
Abstract
Repetitive head impacts (RHIs) in soccer have been associated with long-term risk for neurodegenerative disease. The pathophysiology is largely unknown. This study aims to investigate alterations in cerebral blood flow (CBF) in athletes exposed to RHI compared with athlete controls (CTL). Given that females are known to exhibit higher CBF than males, we also explore sex-specific differences. Finally, we investigate the relationship between CBF and neuropsychological functioning and RHI measures. This study includes 82 amateur athletes (mean age 22.8 ± 1.6 years; 48.9% female). Participants underwent 3T magnetic resonance imaging and completed neuropsychological testing, including questionnaires on stress, resilience, and sleep quality, and computerized assessment of executive function, memory, and processing speed. CBF was assessed using MR pulsed arterial spin labeling. Analysis of covariance was applied to assess the effect of RHI exposure and sex on CBF. Associations between CBF and neuropsychological functioning were analyzed using linear regression models. The analysis was conducted hierarchically, beginning with global gray matter CBF (level 1), followed by cortical and deep gray matter (level 2), and finally brain lobes (level 3). Correction for multiple comparisons was applied at each hierarchical level using false discovery rate, with a significance threshold set at p < 0.05 after correction. We found higher CBF in athletes with RHI exposure (RHI group) compared with athletes with <5 years of exposure to RHI (CTL group; Δ 95% confidence interval [95% CI] = 3.9 [0.5, 7.3] mL/100g/min, p = 0.027). Female athletes with RHI exposure exhibited higher CBF in the global gray matter compared with female CTL (Δ[95% CI] = 6.6 [1.6, 11.5] mL/100g/min, p = 0.013). Among males, individuals with RHI exposure demonstrated higher CBF in the occipital lobe compared with male CTL (Δ[95% CI] = 4.9 [0.3, 9.5] mL/100g/min, p = 0.047). There were no statistically significant associations between CBF and neuropsychological functioning. In the RHI group, years of soccer play were positively associated with whole-brain CBF. Results from this study suggest an association between RHI exposure and higher CBF, a measure of brain activity. Furthermore, we report sex-specific patterns of higher CBF in individuals exposed to RHI, with more widespread elevated CBF in women and more localized higher CBF in men. While these findings highlight the importance of investigating sex-specific effects, there were no associations between CBF and neuropsychological functioning. Future studies are warranted to determine the clinical relevance of the observed sex-specific effects to RHI.
Keywords
Introduction
Repetitive head impacts (RHIs) in soccer have been associated with later-life neurodegeneration, yet the underlying mechanisms remain poorly understood.1,2 Moreover, most studies to date are based on former professional athletes, whereas studies on active amateur athletes remain sparse.3,4 Sensitive measures to detect subtle and early brain changes associated with RHI are currently lacking.3,5–7 Previous studies have investigated the effects of RHI in soccer players, highlighting both acute and long-term changes in brain structure and function.8–13 These findings contribute to the growing body of evidence linking RHI to neurovascular and neurodegenerative changes.14–17 Cerebral blood flow (CBF) serves as a proxy for brain perfusion and is closely coupled with cerebral metabolic rate. 18 Thus, alterations in CBF may reflect underlying changes in cerebrovascular function and regulation, which are closely linked to metabolic demands and may serve as a sensitive marker for detecting subtle brain alterations following RHIs.19–22
Arterial spin labeling (ASL), a magnetic resonance imaging (MRI)-based technique that uses labeled blood–water of the brain-feeding arteries as an endogenous tracer, can be applied to assess CBF.19,23 This technique has been utilized in studies investigating the effects of RHI, revealing findings such as increased regional CBF postseason in male American football players.20–22 Specific regions, including the pre- and postcentral gyri, superior parietal lobule, and inferior and middle frontal gyri, demonstrated significant increases in relative CBF (rCBF). 21 Similarly, within-season increases in rCBF in the occipital lobe were observed in male football players compared with volleyball players, with these changes persisting for up to 6 months postseason. 22 Notably, these studies employed a hierarchical analysis strategy, examining global, cortical, and deep gray matter, and lobar measures to systematically assess CBF changes. This stepwise approach is critical as it enables the detection of both diffuse perfusion alterations across the whole brain and more localized, region-specific changes, which may reflect distinct patterns of vulnerability to RHI. This hierarchical approach provides a comprehensive evaluation of cerebrovascular changes, capturing global effects that may indicate overall brain health impacts while also identifying regional changes in the lobes. This method ensures a systematic assessment of whether localized effects occur within the context of broader cerebrovascular alterations, enhancing the understanding of RHI’s effect on brain perfusion. However, studies that used ASL to assess CBF were small in sample size, and the majority included male athletes only, thus leaving a relevant gap in our understanding of potential sex-specific effects of RHI on CBF.20–22
Previous neuroimaging studies using other methods have revealed sex-specific differences in the brain’s response to RHI, with female athletes exhibiting distinct alterations in brain metabolites, activity levels, and white matter integrity compared with males.24–27 General sex differences in CBF are also well-documented in the normal population. Recent studies employing ASL techniques have consistently shown higher CBF in females throughout the lifespan.28–31 However, no studies to date have specifically investigated sex differences in CBF among individuals exposed to RHI, leaving this an important area for further research.
To comprehensively assess the effects of RHI and sex on CBF, we employed a hierarchical analysis strategy, examining global, deep versus superficial, and lobar measures. This stepwise approach enables the detection of both diffuse perfusion alterations across the whole brain and more localized, region-specific changes, which may reflect distinct patterns of vulnerability to RHI. Such an approach is particularly relevant given prior reports of perfusion differences in specific cortical regions, including the pre- and postcentral gyri and occipital lobe, and allows for a systematic evaluation of whether these localized effects occur in the context of broader cerebrovascular alterations.
The main aim of this study was to investigate the effects of RHI exposure on CBF in individuals participating in amateur sports (i.e., soccer). To this end, we compare athletes with substantial RHI exposure (i.e., more than 5 years) to athletes without substantial exposure. In addition, we test whether CBF in soccer players is associated with specific RHI exposure measures. We also assess potential sex-specific differences in the effects of RHI on CBF. Finally, we explore the relationship between CBF and neuropsychological functioning.
Methods
Participants
NEUROFIT is a prospective, monocentric, cross-sectional research study of young soccer players exposed to RHI and noncontact athlete controls (CTL) aged 20–25 years. All participants engaged in at least three regular training sessions per week in their respective sport. To ensure that comparisons between the RHI and CTL groups are not confounded by differences in physical activity levels, control participants were recruited from noncontact sports. These included fitness/gym (11), volleyball (4), cycling (3), basketball (2), field hockey (3), climbing (1), dance (2), handball (2), running (3), tennis (5), gymnastics (3), swimming (1), fencing (1), horseback riding (1), and rowing (1). The study aims to characterize the effects of exposure to RHI while participating in soccer on neuropsychological functioning (including stress, resilience, sleep quality, executive function, memory, and processing speed), brain structure, diffusion, perfusion, elasticity, as well as biochemistry using multisequence MRI.
A total of 112 participants are enrolled in NEUROFIT (Fig. 1). For this study, we included 96 participants based on the following criteria: For the RHI group: individuals with at least 5 years of soccer training and current participation; for the CTL group: individuals with <5 years of soccer training and no current participation. Participants who did not meet these criteria, such as those with 5 years of experience but no active participation or those currently playing but without at least 5 years of prior training, were excluded.
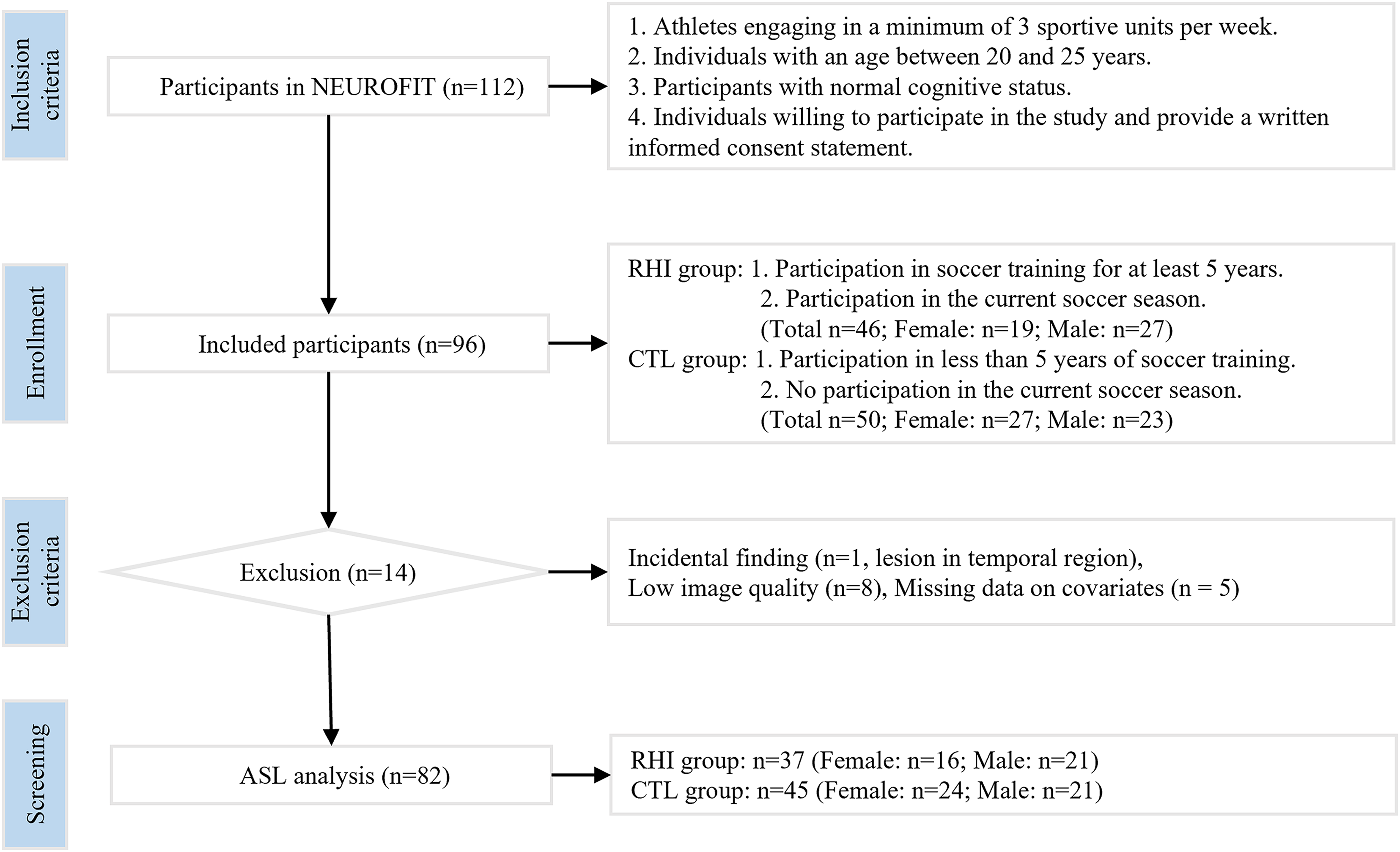
Participant inclusion flowchart. RHI group: individuals with at least 5 years of soccer training and current participation. CTL group: individuals with <5 years of soccer training and no current participation. CTL, controls; RHI, repetitive head impact.
