
Abstract
Introduction
Spinal and central nervous system (CNS) metastases are common in many solid tumors (ie, breast, prostate, lung) and can lead to spinal cord compression (SCC) secondary to extension of the epidural space. 1 Malignant SCC (MSCC) is often a chronic, progressive disease but acute manifestations can occur when vertebral body destruction leads to displaced bone fragments and acute SCC. MSCC most frequently presents in the thoracic spine (60%) and less frequently in the lumbosacral (25%) or cervical (15%) regions. 1 Survival in patients with MSCC is generally less than 6 months but retained ability to walk before treatment is associated with longer survival. 2
Standard treatment of MSCC consists of radiotherapy and surgical decompression, with adjunctive glucocorticoids playing a role in reducing inflammation and preserving neurologic function.3,4 Prompt initiation of therapy is essential, as delays can result in neurologic decline.1,5 Empiric treatment with oral (PO) dexamethasone is recommended, even prior to confirmation of diagnosis by magnetic resonance imaging (MRI).4,6,7 Dexamethasone can improve treatment outcomes by decreasing vasogenic edema through suppression of inflammatory cytokines which reduces capillary permeability and decreases spinal cord pressure to mitigate compression-related neurological injury. 4
Once patients have undergone surgery or initiated radiotherapy, tapering of dexamethasone is recommended. 4 The current evidence for glucocorticoid therapy remains limited to 3 small, randomized trials with varying dosing strategies and results.6-8 Historically, aggressive doses of dexamethasone (96-100 mg over 24 hours) were used to improve symptoms but were associated with high rates of severe side effects, including gastrointestinal perforation and bleeding, hyperglycemia, hypomania, pneumonia, and wound infection, which deterred its use.6-10 Thus, dexamethasone (16 mg/day PO) for 72 hours (day zero to 2) followed by a gradual taper over an additional 12 days has been shown to slow progression of neurologic symptoms, maintain or restore gait, and relieve pain while minimizing the risk of side effects compared to the previously studied aggressive dosing strategy.4,7 Given the lack of evidence to guide real-world use, clinical prescribing patterns are varied and often provider-specific with some preferring an early taper while others prefer prolonged use.
To date, there have been no studies evaluating the difference in cumulative dexamethasone dose patients receive based on taper strategy and associated outcomes. In this population, the optimal dosing, duration, route of administration, and tapering strategy remains unclear. Given the clinical variability in prescribing practices, total dexamethasone dose could be used to compare corticosteroid exposure, provide insight into real-world utilization, and highlight potential implications for safety and efficacy. This study aimed to address this gap by evaluating the use of dexamethasone in hospitalized patients with MSCC.
Methods
Study Design and Population
This study was an IRB-approved, retrospective, single-center review of adult patients hospitalized at an academic medical center from October 4, 2024, to June 30, 2025. Patients who received dexamethasone PO or intravenous (IV) for spinal cord or nerve root compression because of metastatic spinal disease, direct malignant infiltration, or secondary CNS metastases were included. The exclusion criteria included use for primary CNS malignancy, CNS vasogenic edema, or hypersensitivity to dexamethasone. Patients were grouped based on the duration of high-dose dexamethasone (16 mg/day) received: acute course (AC, ≤3 days) or prolonged course (PC, >3 days).
Study Outcomes and Definitions
The primary outcome was total dexamethasone dose compared between the treatment groups. This endpoint was chosen to capture the cumulative corticosteroid exposure, which is clinically relevant due to the known risks of high-dose corticosteroids. Comparing total dose between groups allows for evaluation of treatment intensity and potential differences in clinical practice patterns.
Secondary outcomes were time to initiation of steroid taper, time to intravenous-to-oral (IV-to-PO) conversion (hours), rates of hyperglycemia (blood glucose 180-219 mg/dL) and severe hyperglycemia (blood glucose ≥220 mg/dL), rate of new start insulin therapy during hospitalization and at discharge, hospital length of stay (LOS), provider documentation of improved symptoms (gait, pain), and inpatient mortality.
