
Abstract
Introduction
Gout is the most common inflammatory arthritis and occurs when hyperuricemia leads to the formation and deposition of monosodium urate crystals in and around the joint(s). 1 It is estimated that gout affects approximately 9.2 million people in the United States (about 3.9% of the adult population). 1 Common risk factors for gout include increasing prevalence of obesity, diabetes, chronic kidney disease (CKD), and hypertension. 1 Gout flares are characterized as painful episodes of arthritis and can result in disability and mortality. Left untreated, hyperuricemia can lead to long-term sequelae, including formation of tophi, severe joint damage, and overall poor quality of life and worsened clinical outcomes. 1
Unlike other common rheumatic diseases, the underlying cause of gout, chronic elevation of serum uric acid (sUA), is well known. Current American College of Rheumatology (ACR) Guidelines (2020) strongly recommend a treat-to-target management strategy that includes urate-lowering therapy (ULT) dose titration and subsequent dosing guided by serial sUA measurements to achieve target sUA, over a fixed-dose ULT strategy. 2 The ACR Guidelines recommend that patients with tophaceous or recurrent gout be treated with ULT to a target sUA of <6 mg/dL for non-tophaceous gout or <5 mg/dL for tophaceous gout. 2 Additionally, the ACR guidelines state that ULT titration should occur over weeks to months and not years. 2 However, only a minority of patients receive optimal therapy as gout management is often poorly monitored, and treatment targets are often not achieved. Deficiencies in ULT management include lack of adequate lab monitoring, failure to treat to sUA target, and hesitancy to increase ULT in patients with concurrent conditions such as CKD. When ULT is initiated, especially in primary care setting, it is often started at a fixed dose and not properly titrated as patients do not see their primary care provider frequent enough to perform ULT titrations.3-8
Available, though limited, literature shows that a pharmacist-managed gout clinic is effective in achieving target serum uric acid (sUA) levels and improving ULT adherence.3-8 Additionally, the ACR Guidelines even describe how 2 different pharmacist-led interventions, both incorporating treat-to-target strategies, were superior to usual care in terms of treatment adherence, sUA outcomes, and higher allopurinol dosing. 2 At Veterans Affairs San Diego Healthcare System (VASDHS), a pharmacist-managed, treat-to-target gout clinic (TTGC) was developed to address this need for difficulty managing patients and help bridge the gap in gout therapy. The objective of this study is to conduct analysis of the effectiveness of the TTGC in lowering sUA to target goal levels.
Methods
Setting
The TTGC was established in 2013 and enhanced in 2020 for better care coordination working directly with rheumatology specialty, collaborating with rheumatologists. Patients are usually referred to by primary care providers and initially evaluated by a rheumatologist, then transitioned into the TTGC for full management. The TTGC focuses on treating patients to goal sUA with minimal frequency to no recent gout flares, then discharged back to their primary care providers for ongoing management.
The clinical pharmacist practitioner (CPP) is a mid-level practitioner and has full scope of practice, practicing under evidenced-based practices for managing gout, including prescribing of pharmacotherapy, ordering of labs and referral for additional support. 9 All CPPs have full prescribing privileges and focus on Comprehensive Medication Management (CMM) practices.9,10 To capture these interventions, the Pharmacists Achieve Results with Medications Documentation Tool (PharmD Tool) was utilized to capture pharmacists’ interventions. The PharmD Tool is a clinical reminder within the electronic health record to capture pharmacists’ interventions made at each visit utilizing health factors.9-12 Possible medication interventions documented using the PharmD Tool include initiating a new medication, changing a medication, adjusting medication dose, and discontinuing a medication.9-12
Study Design
This was a single center, retrospective chart review of all patients enrolled in the pharmacy gout clinic from January 1, 2017, to December 31, 2021, and Institution Review Board (IRB) approved exempt status E230004 for this project. All first-time patient referrals to the pharmacy gout clinic were included in the analysis. Patients were excluded if at goal sUA at time of clinic referral, lost to follow-up after initial clinic visit, or if patients were co-managed by another provider for gout. The primary outcome of this study is change of sUA from baseline. The final sUA was defined as the last documented sUA before the study end period or at clinic discharge. Secondary outcomes include reduction of sUA at months 3, 6, 9, and 12. Secondary analysis was conducted to compare patients that reach goal sUA vs patients that didn’t. Patients without tophaceous or recurrent gout were considered to be treated to goal with sUA of <6 mg/dL for non-tophaceous gout or <5 mg/dL for tophaceous gout. 2
Data Collection
Baseline comorbidities, medications, and labs including sUA were collected from the initial pharmacy gout clinic appointment. Since the average time for follow-up clinic visits was 3 months, repeat labs were collected at months 3, 6, 9, and 12. If patients did not have a follow-up appointment at the designated time points, no data was collected. When collecting sUA, levels were recorded up to 2 weeks before the scheduled clinic appointment and up to 1 month after the clinic appointment as some patients obtained updated labs before or shortly after their appointment, and the CPP provided results and treatment plan once available.
