
Abstract
Medications account for nearly two-thirds of all cases of syndrome of inappropriate antidiuretic hormone secretion (SIADH). Numerous psychotropics including antipsychotics have been associated with SIADH but it is difficult to show a causal relationship. We report a unique case where a patient developed hyponatremia and upon rechallenge with aripiprazole resulted in a second incidence. There is limited literature recognizing aripiprazole induced SIADH and especially any focused on medication rechallenge.
Introduction
Syndrome of inappropriate antidiuretic hormone secretion (SIADH) is a common cause of hyponatremia, which is defined as a serum sodium less than 135 mmol/L.1,2 Other laboratory features of SIADH include hypoosmolality (serum osmolality less than 280 mOsm/kg), and concentrated urine as demonstrated by urine osmolality above 100 mOsm/kg and urine sodium concentration above 40 mEq/L. 3 Medications may account for nearly two-thirds of SIADH cases, and a wide range of psychotropic drugs—such as selective serotonin reuptake inhibitors, antiepileptics, and antipsychotics—are known to contribute to its development.4-6
Aripiprazole is an atypical antipsychotic medication that is Food and Drug Administration (FDA) approved for the treatment of various psychiatric conditions. 7 There are limited documented cases of aripiprazole-induced SIADH and none that include medication rechallenges. We present a unique case where a patient developed SIADH and was rechallenged with aripiprazole resulting in a second incidence of hyponatremia, strengthening the causal relationship between aripiprazole and SIADH.8-12
Case Report
First Admission
A 65-year-old male with schizophrenia, heart failure with reduced ejection fraction, cocaine use disorder, and nicotine use disorder was transferred from an outside hospital after management of bilateral frostbite. Of note, his schizophrenia was previously stabilized on haloperidol decanoate, and his last injection was 42 days prior to admission.