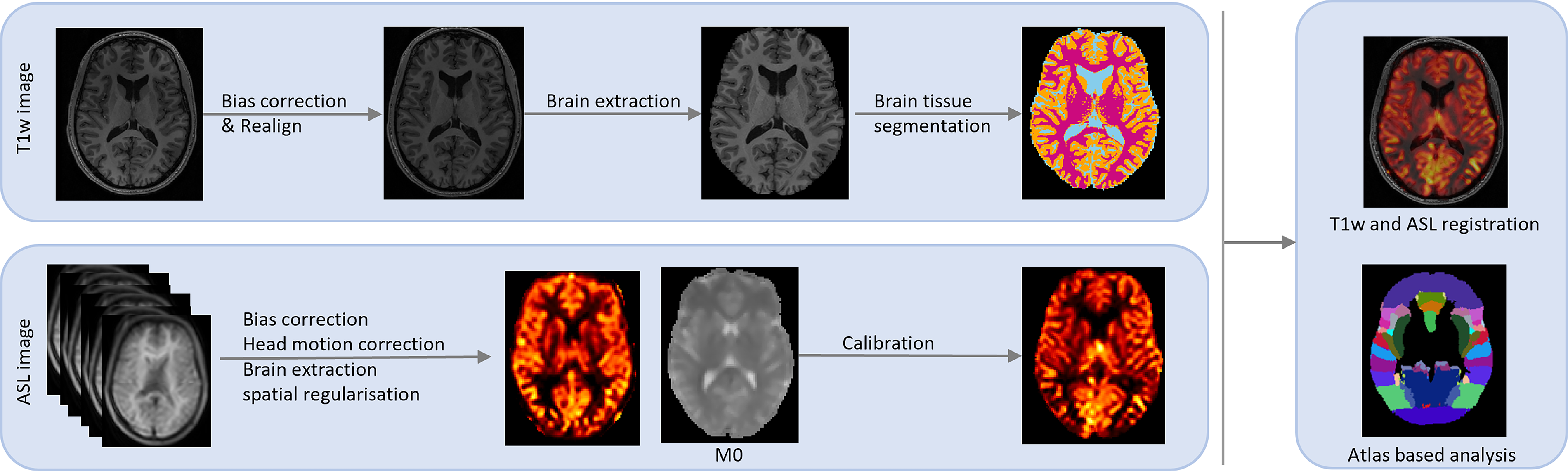
Perfusion image processing pipeline, comprising T1-weighted images and ASL data. Structural processing involved realignment, bias correction, brain extraction, and registration to Montreal Neurological Institute (MNI) template space using FSL. ASL data preprocessing included motion correction, bias correction, brain extraction, and registration to T1 space and subsequently to MNI space. CBF atlas-based analysis was performed using the oxford_asl package. ASL, arterial spin labeling; CBF, cerebral blood flow.
Of the 96 participants, 9 had to be excluded due to incidental finding on MRI (n = 1, a lesion located in the temporal region) or low image quality (n = 8) (Fig. 1). An additional five participants were excluded due to missing data on key covariates (age, years of education, body mass index [BMI], or mean arterial pressure [MAP]). Hence, the sample size analyzed in this study was 82. The RHI group included 37 soccer players (16 females and 21 males), whereas the CTL group included 45 individuals engaged in noncontact sports (24 females and 21 males). Detailed inclusion and exclusion criteria are provided in Figure 1. The study protocol was approved by the ethics committee of the Medical Faculty at Ludwig-Maximilians-University Munich (IRB approval number 20-1054). All participants provided written informed consent prior to inclusion in the study.
Demographics and neuropsychological tests
Demographic information included sex, age, education (in years), BMI (in kg/m2), MAP (in mm Hg), and resting heart rate (via actigraphy; in beats per minute (BPM)). MAP and heart rate were measured before the MRI scan, whereas participants were in a calm and resting state. Neuropsychological tests included cognitive performance and psychological assessments.
Cognitive performance was assessed using a computerized testing battery of digital cognitive tests (Cogstate Ltd.). The Cogstate battery was a well-validated computerized cognitive assessment tool that targets cognitive domains (e.g., attention, processing speed, and memory) highly relevant to RHI-related impairments.8,32 The tests included Continuous Paired Associate Learning (CPAL), Detection (DET), Groton Maze Learning (GML), Groton Maze Learning Recall (GMR), Identification (IDN), Set Shifting (SETS), and Two-Back (TWOB). Executive function, memory, and speed scores were derived from respective cognitive tests. The executive function was calculated as the mean of z-scores from GML, SETS, and inverted TWOB. Memory scores were determined by averaging z-scores from GMR and CPAL. Speed scores were calculated by averaging z-scores from DET and IDN. Lower z-scores indicated better performance.
Psychological evaluations included the Perceived Stress Scale (PSS), the Connor–Davidson Resilience Scale (CD-RISC-10), and the Pittsburgh Sleep Quality Index (PSQI). The PSS assesses perceived stress with scores ranging from 0 to 40, where 0–13 indicates low stress, 14–26 moderate stress, and 27–40 high stress. 33 The CD-RISC-10 measures psychological resilience, with higher scores indicating greater resilience; scores range from 0 to 40, with a reported general population mean (±standard deviation) of 32.1 ± 5.8. 34 The PSQI evaluates subjective sleep quality over the past month, yielding a total score from 0 to 21; higher scores reflect poorer sleep quality, and a global score above 5 is typically used to indicate poor sleep. 35
We also collected data on potential confounding factors, including alcohol intake, caffeine intake, nicotine use, history of diagnosed concussion, years since concussion, time since last intense training (in days), and time of testing (hour of day).
MRI acquisition
MRI scans were performed using a 3T MRI scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) equipped with a 32-channel head coil. T1-weighted images were obtained using a Magnetization Prepared-RApid Gradient Echo sequence, with a repetition time (TR) of 2530.0 ms, echo time (TE) of 3.35 ms, and isotropic voxel size of 1 mm. The scan covered a field of view of 256 mm, with 176 slices at a thickness of 1 mm. The ASL images were acquired using a three-dimensional fast spin-echo pulsed ASL (PASL) sequence with a field of view of 23 cm, slice thickness of 3.5 mm, and 1.8 × 1.8 × 3.5 mm voxel size. The PASL sequence employed a TR of 4600 ms, TE of 15.64 ms, label duration of 800 ms, postlabeling delay (PLD) of 1000 ms, inversion time of 1800 ms, and a control-label sequence repeated four times with Flow-sensitive Alternating Inversion Recovery (FAIR QII). An equilibrium magnetization (M0) image was collected with a field of view of 23 cm, slice thickness of 3.5 mm, and 1.8 × 1.8 × 3.5 mm voxel size. The sequence employed a TR of 7500 ms, TE of 15.64 ms, bolus duration of 800 ms, and inversion time of 7000 ms. Our study focused on absolute CBF to provide a direct and comprehensive assessment of cerebral perfusion. The CBF maps were derived using established formulas from previous studies (Formulas 1–3).36,37



Image data processing
T1-weighted and ASL data were first converted using the dcm2nii software. 38 Quantitative CBF maps were generated using the BASIL (Bayesian Inference for Arterial Spin Labeling) toolkit within FSL (version 6.0.6.5, FMRIB Software Library).39,40 Structural T1-weighted images were first processed using fsl_anat to perform motion correction, realignment, bias correction, brain extraction, bias-field correction, and tissue segmentation. For each subject, the anatomical image was used to guide ASL quantification via the oxford_asl (v4.0.29) package. 41 Two pipelines were implemented: a standard CBF quantification and an atlas-based analysis. Both pipelines included motion correction, spatial regularization, and partial volume correction using tissue probability maps derived from structural segmentation. Labeling was assumed to be control-tag (ct) with a time-encoded scheme (tis), and the kinetic model was defined using the following parameters: bolus duration = 0.8 sec, PLD = 1.0 sec, TR = 4.6 sec, labeling efficiency = 0.98, and T1 of blood = 1.65 sec. Calibration was performed using an M0 image acquired with the same geometry as the ASL sequence. The reference tissue for calibration was CSF, with a T1 of 4.3 sec, T2 of 750 ms for CSF, and 150 ms for blood. Region-based analysis was conducted using the –region-analysis option in oxford_asl, which extracts regional CBF values from predefined anatomical regions of interest. Quality control procedures included visual inspection for motion- and labeling-related artifacts, evaluation of CBF signal distributions to identify statistical outliers, and exclusion of datasets exhibiting severe motion artifacts or failed registration. These standardized procedures ensured reliable and reproducible CBF estimates across all analyses. The detailed perfusion image processing workflow is summarized in Figure 2.
