
Abstract
We investigated the association between diffusion tensor imaging along the perivascular space (DTI-ALPS) and remote mild traumatic brain injury (mTBI) exposures in previously deployed, post-9/11 Veterans. DTI-ALPS is a noninvasive, magnetic resonance imaging (MRI)-based proxy of glymphatic flow. Participants were 140 consecutively enrolled Veterans from the Translational Research Center for TBI and Stress Disorders (TRACTS) Houston cohort at the Michael E. DeBakey VA Medical Center who completed MRI. TBI exposures were assessed with the Boston Assessment of TBI-Lifetime. Individuals with moderate or severe TBI were excluded. We analyzed relationships between the DTI-ALPS index, a ratio of diffusion measures at a priori regions of interest. Participants were median age of 35 (interquartile range = 31, 41) years, predominantly male (91.4%) and white race (56.6%). Age was negatively correlated with DTI-ALPS indices (Spearman’s rs −0.181, p = 0.032). DTI-ALPS indices significantly differed among participants with no TBI (18.6%; DTI-ALPS [M ± SD] = 1.59 ± 0.21), mTBI Grade I (26.4%; 1.65 ± 0.26), mTBI Grade II (45%; 1.72 ± 0.29), and mTBI Grade III (10%; 1.82 ± 0.26) exposures (analysis of variance p = 0.042). The Jonckheere–Terpstra (JT) test was significant (JT = 4117, p value = 0.003), demonstrating an ordinal relationship between DTI-ALPS and increasing mTBI severity. Multivariable linear regression modeling revealed that mTBI Grade III was significantly associated with higher DTI-ALPS (β = 0.209, 95% confidence interval [CI] 0.038, 0.38; p = 0.017) when compared with no TBI, whereas age was significantly associated with lower DTI-ALPS (β = −0.007, 95% CI −0.013, −0.001; p = 0.025). mTBI Grades I and II did not significantly differ from no TBI when considered independently. DTI-ALPS index scores increased with the severity of mTBI. This represents a novel investigation of persistent glymphatic markers associated with remote mTBI in Veterans with neuropsychiatric comorbidities. Future work is needed to understand the temporal progression of changes in glymphatic function following mTBI and whether the observed changes have clinical or functional impacts on Veterans’ quality of life.
Introduction
The presence of a designated lymphatic system in the brain remained elusive until Iliff et al. (2012) demonstrated the flow of cerebrospinal fluid (CSF) via the perivascular area. This system was later named the glymphatic system (GS), a portmanteau of “glia” and “lymphatic.” 1 Structurally, the GS is comprised of three elements: a para-arterial CSF influx route, a para-venous interstitial fluid clearance route, and a trans-parenchymal pathway that is dependent upon astroglial water transport via the astrocytic aquaporin-4 (AQP4) water channels. 2 The GS appears to play an important physiological role in maintaining solute homeostasis in the central nervous system (CNS), and emerging evidence suggests that its dysfunction might be intricately linked to the pathophysiology of several CNS disorders via its role in pathogenic protein removal and promotion of brain health.3–7
Several endogenous and environmental variables may modulate glymphatic flow, including (but not limited to) age, sleep, cardiovascular health, and stress. 8 Many of the factors found to be related to glymphatic flow, such as sleep adequacy and cardiovascular health, are also impaired at high rates in the Veteran population, especially among those with a history of mild traumatic brain injury (mTBI).9–12 Individuals exposed to mTBIs are at a heightened risk of a variety of neuropsychiatric sequelae in the years to decades following the injury, including age-related neurodegenerative disorders.13–16 How biomechanical injuries to the brain impact glymphatic function (and, potentially, other disorders brought on by impaired glymphatic function) in this Veteran cohort requires further elucidation, particularly in the years to decades following the initial injury.
Recent research endeavors have shown that the underlying neurodegeneration/neuroinflammatory state observed in TBIs may be related to the impairment of clearance of inflammatory metabolites from the CSF via the glymphatic flow.9,17 Therefore, it would be ideal to measure glymphatic flow in individuals with a prior history of mTBI to monitor the progression of the disease and measure the effectiveness of any treatments to prevent it.
However, glymphatic flow rates are difficult to measure in humans in vivo. Since the GS is a relatively recent discovery, there has been comparatively little time to develop and validate imaging methods. 1 While contrast agents, such as gadolinium, can be used to measure flow, they need to be injected intrathecally, and the risks of that procedure are not often warranted in research contexts. 11 Phase-contrast magnetic resonance imaging (MRI) is often used to measure flow. However, the expected flow rates of the GS are at the low end of what may be possible to measure with that technique. 12
In response, a technique known as diffusion tensor imaging along the perivascular space (DTI-ALPS) has been developed. 18 The theory of this technique is that in certain areas of the brain, the vasculature (and thus, the perivascular spaces) is relatively well-aligned and perpendicular to nearby predominant white matter tracts, such that the flow through these spaces can be estimated by comparing the amount of diffusion of water in the direction of the vasculature to the amount of diffusion measured in the white matter tracts. Importantly, this technique utilizes the same MRI acquisitions used for typical diffusion tensor imaging and requires no special procedures or equipment beyond what is typical in research and clinical MRI settings.
In this report, we studied glymphatic flow, as measured by DTI-ALPS in a cohort of post-9/11 Veterans. We considered the effects of mTBI exposure number and severity, blast exposures, sleep, and psychiatric comorbidities to determine if the technique was likely to be sensitive enough to measure changes related to brain injuries in the years following the event. We hypothesized that increasing numbers of mTBI exposures and age were associated with reduced DTI-ALPS.
Methods
Participants
Participants were consecutively enrolled at the Houston site of the Translational Research Center for TBI and Stress Disorders (TRACTS; IRB Approval No. H-35944) at the Michael E. DeBakey VA Medical Center (MEDVAMC). TRACTS is a multi-VA cohort study designed to characterize the longitudinal outcomes of TBI and stress disorders in Veterans previously deployed to conflicts in Iraq or Afghanistan, as described elsewhere. 19 TRACTS participants were recruited via letters sent to preselected patients with TBI in their medical records, clinician referrals, and advertisements in hospitals and Veteran community organizations.
