
Abstract
Introduction
Hyperkalemia has been shown to occur in up to 10% of hospitalized patients. Identified risk factors associated with hyperkalemia consist of acute kidney injury, chronic kidney disease, diabetes mellitus, cardiac failure, and medications (e.g., angiotensin-converting enzyme inhibitors, potassium-sparing diuretics, and angiotensin II blockers). If not treated appropriately, hyperkalemia may result in complications such as arrhythmias and cardiac arrest. Current guidelines recommend treating hyperkalemia for potassium values greater than or equal to 5.5 mmol/L by shifting potassium intracellularly and eliminating potassium from the body. A preventative measure for cardiac events resulting from hyperkalemia is to stabilize the myocardium with calcium. In order to shift potassium intracellularly, one of the treatment modalities utilized is intravenous (IV) regular insulin with glucose. 1 Insulin activates sodium-phosphate adenosine triphosphatase, leading to potassium transfer from the extracellular space to the intracellular space. 2 With normal or adequate renal function, IV regular insulin has an onset of action within 15 minutes, a peak of 30 to 60 minutes, and a duration of about 4 hours while subcutaneous regular insulin has an onset of about 30 minutes, a peak of 3 hours, and duration of action of 8 hours.1,3 Intravenous administration of insulin is preferred over subcutaneous insulin administration due to a shorter onset of action. Intravenous glucose in the form of dextrose in water is given with IV regular insulin to assist in preventing hypoglycemic events and does not have any inherent potassium-lowering effects. 2
Hypoglycemic events, including insulin-induced events, are associated with increased mortality in hospital settings. Insulin is designated as a high risk medication, therefore it is important to identify the optimal dosing strategy of IV regular insulin for treatment of hyperkalemia that balances safety and effectiveness. Historically a conventional dose has been utilized consisting of 10 units of IV regular insulin along with 25 g of IV dextrose. 4 Previous studies using this conventional dosing identified potassium-lowering in the range of .65 to 1.14 mmol/L with hypoglycemia rates of 11% up to 75%.5-8 In order to discover a more optimal dosing strategy to reduce hypoglycemia rates, other recent retrospective studies have been conducted evaluating various IV regular insulin and IV dextrose dosing schemes to treat hyperkalemia. These studies contain varying methodologies and have produced conflicting results.9-12
Current guideline recommendations differ on an optimal treatment strategy of hyperkalemia. The 2019 update from Kidney Disease Improving Global Outcomes recommends administering 5 units of IV regular insulin in place of the conventional insulin dose of 10 units for the acute management of hyperkalemia but acknowledged that data is limited. 13 The 2020 UK Renal Association Guidelines recommends 10 units of IV regular insulin with 25 g of IV glucose, followed by an IV infusion of 10% glucose at 50 mL/hour for 5 hours in patients with a pretreatment blood glucose <126 mg/dL to prevent hypoglycemia. 1
Historically at our institution, a large urban academic medical center, inpatient providers could order IV regular insulin to treat hyperkalemia with dosing at their own discretion and clinical judgment. The usual dose was typically 10 units of IV regular insulin. Based on reported safety events of hypoglycemia, a hyperkalemia treatment order set was implemented at our institution in May 2019 that utilized a weight-based dosing strategy (.1 units/kg with a maximum dose of 10 units of IV regular insulin); IV dextrose orders and point of care testing (POCT) glucose orders were also included. This dosing strategy was adopted from findings by Wheeler et al. which revealed a weight-based dosing strategy, .1 units/kg, had reduced hypoglycemic events when compared to the conventional 10 units of IV regular insulin (12.1% vs 27.3%; P = .05) with a similar potassium-lowering effect. 9
Considering the limited evidence and lack of consensus for the appropriate dose of insulin in the treatment of hyperkalemia, identification of the optimal IV regular insulin dosing regimen that minimizes the risk of hypoglycemia is warranted. The purpose of this study is to evaluate differences between patients who experience hypoglycemia (defined as a blood glucose (BG) < 70 mg/dL) vs patients who do not experience hypoglycemia within 6 hours of IV regular insulin administration for the treatment of hyperkalemia at our institution. This study allowed for both assessment of current practices at our institution and contribution to existing literature.
