
Abstract
Previous literature has demonstrated that hyperlipidemia is common post-transplant; however, low statin utilization has been seen post-liver transplant. Furthermore, assessment of statin qualification in this setting is limited. This study’s objective was to evaluate the incidence of hyperlipidemia and determine the rate of qualification for and initiation of statin therapy in liver transplant recipients to better characterize the complication and associated clinical practice behaviors. This single center, retrospective cohort study included adult patients who received an isolated liver transplant between January 1, 2015 and June 30, 2019 and had lipid panels within 15 months pre- and post-transplant. The dual primary outcomes were the incidences of hyperlipidemia and statin qualification, as determined by 2012 AASLD and 2018 ACC/AHA guidance. Secondary outcomes included statin use and tolerability, hypertriglyceridemia, and immunosuppression factors. Of the 282 patients screened, 79 patients were included. Compared to pre-transplant, incidences of hyperlipidemia and statin qualification were both increased post-transplant (hyperlipidemia: 21.5% vs 49.4%, P = 0.0003; statin qualification: 46.8% vs 64.6%, P = 0.025). Of the 51 statin-qualifying patients post-transplant, twenty-two (43%) received statin therapy. One patient experienced muscle aches requiring statin discontinuation. Hypertriglyceridemia was more common post-transplant than pre-transplant (11.4% vs 60.8%, P < 0.0001). Of patients on tacrolimus, 58% qualified for statin therapy compared to 93% of patients on an mTOR inhibitor. Nearly two-thirds of liver transplant recipients qualify for statin therapy post-transplant. Despite increased rates of dyslipidemia and statin qualification post-liver transplant, statin therapy remains underutilized. Optimization of lipid management remains an area of need post-liver transplant.
Introduction
Hyperlipidemia is a common post-transplant complication that is observed in up to 71% of liver transplant recipients. 1 The etiology of hyperlipidemia in these patients can be multifactorial involving factors like age, body weight, and genetics, but the use of immunosuppressive medications and glucocorticoids largely influences the increasing prevalence of lipid disorders in transplant recipients. 1 Lipid disorders are known to significantly increase the risk for atherosclerosis leading to major cardiovascular events. In liver transplant recipients, cardiovascular events are among the leading causes of mortality. 2 A meta-analysis done in 2012 found that liver transplant recipients had a 64% greater risk of experiencing a cardiovascular event compared to the general population. 3 Uncontrolled lipid disorders in transplant recipients not only lead to poor cardiovascular outcomes but can also lead to graft dysfunction and decreased survival. 1 It is essential to manage hyperlipidemia in liver transplant recipients to improve health outcomes and ultimately prolong survival.
The American Association for the Study of Liver Diseases (AASLD) recommends that annual screening for hyperlipidemia occurs in liver transplant recipients.4,5 Per the 2012 AASLD guidelines, an elevated low-density lipoprotein (LDL) level >100 mg/dL with or without hypertriglyceridemia was considered hyperlipidemia and required therapy in these patients. 4 Statin (3-hydroxy-3-methyl-glutaryl-coenzyme A reductase inhibitor) therapy was recommended when diet and lifestyle modifications were not enough to manage dyslipidemia. 4 The more recently published 2025 AASLD and American Society of Transplantation (AST) Practice Guideline on adult liver transplantation recommend hydrophilic statins, such as rosuvastatin for high intensity and pravastatin for moderate intensity, as first line therapy in combination with lifestyle modifications in liver transplant recipients with hyperlipidemia. 5 These guidelines include assessment of the 10-year atherosclerotic cardiovascular disease (ASCVD) risk to help determine statin therapy needs. For those with no risk factors, a LDL level ≥130 mg/dL was the statin qualifier for therapy. 5 As of 2018, the American College of Cardiology (ACC) and the American Heart Association (AHA) recommend that statin therapy be used for secondary prevention of clinical ASCVD and for primary prevention of ASCVD in patients with elevated LDL levels (≥190 mg/dL), those with diabetes mellitus, who are 40 to 75 years of age, and those determined to be at sufficient ASCVD risk after a clinician–patient risk discussion. 6 The intensity of statin recommended depends on the baseline LDL level, comorbidities, and/or overall 10-year ASCVD risk estimation. 6 The 2018 ACC/AHA guidelines do not specifically address liver transplant as a risk factor for hyperlipidemia, but based on the high prevalence of cardiovascular events in this population, lipid optimization must be considered post-transplant. Therapeutic lifestyle and dietary changes should be included in the initial attempt at lowering lipid levels, followed by statin therapy and the addition of ezetimibe.4,5 Dyslipidemia following liver transplant, however, appears to persist despite dietary modifications, making medication therapy often necessary.2,7
