensive care unit (ICU) admission, and hospital and ICU length of stay (LOS). Injury type included blunt, penetrating, or unknown. Injury mechanism was categorized as fall, collision, assault, stab or gunshot wound, or other. Collision included bicycle collision, motorcycle collision, motor vehicle collision or pedestrian struck. Surgery was defined as the need for surgery during hospitalization. All LOS and other durations were calculated as calendar days. The primary outcome was the incidence of opioid prescribing at hospital discharge Pre- and Post-ALTO. Secondary outcomes were the percent of patients with in-hospital opioid, non-opioid and multimodal analgesia, and hospital and ICU LOS.
Non-opioid analgesics included APAP, NSAIDs, topical analgesics, local anesthetics, skeletal muscle relaxants, or gabapentinoids. Analgesic class, drug, dose, frequency, or duration were not collected. Opioids prescribed in-hospital and at discharge were identified using the Drug Enforcement Administration (DEA) lists of controlled substance scheduled class II, III, and IV opioids (e.g., morphine, oxycodone, hydromorphone, fentanyl). 23 In-hospital opioid prescribing was defined as any patient that had an active opioid order during hospitalization. Discharge opioid prescribing included patients who received a prescription for an opioid at discharge, had opioids included in the discharge medication reconciliation or had an opioid in their prescription fill history within 1-week after hospital discharge. Opioid agent, dose, frequency, duration, administration date or time, or MMEs were during hospitalization not collected. Use of discharge prescription, including number of doses or refills used, following discharge was also not collected. Multimodal analgesia was defined as patients who had orders for both opioid and non-opioid analgesics concurrently.
Statistical Analysis