Eligible TRACTS participants were male and female Veterans who had been deployed at least once in post-9/11 military campaigns (Operation Enduring Freedom [OEF], Operation Iraqi Freedom [OIF], or Operation New Dawn [OND]) and were between 18 and 65 years old. Exclusion criteria included disorders of the CNS other than TBI (e.g., stroke, multiple sclerosis, epilepsy unrelated to TBI); bipolar or primary psychotic disorders (e.g., schizophrenia or schizoaffective disorders); and psychiatric disturbances requiring crisis intervention (e.g., acute suicidality). 19 For this analysis, participants were additionally excluded if they declined or were not eligible for MRI or if they had a moderate or severe TBI. The protocol was approved by the Institutional Review Board at Baylor College of Medicine and the Research & Development program of the MEDVAMC.
General procedures
All participants in this study were administered the standardized TRACTS protocol, which has been described elsewhere. 19 In brief, TRACTS participants completed a comprehensive clinical interview, several neuropsychiatric scales, vital sign measurements, blood draws, neuropsychological testing, and neuroimaging. Participants were invited to return for follow-up visits after 1 year and 5 years. Methods specific to this analysis are described below.
Neuroimaging
Participants were scanned on one of three systems: a 3T Siemens Tim Trio located at the MEDVAMC, a 3T Prisma Fit scanner located at the Core for Advanced MRI at Baylor College of Medicine used during the upgrade of the MEDVAMC system, or a 3T Prisma Fit scanner located at the MEDVAMC. T1-weighted anatomical images for alignment and registration were collected using a magnetization-prepared rapid acquisition gradient echo scan (TR/TI/TE= 2350/1100/3.35 ms; 1 mm isotropic; Field of View [FOV] = 256 mm; 176 slices). Diffusion-weighted images were collected with a spin-echo echo-planar imaging sequence (TR/TE = 10,000/103 ms; 2 mm isotropic; FOV = 256 mm; 64 axial slices without gap; 10 b = 0 volumes; 60 directions at b = 700). Both sequences were acquired obliquely to be aligned with the AC-PC axis. Susceptibility-weighted images (TR/TE = 27/20; FOV 230 mm × 172.5 mm; 1.2 mm isotropic; 112 axial slices with 20% gap) were used in 20 participants to confirm the location of vasculature.
Data processing
Diffusion data were processed using the FMRIB Software Library (FSL). As an initial data quality measure, single slices in axial, coronal, and sagittal views from each volume were visually inspected for artifacts and censored (along with their corresponding vector and b-value) from further processing using tools from Analysis of Functional NeuroImages FATCAT pipeline. Subsequently, data were brain-extracted using FSL’s bet, corrected for eddy-current distortions with eddy, and fit to a diffusion tensor model with dtifit. This, among other outputs, created a colorized fractional anisotropy (FA) map. For a subset of 20 representative participants with available images, three-slice minimum intensity projections were calculated for susceptibility-weighted imaging (SWI) images using MATLAB (MathWorks, Natick, MA), and the images were then aligned to the diffusion images using flirt. Using the FA and SWI images for reference, regions of interest in the superior longitudinal fasciculus (where its diffusion was most strongly in the y direction) and corticospinal tract (where its diffusion was most strongly in the z direction) were chosen (see Fig. 1). Additionally, to ensure consistency of region selection, M.E.R. and G.B. manually selected ROIs in 10 randomly selected scans each, based on already published protocols. The interrater differences were negligible. Selected regions were then transformed to the MNI152 template space and averaged, yielding coordinates of 27, 15, 26 for projection fibers and 39, 14, 27 for association fibers. These coordinates were then applied to all participants to extract diffusion in the x, y, and z directions. DTI-ALPS was calculated as the ratio of the diffusion in the x direction (that is, the direction of the vasculature) to the diffusion perpendicular to both the white matter and the vasculature averaged over the two regions, as described by Taoka et al. 18
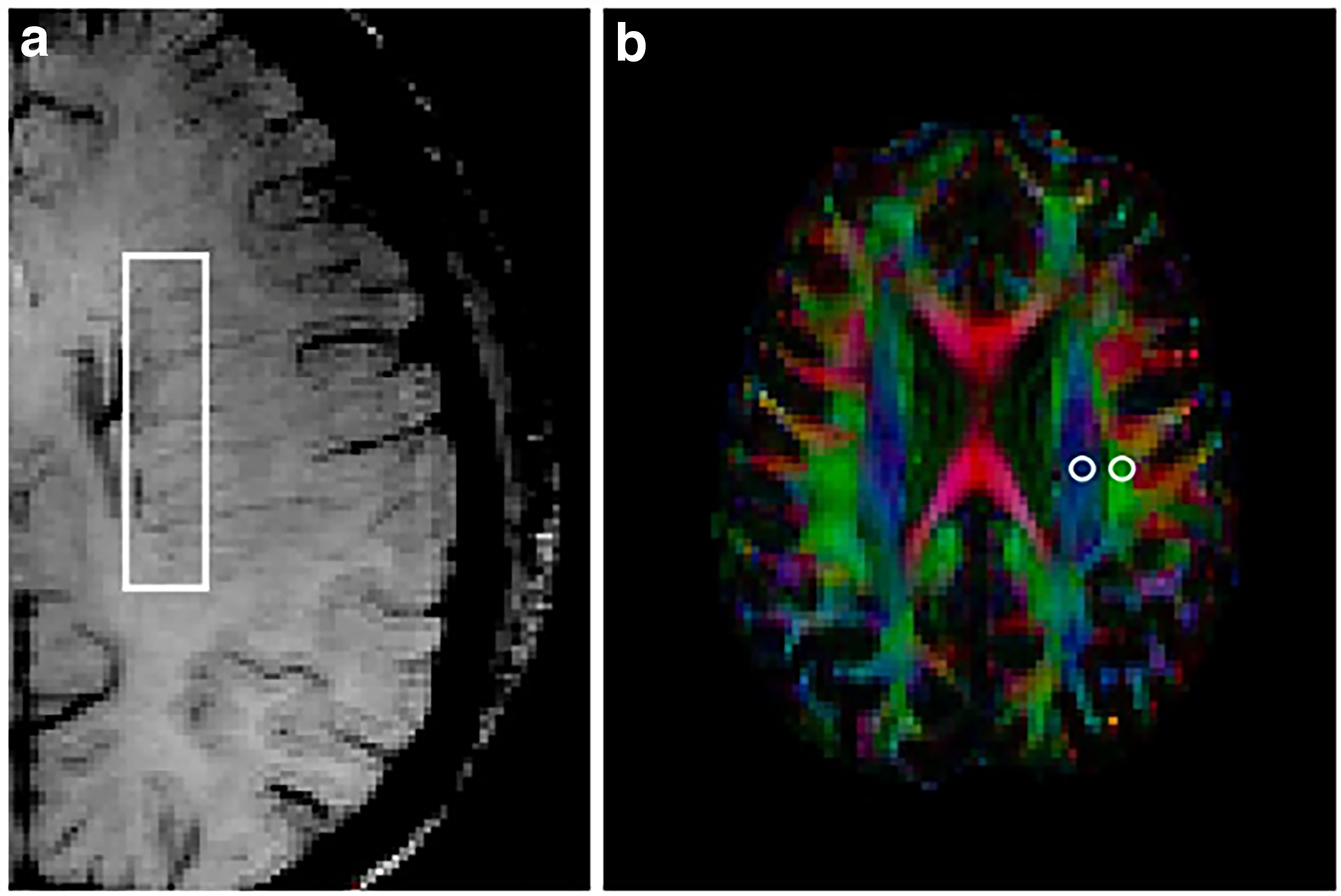
Region selection for DTI-ALPS.
