
Abstract
Purpose
This study assessed the impact of an integrated health system specialty pharmacy (HSSP) on viral load (VL) suppression in HIV patients, compared to patients utilizing non-health system specialty pharmacies (non-HSSPs).
Methods
This was a single-center, retrospective observational cohort study of patients ≥18 years with a HIV diagnosis and an encounter in the outpatient HIV clinic at an academic medical center associated with a HSSP, at least one order for an antiretroviral (ARV) medication, and at least one HIV-1 RNA VL result between January 2018 and May 2022. Outcomes included average rate of VL suppression and socio-demographic factors associated with VL suppression. Comparison of VL suppression between groups was tested using a generalized estimating equation logistic regression.
Results
From January 2018 to May 2022, 889 patients met the inclusion criteria; 326 provided VL results while filling at the HSSP and 681 had results while filling through a non-HSSP (118 patients provided results in both groups). Of the 5295 VL results, 90.6% reflected VL suppression, with the average rate of 91.0% in the HSSP group vs 86.0% in the non-HSSP group (adjusted OR = 1.89 95% CI: [1.40, 2.56]). Sex, ethnicity, and race were not associated with VL suppression. However, VL suppression decreased significantly with Charleson Comorbidity Index 1-3; increased with age; and increased over time from VL index date.
Conclusions
HIV patients filling ARV therapy through a HSSP had a higher rate of VL suppression than those filling through non-HSSPs, highlighting the potential clinical benefit of this specialty pharmacy model.
Keywords
Key Points
• Patients with HIV on complex medication regimens face challenges to adherence, which may affect their clinical outcomes. • Integrated health system specialty pharmacies (HSSPs) provide specialized services for HIV patients, which may help overcome barriers to medication access and adherence. • This study demonstrates that patients filling HIV prescriptions at a HSSP had higher viral load suppression compared to the group using traditional specialty pharmacies. Utilization of HSSPs may lead to improved clinical outcomes for HIV patients.
Introduction
Patients with HIV who adhere to antiretroviral (ARV) therapy can achieve and maintain viral load (VL) suppression (defined as <200 copies of HIV/mL).1,2 VL suppression is associated with reduced risk of disease complications, progression to AIDS and death, and significantly reduces the risk of viral transmission. Adherence to ARV therapy is critical to attaining optimal medication efficacy and clinical outcomes through the achievement and maintenance of VL suppression, which has been demonstrated previously.3-5 However, patients with HIV on ARV face multiple barriers to adherence including, but not limited to, medication side effects, drug access issues, financial barriers including high medication out-of-pocket costs, and social challenges such as stigma surrounding the disease.
Specialty pharmacies, which are licensed by states and often accredited by third-party national organizations, primarily dispense high-cost medications for patients with chronic conditions such as HIV, cancer, rheumatoid arthritis, and multiple sclerosis. 6 Compared to retail pharmacies that dispense primarily lower-cost, less-complex medications, specialty pharmacies are well-equipped to improve adherence to ARV therapy and achieve optimal clinical outcomes for patients with HIV/AIDS. These pharmacies often provide additional services and support for patients, including disease management programs, medication therapy management, medication counseling, financial assistance programs, and specialized delivery services. 6
Within the rapidly growing specialty pharmacy industry, an emerging operational and clinical practice model is that of integrated health system specialty pharmacies (HSSPs), defined as “an integrated advanced practice model that incorporates specialty medication-use management across the continuum of care.” 7 Bridging pharmacy and medical care with health system clinics, the HSSP model utilizes a framework that is patient-centric and involves a systematic cadence of assessments, patient-reported and objective outcome measures, education, and advocacy. An integrated model for specialty pharmacy allows for coordinated care, centralized access to prescribers and medical information through a shared electronic medical record (EMR), and improved communication for both the patient and provider.7,8 Although patients are often limited to filling their specialty medications through traditional specialty pharmacies due to insurance mandates, patients may choose to use a HSSP if it is allowed within the pharmacy benefit.
