
Abstract
Introduction
Polypharmacy in older adults is common, with almost 20% of older adults over age 65 taking ten or more medications.1,2 Use of multiple medications by older adults is associated with a lower adherence rate to medication regimens and increased use of inappropriate medications.3,4 Taking multiple medications also increases the potential for interactions between medications. 5 Prior studies have examined the association between polypharmacy and adverse effects including geriatric syndromes (eg, cognitive change and multiple falls), as well as adverse drug reactions, all of which have the potential to cause injuries and other deleterious health impacts, leading to emergency room visits, hospitalizations, and death.6-10 Efforts to reduce polypharmacy in older adults may yield clinical benefits and improve patient safety. 11
Deprescribing is a planned process of medication review intended to reduce doses or stop medications that may be causing harm or may no longer be of benefit. 12 Approaches to deprescribing have improved use of medications by eliminating those which may be no longer indicated and reducing the use of potentially inappropriate medications that are likely to cause more harm than benefit in older adults.13-16 These approaches consider the risks and benefits of each medication as a potential target for deprescribing, both individually and in combination with other medications, as well as in the context of the patient’s clinical conditions. Because of these factors, deprescribing interventions in clinical studies are inherently complex and often do not reflect real world clinical practice. Given the burden of polypharmacy in the older adult population and its subsequent risks, research investigating enhanced implementation of deprescribing into clinical practice and across health care settings is warranted. 17
The VIONE (Vital, Important, Optional, Not indicated, and Every medication has an indication) deprescribing methodology was developed in 2016 as a straight-forward, reproducible electronic system that is end-user friendly and provides real-time data on deprescribing with rich granularity. Six years of experience data with the VIONE implementation, modernization, medical informatics utilization, sustainability and expansion illustrate many positive outcomes and promising potential avenues to further invest in and expand VIONE’s scope and scalability. 18 The VIONE methodology demonstrates success in facilitating providers to tailor medication use and reduce medication burden, thereby reducing potential drug interactions and clinical waste, and ultimately improving patient safety. 13 VIONE spread to over 130 VA (Veterans Administration) Medical Centers across the US, demonstrating its ability to be adopted in real-world clinical settings. The VIONE program incorporates Veteran, primary care and pharmacist perspectives and utilizes consultative and educational approaches and virtual coaching collaborative models to provide integrated tools for decision support to tailor medication prescribing. 19 Established in 2016, VIONE builds on recommendations published in Beer’s Criteria and STOPP/START.20,21 While Beer’s and STOPP/START primarily focus on the use of potentially inappropriate medications in the elderly population, VIONE takes a broader approach. It is not restricted to addressing polypharmacy and addresses both recommendations to optimize the medication list, as well as to deprescribing of potentially inappropriate medications. Furthermore, VIONE can easily be applied in any clinical setting and medication list.
VIONE has been disseminated through diverse platforms and networking connections including a VIONE toolkit (Implementation Guide), educational materials such as webinars and brochures, and interactive dashboards that report deprescribing activities documented through VIONE. 19 The rapid dissemination of VIONE, the variety of methods of dissemination, and the contextual differences in facilities may have contributed to differences in how and where VIONE was implemented at each facility.
Further evidence is needed on deprescribing interventions that are implemented on a large scale across multiple settings and adapted to local conditions. This need includes evidence for interventions like VIONE, with components of medical informatics enhancement and decision support tools embedded within the Electronic Health Record (EHR). These tools provide clinicians with prompt and specific feedback, as well as population health management insights, to identify and prioritize patients at risk for adverse events due to polypharmacy.18,22-24 In this report, we describe the experience of 3 sites that have implemented VIONE. We aim to describe how each site has adapted the VIONE approach and tools to be used at their respective sites, while maintaining fidelity to the core VIONE methodology.
VIONE Methodology
VIONE methodology for deprescribing has been described elsewhere.13,18 Briefly, VIONE is an acronym for categorizing medications that a Veteran is taking as Vital, Important, Optional, Not indicated, and Every medication has an indication according to its importance to the Veteran’s clinical status and goals of care. Medications classified as Not Indicated or Optional are designated as targets for discontinuation, in order to tailor medication use, avoid interactions and reduce medication burden. The VIONE program originated at the Little Rock VA Medical Center and has been disseminated across the nation by the VIONE team in partnership with the Diffusion of Excellence (DOE) Ecosystem, and leverages group coaching through the VIONE Academy, academic detailing, development of site-level dashboards, and dissemination of tools such as clinical applications enhancements. Local adoption of VIONE is led by a local champion, often a pharmacist and/or a physician. A VIONE Computerized Patient Record System (CPRS) patch that includes the VIONE Polypharmacy Reminder dialog template (clinical applications modification to provider order entry) is available to all VA facilities across the nation. A VIONE deprescribing note template can be completed in CPRS and a menu of deprescribing order reasons (including the VIONE reasons) are also available to document VIONE interventions. These tools are disseminated across sites to encourage implementation fidelity to the VIONE program and to provide trackable data that is culled from CPRS and reported nationwide via a dashboard with daily automation capability and data integrity. This dashboard is automatically updated daily and provides end user-friendly updates, with information such as unique Veterans, location, medication, cost, name of provider/pharmacist, cost avoidance and number of deprescribed medications. These data dashboards provide daily feedback to local VIONE teams and stakeholders to demonstrate in real-time VIONE’s progress and contributions to improve quality of care and patient safety.
