
Abstract
Background
There are a variety of emergent conditions that present with dangerously elevated blood pressures and require rapid blood pressure control. 1 The consequences of untreated or undertreated hypertension in these patients can manifest as hematoma expansion in intracerebral hemorrhage, prolonged time to thrombolytic or hemorrhagic conversion in acute ischemic stroke, or aortic wall stress and shearing in acute aortic dissection.2-4 The recommended time to target blood pressure varies from “as soon as possible” to within an hour, with many clinical practice guidelines (CPG) not specifying a time at all due to a paucity of data to make a concrete recommendation.1-5 There is also an emphasis in recent CPGs for not only rapid blood pressure control but precise (and even cautious) blood pressure control.2,3 This shift echoes the changing practice landscape as more evidence is published suggesting high variability in blood pressure and over correction when lowering blood pressure can have negative impacts as well.2,3,5
Nicardipine and clevidipine are both first-line intravenous (IV) dihydropyridine (DHP) calcium channel blockers (CCB) used for rapid blood pressure control. 1 They exert their effects on blood pressure by inhibiting calcium influx into arterial smooth muscle cells, thus reducing peripheral resistance. 6 The major difference with these two medications relates to their pharmacokinetic profile. Clevidipine has a rapid onset of effect and a very short half-life of 1 minute. 7 Nicardipine also has a fast onset of effect, but a longer half-life of 45 minutes, which can cause unintended hypotension if titrated too aggressively; the package insert for nicardipine recommends down titrating once the blood pressure goal is met, which suggests a propensity to over correct. 8 Clevidipine is metabolized by esterase enzymes in the blood and tissues which makes it unaffected by changes in renal or hepatic function unlike nicardipine, which is extensively metabolized by the liver through cytochrome 450 enzymes 3A4, 2D6, 2C8.7,8 Another important difference is that clevidipine is formulated in a lipid emulsion while nicardipine is not. The lipid component of clevidipine may make it undesirable when managing patients with hypertriglyceridemia or acute pancreatitis and is contraindicated in patients with soy or egg allergies. 7
To date, there has been only one randomized controlled trial comparing these agents. 9 The ECLIPSE trial is a randomized, open-label trial that compared clevidipine to nitroglycerin, sodium nitroprusside, and nicardipine for patients with perioperative hypertension before, during, or after cardiac surgery. This study showed no difference between clevidipine and nicardipine with respect to excursions outside of the specified blood pressure range. 9 However, clevidipine had reduced excursions compared to nicardipine when evaluating a tighter systolic blood pressure goal range of 105-145 mmHg compared to the more liberal range of 75-145 mmHg (77.0 mmHg*min/h vs 101.6 mmHg*min/h, P = 0.0231). 9 Four retrospective analyses have evaluated the use of clevidipine vs nicardipine for blood pressure control in neuroscience indications.10-13 None of the studies found a significant difference in the time to target blood pressure goal, percent of time within target blood pressure range, or percent of patients at goal at 1 or 6 hours after infusion initiation (Supplemental Table 1).10-13 Among cardiac surgical patients, Colomy et al found that perioperative use of clevidipine led to a higher percentage of time within blood pressure goal (55.2% vs 36.4%, P = 0.036) and a non-statistically significant reduction in time to blood pressure goal compared to nicardipine (15 min vs 30 min, P = 0.303). 14
The major limitations of these studies are the restrictive inclusion criteria that focus on only one disease state which inevitably led to small sample sizes and therefore underpowered results. Therefore, the aim of this study is to evaluate if there is a difference in the efficacy and safety of clevidipine vs nicardipine when evaluating a broader range of patients in order to lay the groundwork for larger randomized trials on more specific patient-centered outcomes.
Methods
Study Design
This study was a multi-center, retrospective chart review. It was approved by the hospital-system institutional review board. Patients were identified through electronic medical record reports and categorized into two groups based on having received either clevidipine or nicardipine. If a patient received both medications, the patient was classified based on the medication given first chronologically and data were collected only during the first infusion to avoid introducing bias. For example, if a patient received clevidipine in the ED and then was switched to nicardipine at transfer to the intensive care unit (ICU), they would be included in the clevidipine group. The number of patients in each group who received both medications is reflected in the endpoint “both interventions received”.
Patients were matched in a one-to-one fashion based on indication for blood pressure control and similar pre-intervention systolic blood pressures (SBP). As blood pressure goals can vary widely, matching by indication allowed us to control for this factor since patients with the same indication generally have the same evidence-based blood pressure goal. Pre-intervention SBP were stratified into 6 categories: <140, 140-159, 160-179, 180-199, 200-219, or ≥220 mmHg. For ease of matching, aortic dissection (type A and B) and impending aortic ruptures or dissections were consolidated into a category entitled “aortic emergencies” and subarachnoid hemorrhages were included in the group with other types of intracerebral hemorrhages. Cardiac surgery and neurosurgery were not subdivided based on the type of surgery.