A HSSP model may help patients with HIV overcome barriers to medication access and adherence, ultimately leading to better clinical outcomes. Models integrating specialty pharmacy services with a health-system outpatient infectious disease clinic have demonstrated enhancements in patient monitoring and prescription adherence. 9 Furthermore, a HSSP model has been shown to result in improved outcomes and reduced medical expenses for specialty pharmacy patients, when compared with patients utilizing traditional specialty or retail pharmacies.10-12 Despite literature that suggests a HSSP model plays an important role in overcoming barriers to ARV medication adherence for patients with HIV, data regarding the impact of HSSPs on HIV VLs are limited, especially in comparison to traditional specialty pharmacies. 13
The primary objective of this study was to assess the impact of a HSSP on VL in HIV patients, compared with those utilizing a traditional, non-health system associated specialty pharmacy (non-HSSP).
Methods
This was a single-center, retrospective observational cohort study of patients aged ≥18 years with a diagnosis of HIV and at least one encounter at an outpatient HIV clinic associated with an academic medical center and an affiliated integrated specialty pharmacy. The clinic, which has an enrollment of approximately 750 patients, is located in an urban setting in Central Massachusetts. Patients were identified from the EMR for analysis if they had at least one order for an ARV medication and at least one HIV-1 RNA VL result between January 2018, when the specialty pharmacy initiated services, and May 2022. HIV-1 RNA VL results were excluded if the interval between two results was longer than 18 months. A cut-off of 18 months was selected because maintenance HIV monitoring laboratory tests typically are required to be drawn at least once annually; any gap in laboratory testing longer than 18 months would indicate loss to follow-up. In this case, the VL result 18 months or longer after the previous VL result as well as any subsequent VL labs were excluded. This study was approved by the academic medical center’s Institutional Review Board.
Data were extracted from the health system’s EMR through a standard request process to the organization’s information technology group, which generated four file types: demographic data, prescription data, laboratory data, and comorbidities. Patient demographic data requested included: age, sex, race, ethnicity, language, and primary insurance type. Prescription data from the EMR was used to identify ARV medications ordered, and diagnosis codes were used to create the list of associated comorbidities. The laboratory data file included all HIV-1 RNA VL results reported within the EMR over the study period. Presence of VL suppression was defined as HIV-1 RNA <200 copies/mL. 2 Date of first ARV prescription fill with the HSSP was determined using fill data acquired from the prescription dispensing records.