TBI characterization
TBI exposures were assessed with the Boston Assessment of TBI-Lifetime (BAT-L). 20 The BAT-L queries for head injuries during premilitary, military-related, and postmilitary epochs from potential blasts, falls, training injuries, sports injuries, motor vehicle accidents, assaults, and other causes. The three most severe military blast, military other, premilitary, and postmilitary exposures were further queried to assess loss of consciousness (LOC), post-traumatic amnesia (PTA), and alterations of mental status (AMS).
The BAT-L was performed by a trained rater with at least a master’s level education. Each interview was reviewed in a meeting with senior investigators from Houston and Boston TRACTS sites until consensus was reached as to the presence and severity of every TBI. TBI severity was graded according to the presence and duration of LOC, PTA, and AMS; mTBI was further subdivided into Grades I, II, and III severities based on a hybrid classification system. 20 The number of blast exposures within 10 m, 11–25 m, and 25–100 m was also documented. Special care was taken to delineate the effects of emotional trauma and substance use from cognitive alterations.
Psychiatric assessments
Semi-structured psychiatric interviews were performed by a trained rater with at least a master’s level education. 21 Participants were queried for the presence of a major depressive episode within the past month and throughout their lifetimes. Participants with recurrent major depressive disorder met diagnostic criteria for at least two discrete major depressive episodes; if one such episode occurred in the past month, it was considered “current.” The presence and severity of post-traumatic stress disorder (PTSD) were assessed with the Clinician Administered PTSD Scale for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (CAPS-5). 22 All participants were queried for PTSD symptomatology during the past month (current). Depending on the presence and timing of index trauma(s), participants were additionally queried for PTSD symptomatology during their most problematic month(s) pre- and/or post-deployment. Participants with “lifetime” PTSD reported symptoms meeting diagnostic criteria during pre- and/or post-deployment time frames. Psychiatric diagnoses were reviewed in consensus meetings with senior TRACTS investigators from both sites. Depression and anxiety severity in the past week were measured with the Depression Anxiety and Stress Scale (DASS-21). 23 Alcohol use severity was additionally measured with the self-administered Short Michigan Alcohol Screening Test (SMAST), a screen for problematic alcohol use. 24
Additional assessments
Demographics (e.g., race, marital status, employment) and deployment information were collected via self-report questionnaires. Sleep quality in the past month was assessed with the Pittsburgh Sleep Quality Index. 25 Cardiometabolic indicators used for this analysis were waist-to-hip ratio and body mass index. High sensitivity C-reactive protein (hsCRP), a marker of inflammation was obtained from laboratory blood tests. 19
Statistical analysis
Bivariate associations of DTI-ALPS with demographic, psychiatric, metabolic, and TBI exposure variables were examined with one-way analysis of variance (ANOVA) for categorical variables and Spearman’s correlations for continuous variables. Statistical evaluation of trend in DTI-ALPS values according to mTBI severity was evaluated with the Jonckheere–Terpstra (JT) test. Multivariable linear regression modeling was used to assess associations between DTI-ALPS and mTBI severity while adjusting for age and gender. A linear trend test between DTI-ALPS and TBI severity while adjusting for age and gender was also assessed using a general linear model by incorporating TBI severity as a continuous variable. In additional exploratory analysis, groups were stratified approximately equally into those with most recent TBI less than 10 years before assessment, and 10 years or more. Association between DTI-ALPS and TBI severity was tested as before. All statistical analyses were performed with R Statistical 161 Software (v4.1.0; R Core Team, 2021).
Results
The participant flow is shown in Figure 2. For TRACTS participants with MRIs performed at both baseline and follow-up visits, the scan with the lowest motion was kept. Otherwise, the baseline scan was used.