Patients
Patients were included if they met the following criteria: age
Practice Site
The health system includes 7 acute care hospitals, ranging in size from 122 to 867 inpatient beds with a range of zero to 85 ICU beds. Three of the hospitals were designated trauma centers and volume of emergency department visits ranged from 27,795 to 96,419 visits per year. Institution titration protocols are as follows: clevidipine starting dose 2 mg/hr, max dose 16 mg/hr, titrate by 2 mg every 2 minutes or every 5 minutes when within 20 mmHg of the SBP goal; nicardipine starting dose 2.5 mg/hr, max dose 15 mg/hr, titrate by 2.5 mg every 15 minutes.
Outcomes
The primary outcome was time within range, which was defined as percentage of time within target SBP range, from nicardipine or clevidipine infusion initiation until order discontinuation or 24 hours later, whichever occurred first. The percentage of time in range was calculated based on last recorded value carried forward until a new value was recorded and the sum of the total time in range was divided by the total length of the infusion. The secondary outcomes were time to blood pressure goal, incidence of hypotension during infusion, and use of rescue medications during infusion. Time to blood pressure goal was defined as time from nicardipine or clevidipine initiation to first SBP reading in target SBP range and diastolic blood pressure (DBP) in target DBP range, as indicated on the order. To ensure consistency, readings for blood pressures were taken from cuff readings rather than arterial lines, unless cuff readings were not available. Hypotension was defined as SBP <90mmHg. 15 Rescue medications were defined as any IV anti-hypertensive medication (infusion or bolus) used in addition to nicardipine or clevidipine when the blood pressure was not at goal, which included labetalol, esmolol, diltiazem, hydralazine, nitroglycerin, or sodium nitroprusside.
Statistical Analyses
Based on feasibility, the sample size for this study consisted of 200 records, evenly distributed as 100 in each group. The power calculated was based on the primary endpoint of percent of time in target blood pressure range using a baseline value of 79% and a clinically meaningful difference of ±5%. 10 To achieve 80% power using, approximately 1870 records would be needed, which could not be feasibly done. Therefore, sample sizes of 100 in each group would attain 13%-15% power to detect a difference between the group proportions of 0.05, using a two-sided Z-Test with pooled variance with a significance level of 0.05.