We conducted atlas-based analysis in native space using the oxford_asl package, which allowed for regional assessment of CBF in anatomically predefined brain areas (in mL/100 g/min), including global gray matter (level 1), cortical gray matter and deep gray matter (level 2), and at the lobe level (level 3, including frontal lobe, parietal lobe, temporal lobe, and occipital lobe), using the Harvard-Oxford standard atlas.
For the hierarchical ASL analyses, region-specific brain masks were generated in native space using the regional analysis function of the Oxford ASL toolbox (asl_oxford). These masks were combined to create lobar masks, with deep gray matter masks defined for subcortical structures, whereas global and cortical gray matter masks were also produced using the same pipeline to ensure consistency across analysis levels.
Statistics
Statistical analyses were performed using R (version 4.3.2; https://www.r-project.org/). 42 Covariates across analysis of covariance (ANCOVA) models included age, years of education, BMI, and MAP. MAP was included as a covariate in all ANCOVA and regression models to account for potential vascular influences on CBF, given evidence that higher MAP, even within normative ranges, 43 can be associated with reduced cerebral perfusion and may reflect impaired autoregulation in individuals with prior head impacts.44,45 Standard model diagnostics were performed for all ANCOVA and multiple regression analyses, including visual inspection of residual plots to assess linearity and homoscedasticity, Q–Q plots to evaluate normality of residuals, and Levene’s test to confirm homogeneity of variances.
Group comparisons in demographic data
Group differences between RHI and CTL, as well as between males and females, in demographic variables were assessed using independent t-tests (ttest function, rstats package 42 ). Group comparisons for neuropsychological functioning were conducted using ANCOVA (emmeans_test function from the R package emmeans 46 ). The 95% confidence intervals (CIs) were derived from linear model summaries using the broom::tidy() function.
To evaluate whether potential confounding factors, including alcohol intake, caffeine intake, nicotine use, history of diagnosed concussion, years since concussion, time since last intense training (in days), and time of testing (hour of day), have any significant effect on CBF, we conducted separate linear regression models with whole-brain CBF as the dependent variable and each factor as the predictor. Statistical significance was set at p < 0.05.
RHI and sex effect on CBF
To examine the effect of group (RHI vs. CTL) on CBF, we compared the RHI with the CTL group using ANCOVA, adjusting for sex, age, years of education, BMI, and MAP. Similarly, to assess sex differences in CBF, we performed ANCOVA comparing females and males, adjusting for group (RHI vs. CTL), age, years of education, BMI, and MAP. To investigate whether sex moderates the effect of RHI on CBF, we performed a two-step analysis. First, we tested the interaction between group (RHI vs. CTL) and sex using ANCOVA while adjusting for age, years of education, BMI, and MAP. Second, we conducted post hoc comparisons between RHI females and CTL females, RHI males and CTL males, RHI females and RHI males, and CTL females and CTL males, with covariate adjustments.
All ANCOVA tests were performed at three hierarchical levels. Level 1 examined global gray matter, level 2 differentiated between cortical gray matter and deep gray matter, and level 3 analyzed CBF at the lobe level. Multiple comparisons were corrected for both the number of group comparisons and the number of regions tested at each level. False discovery rate (FDR) correction was applied using the adjust_pvalue function from the R package rstatix, with a significance threshold set at p < 0.05 after correction. 47
Association between CBF and neuropsychological functioning
To investigate the associations between CBF and neuropsychological functioning, including executive function, memory, and processing speed, PSS, CD-RISC-10, and PSQI, we employed multiple linear regression models (lm function from the R package stats 42 ). The models included whole-brain CBF as the dependent variable and neuropsychological functioning as predictors, adjusted for age, years of education, BMI, and MAP. Effect sizes (Cohen’s f2) were calculated to assess the strength of these associations. FDR correction was applied for the number of neuropsychological tests, with a significance threshold set at p < 0.05 after correction.
Association between CBF and RHI exposure measures
We examined associations between CBF and RHI exposure measures within the RHI group. These included age at start of playing soccer, age at start of heading practice, years of soccer play exposure, average duration of play per year, and frequency of play per week. Linear regression models were used to assess these relationships, with whole-brain CBF as the dependent variable and RHI exposure parameters as predictors, adjusted for age, years of education, BMI, and MAP. Multiple comparisons were corrected for the number of RHI exposure measures, with a significance threshold set at p < 0.05 after correction.
Results
Study population
Participant demographics are summarized in Table 1. No statistically significant differences were found between the RHI and CTL groups when considering all subjects (p > 0.05). However, sex differences were observed, with males having more years of education (Δ (95% CI) = 1 (0, 2) years, p = 0.015), a higher BMI (Δ (95% CI) = 1.6 (0.7, 2.5) kg/m2, p < 0.001), and a greater MAP (Δ (95% CI) = 7.8 (4.7, 10.9) mmHg, p < 0.001) compared with females.
Demographics and Neuropsychological Data
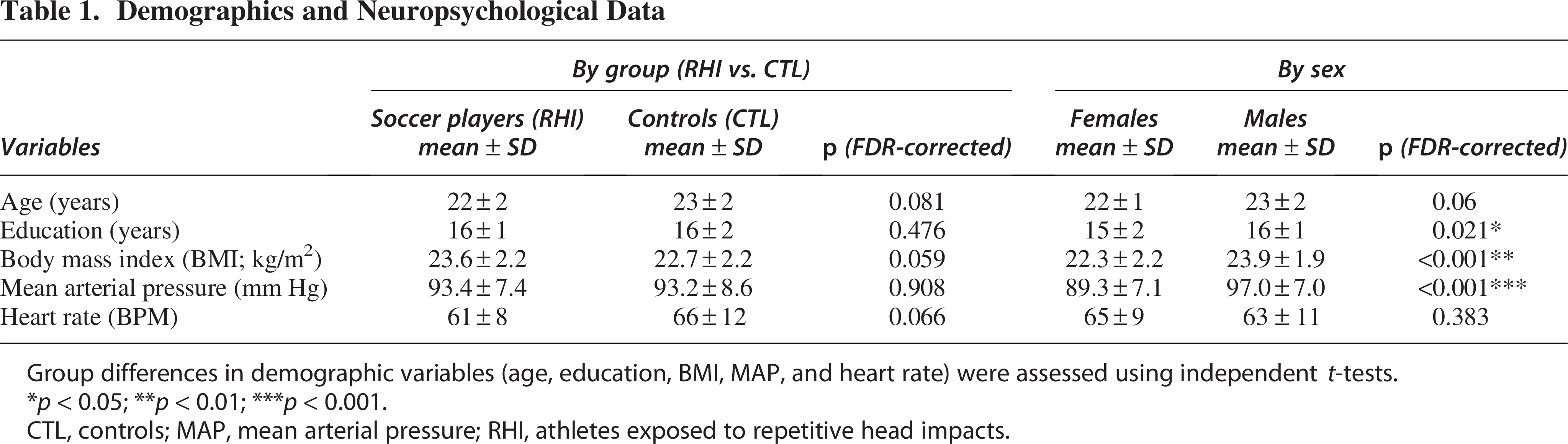
Group differences in demographic variables (age, education, BMI, MAP, and heart rate) were assessed using independent t-tests.
*p < 0.05; **p < 0.01; ***p < 0.001.
CTL, controls; MAP, mean arterial pressure; RHI, athletes exposed to repetitive head impacts.
None of the potential confounding variables (including alcohol intake, caffeine intake, nicotine use, history of diagnosed concussion, years since concussion, time since last intense training, or time of testing) was significantly associated with whole-brain CBF (p > 0.05). A detailed summary of estimated effects and corresponding p values for each factor is provided in Table 2.