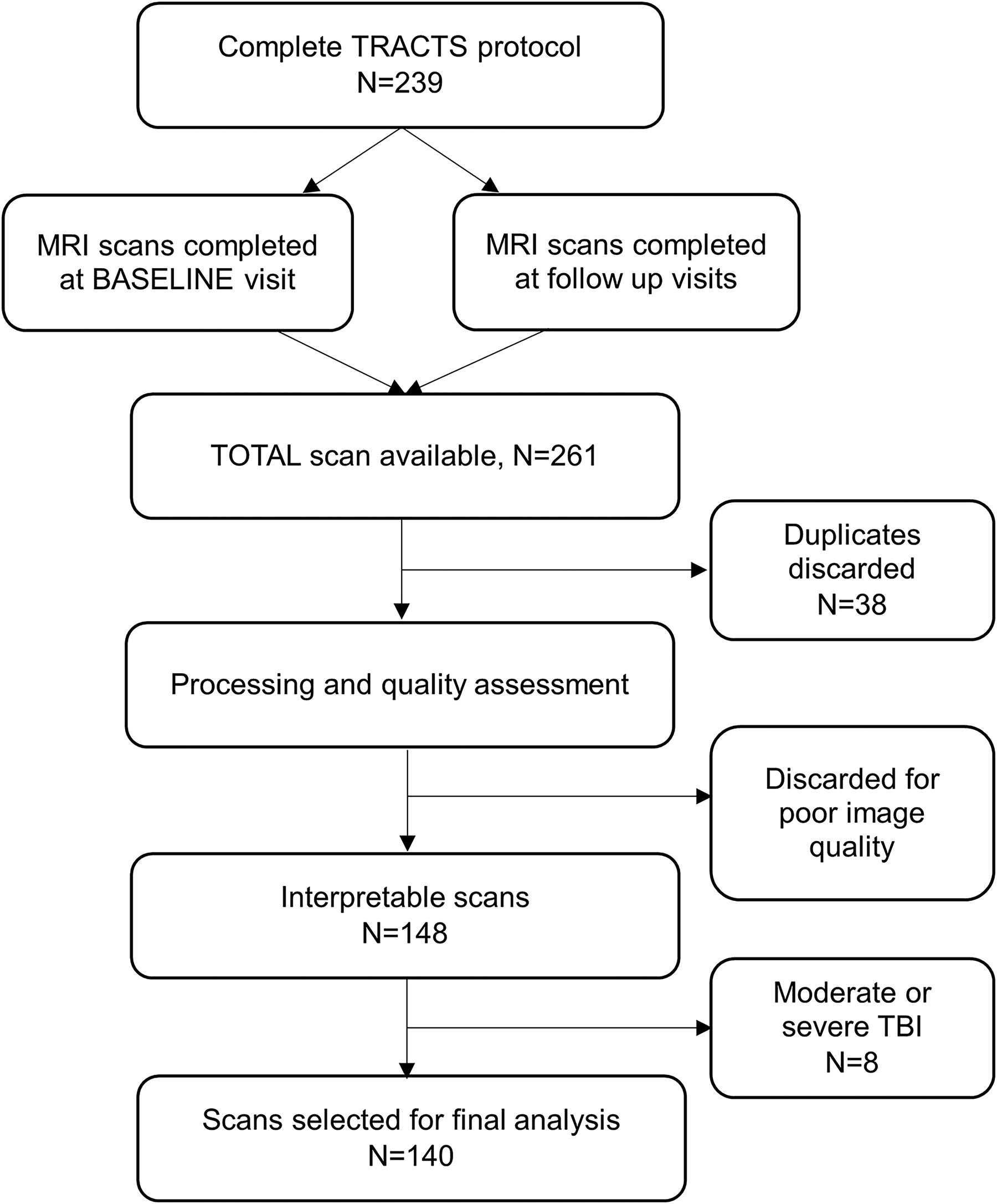
Patient flowchart. MRI, magnetic resonance imaging; TBI, traumatic brain injury; TRACTS, Translational Research Center for Traumatic Brain Injury and Stress Disorders.
Demographic and clinical characteristics of the sample are shown in Table 1. The median age of the participants was 35 (interquartile range [IQR] = 31, 41) years. Participants were predominantly male (91.4%). Race was primarily self-reported as white in 56.6%. Nearly half of the sample met criteria for current PTSD. Of the demographic, psychiatric, and metabolic indices examined (Table 1), only age was negatively correlated with DTI-ALPS indices (Spearman’s rs −0.181, p = 0.032).
Demographic Characteristics and Bivariate Association with DTI-ALPS
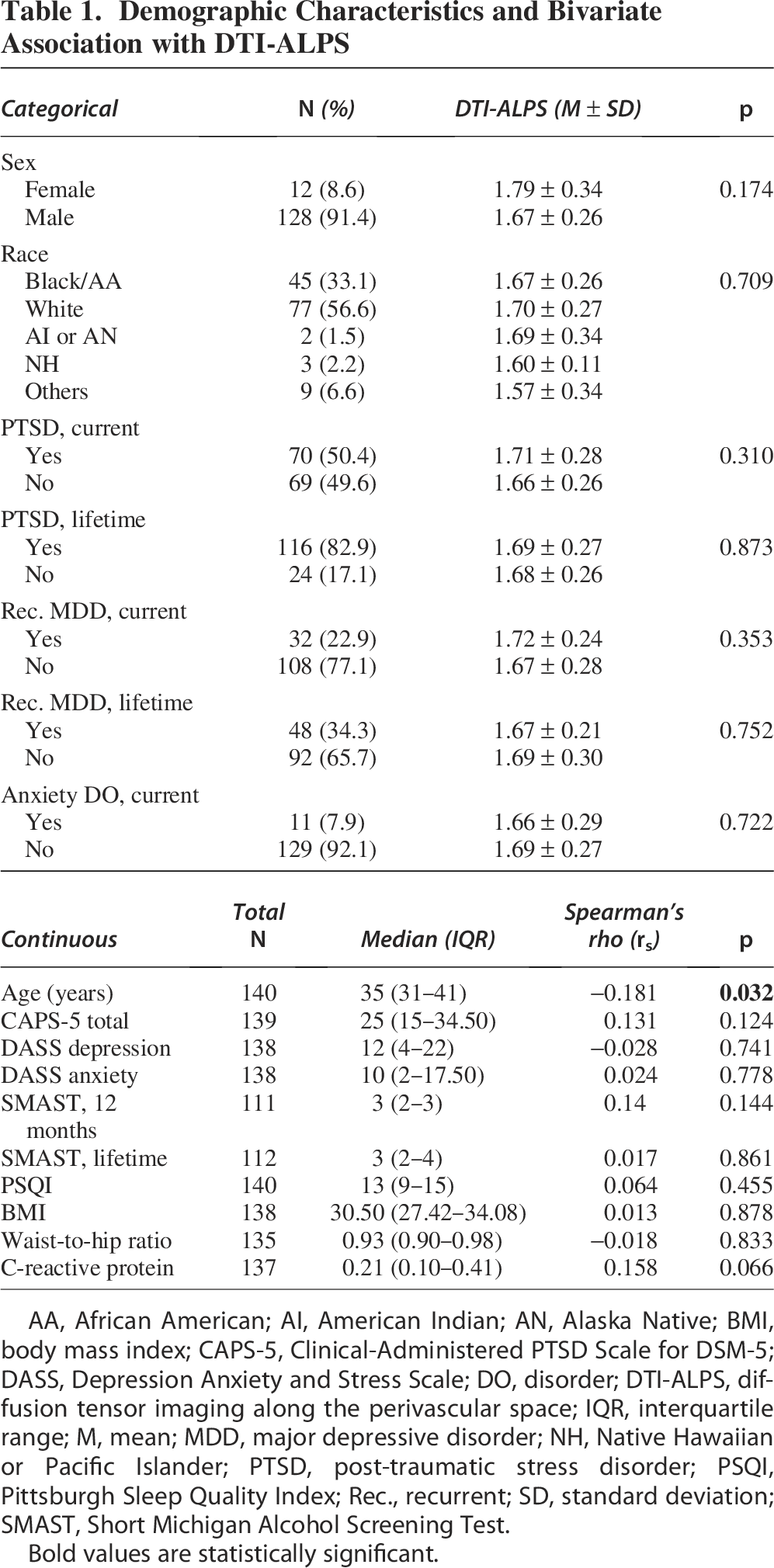
Bold values are statistically significant.