First Admission Labs and Medication Administrations
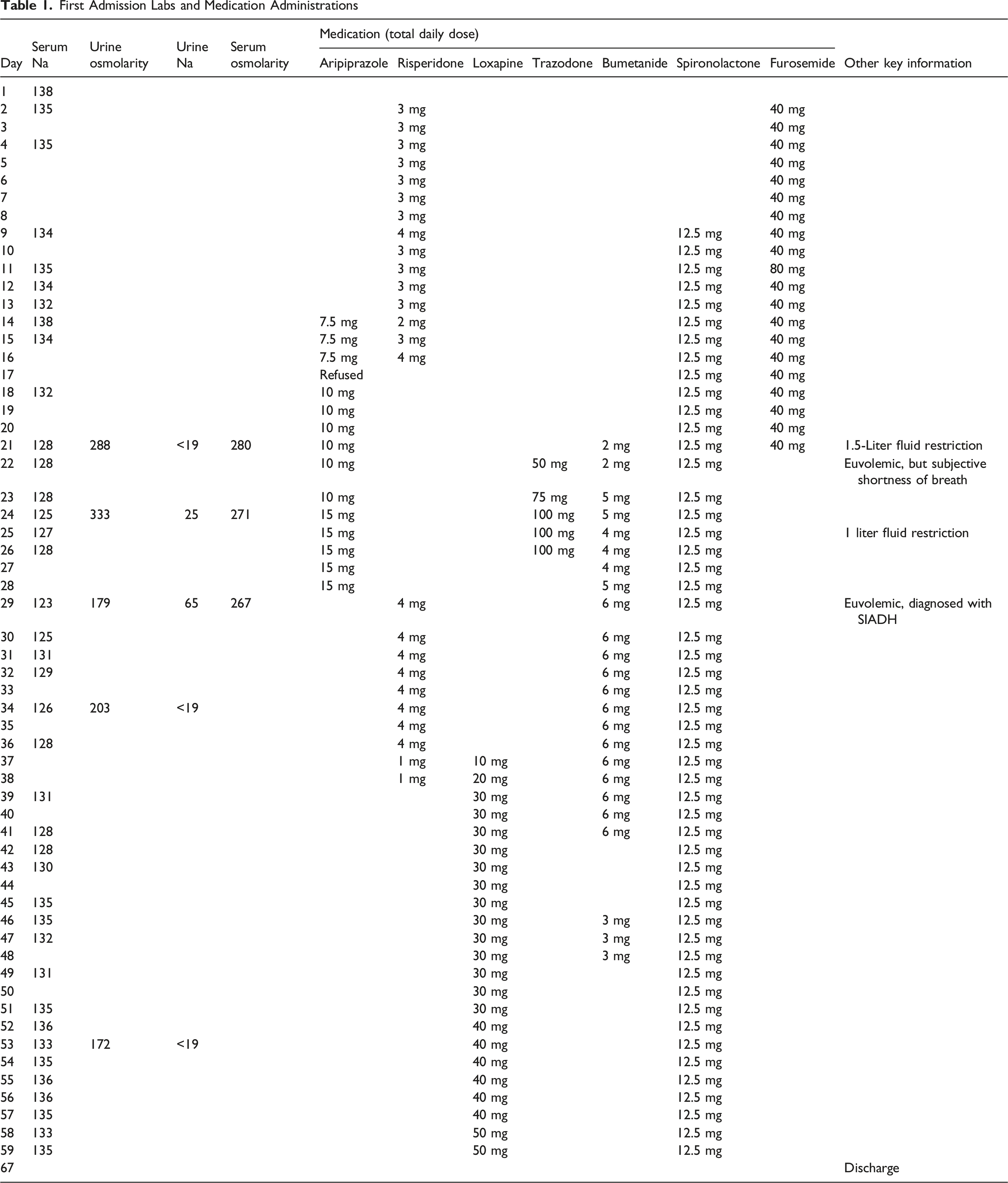
After aripiprazole discontinuation, serum sodium recovered to 125 mmol/L on day 30 and 131 mmol/L by day 31 without administration of hyponatremia treatments such as oral urea, tolvaptan, or sodium chloride tablets. . On day 34, serum sodium decreased to 126 mmol/L, but urine sodium had returned to <19 mmol/L. On day 36 loxapine was initiated and titrated to 50 mg by day 57. By day 43, the serum sodium had recovered to 130 mmol/L and was maintained between 130 and 137 until the patient was discharged on day 67 with loxapine 40 mg twice daily.
Second Admission
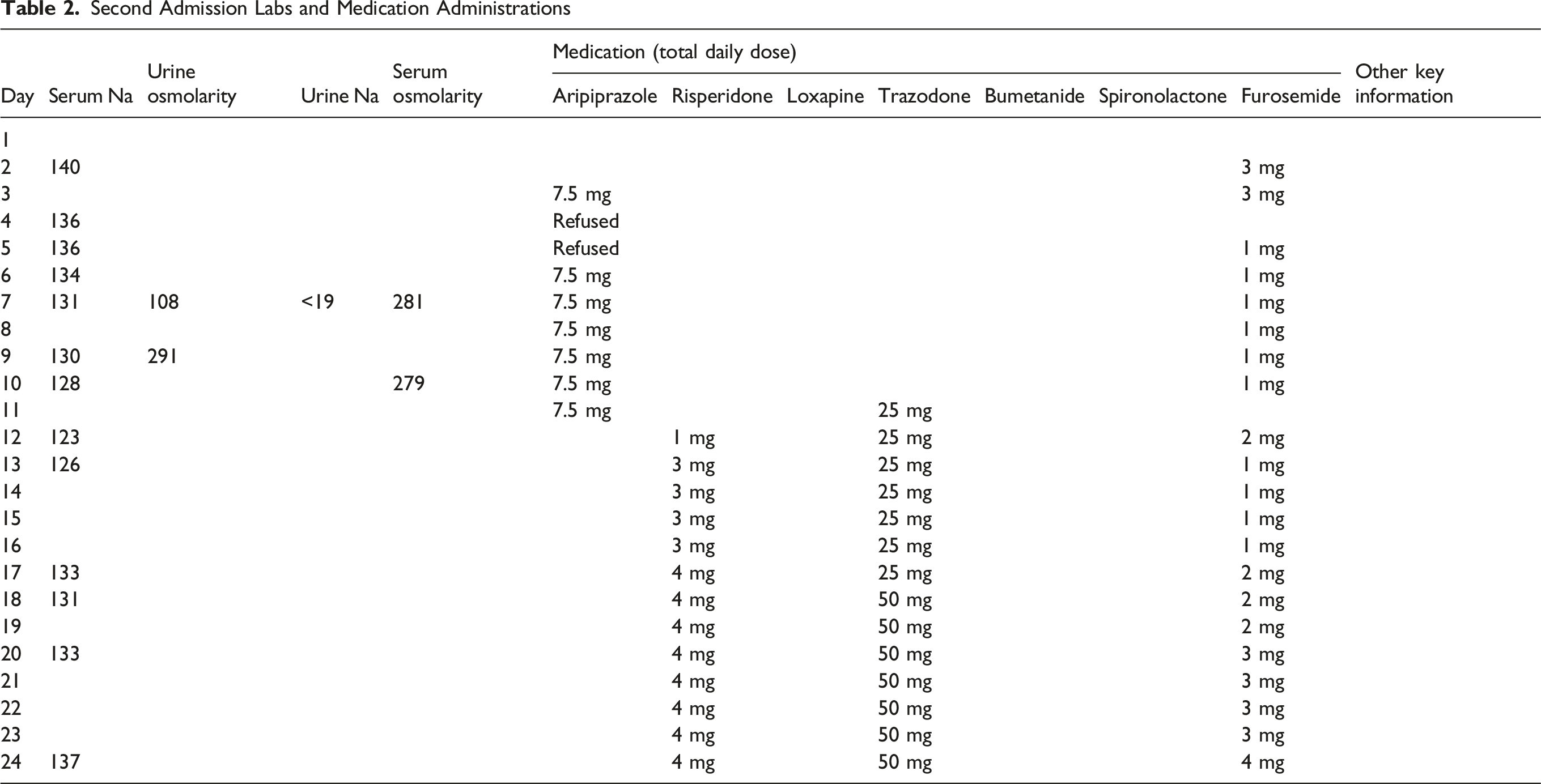
Second Admission Labs and Medication Administrations
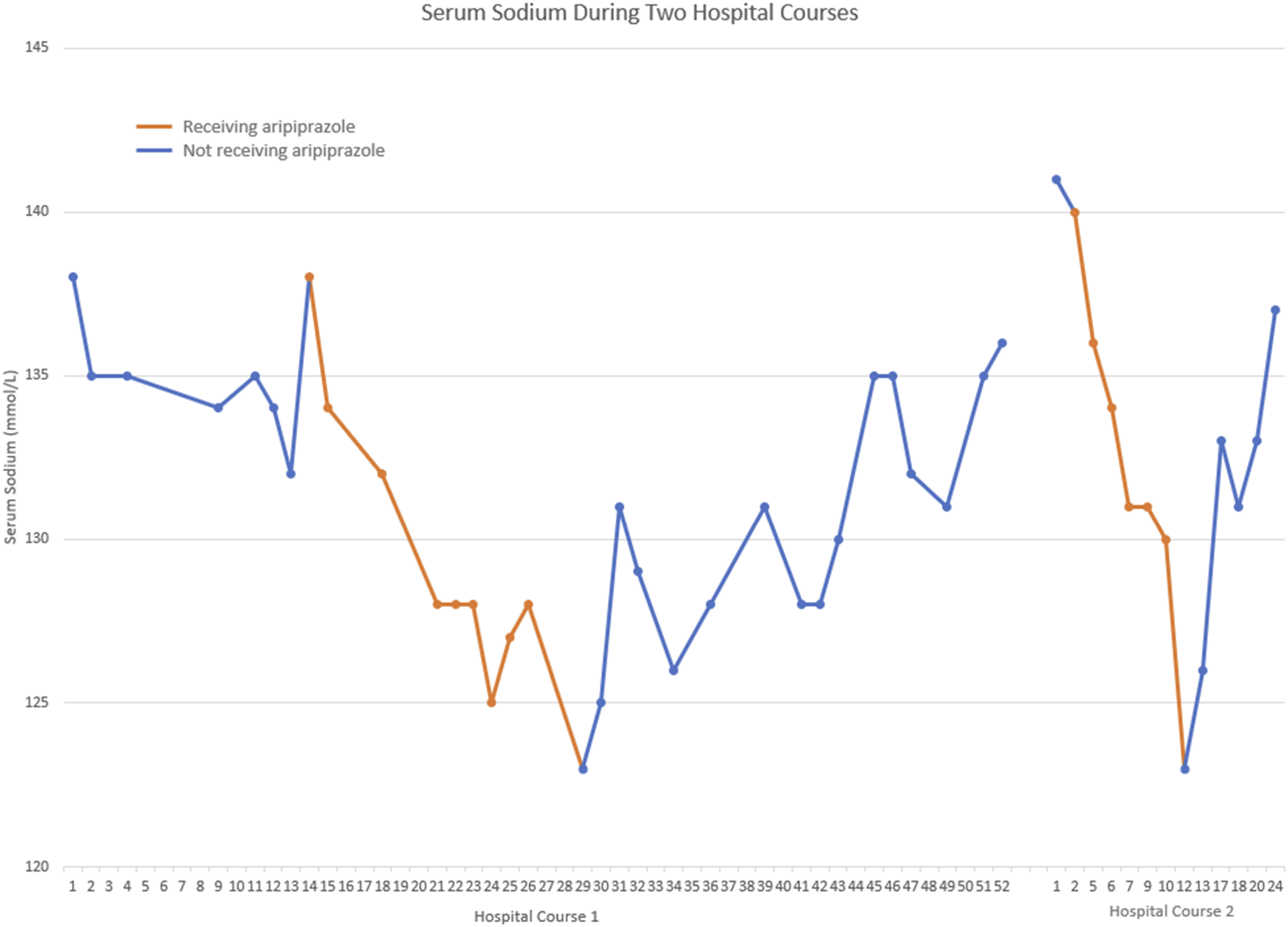
Serum Sodium Druing Two Hopsital Courses.
