
Abstract
Traumatic brain injury (TBI) remains a leading global cause of death and disability, disproportionately impacting low- and middle-income countries (LMICs), where neurosurgical resources are often limited. In these settings, foundational gaps in health system infrastructure—such as limited internet access, absence of electronic medical records (EMRs), and lack of standardized protocols—impede timely diagnosis, intervention, and continuity of care. This study evaluates the relationship between health system infrastructure and neurosurgical capacity, intervention delivery, and TBI outcomes across LMICs. We conducted a systematic review following Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines across PubMed, Embase, and Scopus to identify studies examining TBI care and system infrastructure in LMIC institutions. Extracted data were categorized across two primary domains: (1) clinical management and patient outcomes, and (2) implementation of health system components, including EMRs, information and communication technology access, and standardized care protocols. Quantitative analysis incorporated descriptive statistics, chi-square testing, Kruskal–Wallis tests, Glasgow Coma Scale-adjusted linear regression models, and machine learning classifiers to examine associations. Of the LMIC institutions reviewed, only 41% reported the presence of neurosurgical capacity. Implementation of EMRs and standardized protocols was significantly associated with increased neurosurgical capacity (odds ratio [OR] = 1.1, p = 0.06; OR = 1.1, p = 0.03, respectively). Among facilities with operative capacity, the median neurosurgical intervention rate was 28% (interquartile range [IQR]: 3–33%). Policy implementation predicted reduced post-TBI mortality (B = −10.8, p = 0.06; R2 = 0.56), with a median institutional mortality rate of 19% (IQR: 8–17%). Machine learning models demonstrated strong discriminatory ability to predict TBI mortality based on neurosurgical capacity and infrastructure metrics (area under the curve = 0.76). These findings highlight the potential for health system infrastructure—particularly EMRs, internet access, and standardized clinical protocols—to improve neurosurgical readiness and reduce preventable mortality following TBI in LMICs. Strategic investment in digital health tools and policy standardization could be a high-yield, scalable approach to closing global neurosurgical care gaps and improving TBI outcomes in resource-limited settings.
Keywords
Introduction
Traumatic brain injury (TBI) is a leading cause of injury-related mortality and disability worldwide, affecting an estimated 69 million people annually.1,2 This burden is disproportionately borne by low- and middle-income countries (LMICs), defined as any nation where the gross national income per capita is less than $4,255. Within LMICs, there are low-resource neurosurgical regions where mortality rates from TBI are two to four times higher than those in high-income settings.3,4 Compounding these challenges is the widespread shortage of neurosurgical staffing, posing a significant hindrance to effective intensive care management. This burden is frequently intensified by inadequate health systems infrastructure.1,5 Technology deficiencies are heterogeneous, often including an interplay of reliance on paper-based record-keeping, inconsistent internet connectivity, and lack of international standardization for critical care protocols. Each of these has been shown as a confounding factor that magnifies health care disparities.6,7 Furthermore, inadequate centralized data collection and trauma registries across LMICs obscure the true scope of neurotrauma care needs, consequently complicating health system development and planning. 8
Leading neurosurgical experts urge that improving care in resource-limited settings requires strengthening of health system technology, not just surgeon training and development. 9 Although health care technology is recognized as a key strategy for closing health equity gaps, there is a paucity of research evaluating the impact of specific components of health system frameworks on patient outcomes within neurosurgical trauma settings in LMICs. 10
Therefore, the aim of this systematic review is to evaluate the association between digital health implementation, neurosurgical intervention capabilities, and patient outcomes following TBIs across low-resource neurosurgical environments. This study seeks to elucidate neurotrauma clinical outcome adjuvants within health systems frameworks and identify pathways for resource deployment within global neurosurgical care. This global systematic review represents a pioneering analysis, hoping to serve as a foundation for future research endeavors and global health policy and digital integration efforts within low-income neurosurgical care systems.
Methods
Study design
This systematic review was conducted in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines to identify all available literature evaluating the impact of health systems implementation on TBI care, treatment, and outcomes in low-resource neurosurgical settings. The review adhered to the PRISMA 2020 guidelines, ensuring a transparent and reproducible study process. The review protocol was developed a priori but not preregistered in the International Prospective Register of Systematic Reviews (PROSPERO), as it encompassed both health systems infrastructure and clinical outcome domains and did not fit cleanly within registry categories; however, all objectives, eligibility criteria, and analyses were prespecified and adhered to throughout.
Search strategy
A comprehensive literature search was conducted across PubMed, Embase, and Scopus databases, covering studies published from January 2014 to January 2025. A dual-phase approach was used to identify articles focused on TBI care and articles focused on digital health infrastructure, each with unique search terms. The complete search strategy for both phases can be found in Supplementary Table S1.
Study selection
Given the unique nature of the dual-phase review, study selection included screening and eligibility assessment alongside the identification of study pairs based on the study site(s) of focus. Studies were selected if they met the criteria found in Supplementary Table S2 and were included in a study setting that was represented by at least one study from the partner phase. While the review focused on LMICs, we also included institutions from upper-middle-income countries if the specific study site operated within a low-resource subnational region—for example, lacking consistent access to imaging, EMRs, or neurosurgical services. These institutions reflected similar resource constraints and system barriers as those found in LMICs, making them appropriate for inclusion. For eligible articles, two independent reviewers (C.S.R. and J.J.S.) performed title and abstract screenings alongside a full-text review for eligibility. Discrepancies were resolved through reviewer consensus.
Data extraction
Extracted data from phase 1 included study characteristics, TBI severity measured by the presenting Glasgow Coma Scale (GCS) score, presence and utilization of interventions from emergency department arrival through discharge, time to interventions (when available), length of hospital stay (LHS), and outcomes including all-hospital morbidity and mortality, and subsequent timelines, when available. Extracted data from phase 2 included health systems infrastructure tools such as information and communication technology (ICT), electronic medical records (EMRs), and standardized care protocols.
Variable definitions
EMR and protocol implementation were categorized as absent, partially implemented, or fully implemented. Internet/ICT was classified as reliable, unreliable, or absent. Neurosurgical capacity was defined as the presence of a dedicated neurosurgical service or department staffed by a neurosurgeon and capable of performing operative interventions for TBI. Neurosurgical intervention included any operative procedure used in the management of TBI, such as decompressive craniectomy or craniotomy. TBI severity was assessed using the GCS, categorized as mild (≥13), moderate (9–12), or severe (≤8). Mortality was defined as the percentage of in-hospital deaths among patients with TBI at each institution. Morbidity was defined as the percentage of patients with any functional or neurological disability reported at discharge or last follow-up.
Statistical analysis
Univariate statistics
Descriptive statistics were reported as (% total) for categorical variables and median (range) for continuous variables. All variables and analyses were conducted at the institutional level, with each observation representing a single hospital or clinical site. No patient-level data were used. Pairwise comparisons were conducted between implementation frameworks (EMR, internet/ICT connectivity, standardized protocols) and continuous and categorical clinical variables, in which chi-square tests of independence and Kruskal–Wallis tests were employed, respectively.
Machine learning-based predictive modeling
To evaluate the predictive value of clinical and infrastructure-related factors on neurosurgical outcomes, machine learning analysis was conducted using logistic and linear regression analysis with stratified fivefold cross-validation. Given the heterogeneity of outcome reporting and institutional-level categorical data, traditional meta-analytic techniques were not appropriate. Instead, machine learning provided a flexible framework to extract predictive patterns from sparse and structurally diverse data. Cross-study median GCS scores were included as a covariate in all regression models to adjust for differences in presenting injury severity and reduce potential confounders. Effect sizes were reported either using odds ratios (ORs), Cramer’s V, or Eta-squared (η2). Synthetic Minority Oversampling Technique (SMOTE) was applied within each training fold to address class imbalance, with the number of neighbors adjusted dynamically based on minority class size. Models were plotted with receiver operating characteristic (ROC) curves, and performance was assessed using standard classification metrics, including area under the curve (AUC), sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), accuracy, and F1 score, averaged across folds.
The statistical significance threshold in this study was set at p < 0.1 to account for the heterogeneity of global data sources. For exploratory analyses spanning diverse settings, this relaxed threshold was intentionally chosen to reduce the risk of false negatives (type II errors) in detecting potentially meaningful associations (clarification added to justify p < 0.1 significance level). All statistical analyses were performed using Python (version 3.10).