Statins are the most commonly used medication to manage dyslipidemia. Nonetheless, statin utilization has been shown to be low among liver transplant recipients with hyperlipidemia.8-10 In a retrospective study by Patel et al that evaluated the impact of coronary artery disease in liver transplantation, statin therapy utilization was low with only 46.8% of statin-eligible liver transplant recipients receiving therapy, which was well-tolerated with only 12% of patients having an adverse reaction, most notably muscle aches. 8 Glynn et al also demonstrated low statin utilization in liver transplant recipients with a diagnosis for hyperlipidemia at 36% with minimal adverse reactions observed (5.4%). 9 A meta-analysis of eleven studies, including the 2 previously mentioned, showed an overall statin utilization rate of 32% and an adverse effect rate of 14%. 10 Rationale for underutilization include the concerns for hepatotoxicity and elevations in hepatic transaminases, such as aspartate aminotransferase and alanine aminotransferase, which were not seen commonly in the previously mentioned studies. Moreover, survival benefit of statins post-liver transplant has been observed in multiples studies.8,10-14 In the multicenter NailNASH consortium, patients with liver transplant for non-alcoholic steatohepatitis had improved mortality with statin use (HR 0.38; 95% CI, 0.19-0.75; P = 0.005). 11 A Swiss Transplant Cohort Study of a prospective nationwide database of liver transplant recipients of various transplant indications found that treatment with statins post-transplant was associated with decreased mortality (HR 0.35; 95% CI 0.12-0.98; P = 0.047). 12 Given these observed benefits, optimizing statin therapy in liver transplant recipients should be prioritized.
Current literature, however, is limited by statin indication/qualification, statin intensity and tolerability differences, and specific barriers to statin initiation. This study aims to address these gaps by further characterization of the complication of post-liver transplant dyslipidemia, including assessment of ASCVD risk and immunosuppression implications, and evaluation of statin therapy, dose, intensity, tolerability, and barriers to initiation. The objective of this study is to evaluate the incidence of hyperlipidemia and statin qualification following liver transplantation and the clinical practice behaviors at a large academic medical center regarding statin utilization.
Materials and Methods
All adult patients ≥19 years of age who received a liver transplant between January 1, 2015 and June 30, 2019 at this academic medical center were reviewed for inclusion. Patients were included in analysis if they had a lipid panel within 15 months prior to transplant and a lipid panel within 15 months post-transplant. Multiorgan transplant recipients were excluded. The study was approved by the study center’s Institutional Review Board, which authorized a waiver of informed consent and conformed to the ethical guidelines of the 1975 Helsinki Declaration.
The electronic medical records of included patients were manually reviewed. Data were collected regarding baseline characteristics, cholesterol levels and ASCVD risk pre- and post-transplant, immunosuppressive medication regimens at the time of post-transplant lipid panels, and statin utilization and tolerability. Patient baseline characteristics included age, gender, race, native liver disease transplant indication, Model for End-stage Liver Disease (MELD)-Na at time of transplant, relevant comorbidities, and pre-transplant statin use. Included comorbidities were hypertension, obesity, hyperlipidemia, type 2 diabetes mellitus, coronary artery disease, and clinical ASCVD. Lipid panels were assessed pre- and post-transplant. The 10-year ASCVD risk scores were calculated utilizing lipid panels, blood pressure measurements, and comorbidities. Maintenance immunosuppression medications at the time of post-transplant lipid panel were collected. Based on this center’s steroid protocol, all patients receive a prednisone taper for at least 3 months following transplant. Post-transplant statin use, including statin choice, dose, intensity, tolerability, and barriers, was reviewed.
