
Abstract
With the aging population, symptomatic chronic subdural hematoma (CSDH) is becoming increasingly prevalent in neurosurgical practice. While burr-hole drainage remains the mainstay treatment, the optimal drilling site remains controversial. This single-center, randomized controlled noninferiority trial aimed to compare frontal versus parietal burr-hole approaches in patients aged ≥18 years requiring surgical drainage for CSDH. Participants were randomized (1:1) via computer-generated allocation to frontal or parietal burr-hole groups, with blinding maintained for patients and staff except operating neurosurgeons. All patients received postoperative atorvastatin combination therapy. Primary outcomes included 6-month recurrence rates (noninferiority margin: 5.0%), with secondary outcomes assessing functional status (modified Rankin Scale [mRS] 4–6), mortality, and complications. From July 2020 to December 2022, 135 of 147 screened patients (92%) were enrolled (frontal: n = 67; parietal: n = 68), comprising 79% males (n = 107) and 21% females (n = 28). At 6-month follow-up (completed June 2023), recurrence rates were 1.5% (1/67) in the frontal group versus 4.4% (3/68) in the parietal group (difference: −2.9%; 95% confidence interval [CI]: −8.6 to 2.8; p = 0.31), meeting noninferiority criteria. Functional outcomes (mRS 4–6: 3.0% vs. 4.4%, p = 0.66) and mortality (3.0% vs. 1.5%, p = 0.55) showed no significant intergroup differences. Notably, postoperative pneumocephalus volume was significantly lower in the frontal group (11.6 ± 14.8 mL vs. 20.7 ± 20.4 mL; p = 0.038). Adverse event rates were comparable between groups, with pneumonia being most frequent (53.7% vs. 55.9%) and surgical complications similarly distributed (6.0% vs. 5.9%). These findings establish noninferiority of frontal burr-hole while demonstrating reduced postoperative pneumocephalus, supporting its clinical preference and warranting future superiority trials. (Trial registration: chictr.org.cn, ChiCTR2000033967).
Introduction
Chronic subdural hematoma (CSDH) is a prevalent neurological condition among the elderly, with an annual incidence rate of 80.1 per 100,000 individuals aged 65 years and above. 1 Due to a higher frequency of anticoagulant therapy, brain atrophy, and an elevated risk of head trauma resulting from falls, individuals aged over 65 are particularly vulnerable to CSDH. 2 Data from the Nordic countries and the U.S. reveal a startling trend: over the past 20–30 years, the incidence of a particular condition has nearly tripled, and the number of surgeries performed to address it has doubled.3,4 As China has the largest elderly population in the world, neurosurgeons in the country face a significant challenge in optimizing the treatment benefits for patients with CSDHs. 5 This requires careful consideration of various factors to ensure the best possible outcomes for these patients.
The primary treatment method for symptomatic patients is surgical evacuation of the subdural hematomas. Burr hole craniostomy demonstrated the most advantageous recurrence rate and an acceptable frequency of complications in the management of symptomatic CSDH relative to alternative surgical interventions. 6 However, the hematoma reoccurs in 10–20% of individuals who have undergone surgical intervention. 7 In order to further reduce the recurrence rate, neurosurgery colleagues around the world have conducted many clinical trials involving the number of burr holes, the location of the drainage tube, whether to irrigate, and the temperature of the irrigate fluid, etc.4,8–12 These attempts have contributed to the improvement of surgical results. Nevertheless, no studies have focused on the burr-hole site, and the efficacy of different burr-hole sites has never been tested in a randomized controlled trial (RCT).
Intracranial pneumocephalus constitutes a risk factor for the recurrence of postoperative hematoma in individuals with CSDH.13,14 In our extensive experience with the surgical management of CSDH, we have frequently seen that postoperative intracranial pneumocephalus mostly accumulates in the frontal area. Prior research indicates that positioning the drain point in the frontal area diminishes the occurrence of postoperative intracranial pneumatosis, hence lowering the rate of hematoma recurrence; however, some studies have reported that no such differences were found.15,16
Based on this, we believe that frontal burr-hole should theoretically be noninferior to parietal burr-hole in patients with CSDH. To test the therapeutic efficacy of frontal burr-hole, we conducted a study comparing frontal burr-hole with parietal burr-hole for drainage in adult patients with symptomatic CSDHs. We hypothesized that frontal burr-hole drainage would not be inferior to parietal burr-hole drainage in terms of efficacy and safety at 6 months after surgery.