Study Method
This single center retrospective chart review examined inpatient and emergency department encounters of patients who received IV regular insulin for the treatment of hyperkalemia between May 1, 2018, and May 31, 2020. This date range was chosen to include one year of data pre- and post-implementation of the hyperkalemia treatment order set, which included weight-based IV regular insulin dosing recommendations (.1 units/kg with a maximum dose of 10 units of IV regular insulin). All patients at least 18 years of age administered IV regular insulin within 6 hours of a pre-treatment potassium of ≥5 mmol/L were included. Prisoners, pregnant women, and patients being treated for digoxin toxicity were excluded. Exclusion criteria also included concomitant insulin infusions in order to determine the potassium-lowering effects of a single IV regular insulin dose. Receipt of rapid-acting potassium-redistributing and eliminating treatment modalities including IV sodium bicarbonate, IV loop diuretics and any form of dialysis were excluded in order to assess the effects of IV insulin as the primary potassium-lowering agent. The cation-exchange resins were included due to their delayed effect on potassium lowering as compared to IV regular insulin and the negligible impact on potassium lowering in the inclusion criteria time frame. High-dose albuterol was included since providers may have selected this agent as a potential adjunct therapy with insulin-glucose as recommended by multiple guidelines. Due to time and resource constraints, a random number generator was utilized to provide a sample to be screened for inclusion.
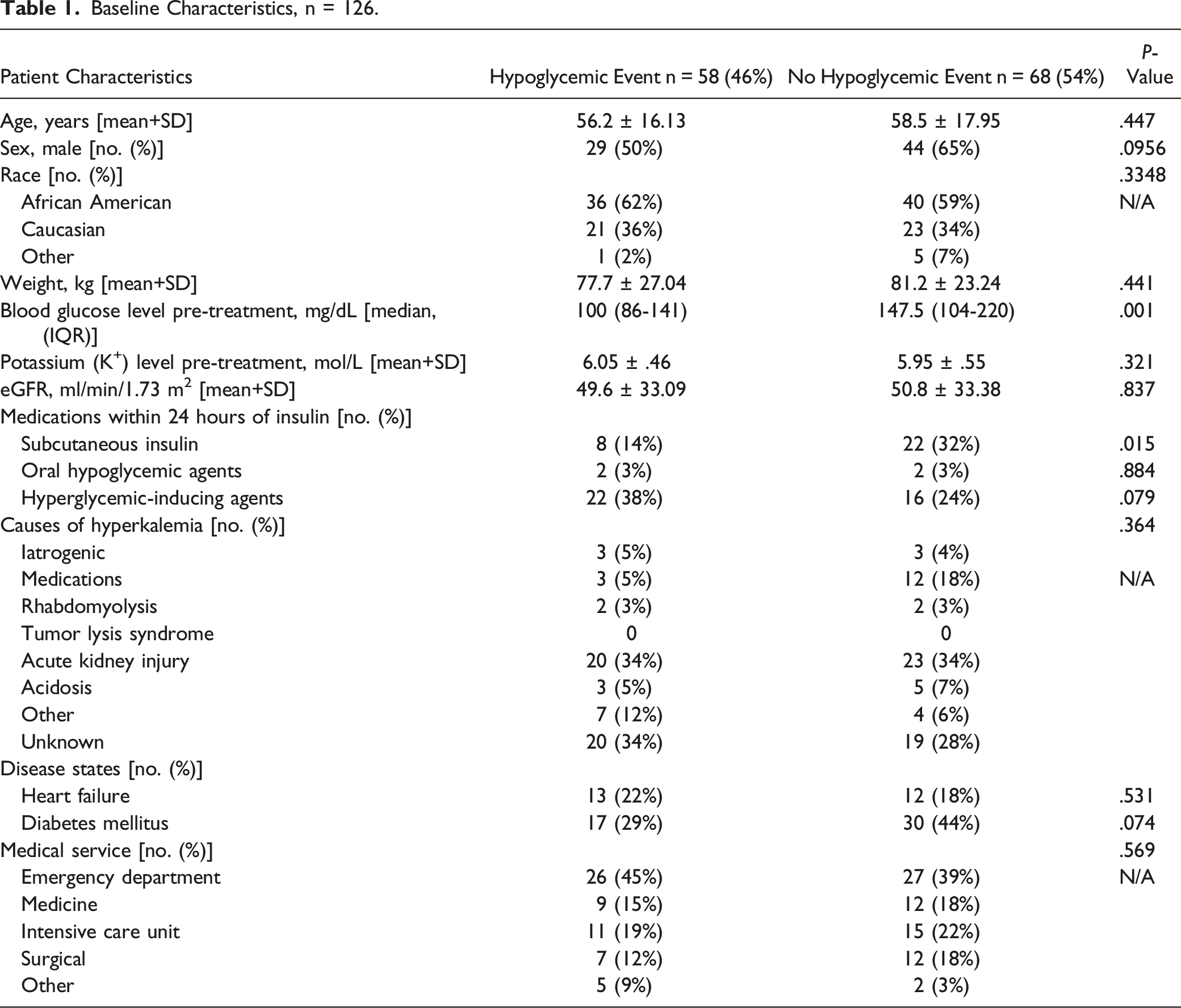
Baseline Characteristics, n = 126.
