
Abstract
Introduction
Between January 2018 to December 2019, 758,000 patients from Australian public hospital waiting lists were admitted for elective surgery, with the number of patients increasing on average by 2.1% per year since between January 2014 to December 2015. 1 Studies have suggested that unintentional medication discrepancies at the time of admission are common in general medical patients. 2 One study showed that 53.6% of older medical patients taking at least 4 medications had unintended medication discrepancies on admission, with more than a third of these medication discrepancies having the potential to cause moderate or severe harm. 2 The availability of accurate medication histories at the time of admission to ensure medication reconciliation is done in a timely manner may help to reduce medication errors. The challenge with obtaining a best possible medication history (BPMH) post-surgery is the delay in clarifying medications due to decreased post-operative cognitive status and pain, which can lead to late administration of medications and medication errors. 3
Pharmacists working in pre-admission clinics can assist with the medication assessment in elective surgery patients by advising on pre- and post-operative medication management and conducting accurate medication histories to improve medication reconciliation and reduce errors.4-6 Internationally, the implementation of pre-admission pharmacists prior to elective surgery has shown to reduce prescribing errors and omissions.3,7,8 In Australia, studies have demonstrated that pre-admission pharmacists have a positive impact on medication management and increase patient safety by increasing the number and availability of completed accurate medication histories and medication reconciliation on admission, helping to reduce workload for surgical ward staff, and documenting more regular prescribed, when required and over-the-counter (OTC) medicines than doctors.9-14
The aims of this study were to investigate if a pre-admission pharmacist completing BPMHs 1 to 3 business days prior to admission for adult elective surgery patients with planned overnight admission increases the proportion of patients with (i) a BPMH completed, (ii) medication reconciliation completed and (iii) all home medications charted correctly within 24 hours of admission, and reduces the number of documented clinical interventions.
Method
Study Design, Setting and Participants
A prospective interventional study was conducted at Casey Hospital during the period of August 2021 to April 2022. Casey Hospital is a 461 bed tertiary teaching hospital, part of Monash Health in metropolitan Melbourne, Australia. Adult patients for elective surgery with planned overnight admission at the hospital were included in this study. Exclusion criteria were: cancelled or delayed surgery, day surgery, non-elective surgery, and patients transferred from other hospitals and residential aged care facilities. Patients that were not taking any medications at home or did not have any documentation of home medications in the Electronic Medical Record (EMR), patients discharged on the same day of admission, patients who declined to participate, or were uncontactable or not contacted, or were seen by another pre-admission pharmacist on the same