Demographic factors and clinical characteristics were summarized with counts and percentages for categorical variables. Continuous variables were summarized using means and standard deviations for normally distributed variables, and medians and interquartile ranges for non-normally distributed variables. Microsoft Excel Tool Pak 2015 and R version 4.02 were used for data analyses. Binary variables were evaluated with logistic regression, whereas continuous variables were assessed using a pairwise student t-test or ANOVA analysis for secondary outcomes. Multivariate logistic regression was used to evaluate differences between subgroups. Subgroup analyses to identify increased odds of the primary outcome evaluated included age (< 30 vs ≥ 30 years old), ICU admission, surgery, injury severity (ISS < 9 vs ≥ 9), and disease severity (CCI ≤ 1 vs > 1). Significance was defined as P ≤ .05. A Post-ALTO sample size of 129 patients was calculated to observe a 30% reduction in primary outcome and maintain 80% power to detect a statistically significant difference using alpha <.05.
Results
Patient Demographics.
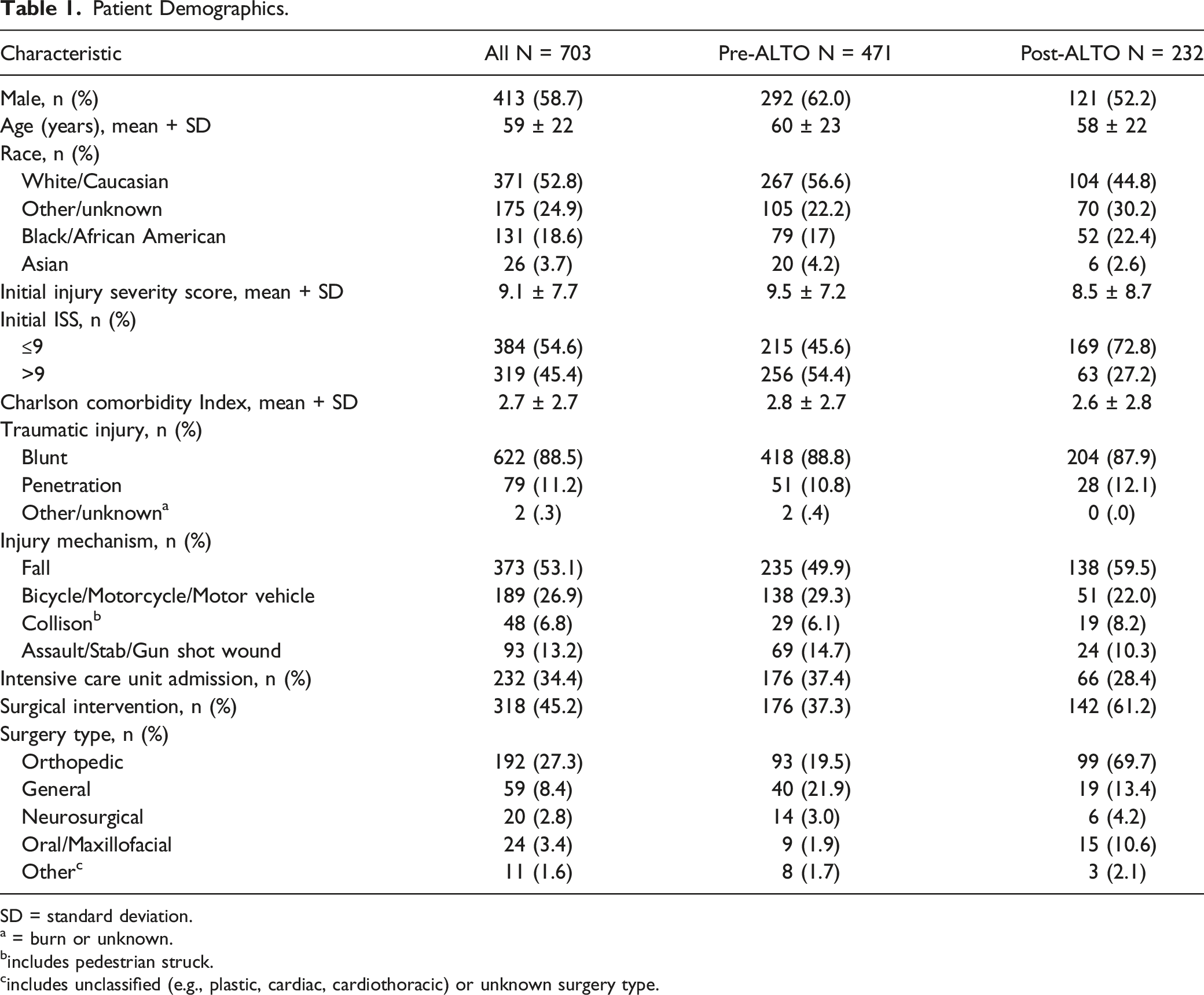
SD = standard deviation.
a = burn or unknown.
bincludes pedestrian struck.
cincludes unclassified (e.g., plastic, cardiac, cardiothoracic) or unknown surgery type.
Overall, opioid prescribing at hospital discharge occurred more often in the Post-ALTO group (132/332, 39.4% vs 90/203, 43.8%; P = .1237) (Figure 1). During hospitalizations, more patients in the Post-ALTO group were prescribed opioid (332/471, 70.4% vs 203/232, 87.5%, P < .0001) and non-opioid (441/471, 93.6% vs 229/232, 98.7%; P = .0027) analgesics. The percent of patients prescribed multimodal analgesia during hospitalization was similar between groups (397/471, 84.3% vs 203/232, 87.5%; P = .2591). In-Hospital Analgesic Prescribing.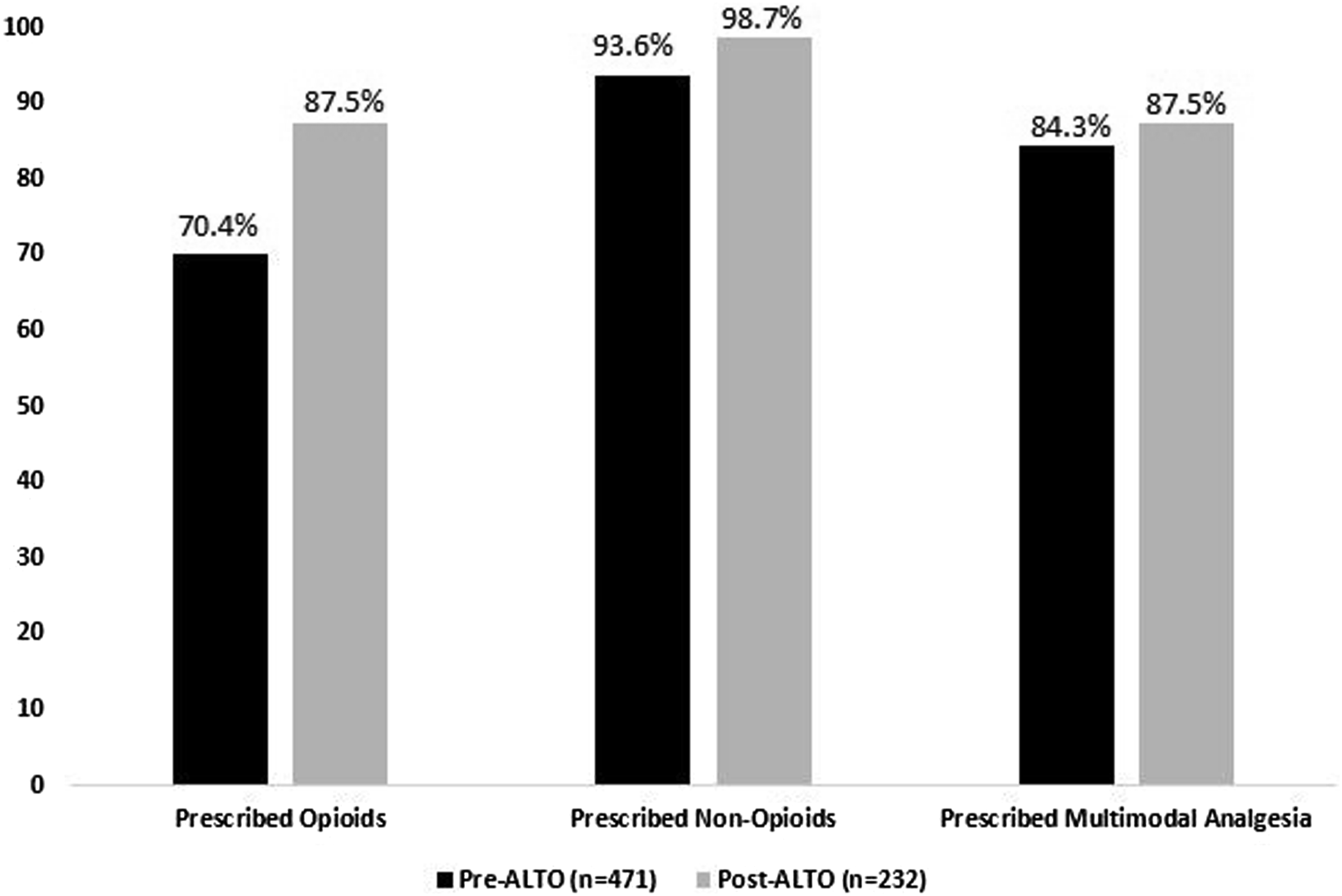
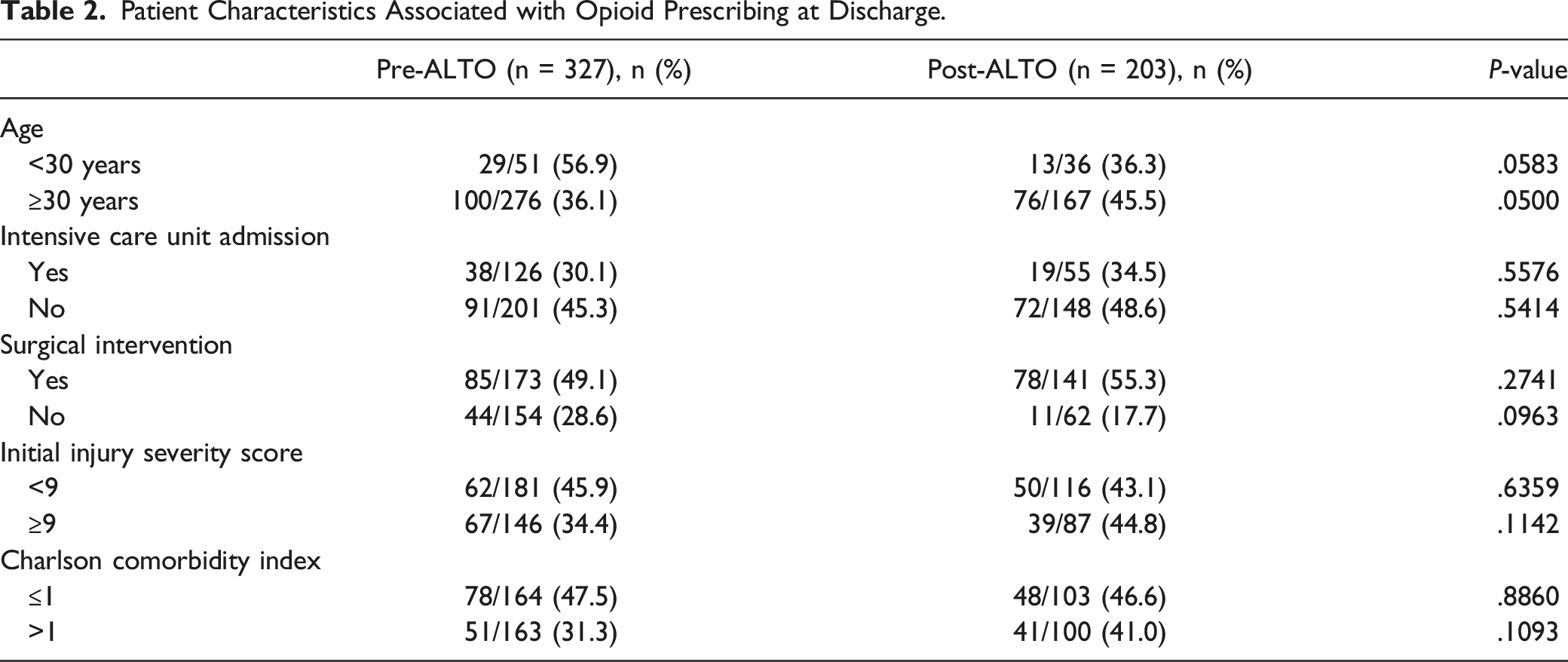
Patient Characteristics Associated with Opioid Prescribing at Discharge.
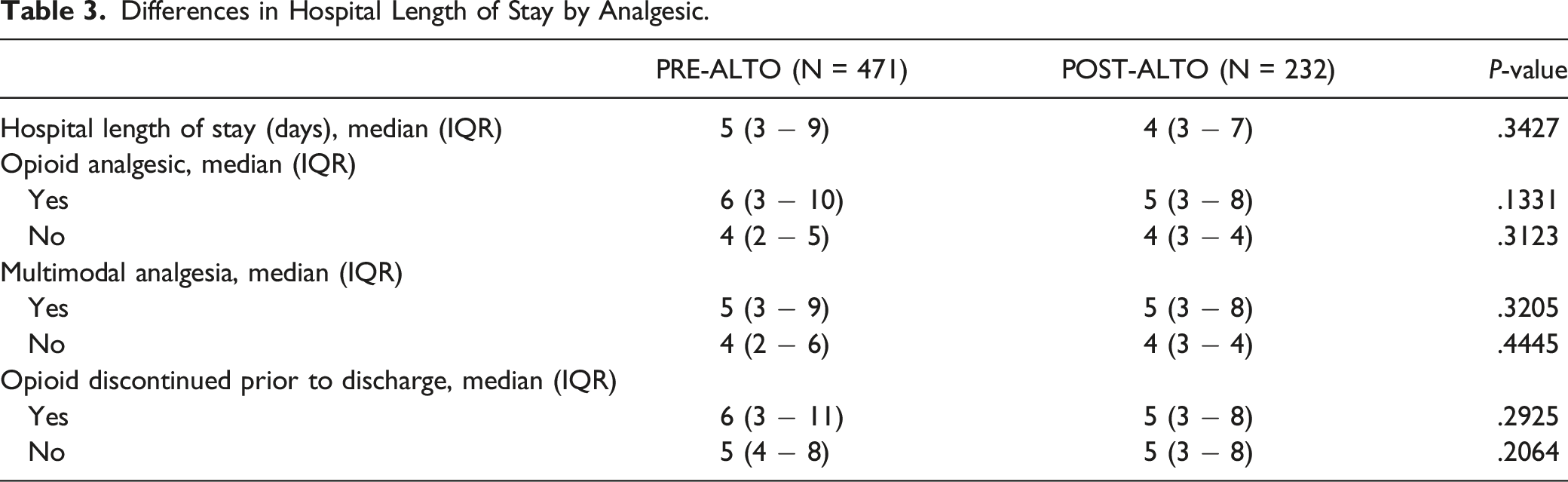
Differences in Hospital Length of Stay by Analgesic.
