
Abstract
Neuroinflammation is known to contribute to worse patient outcomes following severe traumatic brain injury (TBI). Specifically, complement activation as part of the innate immune response has been explored in animal models and post-mortem human tissue. However, it has not been well-characterized in a substantial clinical cohort. We aimed to investigate the complement cascade, specifically focusing on the lectin pathway initiators, in patients with TBI compared with healthy controls. We describe temporal profiles of complement proteins, and investigate their association with outcome, and clinical variables following TBI. Plasma blood samples collected from 64 patients with TBI (on days 1–7, 42, and 365) and 17 healthy controls (single samples) were analyzed for 10 complement proteins using single and multiplexing protein assays. We quantified initiator (MBL, MASP2, ficolin3), effector (C4b, C2, factor D, factor I), and downstream (C5, C5a, C5b9) complement proteins. Clinical variables included injury severity score, Glasgow Coma Scale motor score, pupil reactivity, and Glasgow Outcome Scale Extended at 6 months post-injury. 7 out of 10 measured complement proteins had median concentrations that were significantly different in patients with TBI compared with healthy controls (all p values < 0.05). Ficolin3, an initiator, was particularly lower in TBI versus controls (0.22 vs. 1.84 ng/mL, p < 0.001), and consistently lower over time, showing depressed levels even 1 year post-injury (p < 0.001). Initiators MBL and MASP2, effector C2 and downstream proteins C5, C5a, and factor I demonstrate a steady rise in the first week post-injury, and are consistently elevated compared with control levels. Patients with unfavorable outcome had higher levels of C4b, C5, and factor I, with C5 demonstrating this trend over time (OR: 1.53 [1.52–1.53], p value < 0.001), and showing additional prognostic benefit over and above IMPACT clinical outcome predictors. This study characterized the complement cascade in human TBI with high temporal resolution in initiator, effector, and downstream proteins. Seven out of the 10 measured proteins were significantly different in patients with TBI compared with healthy controls. Notably, C5 has an independent and robust association with outcome in both univariate and linear mixed regression, where a higher C5 concentration was associated with unfavorable outcome 6 months post-injury. Further investigation is required to explore the potential of complement as a therapeutic target in TBI.
Introduction
The complement system, a key mechanism of defense in innate immunity, has been implicated in triggering neuroinflammation and secondary injury following traumatic brain injury (TBI).1–3 Upregulated and uncontrolled complement activation following TBI leads to exacerbated neuropathology after trauma in mouse models, 4 and hence this cascade represents a crucial candidate mediator of secondary damage after human TBI.
The complement system is activated by at least three pathways: classical, alternative, and lectin pathways. All three are triggered by initiator proteins such as antigen-antibody immune complexes, circulating collectin proteins, or those expressed by apoptotic cells, and are closely related but have some unique features. With different initiator and effector proteins, the three pathways activate from different triggers, but all pathways converge at the level of C3 and C5, which are subsequently broken down into various C-fragments. This subsequent cytolytic pathway is common to all activation cascades and results in terminal complement activation, which leads to cell death. Hence, complement plays an important role in pathogen handling, but also, relevant in TBI, damaged cell and debris clearance. The lectin pathway, specifically, has been highlighted in TBI across pre-clinical, clinical, and genome-wide association studies.5–10 While the activation pathways converge and are intertwined, it has been suggested that complement activation in TBI is lectin-dependent, with possible amplification by the alternative pathway.8,11
As with most inflammatory cascades, whether activation of the lectin cascade following TBI is deleterious or advantageous depends on a multitude of factors including, but not limited to, the time after injury. Early activation may be neuroprotective, as mice lacking mannose-binding lectin (MBL, a key initiator) showed worse neurological deficits and increased neurodegeneration shortly after cortical injury. 7 MBL selectively binds to ischemic endothelium within 30 min of focal ischemia, 12 highlighting its rapid response. However, prolonged lectin pathway activity may be harmful, as MBL-deficient mice exhibited reduced neuronal loss 5 weeks post-injury and its deletion, the authors summarize, is protective. 8 Considering the complexities of this pathway, there is a paucity of data regarding the complement’s temporal dynamics in human TBI.