AA, African American; AI, American Indian; AN, Alaska Native; BMI, body mass index; CAPS-5, Clinical-Administered PTSD Scale for DSM-5; DASS, Depression Anxiety and Stress Scale; DO, disorder; DTI-ALPS, diffusion tensor imaging along the perivascular space; IQR, interquartile range; M, mean; MDD, major depressive disorder; NH, Native Hawaiian or Pacific Islander; PTSD, post-traumatic stress disorder; PSQI, Pittsburgh Sleep Quality Index; Rec., recurrent; SD, standard deviation; SMAST, Short Michigan Alcohol Screening Test.
Comparison of DTI-ALPS indices with TBI exposure histories is shown in Table 2. Lifetime mTBI exposures were reported in 81.4% of the sample and were associated with higher DTI-ALPS index (p = 0.049). DTI-ALPS indices significantly differed among participants with no TBI exposures, (18.6%; DTI-ALPS [M ± SD] = 1.59 ± 0.21) mTBI Grade I (26.4%; 1.65 ± 0.26), mTBI Grade II (45%; 1.72 ± 0.29), and mTBI Grade III (10%; 1.82 ± 0.26) exposures (ANOVA p = 0.042). DTI-ALPS was not significantly associated with blast-related exposures, number of TBIs, duration of LOC, or time since last TBI (Table 2).
Relationships Between Remote TBI Characteristics and DTI-ALPS Values Statistically Significant
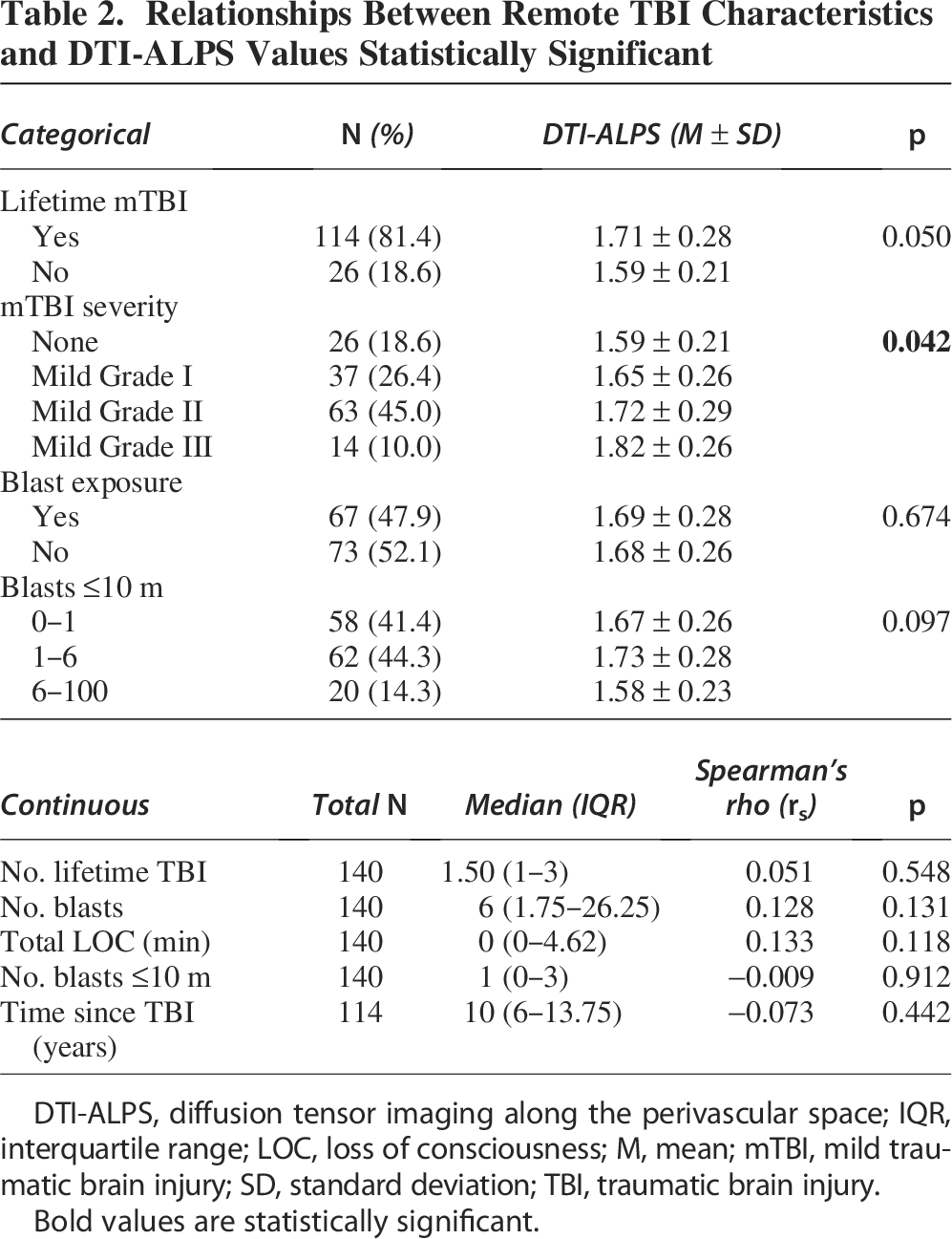
Bold values are statistically significant.
DTI-ALPS, diffusion tensor imaging along the perivascular space; IQR, interquartile range; LOC, loss of consciousness; M, mean; mTBI, mild traumatic brain injury; SD, standard deviation; TBI, traumatic brain injury.