The primary outcome of this study was the difference in weight-based IV regular insulin dosing between the hypoglycemic and non-hypoglycemic groups. Secondary outcomes included the difference in serum potassium concentration reduction after IV regular insulin administration, rates of severe hypoglycemia in the hypoglycemic group, and utilization of the institutional hyperkalemia order set during the time frame that it was available. Characterization of repeat doses of IV regular insulin (e.g., number of repeat doses, similarity of repeat dose to initial dose, and repeat dextrose dose administration) were collected and presented in Table 4.
Statistical analyses were performed on data collected from Cerner Millennium, Cerner Corporation, 2011 using JMP® (Version 16. SAS Institute Inc., Cary, NC, 1989-2022). Descriptive statistics for quantitative variables were presented using the mean with standard deviation for parametric data or the median with first and third quartile (interquartile range [IQR]) for nonparametric data. Categorical variables were presented as number and percentage. Comparisons of proportions were performed using chi-square tests and continuous variables using Student’s t test. A P-value of <.05 was considered statistically significant. A multivariable logistic regression was used to evaluate predictors of hypoglycemia. This study was approved by the Institutional Review Board and Internal Medicine Endocrinology Protocol Review Oversight Committee.
Results
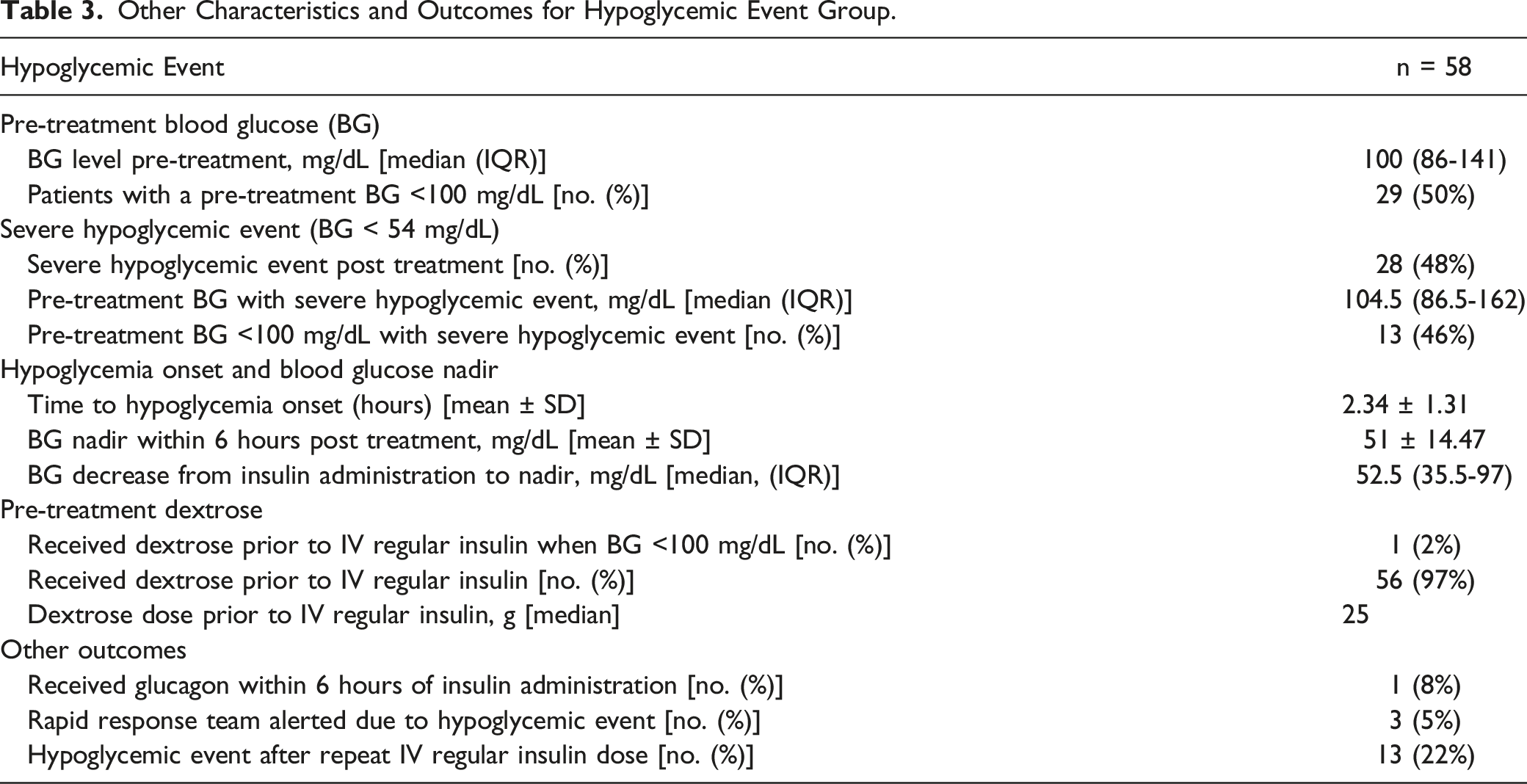
A total of 405 patients were screened for inclusion in the retrospective analysis. As shown in Figure 1, a total of 227 patients were excluded due to receipt of dialysis, IV sodium bicarbonate, and/or IV diuretics and 87 patients were excluded due to not having either a repeat blood glucose value or serum potassium within 6 hours of IV regular insulin administration. A total of 126 were included, of which 58 patients (46%) experienced a hypoglycemic event. Of the patients who developed hypoglycemia, 28 patients (22% of the total sample) had severe hypoglycemia (BG <54 mg/dL). Patient flow diagram of study cohort.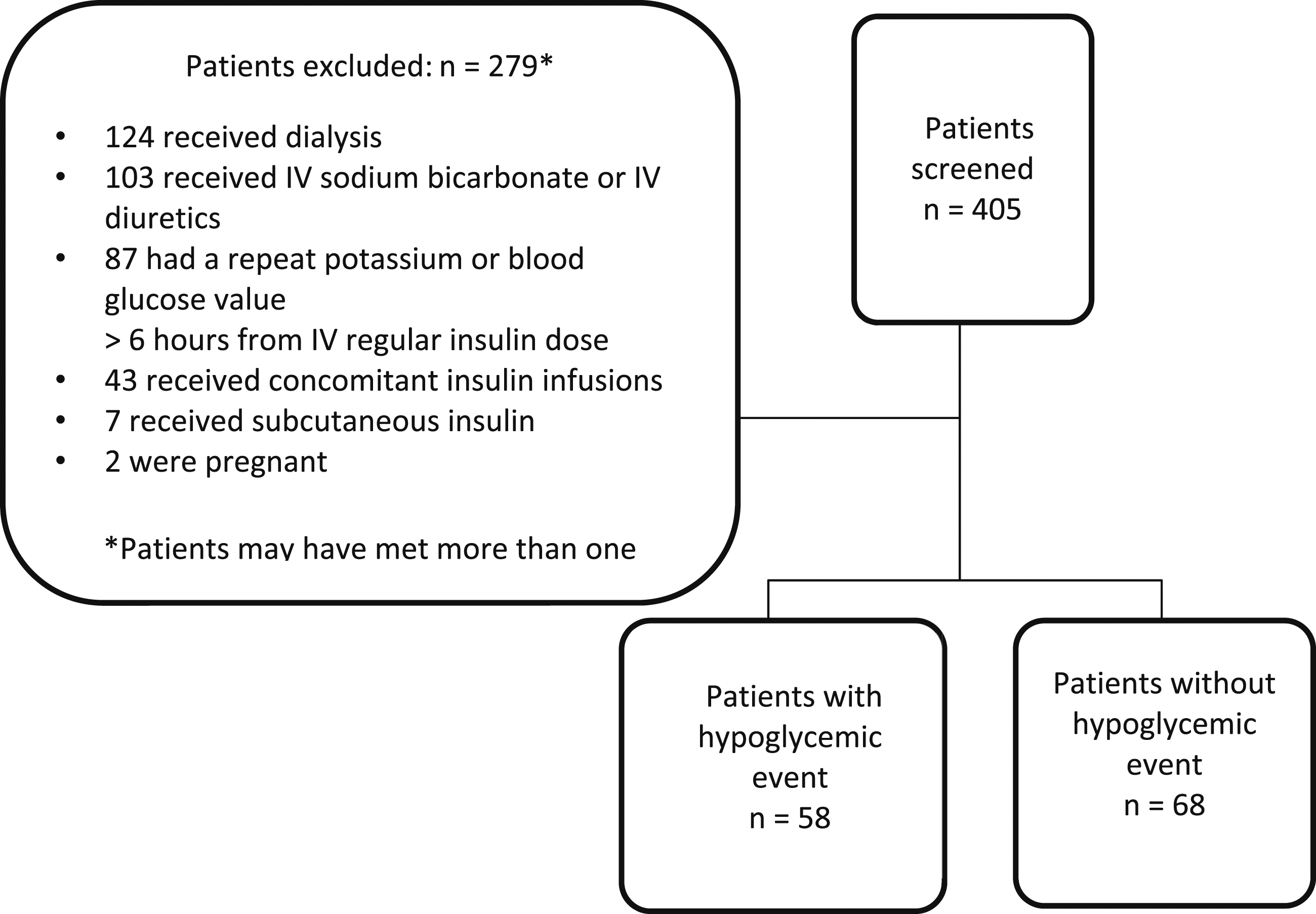
