
Abstract
Sucralfate is a medication that is a chemical complex consisting of aluminum hydroxide and sulfated sucrose. It has been found to cause malabsorption of many different medications, including warfarin, by chelating the drugs within the gastrointestinal (GI) lumen. To minimize potential malabsorption interactions, it is recommended that there be at least a two-hour separation between administration of sucralfate and the second drug. This case report involved a hospitalized patient who was also monitored once discharged, then rechallenged and de-challenged with low dose sucralfate at doses of only 1 gram once daily or 1g twice daily. The case showed that warfarin requirements approximately doubled when the drugs were used concomitantly vs warfarin alone. When the medications were given in the first hospitalization, once daily sucralfate was given at 0900 and warfarin at 2100. Thus, even though the drugs were being separated by about 12 hours, it appears the interaction still manifested. When sucralfate was increased to twice daily in the second hospitalization, it was dosed at 0900 and 2100. Of course, warfarin was also given at 2100 each day for the second admission. Around both hospitalizations, the challenge with sucralfate resulted in subtherapeutic warfarin levels, thereby necessitating dose escalation well above “pre-sucralfate” doses to achieve International Normalized Ratios (INRs) in the therapeutic range of 2-3 for this patient. Also, around both hospitalizations, de-challenge of sucralfate resulted in INRs becoming supratherapeutic in just 2-3 days, yielding INRs of 8.1 after the first discharge and 5.4 after the second discharge.
Introduction
Sucralfate is a chemical complex made of aluminum hydroxide with sulfated sucrose. 1 It works with gastric acid to form a viscous polymer matrix that adheres to the gastrointestinal tract (GIT) mucosal barrier. It then elicits several different actions that lead to its ability to prevent mucosal injury, reduce inflammation, and heal existing ulcers. 2 Since it contains about 18% aluminum and binds to the mucosal epithelium, it has the potential to chelate and reduce absorption of other drugs within the GI lumen. These intraluminal drug-drug interactions may be caused by alterations in drug absorption, adsorption, or influencing the drug dissolution due to pH changes in the GIT. 2
Warfarin achieves its anticoagulant effect by inhibiting the activation of vitamin K-dependent clotting factors. 3 Although it is no longer commonly used as a first line anticoagulant in venous thromboembolism because of the emergence of the newer direct oral anticoagulants (DOACs), warfarin may still be used in individuals with valvular atrial fibrillation, those with contraindications for DOACs, or those who cannot afford DOACs. The potential for warfarin to interact with other medications and food is widely recognized. Although the literature is sparse, previous case reports have demonstrated a potential drug-drug interaction between warfarin and sucralfate. 4 This report aims to highlight the significance of the drug-drug interaction between these 2 agents.
Case Report
A 34-year-old-female presented to the hospital for a workup for a low hemoglobin. She had a past medical history of heart failure with preserved ejection fraction, pulmonary hypertension, hypertension, end-stage-renal disease, and mechanical aortic and mitral valve replacements, for which she was on warfarin. Her medication list prior to admission included aspirin, atorvastatin, calcium acetate, cinacalcet, diltiazem, docusate, gabapentin, hydralazine, levothyroxine, metoprolol tartrate, oxycodone, pantoprazole, quetiapine, sacubitril-valsartan, tizanidine, and warfarin. Of note, although the patient was on pantoprazole 40 mg once daily at home, a hospital policy-driven therapeutic interchange put them on omeprazole 20 mg once daily while inpatient.
On admission, her hemoglobin was 5.7 g/dL, and her INR was 3.1. Her warfarin was held. Given her history of mechanical valve replacements, she was placed on IV heparin infusion during her hospitalization. The source of her anemia was determined to be hemolysis secondary to a paravalvular leak of the mitral valve. The patient continued the omeprazole 20 mg daily and was also started on sucralfate 1 gram once daily at 0900. All other home medications were continued during admission.