Methods
Ethics and approvals
The study was approved by the Medical Ethics Committee of Nanhua University. The study was registered in the Chinese Clinical Trial Register (ChiCTR2000033967) prior to data collection. Reporting is consistent with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Patient
Patient recruitment period was from July 1, 2020 to December 31, 2022. Patients with symptomatic unilateral or bilateral supratentorial CSDH confirmed by cranial computed tomography (CT), aged 18 years or older and ineffective drug treatment, are considered for enrolment. We managed individuals with bilateral hematomas as a single patient, administering the same therapy to both sides.
We excluded patients necessitating surgical interventions beyond burr-hole evacuation, those with cerebrospinal fluid shunts, individuals with a history of intracranial surgery, patients in a comatose state, those unable to cooperate for subdural drain utilization, individuals treated for hematological malignancies within the preceding 5 years, patients with CNS malignancies influencing symptoms or surgical outcomes, those with acute infections, or individuals combined with severe cardiopulmonary dysfunction or coagulation dysfunction or severe liver and kidney damage.
Randomization and blinding
Eligible patients were randomly allocated to either frontal burr hole drainage surgery or parietal burr hole drainage surgery in a 1:1 ratio utilizing a random number table approach. The randomly generated allocation sequence is successively placed into coded, sealed opaque envelopes, which are retained by nonparticipants and unsealed upon the patient’s signing of the informed consent form to partake in the clinical experiment. The group assignment was only known to the doctor performing and the staff in the operating room. Patients and all other medical staff were not told about the treatment assignment. The surgeons who performed the initial surgeries were directed to refrain from involvement in subsequent patient care, including decisions regarding reoperation. Outcome assessors remained blinded during follow-up assessments (1-month, 3-month, and 6-month) by restricting access to treatment-related records; evaluations relied on standardized imaging reviews (CT/MRI) and symptom checklists without intervention details. Statisticians analyzed datasets coded as “Group A” and “Group B,” with the randomization key securely stored and revealed only after primary analysis. An emergency unblinding protocol (sealed envelopes managed by an independent committee) was established but not utilized.
Procedures
We usually performed the procedure under local anesthesia, unless the patient was unable to cooperate or tolerate it, before considering general anesthesia. A standard burr hole was drilled in the frontal or parietal region at the maximum extent of the hematoma (Supplementary Data), according to the assigned treatment group, followed by successive incision of the dura and capsule of the hematoma cavity. In each group, the hematoma cavity was irrigated in all directions with saline at body temperature (37°C). A minimum of 200 mL irrigation fluid was mandatorily administered in all cases, with additional irrigation continuing until the neurosurgeon deemed the exudate to be clear. Subsequently, a closed-system silicone drain (12 Fr) was uniformly positioned in the hematoma cavity. The drain was linked to a passive drainage bag for a duration of 48 to 72 h. All operators followed the standardized protocol described above to minimize operator-dependent variability. Bed rest was advised till the removal of the drainage catheter. Following the surgical procedure, the patient was administered 20 mg of atorvastatin calcium tablets (Pfizer Pharmaceuticals Ltd.) on a nightly basis with the objective of facilitating the resorption of the residual hematoma. 17 A CT scan of the head was performed on patients 24 h after surgery, following extubation and prior to discharge. Subsequent follow-up was conducted at the neurosurgery clinic 1 month postoperatively. Telephone follow-up was performed at 3 and 6 months postoperatively.
Outcomes
The main effectiveness outcome measure was the occurrence of reoperation for a symptomatic, recurring CSDH on the ipsilateral side within 6 months following the original surgery. The determination to perform a reoperation was made by the attending neurosurgeon on the basis of the imaging evidence of a recurrent CSDH and the symptoms resulting from the CSDH.
Secondary outcomes included functional outcomes at 1-, 3-, and 6-month intervals, as measured by the modified Rankin Scale (mRS; which ranges from 0 [asymptomatic] to 6 [death], with a favorable functional outcome indicated by an mRS score of 0–3 and an unfavorable functional outcome indicated by an mRS score of 4–6); 6-month all-cause mortality and the occurrence of relevant postoperative complications during the in-hospital period. Furthermore, imaging features such as hematoma thickness, hematoma volume, midline shift, postoperative pneumocephalus, and postoperative residual hematoma volume will be recorded. The measurement methods for hematomas and intracranial pneumocephalus are as follows: Perform axial thin-slice (0.5 mm) head CT scans on patients. Import the Digital Imaging and Communications in Medicine-formatted CT images into 3D Slicer software (v.5.0.3) for image processing. Use 3D hematoma volume reconstruction to outline and automatically measure the hematoma volume. Similarly, outline the postoperative pneumocephalus to directly obtain its volume. In addition, as long as intracranial pneumatosis is detected in postoperative CT, regardless of its amount, we define it as the presence of pneumocephalus and record its volume. The evaluation of the mRS Score was performed by qualified researchers who were blinded to group assignment, following a standardized procedure.