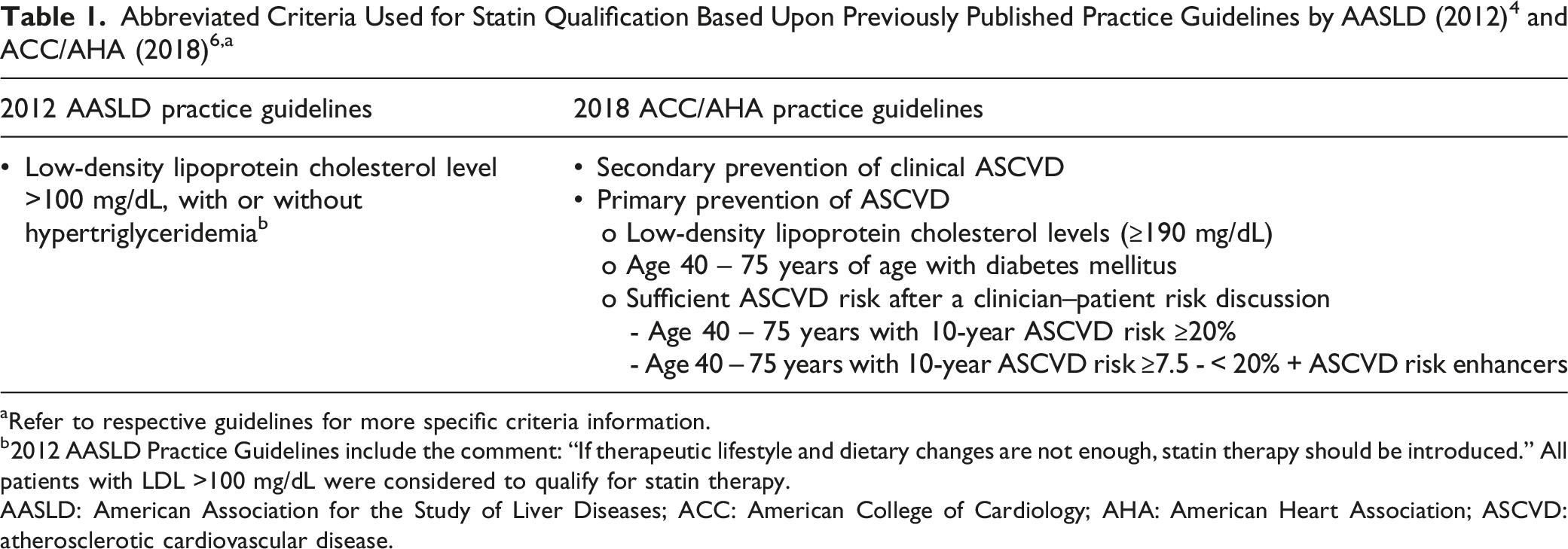
aRefer to respective guidelines for more specific criteria information.
b2012 AASLD Practice Guidelines include the comment: “If therapeutic lifestyle and dietary changes are not enough, statin therapy should be introduced.” All patients with LDL >100 mg/dL were considered to qualify for statin therapy.
AASLD: American Association for the Study of Liver Diseases; ACC: American College of Cardiology; AHA: American Heart Association; ASCVD: atherosclerotic cardiovascular disease.
Secondary outcomes included the incidence of statin qualification, hypertriglyceridemia, and severity of hypertriglyceridemia based upon immunosuppression at the time of lipid panel; statin use and tolerability; and barriers to statin initiation documented in the chart. Hypertriglyceridemia was defined as a serum triglyceride (TG) level greater than 150 mg/dL. Severity of hypertriglyceridemia was defined as follows: mild 150-199 mg/dL, moderate 200-499 mg/dL, and severe ≥500 mg/dL. For patients in whom a statin was initiated, tolerability was reviewed for 3 months post-initiation based upon documentation in the electronic medical record in either provider notes and/or lab results. Statin tolerability was assessed via statin discontinuation, muscle pain experienced with statin utilization, and safety monitoring of transaminases and creatine kinase (CK). In the case of elevation of transaminases or CK, patients were followed for an additional 3 months to observe the resolution or outcome of the safety event.
Descriptive statistics were used for baseline characteristics, immunosuppression at post-transplant lipid panels, and statin use and tolerability. Chi-square or Fisher’s exact test was utilized for analysis of hyperlipidemia, statin qualification, and hypertriglyceridemia outcomes as indicated. Chi-square and Fisher’s exact tests were calculated using GraphPad QuickCalcs Web site: https://www.graphpad.com/quickcalcs/contingency1/ (accessed June 2022).