For the purposes of local population health management, a risk score and corresponding risk dashboard were developed. The risk score accounts for number of active medications, age, 2 or more emergency department visits in 1 year, multiple documented falls in 1 year Care Assessment Need (CAN) score (a risk score that is associated with subsequent hospitalization and mortality using already collected clinical and administrative data) greater than or equal to 90.25,26 Each criterion is worth 1 point and a summation of points represents the VIONE risk score. 13 The score is used as a clinical tool for local teams to identify Veterans to be targeted for deprescribing.
A multipronged approach engaging various hierarchal levels, opinion leaders, stakeholders, and multidisciplinary key players at local, regional, national and international levels supports ongoing dissemination efforts. Several formats of VIONE educational materials including vignettes, patient and provider brochures, VA-TED talks, webinars with PowerPoint presentation, and VIONE toolkits containing reminder dialog templates, were disseminated throughout Veterans Health Administration (VHA) using intranet resources and through the VHA Diffusion of Excellence (DOE) office. With oversight and supportive guidance from the DOE, VIONE academy was launched, and local sites interested in VIONE implementation were invited to apply and compete in a selection process. Motivated local champions who showed promise as effective change agents were recruited to participate in virtual coaching collaborations. The VIONE Academy offers coaching by the VIONE team to local champions on VIONE implementation strategies, followed by open office hours to allow participants to ask questions on implementation specific to their local site. The VIONE Academy disseminated additional materials
The 5 core components to adoption of VIONE are support from leadership, technical readiness, identifying clinical champions, developing an education plan, and identifying a plan to monitor and sustain VIONE. These components can be applied to varying clinical practice areas, all of which do not require the hiring of new personnel, as