
Abstract
Background
Delirium is a neuropsychiatric syndrome provoked by dysregulated neurotransmitter function and characterized by altered level of consciousness, fluctuations in mental status, compromised perception, and irregular behavior.1–4 It is subtyped based on the symptoms the patient is experiencing; hyperactive delirium is categorized by agitation, restlessness, emotional lability, and uncooperative or combative behavior, whereas hypoactive symptoms include flat affect, withdrawal, apathy, and lethargy.2,5,6 The incidence of delirium occurs in up to 87% of patients in the intensive care unit (ICU) and predominately manifests as mixed subtype, fluctuating between hyper- and hypoactive delirium. Risk factors for the development of delirium include the use of benzodiazepines and corticosteroids, receipt of blood transfusions, increased age, dementia, prior coma, pre-ICU emergency surgery or trauma, and increasing Acute Physiology and Chronic Health Evaluation (APACHE) and American Society of Anesthesiologists (ASA) scores.7,8
Non-pharmacological prevention and treatment strategies should be employed first, followed by short-term treatment with pharmacological agents for patients experiencing agitation or sleep disturbances. Therapeutic options may include dexmedetomidine infusions, antipsychotics (ie, haloperidol, risperidone, and quetiapine), or melatonin. 7 Due to the sparsity of evidence in the critically ill population, the specific agent(s) utilized may vary by institution. Quetiapine, an atypical antipsychotic with a short half-life and favorable side effect profile, was shown in a 2010 study by Devlin et al 99 to result in faster resolution of delirium when administered 50 mg orally twice daily (BID) vs placebo. Although some benefit has been shown with BID dosing of quetiapine, once daily dosing at bedtime (QHS) is commonly prescribed due to the risk of daytime somnolence and the desire to regulate the patient’s sleep-wake cycle. 10 No studies have evaluated differences in outcomes of the two prescribing practices. Our aim was to determine if QHS dosing of quetiapine reduces duration of delirium vs BID dosing in the treatment of ICU delirium.
Methods