Summary of Potential Confounding Variables
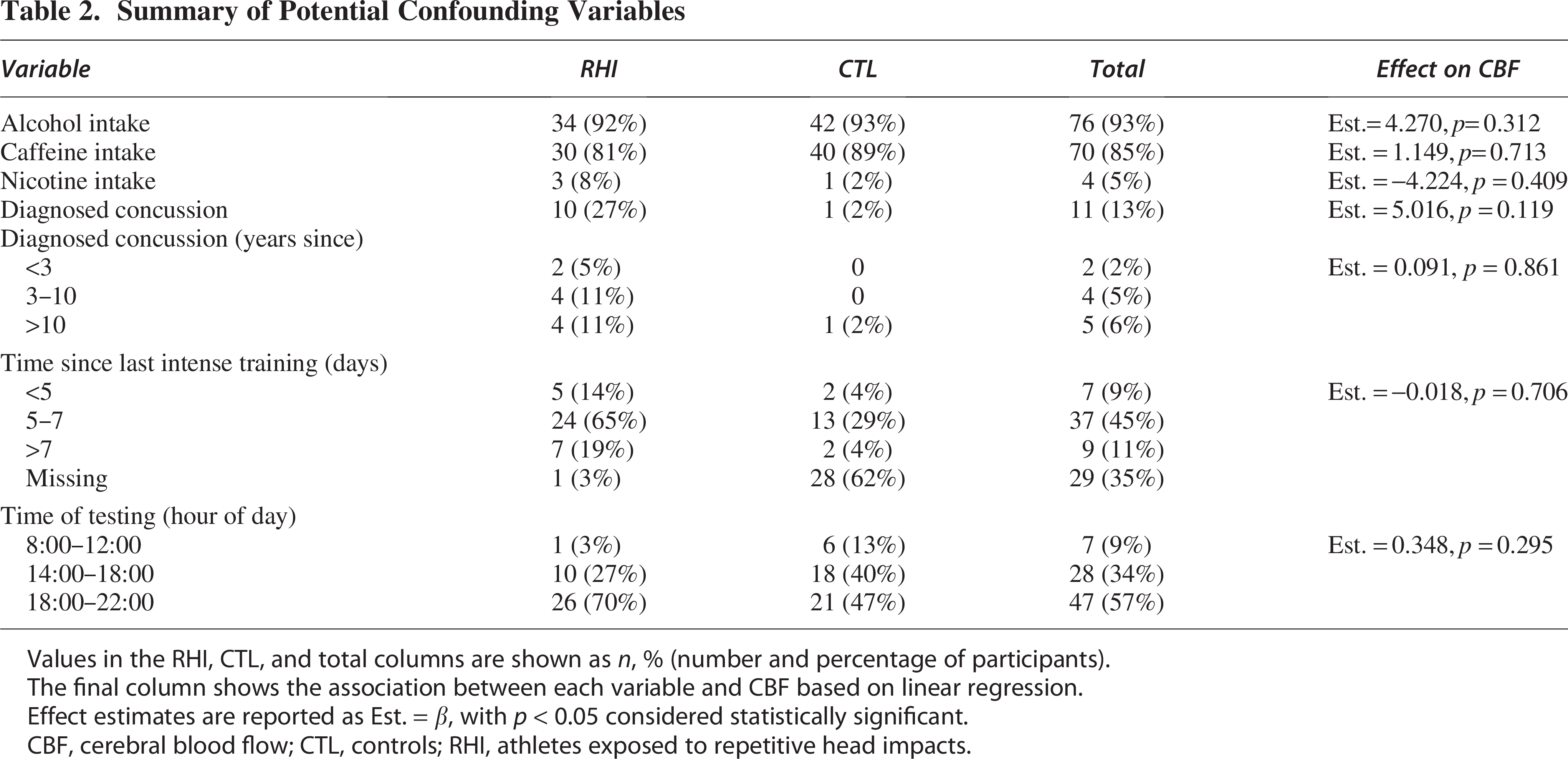
Values in the RHI, CTL, and total columns are shown as n, % (number and percentage of participants).
The final column shows the association between each variable and CBF based on linear regression.
Effect estimates are reported as Est. = β, with p < 0.05 considered statistically significant.
CBF, cerebral blood flow; CTL, controls; RHI, athletes exposed to repetitive head impacts.
CBF changes across group (RHI vs. CTL) and sex
Main effects of group (RHI vs. CTL) and sex
Analysis revealed statistically significant main effects of both group (RHI vs. CTL) and sex on CBF. More specifically, the RHI group exhibited higher CBF in global gray matter compared with the CTL group. At a more detailed level, the RHI group showed higher CBF in both cortical and deep gray matter. Regionally, higher CBF was observed in the occipital lobe (Table 3, Fig. 3).
Effects of Group (RHI vs. CTL) and Sex on CBF across Different Levels of Regions
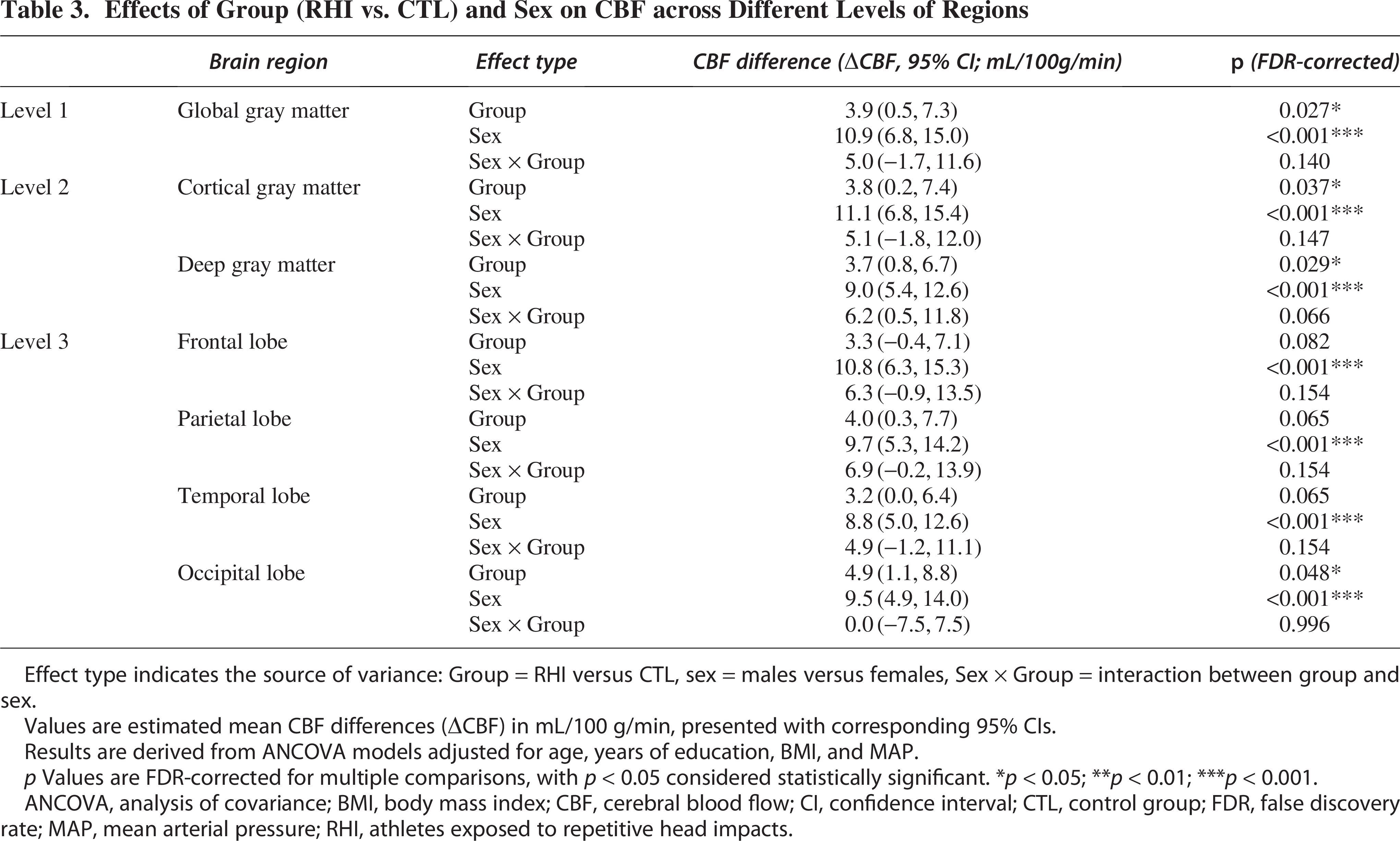
Effect type indicates the source of variance: Group = RHI versus CTL, sex = males versus females, Sex × Group = interaction between group and sex.
Values are estimated mean CBF differences (ΔCBF) in mL/100 g/min, presented with corresponding 95% CIs.
Results are derived from ANCOVA models adjusted for age, years of education, BMI, and MAP.
p Values are FDR-corrected for multiple comparisons, with p < 0.05 considered statistically significant. *p < 0.05; **p < 0.01; ***p < 0.001.
ANCOVA, analysis of covariance; BMI, body mass index; CBF, cerebral blood flow; CI, confidence interval; CTL, control group; FDR, false discovery rate; MAP, mean arterial pressure; RHI, athletes exposed to repetitive head impacts.