Results
Baseline Characteristics for the Entire Cohort
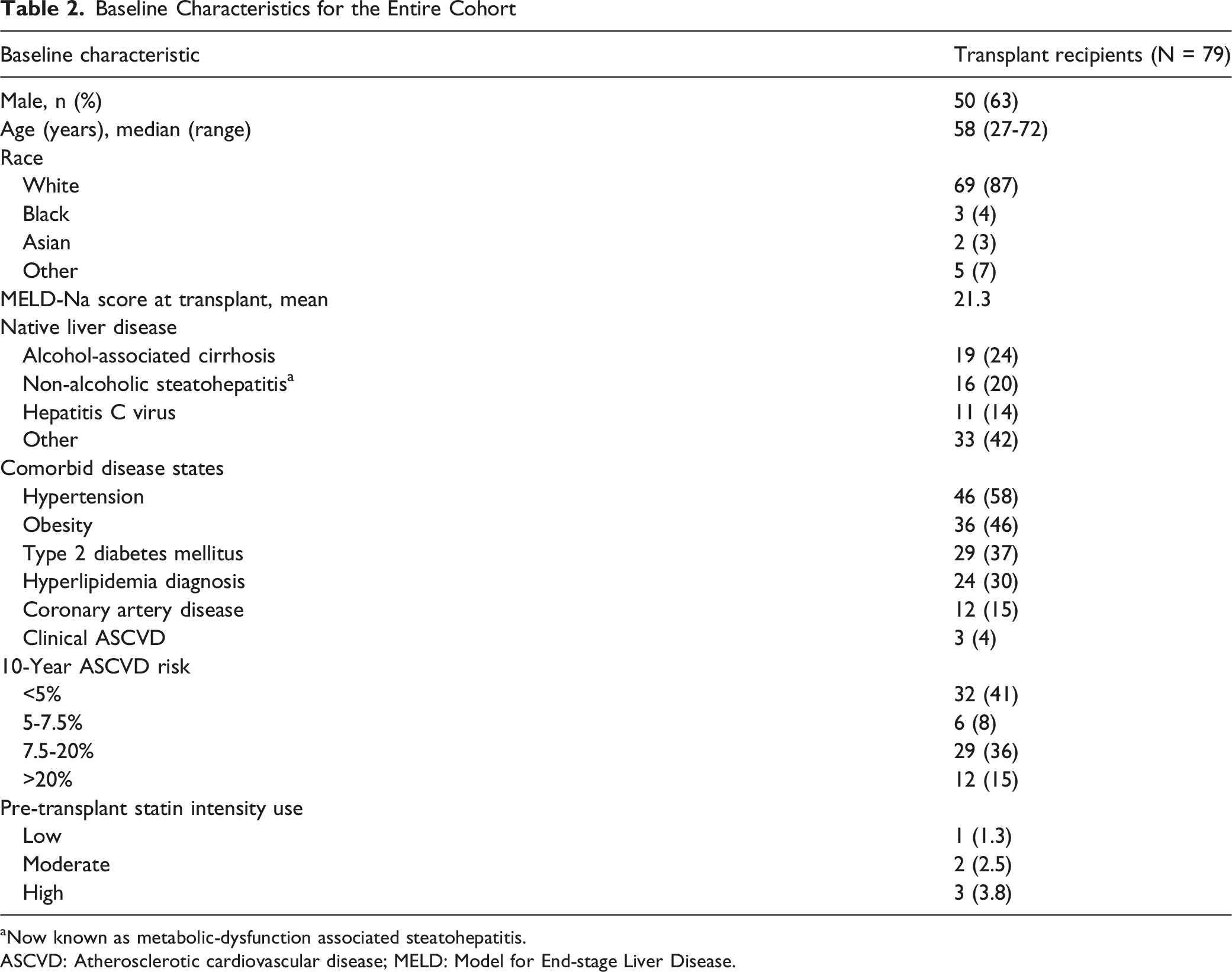
aNow known as metabolic-dysfunction associated steatohepatitis.
ASCVD: Atherosclerotic cardiovascular disease; MELD: Model for End-stage Liver Disease.
After transplant, the most commonly used immunosuppression at the time of the post-transplant lipid panel was tacrolimus (82%), followed by everolimus (16%) and sirolimus (1%). Prednisone use was identified in 42% of patients in addition to the tacrolimus or mammalian target of rapamycin (mTOR) inhibitor at the time of the lipid panel. The median time to first lipid panel post-transplant was 10 months.
Incidence of Hyperlipidemia and Hypertriglyceridemia Pre- and Post-transplant in the Entire Cohort

LDL: Low density lipoprotein; TG: triglyceride.