VL laboratory test results were classified according to whether patients were filling ARV medications within the HSSP or non-HSSP. Time of first HSSP fill date, defined as the date of prescription adjudication, from the health system’s prescription fill data was used to identify patient start time in the respective pharmacy. Patients without any ARV prescription fills indicated at the HSSP were identified as filling only at the non-HSSP. VL results were divided into time under HSSP or non-HSSP. Figure 1 illustrates three patient timelines depending on the VL results and the location at which the patient was filling their ARV therapy. In the first scenario, all VL results were collected while the patient was filling their ARV at a non-HSSP, whereas in the second case, all VL results were collected while the patient was filling through the HSSP. The third scenario depicts a patient for whom VL results were collected while the patient was filling at a non-HSSP before switching to a HSSP. Patient Viral Load Lab Results Over Time (each vertical line represents a lab result)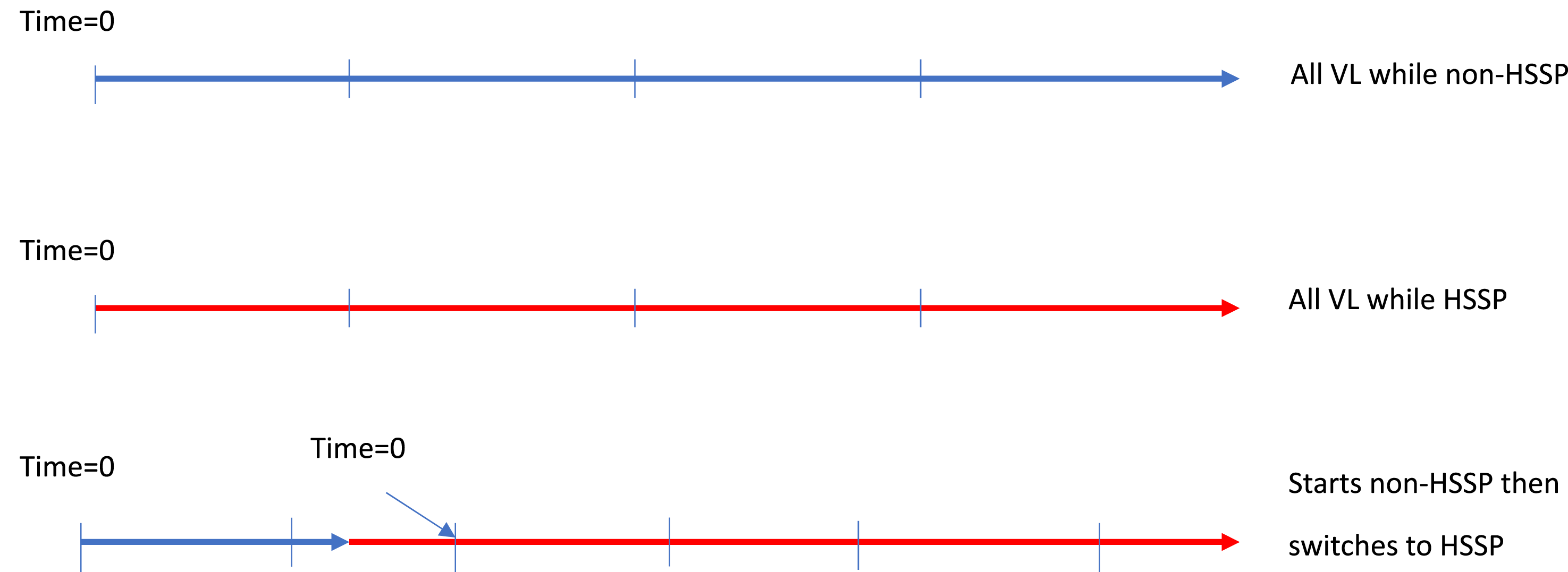
The index time/follow up date (time = 0) was defined as that of the first VL result for patients in either the HSSP or non-HSSP group. The analysis included all VL results for eligible patients during the study period. However, if a patient had VL results that fell within both groups, those results were counted toward the group to which the patient was assigned at the time of the result. Charleson Comorbidity Index (CCI) score 14 was calculated using the Charlson Stata module.15,16
Statistical Analysis
Demographic characteristics at the time of each patient’s first VL result were analyzed using ANOVA for comparison of means and Fisher’s exact test for categorical measures. Distribution of time between lab results between the HSSP and non-HSSP groups was compared using Kruskal-Wallis test. An overall rate of VL suppression across all tests was estimated, then the rate of VL suppression within each patient was estimated and averaged within each group.
The primary analysis comparing VL suppression between HSSP and non-HSSP groups used generalized estimating equation (GEE) logistic regression to account for multiple VL measures within patients. Unadjusted odds ratios (ORs) were estimated for HSSP vs non-HSSP and for patient characteristics. Adjusted ORs were estimated using gender, age, race, ethnicity, CCI, and time from index date. All available covariates were used in the adjusted model to avoid biases that can occur when using variable selection methods. Estimated ORs and 95% confidence intervals are shown, with OR >1 indicating greater VL suppression. Analyses were carried out with Stata 17 (StataCorp, LLC, College Station, TX).