Descriptive statistics were provided for all variables as a function of level of care and for the combined data set. All continuous data were evaluated for normality of distribution. Continuous data were summarized with means and standard deviations (SD) for normally distributed data, or with median and interquartile ranges (IQR) for non-normally distributed data. Categorical variables were reported as frequencies, using percentages. Continuous data were compared between the two treatment groups using a Student’s t test for parametric data or a Mann-Whitney U test for non-parametric data. For comparisons by higher-order grouping, an analysis of variance (ANOVA) or Kruskal-Wallis H test was used. Categorical data were analyzed using a Pearson chi square test or, for 2x2 tables with small cell sizes, a Fisher’s Exact test. All analyses were performed with SPSS v. 26 (IBM; Armonk, NY 2019) using an a priori alpha level of 0.05, such that all results yielding P < 0.05 were deemed statistically significant.
Results
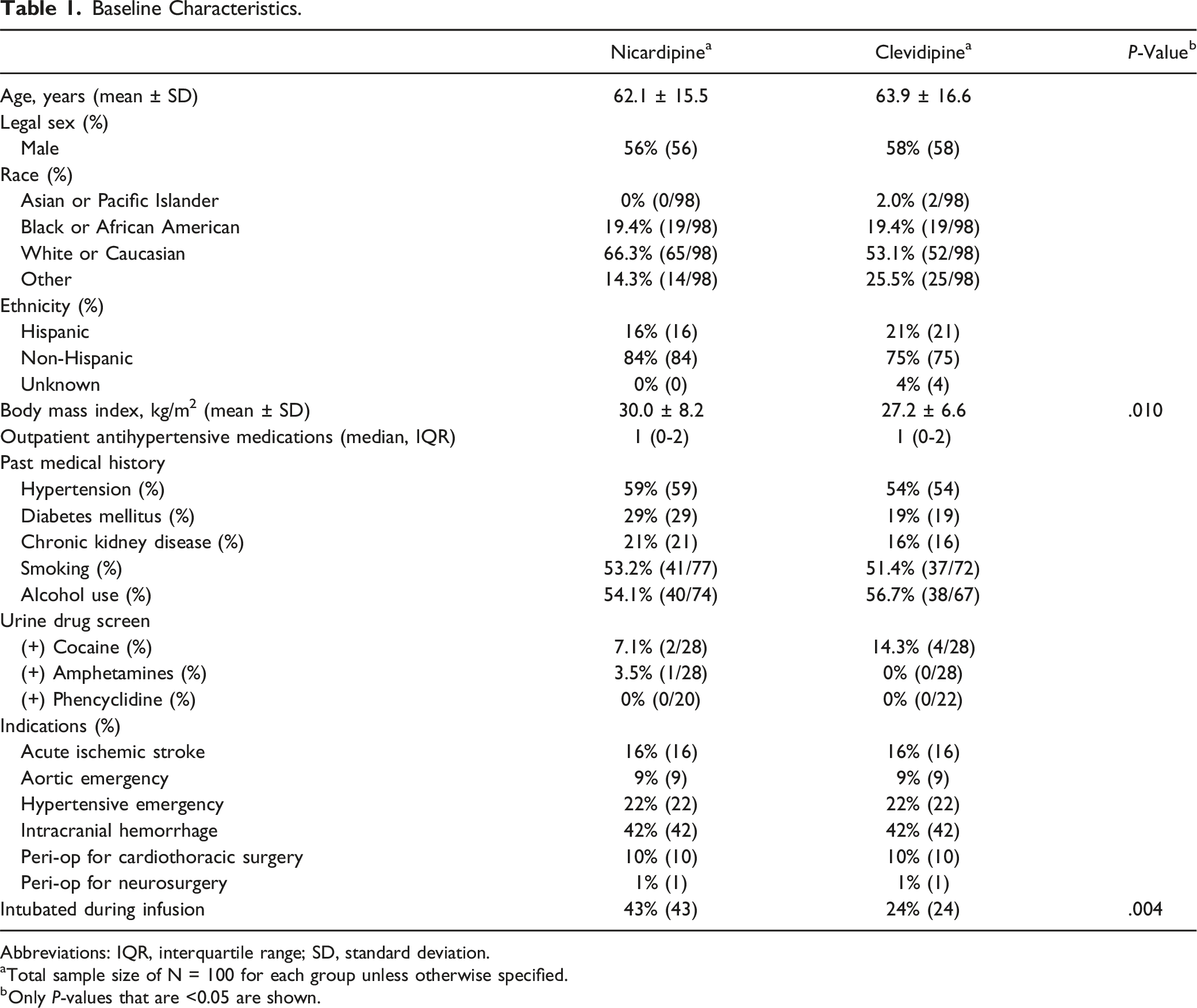
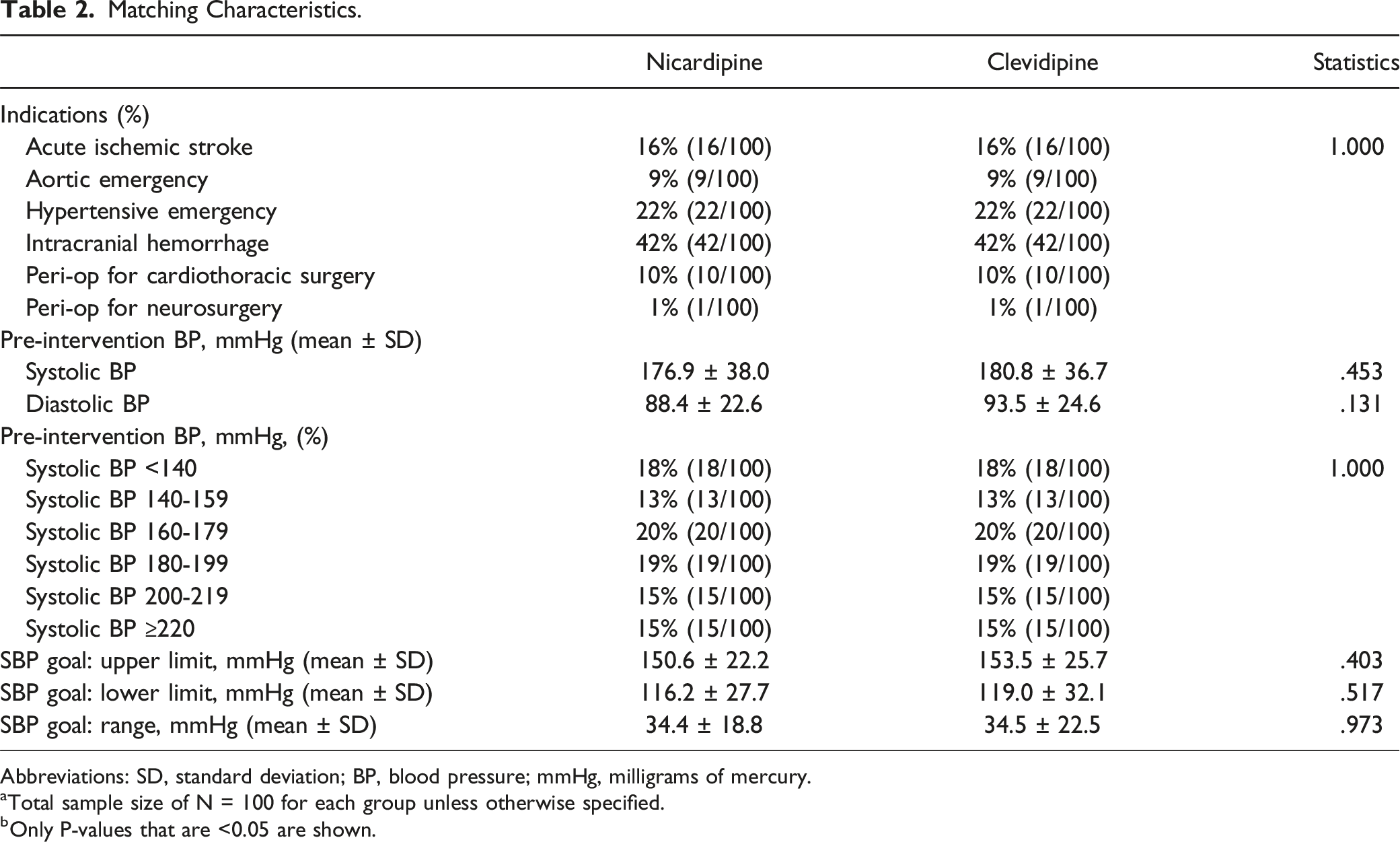
A total of 569 patients who received care between June 1, 2020 and June 30, 2021 were screened to reach the designated sample size, which resulted in 100 matched pairs who met inclusion and exclusion