Two community hospital locations of Singing River Health System in South Mississippi served as the patient population for this study. This retrospective chart review evaluated patient records from January 1, 2017, to December 31, 2021, and was approved by the Singing River Institutional Review Board. Patients were included if they were positive for ICU delirium, per CAM-ICU score, and initiated on quetiapine (any dose) between January 1, 2017, and December 31, 2021. They were excluded for diagnosis of alcohol withdrawal, history of psychiatric conditions requiring current treatment with any antipsychotic, quetiapine therapy for less than 24 hours in the ICU, dosing regimens other than BID or QHS, or utilization of quetiapine as a home medication.
A total of 264 patients were reviewed with 41 meeting inclusion criteria (Figure 1) The 41 patients included were divided into two cohorts: BID dosing (n = 23) and QHS dosing (n = 18). The primary outcome was time to delirium recovery and was calculated as the difference, in days, from the start of quetiapine to the first negative CAM-ICU. Patients that did not experience delirium resolution were not included in the calculation of the primary outcome. Physician and nursing documentation were reviewed for eight patients with missing CAM-ICU scores to determine time to delirium resolution. Secondary outcomes were ICU and hospital lengths of stay, duration of mechanical ventilation, in-hospital death, delirium recovery, and incidence of QTc prolongation. Flow chart of patients included in final analysis. †Other encompasses transferred from ICU within 24 hours, received <24 hours of quetiapine.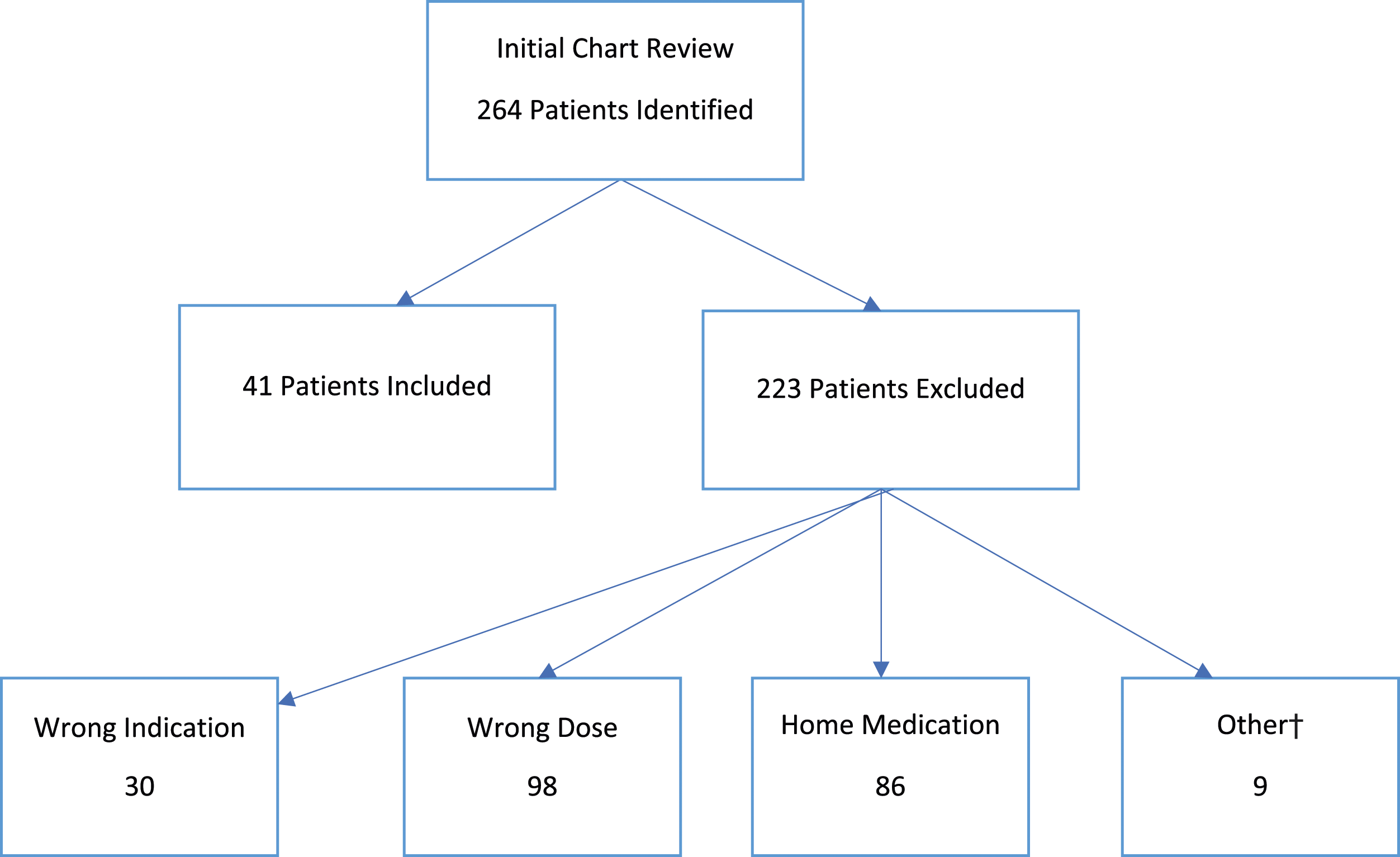
SPSS Statistics software was utilized for statistical analysis. Baseline characteristics were described as means and standard deviations (SD), medians and interquartile ranges (IQR), or numbers and percentages. The primary outcome of delirium duration was analyzed using the Mann-Whitney U test. Hospital and ICU lengths of stay and mechanical ventilation duration were analyzed with unpaired t test, in-hospital death and delirium recovery with chi square with yates’ correction, and QTc prolongation with Fisher’s exact test. A two-sided P-value was used and considered statistically significant if found to be below .05. Subgroup analyses were performed for the primary outcome.
Results
Baseline Characteristics.