Confounding considerations and sensitivity analyses
In addition to adjusting for injury severity, careful consideration was given to ensure that all included institutions were located within low-resource neurosurgical environments. Upper-middle-income country sites were only included if the surrounding region was recognized as resource-limited (e.g., lacking neurosurgical services, advanced imaging, or consistent EMR/ICT capacity), whereas high-resource subnational sites were excluded. This approach ensured that the review captured low-resource settings regardless of national income classification. To further evaluate robustness, sensitivity analyses were utilized with restricted regression models for institutions classified as LMICs. Models were repeated using this subset and compared against the full dataset to assess whether the inclusion of non-LMIC but resource-limited sites materially altered effect sizes.
Risk of bias
A structured risk-of-bias assessment for all included studies was performed using the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool. Each study was evaluated across the seven ROBINS-I domains (bias due to confounding, bias in selection of participants, bias in classification of interventions, bias due to deviations from intended interventions, bias due to missing data, bias in measurement of outcomes, and bias in selection of the reported result), with each domain rated as low, moderate, or serious risk of bias.
Certainty of evidence
In addition to ROBINS-I, this study used the National Heart, Lung, and Blood Institute (NHLBI) 14-item Study Quality Assessment Tool for observational cohort and cross-sectional studies. Each item was rated as yes, no, cannot determine (CD), not reported (NR), or not applicable (NA). A total score was calculated for each study, and the overall quality was classified as good, fair, or poor, as shown in Supplementary Table S3.
Ethical considerations
This study was based on previously published data and did not require ethical approval. All data were sourced from publicly available studies, and no patient-identifiable information was collected or analyzed.
Results
Study characteristics
Through a comprehensive database search, 306 unique records were identified: 221 from phase 1 and an additional 85 from phase 2 (Fig. 1). After rigorous title/abstract screening and full-text evaluation, study pairing produced a cohort of 27 TBI-focused studies (phase 1) and 23 digital infrastructure-focused studies (phase 2). In sum, the final dataset included 50 studies across 52 institutions (Table 1).
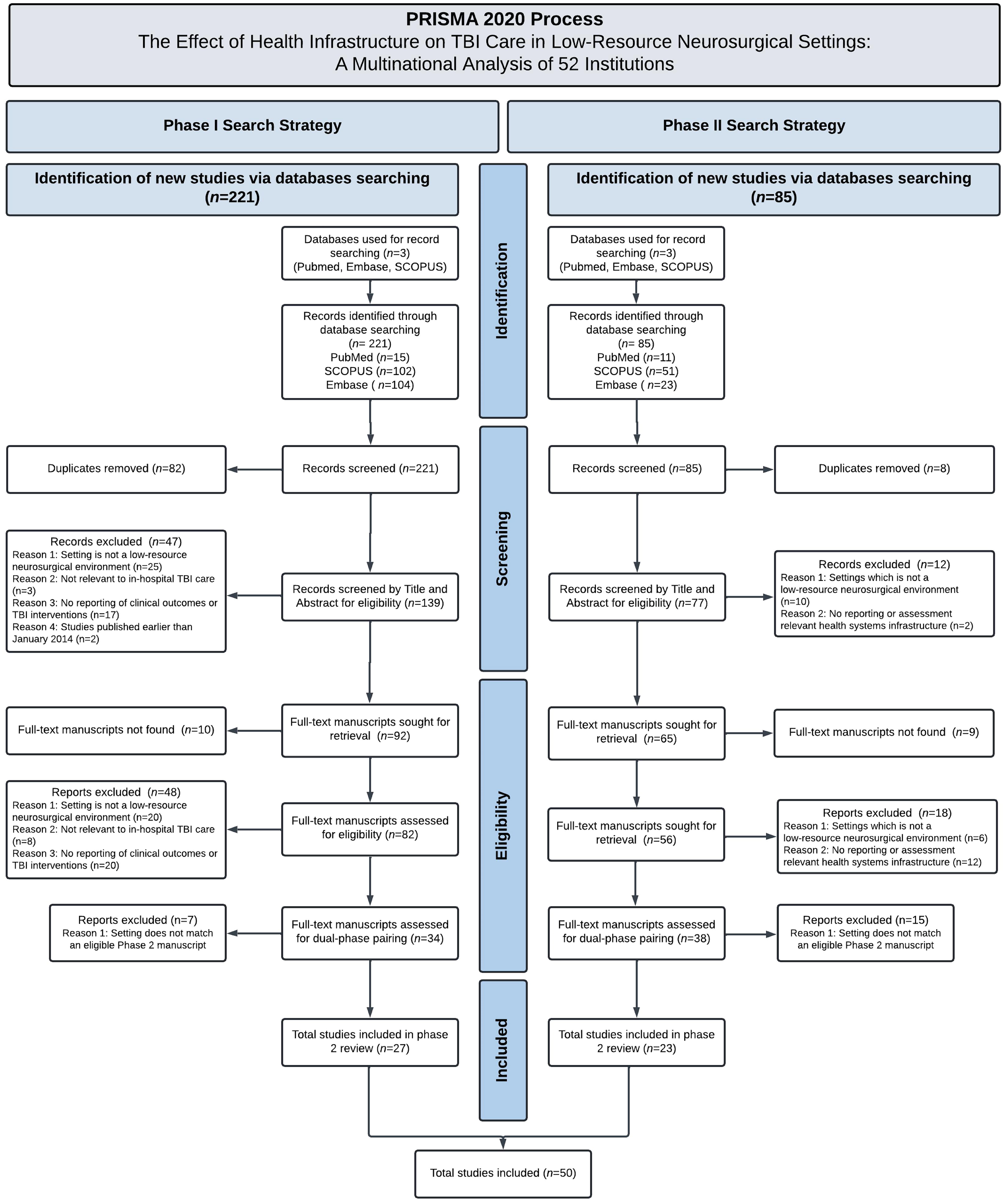
PRISMA diagram of study selection. PRISMA 2020 diagram summarizing the systematic review selection process for evaluating health infrastructure impacts on TBI care in low-resource neurosurgical settings. The review included 50 studies identified through two phases of database searching and screening. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; TBI, traumatic brain injury.
Geographic Distribution of Included Institutions and Respective Phase 1 and 2 Studies
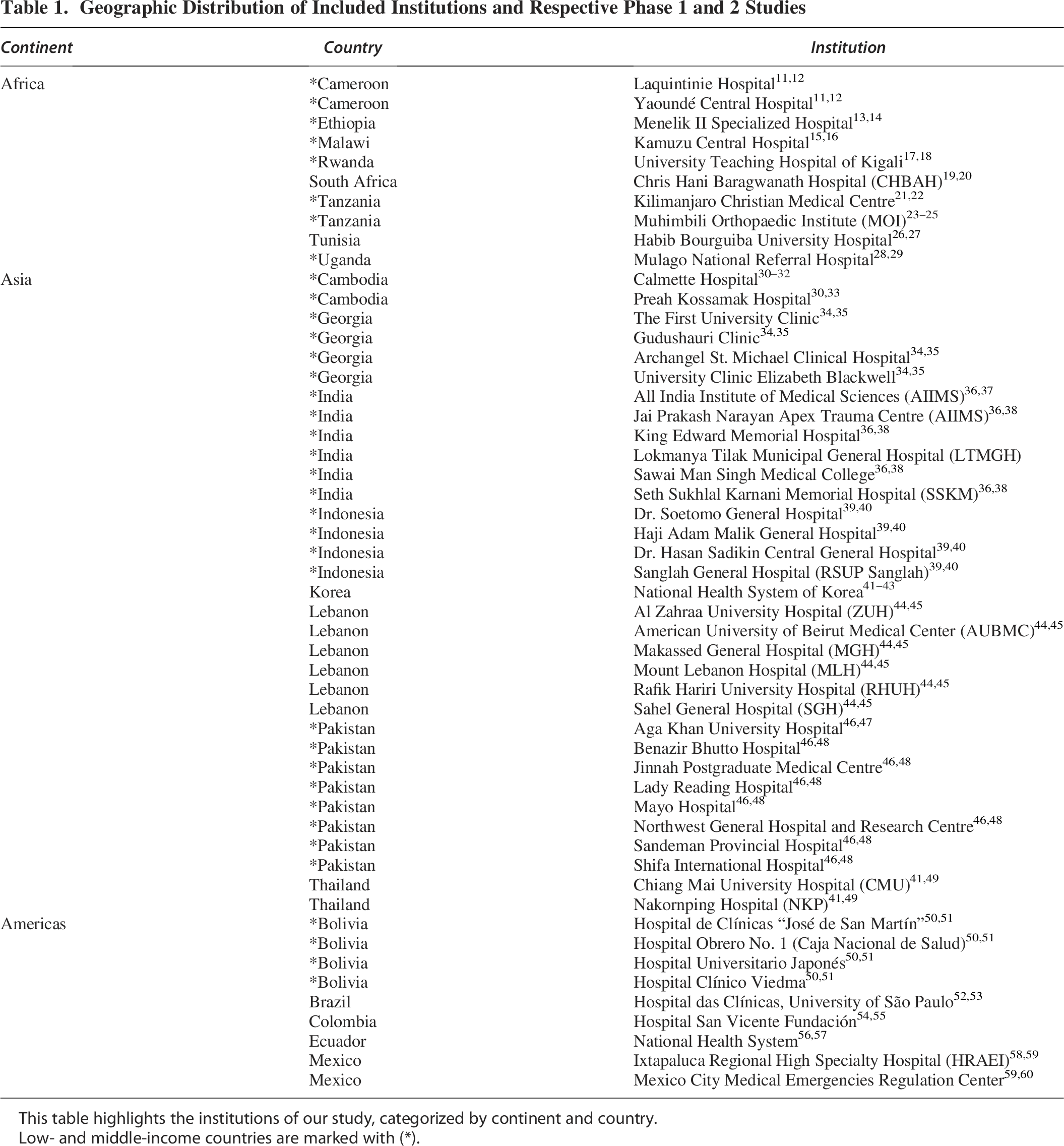
This table highlights the institutions of our study, categorized by continent and country.
