
Abstract
Upon successful completion of the PharmD program at KU, exit interviews revealed limited exposure to pharmacogenomics during clinical rotations. Hence, we surveyed Kansas pharmacy preceptors to investigate why and determine the need for continuing education. In this cross-sectional study, a survey was developed through Qualtrics. CORE ELMS was used to identify active pharmacy preceptors in Kansas who provide experiential education, and the survey was disseminated by email to 319 Kansas pharmacy preceptors. Responses were recorded and subgroup analyses were conducted using the chi-square test and Welch’s t-test. Sixty responses were received (18.8% response rate), and 58 were included in the analysis. Preceptors reported limited practical experiences with pharmacogenomics. Hospital preceptors reported seeing more patients with pharmacogenomics test results than community preceptors (65.0% vs. 27.3%, p = 0.0321). Overall, they demonstrated awareness of foundational pharmacogenomics concepts but limited applied confidence. Pharmacists who completed postgraduate training were more comfortable interpreting pharmacogenomics guidelines compared to those who didn’t (2.5429 vs. 1.6522 out of 5, p = 0.0004317). They all showed positive attitudes toward pharmacogenomics, with 83.9% willing to use as part of standard protocols and 93% agreeing pharmacists should lead its implementation. Additionally, they expressed a desire for online (70.2%) and local training (86%). Our results show that use of pharmacogenomics in clinics has been gradually increasing, but Kansas preceptors still exhibited limited experience and confidence levels. Online or local pharmacogenomics educational programs are needed for preceptors and pharmacists to further improve education and integration in clinics.
Introduction
Pharmacogenomics (PGx) is the study of how an individual’s genetic makeup can predict their response to drugs. It combines genetics and pharmacology to understand how genetic variations influence protein activity, which in turn affects pharmacodynamics and pharmacokinetics. These variations can lead to reduced drug efficacy or increased risks of toxicity.1,2 By understanding drug-gene interactions, pharmacogenomics aims to optimize drug efficacy, minimize adverse drug reactions, and guide personalized dosage adjustments based on genetic variability. 3 Given the complexities of pharmacogenomics, translating genetic information into patient care would be impossible without clear cut recommendations for healthcare providers.
The most widely used pharmacogenomics guidelines come from the Clinical Pharmacogenetics Implementation Consortium (CPIC®). In 2009, CPIC was created to establish guidance on how to use pharmacogenetic test results to adjust drug therapy. 4 Their first published guideline came just 2 years later for thiopurine drugs, adjusting drug doses based on activity of the inactivating-enzyme thiopurine methyltransferase (TPMT). 5 Over the years, CPIC has developed dozens of free, evidence-based, peer-reviewed clinical practice guidelines with specific drug dosing recommendations and evidence quality. As of September 2025, CPIC offers specific guidelines for 165 drugs. 6 Other notable pharmacogenomic guidelines include the Canadian Pharmacogenomics Network for Drug Safety and the Dutch Pharmacogenetics Working Group. Additionally, the Food and Drug Administration (FDA) includes genetic information on drug labeling, including boxed warnings. 7 Despite the numerous resources that exist for clinicians to use, pharmacogenomics has not yet fully been integrated into routine clinical practice.8,9
Numerous studies have investigated the barriers to implementing pharmacogenomics. Unclear cost benefits, challenges integrating genetic data into electronic health records (EHRs), and limited provider education are amongst the most cited obstacles.10-12 However, progress is being made across all areas. While insurance coverage for pharmacogenomic testing remains inconsistent, there is data to support the growing financial viability of PGx testing. A systematic review evaluating drugs with CPIC level A or B evidence found that most studies supported the cost-effectiveness of PGx testing. 13 For pharmacogenomics to be clinically useful, results must be integrated into a health system’s EHR and linked to clinical decision support (CDS) to trigger alerts. Most PGx results are currently delivered as scanned PDF documents, which are incompatible with CDS functions. 14 Some institutions are exploring ways to address this challenge, such as entering pharmacogenomic data into the EHR’s problem list or allergy section or even developing custom platforms. 15 Lack of provider knowledge also remains a key obstacle. CPIC was not established until 2009, with many guidelines not being published until years following. Many clinicians practicing today completed training before these advancements had been made, and many studies have demonstrated a lack of knowledge amongst healthcare professionals. A 2020 survey of Korean physicians reported that 53% of subjects lacked sufficient knowledge in pharmacogenomics. 16 A United States survey published in 2021 of primary care clinicians, which included 87% physicians, showed that only 2 respondents (3.6%) felt confident in their ability to interpret pharmacogenomic test results. 17
Given these challenges, pharmacists are uniquely positioned to lead the implementation of pharmacogenomics. Their advanced knowledge of pharmacodynamics and pharmacokinetics is the backbone of understanding the effects of drug-gene interactions and effectively managing them in clinical practice. The American Society of Hospital Pharmacists (ASHP) supports this, stating that “all pharmacists have a responsibility to take a prominent role in the rational, ethical use and clinical application of pharmacogenomics”. 18 Because of this, there have been many studies to investigate the knowledge, attitude, and confidence of pharmacists related to pharmacogenomics.
Surveys conducted both internationally and nationally reflect low levels of knowledge and confidence but favorable attitudes and perceptions towards pharmacogenomics. A survey published in 2020 of 206 hospital pharmacists in Saudi Arabia showed that only 30% of pharmacists had received formal training on pharmacogenomics, with 83% of pharmacists saying they felt they needed to know more. However, 76% of surveyed pharmacists answered that pharmacogenomic testing should be applied to pharmacy practice, showing positive attitudes towards PGx. 19 In a systematic review published in 2024 of 52 studies over 26 countries that evaluated pharmacists’ or pharmacy students’ knowledge, perception, or attitude towards pharmacogenomics, low levels of knowledge and low self-confidence were identified as the biggest barriers to pharmacogenomics clinical implementation. These findings were not country specific. Out of 34 studies that reported on PGx knowledge or awareness, 23 found that the majority of respondents had low or inadequate knowledge. However, there were 33 studies that reported on pharmacists’ perceptions, and most showed respondents as having positive perceptions towards pharmacogenomic testing. Additionally, there is an increased awareness and consensus of positive attitudes towards PGx compared to 8 years ago. 20
Surveys of pharmacists solely in the United States have shown similar insights. A survey of hospital pharmacists published in 2017 showed only 25% felt confident in their abilities to interpret pharmacogenomic test results, yet 72% favored implementing pharmacogenomics into pharmacy practice. 21 A more recent survey published in 2020 of pharmacists in a large multistate health system showed very mixed comfortability and attitudes towards pharmacogenomics. Interestingly, the survey found that those who had completed a post-graduate year 1 (PGY-1) residency were significantly more likely to have received formal pharmacogenomics training. Those who completed a PGY-1 also demonstrated stronger knowledge of PGx resources and more positive attitudes. 22 Clearly, training and exposure of pharmacogenomics plays a significant role in how willing and comfortable pharmacists are to participate.