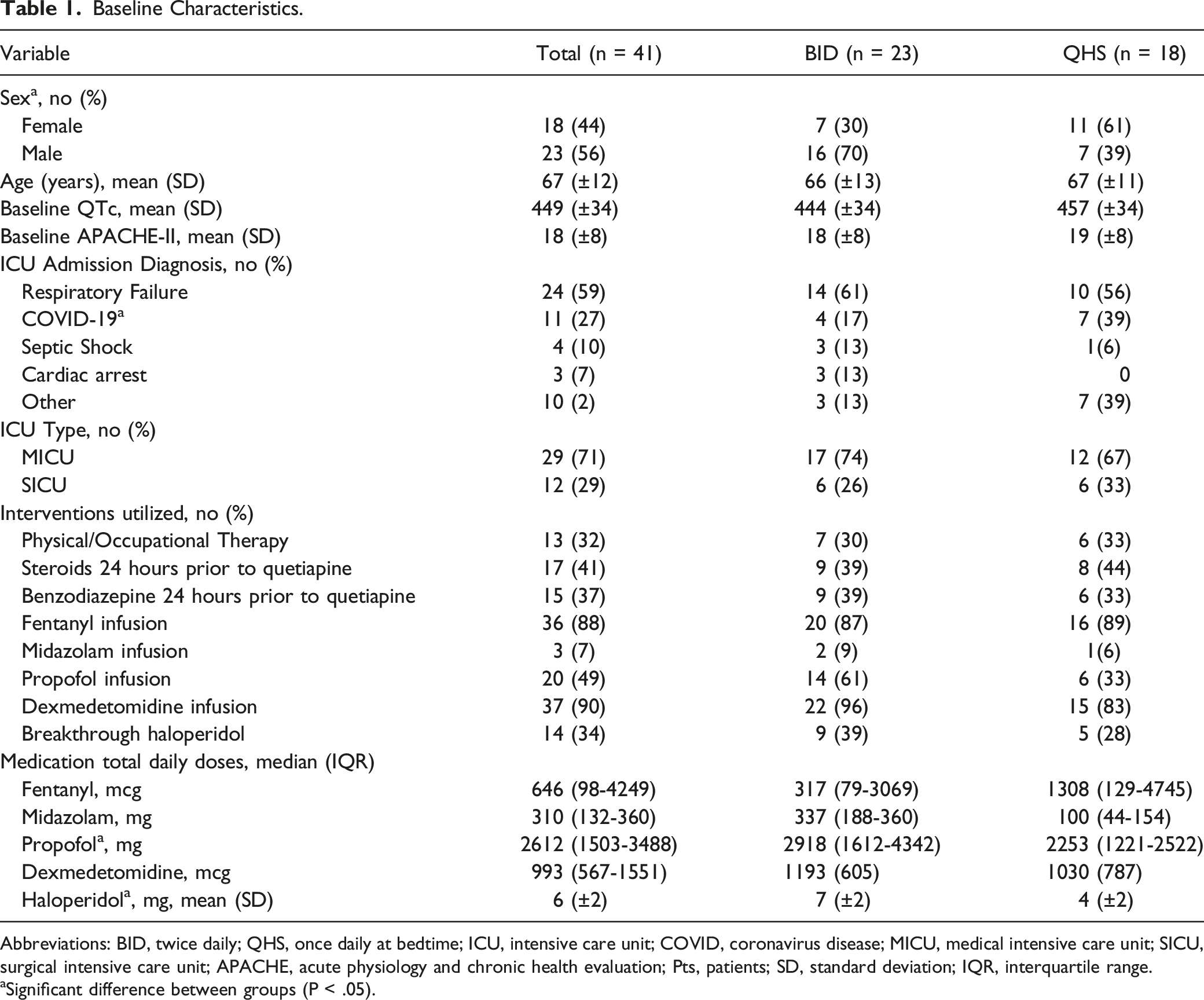
Abbreviations: BID, twice daily; QHS, once daily at bedtime; ICU, intensive care unit; COVID, coronavirus disease; MICU, medical intensive care unit; SICU, surgical intensive care unit; APACHE, acute physiology and chronic health evaluation; Pts, patients; SD, standard deviation; IQR, interquartile range.
aSignificant difference between groups (P < .05).
Primary and Secondary Outcomes.