they can be merged with pre-existing workflows (Figure 1). Sites implementing VIONE are provided with a VIONE Implementation Guide (VIONE Toolkit). The toolkit contains instructions for meeting the technical requirements, which include installation of VIONE Discontinuation Order Reasons, and the VIONE Polypharmacy Template, which both facilitate retrospective tracking of VIONE documented interventions. Provider education and training are also included in the VIONE Implementation Guide and are completed prior to VIONE implementation. The toolkit recommends identification of VIONE Champions (MD, PharmD, Nurse) who will lead the implementation efforts in a certain clinical practice area, and work as change agents across their facility for future implementation efforts. In addition, the VIONE champions develop goals for implementation, track implementation progress using VIONE dashboards, and develop strategies for sustainment. Key Components to Implementing VIONE (Veterans Health Administration, VIONE Implementation Guide. June 11, 2024)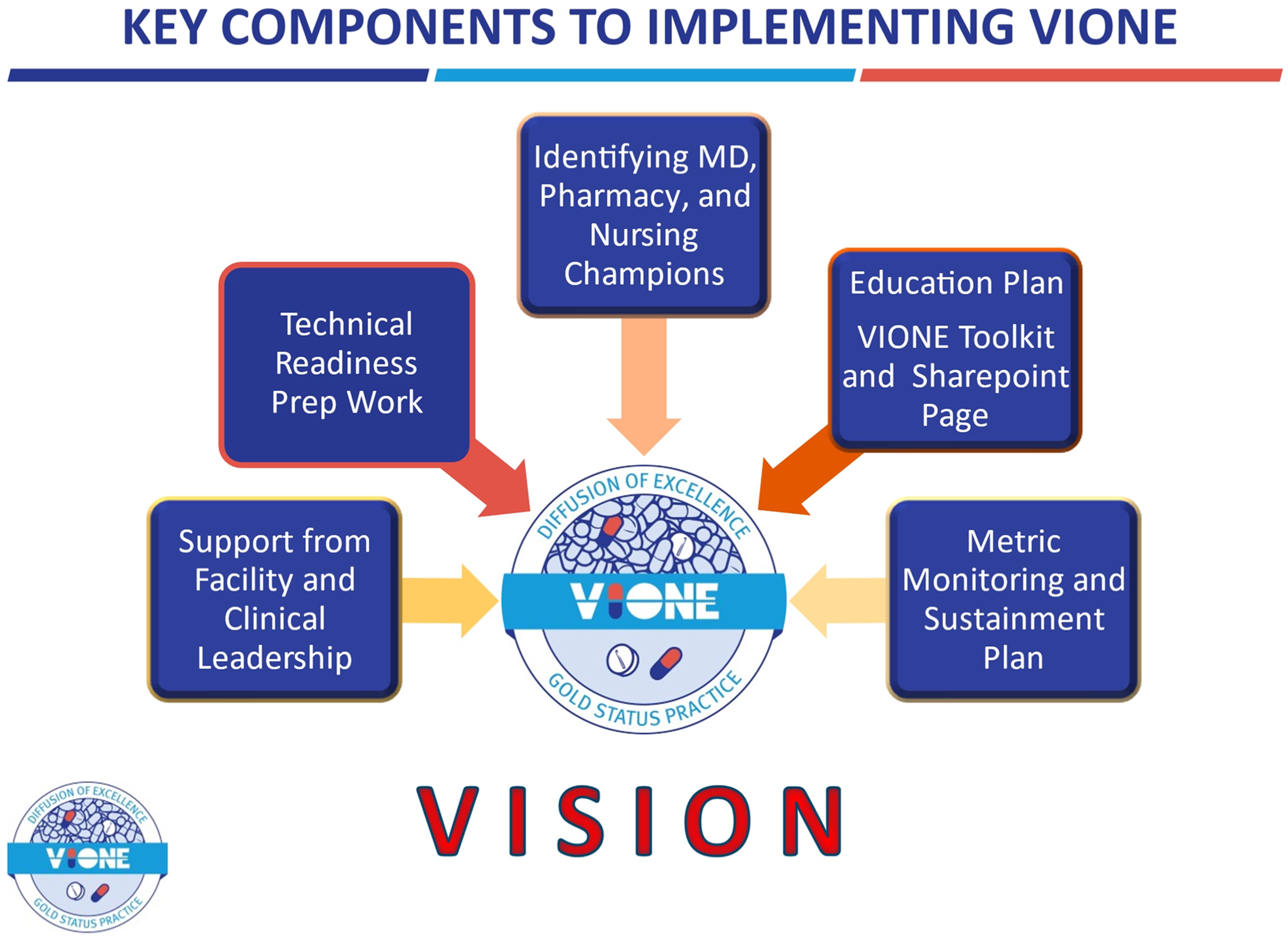
Methods
Here we report experience from 3 sites’ adoption of the VIONE program. These sites reported their experience through presentations at the American Society of Health-System Pharmacist National Conference in 2020. We invited all site teams with abstract presentations pertaining to VIONE to participate in recounting their experience of implementing VIONE (a total of 8 sites) and teams from 3 sites agreed to participate. Sites were asked to describe their implementation in detail, including how they had implemented VIONE at their site, who was involved in implementation, what tools were used, the setting of the VIONE polypharmacy review, what outcomes were tracked, whether barriers were encountered during implementation, and what facilitators were identified by their team during and after their implementation and sustainment. Each site was given the leeway to report the processes and outcomes it deemed salient to its individual implementation. As a VHA system-wide quality improvement effort, each site received determination of research exemption and approval for data collection.