In 2016, the Accreditation Council for Pharmacy Education (ACPE) included pharmacogenomics as a required element of the didactic Doctor of Pharmacy (PharmD) curriculum. 23 Starting that year, the University of Kansas (KU) School of Pharmacy began implementing pharmacogenomics into lectures and lab activities, emphasizing both scientific understanding and clinical application. Within the past 5 years, CPIC has become a central component of how KU school of pharmacy students are taught PGx. Currently, there are 4 pharmacogenomics lectures taken by third year pharmacy students in the fall semester and 2 labs, followed by an implementation project in the spring semester. This longitudinal curriculum design showed promise to provide long-term retention of pharmacogenomics knowledge. 24
Despite their strong foundation, many KU students report lacking opportunities to apply PGx knowledge during their Advanced Pharmacy Practice Experiences (APPEs). APPEs make up the final year of the PharmD program, where students have the opportunity to apply classroom knowledge in real-world settings under the guidance of preceptors before becoming fully licensed. At the end of students’ last year in pharmacy school, exit surveys are conducted to hear students’ thoughts and opinions on the program and what can be improved. Students reported during these exit surveys that they did not have opportunities to utilize pharmacogenomics knowledge and skills on clinical rotations. It was unclear whether this was due to preceptors’ knowledge, lack of patient cases, or other systemic issues. Given this gap, this study sought to investigate the current experiences, knowledge, and attitudes of Kansas pharmacy preceptors towards pharmacogenomics. Knowing preceptors’ perspectives helps us to understand the status of clinical pharmacogenomics. It also helps to identify gaps between education and practice, better aligning experiential training with didactic education. Finally, it helps to understand the need for pharmacists continuing education, ultimately supporting broader PGx implementation within pharmacy practice.
Methods
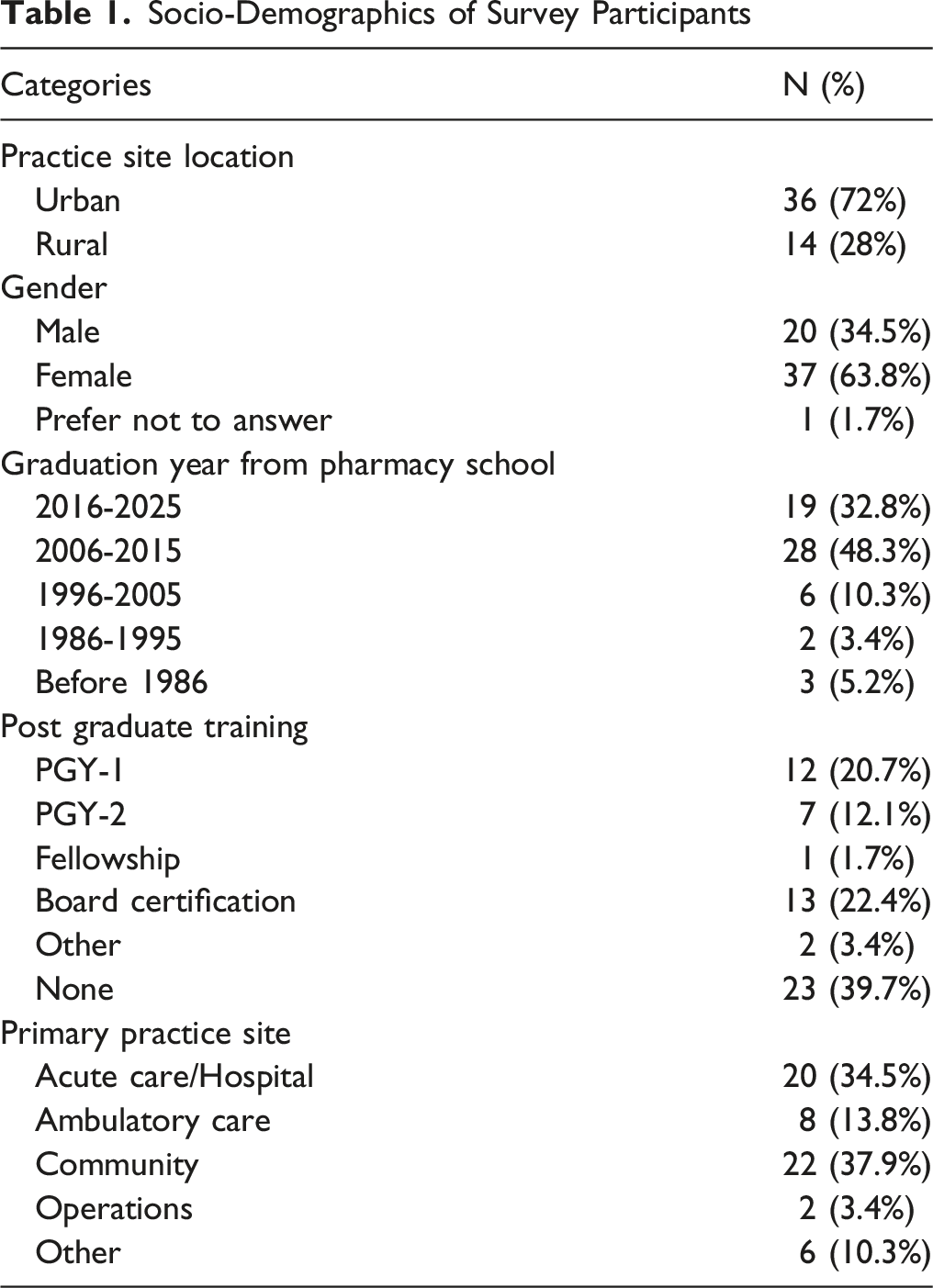
This cross-sectional survey of Kansas pharmacy preceptors was approved by KU’s Institutional Review Board on 4/14/2025. Twenty-one survey questions were initially drafted by the first author. Questions were adapted from those asked in the 2020 Saudi Arabia and US surveys.19,22 These questions were then reviewed, edited, and approved by the corresponding author before being transferred to Qualtrics in May 2025. The first question was an information statement to obtain consent. The other twenty questions were related to sample characteristics as well as experience, knowledge, and attitudes towards pharmacogenomics. Demographic variables included practice location, gender, graduation year, postgraduation training, and primary practice setting. Active preceptors were then identified via CORE ELMS, the administrative site for clinical rotations. Three hundred nineteen active preceptors who were registered with the KU School of Pharmacy, who precepted students exclusively in Kansas, and who had precepted a student within the last 3 years were identified. The survey link was initially shared with active preceptors via email on 6/2/2025, followed by 2 additional reminder emails on 6/18 and 8/6.
The data was secured on Qualtrics with password protection and was downloaded on 9/2/25 for analysis. Survey results were collected in tables on Microsoft Word for demographic variables and questions related to experiences, knowledge, and attitude of pharmacogenomics. The frequencies of each response were listed as both number and percentage. Figures were generated by Microsoft Word and Excel. In subgroup analysis, results were stratified based on demographic variables, excluding gender. Pearsons’s chi-square tests with Yates’ continuity correction were used to analyze experience related questions, and Welch modified two-sample t-tests were used to analyze knowledge and attitude related questions. Conditions and assumptions were checked first for both tests. For the chi-square tests, a couple of cells yielded the expected counts less than 10, so Yate’s continuity correction was used. For the t-tests, Likert-scale outcomes are ordinal but can be considered as scores, the distributions were not extremely skewed, and our sample sizes were not too small. Therefore, continuous data and normality conditions were satisfied. In addition, we checked independent subjects and there were no significant outliers. Effect sizes were also calculated as Cramér’s V for chi-square tests and Cohen’s d for t-tests. Cramér’s V effect sizes were interpreted as V < 0.2 as weak, [0.2, 0.4] as moderate, [0.4,0.6] as moderately strong, >0.6 as strong. Cohen’s d effect sizes were interpreted as ∣d∣<0.2 as negligible, 0.2≤∣d∣<0.5 as small, 0.5≤∣d∣<0.8 as medium, and ∣d∣≥0.8 as large. Lastly, statistical significance was set to P < 0.05. All statistical analyses were conducted using R (version 4.5.1, released on 2025-06-13).