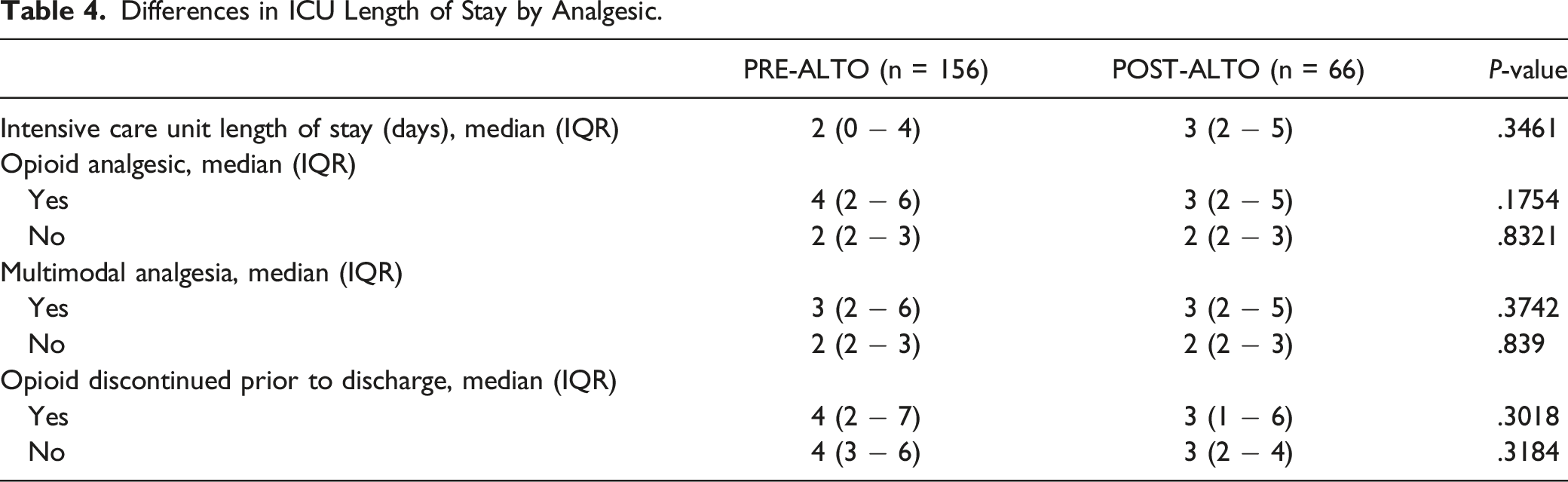
Differences in ICU Length of Stay by Analgesic.
Discussion
Trauma remains one of the most common reasons for emergency department (ED) visits and often result in pain. 1 Untreated pain is associated with consequences (e.g., increased morbidity, hospital length of stay, and health care costs); meanwhile opioid prescribing is of particular concern in the 80% of trauma patients whom are opioid-naïve. 2 ALTOSM, a comprehensive evidence-based approach to pain management, offers providers a multimodal opioid-sparing algorithm for acute pain management and encourages use of non-opioid or alternative analgesics. 21 This study evaluated in-hospital and discharge opioid prescribing among opioid-naïve trauma patients following implementation of a hospital-wide ALTOSM program.
Three-quarters of all patients evaluated in this study were prescribed opioids during hospitalization. Among those with in-hospital opioid prescribing, approximately 40% were prescribed opioids at hospital discharge. While the goal of ALTOSM is to provide an opioid-sparing strategy to pain management after trauma, more patients received opioids during hospitalization and at hospital discharge after implementation. Several factors may have contributed to increase opioid prescribing. First, incorporation of opioids into ALTOSM order sets in the electronic medical record may have inadvertently increased the rate of opioid prescribing. Second, the Post-ALTO group was evaluated immediately following implementation of the ALTOSM program hospital-wide thus may not reflect current prescribing practices. Third, there was a substantially higher rate of surgical interventions in our Post-ALTO group. Recognizing the increased prescribing of opioids among those undergoing surgery, as observed in this study, may have contributed to increases in in-hospital and discharge opioid prescribing. Despite this, the rate of opioid prescribing at hospital discharge after trauma remains lower than previously reported. Contrarily, ALTOSM was associated with an increase in non-opioid and multimodal analgesia prescribing. While drug, dose, duration, administration or MME were not evaluated in this study, it is possible that increased non-opioid and multimodal analgesia prescribing reduced overall opioid consumption.