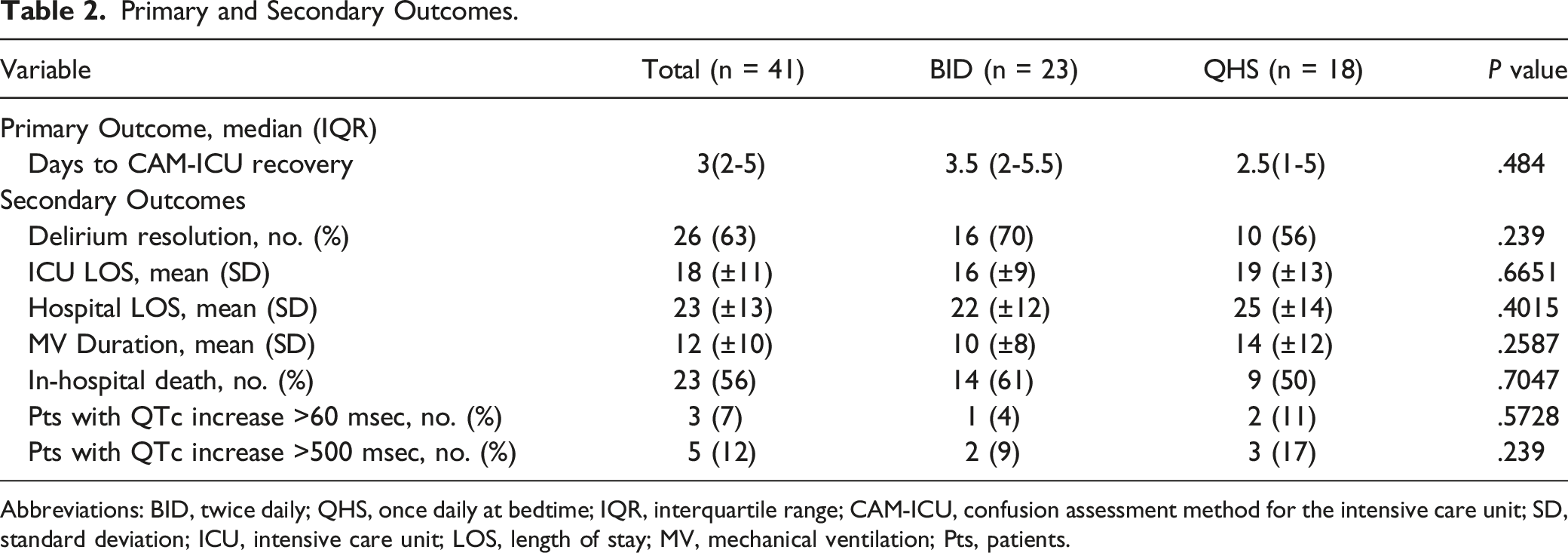
Abbreviations: BID, twice daily; QHS, once daily at bedtime; IQR, interquartile range; CAM-ICU, confusion assessment method for the intensive care unit; SD, standard deviation; ICU, intensive care unit; LOS, length of stay; MV, mechanical ventilation; Pts, patients.
Subgroup Analysis of the Primary Outcome, Days to CAM-ICU Recovery.
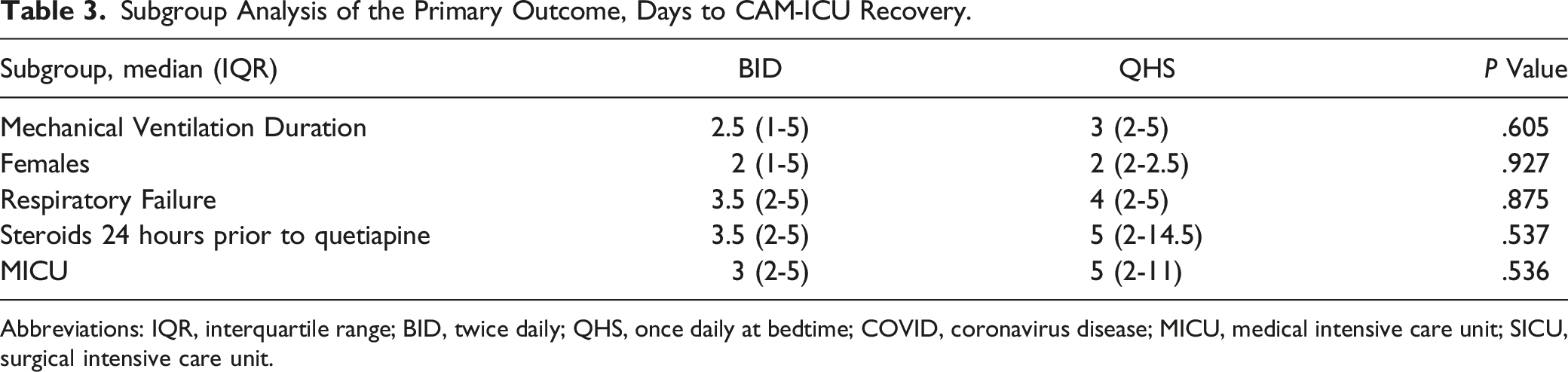
Abbreviations: IQR, interquartile range; BID, twice daily; QHS, once daily at bedtime; COVID, coronavirus disease; MICU, medical intensive care unit; SICU, surgical intensive care unit.