Statin qualification, determined utilizing 2012 AASLD and 2018 ACC/AHA guidelines, was significantly higher post-transplant compared to pre-transplant (46.8% vs 64.6%; P = 0.025). Breakdown of statin qualification by pre- and post-transplant rationale is shown in Figure 1. Pre- and post-liver transplant statin qualification (46.8% vs 64.6%, P = 0.025) including the breakdown of qualifying criteria according to 2012 American Association of the Study of Liver Disease (AASLD) and 2018 American College of Cardiology (ACC)/American Heart Association (AHA) practices guidelines. 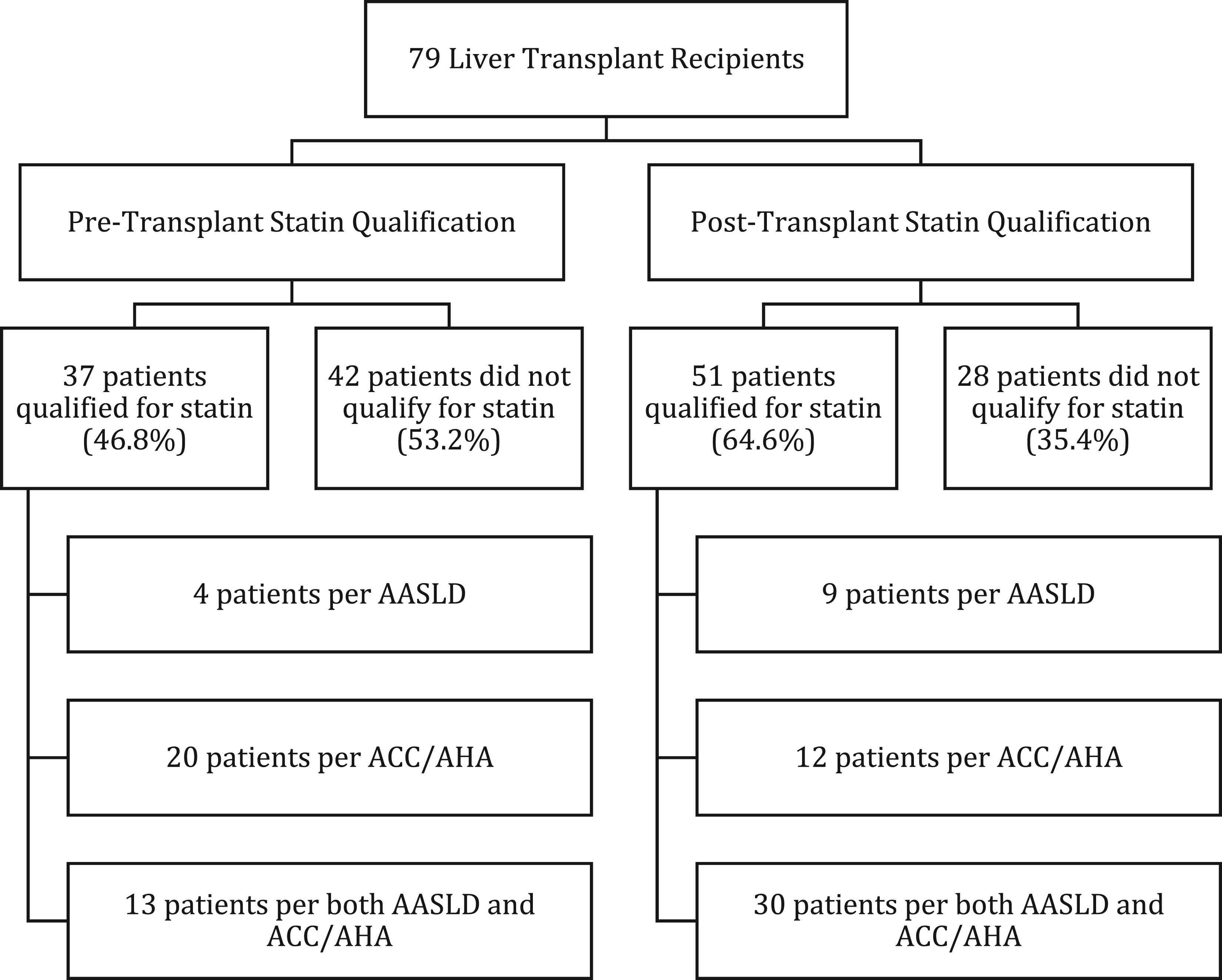
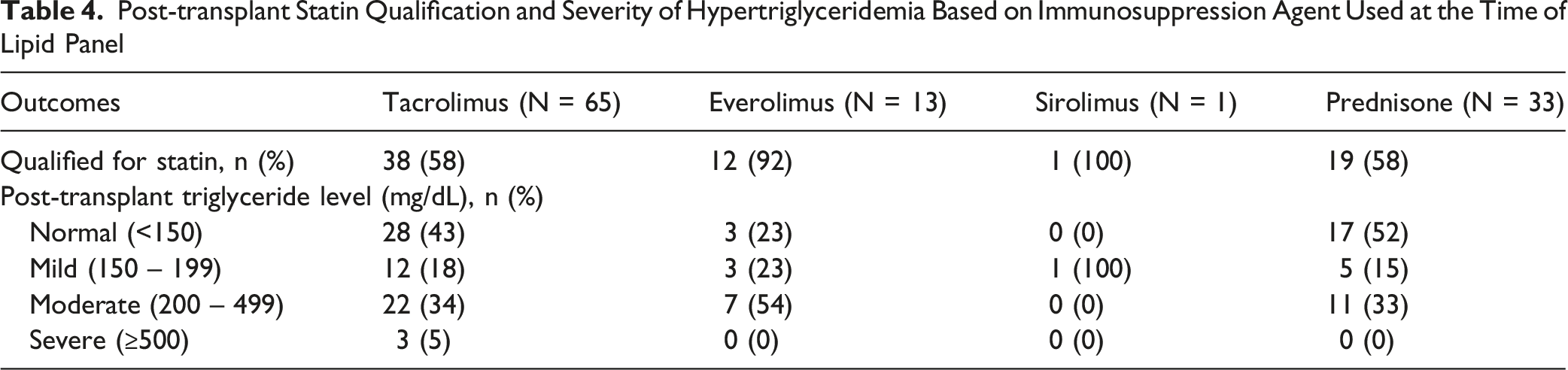
Post-transplant Statin Qualification and Severity of Hypertriglyceridemia Based on Immunosuppression Agent Used at the Time of Lipid Panel
In the fifty-one patients that qualified for statin therapy after transplant, twenty were initiated on a statin after the lipid panel resulted and 2 were continued on a statin from prior to transplant, resulting in 43% of statin-qualifying patients being on statin therapy. Of the twenty new statin initiations, the most commonly used statin was atorvastatin (55%), followed by simvastatin (40%) and rosuvastatin (5%). For atorvastatin, 7 were high intensity and 4 were moderate intensity. For simvastatin, 6 were moderate intensity and 2 were low intensity. The rosuvastatin used was moderate intensity. In total, for all newly initiated post-transplant statins, 35% received high-intensity, 55% received moderate-intensity, and 10% received low-intensity statin therapy.
Regarding statin therapy tolerability assessment, fourteen of the twenty patients started on statins had transaminases drawn after 2 to 4 weeks of therapy. Two patients had transaminases greater than 3 times the upper limit of normal. Both patients were taking simvastatin 40 mg daily and tacrolimus, one with prednisone and one without. In both cases, the transaminase elevations were not attributed to the statin, and statin therapy was continued. One patient who started statin therapy experienced muscle pains eliciting a CK level that showed an elevation from baseline but not greater than 3 times the upper limit of normal. This patient was taking atorvastatin 80 mg daily, and upon discontinuation of the statin, muscle aches resolved. Twenty-nine patients who qualified for statin therapy (57%) did not receive statin therapy during the study period. The reason for lack of statin therapy was undocumented in most patients (83%). Documented reasons included patient refusal (10%) and provider safety concern (7%).