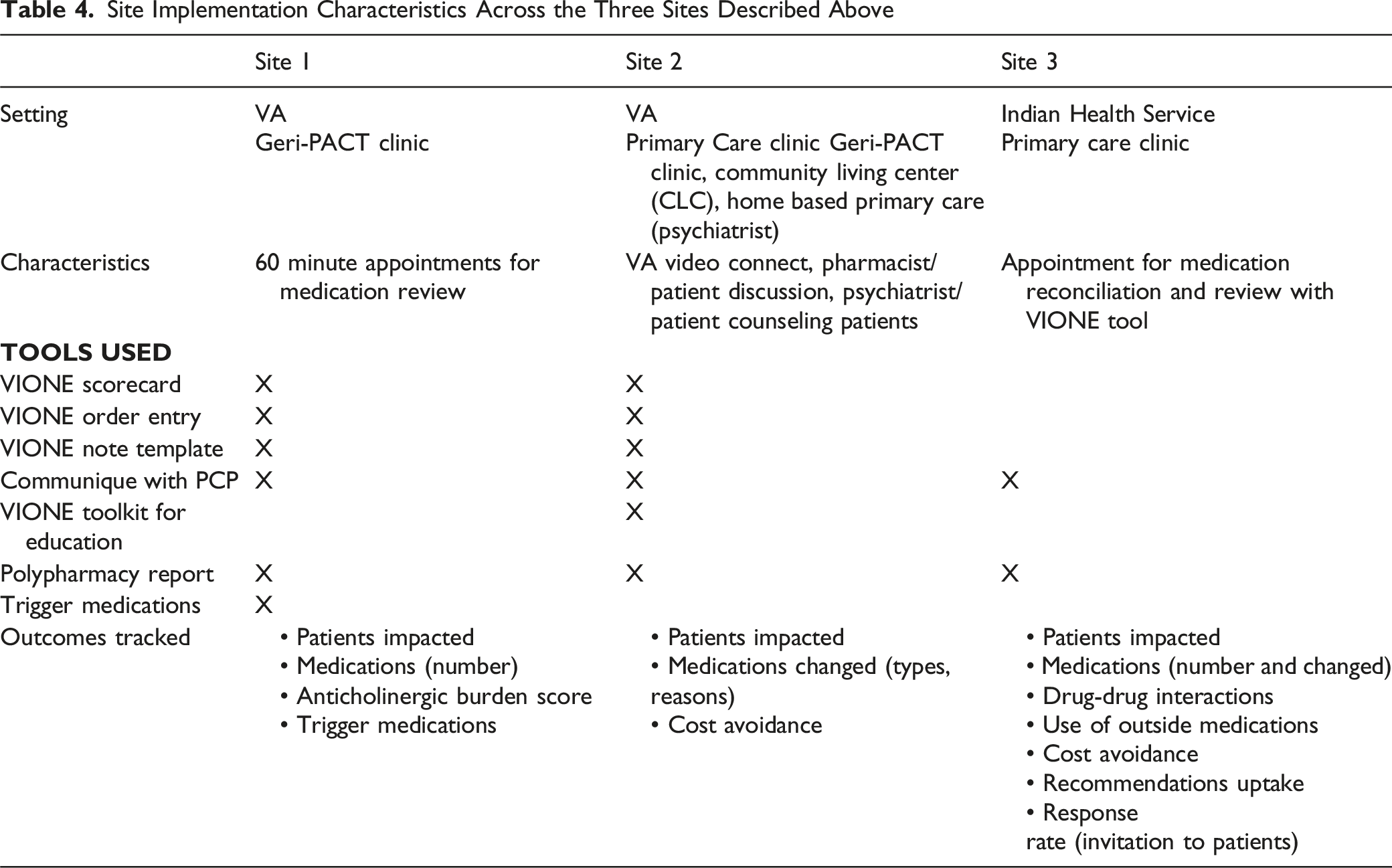
Local VIONE teams described how their VIONE program is conducted, including how they identify patients for medication review and deprescribing, how they conduct medication review, how they implement deprescribing and what outcomes they track. Sites also report on the challenges that they have identified and overcome, and adaptations to suit their site’s needs. Sites report on what tools they have used and what additional methods they considered beyond VIONE. Characteristics of VIONE implementation at each site are summarized, including setting where VIONE is implemented, how VIONE is implemented, what tools were used, and what outcomes were tracked for each VIONE implementation. Sites tracked multiple types of outcomes, including those directly related to medication changes (eg, number of total medications, types of medications changed, and reasons medications were changed, number of trigger medications, use of outside medications), identification of high-risk scenarios (eg, anticholinergic burden, drug-drug interactions), reach of the intervention (eg, number of patients impacted, extent of recommendation uptake, patient responsiveness to invitation to participate), and cost avoidance. The following case reports describe the similarity and variation in the initial implementation and adoption of VIONE at 3 sites.
Results
Site #1 Experience: VA Sierra Nevada Health Care System
Implementation
The implementation of VIONE at the VA Sierra Nevada Health Care System started in late 2019, as part of a project by a second-year geriatrics resident. VIONE appointments were integrated within the pre-existing Geriatric Patient Aligned Care Team (Geri-PACT) clinic, with support from leadership to allow 60-minute appointments during which to complete the VIONE review.
Tools and Setting
Patients were identified using the VIONE risk score dashboard, with priority given to patients under the care of a geriatrician and with higher risk scores. A chart review was performed of these patients’ medication records to identify potential opportunities to deprescribe, as well as patient to screen for use of pre-specified trigger medications including aspirin, proton pump inhibitors, sulfonylureas, HMG-CoA reductase inhibitors (statins), and highly anticholinergic medications. After chart review, patients were scheduled for a VIONE appointment with the geriatric clinical pharmacist and/or the geriatrics resident. During the appointment, the clinician used the VIONE mnemonic within the national VIONE note template to modify drug regimens and send recommendations to the primary care provider. VIONE interventions were tracked throughout the process.