There was an increasing trend for DTI-ALPS according to mTBI severity (Fig. 3). The JT test was significant (JT = 4117, p value = 0.003), demonstrating a statistically significant ordinal relationship between DTI-ALPS and increasing mTBI severity.
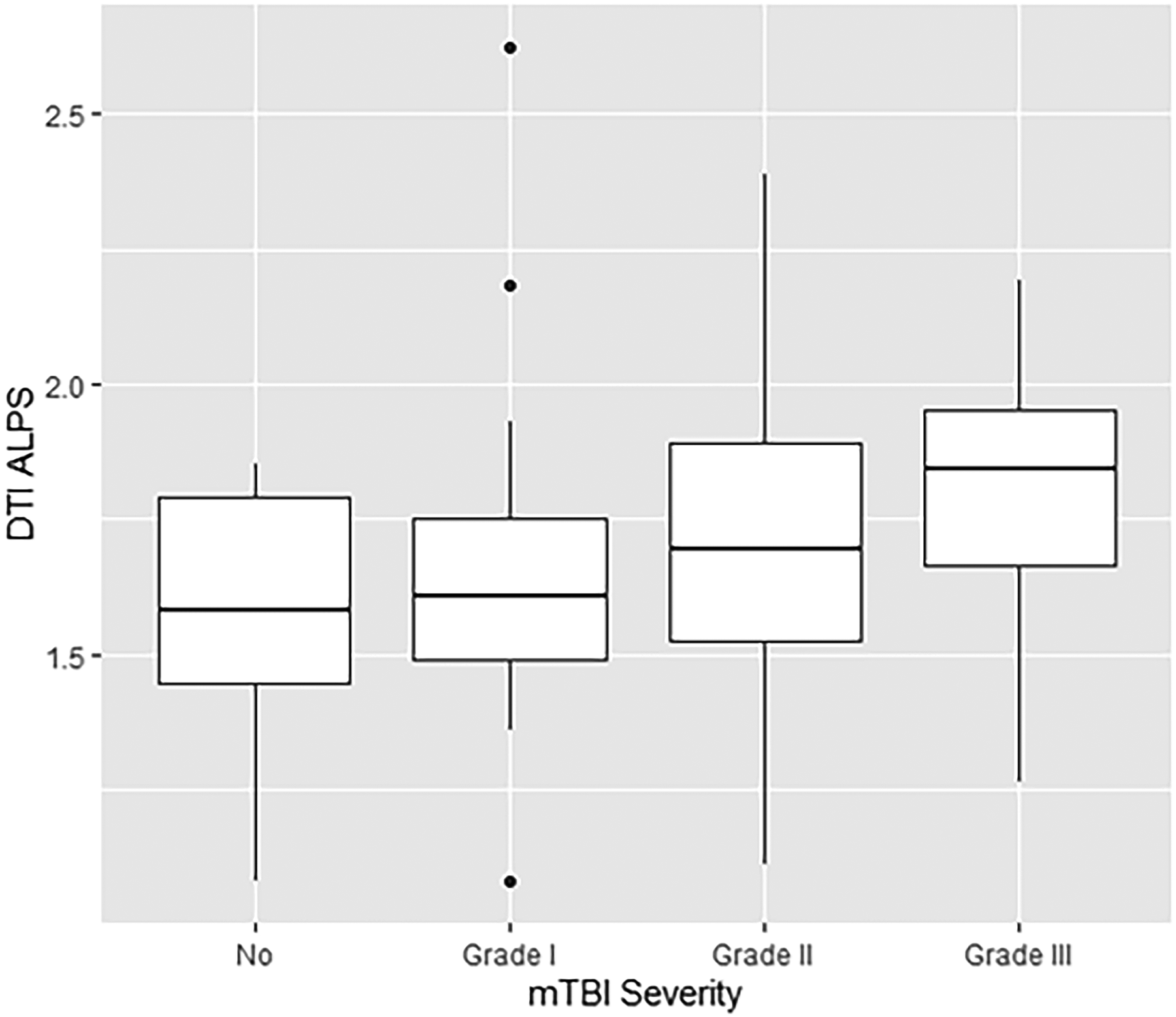
Comparison of DTI-ALPS indices in patients with no (0), mild Grade I (1), mild Grade II (2), and mild Grade III (3) traumatic brain injuries. DTI-ALPS, diffusion tensor imaging along the perivascular space; mTBI, mild traumatic brain injury.
Multivariate linear regression modeling was used to assess the association between mTBI severity groups while adjusting for age and gender (Table 3). mTBI Grade III was significantly associated with higher DTI-ALPS (β = 0.209, 95% CI 0.038, 0.38; p = 0.017) when compared with no TBI, whereas age was significantly associated with lower DTI-ALPS (β =−0.007, 95% CI −0.013, −0.001; p = 0.017). mTBI Grades I and II were not significantly different from no TBI. We additionally tested the linear trend of TBI severity while controlling for age and gender and found that the relationship was still significant (p = 0.008). We tested these relationships while controlling for FA in the model and did not observe any influence of underlying white matter integrity on these results (see Supplementary Data).
Multivariate Linear Regression
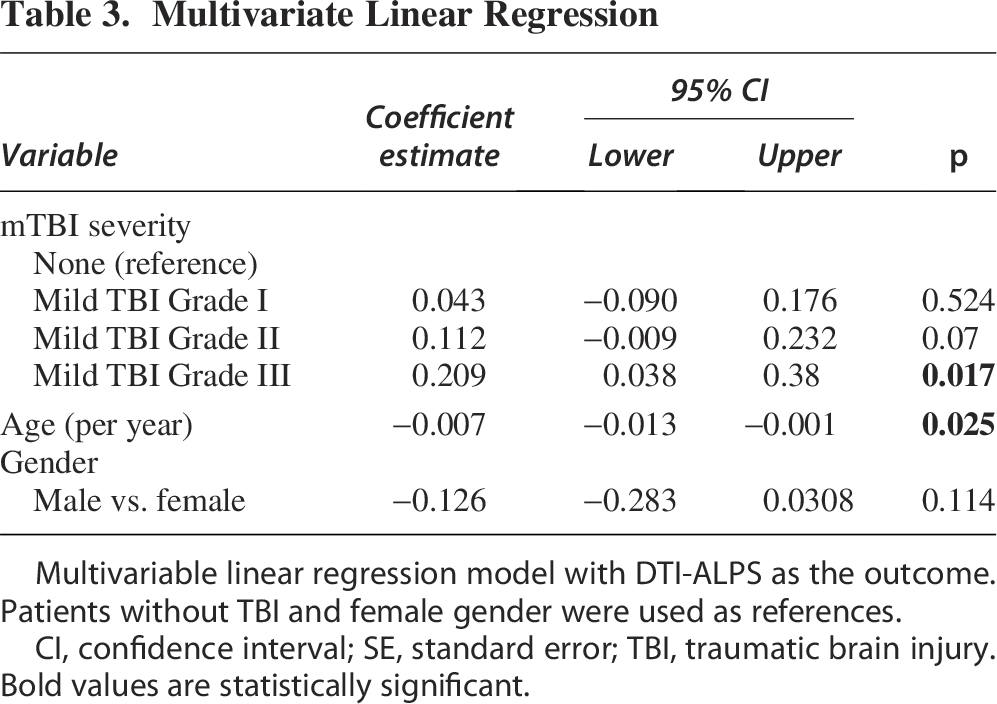
Bold values are statistically significant.