Baseline characteristics of each group are presented in Table 1. There were no differences between the two groups except that patients who experienced a hypoglycemic event had a statistically lower mean pre-treatment glucose value compared to patients who did not experience a hypoglycemic event (100 mg/dL [IQR, 86-141 mg/dL] vs. 147.5 mg/dL [IQR, 104-220 mg/dL] mg/dL; P = .001). The proportion of patients who received other insulin doses within 24 hours of the treatment of hyperkalemia was greater in the group that did not experience a hypoglycemic event, (22/68 [32%] vs. 8/58 [14%]; P = .015).
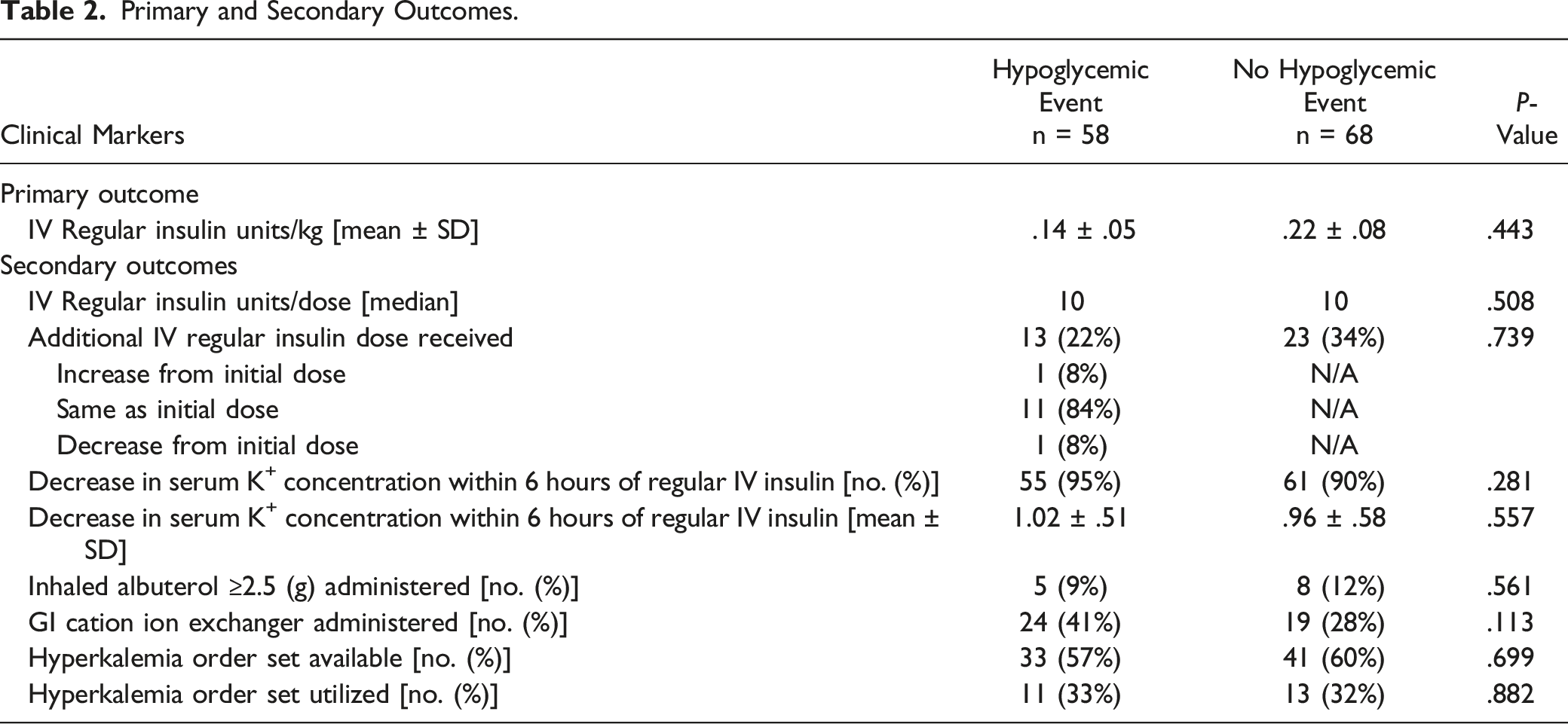
Primary and Secondary Outcomes.
Other Characteristics and Outcomes for Hypoglycemic Event Group.
Patient Characteristics for Hypoglycemic Event After a Repeat Dose of IV Regular Insulin.
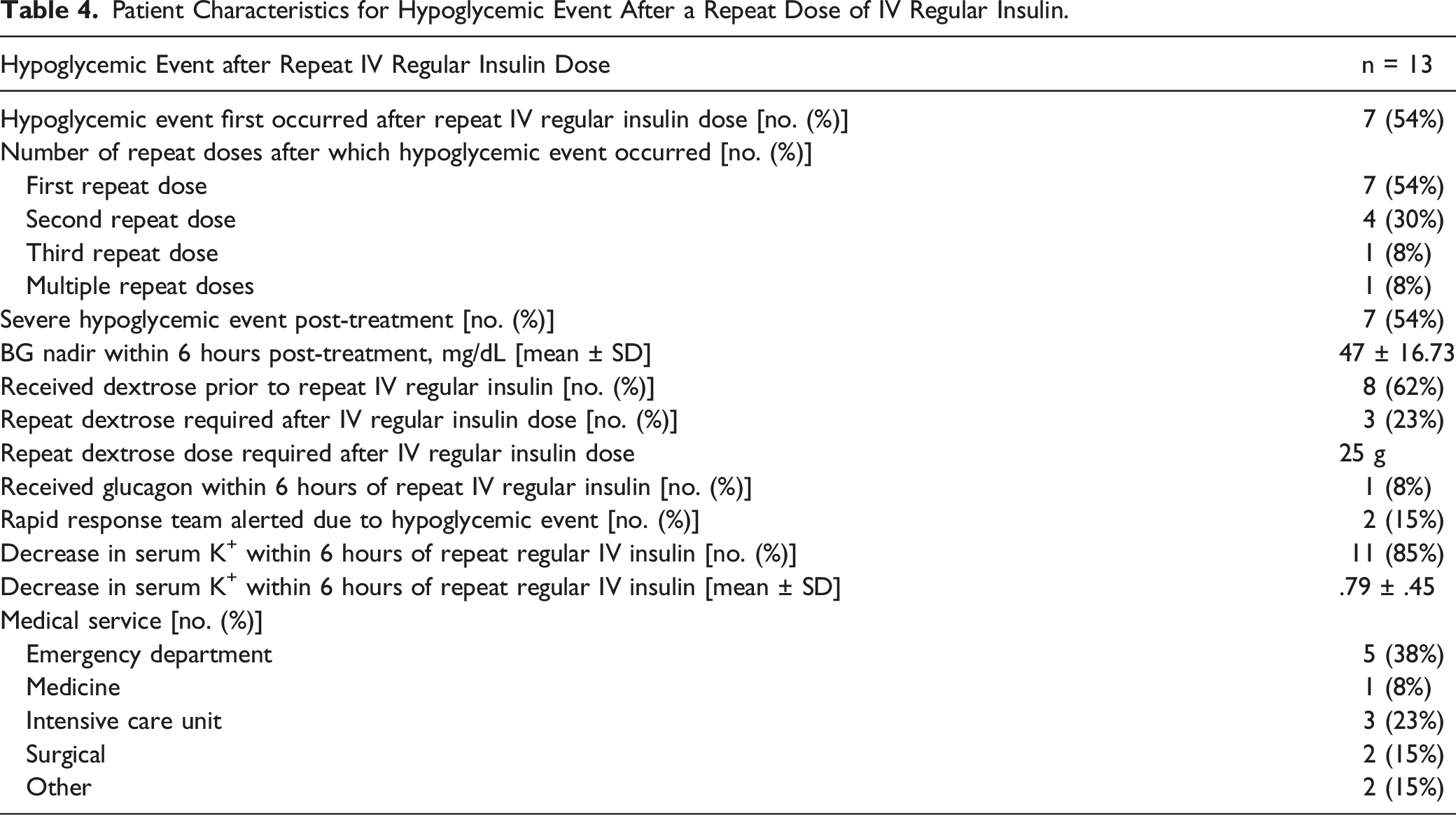
A multivariable logistic regression analysis to determine independent risk factors for hypoglycemia was performed which initially included the following variables: age, sex, race, weight, pre-treatment blood glucose, eGFR, use of other insulin, heart failure, diabetes, weight-based IV regular insulin dose, and repeat IV regular insulin dose. The analysis revealed that independent predictors for hypoglycemia in our study were repeat doses of IV regular insulin, pre-treatment blood glucose, and female sex. The model found that these three risk factors predicted 64% of the variance in our model and was primarily driven by repeat doses of IV regular insulin (R2 = .642; P < .0001).
Discussion