Statistical analysis
We estimated the sample size based on a review of CSDHs, assuming a reoperation rate (i.e., primary outcome) of 15%, and also based on a study from an RCT in Japan that included 135 patients with CSDH, assuming a frontal burr-hole reoperation rate of 5%.15,18 We set a noninferiority cutoff value of 5% based on the design of previous clinical studies, which were supposed to have a recurrence rate of less than 20%. 19 Therefore, based on the above conditions, and assuming a nonadherence rate of 10.0%, we set the original sample size at 130 patients in order to achieve 80% validity and a 2.5% one-sided significance level to establish noninferiority.
SPSS (version 22, IBM Corp. New York, USA) and R (version 4.3.1) software were used for statistical analysis. The independent t-test was employed to statistically test for group differences in continuous data with a normal distribution. The Mann–Whitney U-test was employed to analyze data that did not follow a normal distribution. The Fisher exact test or Chi-square tests were employed to analyze categorical variables. Statistical significance was defined as a p value of less than 0.05.
Results
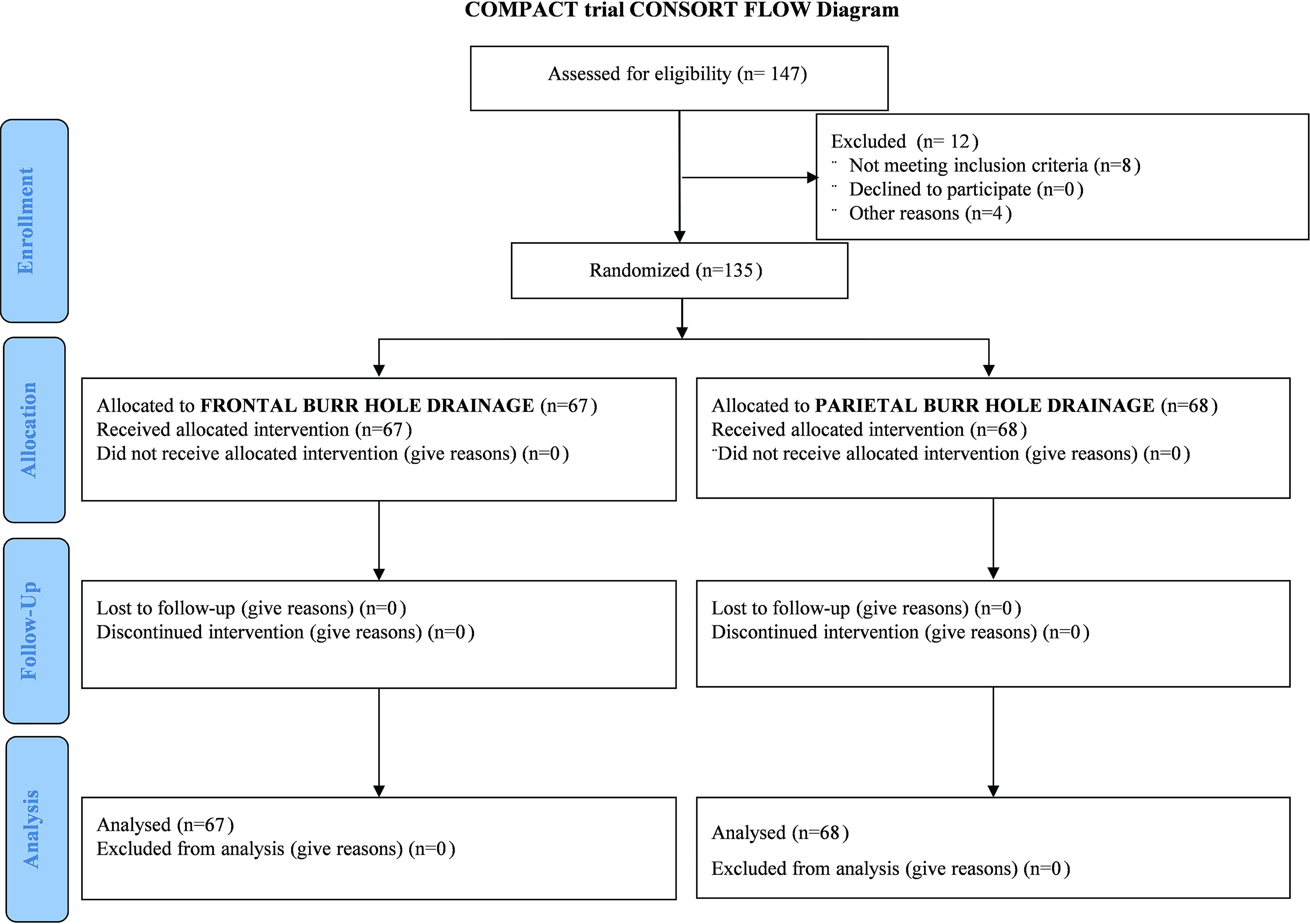
Between January 1, 2020 and December 31, 2022, 147 patients were evaluated for eligibility, of which 135 (92%) were randomly allocated to a therapy group and received treatment (Fig. 1). The 6-month follow-up period was extended till June 30, 2023. Sixty-seven patients were assigned to receive frontal burr hole drainage, and 68 patients were assigned to receive parietal burr hole drainage. No data were missing for the main outcome. The mRS at 1, 3, and 6 months postoperatively was available for 135 patients, and similarly mortality data were available for all patients.