Statistical Analysis
Descriptive statistics were done using JASP statistical program (version 0.19.1). Frequencies were reported as the number of cases with the evaluated outcome divided by the total number of patients (n, %). Test of normality was used to determine the data was non-parametric. Parametric, continuous data was reported as mean ± standard deviation while non-parametric, continuous data was reported as median [interquartile range (IQR)]. When comparing outcomes between groups, nonparametric continuous data was analyzed with Mann-Whitney test. Nominal data was analyzed using chi-square or Fisher’s exact (if n < 5) tests. All P-values <0.05 were considered statistically significant.
Results
Baseline Characteristics
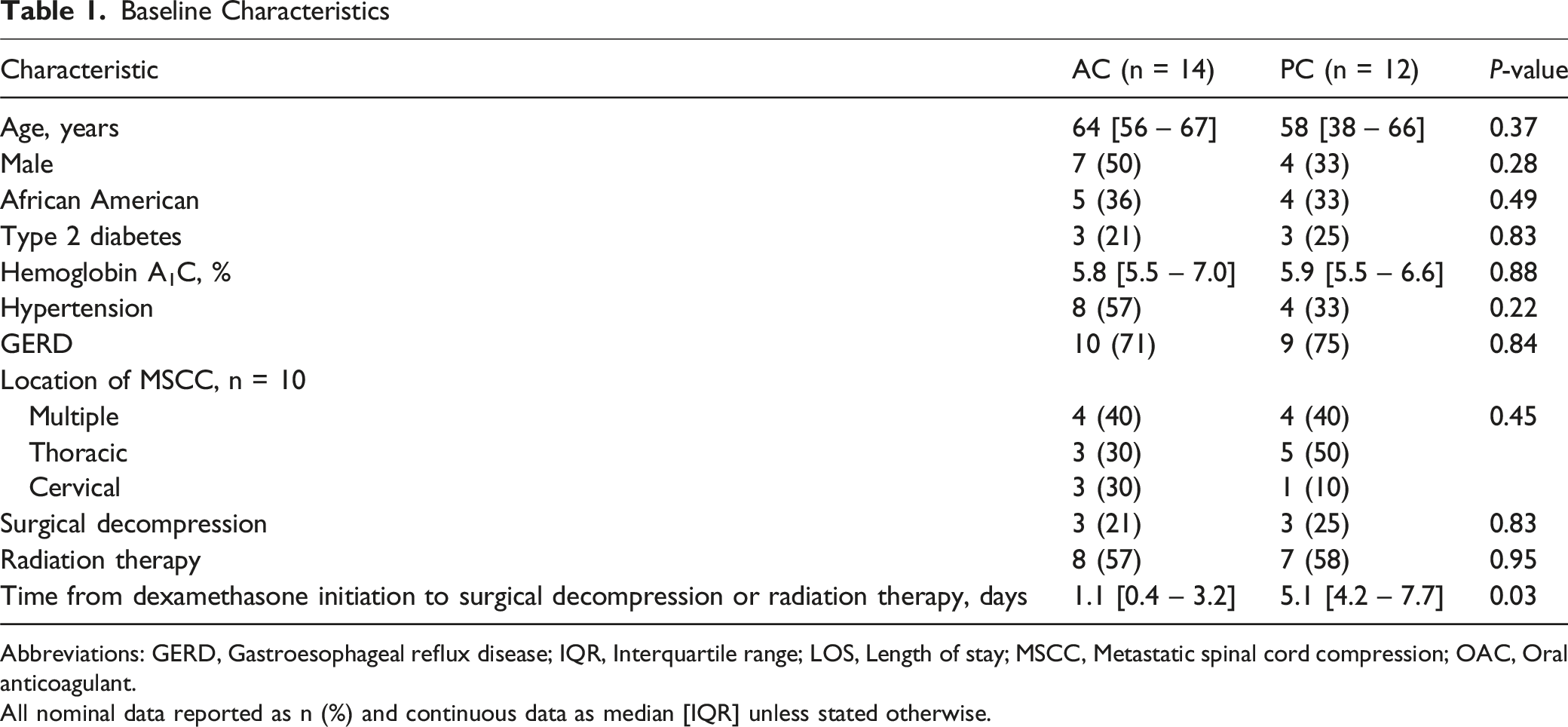
Abbreviations: GERD, Gastroesophageal reflux disease; IQR, Interquartile range; LOS, Length of stay; MSCC, Metastatic spinal cord compression; OAC, Oral anticoagulant.