day were also excluded. The pre-intervention group participants were selected by identifying adult elective surgery patients with overnight stay (ie, not discharged until at least the day after their admission) during the period of August to September 2021 retrospectively. Participants in the post-intervention group were recruited via the EMR, by identifying patients to be admitted to the hospital for elective surgeries that required overnight stay during the period of October 2021 to April 2022. The inclusion and exclusion criteria were the same for both groups (Figure 1). Inclusion and exclusion criteria for the pre-intervention and post-intervention groups.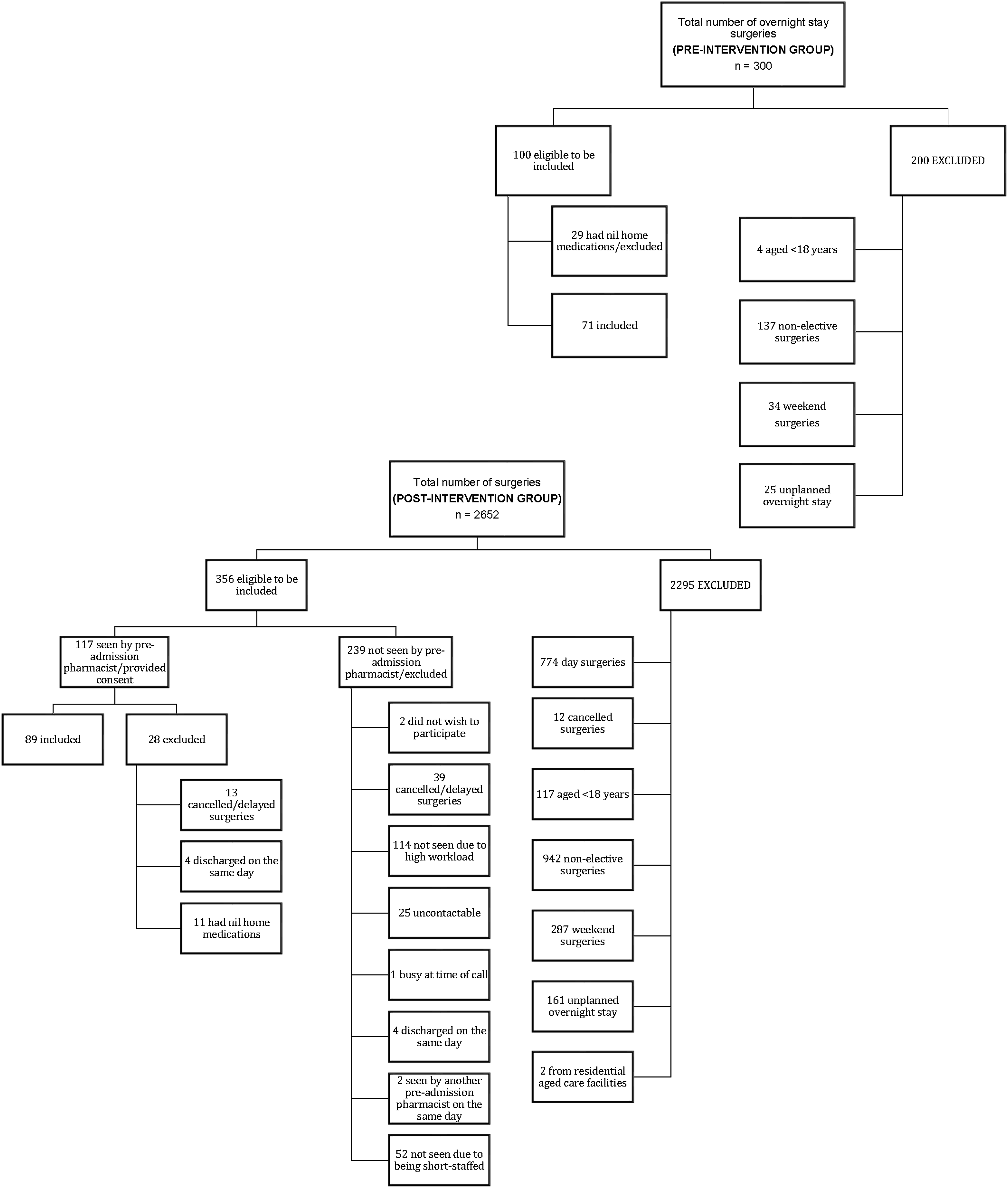
Pre-admission Pharmacist: Prior to Admission
During the study period, Casey Hospital had 2.5 EFT (employed full-time) surgical pharmacists, where 1.5 EFT pharmacists worked on the primary surgical ward and 1 EFT pharmacist cared for surgical outlier patients on other wards across the hospital. The pre-admission pharmacist role was performed by the surgical outliers pharmacist, in addition to their daily workload, which involved caring for 13 patients on average, completing BPMHs, medication reconciliation, reviewing medication charts, providing medications and counselling on discharge. The surgical outliers pharmacist prioritised and completed their daily workload before conducting the pre-admission pharmacist role. Patients were contacted via telephone call 3 business days at the earliest prior to their admission to complete a BPMH, with their home medications confirmed via a second source (eg, community pharmacy or general practitioner). The timeframe of 1 to 3 business days prior to admission was decided upon to take into consideration that patients may not be contactable in the first instance, the high daily workload for surgical ward pharmacists and for when the pre-admission pharmacist may be absent (eg, due to unplanned sick leave). Verbal consent to participate in this study was obtained from patients via the telephone call. In cases where the pre-admission pharmacist was unable to contact the patient at 3 business days prior to admission (eg, the patient was uncontactable or the pre-admission pharmacist had a high workload), the pre-admission pharmacist would re-attempt to call the patient the next business day and the following business day if required to complete a BPMH. Patients were excluded from the study if the pre-admission pharmacist was unable to contact the patients within the 3 business days prior to their admission. If the pre-admission pharmacist identified that a patient did not have appropriate peri-operative medication management (eg, a medication was not withheld pre-surgery), the pre-admission pharmacist would notify the surgical team to assess if the patient was still suitable for surgery. After completing a BPMH, the pre-admission pharmacist documented a handover in the patient’s EMR to notify the surgical ward pharmacists that a BPMH had been completed and to confirm for any medication changes with the patient on admission. The pre-admission pharmacist role was not performed on days where the usual pre-admission pharmacist was absent or when the surgical ward pharmacist team was not fully staffed (eg, due to unplanned sick leave).