criteria (Figure 1). Baseline characteristics of each group are shown in Table 1. The baseline characteristics were well balanced between groups with the exception of BMI, which was statistically higher in the nicardipine group. Characteristics used to match pairs are shown in Table 2. The majority of pairs included in this study had an intracranial hemorrhage (42%) followed by hypertensive emergency (22%) and acute ischemic stroke (16%). There was an even distribution among the SBP blood pressure strata and a similar mean SBP and DBP prior to intervention in each group. Additionally, the mean SBP goal range was similar in size between groups (34.4 ± 18.8 vs 34.5 ± 22.4 mmHg, P = 0.973) Table 2. Patient flow diagram. Baseline Characteristics. Abbreviations: IQR, interquartile range; SD, standard deviation. aTotal sample size of N = 100 for each group unless otherwise specified. bOnly P-values that are <0.05 are shown. Matching Characteristics. Abbreviations: SD, standard deviation; BP, blood pressure; mmHg, milligrams of mercury. aTotal sample size of N = 100 for each group unless otherwise specified. bOnly P-values that are <0.05 are shown.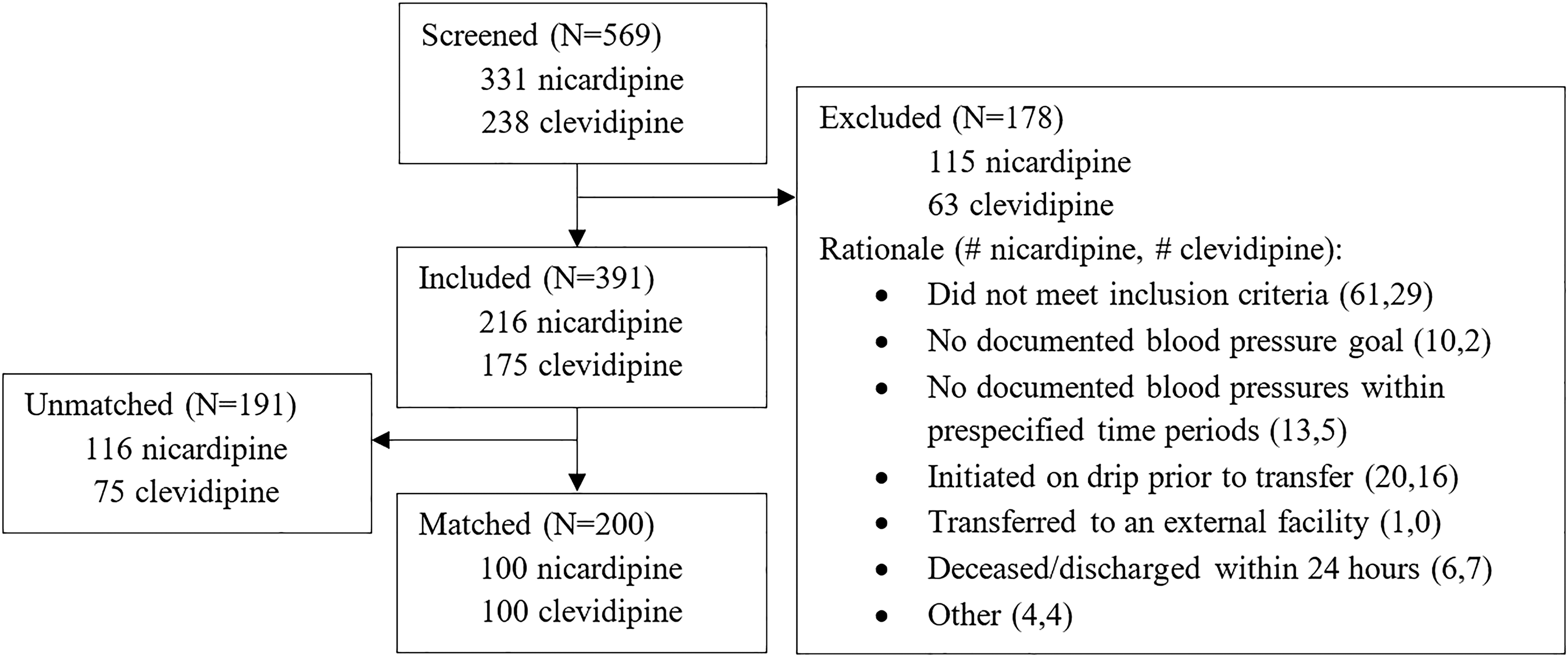
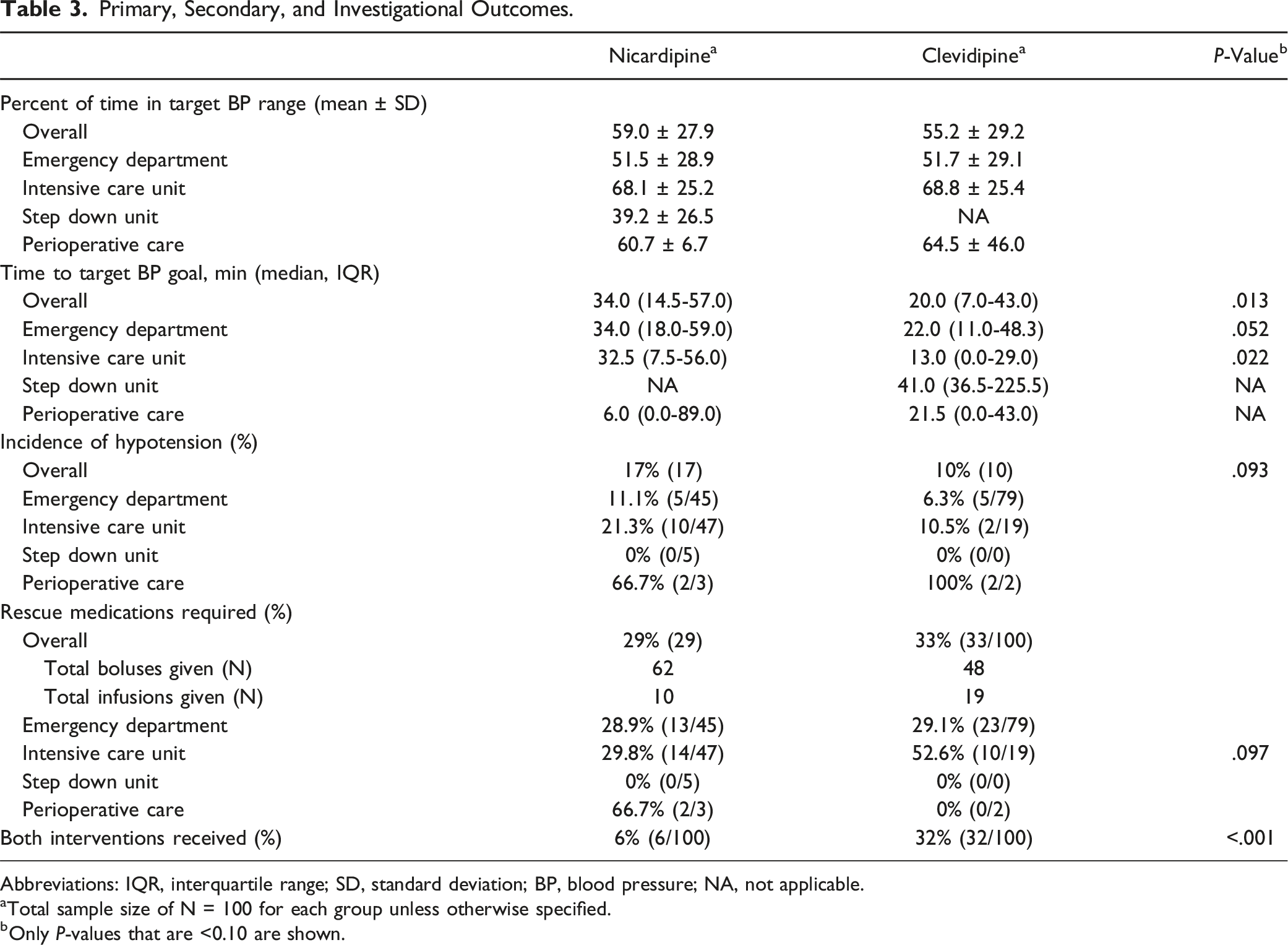
Primary, Secondary, and Investigational Outcomes.