Statistical Analysis
Student t-test or Mann-Whitney U test was performed for continuous data. Pearson chi-squared was used for categorical variables where appropriate. Two-tailed significance was defined as P < 0.05.
Results
Baseline Characteristics and Medications
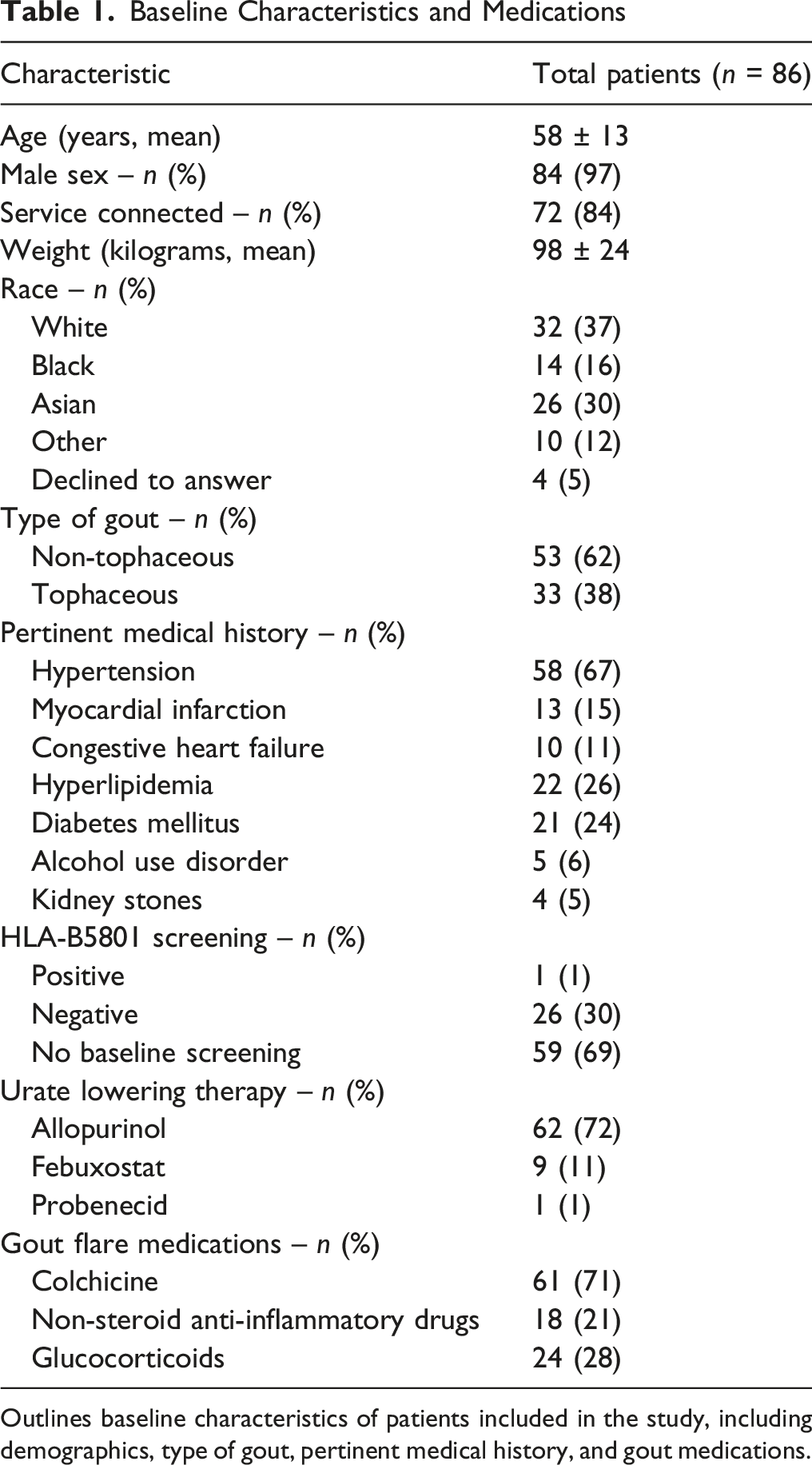
Outlines baseline characteristics of patients included in the study, including demographics, type of gout, pertinent medical history, and gout medications.