Hyperkalemia and hypoglycemia have been associated with an increased risk of morbidity and mortality; therefore, it is imperative to determine the treatment strategy to effectively lower potassium while at the same time preventing or minimizing hypoglycemia. The primary outcome of this study, the difference in weight-based dosing of IV regular insulin between patients who experienced a hypoglycemic event and those who did not experience a hypoglycemic event, was not statistically significant. However, the majority of patients received 10 units of IV regular insulin and a weight-based dose of approximately .1 units per kg per dose. There was also no difference in the potassium-lowering effect between the two groups. Considering almost all patients received 10 units of IV regular insulin and baseline weight was not statistically different between groups, it would be expected to see a similar weight-based dose and potassium-lowering effect. One limitation, however, is that the sample in our study did not include patients with extremes of weight, therefore these results may not be extrapolated to those populations. Recent retrospective studies evaluating reduced doses of IV regular insulin compared to conventional doses have found differing hypoglycemic rates.
Wheeler et al conducted a retrospective study that evaluated hypoglycemia incidence in 132 patients who received either 10 units of IV regular insulin or a weight-based dose of insulin (.1 units/kg up to a maximum of 10 units; actual range 4 to 9 units/dose) with 50 g of dextrose for treatment of hyperkalemia. The number of patients who experienced a hypoglycemic event was not statistically significant between groups (19.7% vs. 10.6%; P = .22) but the number of hypoglycemic events was statistically significant (27.3% vs. 12.1%; P = .05). Although it cannot be inferred directly, repeat insulin doses may have played a role in hypoglycemic events. LaRue et al conducted a retrospective study that compared 675 patients who received either 5 units or 10 units of IV regular insulin for treatment of hyperkalemia. The institution’s hyperkalemia protocol called for IV regular insulin to be given with IV or oral dextrose 25 g, followed by dextrose 25 g 1 hour later, and finally a possible third dose of dextrose 25 g 3 hours later if blood