As part of the demographic data collection, respondents were asked to provide the zip code of their primary practice location. These zip codes were used to identify the corresponding county and Federal Information Processing Standards (FIPS) code, which were then matched to Rural-Urban Commuting Area (RUCA) codes using the United States Department of Agriculture’s 2023 RUCA classification. 25 RUCA codes range from 1-10 and reflect levels of urbanization, population density, and commuting flows. This survey defined RUCA codes 1-3 as urban and 4-10 as rural. These cutoffs are consistent with those used in the 2020 U.S. survey and the 2018 survey it followed, aligning with definitions from the Health Resources and Services Administration.22,26,27
Results
Demographics of Participants
Socio-Demographics of Survey Participants
Participants’ Experience With Pharmacogenomics
Participants’ Experiences With Pharmacogenomics
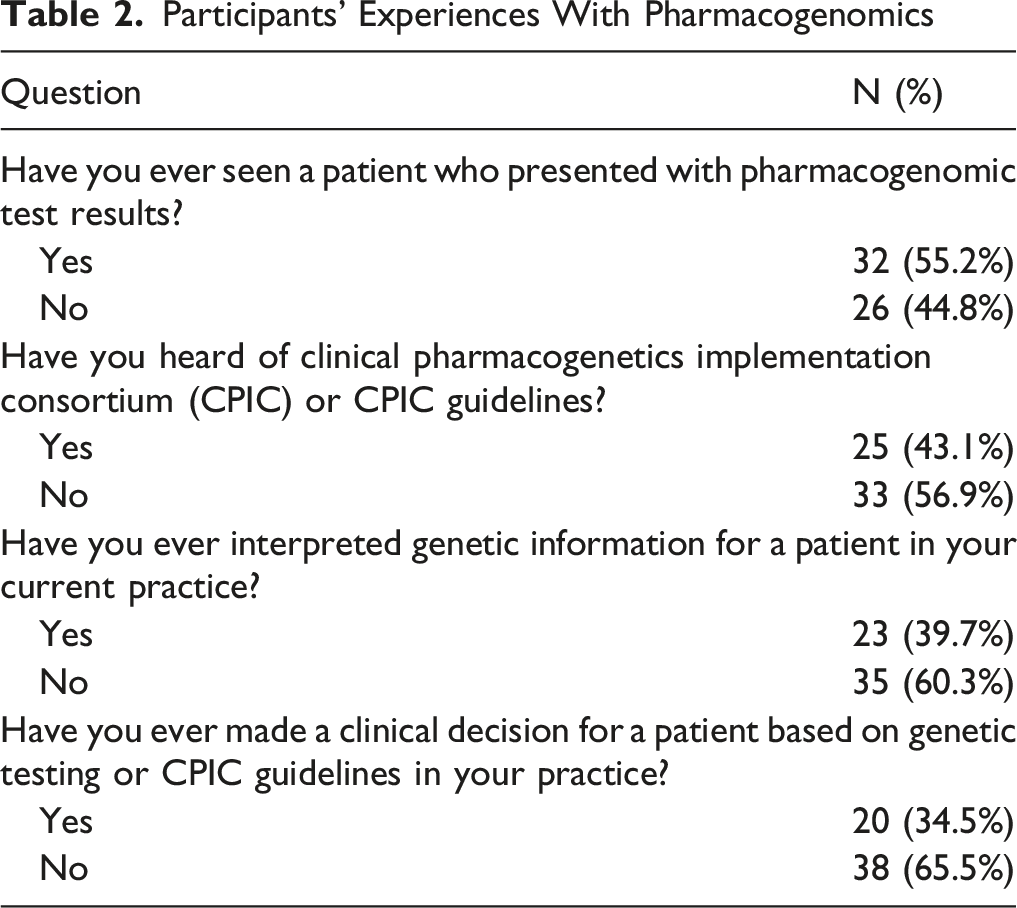
More than half of surveyed preceptors reported that they had seen a patient who presented pharmacogenomic testing results (32, 55.2%) compared to 26 (44.8%) who had not. Subgroup analysis was performed using demographic variables (excluding gender) and results are shown in Figure 1A. No clear difference was observed for those who have seen a patient with pharmacogenomic test results when comparing rural vs urban practice settings (71.4% vs 52.8%, P = 0.3785), graduation year before or after 2016 (53.8% vs 57.9%, P = 0.9923), or postgraduation training status (65.7% without training vs 39.1% with training, P = 0.08515). However, a difference was identified between community and hospital practice settings (27.3% vs 65.0%, P = 0.03211). Subgroup analysis of participants’ experiences with pharmacogenomics. (A) Have you ever seen a patient who presented with pharmacogenomic test results? (B) Have you ever heard of Clinical Pharmacogenetics Implementation Consortium (CPIC) or CPIC guidelines?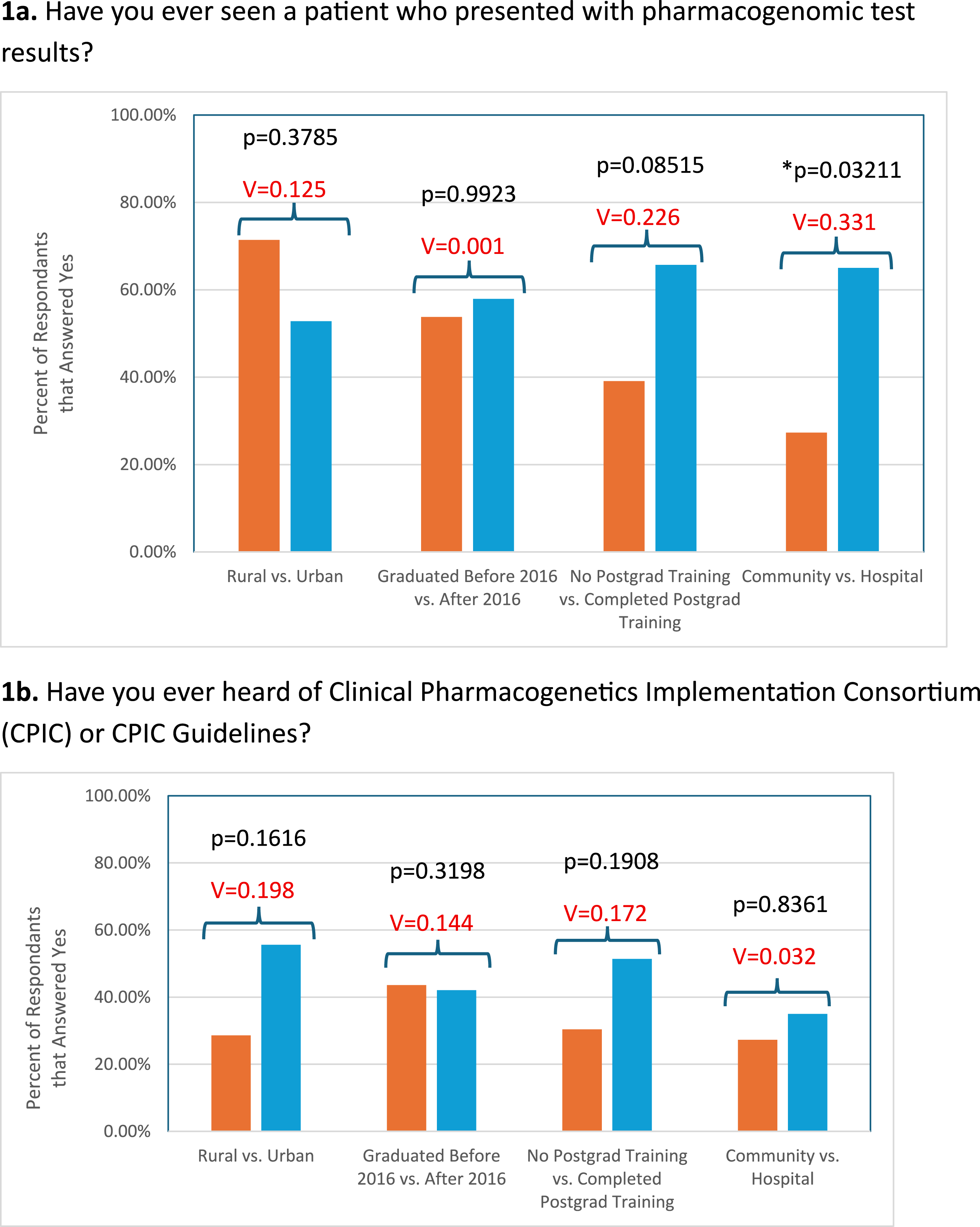