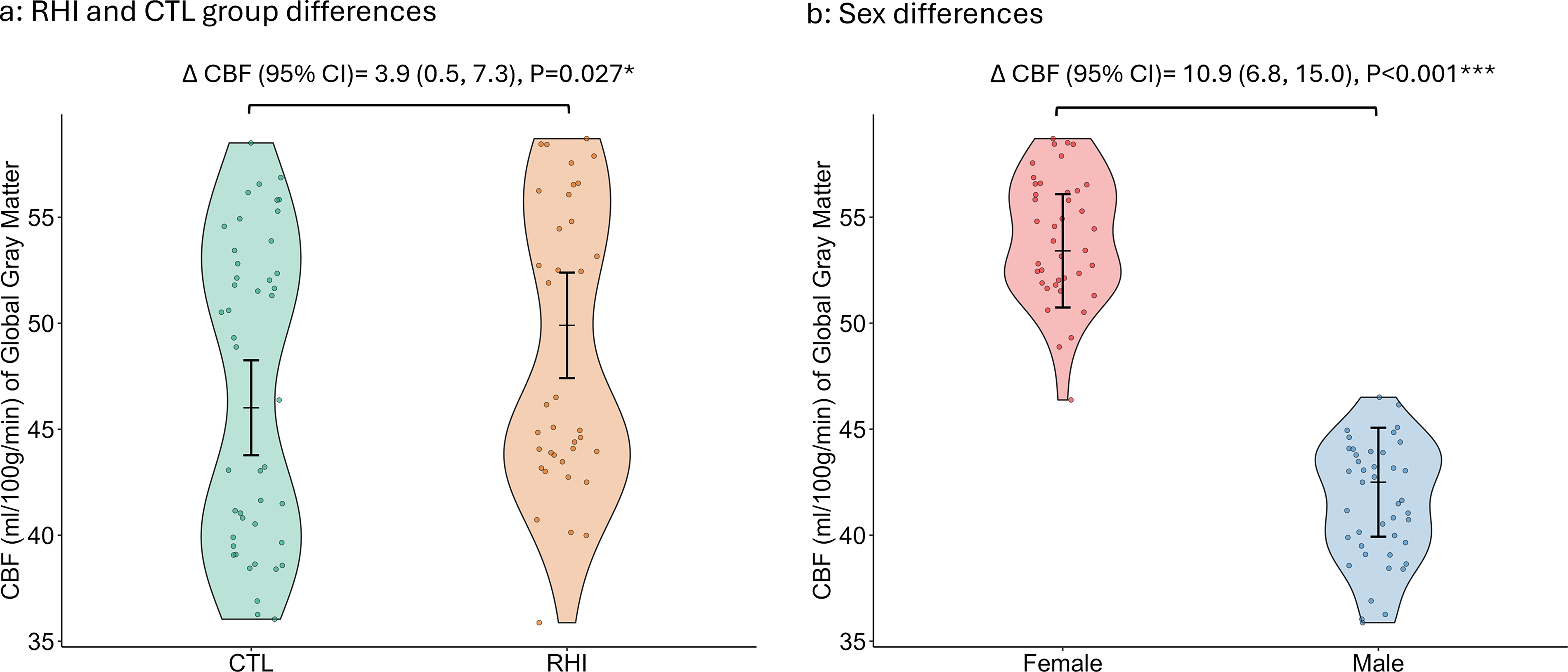
Similarly, a significant sex effect was found, with females exhibiting higher CBF in global gray matter compared with males across all levels of analysis (Table 3, Fig. 3).
Moderation effect of sex on the RHI effect on CBF
No statistically significant interaction between group (RHI vs. CTL) and sex was found at any level (Table 3). However, post hoc analysis revealed a sex-specific effect: in females, the RHI group had significantly higher global gray matter CBF compared with the female CTL group (Δ [95% CI] = 6.6 [1.6, 11.5] mL/100 g/min, p = 0.013) (Fig. 4). At level 2, the female RHI group also showed higher CBF in cortical gray matter (Δ [95% CI] = 6.6 [2.1, 11.1] mL/100 g/min, p = 0.007) and deep gray matter (Δ [95% CI] = 7.1 [2.5, 11.6] mL/100 g/min, p = 0.005). At level 3, higher CBF was observed in frontal lobe (Δ [95% CI] = 6.5 [1.6, 11.4] mL/100 g/min, p = 0.014), parietal lobe (Δ [95% CI] = 7.5 [2.6, 12.4] mL/100 g/min, p = 0.006), temporal lobe (Δ [95% CI] = 5.8 [0.9, 10.7] mL/100 g/min, p = 0.030), and occipital lobe (Δ [95% CI] = 5.5 [0.6, 10.4] mL/100 g/min, p = 0.038).
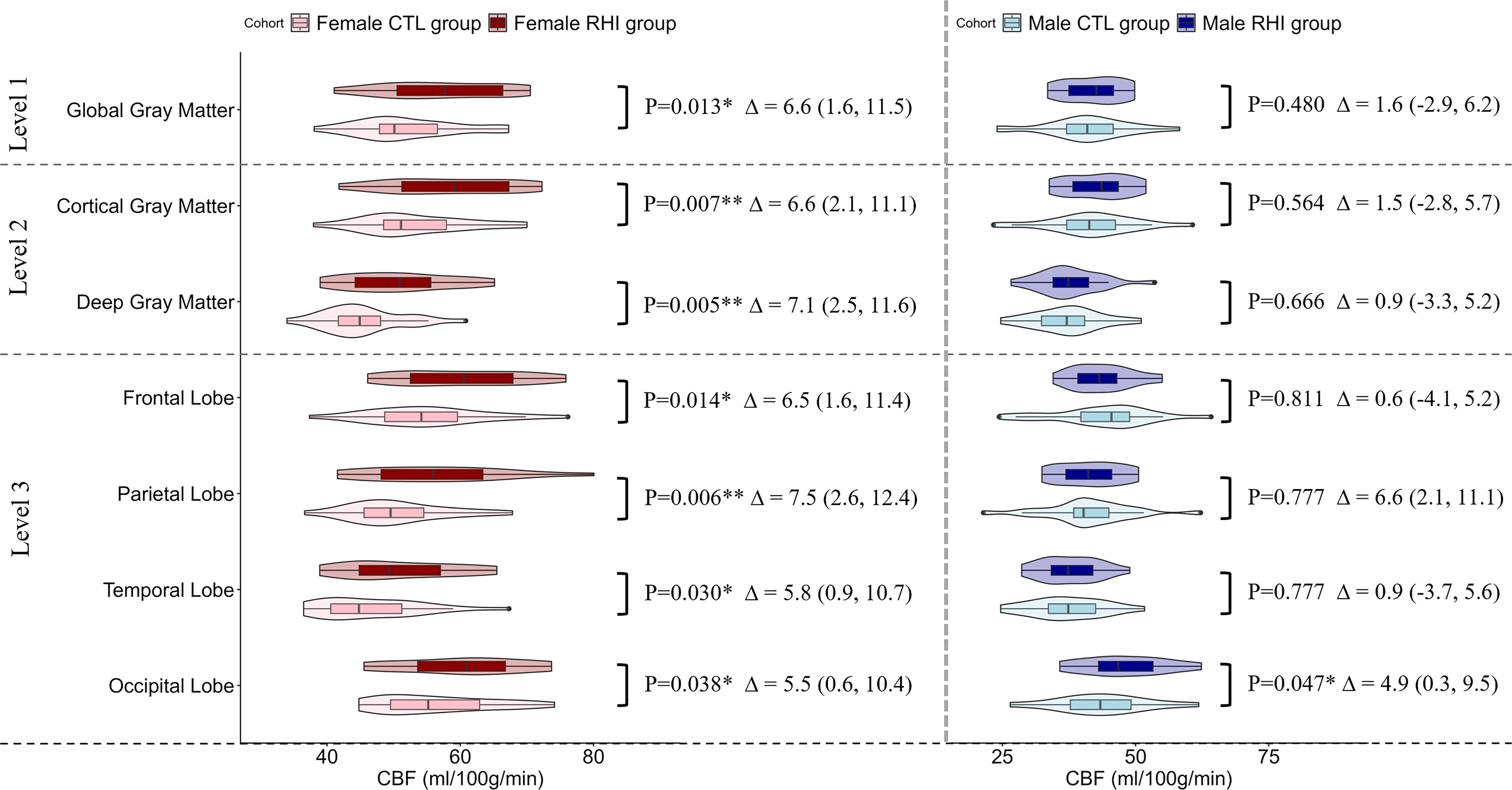
Post hoc comparisons of CBF between groups: The female RHI group showed higher CBF in the region levels 1 and 2 compared with the female CTL group, whereas no significant difference was observed between male RHI and male CTL groups. At the lobe level, females with RHI exhibited higher CBF across all lobes compared with controls, whereas, in males, increased CBF was observed only in the occipital lobe. ANCOVA was performed with age, years of education, BMI, and MAP as covariates. p values are FDR-corrected. Δ indicates group differences in CBF with 95% confidence intervals. ANCOVA, analysis of covariance; BMI, body mass index; CBF, cerebral blood flow; CTL, controls; FDR, false discovery rate; MAP, mean arterial pressure; RHI, athletes exposed to repetitive head impacts. *p < 0.05; **p < 0.01; ***p < 0.001.
In contrast, there were no statistically significant CBF differences found between male RHI and male CTL at levels 1 and 2. However, at level 3, the male RHI group exhibited higher CBF in the occipital lobe compared with the male CTL group (Δ = 4.9 [0.3, 9.5], p = 0.047).
Association between CBF and neuropsychological functioning
We found no statistically significant differences between the RHI group and the CTL group. There was also no statistically significant difference between males and females regarding neuropsychological functioning (Table 4). Additionally, there was no statistically significant association between neuropsychological functioning and CBF at the global gray matter level. Detailed results are provided in Table 4 and Figure 5.