Low- and middle-income countries are marked with (*).
Health systems and geographic distribution
The included studies (2014–2024) provided data on 52 institutions, representing 21 countries in Asia, Africa, and the Americas, with 33,30–49 10,11–29 and 950,51,53–60 institutions per continent, respectively (Fig. 2). Seventy-one percent of the included institutions (n = 37) were within LMIC countries, with the rest of the included institutions (n = 15) being located within countries having upper-middle-class economies (gross net income per capita of $4,256–$13,205). Reliable internet connectivity was reported in 9 institutions (17%),36,39,44,46,55,57 absent ICT infrastructure was reported in 3 institutions (6%),36,46 and present but unreliable connectivity was reported in the remaining 40 (77%). All institutions in the Americas and Asia reported at least unreliable internet access, with the Americas having the highest proportion of reliable access (22%, n = 2),55,57 closely followed by Asia (21%, n = 7).34,36,44,46,49 All African institutions reported unreliable internet. EMR systems were fully implemented in only four institutions (11%)36,39,46,52 and partially implemented (n = 20, 38%) or absent elsewhere (n = 27, 52%). The Americas demonstrated the greatest presence of progressing EMR system use (89%, n = 8)50,52,55,57,59 compared to only 10% in Africa (n = 1), 23 with Asia exhibiting a mid-tier presence (48%, n = 16). Across all continents, standardized clinical protocols were fully implemented in 11 institutions (21%),36,39,44,46,52,55,57 partially implemented in 8 (22%),39,41,44,46,50,59 and absent in the remaining 27 (52%). Comprehensive standards of care were most adhered to in the Americas (33%, n = 3)52,55,57 and Asia (24%, n = 8),36,39,44,46 but were notably absent in Africa (n = 0) (Fig. 3). Overall, EMR, ICT, and policy adoption were limited, with Africa consistently lagging behind Asia and the Americas in digital health infrastructure.
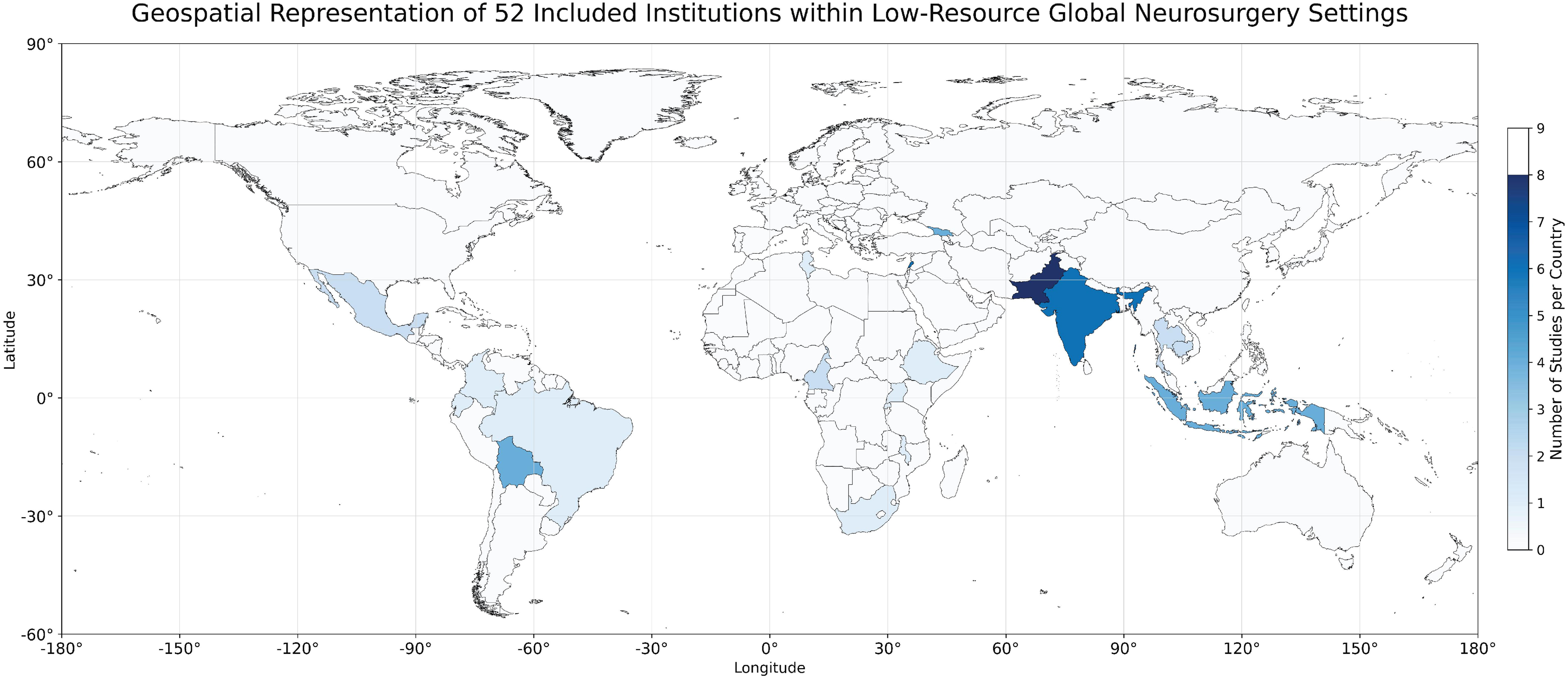
Geographic distribution of included institutions by country setting. Geographic distribution of the 52 institutions included in the systematic review, stratified by country setting. Color intensity indicates the number of studies per country.