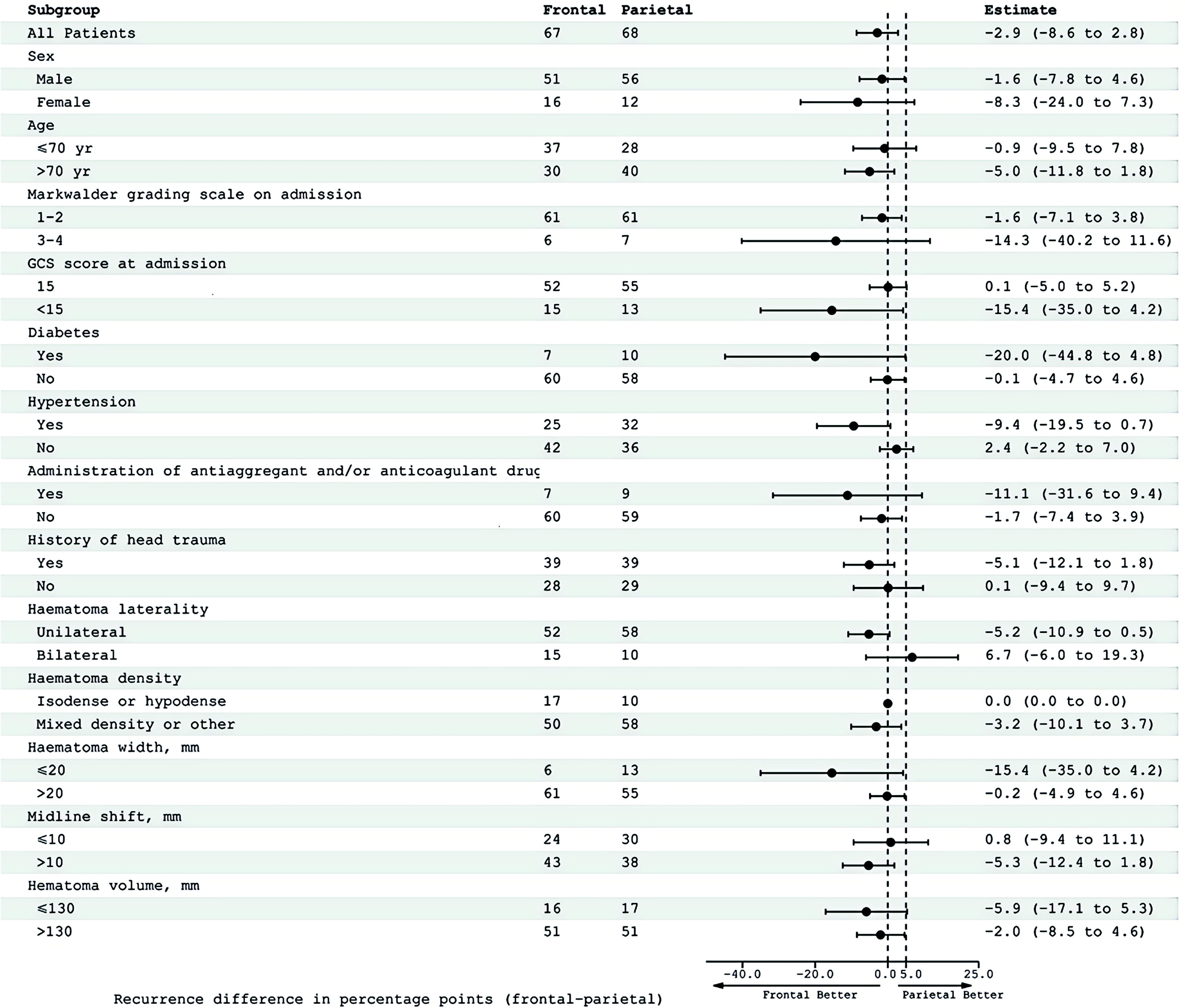
Percentage-point differences in recurrence at 6 months. Differences are calculated as the percentage in the frontal group minus the percentage in the parietal group.