All nominal data reported as n (%) and continuous data as median [IQR] unless stated otherwise.
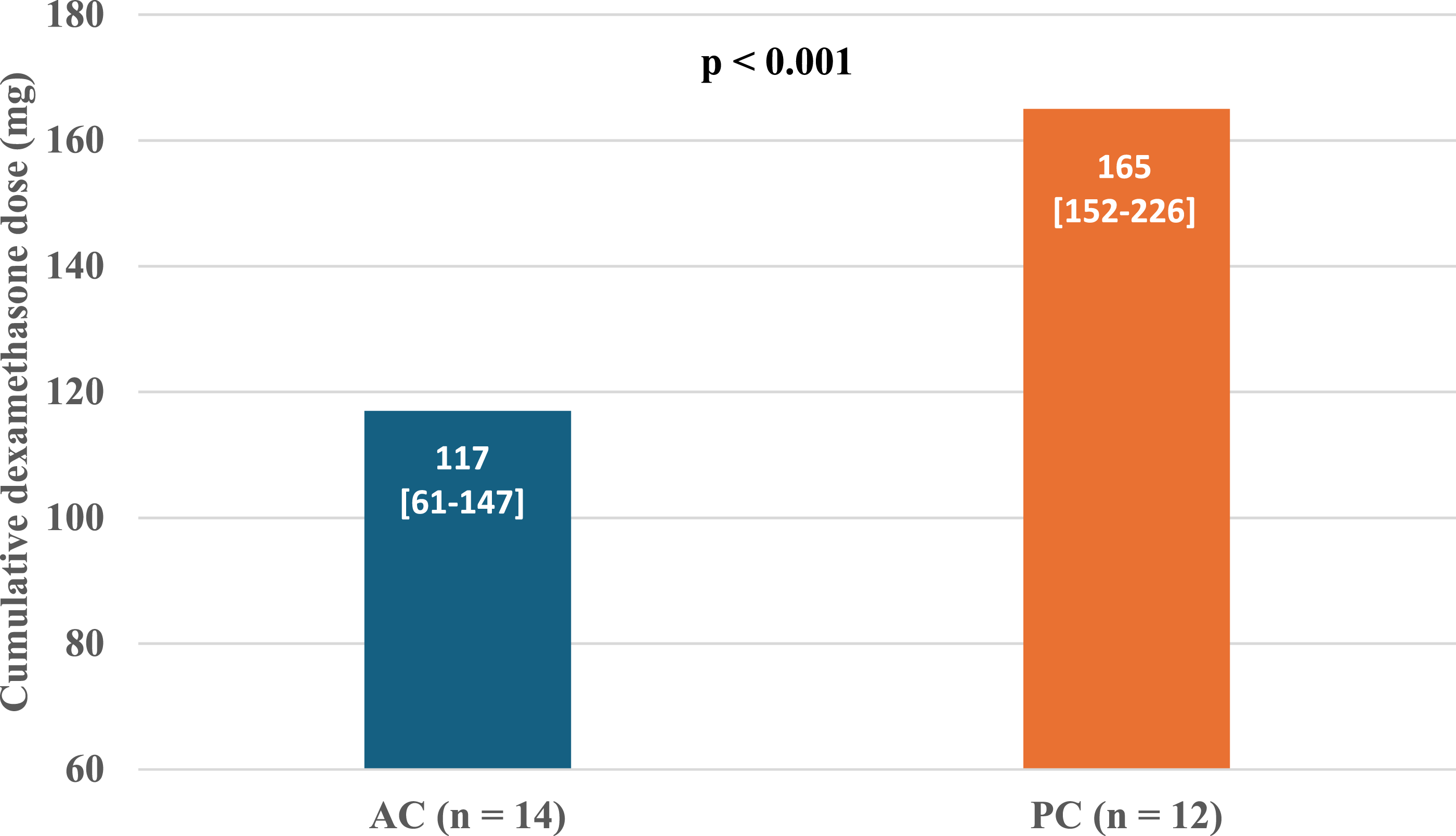
Median cumulative dexamethasone dose between groups. AC: acute course (≤3 days), PC: prolonged course (>3 days)
Secondary Outcomes
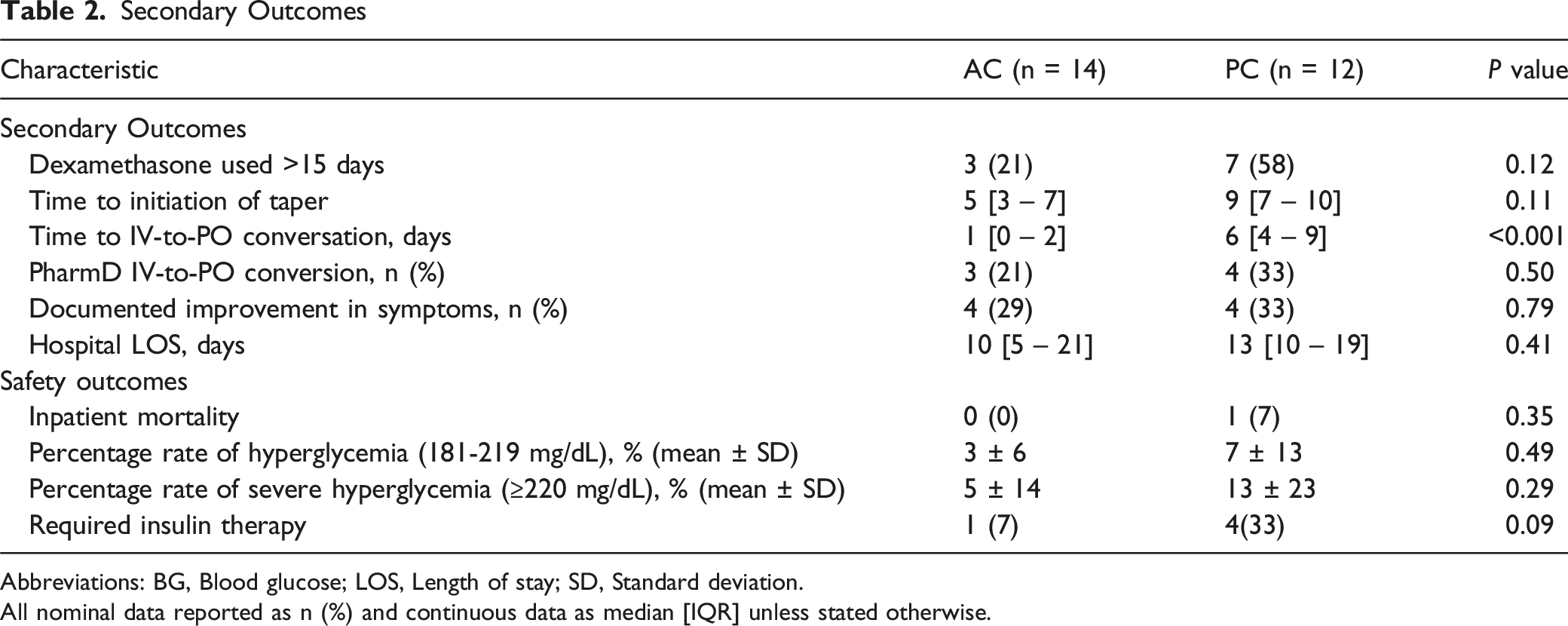
Abbreviations: BG, Blood glucose; LOS, Length of stay; SD, Standard deviation.
All nominal data reported as n (%) and continuous data as median [IQR] unless stated otherwise.
There were notable, clinically meaningful, numerical differences in the secondary outcomes between groups. The AC group had a numerically shorter hospital LOS compared to the PC group (10 vs 13 days, P = 0.41). Less patients in the AC group remained on dexamethasone longer than 15 days (21% vs 58%, P = 0.12), experiencedsevere hyperglycemia (5% vs 13%, P = 0.29), or required initiation of insulin therapy (7% vs 33%, P = 0.09); although none of these outcomes were statistically significant.