Abbreviations: IQR, interquartile range; SD, standard deviation; BP, blood pressure; NA, not applicable.
aTotal sample size of N = 100 for each group unless otherwise specified.
bOnly P-values that are <0.10 are shown.
Characteristics of the Hospital Stay.
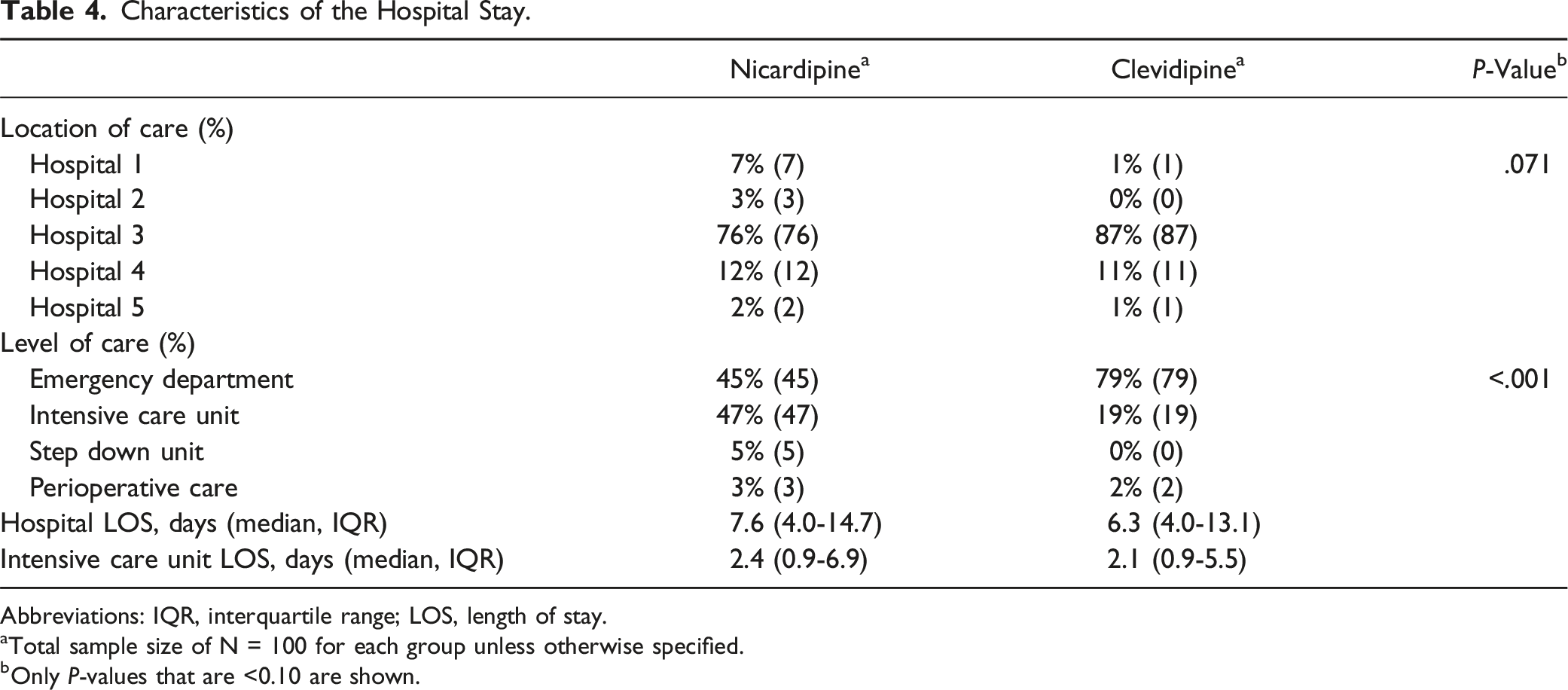
Abbreviations: IQR, interquartile range; LOS, length of stay.
aTotal sample size of N = 100 for each group unless otherwise specified.
bOnly P-values that are <0.10 are shown.