Results
Within the study period, 889 patients with a total of 5295 VL results meeting the outlined inclusion criteria were identified. Each eligible patient had a range of 1 to 24 VL results (Supplemental Table 1). A total of 141 VL results from 71 patients were excluded, as they exceeded the 18-month duration cut-off between results (no patient was excluded due to this criterion). Figure 2 outlines the number of patients and VL results in each of the groups. Of these patients, 326 provided VL results while filling through a HSSP and 681 contributed results while filling through a non-HSSP; 118 patients provided results for both groups. Of the 5295 total VL results, 2028 were from patients while in the HSSP group and 3267 from those while in the non-HSSP group. Since some patients provided VL results to both groups, the total number of patients in both groups add up to more than the total number of eligible patients. Of the 5295 total VL results, 90.6% indicated VL suppression, with an average rate of 91.0% in the HSSP group vs 86.0% in the non-HSSP group (adjusted OR = 1.89 95% CI: [1.40, 2.56]). Eligible Patients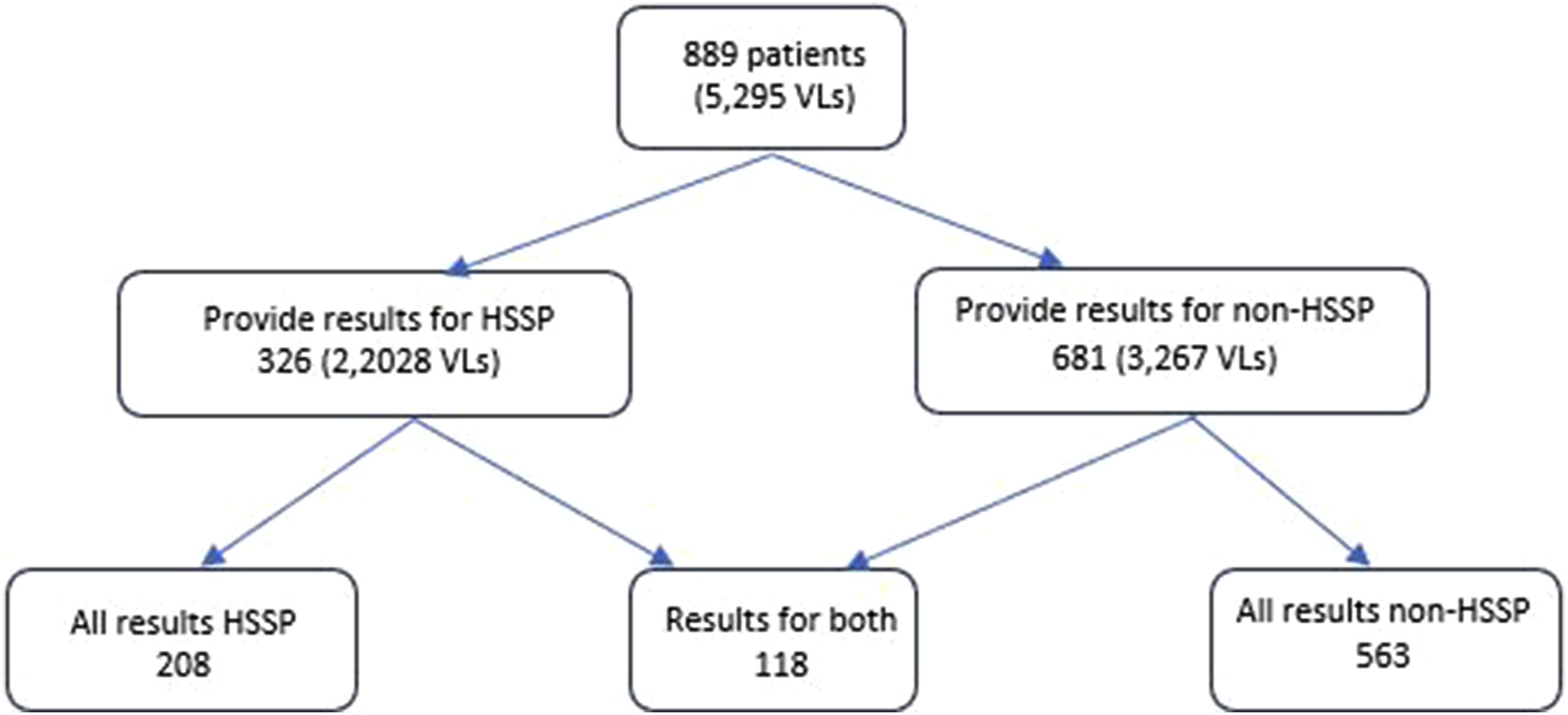
Baseline Characteristics
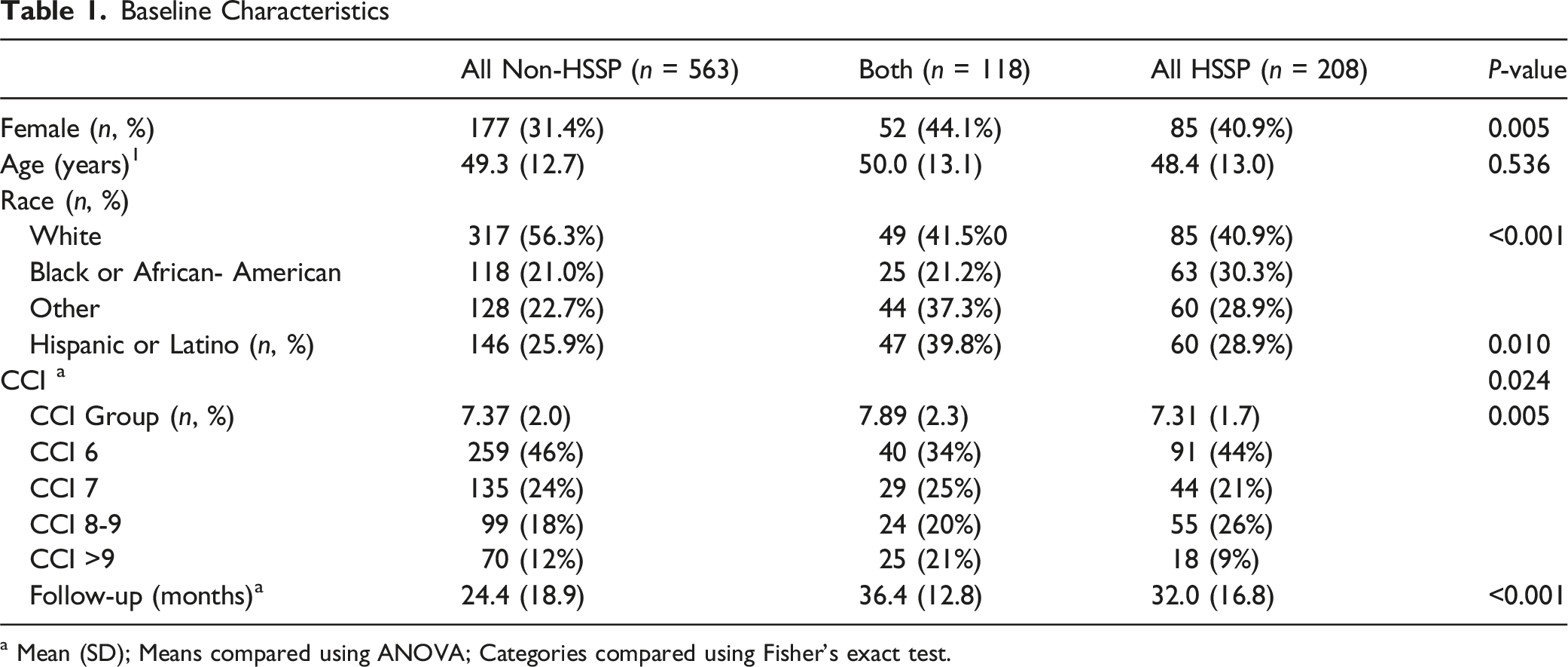
a Mean (SD); Means compared using ANOVA; Categories compared using Fisher’s exact test.