Outcomes
Presents Information on Prescription Medications for a 15-Patient Pilot of VIONE at the VA Sierra Nevada Health Care System
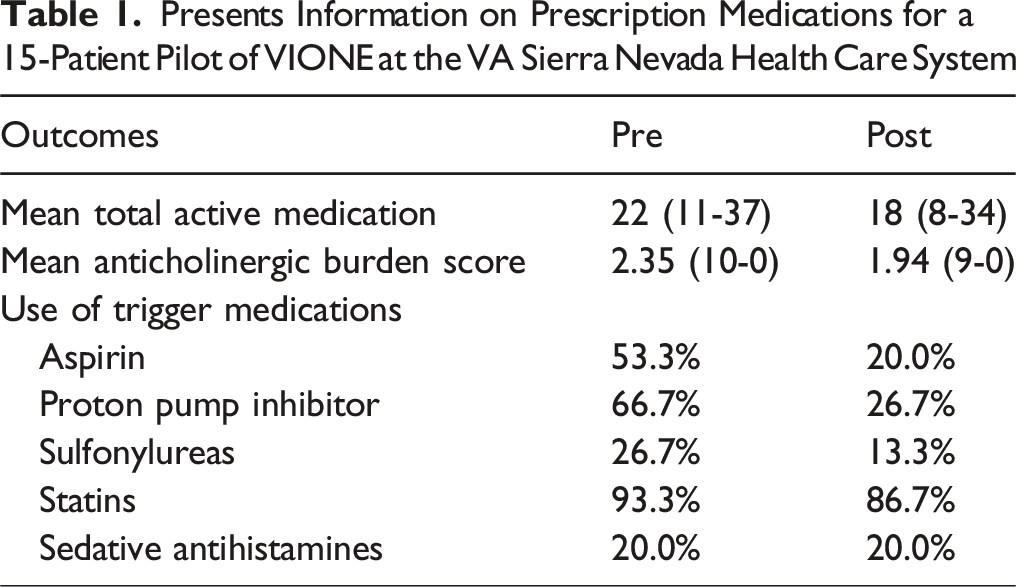
While VIONE clinic visits were found to be beneficial to patients, several barriers were identified, which played a role in limiting the number of completed deprescribing clinic visits. First, there was a low correlation between the polypharmacy risk score and the potential for interventions. Second, time spent on chart review prior to scheduling pharmacy clinic appointments added to pharmacists’ workload. While time required for dashboard identification and chart review was not tracked, it was retrospectively estimated to range from 30-40 minutes. Additional time requirements were 60 minutes spent face-to-face with patients and 20-30 minutes on documentation. Finally, visits were limited by the availability of the clinical pharmacist, by existing clinic appointments, and by COVID-19 restrictions on face-to-face visits.
To address these barriers and expand outreach, providers and other clinical pharmacists were educated on the VIONE risk scorecard and deprescribing tool to enable all primary care patients undergo review for polypharmacy and medication interventions as part of routine clinic appointments. Additionally, to conserve pharmacist time, patients were scheduled for VIONE clinic visits using only the scorecard without prescreening for trigger drugs. Finally, appointments were completed via telephone or video call.
Site #2 Experience: VA Caribbean Healthcare System (VACHS)
Implementation
VACHS identified polypharmacy as an area for improvement. After several other deprescribing strategies for polypharmacy evaluation were implemented but failed to be sustained in practice, VACHS adopted VIONE on June 5th, 2020, as the methodology to reduce polypharmacy and to improve patients’ safety and adherence to medication therapy.
Tools and Setting
In June 2020, a total of 11 226 patients with more than 15 medications were identified. VIONE was presented to primary care staff in the main facility, Community-Based Outpatient Clinics (CBOCs), Home Based Primary Care (HBPC) programs, and Community Care Living Centers (CLCs) using a PowerPoint presentation obtained from the Pharmacy Benefits Management (PBM) Academic Detailing Campaign VIONE/Polypharmacy resources. At the beginning of implementation, 7 Clinical Pharmacy Practitioners (CPPs) (1 in Geri-PACT, 5 in Primary Care, and 2 from HBPC), in addition to 1 HPBC psychiatrist, were involved in reviewing the VIONE Dashboard for patients with more than 15 medications enrolled in their PACT team patient panel or in the HBPC.
All PACT CPPs who had been assigned to 1 day of prescriptions processing reviews were instructed to perform VIONE reviews instead. On that day, the CPP reviewed the VIONE dashboard for patients with VIONE risk scores of 4 and 5 and attempted to contact the patient using VA Video Connect (VVC) as the first modality, and telephone appointment as the second modality. The “VIONE Polypharmacy Review Note” was used to document interventions and to capture health factors associated with polypharmacy. The CPP added the primary provider as cosigner on documentation when the pharmacy provider considered deprescription of medications to be necessary. Any patient seen by a CPP underwent medication therapy evaluation using the VIONE mnemonic to deprescribe medications considered potentially inappropriate for that patient.