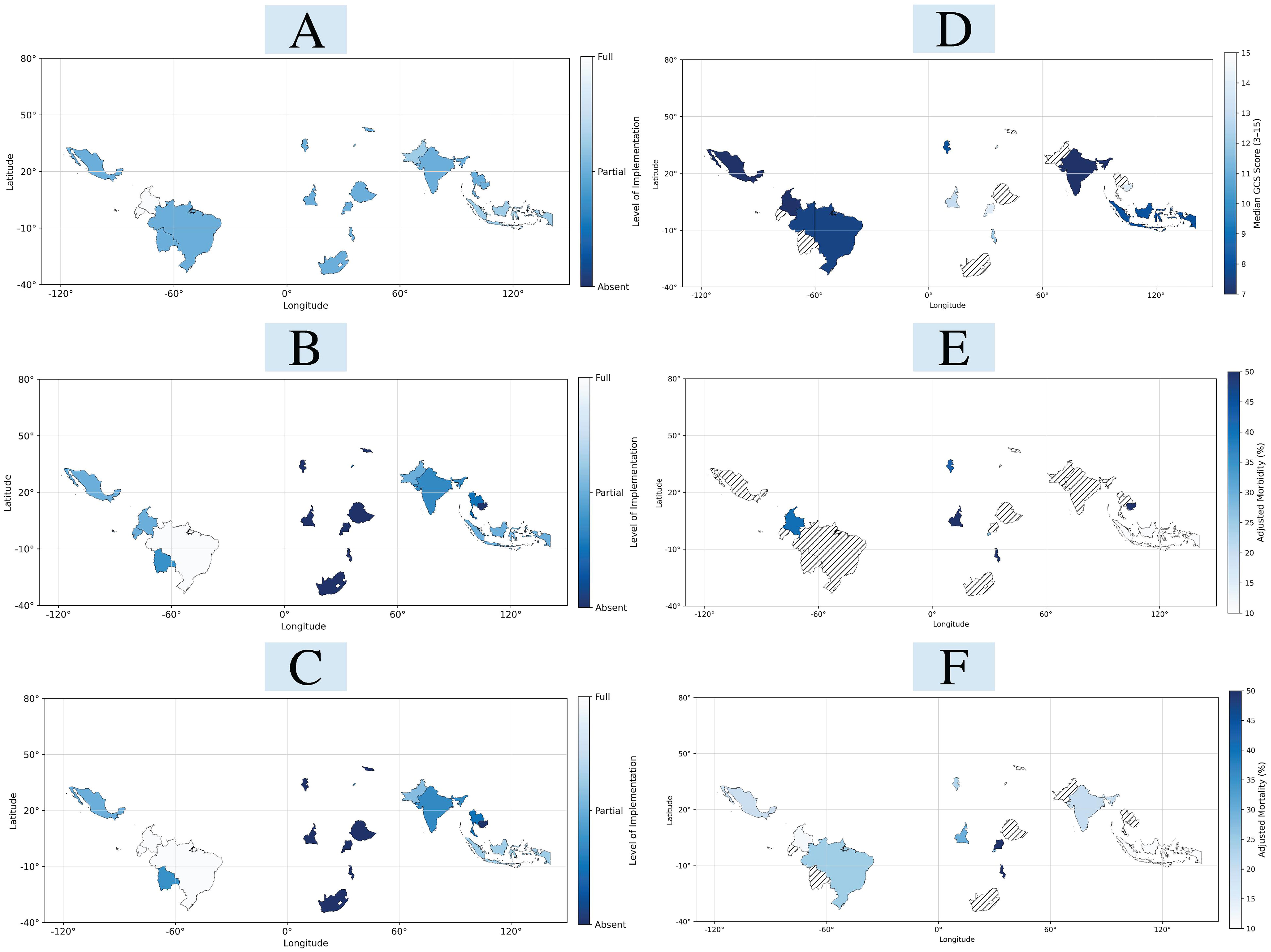
Clinical outcomes and infrastructure implementation status stratified by included LMIC. Geospatial distribution of health system infrastructure implementation across institutions in low- and middle-income countries (LMICs), categorized by electronic medical records (EMR) status
Current state of care
Patient presentation
GCS assessment was utilized in 67% (n = 35) of institutions, with a cross-study median of 9 at presentation (interquartile range [IQR]: 7–14). Presenting GCS was lowest in the Americas (7, IQR: 6–8) (Fig. 3). Severe TBI was observed in a median of 39% of cases across studies (IQR: 12–61%), and it was most common in the Americas, accounting for 65% (IQR: 57–66).32,51,53,54,58,60 Africa showed the longest time from injury to hospital arrival at 4 h (IQR: 3–8 h), compared to a cross-study median of 3 h (IQR: 2–7).16,22 Across regions, patients typically presented late and with moderate-to-severe TBI, with the Americas reporting the most severe injury profiles.
Procedures and hospital management
Cervical spine immobilization was the most consistently documented intervention, reported in 85% (n = 44) of institutions. Oxygenation and ventilation support were documented in 38% (n = 20) and provided at a median of 22% (IQR: 7–24%). Intubation was reported by 33% (n = 17) and was performed in a median of 31% (IQR: 5–50%) of cases. Fluid management practices were less often documented, noted in 29% (n = 15) of institutions. When documented, usage was widespread, with isotonic fluids administered to a median of 51% (IQR: 40–56%) of patients. Osmotic diuretics, mainly mannitol or hypertonic saline, were used in 21% (n = 11) of institutions, administered to a median of 30% (IQR: 13–58%) of patients with TBI. Additional pharmacologic interventions, including seizure prophylaxis and thromboprophylaxis, were least reported, documented in only 17% (n = 9)24,32,37 and 4% (n = 2)24,27 of institutions, respectively.
Neurosurgical capacity
Neurosurgical capacity was present in 50% (n = 26) of institutions, and 58% (n = 15) of those without neurosurgical care were from LMIC countries.35,48,51 Among those with neurosurgical capacity, surgical evacuation—primarily by craniectomy or craniotomy—was performed in a median of 28% (IQR: 13–33%) of TBI cases. Only two studies reported the median time from evaluation to surgery, at 12 and 92 h.22,29 Neuroimaging availability (computed tomography [CT] and magnetic resonance imaging [MRI]) was noted in only 65% (n = 34) of institutions, with 72% (n = 13) of these indicating limited or no accessible imaging, mainly within LMICs. When available, neuroimaging was used in a median of 81% (IQR: 50–99%) of cases. Only three studies reported the median time to first imaging, at 3 h (IQR: 3–17), with the longest duration being 17 h in Tanzania.22,24,29 Intracranial pressure (ICP) monitoring was available in 35% (n = 18) of institutions. Overall, neurosurgical, imaging, and invasive monitoring capabilities were available in only about half of the institutions, with significant variability across continents and notable delays when reported.
Clinical outcomes
The median LHS from injury to discharge was 21 days (IQR: 14–27). The pooled median hospital morbidity and mortality rates were 49% (IQR: 23–56%) and 9% (IQR: 8–17%), respectively, though mortality (n = 43) was reported more frequently than morbidity (n = 15) (Fig. 3). Glasgow Outcome Scale assessments were documented in only 29% (n = 15) of institutions, and reporting consistency varied significantly.
Effect of health systems infrastructure
Intervention capacity
Compared to institutions without EMR, those with partial EMR implementation showed a significantly higher availability of intravenous (IV) fluids (OR = 17.0, p = 0.040) (Table 2). Additionally, implementing policies and standards at any stage was linked to greater access to IV fluids (OR = 10.79, p = 0.041). Among institutions with partial policy and standards adoption, there was also a notable increase in specialized fluid management, especially osmotherapy (OR = 12.2, p = 0.039). GCS-adjusted linear regression indicated that partial implementation of policies and standards was significantly associated with increased use of oxygenation and ventilation support compared with institutions without such implementations (β = 55.8, p = 0.012) (Table 3).
GCS-Controlled Logistic Regression of Health Systems Implementation and Care Capacity
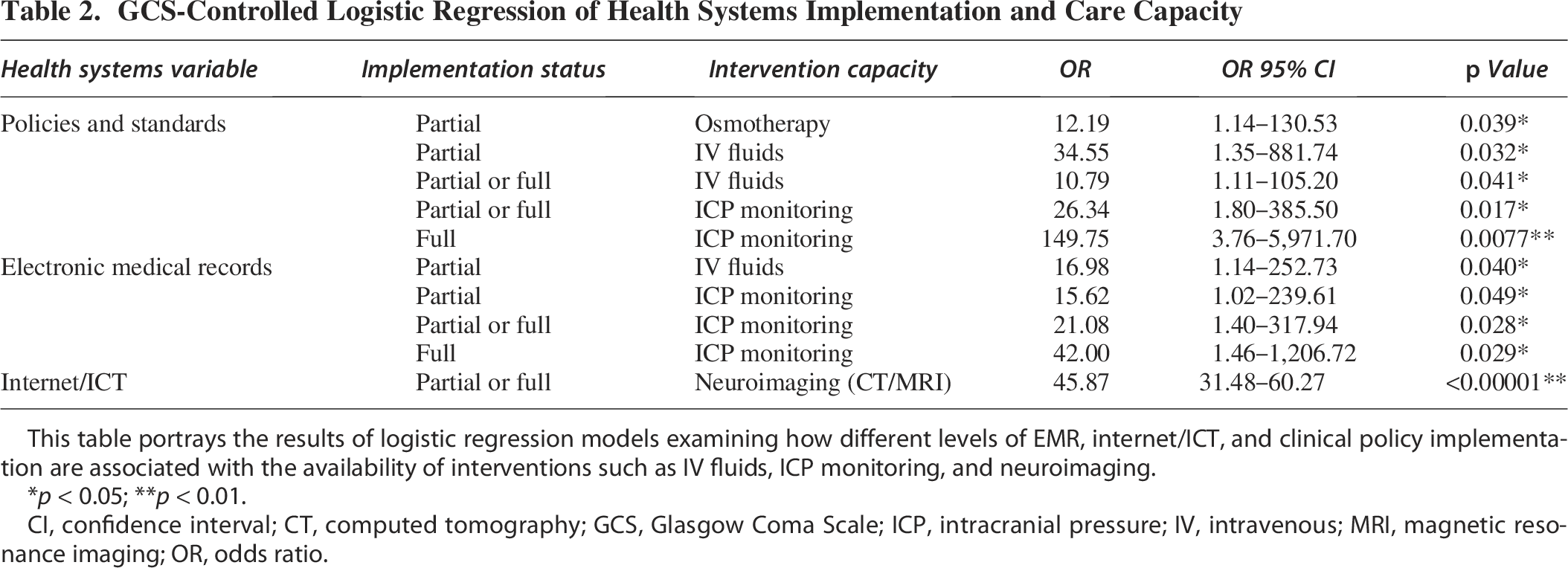
This table portrays the results of logistic regression models examining how different levels of EMR, internet/ICT, and clinical policy implementation are associated with the availability of interventions such as IV fluids, ICP monitoring, and neuroimaging.
p < 0.05; **p < 0.01.