glucose was <70 g/dL. The patients who received 5 units of IV regular insulin had less hypoglycemia episodes than those who received 10 units of IV regular insulin (19.5% vs. 28.6%) and reported less severe hypoglycemic episodes (defined as a BG <40 mg/dL) (6.8% vs. 3.0%). However, the change in serum potassium concentration was similar between the two groups (−1.0 ± .8 with 5 units vs −1.0 ± .7 mEq/L with 10 units, 95% CI -.1 to .1 mEq/L). 10 In another retrospective study, Moussavi et al evaluated 700 adults who received either less than 10 units of IV regular insulin vs. 10 units of IV regular insulin for the treatment of hyperkalemia. It was found that 10 units of IV regular insulin resulted in more hypoglycemia episodes (11.2% vs. 17.6%, P = .008). Patients treated with less than 10 units had a more modest potassium reduction (.94 vs. 1.11 mEq/L, P = .008) while the mean post-treatment potassium did not differ between groups (5.22 vs 5.26 mEq/L, P = .566). This study also identified other risk factors for hypoglycemia which included younger age, dialysis dependence, lack of diabetic history, and lower pre-treatment serum glucose. Finally, Finder et al conducted a retrospective study of 377 patients with eGFR of 15-59 mL/min/1.73 m2 who received 5 units vs. 10 units of IV regular insulin for the treatment of hyperkalemia. The mean eGFR was significantly different amongst the patients who received 5 units vs 10 units (28.8 ± 11.1 mL/min/1.73 m2 vs. 37.5 ± 12.5 mL/min/1.73 m2; P = <.001). There was no difference in the rate of hypoglycemia between the groups (6.5% vs 8.4%; P = .476), however in the institution’s protocol, patients with a blood glucose <250 mg/dL received 50 g of IV dextrose. Although it cannot be inferred directly, this increased dextrose dose may have been a factor in the reduced reported rates of hypoglycemia. 12