Surgical Ward Pharmacist: On Admission
On admission, the surgical ward pharmacists confirmed with the patients if there were any medication changes since the BPMH that was completed by the pre-admission pharmacist. The patient’s home medication list in the EMR was updated if there were any medication changes. The time and date in which the surgical ward pharmacists re-confirmed the medications with the patient on admission was documented in the EMR. The surgical ward pharmacist then completed medication reconciliation as per usual standard of practice by comparing the BPMH to the medication chart, and clarified any medication discrepancies with the surgical doctors. Medication discrepancies were documented as clinical interventions in the EMR.
Outcomes
The primary outcomes of this study were the proportion of patients with (i) a BPMH completed, (ii) medication reconciliation completed and (iii) all home medications charted correctly within 24 hours of admission. The secondary outcome was the number of documented clinical interventions.
Data Collection
Data were extracted from the EMR and included patient demographic characteristics such as age, gender, surgical team/type of surgery, English or non-English speaking background, number of medical conditions and number of home medications (including regular prescribed, when required, OTC and vitamin/herbal supplements). Other data collected included completion of the BPMH by the pre-admission and/or surgical ward pharmacist, the percentage of home medications charted correctly within 24 hours, the number and type of documented clinical interventions, the number of medication changes on admission from the BPMH completed by the pre-admission pharmacist, the time taken to chart home medications from the time of admission and the number of attempts the pre-admission pharmacist contacted the patients prior to admission. The time the pre-admission pharmacist spent contacting patients was not collected in this study. Clinical interventions are medication-related problems identified by the pharmacist such as medication omission or wrong dose charted, where a recommendation is made to the doctors to ensure patient safety. Charting of home medications was considered completed if all home medications were charted correctly on the medication chart. All home medications were deemed as being charted correctly if there was explicit documentation to determine if a medication discrepancy was intentional.
Sample Size Estimate
In a previous similar study conducted at the organisation looking at pre-admission clinic pharmacists and medication management (prior to the implementation of the EMR), a reconciliation rate on admission of 90% was considered achievable for the intervention group, compared to 75% for the control group. 9 Based on this, using an online sample size calculator, 15 to power the study to 80% with a confidence level of 95% and significance α of .05, the minimum number of patients required to detect an increase of 15% for patients with a medication reconciliation completed was n = 200 in total.
Statistical Analysis
The data were analysed using the Microsoft Excel Data Analysis ToolPak (Version 2013, Microsoft Corporation, Redmond, Washington, USA) for the Chi-squared test and descriptive statistics, and the Statistics Kingdom Mann-Whitney U online statistical test calculator was used for the Mann-Whitney U test. 16 The Chi-squared test was used to compare gender, types of surgeries, English preferred language, completion of BPMH, medication reconciliation and correct charting of home medications between groups. The Mann-Whitney U test was used to compare age, medical conditions, home medications and time taken to chart medications between groups. The data were summarised as percentages, frequencies, medians and interquartile ranges. Statistical significance was set at P < .05.
Ethical Review
This study was assessed as a quality improvement activity by the Monash Health Human and Research Ethics Committee and exempt from ethical review (Monash Health reference number: RES-21-0000-279Q-74895).
Results
A total of 160 patients were included in this study, with 71 patients in the pre-intervention group and 89 patients in the post-intervention group.
Patient Demographic Characteristics and Home Medication Documentation.