CI, confidence interval; CT, computed tomography; GCS, Glasgow Coma Scale; ICP, intracranial pressure; IV, intravenous; MRI, magnetic resonance imaging; OR, odds ratio.
GCS-Controlled Linear Regression of Health Systems Implementation, TBI Care, and Outcomes
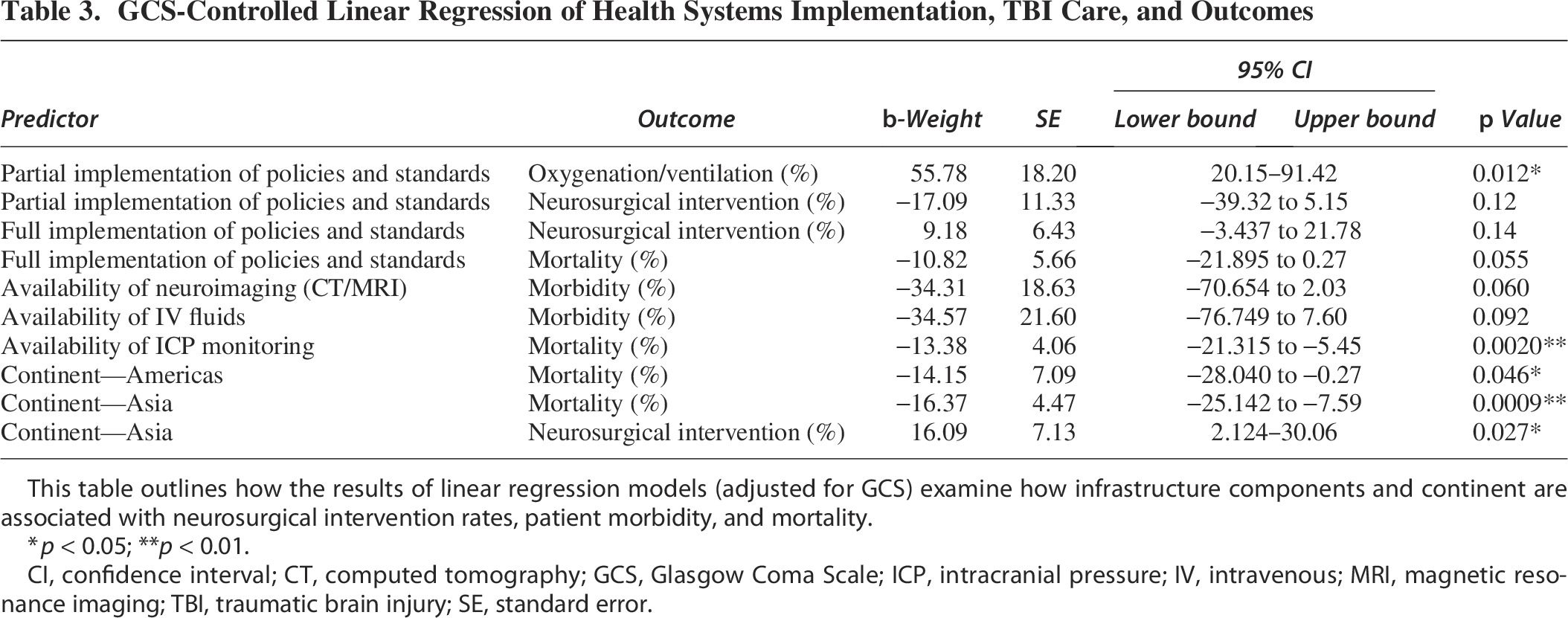
This table outlines how the results of linear regression models (adjusted for GCS) examine how infrastructure components and continent are associated with neurosurgical intervention rates, patient morbidity, and mortality.
p < 0.05; **p < 0.01.
CI, confidence interval; CT, computed tomography; GCS, Glasgow Coma Scale; ICP, intracranial pressure; IV, intravenous; MRI, magnetic resonance imaging; TBI, traumatic brain injury; SE, standard error.
Neurosurgical capacity
Implementation status was strongly linked to the availability of neurosurgical capacity and the frequency of surgical interventions. The presence of EMR (whether partial or full) correlated with higher neurosurgical capacity, χ2(2, N = 52) = 8.61, p = 0.013, Cramer’s V = 0.41. GCS-controlled linear regression revealed notable findings regarding infrastructure implementation and neurosurgical decision-making. The framework most significantly associated with operative intervention was protocols and standards of care, χ2(2, N = 52) = 9.42, p = 0.009, Cramer’s V = 0.50. Interestingly, partial and full implementation had contrasting effects on neurosurgical intervention rates (%). Partial implementation showed a negative trend (β = −17.1, p = 0.12), whereas full implementation indicated a positive trend (β = 9.2, p = 0.14). Additionally, neurosurgical intervention rates were higher in countries from Asia, which had the greatest likelihood of increased operative TBI treatments (β = 16.1, p = 0.027).
Monitoring and imaging
The presence of EMR, policies, and standards independently correlated with increased availability and use of ICP monitoring. EMR showed a positive association with higher ICP monitoring availability at both partial (OR = 15.6, p = 0.049) and full implementation stages (OR = 42.0, p = 0.029), with availability increasing as infrastructure completeness improved. Similarly, policies and standards were associated with greater ICP monitoring capabilities, especially at full implementation (OR = 149.8, p = 0.008). The strongest framework related to neuroimaging capacity was internet/ICT, where its presence alone significantly increased the likelihood of neuroimaging (OR = 45.9, p < 0.00001).
Patient outcomes
Among the three domains, implementing policies and standards was the most significant framework associated with patient outcomes. The GCS-adjusted linear regression model showed that full implementation of policies and standards was linked to lower post-TBI mortality (B = −10.8, p = 0.055). Partial implementation did not yield similar effects, indicating that complete policy adoption might be necessary to improve survival. Equally important, the presence of three treatment interventions stood out through GCS-adjusted linear regression as the intervention capacities with the greatest effects on patient outcomes. The availability of IV fluids (B = −34.6, p = 0.09) and on-site neuroimaging capabilities (CT/MRI; B = −34.3, p = 0.06) both showed inverse associations with post-TBI morbidity (%), while ICP monitoring capabilities (B = −13.4, p = 0.002) demonstrated a significant association with reduction in post-TBI mortality (%). Additionally, Asia (β = −16.4, p = 0.0009) and the Americas (β = −14.2, p = 0.046) demonstrated protective links with post-TBI mortality.
Predictive modeling of clinical contributors
Machine learning-based classification models further illustrated key dynamics between infrastructural predictors, intervention availability, and clinical outcomes (Table 4 and Fig. 4). The presence of EMR systems and implementation of clinical policies and standards showed modest predictive value for both access to neuroimaging (AUC = 0.66; F1 = 0.68) and presence of neurosurgical capacity (AUC = 0.65–0.64; F1 = 0.64), further indicating that infrastructure presence correlates with system-level readiness. ICP monitoring capabilities demonstrated high specificity (0.93) and PPV (0.94) for predicting access to neuroimaging (AUC = 0.71), verifying their role as a marker of specialized neuromonitoring and advanced neurocritical care. The strongest predictive performance was observed in neurosurgical capacity, which showed high potential in predicting oxygenation and ventilation support (AUC = 0.79, F1 score = 0.74). This aligns with regression analyses showing significant associations between infrastructure strengthening and increased intervention compliance. Notably, both oxygenation/ventilation and neurosurgical capacity showed potential discriminatory power in predicting patient mortality (AUCs = 0.68 and 0.76, respectively), suggesting these features may function as foundational indicators of institutional treatment readiness and survival potential. Machine learning findings paralleled regression results, further supporting the role of EMR, ICP monitoring, and neurosurgical capacity as core predictors of readiness and outcomes.