In terms of baseline characteristics (Table 1) and perioperative features (Table 2), the groups were evenly distributed among themselves. The mean age of the participants was 70.0 years (SD 9.3). Of the 135 patients, 28 (21%) were female and 107 (79%) were male. Forty-seven (35%) patients with a mRS score of 1–3 and 107 (79%) patients with a Glasgow Coma Scale score of 15 on admission. Seventy-eight (58%) patients had a recorded history of head trauma, 16 (12%) had a history of anticoagulant or antiplatelet treatment, and 25 (18.5%) of the 135 patients with accessible scans had bilateral hematomas on preoperative imaging. One hundred and twenty-six (93%) of the 135 patients underwent a unilateral operation, and 110 (81%) got local anesthetic. There were 61 patients with drainage tubes left in place for 1 day, 64 people with drainage tubes left in place for 2 days, and 10 people with drainage tubes left in place for 3 days.
Baseline Characteristics
Patients could have more than one comorbidity.
Patients with cardiovascular diseases other than hypertension such as coronary atherosclerotic heart disease, arrhythmia, and heart failure.
Patients could have more than one symptom.
Patients could have a hematoma that was not operated on.
Sum of left and right hematoma volume.
Sum of left and right hematoma widths.
GCS, Glasgow Coma Scale; mRS, modified Rankin Scale.
Perioperative Details
A total of 4 patients (3.0%) out of 135 required reoperation within 6 months following the original surgery. The proportion of patients who underwent reoperation within 6 months was lower in the frontal burr hole drainage group than in the parietal burr hole drainage group (difference of 2.9 percentage points, 95% confidence interval [CI] −8.6 to 2.8; p = 0.31; Fig. 2; Table 3). Of the 135 participants for whom mRS data were available at 6 months, 5 patients (3.7%) had an unfavorable functional outcome. Out of 135 patients, 3 (2.2%) passed away within 6 months following the original operation. Both treatment groups had comparable 6-month mortality rates (difference of 1.5 percentage points, 95% CI −3.5 to 6.5; p = 0.55; Table 3) and proportions of patients with an unsatisfactory functional outcome (difference of −1.4 percentage points, 95% CI −7.8 to 4.9; p = 0.66; Table 3, Fig. 3).
Trial profile. The primary outcome, recurrent chronic subdural hematoma requiring reoperation was available for all participants.
Primary and Secondary Outcomes
Patients could have more than one complications.
The p value for noninferiority was defined as p([Frontal burr-hole-Parietal burr-hole] ≥noninferiority margin).
mRS, modified Rankin Scale; DVT, deep venous thrombosis.