Despite the potential importance of this cascade, research into the complement cascade is largely limited to animal and postmortem studies. Where studies of human samples have been possible, investigations have been limited to narrow protein explorations. To characterize this pathway in human TBI, a detailed exploration of multiple proteins representing different aspects of the complement cascade in humans is necessary. Therefore, we aimed to explore the complement system in 64 TBI patients, in whom we had daily plasma samples for both the acute period (days 1–7 post-injury), as well as persistent inflammation following injury (days 42, 180, and 365). We describe and demonstrate the temporal profile of complement proteins categorized into initiator, effector, and downstream groups, as well as comparisons with healthy controls. Lastly, we investigate the association between complement proteins, outcome, and clinical variables in patients with TBI.
Materials and Methods
Study cohorts and ethical approvals
The International Collaboration On Neuroinflammation in Traumatic Brain Injury (ICON-TBI Study) is an observational study designed to characterize the inflammatory response to TBI (project reference MR/R005036/1). The study included two recruitment centers—Addenbrooke’s Hospital, Cambridge, United Kingdom (local ethics: 13/EE/0119), and APHP-Sorbonne University Hospital, Pitié-Salpêtrière, Paris, France (local ethics: RCB 2017-A03281-52). Patients were considered for inclusion if they were adults aged 18–70 years old, admitted to the intensive care unit with moderate–severe TBI (Glasgow Coma Scale [GCS] < 12), and were recruited over a 5-year period (2017–2021). Informed consent was obtained from the patient’s next of kin.
The control cohort consisted of healthy adults (aged 18–70 years), with no history of neurological disease or past head injury. Controls were recruited from Addenbrooke’s Hospital, Cambridge, United Kingdom (Research Ethics Committee [REC] study number 97/290), Biomedical Research Centre (REC 11/33/0007), and provided written consent.
Patient sample collection and storage
Plasma samples were collected into ethylenediaminetetraacetic acid (EDTA)-containing tubes for the following days post-injury (injury = Day 0): Days 1–7, 42, 180, and 365, where possible. Sampling was done via the arterial line for days 1–7, with venous sampling used for the later timepoints.
Samples were processed (centrifuged at 1200 g for 10 min, the supernatant aspirated and aliquoted), anonymized, and frozen at −80°C immediately until batch analysis. Biological samples from Paris were shipped on dry ice with temperature monitoring to Cambridge University.
Quantifying the proteins in patient samples: Single and multiplexing assays
Complement proteins of interest (ficolin-3, MASP2, MBL, C2, C4b, C5, C5a, factor D, factor I, C5b9) were quantified using single-plex and multiplex assays as per manufacturer’s instructions. A commercially available multiplexing Luminex assay for complement analytes was used (MILLIPLEX® Human Complement Magnetic Bead Panel 1, Merck, UK). This method relies on the use of Luminex magnetic beads and analyte specific capture antibodies. As this single Luminex panel included assays for MBL, C2, C4b, C5, C5a, factor D, and factor I, we did additional single-plex assays to fully characterize the complement cascade. Standard sandwich enzyme-linked immunoabsorbent assays (ELISAs) were used to quantify ficolin-3 (Abcam, UK), MASP2 (Abcam, UK), and C5b9 (Abbexa, UK). This method of protein quantification uses pre-coated monoclonal antibodies and an enzyme-linked color change reaction. Plasma samples were thawed, diluted appropriately (1:150 for the multiplex assay, 1:10 for ficolin-3, and 1:500 for MASP-2 and C5b9), and assayed using the four kits. The resultant output is optical density (OD) and median fluorescent intensity (MFI) for ELISA and Luminex, respectively, with absolute concentrations of each analyte calculated by plotting standard curves against known standard concentrations. In the cases of ficolin-3 and C5b9, ODs beyond the standard curve were extrapolated to achieve an estimated absolute concentration. For factor I assays, 63.6% of datapoints were above the highest standard, and hence extrapolation was not recommended. Dilution based on factor I alone was not possible as it was part of a multiplexing plate, and hence, after multiple testing stages, the dilution factor selected was based on optimization for all analytes, which negatively affected factor I.