Compared to these previous studies, our study design differed in that it compared the weight-based insulin doses in hypoglycemic vs. non-hypoglycemic patients as opposed to comparing the incidence of hypoglycemia with different insulin dosing strategies. In addition, our study also excluded many patients that were included in these other study populations, such as those receiving IV sodium bicarbonate and loop diuretics as well as dialysis-dependent patients. Furthermore, while all of these studies, including ours, had similar definitions for hypoglycemic events, the blood glucose concentration defined as severe hypoglycemia differed as did dextrose administration strategies and follow-up time periods to determine safety and effectiveness. The incidence of hypoglycemia in our study (46%) was higher than those reported in these studies, but this is consistent with previous reports of hypoglycemic events in up to 50% of patients. 15 Potential contributors to the higher hypoglycemic rate in our study may have included lower pre-treatment blood glucose values (i.e., <100 mg/dL) in half of the hypoglycemic population, lower dextrose doses given compared to most of the cited studies, most patients receiving 10 units rather than a lower dose of IV regular insulin, and diet status at time of insulin administration (which was not a data point recorded directly in our study). However, all of these studies found consistent risk factors for hypoglycemia and while our study did not find a difference in weight-based dosing, previous evidence suggests a lower insulin dose may improve safety while not compromising efficacy.
Our study had several limitations, partly due to its single-center retrospective design. Limitations included the potential for selection bias due to the retrospective nature of the study. The study did not account for other forms of dextrose the patients may have received in forms of food intake and dextrose in other IV medications or infusions. There were a large number of patients excluded (n = 87) because no repeat potassium or blood glucose level within 6 hours of IV regular insulin administration was completed. This could have underestimated the