When asked if they have ever heard of CPIC or CPIC Guidelines, less than half answered “Yes” (25, 43.1%), while 33 (56.9%) responded “No”. Subgroup analysis was also performed for this question, with results presented in Figure 1B. No clear differences were observed between any of the demographic subgroups analyzed: rural vs urban (28.6% vs 55.6%, P = 0.1616), graduation year before or after 2016 (43.6% vs 42.1%, P = 0.3198), postgraduation status (30.4% without training vs 51.4% with training, P = 0.1908), and community vs hospital setting (27.3% vs 35.0%, P = 0.8361). These results suggest a general lack of familiarity with foundational pharmacogenomics resources, such as CPIC Guidelines, regardless of training background or practice setting.
For the third experience question, most preceptors reported that they have never interpreted genetic information for a patient (35, 60.3% vs 23, 39.7%). In the last experience question, most preceptors indicated that they have never made a clinical decision for a patient based on genetic testing or CPIC guidelines (38, 65.5% vs 20, 34.5%). Although a majority of Kansas pharmacy preceptors reported having seen patients with pharmacogenomic test results (particularly in hospital settings), their experience in using pharmacogenomics to inform clinical decision making remains limited. These findings highlight substantial gaps in the integration of pharmacogenomics into routine pharmacy practice.
Participants’ Knowledge About Pharmacogenomics
Participants’ Knowledge of Pharmacogenomics
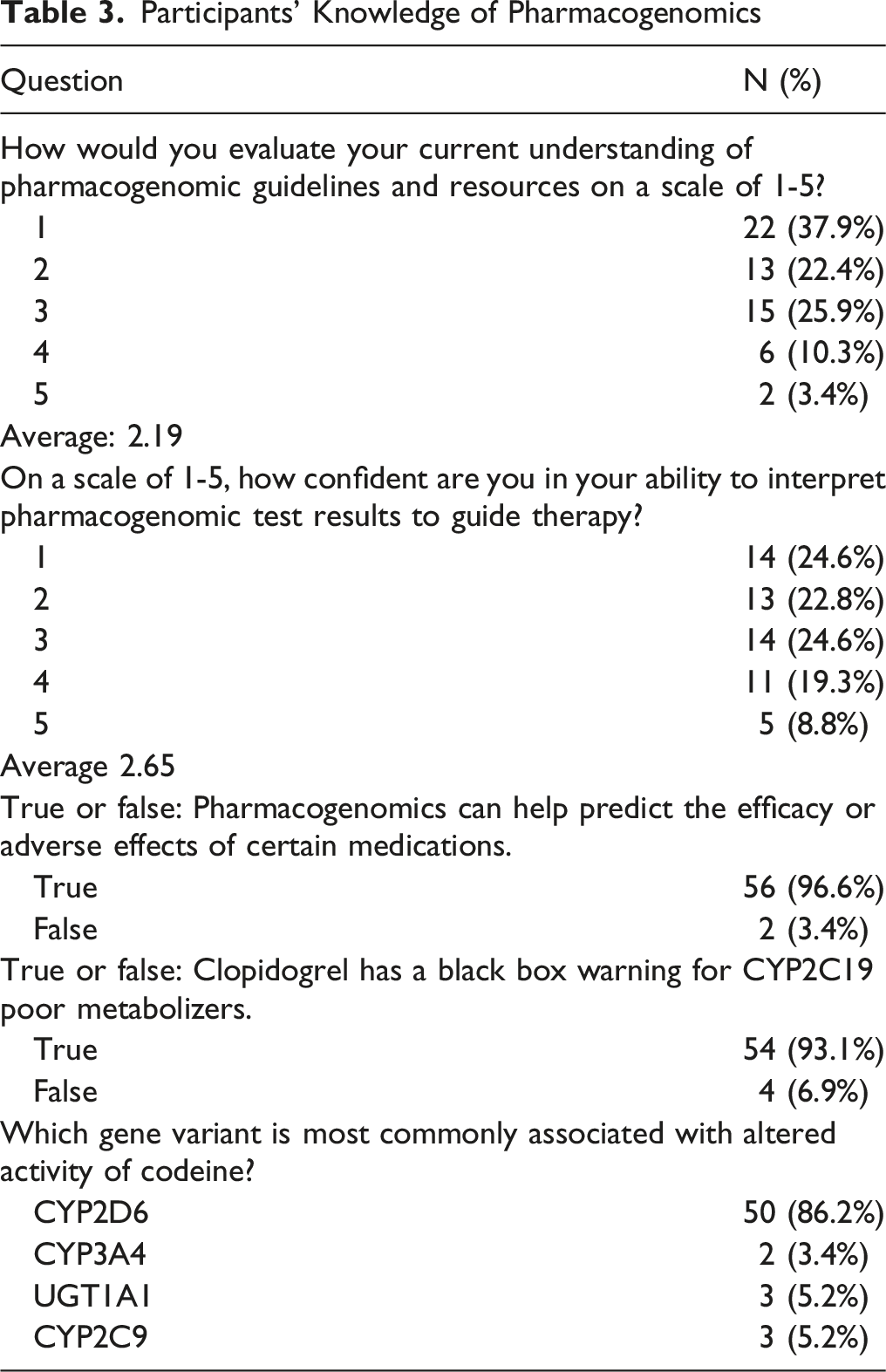