As we had multiple samples from multiple patients, we analyzed 10 96-well plates for each assay type. Each assay was performed according to manufacturer instructions, with quality control metrics according to assay specifications (Supplementary Data S1). Figure 1 is a summary of the complement pathway, placing the proteins quantified in context. To aid biological interpretability, we considered the complement proteins to belong to one of three groups: initiator (ficolin-3, MASP2, MBL), effector (C2, C4b, factor D), and downstream (C5, C5a, factor I, C5b9) proteins, with the knowledge that this is an arbitrary grouping as complement proteins have complex and varying roles within the complex pathophysiology of brain trauma.
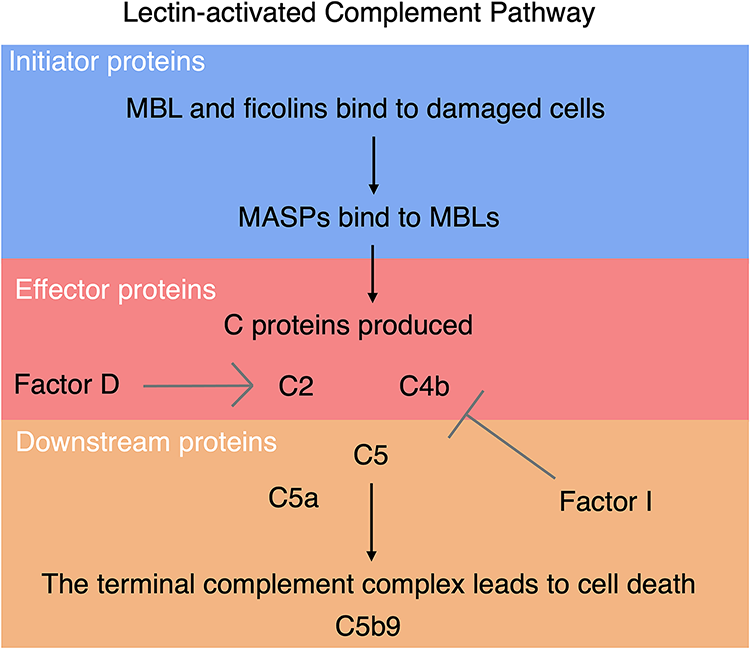
The lectin complement pathway is initiated by MBL and ficolin proteins binding to damaged cells, and results in cell death via the terminal complement complex. Complement activity is amplified by factor D, and inhibited by factor I. We have quantified proteins from various stages of this pathway and to aid interpretability, we have grouped them into initiator (MBL, MASP2, ficolin3), effector (C4b, C2, factor D, factor I), and downstream (C5, C5a, C5b9) groups.
Clinical variables
Baseline clinical characteristics included pre-intubation GCS, pupil reactivity, Marshall score of admission CT brain images, and the Abbreviated Injury Scale 2015 (AIS), which is used to calculate the Injury Severity Score (ISS). To investigate the effect of systemic injury, the ISS total is reported, as well as the extracranial ISS (which is calculated as the ISS total—ISS Head/Brain/Cervical [the ISS relating to head and neck injury]). Further, to advise analyses, we created a categorization of patients based on the extracranial ISS. The following categories were defined: isolated head injury (extracranial ISS = 0), minor polytrauma (0 < extracranial ISS < 16), and major polytrauma (extracranial ISS ≥ 16). The use of 16 as a categorization value is accepted in most clinical studies as the Major Trauma Outcome Study associated the threshold with a mortality risk of 10%13,14; however, grouping will be stricter than intended, as it considers the extracranial component of injury only. For example, a patient with total ISS > 16 would traditionally be classed as major trauma but would be classified as minor polytrauma (minor systemic + head injury) in our grouping system.
Statistics
Missing data handling: factor I
Missing data were excluded from any analyses. Of note is the handling of factor I values. Samples were diluted based on the optimal factor for all analytes of the multiplexing assay, which was inappropriate for factor I. Hence, only 36.4% of MFI values were interpolated to the concentrations within the standard curve. For this reason, concentrations reported are for MFIs that fell within the standard curve (36.4%), and hence MFIs are used for temporal representation (recognizing that these results should be interpreted with the above limitation in mind).
Complement inflammation in TBI compared with healthy controls
Median complement concentrations for the patient’s first week post-injury were compared with the single time point of healthy controls using the Wilcoxon rank sum test.