Description of Infusion Parameters.
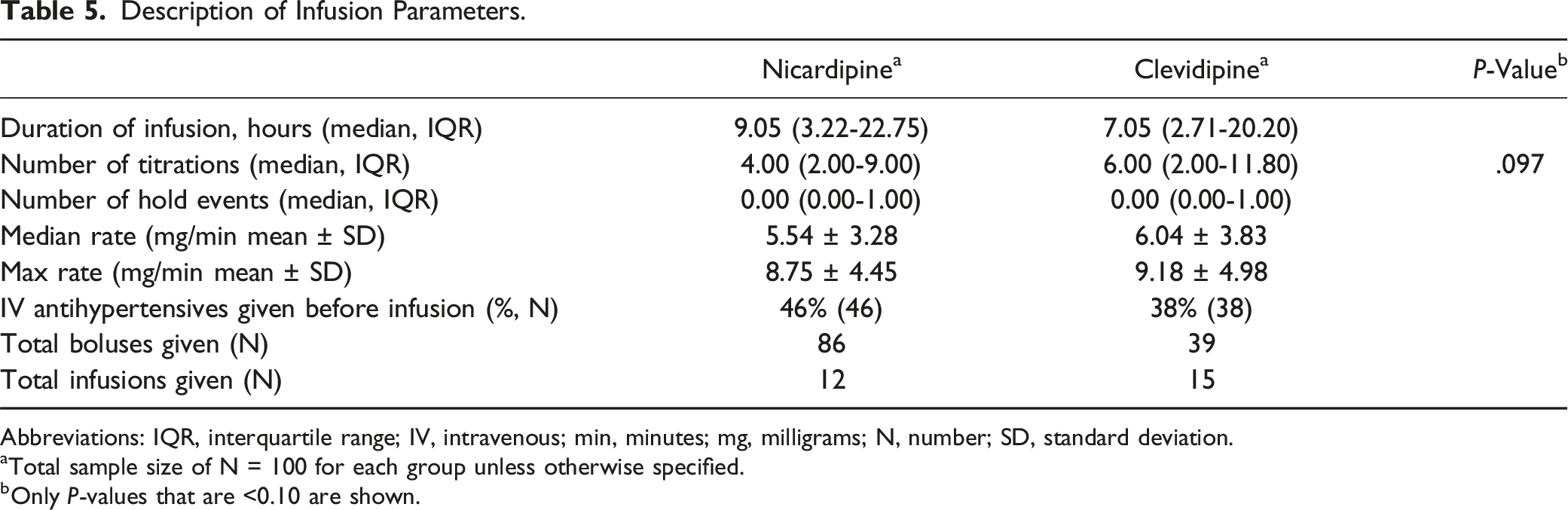
Abbreviations: IQR, interquartile range; IV, intravenous; min, minutes; mg, milligrams; N, number; SD, standard deviation.
aTotal sample size of N = 100 for each group unless otherwise specified.
bOnly P-values that are <0.10 are shown.
Discussion
This study demonstrates that clevidipine was associated with a significantly faster time to target blood pressure compared to nicardipine among a diverse population of patients across a large healthcare system. This finding was most pronounced in the ICU setting where clevidipine reached the goal blood pressure approximately 20 minutes faster than nicardipine. Although the percentage of time in goal blood pressure range was similar between the two groups, nicardipine use was associated with non-significantly greater incidence of hypotension and required more IV boluses overall. This likely reflects the effects of the longer half-life with nicardipine and inability to titrate the infusion as quickly as clevidipine.
The time to target blood pressure has been assessed in a handful of retrospective analyses (Supplemental Table 1). With the exception of Saldana et al and Rosenfeldt et al, all of the previous retrospective studies showed similar trends, but none reached significance for this endpoint, presumably as a result of being underpowered.10–14 Despite the fact that our study was also underpowered, we enrolled enough patients to see a significant difference favoring clevidipine, which corroborates the trends seen in previous studies.