Preceptors were first asked to evaluate their current understanding of pharmacogenomic guidelines and resources on a scale of 1-5. The average response was 2.19 out of 5 with 37.9% answering 1. Subgroup analysis was performed for this question using demographic variables, excluding gender, and the results are shown in Figure 2. No clear differences were observed between rural and urban preceptors (1.79 vs 2.42, P = 0.0649), those who graduated before or after 2016 (2.05 vs 2.26, P = 0.5373), or those practicing in community vs hospital settings (1.68 vs 2.15, P = 0.1515). However, there was a difference when comparing postgraduation status. Those who had not completed postgraduation training had an average score of 1.6522 while those who completed postgraduation training had an average score of 2.5429 (P = 0.004317). Subgroup analysis of participants’ knowledge of pharmacogenomics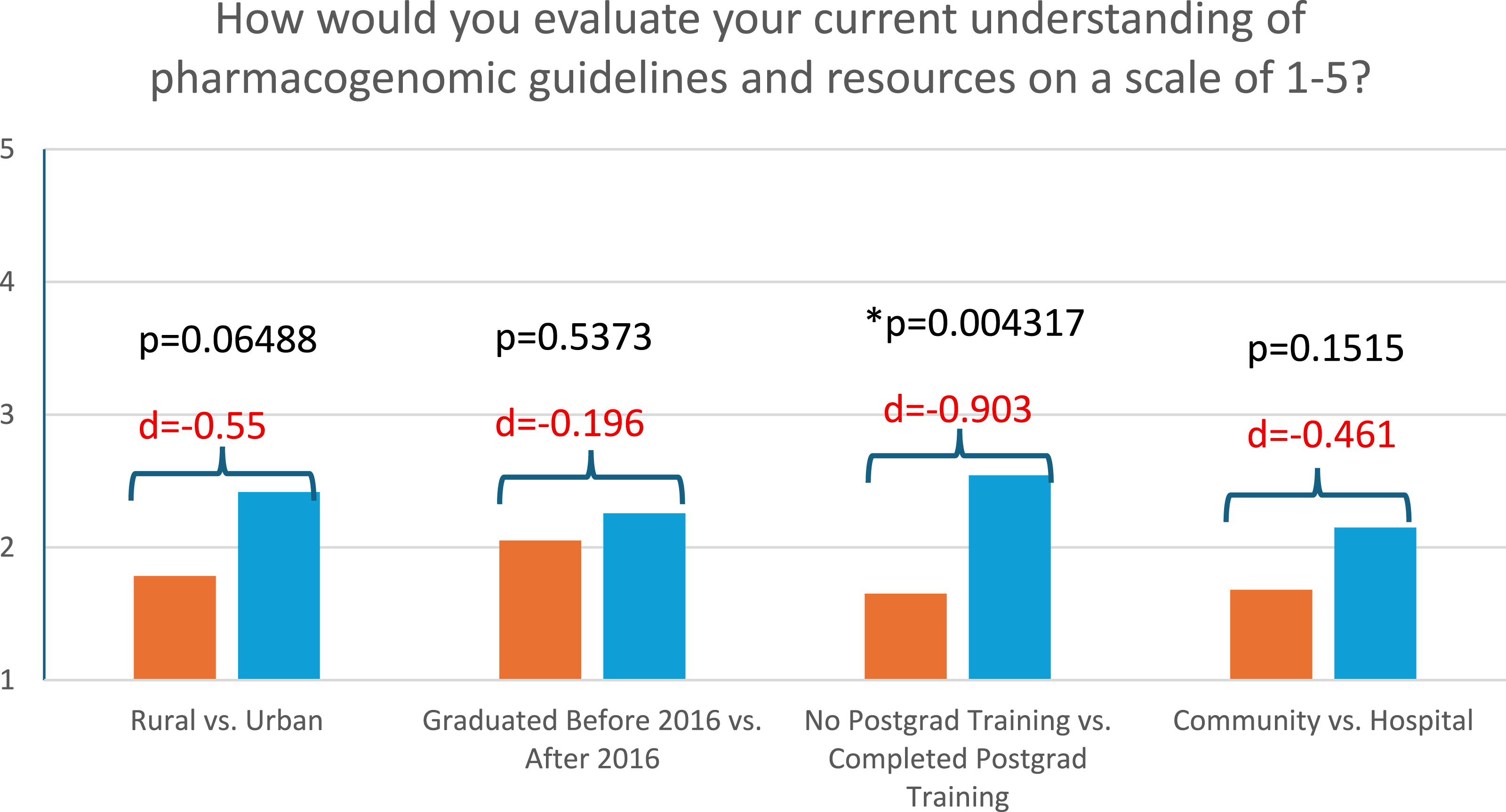
Next, preceptors were asked how confident they felt on a scale of 1-5 to interpret pharmacogenetic test results to guide therapy. Responses were slightly better compared to the first question, but the average response remained low (2.65 out of 5). These results suggest a generally low level of confidence utilizing pharmacogenomics, although those with postgraduate training appeared more confident.
Despite a self-reported lack of confidence and understanding, preceptors overwhelmingly answered direct knowledge-based questions correctly. Nearly all preceptors (56, 96.6%) correctly answered that pharmacogenomics can help predict the efficacy or adverse effects of certain medications. Preceptors also correctly selected that clopidogrel has a black box warning for CYP2C19 poor metabolizers (54, 93.1%). Lastly, 50 respondents (86.2%) correctly identified CYP2D6 as the gene variant associated with altered activity of codeine. These questions were relatively straightforward and did not involve interpretation of genetic information or application of clinical guidelines. However, the majority of Kansas preceptors demonstrated awareness of foundational pharmacogenomics concepts.