Multivariate Analysis of Factors Associated With HIV Viral Load Suppression
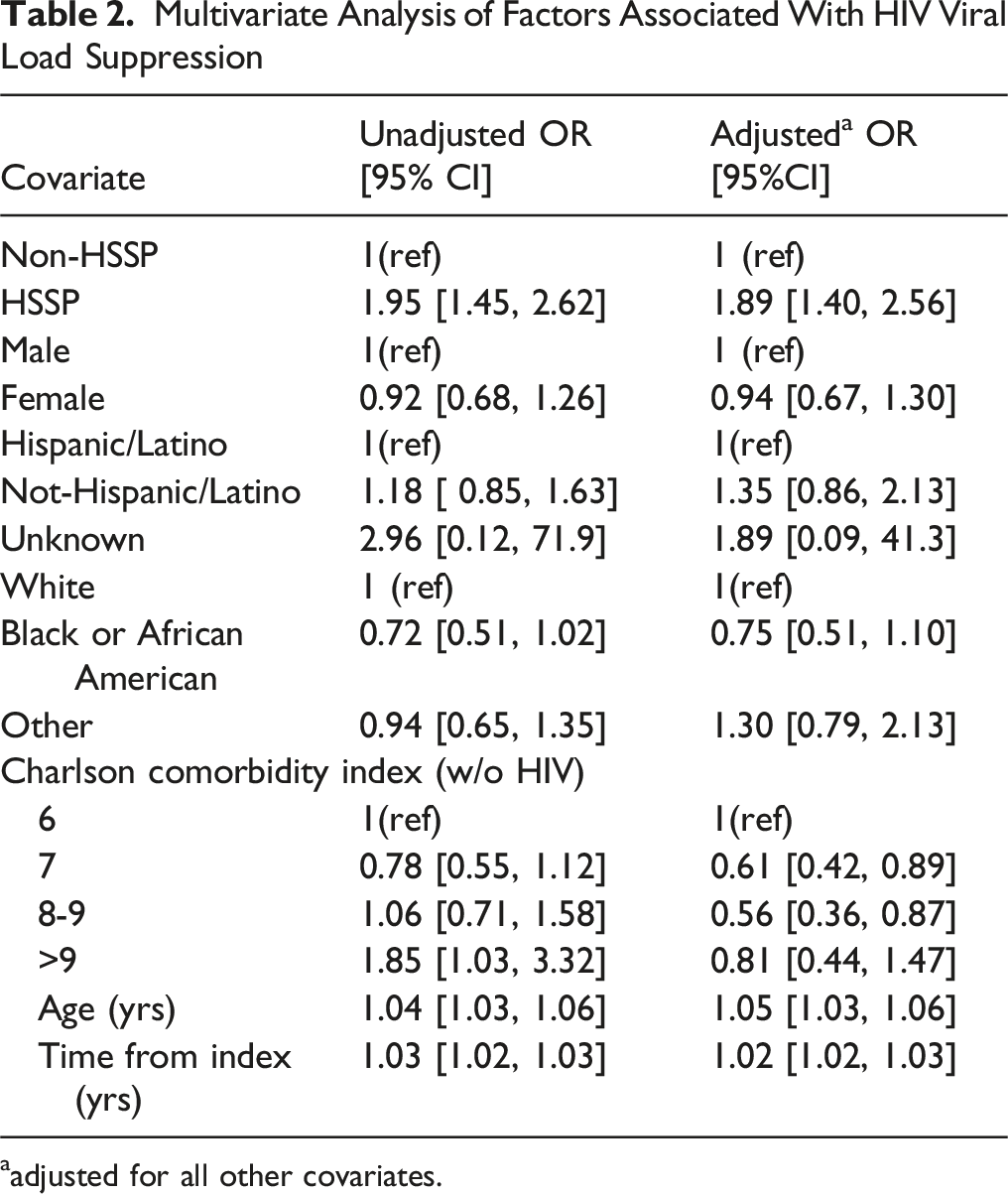
aadjusted for all other covariates.