Our study showed that clevidipine and nicardipine produced a small (non-significant) numerical difference in percent of time in range overall, which was negligible when stratified by location of care. This can be attributed to the fact that more patients who received clevidipine were treated in the ED whereas more patients who received nicardipine were treated in the ICU. The nursing ratios are quite different in these settings (one-to-two in the ICU vs one-to-five or higher in the ED), which has an impact on the ability to closely monitor and titrate a drip. The differences seen here are reflective of the provider preferences within the health system: anecdotally, the physicians in the ED tend to favor clevidipine and the ICU physicians tend to favor nicardipine. This observation also is supported by the fact that patients who received clevidipine were more likely to be switched to nicardipine over the course of their care as they transitioned from the ED to the ICU. Since the ICU had higher percentages of time in range, this works against clevidipine when interpreting the overall analysis. Previously published literature did not differentiate between settings of care when reporting outcomes so it is impossible to report whether this trend is present elsewhere.10–13
The size of the target range is another factor that can impact percentage of time in blood pressure range.9,14 Both the ECLIPSE trial and the study by Colomy et al demonstrated a difference between clevidipine and nicardipine when looking at a tighter blood pressure range of 40 mmHg or 30 mmHg, respectively.9,14 This suggests that clevidipine may be a better agent to use when patients require tighter blood pressure control; however, despite having the same range (34 mmHg) in our study as Colomy et al, these findings were not replicated. 14
The optimal blood pressure endpoint may also vary by indication. For example, the time to goal for acute ischemic stroke is key for reducing the time to alteplase administration and ensuring it can be given within the three to four-and-a-half hour window. 3 For other indications like intracranial hemorrhage or aortic dissection, the percentage of time in range may provide a better overview of blood pressure control rather than time to target. These are surrogate endpoints that do not directly measure the effect on functional outcomes or mortality. A future direction that would solidify the findings in this paper would be to assess outcomes such as in-hospital mortality, 30-day mortality, and level of disability, as assessed by the modified Rankin scale (mRS). More patient-centered outcomes like these would be best assessed within each respective disease state, as the key outcome metrics may vary. For example: with an ischemic stroke mRS 3-12 months after the event may be most meaningful compared to aortic emergency where in-hospital mortality may be more relevant.
The key outcome assessing safety in this study was incidence of hypotension. Based purely on pharmacokinetics, nicardipine is more likely to be over-titrated based on its longer half-life but the findings from the previous studies do not universally support this hypothesis. In our study, there was a non-significant increase in episodes of hypotension associated with nicardipine use compared to clevidipine, which remained true when stratified by location of care. However, there were several possible confounders of this endpoint, primarily intubation during infusion and IV antihypertensives used prior to infusion. Since many of the agents used for sedation in intubated patients (i.e., propofol, midazolam) can cause hypotension, this may have interfered with the hemodynamics. An additional consideration is that this study was not powered to see a difference in this outcome, and a larger sample size may have produced a significant finding for hypotension. A future direction that would confirm the numerical trends seen in this paper and shed light on the clinical impact of hypotension would be to assess the patient centered outcomes associated with hypotension, such as myocardial ischemia, cerebral ischemia, and acute kidney injury. These outcomes would be best assessed within each respective disease state, as the pathophysiology of the disease process may impact likelihood of adverse outcomes associated with hypotension. For example: with an intracranial pathology (ischemic stroke, intracranial hemorrhage, or subarachnoid hemorrhage) there is higher risk of ischemia with hypotension due to loss of autoregulation which may occur at higher systolic blood pressure values than in a patient who required blood pressure control for an aortic dissection or cardiac surgery.16,17
The strengths of this study include having a larger population of patients compared to most of the previously published trials. We also evaluated a broad range of patients with several different types of indications. The two groups in our study were well-matched at baseline, with the exception of BMI and percent of patients intubated.
Limitations of the study include the frequency of charting for the accuracy of the endpoints related to blood pressure. This study was underpowered for the primary endpoint based on the low feasibility of obtaining 1870 patients to detect a difference of ±5% between the two groups, which was a known limitation at study inception. The institutional titration protocol for clevidipine and nicardipine both deviate from the package insert and may alter results when different titration parameters are used. There were no statistical tests performed to deduce if duration of infusion impacted the outcomes. There was an underrepresentation of cardiothoracic and neurosurgical patients due to matching constraints since nicardipine was preferred almost exclusively for these patients. Additionally, poor documentation made it difficult to ascertain the exact reason why a provider switched from one agent to the other.
Conclusion
This study suggests that while clevidipine and nicardipine produce similar percentages of time in range, blood pressure control can be attained faster using clevidipine with similar rates of hypotension and rescue medication requirements. These findings remain consistent across diverse patient populations and various settings of care in a large health system. These findings reflect the pharmacokinetic differences in these medications and demonstrate that clevidipine is as safe and potentially more effective than nicardipine for rapid blood pressure control.
Supplemental Material
Supplemental Material - Impact of Clevidipine Versus Nicardipine on Time in Range when Lowering Blood Pressure (CTRL-BP)
Supplemental Material for Impact of Clevidipine Versus Nicardipine on Time in Range when Lowering Blood Pressure (CTRL-BP) by Kaitlin J. Armstrong, Kelly Shepard, Michelle Horsfield, Alexander R. Levine, David M. O’Sullivan, and Abigail L. Zeiner in Journal of Pharmacy Practice
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.