Predictive performance of structural and infrastructure variables on neurosurgical outcomes. Receiver operating characteristic (ROC) curves for logistic regression models
Performance Metrics for Predictors of Structural and Clinical Outcomes Across Low-Resource Neurosurgical Settings
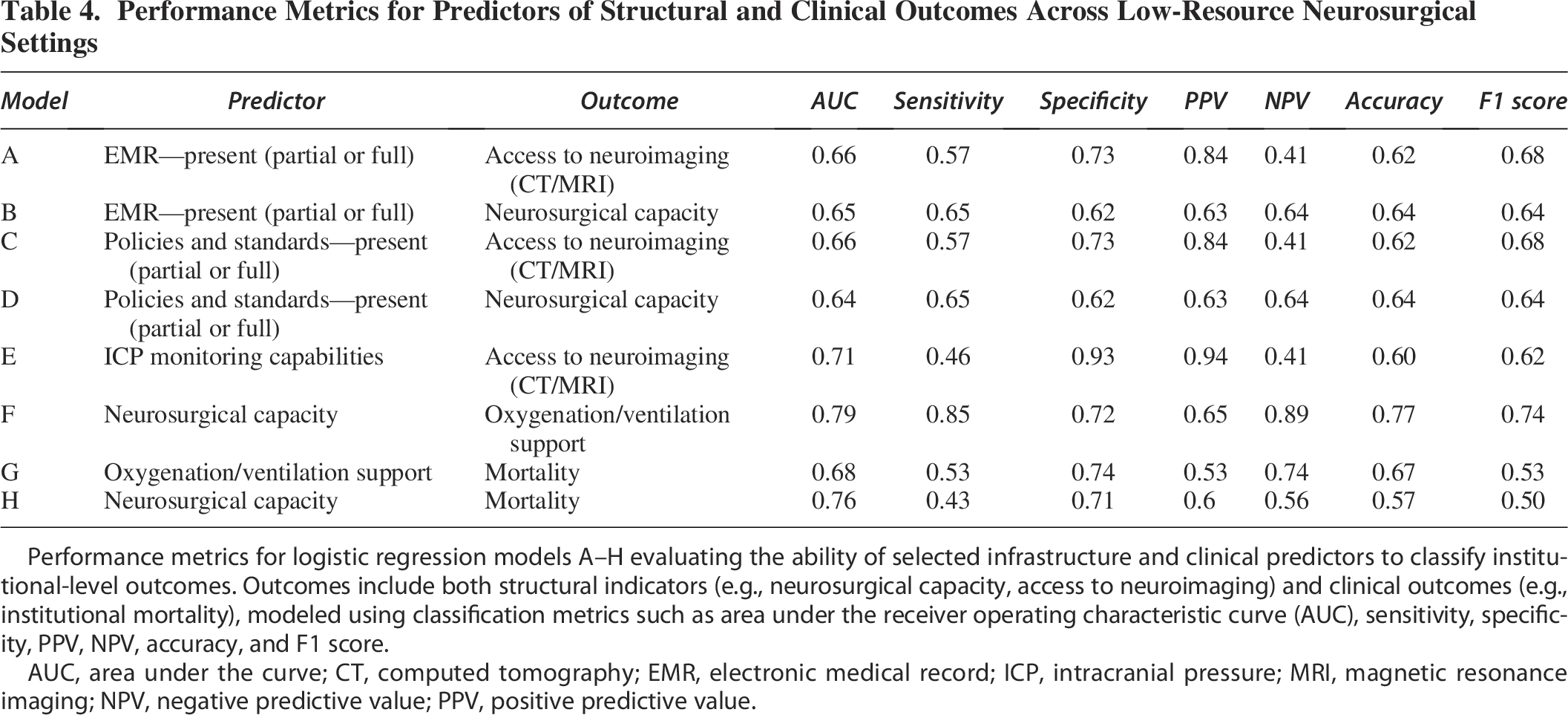
Performance metrics for logistic regression models A–H evaluating the ability of selected infrastructure and clinical predictors to classify institutional-level outcomes. Outcomes include both structural indicators (e.g., neurosurgical capacity, access to neuroimaging) and clinical outcomes (e.g., institutional mortality), modeled using classification metrics such as area under the receiver operating characteristic curve (AUC), sensitivity, specificity, PPV, NPV, accuracy, and F1 score.
AUC, area under the curve; CT, computed tomography; EMR, electronic medical record; ICP, intracranial pressure; MRI, magnetic resonance imaging; NPV, negative predictive value; PPV, positive predictive value.
Risk of bias and certainty of evidence
None of the studies had a “low” bias risk across all ROBINS-I domains. Most were at least moderately biased in one or more areas, with some showing serious bias. Common issues included lack of confounder adjustment and inconsistent outcome reporting. No study was excluded for critical bias, but the biases highlight caution needed in interpreting results. Figure 5 summarizes risk assessments, and study quality ratings are in Supplementary Table S3—most rated fair, some good, and a few poor.
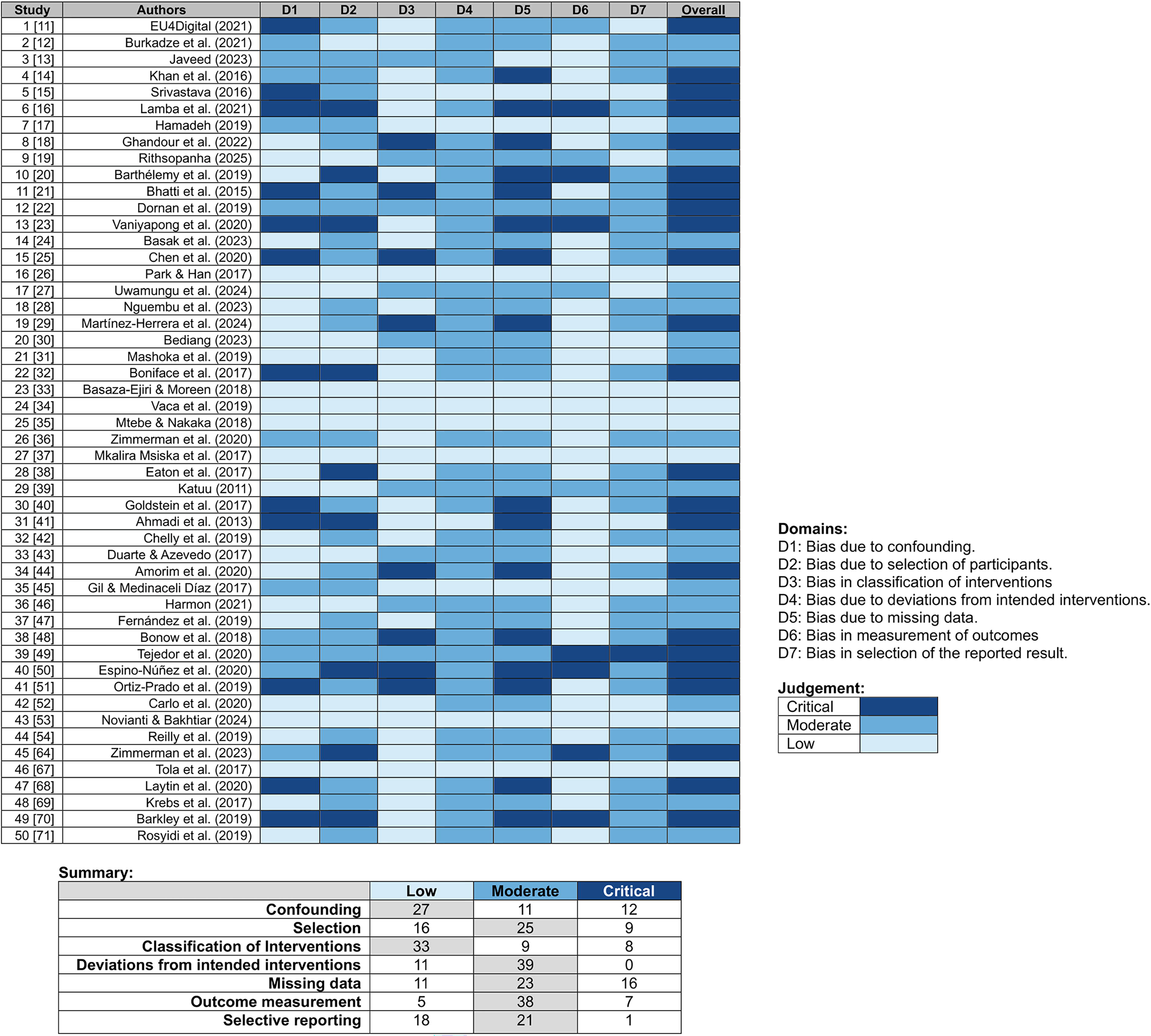
ROBINS-I risk-of-bias assessment across included studies. Matrix plot displaying the risk-of-bias assessments across seven ROBINS-I domains for all included studies. Each row represents an individual study (ordered by reference number), and each column corresponds to a ROBINS-I domain: D1 (bias due to confounding), D2 (bias due to selection of participants), D3 (bias in classification of interventions), D4 (bias due to deviations from intended interventions), D5 (bias due to missing data), D6 (bias in measurement of outcomes), and D7 (bias in selection of the reported result). Colors indicate the risk-of-bias judgment: light blue = low risk, medium blue = moderate risk, dark blue = serious/critical risk. The “Overall” column reflects the highest level of bias judgment across domains for each study. ROBINS-I, Risk of Bias in Nonrandomized Studies of Interventions.