Discussion
This is the first real-world study comparing outcomes between patients who receive an acute course (≤3 days) and those receiving a prolonged course (>3 days) of adjunctive high-dose dexamethasone therapy (16 mg/day) for the management of MSCC. The findings demonstrate the use of prolonged, high-dose dexamethasone was associated with numerically higher cumulative dexamethasone exposure. Subsequently, our data demonstrates that exposure to higher cumulative dose of dexamethasone potentially increases the risk of patients experiencing severe hyperglycemia, requiring initiation of insulin therapy, and even longer hospital LOS; however, these findings require validation from large multi-center, prospective studies.
The practical use of adjunctive dexamethasone in the management of MSCC is highly variable due to the lack of robust evidence to guide use. The historical trials demonstrated the benefits of dexamethasone 16 mg/day for the first 3 days followed by a gradual taper with completion by day 15.6-8 In our study, the 72-hour mark was utilized to define our study groups based upon receipt of high dose dexamethasone, not the time in which the taper was started.6-8 Furthermore, the median time to taper initiation was 4 days longer in the PC group compared to the AC group. In our cohort, the PC group had a longer time to surgery which likely impacted the time on prolonged, high dose therapy as current recommendations recommend tapering only once definitive therapy starts. 3 Additional explanations for the use of prolonged, high dose dexamethasone could be attributed to provider preference or subjective severity of symptoms, neither of which could be reliably assessed given the retrospective nature of this study.
Various Dexamethasone Tapering Regimens
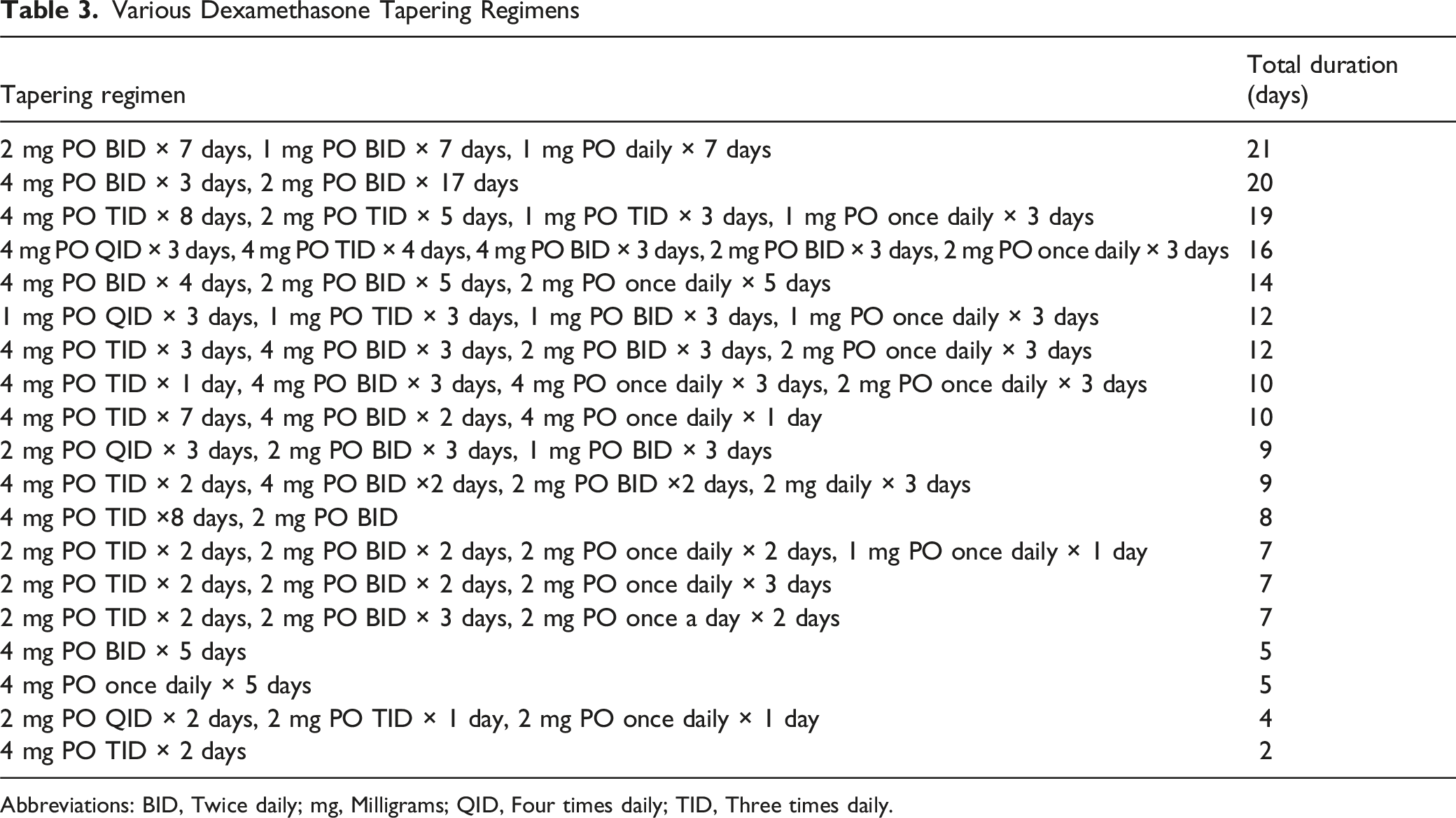
Abbreviations: BID, Twice daily; mg, Milligrams; QID, Four times daily; TID, Three times daily.
From a pharmacoeconomic perspective, prolonged high-dose IV dexamethasone therapy may increase healthcare costs due to extended hospital LOS for IV access, increased monitoring, and management of complications such as hyperglycemia. The time to IV-to-PO conversion was 5 days longer in the PC group, outlining an opportunity for earlier de-escalation or consideration for initial treatment being PO. This de-escalation represents an opportunity for enhanced pharmacy intervention as there was relatively low rates of pharmacist-driven conversions in the study.