Once her hemoglobin was stable, warfarin was restarted at 10 mg daily. Per hospital policy, warfarin was given routinely at 2100 daily. Thus, warfarin and sucralfate doses were separated by about 12 hours. The patient’s warfarin dose prior to admission was 10 mg every Tuesday and Thursday and 5 mg the rest of the days of the week, and her INR was previously therapeutic on this regimen. Although the patient was continued on warfarin at doses of at least 10 mg daily, which was higher than her previous home dose, she remained subtherapeutic for several days (see Figure 1). Given the escalating doses of warfarin with subtherapeutic INR, sucralfate was discontinued. The patient was discharged on warfarin 12.5 mg daily on day 16 with no sucralfate. Two days later, her INR was 8.1. She denied any new interacting medications or changes to diet. No Vit K- containing reversal agents were given due to lack of bleeding, but the patient was instructed to hold warfarin and eat additional servings of vegetables containing vitamin K. After holding several doses of warfarin, care notes indicated that she was instructed to restart at a dose of 5 mg PO daily when her INR was 1.4. INR response and warfarin dose requirements during periods of concomitant sucralfate therapy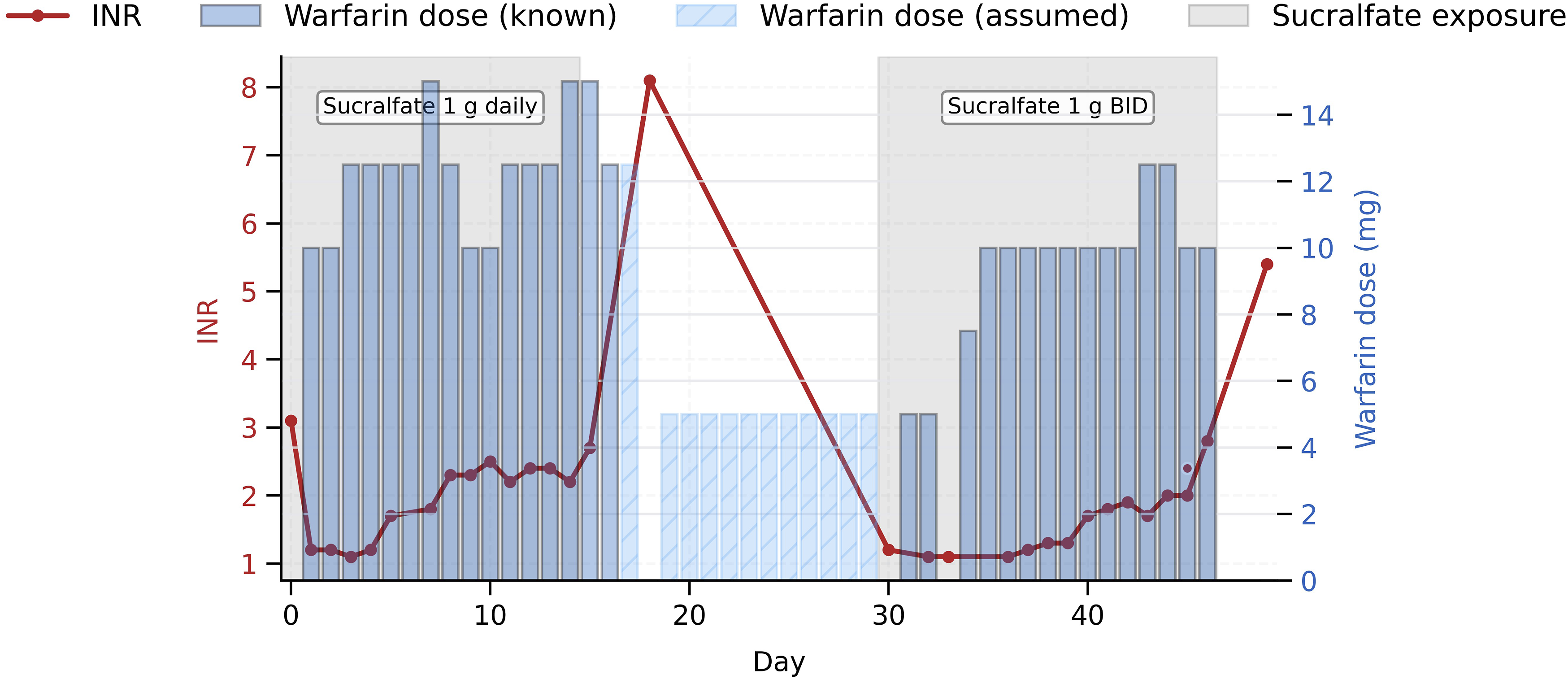
Unfortunately, 14 days after the last discharge, the patient was re-admitted to the hospital because of fatigue and a low hemoglobin of 6.9 g/dL. Her INR was only 1.2 on admission, and it was verified that no reversal agents had been given. The patient continued all of her current home drugs and doses, and the omeprazole and was again substituted for the pantoprazole. Once again, she was also started on sucralfate, but this time at a dose of 1 gram twice daily at 0900 and 2100. During this admission on sucralfate, warfarin was restarted in the second hospital day, but her INR continued to be subtherapeutic even while kept on 10 mg daily for 8 consecutive days. (see Figure 1). Higher-than- home-dosing of warfarin was required to achieve a therapeutic INR.