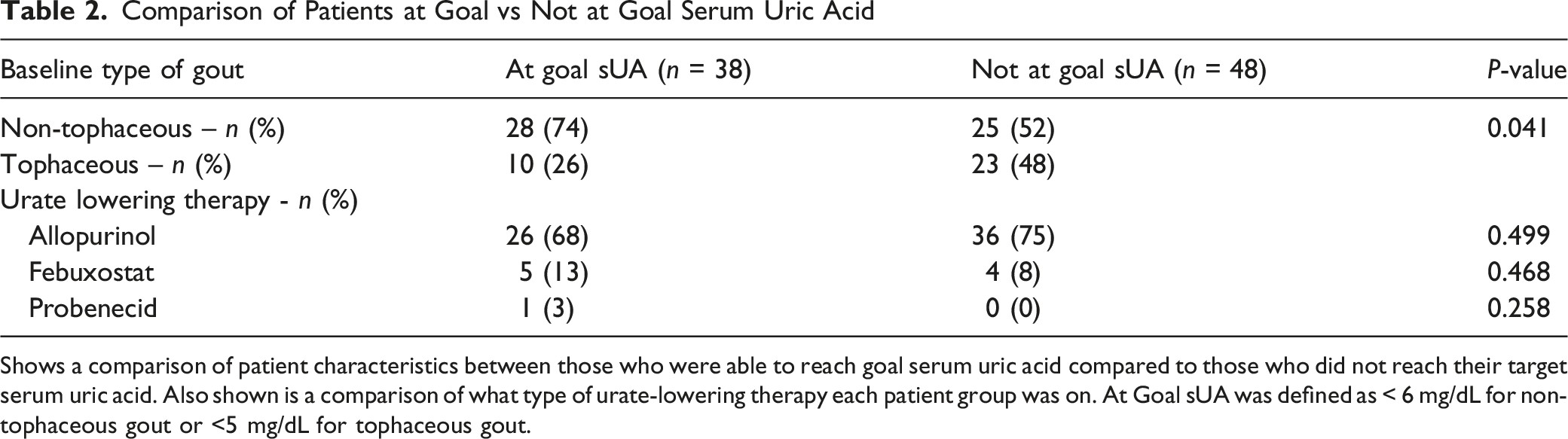
The mean baseline sUA was 8.1 ± 1.6 mg/dL, and the final mean sUA was 6.1 ± 1.8 mg/dL (P < 0.001, Figure 1). A total of 38 (44%) patients reached target sUA at discharge from the clinic. There was a statistically significant reduction of sUA from baseline at months 3, 6, 9, and 12 (Figure 1). Of those who achieved target sUA goal (n = 38), there was a statistically significant greater number of patients with non-tophaceous gout than tophaceous gout (P < 0.041, Table 2). There was no difference in which ULT medications were used between those who reached target goal vs those who did not. Baseline Serum Uric Acid Compared to Follow-Up Clinic Visits. Depicts serum uric acid levels measured throughout the study at the designated time points. Serum uric acid levels were collected at initial visit, 3-month, 6-month, 9-month, and 12-month, and then compared to baseline levels. There was a statistically significant difference when comparing baseline sUA to the final sUA at month 12 (P < 0.001) Comparison of Patients at Goal vs Not at Goal Serum Uric Acid Shows a comparison of patient characteristics between those who were able to reach goal serum uric acid compared to those who did not reach their target serum uric acid. Also shown is a comparison of what type of urate-lowering therapy each patient group was on. At Goal sUA was defined as < 6 mg/dL for non-tophaceous gout or <5 mg/dL for tophaceous gout.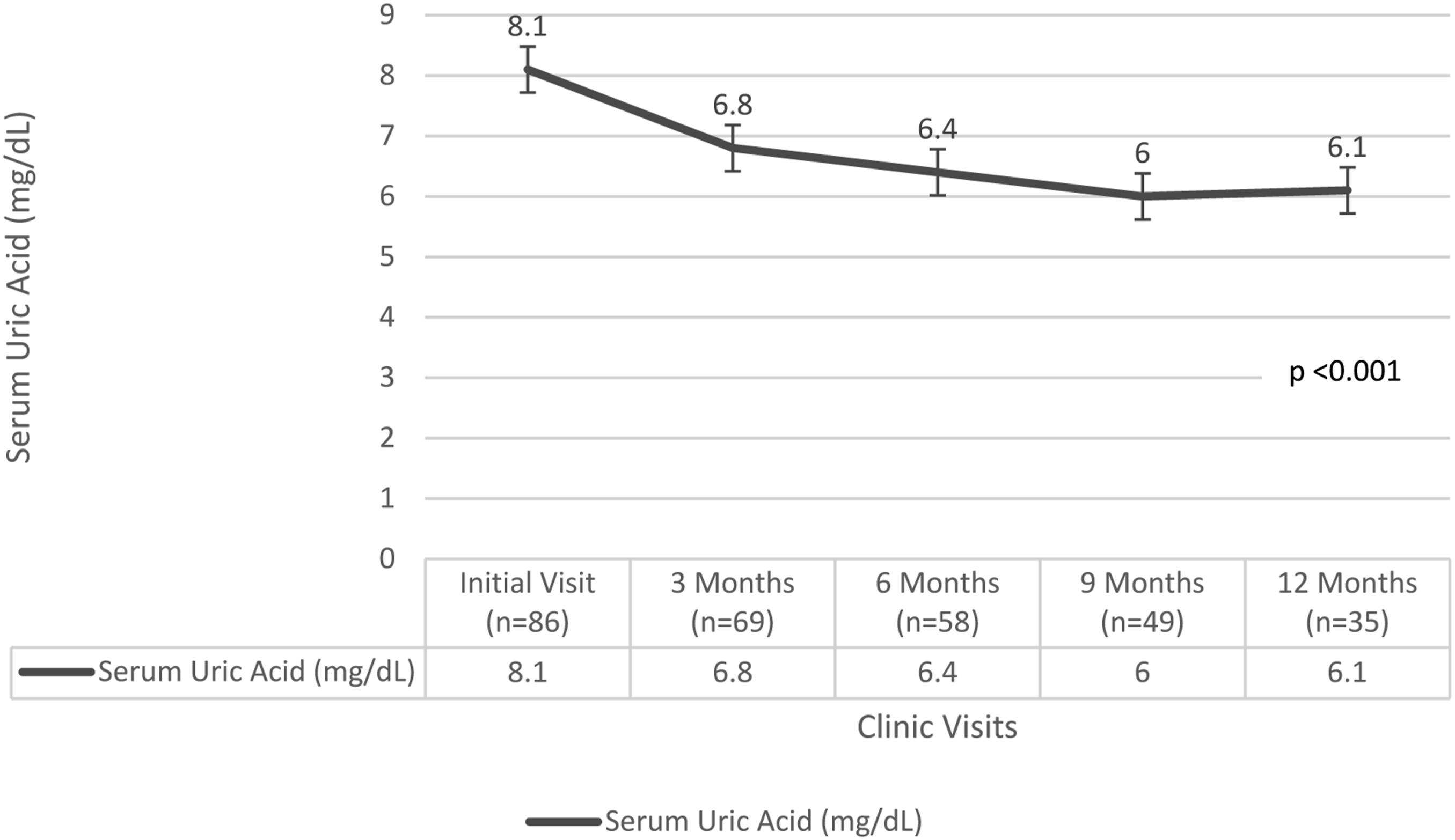
Pharmacist Interventions
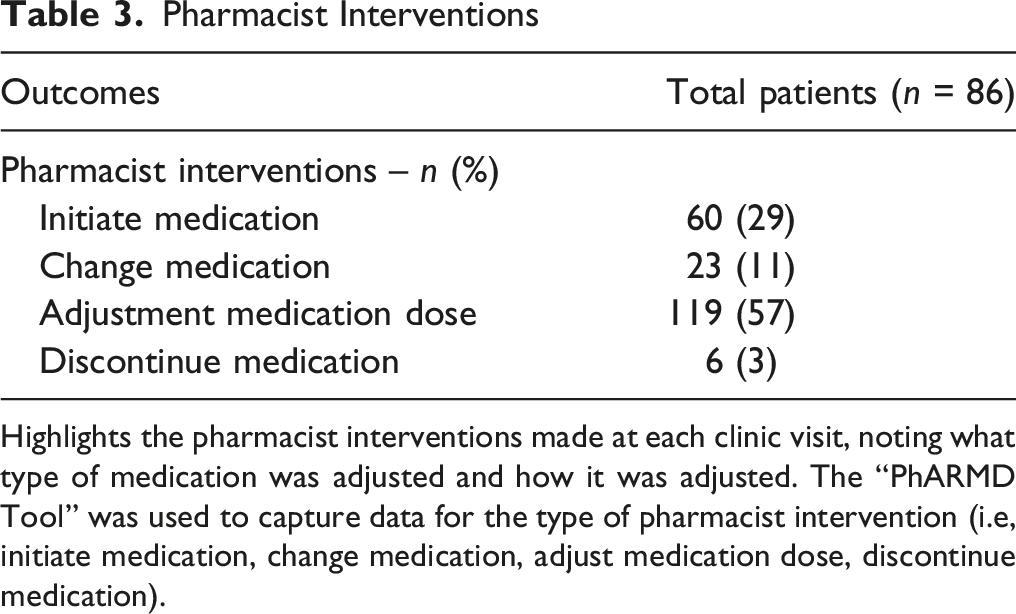