Trends in low-resource sensitivity analysis
Sensitivity analyses demonstrated that the protective association between higher GCS and reduced institutional mortality was consistent across both full and LMIC-only datasets (Table 5). In the full dataset, GCS was a strong predictor of mortality (b = −3.49, p = 0.021), and the association remained directionally stable but less precise in LMIC-only analyses (b = −5.54, p = 0.309). When examining system capacity variables adjusted for GCS, ICP monitoring was consistently associated with lower mortality (full: b = −13.38, p < 0.001; LMIC-only: b = −18.99, p = 0.012). Neurosurgical capacity showed a similar protective effect (full: b = −1.12, p = 0.027; LMIC-only: b = −1.12, p = 0.030). Policies and standards trended protective in both analyses, with borderline significance in the full dataset (OR = 0.35, p = 0.080) and a nonsignificant but consistent direction in LMIC-only (OR = 0.33, p = 0.159). Together, these sensitivity analyses suggest that associations observed in the full dataset are robust and not driven by the inclusion of non-LMIC institutions, though power is reduced in LMIC-only models.
Sensitivity Analyses of Mortality Predictors in All Institutions Versus LMIC-Only Cohorts
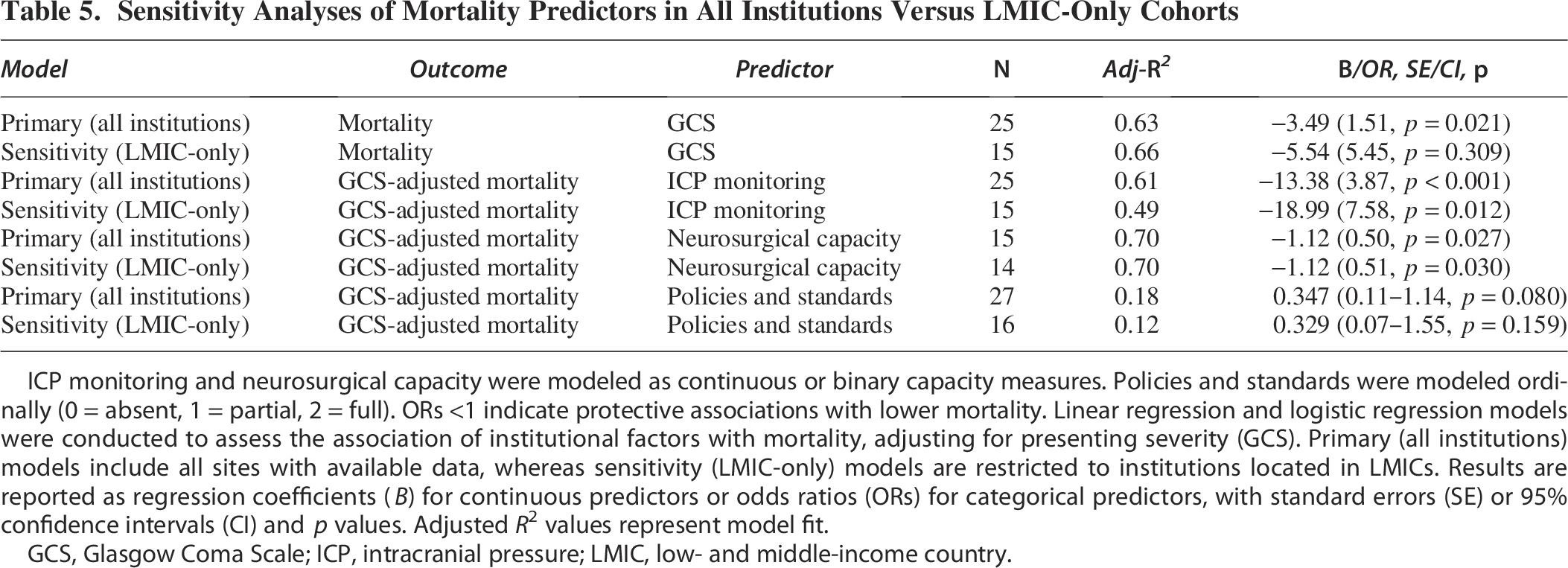
ICP monitoring and neurosurgical capacity were modeled as continuous or binary capacity measures. Policies and standards were modeled ordinally (0 = absent, 1 = partial, 2 = full). ORs <1 indicate protective associations with lower mortality. Linear regression and logistic regression models were conducted to assess the association of institutional factors with mortality, adjusting for presenting severity (GCS). Primary (all institutions) models include all sites with available data, whereas sensitivity (LMIC-only) models are restricted to institutions located in LMICs. Results are reported as regression coefficients (B) for continuous predictors or odds ratios (ORs) for categorical predictors, with standard errors (SE) or 95% confidence intervals (CI) and p values. Adjusted R² values represent model fit.
GCS, Glasgow Coma Scale; ICP, intracranial pressure; LMIC, low- and middle-income country.
Overall, neurosurgical capacity and outcomes remained highly constrained across LMIC institutions, with digital infrastructure—especially EMRs, ICP monitoring, and policies—consistently associated with improved readiness and lower mortality.
Discussion
This systematic review presents a strong association between digital health systems infrastructure and neurosurgical capacity, intervention delivery, and patient outcomes following TBI in LMICs. By evaluating TBI as an index condition, we identified foundational deficits and opportunities for growth within LMIC health systems with great promise to improve neurosurgical care outcomes.61–63 EMR implementation, standardized policies, and ICT infrastructure each demonstrated distinct associations with improved intervention availability, neurosurgical readiness, and patient outcomes. Among these, structured policies and care standards exhibited the most consistent correlations across domains, with both essential and specialized interventions correlating with reduced post-TBI mortality. To evaluate the robustness of these associations, we performed sensitivity analyses comparing models fitted to all institutions versus LMIC-only subsets. GCS remained a strong predictor of mortality in both datasets, although its precision was lower in the LMIC-only analysis due to the smaller sample size. After adjusting for GCS, ICP monitoring, and neurosurgical capacity consistently showed protective effects, being significantly linked to lower mortality in both cohorts. Policies and standards also showed a trend toward protection, approaching borderline significance in the full dataset and maintaining a consistent trend in LMIC-only analyses. These findings suggest that the results were not influenced by the inclusion of non-LMIC institutions and that essential infrastructure components remained strongly associated with reduced mortality across different analytic subsets.
Furthermore, our findings support the potential beneficial capacity of digital infrastructure to enhance the utilization of critical neuromonitoring. EMR implementation was significantly associated with an increased availability of ICP monitoring, with the likelihood of monitoring increasing with the degree of care implementation completeness. Additionally, the findings in this study corroborated the existence of stark global disparities, where ICP monitoring was reported in only 35% of the institutions included, compared with a 77% prevalence in the United States. 64 Neuroimaging availability (CT/MRI) was similarly scarce, reported in just 29% of institutions. India exhibited the lowest neuroimaging capacity, aligning with data indicating India’s extremely low per capita MRI density (0.21 units per million people).65,66 In follow-up machine learning analysis, ICP monitoring capabilities demonstrated high specificity in predicting neuroimaging access, verifying that digital connectivity frameworks represent reciprocal frameworks for allocating resources to expand global neurosurgery.