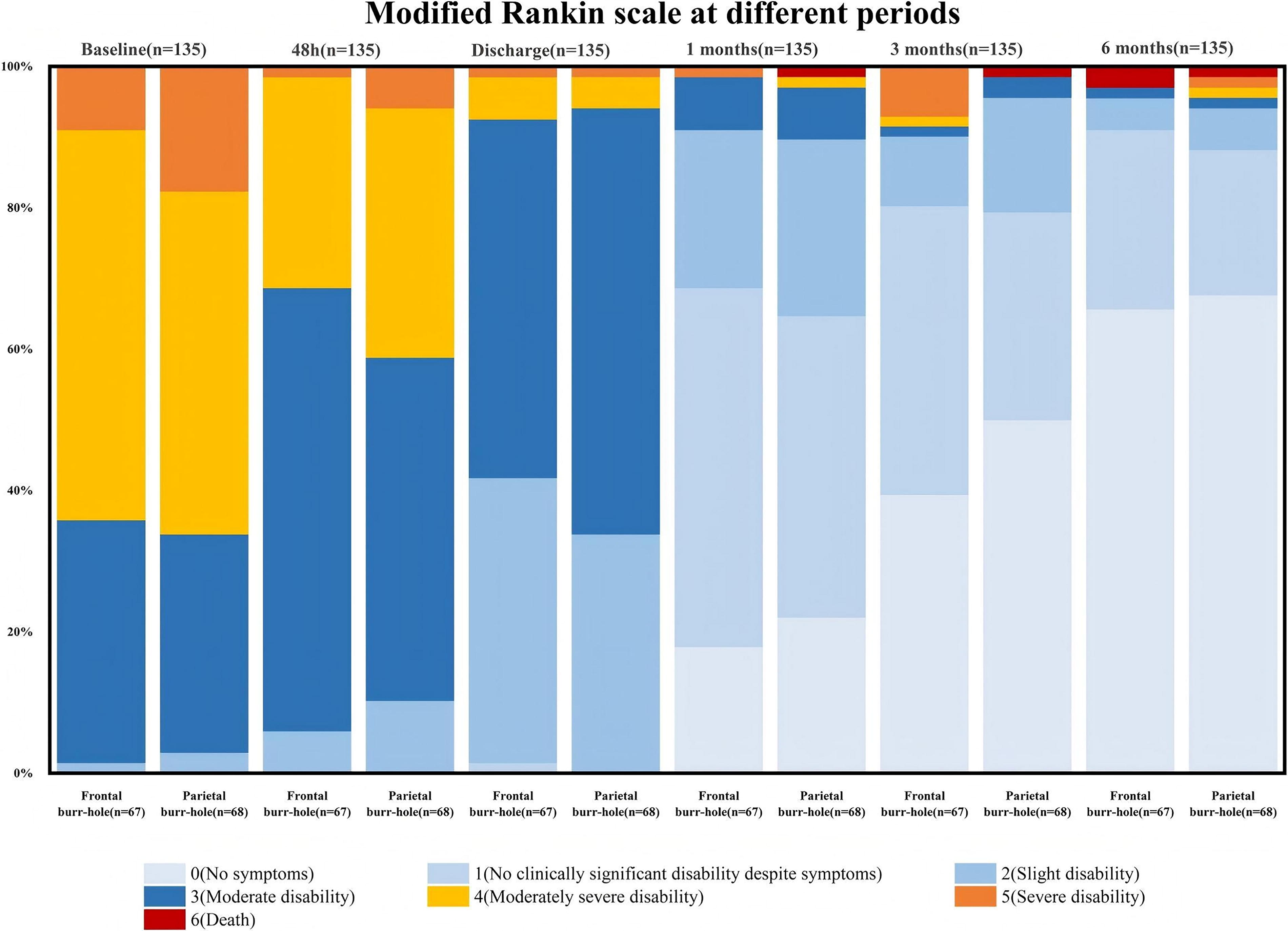
mRS score distribution between frontal and parietal at different periods. Data are shown as the proportion of participants with each mRs score in the frontal versus the parietal group. A score of 0 indicates no symptoms, 1 indicates no clinically significant disability despite symptoms, 2 indicates slight disability, 3 indicates moderate disability, 4 indicates moderately severe disability, 5 indicates severe disability, and 6 indicates death, mRs, modified Rankin Scale.
There was no significant difference in operative time between the two groups performing unilateral burr-hole for drainage, but the frontal drilling group performing bilateral drilling had a significantly shorter time than the parietal burr-hole group (Difference of −53min, 95% CI −95.7 to −10.3; p = 0.038; Table 3). In addition, the frontal burr-hole group had markedly reduced postoperative pneumocephalus on CT at 48 h postoperatively compared with the parietal burr-hole group (Difference of −9.1 mL, 95% CI −15.1 to −3.1; p = 0.034; Table 3). However, the difference in length of stay between the two groups was not statistically significant.
There were no significant differences between the groups in the incidence of surgical operation-related complications, postoperative seizures, or any other adverse events (Table 3). The most common complication was pneumonia, which occurred in 74 (54.8%) patients, including 36 in the frontal burr-hole group and 38 in the parietal burr-hole group. Adverse events related to the surgical operation occurred in 8 patients, mainly in the following situations: acute subdural hemorrhage, cerebral contusion, or placement of a drain through the hematoma envelope into the brain parenchyma.