Participants’ Attitudes Towards Pharmacogenomics
Participants’ Attitudes Towards Pharmacogenomics
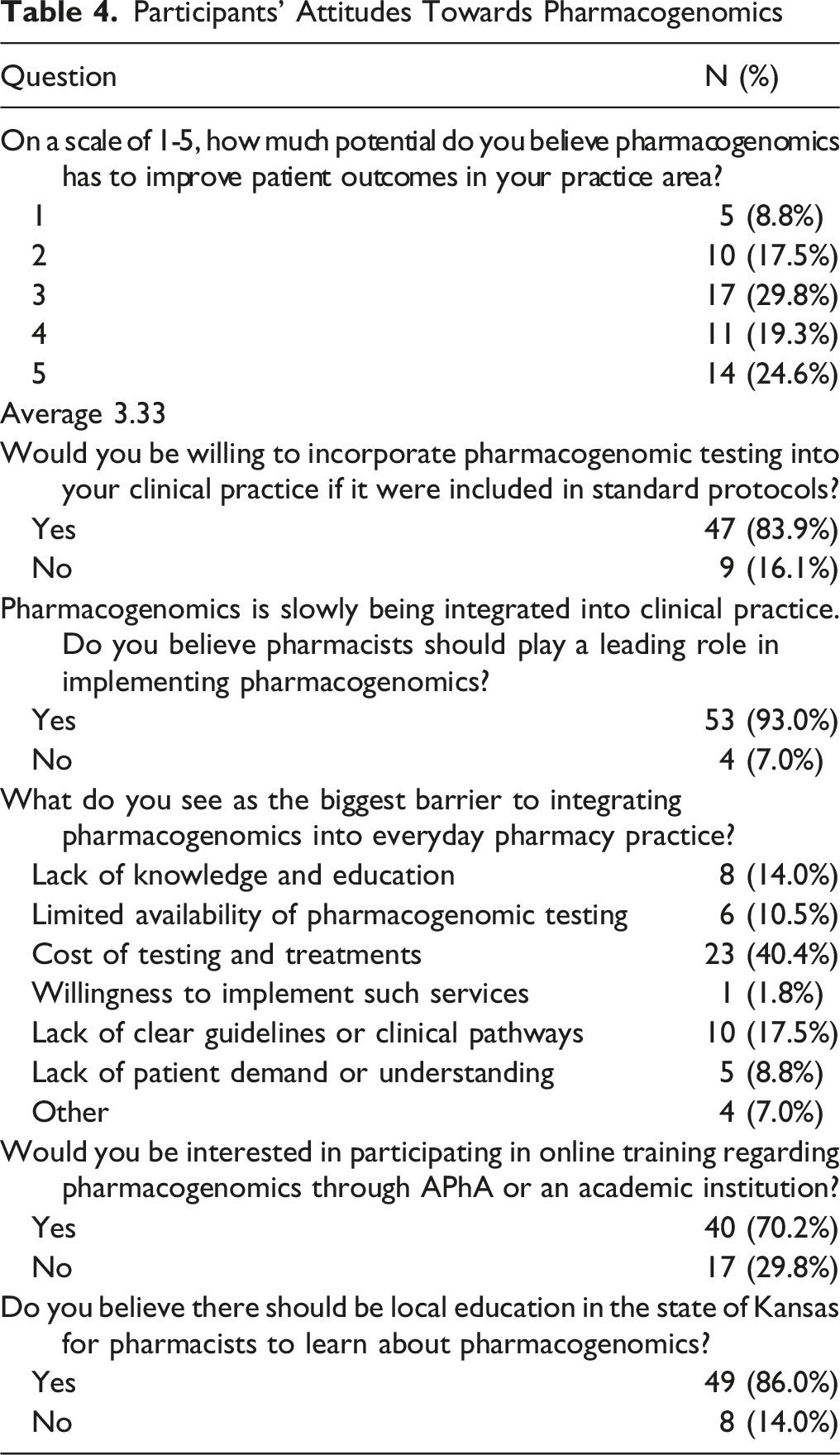
The first attitude-based question asked preceptors how much potential they believed pharmacogenomics has to improve patient outcomes in their practice areas. The responses were well dispersed with a mean response of 3.33 out of 5, showing mixed beliefs about pharmacogenomics’ potential clinical benefits. Subgroup analysis was conducted with demographic variables, excluding gender. Results are shown in Figure 3, and no clear differences were observed. Specifically, it shows rural vs urban (2.9286 vs 3.4722, P = 0.1493), graduation year before or after 2016 (3.4872 vs 3, P = 0.1612), postgraduation training status (3.3429 vs 3.3182, P = 0.9452), and community vs hospital settings (3.5714 vs 3.2, P = 0.3245). Subgroup analysis of participants’ attitudes towards pharmacogenomics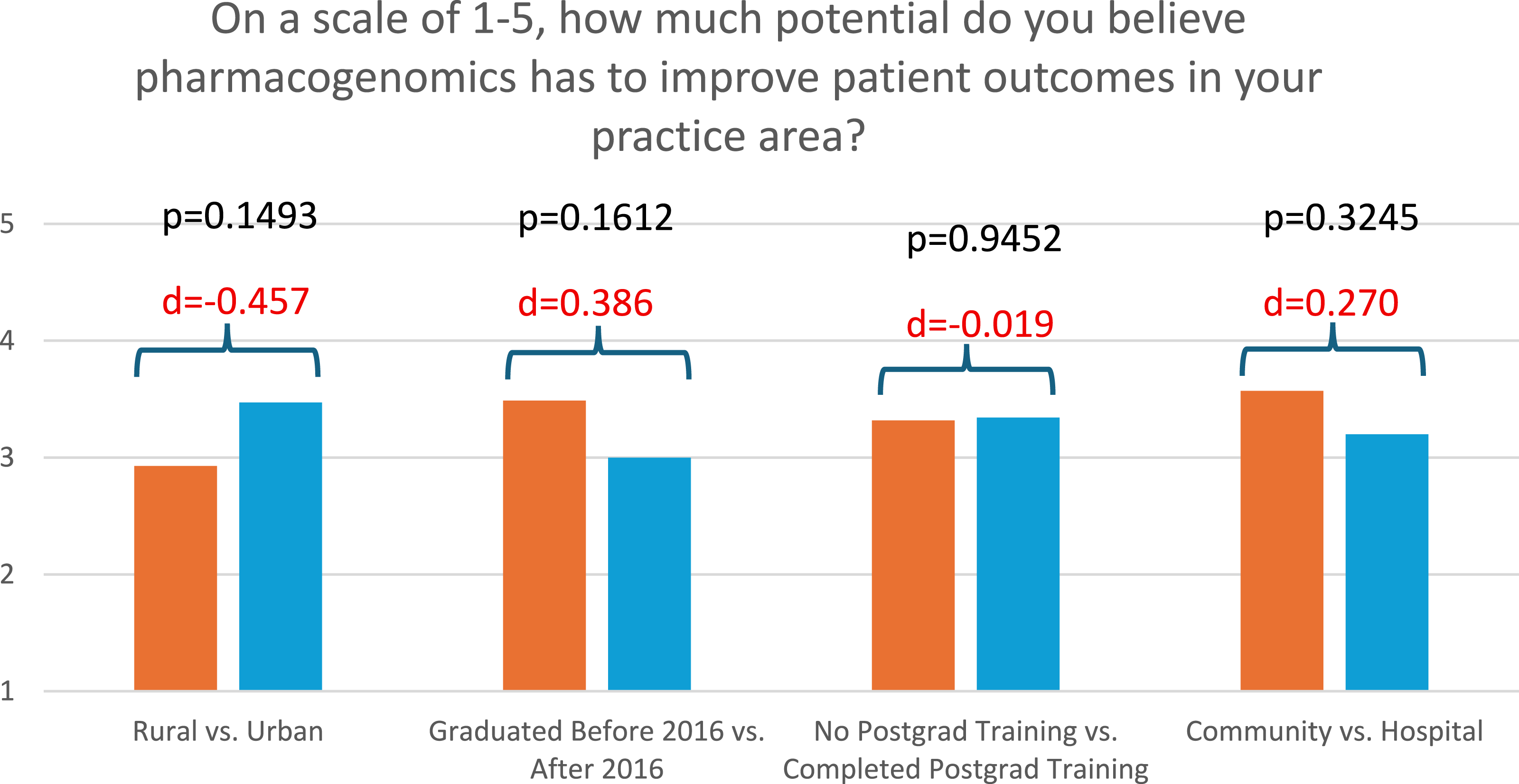
Even though preceptors showed inconsistent beliefs in pharmacogenomics’ clinical benefit, most of them answered they would be willing to integrate pharmacogenomic testing into their practice if it were included in standard protocols (47, 83.9% vs 9, 16.1%). In addition, most respondents believed that pharmacists should lead the integration of pharmacogenomics into practice, with 53 (93.0%) of subjects answering “Yes” and only 4 (7.0%) answering “No”. When asked what they perceived to be the biggest barrier to integrating pharmacogenomics into routine practice, more than 40% of the preceptors (23, 40.4%) believed that the costs of genetic testing were the largest barrier. Distribution for other barriers is shown in Table 4.