Investigating complement inflammation over time
Daily median concentrations were plotted for the first week (days 1–7), showing the temporal characterization of complement in acute TBI. Then, to investigate how the complement proteins relate to each other within the first week from injury, Spearman’s rank correlations were done on median complement concentrations. Hierarchical clustering was performed using complete linkage and correlation-based distance (1-Spearman correlation) to group similar proteins and cytokines. Spearman’s coefficients reported in the text are reported with 95% confidence intervals estimated via bootstrapping with 1000 resamples.
To investigate how each analyte changes over the course of TBI (acute and long-term), the half boxplot/half jitter plot shows the data distribution for the cohort by day, with single-timepoint healthy controls included for reference.
Principal component analysis
Median concentrations for the first week of injury for each complement protein were scaled for principal component analysis (PCA). Visualizations were subsequently informed by (1) dichotomized outcome at 6 months post-injury (Glasgow Outcome Scale Extended [GOS-E] 1–4 = unfavorable outcome; GOS-E 5–8 = favorable outcome) and (2) trauma category to investigate the effect of isolated head versus polytrauma.
Association between complement and patient outcome
The relationship between scaled complement concentrations and dichotomized outcome was explored with Mann–Whitney’s U test and logistic regression. Analytes that had significant associations with outcome in univariate regression were further explored using a generalized linear mixed effects model, with patient and time from injury taken as random effects. A locally estimated scatterplot smoothing function (LOESS) was used to observe temporal trends. Furthermore, the added prognostic effect of relevant complement proteins was explored with multivariate mixed models. The base model included the International Mission for Prognosis and Analysis of Clinical Trials in Traumatic Brain Injury (IMPACT)-Core 15 clinical prognostic variables age, GCS motor, and pupil reactivity, with day from injury as a random variable. Note that independent patient effects were not considered to reduce model complexity. The adjusted model added C5 as a covariate. Comparison of model performance was evaluated using an ANOVA comparison of log-likelihoods of the two models, the Chi-squared statistic χ2 and p value is reported. Further, we compared the two models using the Akaike Information Criterion (AIC), where a lower AIC indicates a better predictive power. The area under curve (AUC) for receiver operating characteristic (ROC) analyses is reported and plotted.
Association between complement and clinical variables
The association between patient complement analytes (as a median value for the first week post-injury) and clinical variables were explored using Spearman’s correlations, with a correlation matrix plotted for visualization. First week median complement concentrations per trauma patient group (isolated head, minor or major polytrauma) were investigated with the Kruskal–Wallis rank sum test.
All statistics were performed in R Studio (version 4.3.3) with the following R packages: dplyr, 16 tidyr, 17 tidyverse, 18 ggplot2, 19 ggbiplot, 20 ggsignif, 21 gtsummary, 22 pROC, 23 corrplot, 24 pheatmap, 25 caret, 26 lme4, 27 and nlme.28,29 Significance was set at the 0.05 level.
Results
Cohort demographics
Complement proteins of interest (ficolin-3, MASP2, MBL, C2, C4b, C5, C5a, factor D, factor I, C5b9) were quantified in 382 samples from 64 TBI and 17 control patients. The mortality rate of the cohort was 10.9% (7 out of 64 patients died), and dichotomized outcome was available in 55 out of the 64 patients. Table 1 shows the demographic data of the patient population, including clinical and radiological markers of injury severity. Patients with favorable and unfavorable outcome groups were largely similar for all clinical and demographic considerations.