Discussion
Previous case reports have highlighted aripiprazole-mediated SIADH is more likely to occur during initial administration, rather than chronic use.8,9,13,14 This patient had been managed with various antipsychotics for many years without any episodes of SIADH. Prior to the initiation of aripiprazole, he was isotonic and euvolemic with a normal serum sodium. However, the patient experienced a pronounced episode of hyponatremia 7 days after introduction of aripiprazole, which began improving immediately after aripiprazole discontinuation and resolved 17 days later. He then experienced a second episode of hyponatremia 7 days after reintroduction of aripiprazole, which also began improving immediately after aripiprazole discontinuation and resolved 13 days later.
This patient has a history of schizophrenia and HFrEF both of which can result in hyponatremia from psychogenic polydipsia or predisposition to hypervolemic hyponatremia respectively. The authors ruled out these causes as the patient was on a fluid restriction with strict intake monitoring and there was a lack of significant urine dilution. Additionally, physical exam consistently noted euvolemia, and the hyponatremia did not respond to escalating diuresis.
SIADH was the most likely cause of this patient’s hyponatremia based upon lab values and patient presentation. Characteristic features of SIADH include a euvolemic hypotonic hyponatremia, with serum osmolarity <280 mOsm/kg and urine osmolality >100 mOsm. During the first episode of hyponatremia concern for excessive water intake was eliminated because serum osmolality steadily decreased as the hyponatremia worsened despite urine osmolality remaining above 100 mOsm/kg. Accordingly, the abrupt increase in urine sodium on hospital day 29 despite continued euvolemia was determined to be most consistent with SIADH. The patient received multiple other psychotropics during these admissions including risperidone, haloperidol, loxapine, and trazodone which have also been associated with the development of SIADH. However, the temporal relationship between drug exposure and the laboratory findings detailed above does not exist for these medications.
Aripiprazole was further determined to be the most likely cause of this patient’s SIADH based on a Naranjo Drug Reaction Probability Scale score of 9, indicating “definite adverse drug reaction”. 15 This score was derived from the following criteria: there are previous conclusive reports of this reaction (+1); the adverse event appeared after the suspected drug was administered (+2); the condition improved upon discontinuation of the drug (+1); the reaction reappeared when the drug was readministered (+2); no placebo was given to assess a recurrence of reaction (0); no alternative causes were identified that could have explained the reaction (+2); the presence of the drug in toxic concentrations in body fluids was not assessed (0); the reaction did not become more severe with increased dosage or less severe with decreased dosage (0); the patient did not have a similar reaction to the same or similar drugs in previous exposure (0); and the adverse event was confirmed by objective evidence (+1). Though not a commonly reported adverse reaction, there are multiple reports of aripiprazole induced SIADH as detailed previously. This report details a concrete temporal relationship between the exposure to aripiprazole and the onset of hyponatremia 7 days later, with resolution following discontinuation. The two extended admissions allow for an abundance of objective data including lab values, physical assessments, and documentation of fluid status which adds to the confidence of the relationship between aripiprazole and hyponatremia.
Conclusion
The repeated occurrence of SIADH upon rechallenge and resolution with discontinuation, strongly suggests that aripiprazole is the direct cause of SIADH despite possible confounders. There is limited guidance on rechallenging patients who have experienced antipsychotic-induced hyponatremia. This documented case demonstrates that hyponatremia may recur with rechallenge, which can guide risk assessment and influence prescribing practices in the future.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.