Lastly, this survey explored interest in pharmacogenomics education. A large majority of 40 respondents (70.2%) answered that they would be interested in online training for pharmacogenomics through the American Pharmacists Association (APhA) or an academic institution, while 17 (29.9%) answered they would not. Additionally, a larger majority of 49 respondents (86.0%) answered that there should be local education in the state of Kansas for pharmacists to learn about pharmacogenomics. Only 8 respondents (14.0%) disagreed. While overall data suggests limited experience and basic knowledge of pharmacogenomics, Kansas pharmacy preceptors largely showed positive attitudes towards pharmacogenomics and the idea of continuing education.
Discussion
Kansas pharmacy preceptors’ current experiences, knowledge, and attitudes towards pharmacogenomics were investigated in this study. Our study uncovered a few important changes reflecting recent improvements in clinical pharmacogenomics. However, our results are largely similar to previous national and international surveys. Most respondents reported limited experiences with pharmacogenomics in clinical practice. Most preceptors also expressed low confidence in their ability to apply PGx in patient care, even though they answered basic pharmacogenomics knowledge questions correctly. Lastly, respondents exhibited positive attitudes towards PGx, with a large majority supporting online or local training. While this survey only examined Kansas pharmacy preceptors, our study provides broader implications for pharmacy experiential education, pharmacists continuing education, and pharmacogenomics practice across the country.
The first block of survey questions focused on experiences with pharmacogenomics. This is 1 area that previous studies rarely diverge into, but it was included in our study as we felt it would provide insight into the current landscape of PGx implementation in practice. While some participants reported having seen a patient present with pharmacogenomic test results, most had never heard of CPIC, interpreted genetic information, or made a clinical decision based on genetic testing or CPIC guidelines (Table 2).
In 2020, Hundertmark et al reported that only 16% of the 75 respondents have had a patient or provider bring PGx test results for guidance in dosing or selection. 22 Our 2025 study found that 55.2% of the 58 preceptors had seen a patient with PGx test results. This suggests that pharmacogenomic testing has become increasingly more common over the past 5 years. Subgroup analysis showed clear differences between community and hospital settings for exposure to PGx results (P = 0.03211) (Figure 1A). This may be attributed to more robust access to electronic health records in hospital settings, which community pharmacists typically lack. Another explanation may be that hospitalized patients often present with more complex medical conditions, which may increase the likelihood of pharmacogenomic testing.
When subgroup analysis was conducted among preceptors who reported having heard of CPIC, no differences were observed across demographic groups (Figure 1B). We expected to see a difference in urban practice sites compared to rural areas since larger practice sites generally offer more advancements in emerging tools and resources. While more urban participants had heard of CPIC compared to rural participants, the results were not significant. This may be due to higher-than-expected pharmacogenomics opportunities in the specific rural areas that completed the survey, rural preceptors who completed training at schools where CPIC was taught, or limited awareness overall. Additionally, we expected to see differences based on graduation year since pharmacogenomics became a required component of pharmacy education in 2016. One possible explanation for the negative result is that the University of Kansas only started to emphasize CPIC within the past 5 years. To become a preceptor in the state of Kansas, pharmacists must practice for a minimum of 2 years. 28 Therefore, it’s possible that recent graduates who have received more comprehensive PGx education are not yet eligible to become preceptors. In addition, our surveyed preceptors may have graduated from other schools. Therefore, we cannot draw conclusions regarding KU’s curriculum as to why there is no difference between recent and previous graduates. Overall, the lack of awareness about CPIC illustrates the minimal practical exposure of Kansas pharmacy preceptors to pharmacogenomics in practice and emphasizes the importance of incorporating CPIC guidelines into future education.
The next block of questions focused on knowledge, consisting of both self-reported and direct knowledge-based questions. Pharmacy preceptors were asked to evaluate their current understanding of PGx guidelines and their confidence in interpreting PGx test results to guide therapy on a scale of 1-5. The average scores were 2.19 and 2.65, respectively (Table 3). This indicates low confidence in their knowledge and abilities to apply PGx, which is consistent with the international systematic review results. 20 Our results are also consistent with the 2020 US survey, where authors reported that over half of respondents expressed some degree of discomfort when asked to describe their ability to interpret PGx tests or provide recommendations based on results. They also rated themselves as not knowledgeable regarding PGx guidelines and resources. 22
Subgroup analysis for preceptors’ current understanding of PGx guidelines and resources showed a difference based on completion of postgraduate training (P = 0.004317) (Figure 2). The analysis combined all forms of postgraduate training surveyed (PGY-1, PGY-2, fellowship, board certification, and other). While there may be heterogenicity in their training experiences, the low sample size prevented further subgroup analysis into distinct postgraduate training groups. In the US 2020 survey, nearly all respondents completed a PGY-1 residency, and 1 third of our respondents completed PGY-1. Their survey reported that pharmacists who completed a PGY-1 were more likely to have received formal PGx training (P = 0.02) and assessed their own knowledge of PGx resources and guidelines higher than those without a PGY-1 (P = 0.03). 22 Although PGY-1 competency requirements list pharmacogenomics under the umbrella of “relevant health data” that pharmacists are expected to collect if available, there is currently no requirement to apply PGx or CPIC guidelines in therapeutic decision-making. 29 The increased confidence observed for those with post-graduation training may be attributed to their broader exposure to advanced clinical rotations and current literature where PGx is increasingly being referenced.
Despite the low self-reported knowledge of pharmacogenomics, Kansas pharmacy preceptors performed well on direct knowledge-based questions (Table 3). The 2020 US survey did not include direct knowledge questions, but the 2020 Saudia Arabia study did. In the Saudia Arabia survey of hospital pharmacists, 73.3% of pharmacists correctly responded that PGx is important to identify drug-drug interactions, and 58.7% correctly answered that the warfarin package insert warns of specific genes that may alter warfarin metabolism. 19 Kansas pharmacy preceptors in 2025 outperformed the surveyed Saudi Arabia pharmacists in 2020. However, this may mean little without a deeper evaluation of differences in PGx education, pharmacy curricula, and practice environments. More importantly, it should be noted that the direct knowledge questions included in our study were simple and don’t reflect the complexity of PGx application in real life. The drug-gene pairs asked about in this survey are baseline pharmacy knowledge and appear in literature and guidelines outside of pharmacogenomics. In addition, with artificial intelligence (AI) being widely available, our participants may have used AI when answering these questions. This may explain why our participants answered knowledge-based questions well but still lacked confidence in interpreting PGx test results. Overall, the high accuracy on these questions is encouraging, but it should not be interpreted as evidence of true proficiency or readiness to apply CPIC guidelines or pharmacogenetic principles in practice.