Multivariable linear regression model with DTI-ALPS as the outcome. Patients without TBI and female gender were used as references.
CI, confidence interval; SE, standard error; TBI, traumatic brain injury.
In an exploratory analysis to understand the effect of time since the most recent TBI, the cohort was divided into those with mTBIs that occurred within 10 years of assessment and those with mTBIs that had occurred 10 years or more before assessment. Although the effect of time since TBI was not itself associated with DTI-ALPS, we found that in the cohort with more recent mTBIs, the same associations with DTI-ALPS were observed (JT = 577, p = 0.004) while in the cohort with less recent TBIs they were not (JT= 571, p = 0.561). Similarly, when assessing the trend in a general linear regression controlling for age and gender, we observed a significant trend (p = 0.036) in the more recent group and no significant trend (p = 0.524) in the less recent group.
Discussion
To the best of our knowledge, this is the first study to investigate glymphatic dysfunction in Veterans of OEF, OIF, and OND with remote TBI exposures. We observed a relationship between the severity of mild brain injury and DTI-ALPS index scores. Specifically, DTI-ALPS index scores tended to increase with increasing severity of mTBI. Additionally, we noted a significant decline in DTI-ALPS scores with advancing age. While prior studies have indicated that sleep disturbances, and acute immune responses may also influence glymphatic function, our findings did not fully align with these outcomes. Given that our cohort includes many individuals with multiple injuries of varying degrees and causes and numerous concurrent conditions, such as chronic pain, PTSD, and depression, it is plausible that competing factors affect glymphatic flow. Further research is warranted to explore these effects in more detail.
Prior work has utilized the DTI-ALPS technique to understand the sequelae of TBI. In a study conducted by Park et al. (2023), the DTI-ALPS index was lower in patients with mild/moderate TBI compared with healthy controls. 26 In contrast, Dai et al. (2023) observed an increase in the DTI-ALPS index in cases with mTBI compared with healthy controls. 27 Our study corroborates the observation of increasing DTI-ALPS in mTBI. Our cohort had very limited representation of moderate or severe TBI, but it should be noted anecdotally that the cases that were available (data not shown) had lower DTI-ALPS compared with controls. Thus, our findings corroborate recent work in mTBI but do not necessarily refute studies in more severe TBI. Of note, these prior studies examined patients in the acute stages of injury, while our population reported injuries that primarily occurred during their deployment some years prior. Consequently, our findings suggest that these changes are persistent.
Our findings of increased DTI-ALPS with increasing injury severity are somewhat at odds with most findings of low glymphatic flow in pathological conditions. However, there have been pre-clinical studies showing that brain injury may alter the function of AQP4 water channels in ways that would increase glymphatic flow. The AQP4 water channels on perivascular endfeet of astrocytes appear to be an important bottleneck regulating the glymphatic flow as pre-clinical genetic research has demonstrated a disruption in the glymphatic flow in AQP4 knockout animals and genetic variations in the AQP4 gene.1,28 The alterations in the AQP4 channels in animal models of TBI29–32 may be a compensatory mechanism to combat cerebral edema following injury. While it is not well established that DTI-ALPS is a measure (even indirectly) of AQP4 function in humans, this animal work nonetheless provides a speculative mechanism for our observations. Further, a recent mouse study demonstrated that there may be more complex alterations in the dynamics of glymphatic flow following brain injury than a brain-wide increase or decrease, and the DTI-ALPS technique does not have the spatial specificity to assess these complex dynamics well. 33
The pre-clinical studies were able to utilize techniques that more directly assessed glymphatic function in animals, whereas human studies are more limited in available techniques. Although DTI-ALPS may fill a significant hole in the set of tools available to neuroscientists to measure aspects of brain function, there are still limitations to the technique. DTI-ALPS utilizes a priori regions of interest that were chosen because of the structure of the white matter and vasculature in that area, and as such, is unable to offer any spatial specificity to changes in glymphatic function. Pre-clinical TBI studies suggest several regions where the GS might be more susceptible to TBI, such as the limbic structures and olfactory bulbs,9,17,34 and the DTI-ALPS technique in humans is unable to assess these features. Diffusion imaging itself is relatively limited in its spatial resolution, and partial volume effects in the areas probed may limit both the precision of DTI-ALPS measures and their specificity to glymphatic flow. There may be other factors that affect diffusion signal or water movement in these regions besides the GS. 35 The TRACTS MRI protocol was developed in 2009 before multi-slice accelerated diffusion imaging was readily available, and newer sequences with higher angular resolution and finer spatial resolution may be able to provide more precise measures of diffusion along vasculature and white matter throughout the brain. It is also worth noting that pre-clinical studies have demonstrated that glymphatic flow is enhanced during sleep, and these measures may be improved by efforts to image individuals who are asleep in the scanner or to control for whether or not the individuals being scanned had fallen asleep. To eliminate a source of variability between individuals, the current study tried to eliminate observer bias by automating the process of selecting ROIs. Finally, our data were acquired on three different scanners due to changes in the facility. Although Taoka et al. (2022) showed that the difference in scanner did not influence the DTI-ALPS index, this may nonetheless introduce variability that limits our statistical power. 36
Diagnosing remote TBI heavily relies on participants’ recollections of events (recall bias). This introduces a risk of underreporting or overreporting of symptoms, which could influence the study’s findings. The BAT-L questionnaire divides TBIs into three categories (mild [Grade I, Grade II, Grade III], moderate, and severe) based on the duration of LOC, PTA, and AMS. 20 Although this classification is useful for categorizing TBIs from a research perspective, the clinical reproducibility of this classification is not established. There is nonlinearity in the BAT-L findings, that is, similar grades of TBIs might present with different clinical presentations, and the severity of these findings can also vary. The time since injury is of vital importance since it can introduce recall bias. Through exploratory analyses, we examined the relationship between time since injury and the association between mTBI severity and DTI-ALPS. We found that the effect was significant in more recent injuries (<10 years), and not observable in less recent injuries (≥10 years). This may be indicative of some degree of recovery over time, although this cannot be addressed directly in a cross-sectional study. Even in the cohort with more remote injuries, participants with Grade III concussions had higher DTI-ALPS values. It may also be indicative of different circumstances surrounding injuries that occurred at different parts of the participants’ lives.