Discussion
This single-center, randomized controlled, noninferiority trial involving adults with symptomatic CSDHs indicated that the 95% CI for the difference in recurrence rates within 6 months postinitial procedure between the frontal burr-hole group and the parietal burr-hole group spanned from −8.6 to 2.8. Given our predefined noninferiority margin of 5.0%, we can conclude that frontal burr-hole is noninferior. However, considering our observation that the recurrence rate was lower in the frontal bore-hole group than in the parietal bore-hole group and that the amount of postoperative intracranial air was much less in the frontal bore-hole group than in the parietal bore-hole group, together with the fact that there was no significant difference between the groups in terms of functional outcome, mortality, or adverse events at 6 months, the results of the trial support frontal bore-hole.
While the advantages of burr-hole surgery for CSDHs were well-documented, and its application had become widespread, the existing literature had primarily focused on factors such as the need for irrigation, irrigation fluid temperature, drain placement, drainage time, and number of burr-holes, with limited examination of the burr-hole site itself.11,12,20–23 In fact, recent studies have shown that there was no specific difference in improving the prognosis of patients after surgery for CSDHs whether it was a double burr hole or single burr hole, but single burr hole had the advantage of shorter operation time and less trauma, so single burr hole craniotomy was more and more accepted by neurosurgical colleagues.9,12,20 Therefore, it is necessary to know whether there is an impact on the prognosis of patients with CSDH when a single burr hole is performed at different sites. We selected a noninferiority design to evaluate the hypothesis that a frontal burr hole can diminish postoperative intracranial air accumulation, eliminate adverse events such as brain injury resulting from the placement of the tube from the parietal to the frontal region, and can be executed without compromising the efficacy or safety of the treatment.
As expected, the important finding of our study was that the frontal burr hole had a significant advantage in reducing the incidence of postoperative pneumocephalus. And it had translated into clinically visible benefits, with a lower reoperation rate in the frontal burr-hole group than in the parietal burr-hole group. Key factors influencing CSDH recurrence after burr hole surgery included postoperative brain re-expansion, intracranial pneumatosis, and residual hematoma size. 24 Poor brain re-expansion is linked to higher recurrence, with larger residual hematomas correlating with less re-expansion. 25 Pneumocephalus postsurgery can hinder brain re-expansion by maintaining the subdural space. 24 Poor brain tissue re-expansion can increase the elasticity of the surface of the local brain tissue, further preventing brain re-expansion and forming a vicious cycle. 26 Additionally, nasal endoscopic surgery patients with pneumocephalus may develop CSDH, with a higher risk correlating with pneumocephalus size. 27 In summary, reducing postoperative pneumocephalus and residual hematoma could promoted brain expansion and thus reduced the recurrence rate. Frontal burr hole surgery, performed with the patient supine, facilitates pneumocephalus discharge, reducing postoperative pneumocephalus, as confirmed by this study.
Current research suggests that parietal drainage was more effective for hematoma drainage in CSDH patients who remain supine post-drilling, as it benefited from higher hydrostatic pressure compared with frontal drainage. 28 However, our trial results indicated that frontal burr-hole was not inferior to parietal burr-hole for postoperative drainage. A recent research by Serag et al. showed that head elevation or retaining a prone position in patients following CSDH drilling did not significantly influence postoperative drainage or recurrence. 29 Notably, Raj et al. in their RCT investigation of CSDH patients, permitted ambulation and unrestricted movement during drainage. 12 So all these showed that drainage of residual hematoma following drilling in CSDH patients did not depend principally on pressure difference, but more likely on brain re-expansion and brain pulsation. The absence of a notable disparity in postoperative drainage outcomes between the two groups in our research further corroborated this perspective. In conclusion, frontal burr hole reduced postoperative pneumoperitoneum and promoted cerebral re-expansion while not affecting drainage at all.
Regarding our primary result, we identified a total recurrence rate of 3%, which was lower than the recurrence rates reported in other RCTs.11,12,20,22 Through comparison, we found that our enrolled patients were given oral atorvastatin postoperatively, a medication that can promote hematoma absorption, which might be the reason for our lower recurrence rate. 17
There were no significant differences between the groups in the incidence of poor functional outcome or death. The incidences of poor functional outcomes (4.0%) and death (2.2%) seen in our experiment align with those reported in previous studies.20,28 For these secondary outcomes, the study might indeed be underpowered to detect smaller but clinically relevant effects, increasing the risk of Type II error. This was an inherent limitation of trials designed around a single primary outcome, particularly for rare events. While our findings for low-frequency endpoints should be interpreted as exploratory, they remained hypothesis-generating for future studies with larger cohorts or pooled meta-analyses. In addition, frontal drilling in bilateral CSDH drilling saves a great deal of time compared with parietal drilling. Our single-center experience is that the patient’s head can be placed in a neutral position during frontal drilling without the need to deflect the patient’s head, which saves the time required to oscillate the patient’s head position during the operation.