In response to the sluggish INR response on 10 mg daily while in hospital and on sucralfate, the patient was discharged without sucralfate and put on warfarin 12.5 mg Monday and Friday and 10 mg the rest of the days of the week. Three days later, her INR was 5.4. Warfarin was held and the patient was again instructed to eat vegetables containing vitamin K. Once in therapeutic range, she restarted on warfarin 7.5 mg daily. Afterwards, the patient achieved therapeutic range on this dose and was maintained on this regimen.
Discussion
This case highlights an important interaction between sucralfate and warfarin. It was manifested in both admissions as she required higher-than- home-dosing of warfarin while being administered concomitant sucralfate. In the first admission, sucralfate was separated from warfarin by about 12 hours. In the second admission, the 2 medications were given together at night. In either case, there was a significant blunting of the warfarin response when sucralfate was on, and a significant potentiation of the warfarin shortly after the sucralfate was stopped.
Case reports of the interaction between sucralfate and warfarin have been previously reported.4-6 The authors proposed that sucralfate acts similarly to cholestyramine to prevent absorption of warfarin. Interestingly, in the aforementioned case, the patient received warfarin 5 hours after sucralfate dosing. 1 Drug interactions with sucralfate are thought to be due to the drug forming a strong GIT mucosal barrier while impeding the absorption and reducing bioavailability of many other oral medications. However, it has often been said that these drug-drug interactions could be mitigated by administering these agents at least 2 hours apart from sucralfate.
In our case, warfarin was administered about 12 hours from warfarin on the first admission. This suggests that the interaction between sucralfate and warfarin goes well beyond the two-hour separation window. One possible explanation for this prolonged malabsorption effect is the enterohepatic recycling process, whereby the chelating component of the sucralfate sequesters warfarin and its active congeners through more than one pass through the intestinal tract. For the second admission, we confirmed that the second daily dose of sucralfate was given along with warfarin at 2100. While the patient was on numerous other medications, both the medications and the doses used remained stable throughout the observation period. Furthermore, we could find no evidence that any of these other medications, including the concomitant proton pump inhibitor changes, could have elicited an interaction with warfarin that may have contributed to these observed changes.
Of course, there is an often-cross-referenced interaction between warfarin and proton pump inhibitors (PPIs). Much of the attention is because omeprazole is indeed a moderate inhibitor of CYP 2C19, the enzyme that metabolizes the less potent R-warfarin isomer. Pantoprazole also has this characteristic, but to a lesser degree than omeprazole. 7 However, we found 3 studies in humans that concluded while omeprazole increased the plasma concentration R-isomer of warfarin to a small degree, the increases did not significantly alter coagulation times, as thus were not clinically significant.8-10 Meanwhile, 2 studies with pantoprazole reached the same conclusion.10,11
A prospective cross-over study was done in 8 patients on long-term warfarin therapy. 12 The study consisted of a 1-week control phase and a 2-week sucralfate-warfarin phase. It was followed by a 1-week control phase. The dosing of sucralfate used in this study was 1 gram administered 3 times daily, with the last dose being given at the same time as warfarin. Warfarin dosing was not changed throughout the study period. The study found no significant difference in warfarin concentrations or thromboplastin times during the study phases. Some have theorized the difference in these interactions may be accounted for during the initiation phase of warfarin therapy. 5 This concept may also explain the reasoning behind the drug-drug interaction during both of the patient’s hospitalizations given warfarin had been held and reinitiated while the INR was subtherapeutic.