The final block of questions investigated the attitudes of Kansas pharmacy preceptors towards pharmacogenomics. Preceptors rated the potential of PGx to improve patient outcomes in their practice area at 3.33 out of 5 (Table 4). Subgroup analysis did not show any differences among demographic groups (Figure 3). Overall, these findings suggest that Kansas pharmacy preceptors hold moderately positive views regarding the potential impact of PGx, which is slightly different compared to previous studies. The international systematic review reported that most pharmacists believed PGx testing would improve overall patient safety and guide appropriate therapy. 20 The US survey did not report on potential benefits but found most respondents believed PGx has a significant impact on current practice. 22 While the respondents in this study had moderate views on the potential of pharmacogenomics, they are still favorable.
A large majority of subjects expressed a willingness to incorporate PGx testing if it was included in standard protocols (83.9%) and believed pharmacists should play a leading role in implementing PGx (93.0%) (Table 4). In the 2020 US survey, only 72% of respondents were willing to offer PGx testing and interpretation through pharmacy services. 22 This 11.9% increase from 2020 to 2025 likely comes from recent improvement in pharmacogenomics education. Additionally, both the systematic review and US survey provided strong data that support pharmacists leading pharmacogenomics implementation efforts.20,22 It is encouraging that despite limited experience and confidence, pharmacy preceptors still view pharmacists as the leading profession for pharmacogenomics implementation.
In our study, cost was identified by most Kansas preceptors (40.4%) as the largest barrier to PGx implementation, followed by lack of guidelines (17.5%) and lack of knowledge (14.0%) (Table 4). This is different from the systematic review and the 2020 US study that listed lack of education as the largest barrier.20,22 While lack of education is still undeniably an obstacle, the continued development of PGx education in pharmacy schools and postgraduation programs likely reflects recent progress. A tremendous stride has also been made in the affordability of pharmacogenomics. On July 12th, 2025, 1 Medicare Specific Local Coverage Determination deemed pharmacogenomic testing “reasonable and necessary” for medications with a known, clinically actionable drug-gene interaction as defined by the FDA and CPIC guidelines. 30 This policy not only recognizes CPIC as the central source for pharmacogenomic guidelines but also reduces cost barriers. This further emphasizes the importance of including CPIC in education and ultimately improving patient access to genetic testing.
Finally, most Kansas preceptors showed interest in online (70.2%) or local training (86.0%) for pharmacogenomics (Table 4). This enthusiasm is consistent with other studies. The 2016 survey of hospital pharmacists found that 97% of respondents would be interested in PGx related continuing education. 21 The international systematic review found that in 27 studies that accessed this metric, most subjects (with some studies reporting over 90%) expressed a desire for continued PGx education. 20 Pharmacogenomics has a bright future, as pharmacists who report limited knowledge are eager to learn. Interestingly, our data showed a 15.8% higher preference for local training compared to online training. Traditional methods of continuing education in pharmacogenomics, such as online clinical professional education (CPE), have not been shown to advance or change a pharmacist’s practice behavior. This is likely due to the complexity of PGx and the need for practice-based application. 31 Pharmacogenomics certificate training programs and institution specific programs at various health systems are much more likely to increase long-term retention.31,32 Institutions can generate their own PGx programs that fulfill their facility’s individual needs. Organizations and institutions can also collaborate with pharmacy schools to generate local PGx programs.
Based on these considerations, we strongly recommend the development and dissemination of institution-specific local PGx training programs, in addition to online certificate courses. These programs should emphasize practice using modules aligned with CPIC drug-gene pairs. Pharmacy schools should also incorporate PGx education into their preceptor development programs to improve integration into APPE’s. Lastly, schools can collaborate with local organizations to generate state-level pharmacogenomics initiatives. These efforts will not only enhance pharmacist knowledge but also support PGx implementation in clinics.
There were several limitations in this study. First, this study only surveyed Kansas pharmacy preceptors, so our results cannot be generalized to all pharmacists in Kansas. Preceptors generally demonstrate a strong desire for education. They are more likely to stay current with professional advancements and engage in continued learning. Therefore, our results may not truly reflect Kansas pharmacists’ experiences, knowledge, and attitudes towards pharmacogenomics. Second, this survey had a low response rate of 18.8%. While a response rate of 20-30% is considered reasonable for most survey-based research, our response rate was similar to other PGx surveys. For example, the Saudi Arabia study had a response rate of 17%, 19 and the 2017 hospital pharmacist survey had a response rate of 23%. 21 Our survey distribution occurred during the summer months, a period when many preceptors may be on vacation or managing multiple emails from students and new residents. Also, those who took the time to complete the survey may inherently be more interested in PGx or professional development. This can potentially lead to non-response bias and inflated results with limited generalizability beyond Kansas. Third, many of the survey questions were self-assessments which may not reflect true capabilities related to pharmacogenomics. The direct knowledge questions about clopidogrel and codeine are considered to be widely known drug-gene pairs and are referenced in various clinical practice guidelines. Thus, performance on these questions cannot be translated to pharmacogenomics as a whole or the ability of preceptors to apply PGx in clinical practice. In addition, participants were not warned against using AI or other drug information resources when answering knowledge-based questions. Therefore, it is a possibility some respondents looked up or checked the answer prior to submission. As AI becomes increasingly available, a request to avoid the use of online resources should be included in future survey studies assessing participants’ direct knowledge. Fourth, since subgroup analysis was not conducted on postgraduate training, it remains unclear if certain programs offer more pharmacogenomics exposure than others. Experiences in postgraduate training can vary significantly, and it is very possible that specific training types drove the derived differences. While the US 2020 survey supported benefits of PGY-1 residency training related to pharmacogenomics, similar conclusions cannot be drawn for PGY-2 training, board certification, and fellowship.
Conclusion
The use of pharmacogenomics in clinical practice has been gradually increasing, with testing becoming more common and pharmacists gaining knowledge in this field. However, Kansas pharmacy preceptors still reported limited practical experiences with pharmacogenomics. Participants demonstrated awareness of foundational pharmacogenomics concepts but limited applied confidence. Yet they still showed positive attitudes toward pharmacogenomics and a desire for continuing education. While this study cannot evaluate KU’s PGx curriculum and does not represent all pharmacists, preceptors’ limited experiences and confidence levels likely explain students’ lack of opportunity to practice pharmacogenomics during APPE rotations. Our findings also highlight the need for local continuing education programs that incorporate CPIC guidelines for preceptors and pharmacists in addition to online programs. Such initiatives are needed not only to further improve education but also to provide the tools necessary to integrate PGx into clinical practice.
Footnotes
Ethical Considerations
This project was approved by the University of Kansas’ Institutional Review Board on 4/14/2025.
Consent to Participate
Informed consent was obtained from all participants prior to survey participation via an information statement.
Author Contributions
Ryan Claycamp: Investigation, writing-original draft. Ming Wang: statistical analysis. Madison Shotton: writing- recruitment email. Jessica Bates: survey distribution. Andrea Reynolds: writing- review and editing. Susan King: writing- review and editing. Judy Wu: conceptualization, supervision, writing- review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.