Demographics for the Entire Cohort, and by Dichotomized Outcome Groups
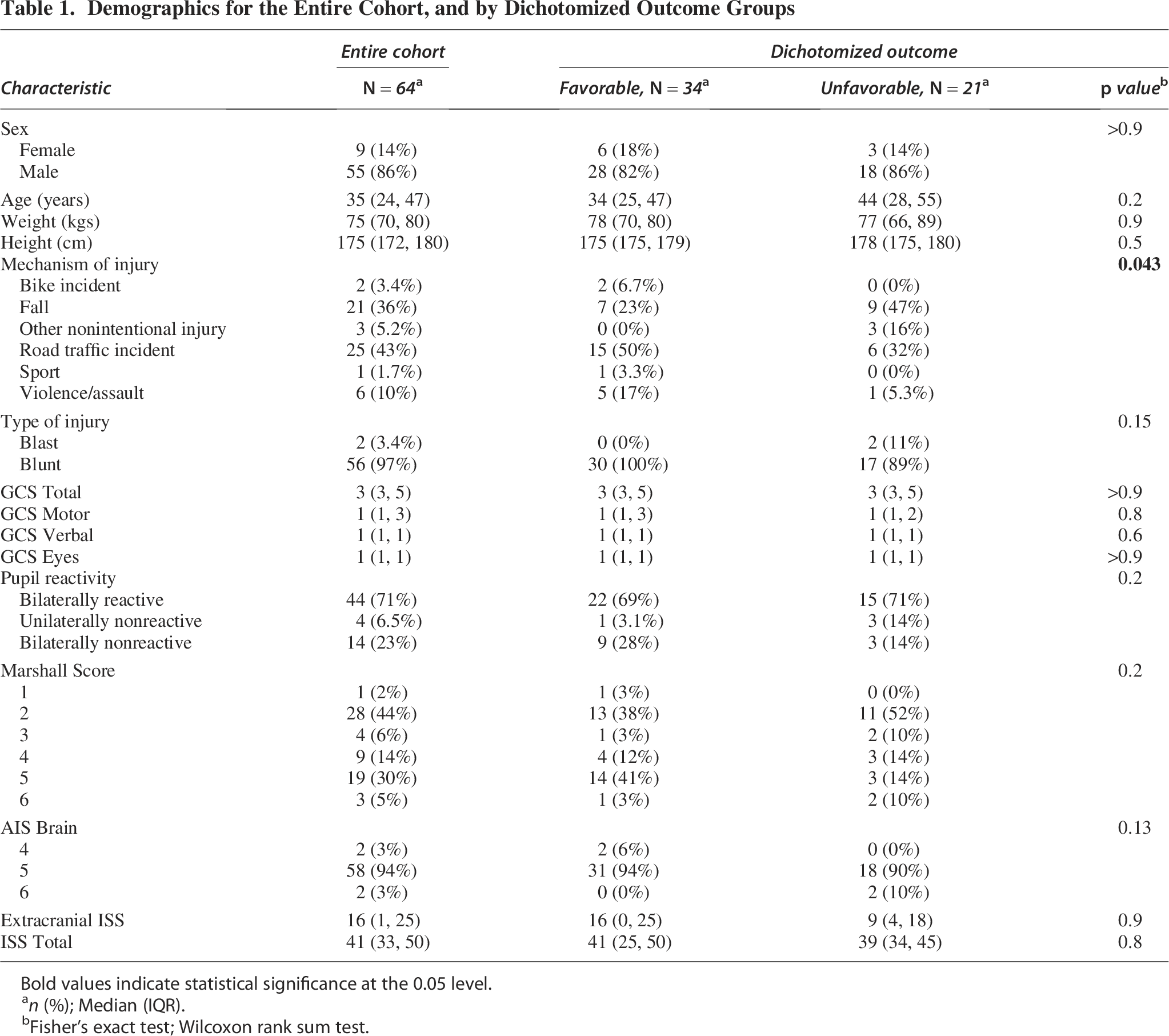
Bold values indicate statistical significance at the 0.05 level.
n (%); Median (IQR).
Fisher’s exact test; Wilcoxon rank sum test.
Complement inflammation in TBI compared with healthy controls: The complement system is activated
Overall, TBI patients had significantly different complement concentrations in their first week post injury compared with healthy controls (Table 2). Initiator MASP2, effector C2, and downstream proteins C5, C5a, and factor I were significantly elevated in TBI patients versus controls. Notably, initiator ficolin-3 was markedly lower in TBI compared with controls (median of 0.22 ng/mL vs. 1.84 ng/mL, p < 0.001). Similar is true for factor D (controls 2044 ng/mL vs. patients 955 ng/mL, p < 0.001).