In HBPC, the consultant psychiatrist and the CPP began using VIONE as soon as the patient was admitted to the program. New patients were referred to the psychiatrist, who evaluated the patient’s pharmacotherapy regimen, including psychotropics, benzodiazepines, and all other medications for deprescribing opportunities using the VIONE mnemonic. In addition, duplicate drug class, drug-drug, and drug-disease interactions were evaluated by the psychiatrist and the CPP. The course of therapy with antipsychotics for the treatment of behavioral disturbances for patients with dementia was tracked to identify attempts to discontinue them. The HBPC CPP also used VIONE methodology during quarterly medication reviews and interdisciplinary meetings.
In the HBPC program, a face-to-face visit was coordinated with the patient with or without a caregiver for a psychiatric diagnostic evaluation. The patient and caregiver were interviewed separately to identify the patient’s active behavioral symptoms and their frequency, patterns, and intensity, and how these symptoms influenced the patient’s safety (falls, self-harm behavior, harm to others, or the property) and psychological distress. Besides pharmacological interventions, nonpharmacological strategies were discussed with the patient and/or caregiver. The consultant psychiatrist identified what pharmacotherapeutic factors were most important to the patient and/or caregiver; in some cases, the caregivers wanted to decrease pharmacotherapy, while others questioned the clinical implications in continuing some medications (eg, cholinesterase inhibitors). This intervention provided an opportunity for deprescribing as well as time for the clinician to provide education on the medication regimen, and to strengthen caregiver support and education.
For the consultant psychiatrist, deprescription began with psychotropics for which the risk of harm is greater than the benefit, due to observed side effects, interactions with other medications, and need for frequent monitoring. Tapering psychotropics was individualized and started by gradually reducing the dose slowly over an extended period, focusing on 1 medication at a time to avoid confusion of symptoms that could appear during this process. Also, the consultant psychiatrist was available by telephone for consultation on weekdays to address unexpected clinical issues and to provide continuous support to the patient and/or caregiver. Face-to-face visits were scheduled every 4-8 weeks, adjusted according to which psychotropics were under evaluation. Visiting nurses reviewed medication lists during their monthly visit and answered patient and/or caregiver questions or referred questions to the consulting psychiatrist.
In this setting, VIONE was able to be implemented with the assistance of the VIONE Toolkit and initial VIONE education. The use of VA Video Connect, which provided video visits to patients’ homes, was advantageous for performing VIONE polypharmacy reviews, especially during the COVID-19 pandemic. During the video call, patients were able to show their medication bottles to the CPP, while caregivers were available to support the most vulnerable patients in need of assistance. This modality was continued by PACT CPPs even after the initial months of the pandemic, augmented by face-to-face and telephone interventions for patients contacted for a comprehensive evaluation for identification and discontinuation of unnecessary, ineffective, and inappropriate medications.
Outcomes
Implementation Outcomes at the VA Caribbean Healthcare System (VACHS)

Site #3: Woodrow Wilson Keeble Memorial Health Care Center (WWKMHCC), Indian Health Service Indian Health Service
Implementation, Tools and Setting
To implement VIONE at the WWKMHCC, a report was run through the Resource and Patient Management System (RPMS) to identify patients with more than 5 active medications listed. Subsequently, the report was run to identify the number of patients with more than fifteen active medications to narrow the patient sample to include patients at highest risk of complications due to polypharmacy. Once these patients were identified, VIONE served as a tool to facilitate conversations about deprescribing, helped the pharmacist arrange a patient’s medication list prior to his or her appointment, provided ideas for deprescribing and assisted in determining any necessary laboratory tests the patient needed based on active medications and disease states. The pharmacist conducted a full medication reconciliation using the VIONE tool, creating an updated medication list and discussing findings with the patient. Throughout these medication reconciliations, patients were able to ask questions about their medications and clarify their specific medication regimens. Patients left their appointments with an up-to-date medication list and additional information about their medications. During the medication reconciliation, the patients’ over-the-counter medications, herbal products, teas, and roots were documented in the clinical note and added to their medication list as outside medications, allowing for drug interactions to be identified when new medications were prescribed. The pharmacist followed up with the patient after the encounter to ensure the patient received any recommended follow up care or to address any questions or concerns.