Highlights the pharmacist interventions made at each clinic visit, noting what type of medication was adjusted and how it was adjusted. The “PhARMD Tool” was used to capture data for the type of pharmacist intervention (i.e, initiate medication, change medication, adjust medication dose, discontinue medication).
Discussion
Previous studies on pharmacists led gout programs appear to focus more on compliance, titration and protocol driven management of gout, vs the current analysis focuses on independent mid-level practitioners operating under an open scope of practice for gout management.3-7 More recent systematic review literature has also evaluated pharmacist-led interventions and the role of pharmacists as collaborative members of the gout care team. 13 The final systemic review consisted of 5 studies with a total of 1805 patients, for which 2 studies were randomized controlled trials (RCTs) and 3 studies were non-randomized studies (non-RCTs). 13 It was found that pharmacist involvement resulted in greater achievement of sUA to target levels and facilitated appropriate dose titrations of ULT to reach the target levels in the intervention groups vs the control groups. 13 Pharmacist intervention also contributed to reduction of gout flares, and improvement of medication adherence. 13 Barriers in meeting treatment goal could include medication non-adherence or prescriber undertreatment in the primary care setting where most of gout management typically occur. 14 Therefore, it is important to optimize ULT through multiple rounds of monitoring labs and making dose adjustments in order to titrate doses appropriately. 14