Discussion
This study demonstrates that the incidences of hyperlipidemia and statin qualification significantly increased within 15 months following liver transplantation. Despite that increased need for medical management, the use of statin therapy remained suboptimal with a rate of 43% in statin-qualifying patients. This study is the first to evaluate the need for statin therapy based upon the 2012 AASLD and 2018 ACC/AHA guidelines. These data suggest that nearly two-thirds of liver transplant recipients may be candidates for statin therapy in the first-year post-transplant.
This rate of statin qualification at 1-year in this study is higher than what was seen in a previous study assessing statin qualification based upon 2018 ACC/AHA guidelines alone. Yen et al showed a rate of 47.5% for 1-year post-transplant for patients who had a statin indication for primary or secondary prevention of ASCVD. 15 Our study’s investigators, however, used a broader approach to statin qualification than Yen et al. Our study also included the 2012 AASLD liver transplant guidelines that recommended statin therapy for LDL level >100 mg/dL when lifestyle and diet changes were not enough. 4 The decision to include this qualifier was based upon the lack of response to lifestyle and diet modifications alone that is commonly seen in transplant recipients.2,7 Nonetheless, when assessing 2018 ACC/AHA qualification alone in our study, the rate was 53%, which is closer to the findings of Yen et al. It is worth noting the statin qualification rate increased to 59.6% by 5-year post-transplant in Yen et al’s study. 15 Knowing that the risk of cardiovascular disease will increase as time progresses post-transplant, using the broader criteria of both hyperlipidemia and ASCVD risk criteria to determine statin therapy may be prudent in order to optimize cholesterol in the early post-transplant period. This broader approach was highlighted in the more recent AASLD/AST guidelines, which recommend statin therapy for patients with LDL level ≥130 mg/dL regardless of risk factors. 5 Thus, use of both LDL level and ASCVD risk criteria should be considered post-transplant.