Association Between CBF and Neuropsychological Outcomes
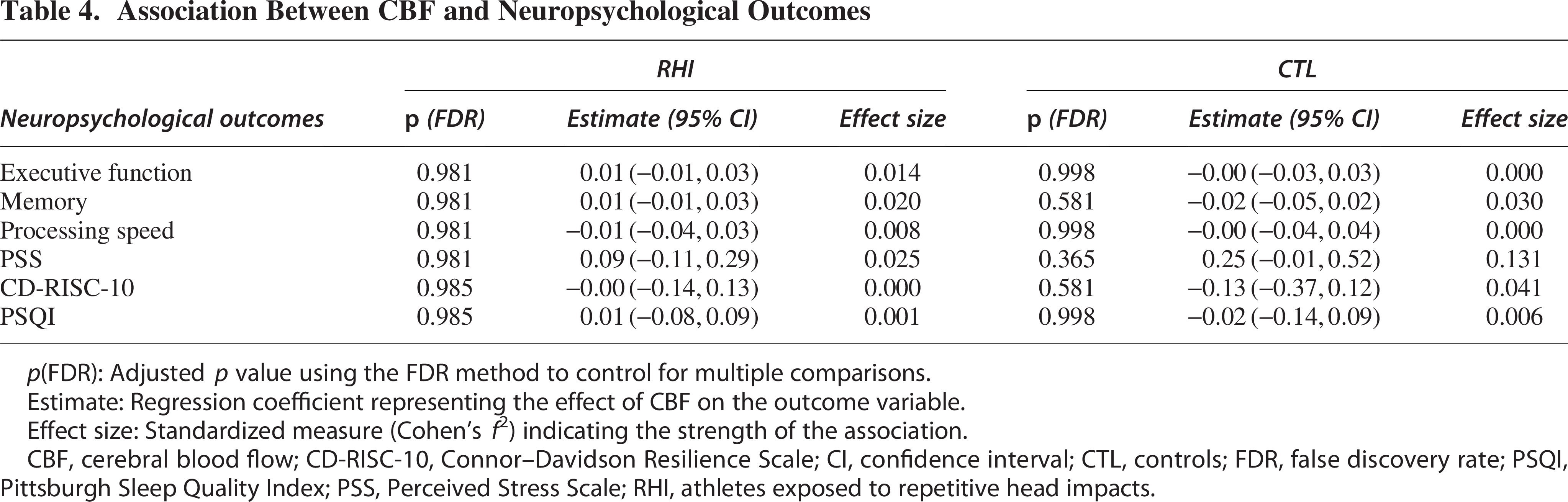
p(FDR): Adjusted p value using the FDR method to control for multiple comparisons.
Estimate: Regression coefficient representing the effect of CBF on the outcome variable.
Effect size: Standardized measure (Cohen’s f²) indicating the strength of the association.
CBF, cerebral blood flow; CD-RISC-10, Connor–Davidson Resilience Scale; CI, confidence interval; CTL, controls; FDR, false discovery rate; PSQI, Pittsburgh Sleep Quality Index; PSS, Perceived Stress Scale; RHI, athletes exposed to repetitive head impacts.
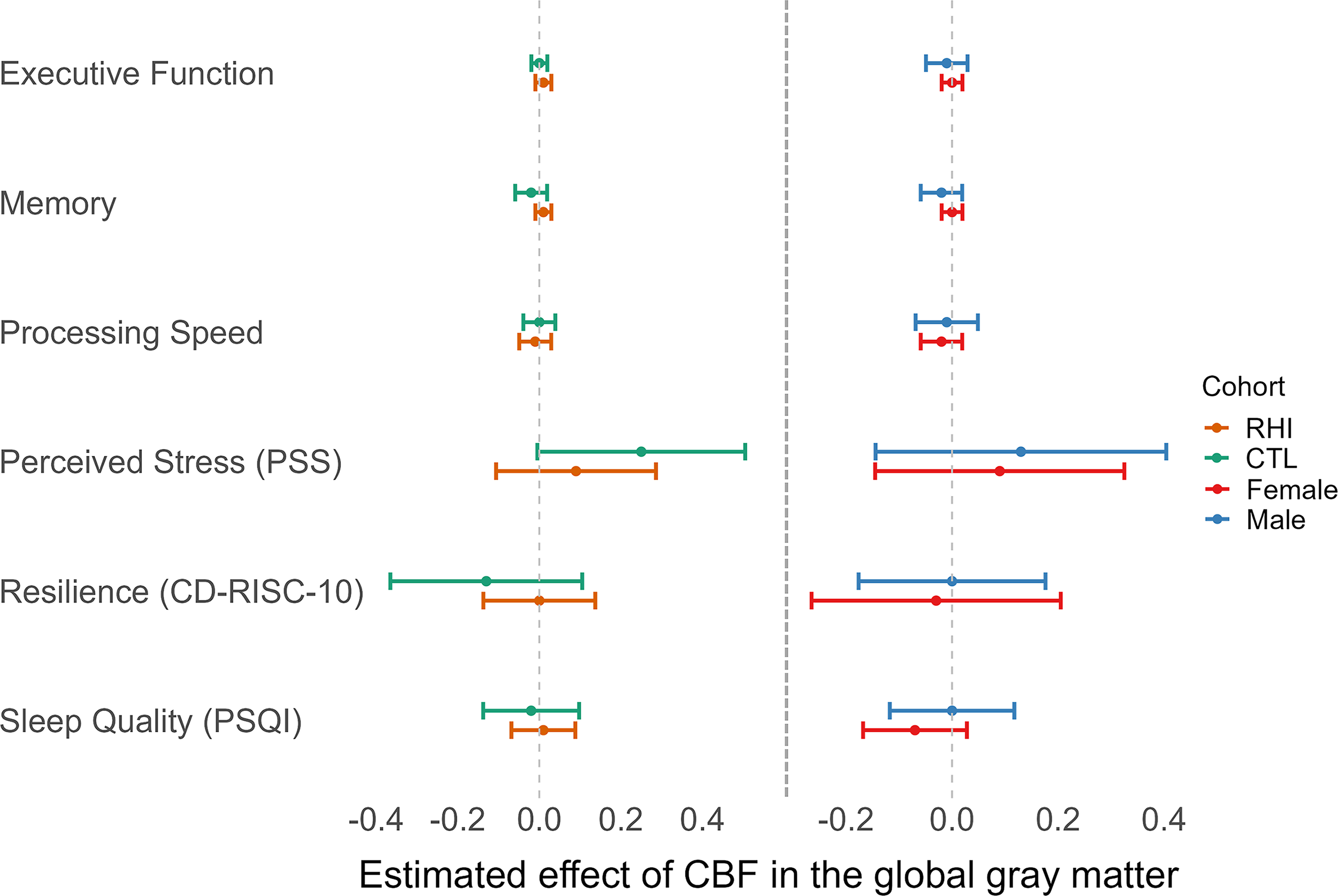
Associations between neuropsychological functioning and CBF. Each point represents the estimate ± 95% CI for each variable. Left: associations between neuropsychological functioning and whole-brain CBF in the RHI and CTL group. Right: associations between neuropsychological functioning and whole-brain CBF in female and male group. No statistically significant association was found. CBF, cerebral blood flow; CI, confidence interval; CTL, controls; RHI, athletes exposed to repetitive head impacts.
Association between CBF and RHI measures
Within the RHI group, male soccer players had significantly longer exposure to soccer play compared with female players (p = 0.005). A significant association was observed between years of soccer play and whole-brain CBF when analyzing the entire RHI group (Est. = −1.347, p = 0.041*) (see Table 5). However, when stratified by sex, this association was no longer statistically significant. Detailed results for the sex-specific analyses are presented in Figure 6.
RHI Exposure Measures in Amateur Soccer Players
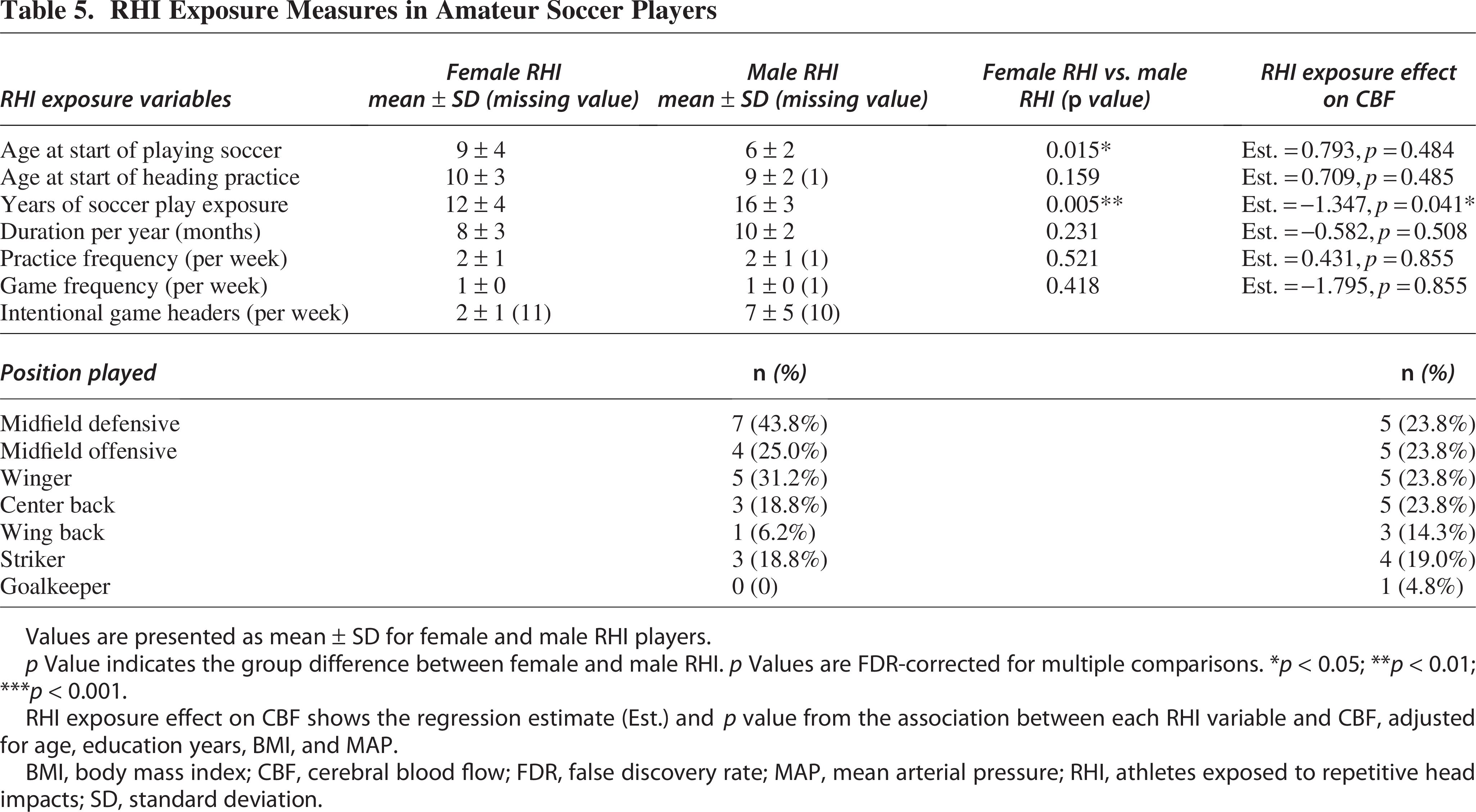
Values are presented as mean ± SD for female and male RHI players.