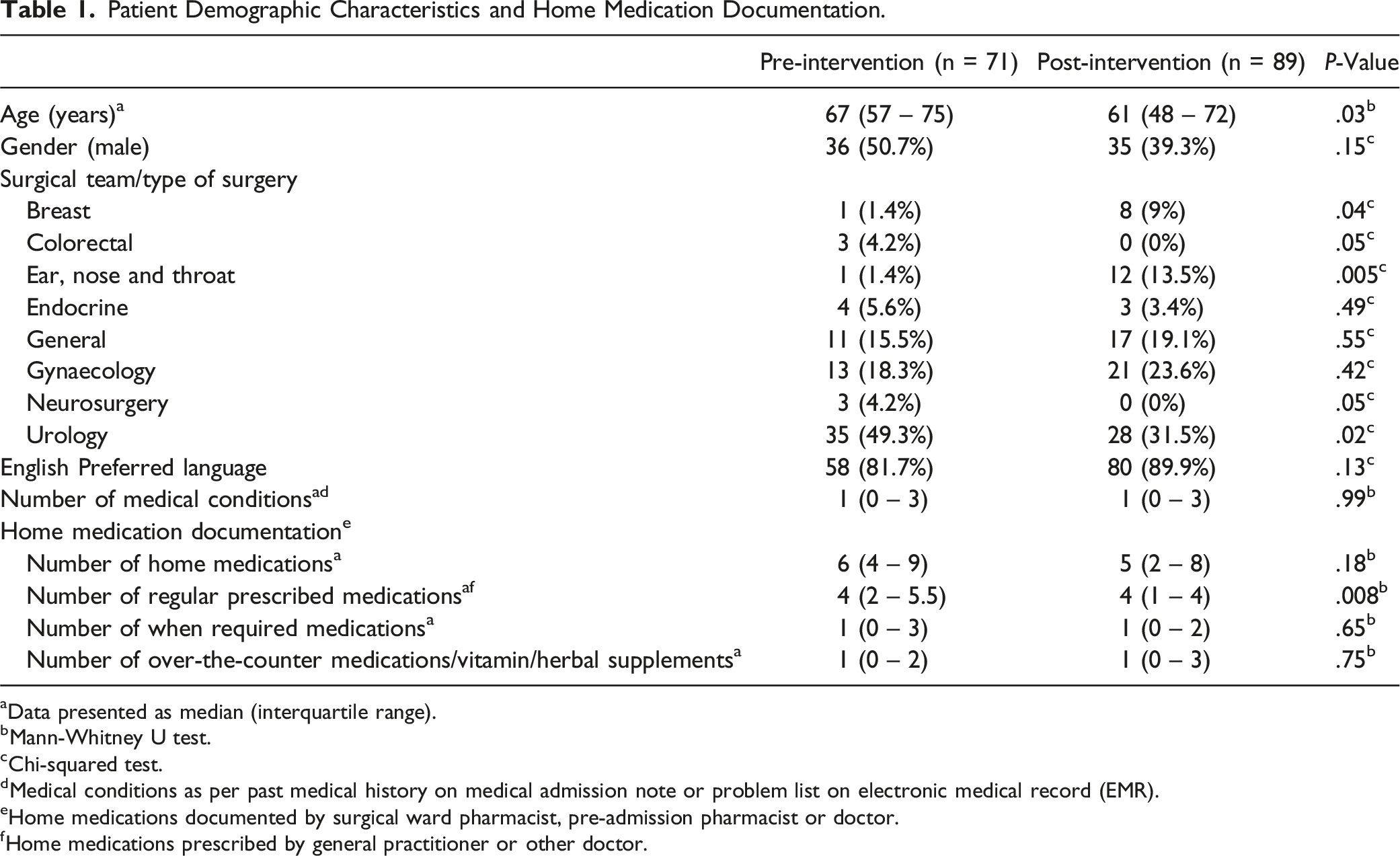
aData presented as median (interquartile range).
bMann-Whitney U test.
cChi-squared test.
dMedical conditions as per past medical history on medical admission note or problem list on electronic medical record (EMR).
eHome medications documented by surgical ward pharmacist, pre-admission pharmacist or doctor.
fHome medications prescribed by general practitioner or other doctor.
BPMH, Medication Reconciliation and Charting of Home Medications
Best Possible Medication History (BPMH), Medication Reconciliation and Charting of Home Medications.