This analysis highlights the potential role of CPPs in managing gout. The study showed statistically significant reduction in sUA to target goal level from baseline to discharge or 1-year post clinic enrollment in a patient population not controlled and already prescribed both ULT and gout flare medications. The mean difference in sUA lowering was 2 mg/dL which may impact gout outcomes and reduction of flares, but this was not evaluated in this study. Though there was a statistically significant reduction in sUA, the mean sUA remained above goal for both non-tophaceous and tophaceous gout, and the target sUA was only achieved in less than half of the total number of patients. However, this finding may not be clinically relevant as patients can be above sUA goal and still be gout flare free or have low frequency of flares. More than half of the patients did not reach their sUA goal; however, for those who achieved their sUA goal, there were significantly more patients with non-tophaceous gout compared to tophaceous gout. This is likely due to the potential difficulty of managing patients with more stringent sUA goals of <5 in patients presenting with tophaceous gout. More than half of the total pharmacist interventions were adjusting and titrating ULT doses which support that with adequate follow-up and appropriate dose titrations like previous titration programs,3-7 patients can achieve target sUA goals. With that said, having an open scope of practice also can elevate pharmacists’ roles as 29% had new initiation of pharmacotherapy for gout management in this analysis. In addition, the patients enrolled in this study were likely to be more difficult to manage patients, as they were referred by primary care providers, or rheumatologists to the TTGC, further supporting the effect of this specialized pharmacist managed clinic.