Discussion
The development of delirium in patients admitted to the ICU is associated with poor patient outcomes and increased burden on the health system. To allow for early ICU delirium detection and intervention, the 2018 Clinical Practice Guidelines for the Management of Pain, Agitation, Delirium, Immobility, and Sleep Disruption (PADIS) in Adult Patients in the ICU recommend performing the CAM-ICU screening tool once per shift in all critically ill patients. 7 It is a valid and reliable assessment tool that has shown superior sensitivity and specificity of detecting delirium in ICU patients. 11 Once patients meet the criteria for a positive CAM-ICU, diagnosis of ICU delirium is established. In conjunction with non-pharmacologic therapies, PADIS guidelines support the use of quetiapine in the treatment of ICU delirium. This recommendation is based on a single study by Devlin et al, utilizing quetiapine twice daily vs placebo.7,9 Once daily dosing at bedtime (QHS) is commonly prescribed to reduce daytime somnolence; however, it is unknown if bedtime dosing vs twice daily dosing results in different outcomes in the treatment of ICU delirium.
In this retrospective, double-center study, patients received quetiapine either BID or QHS for treatment of ICU delirium. The sample in this study represents a heterogeneous population of critically ill patients. The small sample size (n = 41) and mean age [66.5 years (±12)] are similar to those found in prior literature.2,3,5,9 In this study, the BID dosing group included more male patients than the QHS dosing group (69.6% vs 38.9%), potentially confounding the results.12,13 Male patients are more frequently diagnosed and treated for ICU delirium compared to females; however, a subgroup analysis did not reveal significant differences among sexes.
Although no statistical difference in time to delirium recovery (based on CAM-ICU score) was observed in this study, a pattern of shorter recovery time was seen in the QHS dosing group. Duration of mechanical ventilation and lengths of hospital and ICU stay were similar to the results found by Devlin et al. 9 Patients in the BID dosing group received higher total daily doses of propofol (3268 mg/day vs 1507 mg/day), midazolam (337 mg/day vs 100 mg/day), and haloperidol (7 mg vs 4 mg), and the QHS dosing group received higher doses of fentanyl equivalents per day (1308 mcg/day vs 317 mcg/day).
A strength of this study is that 88% of patients received appropriate pain control. Since uncontrolled pain is a risk factor for the development of delirium, it is important to account for this potential confounder. 14 Additional strengths include that CAM-ICU scores were available in all except eight patients to determine presence or absence of delirium, similar distribution of the use of benzodiazepines and corticosteroids between groups, and the exclusion of patients with confounding diagnoses at baseline.
This study was limited by chart convenience sampling and lack of randomization, as well as a retrospective, observational design. A priori power analysis was conducted, and 61 patients were required per group to achieve an 80% power. Since the sample size was not large enough to meet power, this may have resulted in a type 2 error. The differences in total daily doses of sedatives and analgesics in the BID dosing group represent a major limitation as this suggests that analgosedation may have been suboptimal in this cohort. With regard to sedatives, the receipt of higher midazolam doses in the BID cohort is important to note since benzodiazepine exposure is a major risk factor for delirium development. Total daily doses of quetiapine were not collected and could have strengthened the analysis by better defining the quetiapine exposure in each cohort. There were missing CAM-ICU scores for eight patients, which prompted researchers to rely on physician and nursing notes to determine the time to delirium recovery. Lastly, CAM-ICU scores are not a required nursing assessment, so it is possible that the time to delirium recovery was shorter in either group, suggesting that the first instance of a negative CAM-ICU score may have occurred earlier than the documented CAM-ICU assessment suggested.
Conclusion
This is the first study comparing BID vs QHS dosing of quetiapine for the treatment of ICU delirium. This retrospective chart review of 41 patients found no statistical difference in patient outcomes. These findings suggest similar efficacy of both dosing strategies without an increase in adverse events. Further studies with larger sample sizes are warranted to confirm the results.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.