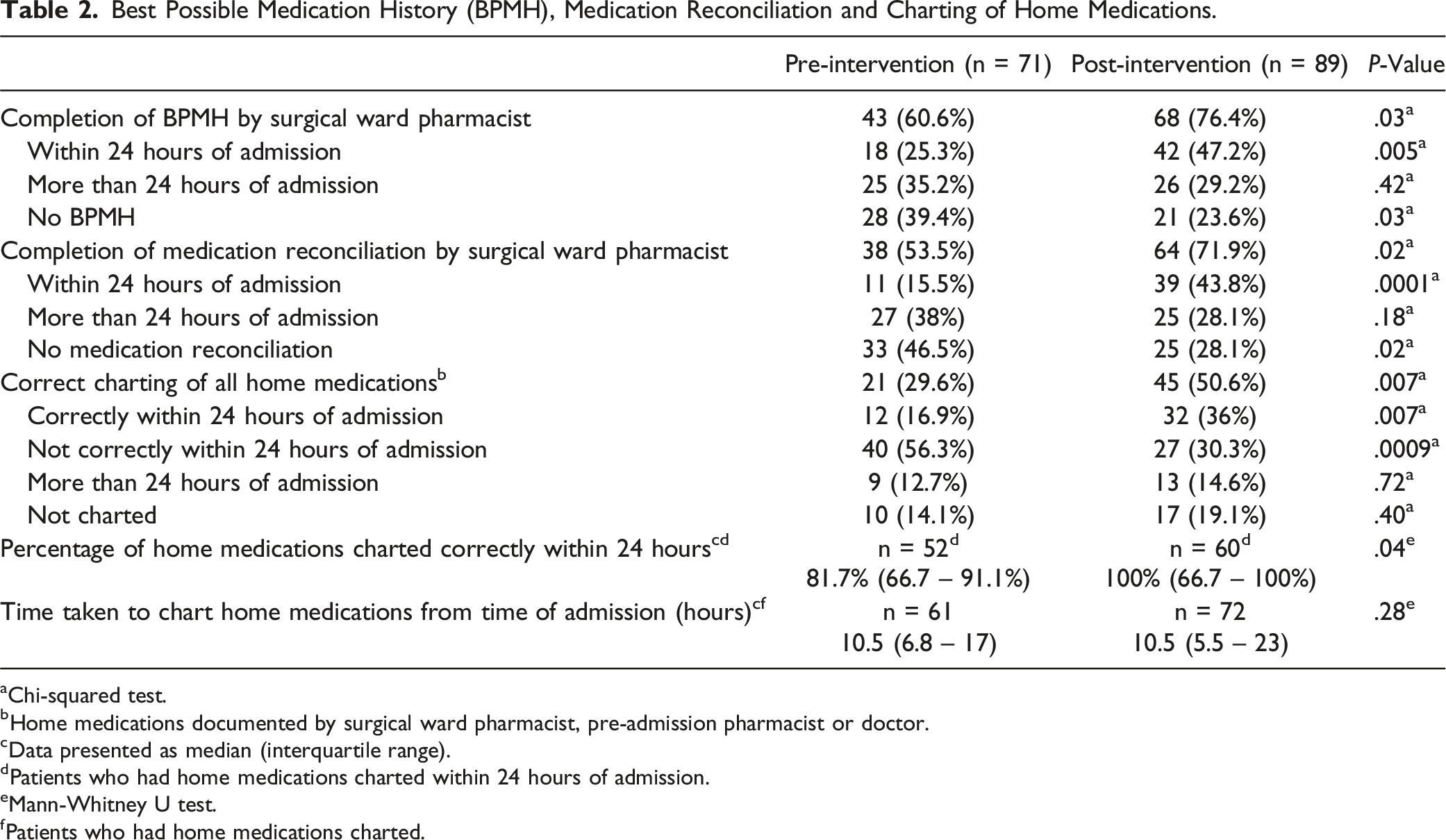
aChi-squared test.
bHome medications documented by surgical ward pharmacist, pre-admission pharmacist or doctor.
cData presented as median (interquartile range).
dPatients who had home medications charted within 24 hours of admission.
eMann-Whitney U test.
fPatients who had home medications charted.