The results of this study align with current literature that shows a pharmacist-managed gout clinic can help bridge the gap in gout therapy. Patient management is individualized. Therefore, a holistic approach to gout management and emphasis in diet and lifestyle factors play a key role in gout therapy. 15 Though non-pharmacological interventions and types of education provided were not collected for this study, each visit with the CPP included counseling on diet and education of the disease state and medications. It can be suggested that by increasing patient education and healthcare literacy, then patient outcomes also improve. 16
Additional pharmacological interventions that were not captured in this study but are important to note include CPP recommendations to change pertinent medications for other comorbidities that may be negatively affecting gout outcomes and sUA. With a scope of practice, CPPs can perform comprehensive medication management (CMM) to address gaps in care to optimize patient therapy and outcomes. 9 These interventions for pertinent comorbidities highlight the benefit of utilizing pharmacists for medication management and adjustments that may be overlooked by other providers.
It is also important to consider that no baseline HLA-B5801 screening is defined as not having an HLA-B5801 lab on file at the time of the initial TTGC visit, however it does not suggest that it was not ever completed prior to being referred to the TTGC since some of the patients may have had the lab drawn at a different healthcare institution. Therefore, while 30% of patients were of Asian descent and 69% of patients had no baseline HLA-B5801 screening on file, these patients were already established on allopurinol for at least 1 year by the time that they were transitioned to the TTGC from their primary care provider or rheumatologist. Many of the patients have already taken allopurinol for years and tolerated without cutaneous adverse drug reactions and were then referred to the TTGC for continued management and further dose titrations.
There were several limitations to this study. First, this study was only performed at a single center which limits the generalizability of the results. Additionally, given that the clinic was only open one half-day each week, there was a smaller sample size to evaluate which also limited the findings. The study only followed per protocol inclusions of patients and did not follow intention-to-treat analysis. There was no control group for this study, further limiting causations. Because this was a small, real-world, retrospective observational study with substantial attrition over time, several advanced longitudinal techniques (such as mixed-effects modeling or repeated-measures ANOVA) were not statistically appropriate or feasible. The study was not originally powered for longitudinal modeling but rather for descriptive evaluation of serum uric acid (sUA) trends in routine clinical practice. Follow-up intervals were not strictly protocolized, and measurements beyond baseline were obtained only when clinically indicated, resulting in irregular timing and variable availability of data points. Also, these were patients referred from primary care that were unable to reach targets, thus potentially signifying that this cohort may be more difficult to manage compared to standard of care patients. The study focused only on sUA values vs actual clinical outcomes (ie, reduction in flares, emergency room visits, or hospitalizations). Lastly, the full impact of non-pharmacological interventions was not assessed but extensive counseling on diet and other pertinent lifestyle factors were provided at every clinic visit.
The study suggests the value of the clinical pharmacist TTGC in managing gout in a veteran population. Pharmacist TTGC can be effective in lowering serum uric acid levels and achieved serum uric acid goals. The results of this study are consistent with the results of limited literature, and this study expands to the veteran population.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. The material is the result of work is only supported with resources and the use of facilities at the VASDHS.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will not be made available.
IRB Protocol
IRB Exempt Status approval granted.