This study is limited by its small sample size, retrospective design, and reliance on provider documentation for symptom assessment. Historical trials leading to the standard incorporation of dexamethasone in the management of MSCC also had relatively small patient populations, so it was not unexpected to get the small sample from a single center review. The limited sample sizes in this study as well as previous studies have limited the evaluation of adverse events from lack of power and further support the need for a large, prospective, randomized control trial. Additionally, the possibility of selection bias is present as this review focused only on hospitalized patients. As for possible confounding factors, the lack of standardized tapering protocols as well as timing of definitive intervention (surgery or radiation) may have introduced variability in treatment approaches. It is important to note that the generalizability of these findings may be limited as this practice is reflective of a single center in the United States and may vary significantly internationally or at other institutions. Lastly, patient-centered outcomes were not evaluated but warrant consideration. While symptom improvement was evaluated when documented, prolonged dexamethasone use may negatively impact patient quality of life through mood changes, sleep disturbances, and muscle weakness. Future studies should incorporate patient-reported outcomes to better assess functional and symptomatic benefits.
Despite these limitations, our study provides real-world relevance into the use of dexamethasone in MSCC and opportunities for improvements. The findings underscore the need for evidence-based guidelines to optimize dexamethasone use in MSCC and support the consideration of early tapering strategies when clinically appropriate. Future prospective studies are warranted to further define the role of dexamethasone duration and tapering in this population, with a focus on balancing efficacy and safety.
Conclusion
Compared to an acute course (AC, ≤3 days), the prolonged course (PC, >3 days) of continued 16 mg/day dexamethasone was associated with higher cumulative doses and increased rates of metabolic complications, with no significant improvements in symptom resolution or hospital length of stay. These findings support early tapering strategies as a safe and effective alternative approach, minimizing adverse effects without compromising clinical outcomes. Given the lack of standardized protocols, the study highlights the role clinical pharmacists can play in time to IV-to-PO conversion, steroid tapering, and decreasing adverse effects secondary to prolonged steroid use in MSCC patients. Future multicenter, prospective studies are warranted to validate these findings and inform guideline development for optimal dexamethasone use in MSCC management.
Footnotes
Ethical Considerations
The study was approved by the UTHSC Institutional Review Board.
Author Contributions
All authors contributed to the analysis, writing, and editing of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.