p Value indicates the group difference between female and male RHI. p Values are FDR-corrected for multiple comparisons. *p < 0.05; **p < 0.01; ***p < 0.001.
RHI exposure effect on CBF shows the regression estimate (Est.) and p value from the association between each RHI variable and CBF, adjusted for age, education years, BMI, and MAP.
BMI, body mass index; CBF, cerebral blood flow; FDR, false discovery rate; MAP, mean arterial pressure; RHI, athletes exposed to repetitive head impacts; SD, standard deviation.
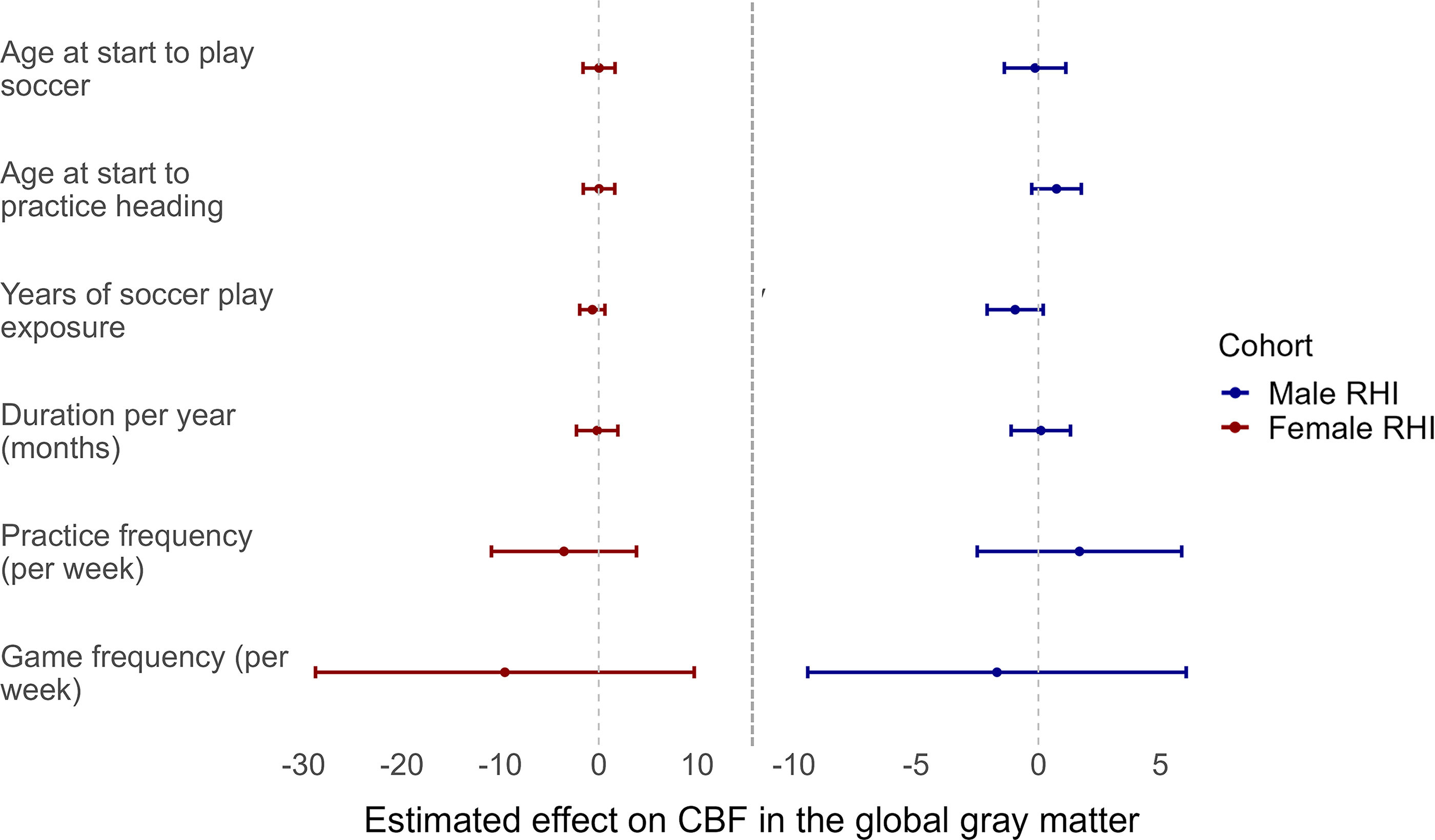
Associations between RHI measures and CBF. Each point represents the estimate ± 95% CI for each variable. Left: associations between RHI measures and whole-brain CBF in the female RHI group. Right: associations between RHI measures and whole-brain CBF in male RHI group. No statistically significant association was found. CBF, cerebral blood flow; CI, confidence interval; RHI, athletes exposed to repetitive head impacts.
Discussion
This study investigated the effects of RHI exposure on CBF, as well as sex-specific differences and associations between CBF and neuropsychological functioning. We found significantly higher CBF in females compared with males. More importantly, our findings reveal globally higher CBF in the RHI group compared with the CTL group across both sexes. Although no significant interaction between RHI exposure and sex was observed, post hoc analysis revealed that the RHI-related higher CBF was evident in females but not in males. Taken together, these findings suggest that RHI exposure and sex independently influence CBF, with potential sex-specific mechanisms underlying the observed differences. Of note, there was no statistically significant association between CBF and neuropsychological functioning. Future studies are needed to determine the clinical relevance of the observed sex-specific effects of elevated CBF associated with RHI.
Sex differences in CBF
In healthy populations, females are consistently reported to have higher CBF than males.28–31,48 Our study confirms these previous reports by demonstrating higher CBF in females compared with males on all three levels of analysis (global gray matter, cortical and deep gray matter, and brain lobes).
The physiological mechanisms underlying sex differences in CBF remain unclear, although sex hormones are likely to play a role in modulating CBF.49,50 Estrogen has been shown to upregulate endothelium-dependent, nitric oxide-mediated vasodilation, reducing cerebrovascular tone and increasing CBF, whereas testosterone is associated with higher cerebrovascular tone.49,50 Furthermore, females generally have higher cerebral metabolic rates for glucose and oxygen compared with males.29,51 This higher metabolic demand in females, coupled with lower hematocrit levels, could contribute to higher CBF. Lower hematocrit reduces oxygen-carrying capacity, necessitating higher CBF to meet oxygen demand. 52 Additionally, reduced hematocrit is associated with lower blood viscosity, which may result in increased blood flow velocity and, consequently, higher CBF. 29 Further research is required to fully understand the relative contributions of these factors to the observed sex differences in CBF.
Higher CBF in athletes exposed to RHI
Our findings demonstrate higher global gray matter CBF in the RHI group compared with the CTL group, especially among female athletes, potentially reflecting adaptive or stress-related vascular responses to RHI associated with contact sports.53,54
Although no previous studies have specifically identified CBF alterations in females exposed to RHI, reduced cerebrovascular reactivity in female soccer players has been reported, potentially leading to compensatory increases in CBF.55,56 Our findings are also in line with a previous study that reports sex differences in CBF after mild traumatic brain injury (mTBI): compared with males, females showed higher CBF in the left inferior frontal cortex at 1 month after mTBI. 57
In male soccer players, we observed higher CBF in the occipital lobe compared with male CTL. These findings align with prior longitudinal studies in athletes exposed to RHI.20–22 Male American football players showed increased global rCBF (reference region was the cerebellum) postseason relative to preseason.20,22 Additionally, male contact sport athletes (including football, ice hockey, and soccer) exhibited increased rCBF after the season, whereas noncontact sport players showed a decrease in rCBF (reference region was cortical gray matter) over the same period. 21 Of note, while rCBF provides a ratio of perfusion relative to a chosen reference region, absolute CBF measures perfusion without normalization, offering a direct assessment of blood flow dynamics. However, the accuracy of absolute CBF estimates is strongly dependent on the validity and robustness of the kinetic modeling assumptions used for quantification. Our study focused on absolute CBF to provide a direct and comprehensive assessment of cerebral perfusion.