While the focus of this study was on the relationship between mTBI and glymphatic function, other factors may be at play in this cohort. Veterans as a patient group are notable for facing multiple simultaneous comorbidities, including PTSD, depression, substance abuse, sleep disorders, and more. We examined the relationship between these comorbid factors and DTI-ALPS and did not find significant relationships. Age was a significant contributor to DTI-ALPS, as has been reported elsewhere. 37 Although the relationship between sleep and glymphatic flow is well established,11,38–45 we did not observe a relationship between DTI-ALPS and sleep disorder in our cohort. There may be an interaction between the effects of age and brain injury on DTI-ALPS, 27 but this was not considered in our study due to the cohort having complex injury histories with multiple events occurring at a range of times prior to their imaging. Numerous studies indicate that the GS performs more efficiently during sleep, likely due to the enlargement of the interstitial space.27,36 Sleep disturbances are of particular interest in the Veteran population due to their prevalence and their association with multiple concurrent conditions such as PTSD and TBI. The latter affects both the timing and architecture of sleep patterns—insomnia, hypersomnia, excessive daytime sleepiness, and fragmented sleep; obstructive sleep apnea and insomnia are some of the sleep ailments that are more frequent among individuals with a TBI history.14,46–48 The comorbidity between TBI and sleep disorder may have contributed to a lack of power to detect effects of sleep, especially as the effect on DTI-ALPS is in opposite directions; however, that will need to be established definitively with further work.
Conclusion
In all, this study contributes to the relatively sparse literature examining chronic mTBI and glymphatic function in numerous ways. First, the sample size is relatively large as compared with other studies with a similar purview. This enhances the robustness of our findings by increasing the statistical analysis’s power and allows us to more carefully examine potential confounding factors that are common in the Veteran population. Second, the automated ROI selection mitigated observer bias, whereas the previous studies relied on the radiologist to select ROIs in each scan. This innovation enhances the objectivity of our research. Third, the study provides an important step forward in understanding the long-term sequelae of TBI in the Veteran population. Future work will be required to understand the temporal progression of changes in glymphatic function following mTBI, and to understand if the observed changes have clinical or functional impacts on the quality of life of Veterans.
Authors’ Contributions
G.B.: Methodology, formal analysis investigation, data curation, writing—original draft, review and editing. M.E.R.: Conceptualization, methodology, software, validation, formal analysis, investigation, data curation, writing—original draft, review and editing. T.W.: Data curation, writing—original draft, review and editing. R.L.: Methodology, formal analysis, data curation. M.B.J.: Methodology, data curation, writing—original draft, review and editing. R.E.J.: Conceptualization, methodology, writing—original draft, review and editing, supervision, project administration, funding acquisition.
Footnotes
Author Disclosure Statement
The authors declare the following potential competing interests: M.B.J., R.E.J., and R.L. received study drug support for a VA Clinical Science Research and Development (CSR&D) trial from Acadia Pharmaceuticals. R.E.J. received study drug support for a VA Cooperative Studies Program (CSP #2018) from Pfizer Pharmaceuticals. The other authors have no competing interests to disclose.
Funding Information
This work was supported by the Career Development Award # IK2CX002363-01A1 from the U.S. Department of Veterans Affairs CSR&D Service (M.B.J.) and the Translational Research Center for TBI and Stress Disorders (TRACTS; B9268-X) from the U.S. Department of Veterans Affairs Rehabilitation Research and Development (RR&D) service (R.E.J.).
Disclaimer
The findings and conclusions presented are solely those of the authors and do not reflect the views of the U.S. Department of Veterans Affairs (VA), Baylor College of Medicine, UT Health, or KBR, Inc.
Transparency,Rigor,and Reproducibility Summary
This study was not formally registered because the TRACTS study is designed to facilitate multifaceted analyses and establish a longitudinal cohort. Details of participant recruitment, eligibility criteria, data analysis, and limitations of the methods are described above. In one-way ANOVA, the sample size of n = 140 (26, 37, 63, and 14 in the four mTBI severity groups) provides 80% power to detect an effect size η2 of 0.075 for the association between DTI-ALPS and mTBI severity with an alpha of 0.05, where η2 represents the proportion of the variation in the outcome explained by the groups. Similarly, in multiple linear regression, a sample size of 140 achieves 80% power to detect an effect size (Cohen’s f2) of 0.083 attributable to mTBI severity groups using an F-test with an alpha of 0.05 adjusting for other variables. Analyses were not adjusted for multiple comparison, as we have a single primary outcome (DTI-ALPS) that is a univariate continuous outcome. The main research question and analysis centers around the association between DTI-ALPS and mTBI severity, and other analyses are considered secondary and exploratory. The histogram of DTI-ALPS is reasonably bell-shaped with limited skewness (skewness = 0.47). We also did not detect violation of the homogeneity of variance over the four mTBI severity groups according to the Levene’s test (p = 0.4). Thus, one-way ANOVA is appropriate for comparing DTI-ALPS. For the multiple linear regression, we have conducted model checking using residuals to verify the assumptions of linearity, normality, and homoscedasticity. De-identified data from this study are not available in a public archive; summary data may be available upon request by emailing the corresponding author as of March 3, 2025.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.