The Drug Interaction Probability Scale
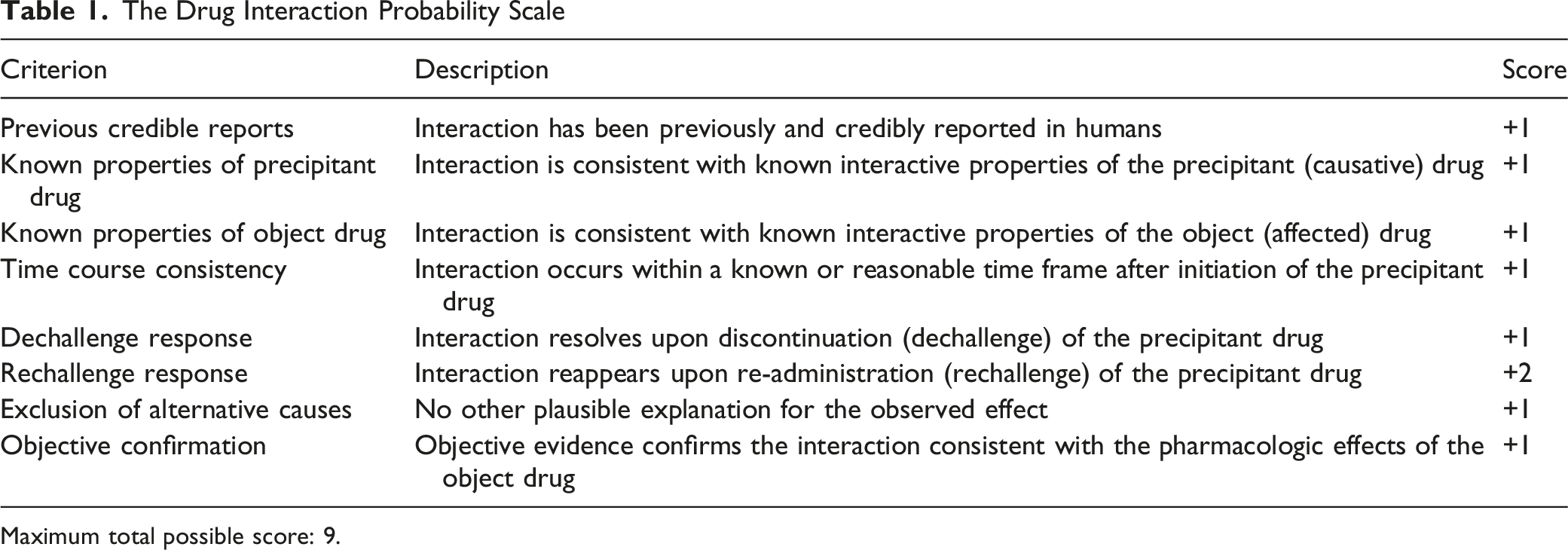
Maximum total possible score: 9.
From a polypharmacy standpoint, this drug-drug interaction could have been avoided altogether. For GI bleeds, although the sucralfate-PPI combination is sometimes recommended, 14 there are no well controlled studies that demonstrate that addition of sucralfate to a PPI is clinically beneficial. Also, in theory, gastric acid is needed to “activate” ingested sucralfate into its viscous coating polymer; and, with a PPI on board, gastric pH is often at or above a pH of 4.2,15,16 Furthermore, in addition to the possibility of sucralfate causing malabsorption of other drugs taken by a patient, its high aluminum content results in it often being associated with constipation. If sucralfate is used long term, aluminum accumulation within bone and brain tissues have been thought to potentiate osteomalacia and various CNS abnormalities, especially in patients with renal impairment.17,18
This case demonstrates a highly probable drug-drug interaction between sucralfate and warfarin. It also serves as a reminder of the importance of close therapeutic drug monitoring for those on this combination. Furthermore, if a patient is taking daily warfarin and in need of some form of anti-ulcer therapy, the two-hour spacing may not be sufficient to mitigate the interaction, and sucralfate should best be avoided in lieu of other alternatives such as PPIs or H-2 receptor antagonists.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.