The higher CBF in the RHI group may potentially reflect distinct cerebrovascular adaptations to head impacts. However, as the extent of these impacts was not quantified and the absolute differences between groups were small, their biological and clinical relevance remains uncertain. This adaptive vascular response may help maintain cognitive function under stress by increasing blood flow to meet metabolic demands in regions at risk of injury. 55 Altered cerebrovascular responses have been reported in both male and female amateur soccer players, supporting RHI-induced vascular dysregulation.55,58,59 Several mechanisms may underlie this alteration. First, RHI may lead to microvascular injury and endothelial damage, resulting in blood–brain barrier (BBB) disruption.60,61 These disruptions may trigger inflammatory responses and promote vasodilation, potentially mediated by nitric oxide production. Supporting this, animal studies on TBI have shown that hypermetabolism during the acute injury phase following cortical contusion is associated with increased CBF.62,63 Furthermore, vascular and BBB dysfunction may impair the regulation of vasoactive metabolites. Specifically, cytochrome P450 activity, which produces 20-HETE—a metabolite involved in vasoconstriction—may be reduced, whereas prostanoid receptors may become less sensitive to 20-HETE. 64 This disruption could contribute to sustained vasodilation and impaired cerebrovascular autoregulation. 64
Additionally, in women exposed to RHI, elevated progesterone levels may play a neuroprotective role, lowering perceived stress and increasing regional CBF following injury. 65 Despite these initial compensatory mechanisms, male athletes have been reported to experience CBF reductions in the months or years following the season’s end.22,66,67 This pattern suggests that the protective vascular adaptations observed during a period of ongoing RHI exposure, as investigated in this study, may diminish over time, potentially exposing athletes to greater vulnerability to neurovascular and neurodegenerative pathologies.
Of note, although subgroup analyses revealed that RHI females exhibited higher CBF across global gray matter compared with CTL females, whereas RHI males showed a significant CBF increase confined to the occipital lobe, the primary ANCOVA detected no significant sex-by-group interaction. These findings, while exploratory, may suggest sex-specific cerebrovascular responses to RHIs that warrant further investigation. Given the modest sample size and lack of a significant interaction effect, these results should be regarded as hypothesis-generating. Larger, adequately powered studies are needed to clarify whether these preliminary sex-specific patterns represent true physiological differences.
Associations between CBF and neuropsychological functioning
Of note, there was no statistically significant association between CBF and neuropsychological functioning. Previous research has reported inconsistent findings regarding the impact of contact sports on neuropsychological functioning.3,21,68–80 While some studies have identified changes in verbal memory from preseason to postseason in contact sport athletes,21,68 most report no statistically significant differences in these outcomes.69–73 Long-term studies, however, have shown impairments in neuropsychological functioning among retired male American football players.3,74–80 The stability of neuropsychological functioning observed in active soccer players may potentially reflect a protective mechanism due to higher CBF. Further studies are needed to investigate potential long-term sequelae of RHI-associated higher CBF.
Associations between CBF and RHI measures
In this study, we found a significant negative association between years of soccer play and whole-brain CBF in the RHI group (Table 5). Longitudinal studies indicate a biphasic CBF response to head impacts: Short-term exposure increases CBF, whereas long-term exposure is linked to reductions.21,22 Our findings align with this pattern, showing higher in-season CBF in the RHI group, yet a negative correlation with years of soccer play, suggesting cumulative microvascular changes from RHI.
However, when stratified by sex, this association was no longer statistically significant (Fig. 6). Prior research consistently reports higher CBF in females than males across age groups.28–31,48 Our study confirmed this, with female participants exhibiting higher CBF than males. Additionally, male soccer players reported significantly longer exposure to soccer play than females. Consequently, the negative association between years of play and CBF in the entire RHI group may be driven by males, who have greater exposure and lower baseline CBF, potentially confounding the overall findings.
The lack of a significant association within each sex suggests that years of soccer play alone may not substantially affect CBF, or that the sample size per sex was insufficient to detect such effects. Alternatively, factors such as the number, frequency, or severity of head impacts may have a greater influence on CBF. Years of play, as a proxy for cumulative RHI exposure, do not account for impact intensity or frequency, which vary by playing style, position, or competitive level. Future studies should use objective measures, such as wearable sensors, to quantify head impact exposure more accurately. These findings highlight the importance of considering sex differences when evaluating the effects of RHI measures on cerebral perfusion.
Limitations
First, the cross-sectional design limits the ability to infer causal relationships between RHI exposure and observed CBF alterations. Longitudinal studies are needed to differentiate between temporal changes in CBF and their potential long-term implications. Second, the sample size may limit the statistical power to detect interaction effects between RHI exposure and sex. Despite this limitation, our study is among the first to examine these sex-specific differences in CBF in the context of RHI, providing a foundation for future research with larger cohorts. Third, while ASL provides a noninvasive measure of CBF, it does not capture microvascular changes or hemodynamic factors that may influence perfusion dynamics. Additionally, we used PASL, which has a lower signal-to-noise ratio and shorter labeling duration compared with the more commonly used pseudocontinuous ASL, potentially affecting sensitivity to subtle perfusion changes. Detailed quantification of head impacts was limited, with self-reported heading data available for only a subset of participants (11 males and 5 females), restricting precise estimation of RHI exposure and its associations with outcomes. RHI exposure in soccer is highly individual and influenced by factors such as playing style, position, and frequency of heading, which were not fully captured in our study. This variability may introduce noise or systematic bias. Future studies with more precise exposure assessment are needed to address this limitation. Finally, given the exploratory nature of this study and the limited prior literature to guide specific hypotheses, we examined a broad range of outcomes to identify potential associations. While this approach increases the risk of type I error in a relatively small cohort, we applied FDR correction to balance false-positive control with statistical power. These findings should be considered hypothesis-generating, and replication in larger, independent cohorts will be essential to confirm their validity.
Conclusions
We report associations between RHI exposure and higher CBF among soccer players and CTL. However, there were no associations between CBF and neuropsychological functioning, suggesting that higher CBF may potentially serve as a compensatory response to RHI exposure. Further, we report sex-specific patterns of higher CBF in individuals exposed to RHI, with more widespread elevated gray matter CBF in women and more localized higher CBF in men. These findings highlight the importance of investigating sex-specific effects associated with RHI exposure. Future studies are warranted to investigate the sex-specific mechanisms underlying these differences and to determine their potential long-term sequelae.
Transparency, Rigor, and Reproducibility Statement
This study was not formally preregistered because it was exploratory in nature. The analysis plan was not preregistered, but the imaging processing pipeline and statistical models were defined prior to conducting group-level comparisons, and a team member with primary responsibility for the study and the analysis confirms that the analyses were prespecified and implemented consistently across participants. Sample size was determined based on available data from the recruited cohort of amateur soccer players and matched controls. No a priori power analysis was performed due to the observational nature of the study. A total of 112 participants were screened, 96 were enrolled, and neuroimaging data were acquired from all enrolled participants. After systematic quality control, data from 82 participants were retained for ASL analysis. Reasons for exclusion included incidental finding (n = 1), image artifacts (n = 8), and missing data on covariates (n = 5). Imaging acquisition and analyses were performed by team members blinded to relevant characteristics of the participants, and clinical outcomes were assessed by team members blinded to imaging results. Complete acquisition and preprocessing parameters are reported in the Methods section. All equipment and software used to perform imaging and preprocessing are widely available from commercial sources. The key inclusion criteria and outcome evaluations are established standards. This is a primary report of novel findings. No internal or external replication was performed. Future studies are planned for validation in larger and independent cohorts. The anonymized imaging and neuropsychological datasets, along with custom analysis code, will be made available by the corresponding author upon request.
Authors’ Contributions
Z.L.: Conceptualization, methodology, software, validation, formal analysis, resources, data curation, writing—original draft, writing—review and editing, and visualization. A.V.A.: Methodology, software, data curation, validation, resources, writing—review and editing. A.B.: Data curation, validation, resources, and writing—review and editing. L.S.S., J.J., and L.L.: Validation, resources, and writing—review and editing. N.S.: Methodology, validation, resources, and writing—review and editing. I.K.K.: Supervision, funding acquisition, conceptualization, validation, resources, and writing—review and editing.
Footnotes
Author Disclosure Statement
I.K.K. is a professor at Ludwig-Maximilians-Universität Munich (paid position). She serves as President of the European Neurotrauma Organization (unpaid position). She receives research grant funding from the National Institutes of Health, the European Research Council, and the German Ministry for Research and Education. She receives funding for a research study on sport-related concussions from Abbott Inc. The Ludwig-Maximilians-University Hospital received donations for her research from Mary Ann Liebert Inc. She receives royalties for book chapters published by Thieme Publishers. Her spouse is managing board member of Siemens AG, and she thus holds stock options at Siemens and Siemens Healthineers. I.K.K.’s in-kind contributions: PhD students working under her supervision receive scholarships from the Villigst Foundation, the China Scholarship Council collaboration with Ludwig-Maximilians-University Munich, and Fulbright. The other authors disclose no financial or other biomedical interests or potential conflicts of interest.
Funding Information
The authors of this work were partially supported by the following research grants: ERC Starting Grant No. 804326 (I.K.K. as principal investigator) and the ERA-NET NEURON project Neu-vasc under the funding code 01EW2011, the German Center for Child and Adolescent Health (DZKJ) under the funding code 01GL2406A, and research awards no. R01NS100952 from the National Institute of Neurological Disorders and Stroke (NINDS).