Clinical Interventions
Number and Types of Documented Clinical Interventions.
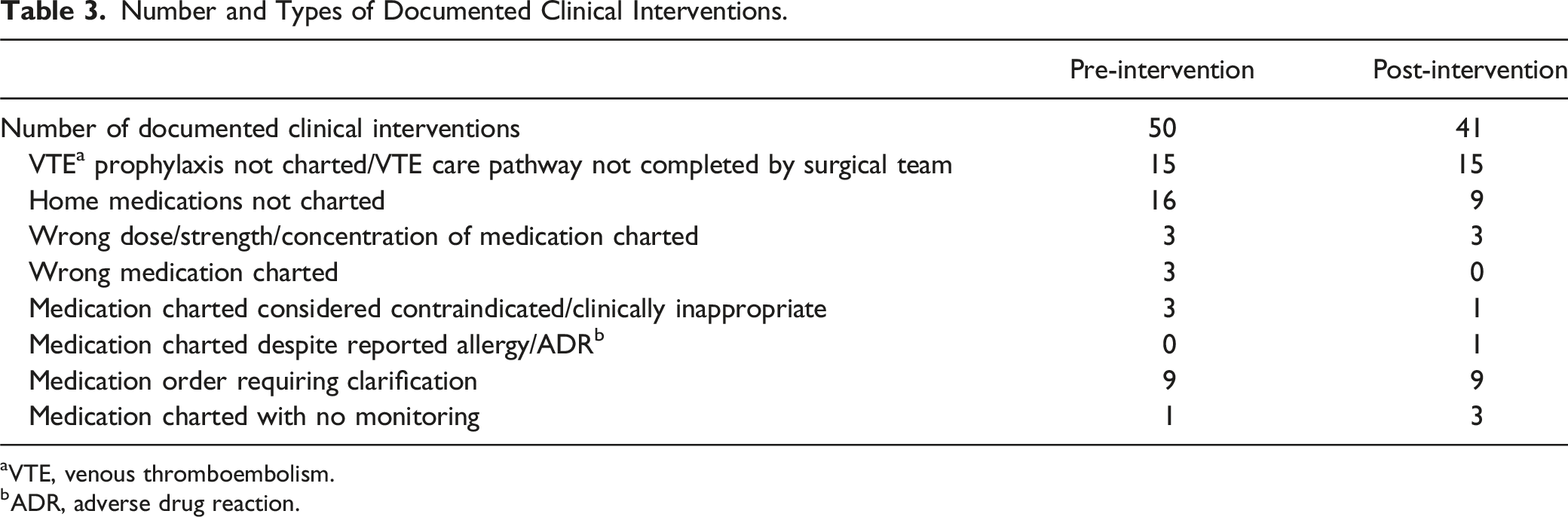
aVTE, venous thromboembolism.
bADR, adverse drug reaction.
Discussion
The introduction of the pre-admission surgical pharmacist at Casey Hospital has improved the completion of BPMHs and medication reconciliation, as well as the charting of all home medications correctly overall, particularly within the first 24 hours of admission. This is consistent with other studies showing the benefits of having pre-admission pharmacists in enabling the availability of accurate medication histories to assist with reducing prescribing errors.9-13,17 The medication reconciliation rate in the pre-intervention group of this study (53.5%) was lower than that of a similar study (75%) used to estimate the sample size. 9 This may be attributed to surgical ward pharmacists in this study using time to confirm with patients for any medication changes on admission, whereas in previous studies patients were asked to contact the pre-admission pharmacists if there were any changes to their medications during the perioperative period. However, the results seen from the introduction of the pre-admission pharmacist with the smaller sample size were still statistically significant.