Only half of the included institutions reported the presence of neurosurgical services, aligning with previous literature, indicating that LMICs comprise 72% of countries lacking adequate neurosurgical access. 67 Institutions with neurosurgical staffing demonstrated a median post-TBI surgical intervention rate of 28%, markedly higher than the 13% reported by the high-resource U.S. TRACK-TBI cohort. 68 Furthermore, global neurosurgical workforce shortages contribute to significant delays in treatment (median: 52 h in low-resource settings vs. 1.8 h in high-resource settings). 67 Such systemic inefficiencies in clinical care delivery likely increase surgical intervention rates through delayed or inappropriate care escalation. Interestingly, our analysis supports this finding, as even partial implementation of standardized protocols reduced intervention rates by promoting timely, appropriate nonoperative management. Thus, enhanced health system frameworks have the potential to optimize clinical decision-making and operative resources, fostering both accessible and high-quality neurosurgical care.6,62,69
This study employed a strong methodological approach that uniquely paired clinical outcomes with detailed assessments of institutional capacity and policy implementation status. The inclusion of both binary and continuous variables allowed for granular analysis and circumvented typical global health research limitations. Multivariable modeling techniques also mitigated bias introduced by inconsistent reporting and allowed for isolation of health system factors and clinical outcomes, surpassing the scope of conventional reviews.25,53
The implications of this study are potentially substantial for global neurosurgery resource planning. Strategic investment in EMRs, protocols, and digital infrastructure may provide an avenue for scalable improvements to care. These tools have been shown to support clinical decision-making, standardization, and interinstitutional communication.6,37,69,70 Additionally, as AI-assisted triage and real-time decision support systems become more readily accessible, their potential intervention should be layered upon EMR and ICT platforms. Strengthening digital infrastructure can also occur independently of workforce expansion, making it a practical and immediate pathway for global neurosurgical development in low-resource settings. It is important to note, however, that many of the factors examined—such as EMR presence or standardized protocols—may also serve as markers of broader systemic wealth. As such, other unmeasured covariates (e.g., ambulance availability, skilled nursing staff, or regional trauma networks) may confound the observed associations. We sought to mitigate this by excluding high-resource sites and only including non-LMIC institutions when they had apparent resource limitations (Supplementary Tables S1 and S2). We also conducted LMIC-only sensitivity analysis, which confirmed that our main results remained consistent. Nonetheless, residual confounding by national wealth and health system strength is likely to persist.
This analysis contributes key data to the broader understanding of low-resource neurosurgical care. While scarcely reported, the median injury-to-arrival time observed stretched far beyond the critical 2-h window in which most TBI deaths occur. 71 This delay was particularly reported in Africa, supporting findings suggesting severe access limitations to timely neurosurgical care across sub-Saharan Africa.62,67 Given that TBI often serves as an entry point to requiring neurosurgical services, evaluation delays suggest wide-spanning access disparities.1,2,8,22,29 While this review primarily targeted LMICs, some included institutions were located within upper-middle-income countries but operated in clearly defined low-resource subnational settings. Their inclusion was based on documented infrastructure limitations—such as lack of neurosurgical services, absence of imaging, or inadequate ICT—rendering them appropriate for inclusion in the scope of this review. Our findings further validate TBI as a lens through which broader neurosurgical care gaps can be analyzed and addressed.
This review has several limitations. Heterogeneity in definitions and reporting standards across studies introduced variability, which we addressed through broad categorization and standardization of implementation and outcome measures. Our data were primarily urban-centric and may underrepresent rural deficiencies, and reporting bias may favor institutions with more robust data infrastructures.3,11,57 Future studies should target data within rural contexts and assess related treatment delays.11,31,32,42 Moreover, this study is observational in design, and while regression and machine learning models adjusted for covariates such as GCS, the identified associations do not imply causation. Additionally, it is important to note that although several factors were significantly associated with improved outcomes, this study design cannot prove causality. As reflected in the NHLBI assessment, the evidence base is comprised primarily of fair-quality observational studies, with good-quality multicenter cohorts supporting key inferences and a small number of poor-quality descriptive reports providing contextual system information (Supplementary Table S3). Furthermore, our risk-of-bias evaluation using the ROBINS-I tool revealed that most studies were at moderate risk of bias across several domains, with a subset at serious risk due to missing data and outcome reporting. Only seven of the included studies achieved a uniformly low risk of bias. This highlights that while the direction of associations was robust in sensitivity analyses, the overall certainty of evidence remains moderate. The findings in this study should be viewed as associations rather than conclusive evidence of effect. At this foundational stage, they provide a critical platform for future prospective and experimental research aimed at establishing causality and strengthening these results. Such work will be essential for informing policy and guiding standard-of-care interventions in resource-limited settings. Ultimately, even at this early stage, our review provides a compelling framework: health systems infrastructure—particularly EMRs, care standards, and digital connectivity—emerges as a potentially powerful driver of improved neurosurgical intervention capacity and patient survival in low-resource environments.
Conclusion
This systematic review demonstrates that strategic implementation of digital health infrastructure is associated with enhanced neurosurgical care outcomes following TBI in low-resource settings. While workforce limitations remain a significant barrier in global neurosurgery, these findings suggest that strategic, system-level investments are associated with improved neurosurgical capacity and outcomes, though causal inferences cannot be definitively drawn from observational data and may reflect broader systemic wealth and care readiness. Despite this, addressing these deficits through actionable interventions has the potential to be critical in narrowing the divide in global care standards and improving the quality of neurosurgical care and knowledge sharing worldwide.
Transparency, Rigor, and Reproducibility Statement
This systematic review was conducted in accordance with the PRISMA 2020 guidelines. The review protocol was developed a priori (objectives, eligibility criteria, data extraction plan, and analytic methods) but was not preregistered in PROSPERO because it encompassed both clinical and health systems domains, which did not align cleanly with registry formats. All planned objectives and methods were nevertheless defined a priori and consistently adhered to throughout. A dual-phase search strategy was performed across PubMed, Embase, and Scopus in October 2023 to identify studies reporting on neurosurgical care and digital health infrastructure in LMICs. The complete search strategy and search terms are provided in Supplementary Table S1.
After removal of duplicates, 306 unique records were screened. Two independent reviewers (C.S.R. and J.J.S.) conducted title and abstract screening using Rayyan. Conflicts were resolved through consensus discussion. A total of 78 full-text articles were assessed for eligibility, resulting in the inclusion of 50 studies representing 52 unique institutions across 21 LMICs. Inclusion and exclusion criteria are detailed in Supplementary Table S2. No automation tools were used during the screening or data extraction phases.
Data were extracted using a standardized, piloted extraction template. Extracted variables included TBI severity (GCS), intervention types, time to neurosurgical care, and patient mortality. System-level variables included EMR presence, internet/information and communication technology (ICT) access, and presence of formal institutional care protocols. Data were manually entered and verified by two independent reviewers.
Categorical comparisons were conducted using chi-square tests, while nonparametric comparisons utilized Kruskal–Wallis tests. Associations between health infrastructure and post-TBI outcomes were modeled using GCS-adjusted linear regression. To assess the predictive value of neurosurgical capacity for mortality, we developed an XGBoost machine learning classifier trained with stratified fivefold cross-validation and SMOTE to address class imbalance. Performance was evaluated using the mean area under the ROC curve (AUC). All analyses were conducted using Python v3.10.
Due to data heterogeneity across international sources, a relaxed significance threshold of p < 0.1 was used for exploratory inference. Risk of bias was assessed using ROBINS-I and the NHLBI 14-item tool; results are presented in Figure 5 and Supplementary Table S3. No human subjects were directly involved in this research. All data were derived from publicly available publications, and therefore, ethical approval was not required.
All data, code, and models used in this analysis will be deposited in a FAIR-compliant public repository and made freely available under a Creative Commons Attribution 4.0 International License (CC-BY 4.0) upon publication and request.
Authors’ Contributions
C.S.R.: Conceptualization, methodology, formal analysis, investigation, data curation, writing—original draft, visualization, and project administration. J.J.S.: Methodology, data curation, writing—review and editing, and validation. C.N.: Data curation, writing—review and editing, software, and visualization. V.M.L.: Supervision, writing—review and editing, resources, and validation. All authors have reviewed and approved the final article and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgments
The authors would like to thank EMERGE (Empowering Medical Education and Research for Global Equity) for their continued contributions.
Author Disclosure Statement
The authors declare no conflicts of interest relevant to this study. No financial relationships, personal activities, or affiliations influenced the development, execution, or publication of this article.
Funding Information
This research received no external funding from public, commercial, or not-for-profit agencies.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.