In this study, over half of liver transplant recipients qualified for statin therapy, but less than half of these patients were initiated on a statin. In the general population, statins have been shown to reduce cardiovascular disease through their lipid lowering effects, improvement of endothelial function, anti-inflammatory effects, pleiotropic effects, and anti-thrombotic effects.6,16-18 In liver disease, statins have those same beneficial effects for cardiovascular disease risk reduction, but they also have been shown to reduce portal pressure, improve hepatic endothelial and microvascular dysfunction, reduce fibrogenesis, protect against injury after shock, protect against ischemic injury, and reduce endotoxin-mediated liver damage. 16 In the liver transplant setting, a meta-analysis including 11 studies assessing statin use following liver transplant showed a significant mortality benefit with statin use (HR 0.282; 95% CI 0.154-0.517, P < 0.001). 10 The use of statins also decreased the odds of graft rejection (OR 0.33; 95% CI 0.15-0.83) and hepatocellular carcinoma recurrence (HR 0.32; 95% CI 0.11-0.89). 10 There is clear benefit to utilizing statin therapy in liver transplant recipients, such that Spiritos and Abdelmalek suggest that statins should be considered in all liver transplant patients independent of their lipid levels. 19 Nonetheless, despite the elevated incidences of hyperlipidemia and hypertriglyceridemia and increased cardiovascular risk in our cohort, overall statin utilization was low. Our statin utilization rate of 43% of statin-qualifying patients is similar to previous literature in post-liver transplant recipients with documented statin use of 24-47%.8-10,15 The fact that the majority of patients who qualified for statin therapy post-transplant were not started on statin therapy demonstrates a gap in practice. Though barriers to statin initiation were reviewed in this study, documentation of rationale for lack of statin therapy was only present in 5 instances (17%), including 3 patient refusals and 2 provider concerns. Although not explicitly noted in this study, provider hesitancy due to concern for hepatotoxicity, side effects, and drug-drug interactions may remain a key consideration. Like previous literature, the patients in our cohort had an overall low rate of muscle pain, CK elevations, or transaminase changes, which should help reduce that hesitancy.8-10,20 Another potential reason for low overall statin utilization could be lack of provider time and/or prioritization of statin therapy. Given the demonstrated low use of statins across multiple studies, opportunities for optimization of lipid management should be explored. One consideration is standardization of documenting reasons for not using statin therapy post-liver transplant, which would be helpful to prevent inadvertent missed therapy and provide clear rationale for therapy decisions. In light of our findings, our center developed a collaborative practice agreement between the transplant hepatologists and transplant pharmacists to help with review of lipid panels to better manage this complication. Having a standardized approach allows for enhanced emphasis on statin therapy and ensures that cardiovascular risk is assessed and managed appropriately.
Further optimization of statin selection may be necessary to ensure optimal care. Forty percent of patients who were started on statin therapy were initiated on simvastatin, which is more susceptible to drug-drug interactions with immunosuppression and adverse effects. 21 As previously mentioned, the recent 2025 AASLD/AST guideline recommend hydrophilic statins, such as rosuvastatin for high intensity and pravastatin for moderate intensity, as first line therapy post-liver transplant. 5 Neither of these statins were commonly seen in this study with only one patient receiving rosuvastatin. Choice of statin in this cohort was likely driven primarily by provider experience with each agent. In order to better align with updated guidelines, our center has developed a decision tree diagram to help direct providers to prescribe the recommended statin. This decision tree is also part of the collaborative practice agreement.
Baseline characteristics and immunosuppression may have impacted some of these findings as well. Metabolic syndrome is a known complication occurring in up to half of all patients post-liver transplant that elevates risk for cardiovascular disease.22,23 The prevalence of diabetes pre-transplant is generally around 15% and increases to up to 30-40% post-transplant due to risk factors including use of corticosteroids, calcineurin inhibitors, and mTOR inhibitors. 22 In our cohort, there was a higher rate of diabetes prior to transplant (37%) compared to the aforementioned study. This increased rate of diabetes subsequently increased the rate of statin qualification as it is a risk factor for ASCVD. 6 A potential reason for this increased prevalence is selection bias given inclusion criteria for this study required lipid panels and patients with diabetes may have a more compelling indication to assess cardiovascular risk. Considering immunosuppression, the majority of patients in this cohort were on tacrolimus at the time of the lipid panel (82%). Tacrolimus has been associated with increased rates of new-onset diabetes after transplant, which would only augment the cardiovascular risk. 24 Everolimus was used in 16% of patients, and it is well documented that everolimus increases the risk of developing hyperlipidemia and hypertriglyceridemia.25,26 Zimmermann et al compared calcineurin inhibitors-only containing regimens to mTOR-containing regimens in 92 adult liver transplant patients and found that mTOR inhibitor-containing regimens were at a higher risk of dyslipidemia, with increased LDL (9% vs 35.7%; P = 0.016) and TG (32.1% vs 92.9%; P = 0.0001).27 Our study was consistent with these concerns with 93% of patients on an mTOR inhibitor qualifying for statin therapy and 79% demonstrating hypertriglyceridemia, compared to 58% and 57% of patients on tacrolimus; respectively. Lastly, our study evaluated the rate of hyperlipidemia and statin qualification within 15 months of liver transplant, which would be the time frame when corticosteroid use would occur more frequently. All patients receive at least 3 months of prednisone post-transplant, and 42% of patients were still on prednisone at the time of the post-transplant lipid panel. The recent corticosteroid exposure may have contributed to the overall high rate of hyperlipidemia seen in this cohort.