On admission, there were usually no changes to the home medications documented by the pre-admission pharmacist. This demonstrates another potential benefit of introducing the pre-admission pharmacist role, as the surgical ward pharmacist can complete BPMHs for patients 1 to 3 business days prior to admission when their workload permits with there being minimal medication changes on admission. This may help reduce the workload for the surgical ward pharmacist, by assisting with the prioritisation and planning of the workload for the day, to allow completion of other tasks such as medication chart reviews. One audit showed that the implementation of pre-admission pharmacists allowed clinical ward pharmacists to perform more medication chart reviews, where 85.8% of patients had a medication review within 1 day of admission. 12 Another study showed that more than 30% of surgical patients had a BPMH completed prior to surgery, significantly reducing the burden on the pharmacist workload on the morning of surgery. 17
In the post-intervention group, there were less documented clinical interventions compared to the pre-intervention group. There was a higher proportion of clinical interventions in the pre-intervention group relating to home medications not charted and the wrong medication charted. This finding may be attributed to the surgical doctors having earlier access to the BPMH completed by the pre-admission pharmacist. Additionally, the surgical ward pharmacist could confirm for any medication changes within 24 hours of admission, allowing home medications to be charted if appropriate. The median accuracy of home medications charted correctly within 24 hours of admission was higher in the post-intervention group (100%) compared to the pre-intervention group (81.7%). A study found that 97% of BPMHs completed by health professionals other than pharmacists were associated with at least 1 medication discrepancy, with the most common medication discrepancies being medication omission, wrong frequency and incorrect dose. 18 It was also shown that more than 25% of patients had at least 1 medication discrepancy on the medication chart on admission, which were resolved via medication reconciliation by the pharmacist. 18 This further supports the role that pre-admission pharmacists have in enabling availability of an accurate BPMH, and completing medication reconciliation to reduce prescribing errors.
The implications of this study are that by having accurate BPMHs available on admission, this can increase patient safety by allowing medication reconciliation to be completed in a timely manner and assist with doctors charting home medications correctly to reduce unintentional medication discrepancies. The increased accessibility of the completed BPMH for the surgical doctors may help with decision-making in the perioperative period and recommencement of home medications post-surgery. The pre-admission pharmacist may also be able to identify patients who may not have had appropriate peri-operative medication management and notify the surgical team to avoid surgery cancellations upon admission. 4
One of the strengths of this study was that the pre-admission pharmacist role was completed by a current surgical ward pharmacist, which meant utilising existing resources and demonstrating that surgical ward pharmacists may be able to incorporate the pre-admission pharmacist role into their existing role to allow follow up and continuity of patient care. Some of the limitations to be considered when interpreting the results of this study are that it is a pilot study at 1 hospital site and these results may not be translatable to other hospitals. A large-scale study across multiple hospital sites can be considered in future. This study was completed during the COVID-19 pandemic where elective surgeries were reduced and not consistently scheduled, thus data collection was completed over a longer period of time than originally planned for to recruit participants for this study and the actual recruited sample size was smaller than the estimated sample size. As the number of elective surgeries increases after the COVID-19 pandemic, the pre-admission pharmacist can prioritise the order of which they complete BPMHs for elective surgery patients with planned elective surgery each day, by first contacting all the patients planned for admission in 3 business days, and then if time permits, the patients planned for admission in 2 business days and then followed by the patients planned for admission the next day. There was a significant difference in the number of regular prescribed medications between the pre-intervention and post-intervention groups. This may be attributed to there being more ear, nose and throat (ENT) surgeries in the post-intervention group, who generally had less medical conditions compared to the other surgery types. At the study hospital, elective surgery patients are admitted to the day surgery unit prior to transfer to the surgical ward and therefore, the medication chart is not completed until the patient is transferred to the ward where there may be a delay in the charting of home medications, and the delay of medication reconciliation where the surgical ward pharmacist has left for the day.
Conclusion
Accurate and timely medication charting in surgical patients was improved following the introduction of a pre-admission pharmacist service. It has also helped to reduce the number of documented clinical interventions, specifically clinical interventions relating to home medications not charted and the wrong medication charted. Future studies should explore how the introduction of the pre-admission pharmacist can help to reduce the daily workload of the surgical ward pharmacist.
Footnotes
Acknowledgements
The authors would like to acknowledge Anh Nguyen, Michelle Guo and Praneel Chandra for providing pharmacy services to the Casey Hospital surgical wards, and Emma Agnus and Mayumi Roder for assisting with data collection. The authors would also like to acknowledge Eugene Ong, Samuel Shepherd and Samanta Wood from the Monash Health Pharmacy Education Services for their critical review of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.