Additional analysis of the primary outcome aimed to determine which patient specific variables were associated with increased opioid prescribing at discharge. In both the Pre- and Post-ALTO groups, lack of ICU admission, need for surgery and CCI ≤ 1 were associated with increased opioid prescribing at hospital discharge. While ICU admission often goes hand-in-hand with disease severity, those who were not admitted to the ICU more often received opioids at discharge. One plausible explanation is the correlation between ICU admission and transition of care points. Transitional care points provide the opportunity for medication reconciliation and discontinuation of unnecessary therapies. Patients admitted to the ICU typically have more transition of care points (e.g., ICU → Step Down Unit → General Floor → Hospital Discharge) and thus more opportunities for opioid discontinuation before hospital discharge. A 2-fold increase in the number of patients requiring surgery Post-ALTO implementation was observed, and subsequently more patients were prescribed opioids at discharge. Therefore, patients undergoing surgery remain a population of focus to further reduce opioid prescribing. Lastly, CCI ≤1 was associated with more opioid prescribing at discharge. While a lower CCI correlates with less comorbidities preventing use of non-opioid analgesics, it is unclear why an overall healthier population were more often discharged with opioids.
Despite differences in analgesic use before and after ALTOSM implementation, hospital and ICU LOS were similar between groups. As these groups were similar with regards to initial ISS, CCI and rate of ICU admission, these results are not surprising. Of interest, though, is the similarity in hospital and ICU LOS despite the drastically different need for surgery in the Post-ALTO group.
There are several limitations to our study. First, this is a single-center retrospective analysis. Therefore, the results of this study represent that of a single Level II Trauma Center. Second, this study only evaluated an opioid-naïve population excluding individuals with history of or current alcohol or polysubstance abuse, as well as chronic opioid use. Twenty percent of trauma patients report opioid use prior to injury, although the actual rate may be even higher. Thus, these results do not reflect those of the general trauma population. Third, this study did not evaluate opioid drug, dose, duration, administration or MME, nor did it evaluate the appropriateness of opioids. As a result, all effects of ALTOSM may not have been captured. Fourth, post-discharge opioid prescribing, rates of subsequent opioid prescribing or hospital readmissions associated with opioid analgesics were not evaluated. Forth, this study did not evaluate differences in opioid prescribing between surgery types which may have contributed to variations in lengths of stay and opioid prescribing. Fifth, the impact of ALTO on hospital and ICU LOS was not specifically evaluated in this study. Despite these limitations, this study highlights the benefits of an opioid-sparing pain management approach.
To our knowledge, this is the first study evaluating the incidence of opioids prescribing at hospital discharge in opioid-naïve trauma patients following the implementation of an opioid-sparing pain management program. While the study represents prescribing trends in an opioid-naïve population, these results may be applicable to the general trauma population.
Conclusions
Opioids remain mainstay for trauma-related pain management. Implementation of ALTOSM was not associated with a reduction in in-hospital or discharge opioid prescribing, but did lead to an increase in non-opioid and multimodal analgesia use. Further studies are warranted to identify specific populations (e.g., surgery type, injury mechanism) and additional strategies to reduce rates of opioid prescribing at hospital discharge.
Supplemental Material
Supplemental Material - Effect of Alternatives to Opiates Program on Discharge Opioid Prescribing in Trauma Patients
Supplemental Material for Effect of Alternatives to Opiates Program on Discharge Opioid Prescribing in Trauma Patients by Steven F. Nerenberg, PharmD, Caitlin E. Kulig, PharmD, Alexis M. LaPietra, DO, FACEP, Osama A. Elsawy, DO, Antai Wang, PhD, Lindsey A. Foran, DO, Ahmad F. Hlayhel, MD, James Yang, DO, Dinesh Parmar, MD, and Jackie P. Johnston, PharmD, BCPS in Journal of Pharmacy Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.