This study has several limitations that must be addressed. The overall sample size was relatively small, but despite that, a statistically significant difference was seen in hyperlipidemia, hypertriglyceridemia, and statin qualification. The retrospective nature of this study demonstrated substantial missing data and lack of standardization regarding lipid monitoring and statin prescribing. Because AASLD guidelines recommend annual lipid panels in liver transplant patients, the time frame of 15 months was selected in which a lipid panel was to be drawn pre- and post-transplant to allow for 3-month delays in lab monitoring. This time frame led to exclusion of 203 patients, which has potential implications for interpretation of the study results and clinical practice behaviors. First, the exclusion of so many patients due to missing lipid panels clearly shows an opportunity for better alignment with clinical practice guidelines regarding annual screening for hyperlipidemia. It is, however, worth mentioning that patients who were monitored through their primary care providers may have had lipid panels that were not accessible through our electronic medical record, resulting in exclusion from this study. Nonetheless, use of standardized order sets and clinical decision support in the electronic medical record are potential ways to improve adherence to guideline recommendations. When interpreting this study in light of the missing data, selection bias must be considered as lipid panels may have been ordered for cause rather than routine screening or only in high-risk individuals as deemed by the provider. Another limitation to this study is the variability of the timing of lipid panels in relation to transplant, which would affect the level of immunosuppression exposure, potentially impacting outcomes. Use of a specified time frame pre- and post-transplant may mitigate this confounder to some extent but does not eliminate it. This study specifically looked at early outcomes for hyperlipidemia, statin qualification, and statin use when caution or hesitation may be heightened. Providers may become more comfortable prescribing statin therapy as the time from liver transplant increases. 15 Thus, longer-term follow-up may provide additional insight of overall cardiovascular risk and long-term statin use in this patient population.
In summary, while the meta-analysis from Ho and colleagues has shown this underutilization despite potential benefit and safety of statin therapy post-liver transplant, our study adds to that data in multiple ways. 10 First, our study highlights that evaluation of lipid panels may be underutilized in the early post-transplant period. Given the high overall prevalence of statin qualification, identification of the potential medical need is crucial for the ability to intervene. Optimizing monitoring of lipid panels should be an area of priority post-liver transplant. Second, our study emphasizes that identification alone does not address the issue entirely as statins were often not initiated in the patients who qualified. In addition, the choice of statin therapy post-transplant is another area of improvement identified, demonstrating the need for increased use of hydrophilic statins, such as rosuvastatin and pravastatin. From these study findings, our center was able to develop practical interventions, including a collaborative practice agreement, to align clinical practice with published guidelines. Furthermore, our study also was able to describe statin qualification rates among immunosuppression medications that were not addressed in the meta-analysis. This study provides pharmacists with additional evidence to help implement changes that could enhance the cardiovascular health of liver transplant recipients.
Conclusion
Nearly two-thirds of liver transplant recipients qualified for statin therapy post-transplant based upon 2012 AASLD and 2018 ACC/AHA guidelines. Despite increased rates of dyslipidemia and statin qualification post-liver transplant, statin therapy was underutilized. Optimization of lipid management remains an area of need post-liver transplant. Post-transplant lipid panel monitoring and statin initiation protocol implementation may be useful in mitigating the cardiovascular risk in liver transplant recipients. Further studies are warranted to confirm these findings.
Footnotes
Author Note
This original research was accepted as an abstract for poster presentation at the 2023 American Transplant Congress (the joint annual meeting of the American Society of Transplantation and the American Society of Transplant Surgeons).
Ethical Consideration
The study was approved by the Nebraska Medicine Institutional Review Board, which authorized a waiver of informed consent, and conformed to the ethical guidelines of the 1975 Helsinki Declaration. The approved IRB protocol was #0740-21-EP.
Consent to Participate
A waiver of informed consent was granted by the Nebraska Medicine Institutional Review Board.
Author Contributions
Dr. Blocker contributed to the design of the study, acquisition of data, analysis of data, and drafting of the article. Dr. Henry contributed to the performance of the research, analysis of the data, and revising of the article intellectual content. Dr. Leick contributed to the design of the study, the performance of the research, analysis of the data, and the writing and revising of the article for intellectual content.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Mary Leick is a Specialty Topic Editor for DynaMed. The remaining authors declared no potential conflicts of interest with the research, authorship, and/or publication of this article.