amount of patients who became hypoglycemic following the IV regular insulin dose due to this omission. Patients who received IV sodium bicarbonate and IV diuretics were also excluded which limits the generalizability to those who may receive other potassium-lowering treatment modalities. Dialysis-dependent patients were also excluded from this study which warrants more research in treating hyperkalemia in this specific patient population. Our study also focused on surrogate measures instead of clinical outcomes such as symptomatic hypoglycemia, arrhythmias, cardiac arrest, inpatient length of stay, and inpatient mortality. Additionally, there was the unknown possibility of user or machine error with point-of-care blood glucose testing and blood collection for basic metabolic panels that may have given inaccurate results.
Conclusion
The primary outcome in this study, the difference in weight-based dosing of IV regular insulin between patients who experience a hypoglycemic event and those who do not experience a hypoglycemic event, did not differ between the two groups. The potassium-lowering effect also did not differ between the two groups. Lower blood glucose prior to administration of IV regular insulin, repeat doses of IV regular insulin, and female sex were found to be independent risk factors for development of hypoglycemia. Based on the results of our study, an optimal IV regular insulin and dextrose dosing strategy to treat hyperkalemia cannot be determined. However, our results may help providers take extra precautions prior to initiating repeat doses and in patients who have a reduced baseline blood glucose prior to treatment. One may consider administering higher dextrose doses if pre-treatment blood glucose is <140 mg/dL or if giving repeat IV regular insulin doses. Considering the limited evidence and lack of consensus, identifying the optimal IV regular insulin dosing regimen that minimizes the risk of hypoglycemia is still warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.