Patient Median Protein Concentrations for the First Week Post-Injury, as Compared with Single Timepoint Controls
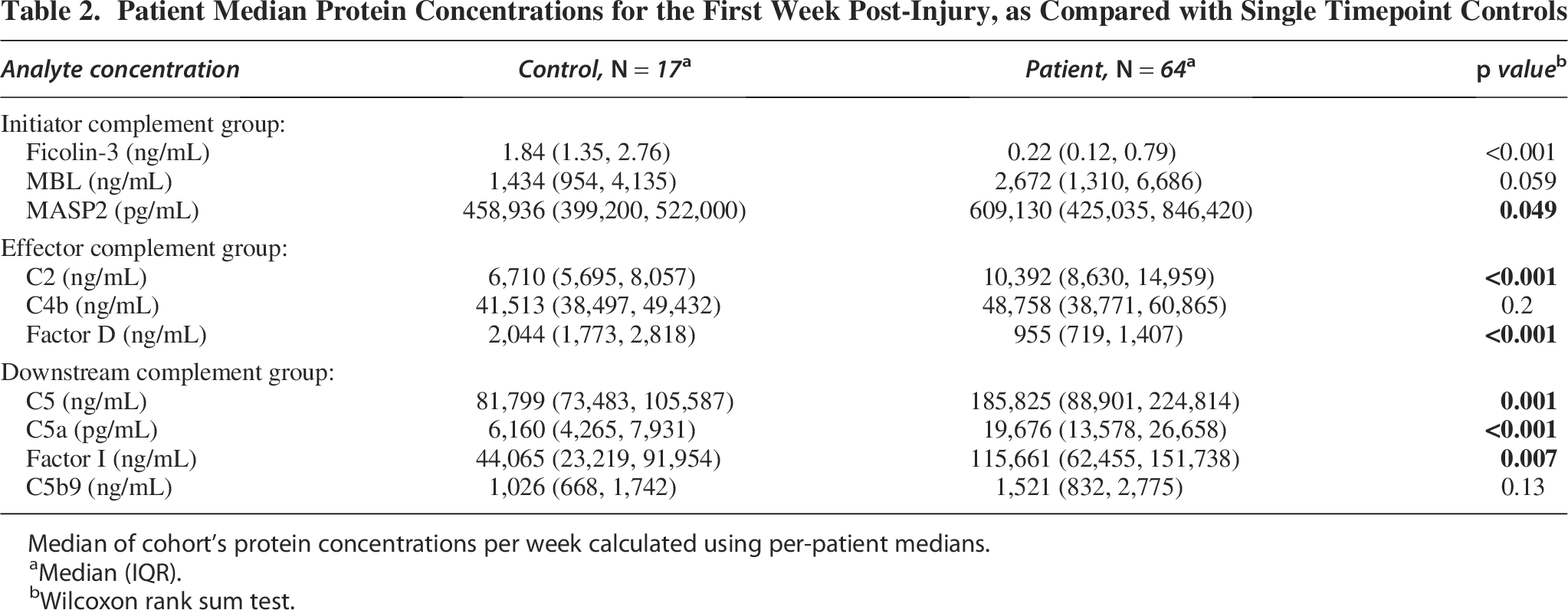
Median of cohort’s protein concentrations per week calculated using per-patient medians.
Median (IQR).
Wilcoxon rank sum test.
Characterizing the temporal trends of complement inflammation in TBI
Figure 2 shows the cohort’s median analyte concentrations per day for the first week post-injury. Single timepoint healthy control concentrations are shown as a dotted horizontal line for reference. Visual inspection of Figure 2 shows that ficolin-3 and factor D levels are consistently lower in TBI patients throughout the first week post-injury and steadily decline in the first week post-injury. Most proteins demonstrate dynamic changes within the first 3–4 days from injury, with some consistent increases or decreases observed after this acute period. MBL, MASP2, C2, C5, C5a, and C5b9 demonstrate steady increases within this first week, remaining elevated compared with the healthy control reference. C4b has a consistent drop in concentration levels in the first 3 days, but then steadily increases to day 1 levels by the end of the first week post-injury.