Discussion
Overall, the group of patients with HIV filling ARV therapy through the HSSP had a significantly higher rate of VL suppression than the group filling through traditional, non-integrated specialty pharmacies. Although several studies have investigated the role of pharmacy services and specialty pharmacies on medication adherence and clinical outcomes in this population, data on the impact of HSSPs in the management of patients with HIV are limited. One recent study evaluated the impact of a HSSP service on ARV medication adherence rate, VL, and CD4 count, compared to a group utilizing non-integrated specialty pharmacies. However, in this study, when the two groups, each with ≤50 patients, were compared, there was no statistically significant difference in VL suppression. 13 The large sample size of our study and access to VL results from HIV patients in both groups allows for a robust comparison of the impact of an integrated HSSP with that of traditional, non-integrated specialty pharmacies on VL suppression.
The integrated health system model for specialty pharmacy services encompasses a more comprehensive level of support for patients with complex, chronic diseases, including close follow-up by pharmacy liaisons and clinical pharmacists, which may contribute to superior clinical outcomes. Integrated clinical pharmacists ensure optimal adherence to medications through comprehensive initial medication counseling and cadenced follow-up reassessments to address side effects, toxicities, and barriers to compliance.8,17 Access to the EMR allows for cohesive communication with health-system clinicians, facilitating immediate resolution of barriers to medication access. Access to results of patient laboratory test monitoring, including HIV VL results, allows clinical pharmacists to detect delayed lab monitoring and identify opportunities to optimize therapy. Furthermore, specialty pharmacy liaisons within the HSSP model engage patients by telephone with monthly refill notifications, which reinforces adherence to medications. Previous studies have demonstrated the impact of a HSSP model on outcomes including time to therapy approval and initiation, medication adherence, and continuity of care.18,19 The multiple layers of patient support provided by the HSSP may have contributed to the higher level of VL suppression observed in the group utilizing the HSSP in our study.
In our study, patients in the non-HSSP group demonstrated high VL suppression rates at the index time, possibly due to the same amount of initial support from the HIV clinic that was received by patients in the HSSP group. It is important to recognize that all patients prescribed specialty medications from the clinic receive the same level of basic specialty pharmacy services from the integrated specialty pharmacy, regardless of the pharmacy at which they ultimately fill their ARV therapy. Upon receipt of a specialty medication prescription, the HSSP staff investigate benefits and obtain required prior authorization, regardless of the pharmacy at which the prescription is ultimately filled. After these initial steps are completed, the medication is dispensed by the specialty pharmacy if allowed by the insurance provider and selected by the patient. Often, a patient may wish to use the HSSP but is mandated to use a payor-owned specialty pharmacy, which poses a challenge to the expansion of the health system model. The additional layers of services that are subsequently provided to patients in the HSSP group, including prescription refill reminders and pharmacist assessments from the HSSP, may have contributed to higher patient engagement and adherence, which has been demonstrated previously, allowing for a higher subsequent rate of VL suppression in that group. 13
In our study, we observed an association between the higher level of VL suppression and lower CCI in the HSSP group. Patients with a greater number of comorbidities and associated polypharmacy may experience more challenges in medication adherence managing their HIV, which ultimately could impact the level of VL suppression that they achieve.20,21 Furthermore, polypharmacy associated with a higher number of comorbidities increases pill burden or may lead to unrecognized drug interactions, impacting VL suppression.
VL suppression increased over time from the index VL, indicating that longer duration of ARV therapy is associated with greater VL suppression. The observed association of higher VL suppression with increased patient age may also be due to a longer duration of treatment in this group. Older patients who have been receiving long-term treatment may be more adherent because of their prior experience with multiple pill ARV regimens. A reduced risk for non-adherence to ARV therapy in older patients, compared to younger individuals, has been shown in a previous meta-analysis. 22 Younger patients who have only had experience with modern, simple ARV medication regimens may not exhibit the same attention to adherence.