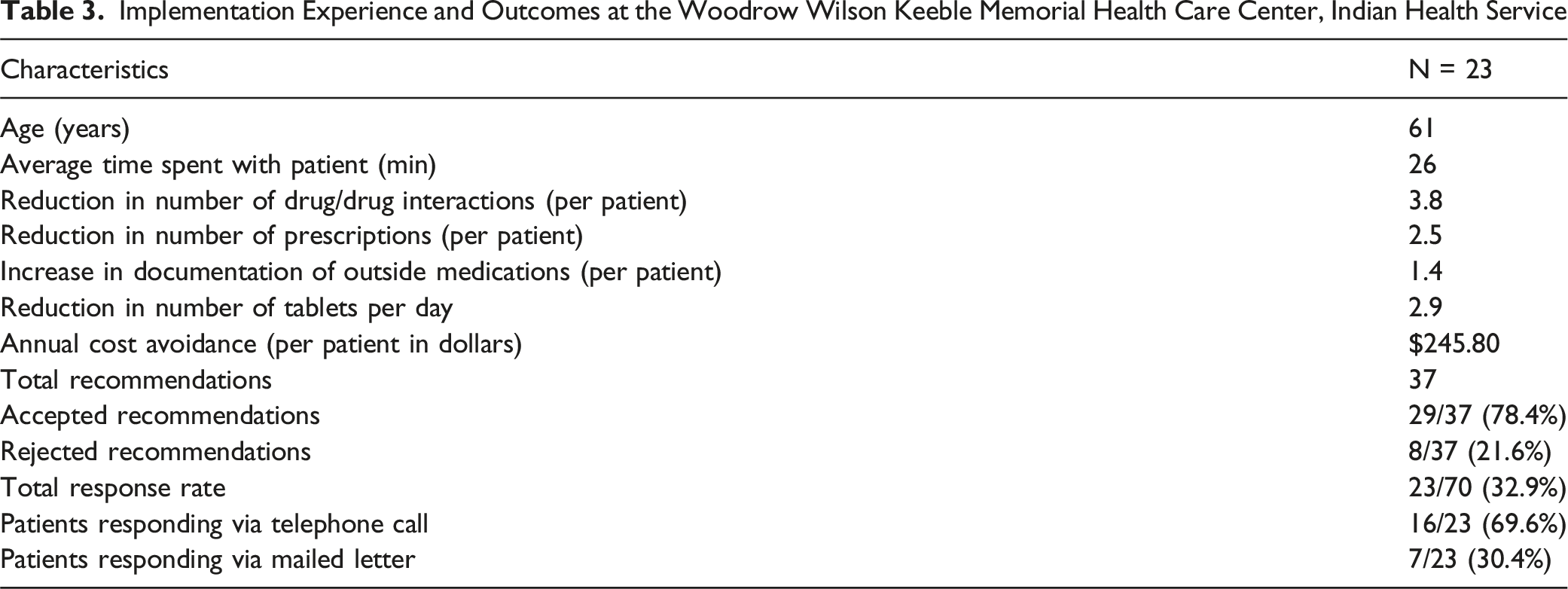
Specifically for the WWKMHCC, it was found to be ideal to meet with the patient prior to a primary care appointment to complete the medication reconciliation utilizing the VIONE tool. This process allowed for subsequent patient and provider involvement and action to assess the recommendations from the pharmacist during the appointment. To track outcomes of the program, the number of changes in total medications, drug-drug interactions, annual cost avoidance, and all other calculations were manually determined and tracked for each patient of the total sample of 70 patients. Because this site did not have access to some of the dashboard tools, tracking was performed by residents as part of a residency project. This site would have benefitted from a tool that tracked these outcomes automatically, as well as 1 that flagged patients that have more than fifteen active medications in order to signal he provider to consider using the VIONE tool assist in decreasing polypharmacy.
Outcomes
Implementation Experience and Outcomes at the Woodrow Wilson Keeble Memorial Health Care Center, Indian Health Service
Summary
Site Implementation Characteristics Across the Three Sites Described Above
Discussion
Although polypharmacy among older adults is prevalent, the lack of standardized approaches for medication review and deprescribing limits opportunities for improving medication use and prevent potentially preventable adverse outcomes related to polypharmacy. VIONE provides a simple and pragmatic approach to help clinicians conduct medication reviews and consider targets for deprescribing. Implementation experience from 3 sites that have adopted VIONE deprescribing methodology demonstrated that VIONE was able to be successfully implemented in each of the sites, which resulted in improved impact on medication prescribing and use in older adults. Although site implementation varied by clinical setting, team composition, tools utilized and metrics impacted, site teams were able to utilize clinical tools and approaches to target older adults with polypharmacy to yield improvements in medication use, thereby improving safety while reducing costs. While the VIONE toolkit and dashboards offer a means to track a host of measurable outcomes, sites were able to tailor their tracking based on the individual needs. Clinical settings where VIONE is implemented include primary care clinics, geriatric clinics delivering care similar to a patient centered medical home, home based care and community living centers or nursing homes. Several tools that the VIONE project has developed nationally have been adopted in these sites, including tools for patient identification, clinician decision support tools such as order entry and a medication review template, and a dashboard for tracking implementation and project outcomes. 18 A plethora of implementation resources (such as note templates, patient vignettes, and webinars) and customized clinical decision tools (such as site-specific patient risk dashboards and PIMs dashboards) provided site teams with a choice of tools to be used and adapted for their site’s implementation based on the site’s structure, characteristics, staff, and patients, while maintaining fidelity to the VIONE methodology. Of note, each site had driven early adopters, who demonstrated leadership and commitment to collaboration with the core VIONE teams on an ongoing basis. These leaders included trainees creating educational opportunities in polypharmacy, deprescribing, and quality improvement.