The high incidence of postoperative pneumonia in our study warrants further discussion. pneumonia is a recognized complication following surgical procedures, particularly in neurosurgical patients. Although pneumonia occurred frequently, regression analysis found no significant link between pneumonia and mortality. Multivariate analysis revealed that general anesthesia was significant risk factors for pneumonia (Table 4). Patients who received general anesthesia had a higher likelihood of developing pneumonia compared with those who received local anesthesia. In addition, although there was no significant correlation between the duration of postoperative bed rest and the development of pneumonia, the risk of postoperative pneumonia increased as the duration of postoperative bed rest increased (Supplementary Fig. S1). These findings highlight the importance of considering anesthesia type and encouraging early patient mobilization as potential strategies to reduce the incidence of postoperative pneumonia.
Results of Multifactorial Logistic Regression Analysis for Pneumonia
The trial has certain limitations. First, the actual rate of reoperations was lower than the rate used to determine the sample size, potentially reducing statistical power and increasing the risk of type II error. However, the consistent findings of noninferiority across multiple subgroups with different risk profiles support the robustness of the direction: the 95% CIs for the risk difference were entirely below the noninferiority margin (Δ = 5%). This reduces the likelihood of chance-driven false-positive conclusions and indicates the stability of our noninferiority conclusion. Second, although we provided training to all surgeons beforehand, not all surgeries were performed by the same group of surgeons. There is variation among surgeons in specific surgical techniques such as irrigation, evacuation of pneumocephalus, and other operating procedures. Future studies should adopt protocolized workflows, such as standardizing the volume of intraoperative irrigation, to mitigate such variability. Finally, the administration of atorvastatin to all patients may have attenuated the observable effect size between surgical approaches. In populations with low statin utilization, the anatomical advantage of frontal burr hole placement may translate into larger clinical differences. Thus, the generalizability of our findings to nonstatin-treated populations requires validation.
In this single-center, randomized, controlled trial of symptomatic CSDH patients undergoing burr-hole surgery, we found that the number of recurrences was lower in the frontal burr-hole group than in the parietal burr-hole group within 6 months of the initial procedure, although this did not demonstrate a statistically significant difference. Notably, the frontal burr-hole procedure demonstrated a particularly significant advantage in that it was effective in reducing the amount of postoperative pneumocephalus. Furthermore, when comparing functional recovery outcomes as well as mortality between the two groups, no significant differences were found. Therefore, our noninferiority regarding frontal burr-hole is established. We believe that frontal burr hole is not only safe, but also has practical clinical implications in terms of reducing pneumocephalus and decreasing recurrence rates. In the future, it will be necessary to further expand the sample size and conduct a superiority trial to further demonstrate the overall benefits of frontal burr hole.
Footnotes
Authors’ Contributions
B.W. and P.C. planned and designed the study. B.W., P.C., and P.O. were the principal investigators. All study investigators contributed to trial conduct and data collection. P.C. was responsible for the methods. P.C. and P.O. were responsible for data integrity. P.C. and B.W. wrote the draft. Z.N. conducted the statistical analyses. All authors read, commented on, and approved the final article. P.C., P.O., B.W., and Z.N. accessed and verified the data. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Transparency,Rigor,and Reproducibility Statement
We are committed to ensuring the transparency, rigor, and reproducibility of our research. All study data and methodologies are reported in detail, and the data are available upon request to allow for independent verification. We followed established ethical guidelines and employed standard, validated methods for data collection and analysis. Our findings are presented accurately and transparently, and we acknowledge any limitations in the study. By adhering to these practices, we aim to contribute to reproducible and reliable scientific knowledge.
Data Sharing
All data requests should be submitted to B.W. by email for consideration.
Author Disclosure Statement
We declare no competing interests.
Funding Information
This study was supported by the Hunan Provincial Natural Science Foundation (General Project, CLC-3/SGK1 axis regulates YAP/TAZ to promote glial cell ferroptosis in secondary brain injury, 2022JJ30520) and the Hunan Provincial Health Commission’s National Clinical Key Specialty Major Project (HSPH1’s role in the mechanisms and cognitive function related to medium- and long-term secondary brain injury, 20230279).
Supplementary Material
Supplementary Data
Supplementary Figures
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.