The reduction in HIV VL associated with the use of a HSSP shown in our study may have implications on health care costs. Higher rates of VL suppression could result in less unplanned inpatient hospitalization and outpatient clinic utilization, which could reduce the total cost of care to the health system and managed care organizations. Previous studies have demonstrated lower monthly health care costs for patients using HSSPs compared to non-HSSP patients; however such studies have not been conducted specifically for patients with HIV.10,11 Establishment of a HSSP is a significant undertaking and investment for a health system, requiring physical infrastructure for prescription dispensing, a call center for patient management, and qualified clinical and technical staff. Other challenges to both the creation and maintenance of a HSSP include payer network lock-outs, restricted access to limited distribution drug networks, lowered payer reimbursements, specialty pharmacy accreditation requirements, and staff recruitment and retention. 7 Even if patients wish to utilize a HSSP, insurance benefits may mandate the use of a payer-owned specialty pharmacy, preventing access to this model. Although providing the necessary infrastructure and clinical services to support a HSSP model poses financial challenges to health systems, doing so could provide a return on financial investment if the model ultimately reduces the total cost of patient care. Future studies should be performed to investigate the financial impact of a HSSP model for care of patients with HIV.
Limitations
This study investigated VL suppression among patients from an HIV clinic at a single academic medical center using the HSSP associated with that institution. Therefore, the findings may not be generalizable to other geographical areas. In addition, while we adjusted for several potential confounders including race, ethnicity, and CCI, we did not consider other socioeconomic variables like income, insurance type, and literacy levels. These confounders are factors that could potentially impact the patient’s choice of pharmacy.
The study was hindered by inconsistent documentation of the original date of HIV diagnosis and the start date of ARV therapy. Consequently, treatment duration for treatment-experienced patients could not be reliably determined. Analysis of the data revealed that most patients were already receiving ARV therapy at the time of assessment, potentially influencing VL suppression rates in both groups. Patients already on ARV therapy might achieve faster and more complete VL suppression compared with treatment-naïve individuals and may not benefit as greatly from the additional HSSP support during initiation of therapy. Across both groups, VL suppression rates were notably high, possibly due to effective management of patients established on ARV therapy.
Future studies aiming to evaluate different specialty pharmacy models’ impact on HIV clinical outcomes should carefully account for date of patient diagnosis dates, ARV initiation dates, and treatment durations. Additionally, VL results from external laboratories not integrated into the academic medical center’s EMR may have been missing. This study focused solely on the number of VL tests conducted, without considering the timing of these tests in relation to prescription fills, dose adjustments, or clinic visits. Some tests could have been performed too soon after medication changes, potentially not accurately reflecting the impact of the ARV medication.
Finally, due to the intrinsic nature of patient pharmacy switching mandated by insurance, the determination of the primary pharmacy was challenging. During the study period, patients may have switched between both HSSP and non-HSSP pharmacies and filled at both locations. As a result, the impact of each type of specialty pharmacy on VL suppression for patients filling at more than one location is difficult to isolate.
Conclusions
Patients with HIV utilizing a HSSP model for filling their ARV medications showed higher rates of VL suppression compared with those who filled their medications at non-integrated specialty pharmacies. Establishing integrated specialty pharmacy services within health systems is challenging, but expanding this model to other health systems and to the HIV population could improve clinical outcomes. Evaluating the impact of integrated health system specialty pharmacies on total medical expenditures for Patients with HIV could support the model’s growth and warrants further investigation.
Supplemental Material
Supplemental Material - Greater HIV Viral Load Suppression in Patients Using an Integrated Health System Specialty Pharmacy
Supplemental Material for Greater HIV Viral Load Suppression in Patients Using an Integrated Health System Specialty Pharmacy by Karen Salomon-Escoto, Martha Stutsky, George Reed, Monica Y. Hinestroza Jordan, Jonathan Kay, Mireya Wessolossky in Journal of Pharmacy Practice
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Wessolossky reported receiving a consultation fee from Gilead. No other disclosures were reported.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.