Other deprescribing approaches that have been tested in more rigid experimental conditions have yielded improvements in medication use,14,16,27 yet wide dissemination of these approaches have limitations because of complexity and perhaps limited flexibility to adapt to in real world practice. 17 VIONE uses a simple, easily teachable mnemonic that offers a structured approach to critical review of medications and their use, which may have been advantageous for flexibility in adoption at sites around the country. 28 The use of the VIONE methodology, VIONE documentation tools in the EHR, and VIONE population health management tools provide additional opportunities for sites adopting the approach to further enhance and adapt these tools to fit their needs. Sites have adapted the approach and tools to incorporate the use of indices (eg, the frailty index) for targeting patients, and they have incorporated an adherence questionnaire, and medication anticholinergic burden tool into documentation tools as they have implemented VIONE. These approaches have the potential to create a feedback loop which could inform changes to VIONE tools disseminated to future sites. The effect of adopting a program like VIONE with a set toolkit and centralized support has the potential to transform practice across health care systems with elements that support the fidelity of its approach while offering adaptability for local enhancement. 18 As the VHA, the largest single payor health care system in the US, and the Indian Health System, a federal funded healthcare system that aspired to transform into High Reliability Organizations (HROs), programs such as VIONE offer a template of how care enhancement could be applied and disseminated widely across the systems.13,26 As this report is a snapshot of individual site implementation rather than examination of implementation across all facilities that adopted VIONE, we are limited in drawing conclusions as to what characteristics of implementation systematically is mapped to implementation outcomes; further examination should expand upon our current observations of site implementation. Nonetheless, we are able to observe in a variety of settings how VIONE was implemented, demonstrating similarities and differences in approach. There is inherent variability in the outcomes of each site; future work should compare outcomes across sites with similar implementation, with attention to other confounders and/or prescribing initiatives that may impact results. Additionally, the Indian Health Service did not have access to certain population health management tools, such as the Risk Score and the PIM Dashboard, which further limits comparisons across sites. Also, this report documents instances of the initial implementation of VIONE rather than maintenance of the intervention; further examination of how these implementations of VIONE are maintained after initial implementation and expansion would demonstrate sustainability and impact on older adults the program serves. Furthermore, future studies may be helpful to shed light on the association between participation in VIONE and avoidance of adverse health outcomes.
In conclusion, this description of implementation of VIONE medication deprescribing methodology by 3 sites has demonstrated how each site used the approach and tools offered by the VIONE program to adapt VIONE to their local sites. VIONE medication optimization and safe medication deprescribing methodology offers a results-driven, holistic, and evidence-based approach to improve quality of life and patient safety, especially in older population across various clinical settings and across the continuum of care. Its features can be adapted to end user experiences based on lessons learned during implementation experiences. More research is needed regarding the association between VIONE deprescribing and reduction in adverse drug events such as falls, emergency department visits, unnecessary hospitalizations and mortality. Further evaluation of VIONE implementation, scope expansion, and scalability strategies across sites may generate an understanding of what drives differences in implementation and links differences in implementation, customization, sustainability patterns specific to VIONE medication optimization and safe deprescribing methodology, and deprescribing practices in general.
Footnotes
Acknowledgments
(1) Madelyn Cartagena, PharmD, BCGP; HBPC CPP. (2) Dhilma L. Alicea, MD; Psychiatrist, HBPC. (3) Ingrid Belaza, PharmD; Clinical Pharmacy Practitioner. (4) Lori Braaten, Pharm. D., BCPS, BCACP, CDR, United States Public Health service.
Ethical Considerations
This work was approved by the Great Plains IHS IRB/Research and Publication Committee.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by U.S. Department of Veteran Affairs Health Systems Research Service (Grant 5I01HX002905).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The opinions expressed in this paper are those of the authors and do not necessarily reflect the views of the Indian Health Service. The opinions expressed in this paper are those of the authors and do not necessarily reflect the views of the VA.