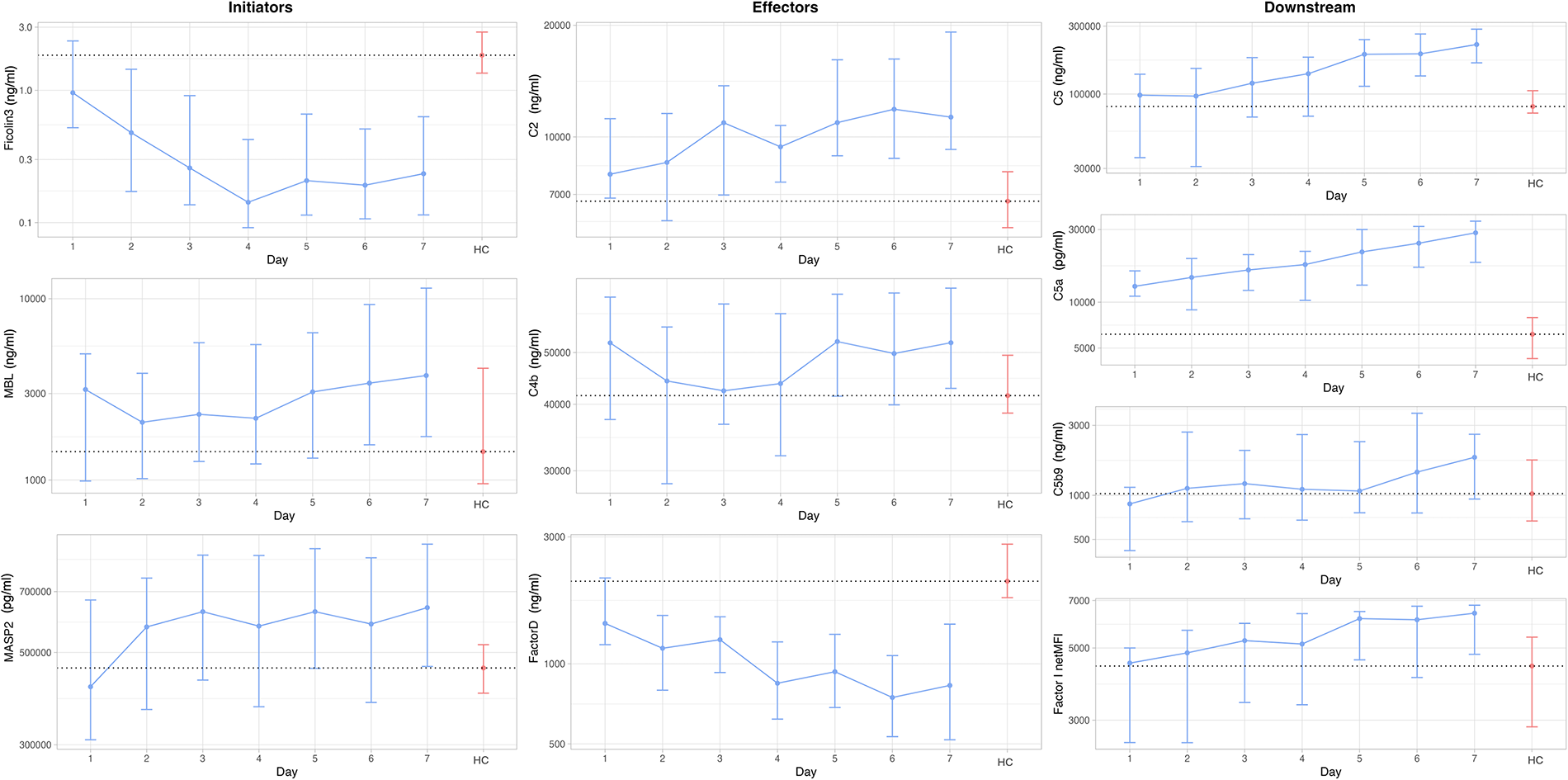
The analyte concentrations for the first week post-ictus, plotted with the single time-point control level as a horizontal dotted line for reference. Proteins are plotted into initiator, effector, and downstream categories for interpretation purposes. Error bars represent the interquartile range, with the sample size used for each time point (across all proteins) presented at the bottom left. Note that factor I is plotted as a net MFI. HC, healthy control timepoint, n, number of data points.
To explore how the complement proteins act in relation to each other, a hierarchical dendrogram shows the correlations of median complement concentrations for the first week post-injury (Supplementary Data S2). Overall, there was a predominance of positive correlations among the proteins, with the strongest correlation being between C5 and factor I (Spearman’s ρ = 0.76, 95% CI [0.62, 0.84]).
Figure 3 shows the data distribution for the cohort during this time, as well as at the later time points day 42, 180, and 365. Notably, ficolin-3 concentrations remain consistently lower than healthy controls, even 1 year post-injury (Wilcoxon rank-sum test between median values, p < 0.001). Large box and whisker plots at all post-injury timepoints suggest a wide range of protein concentrations among patients in the TBI cohort.
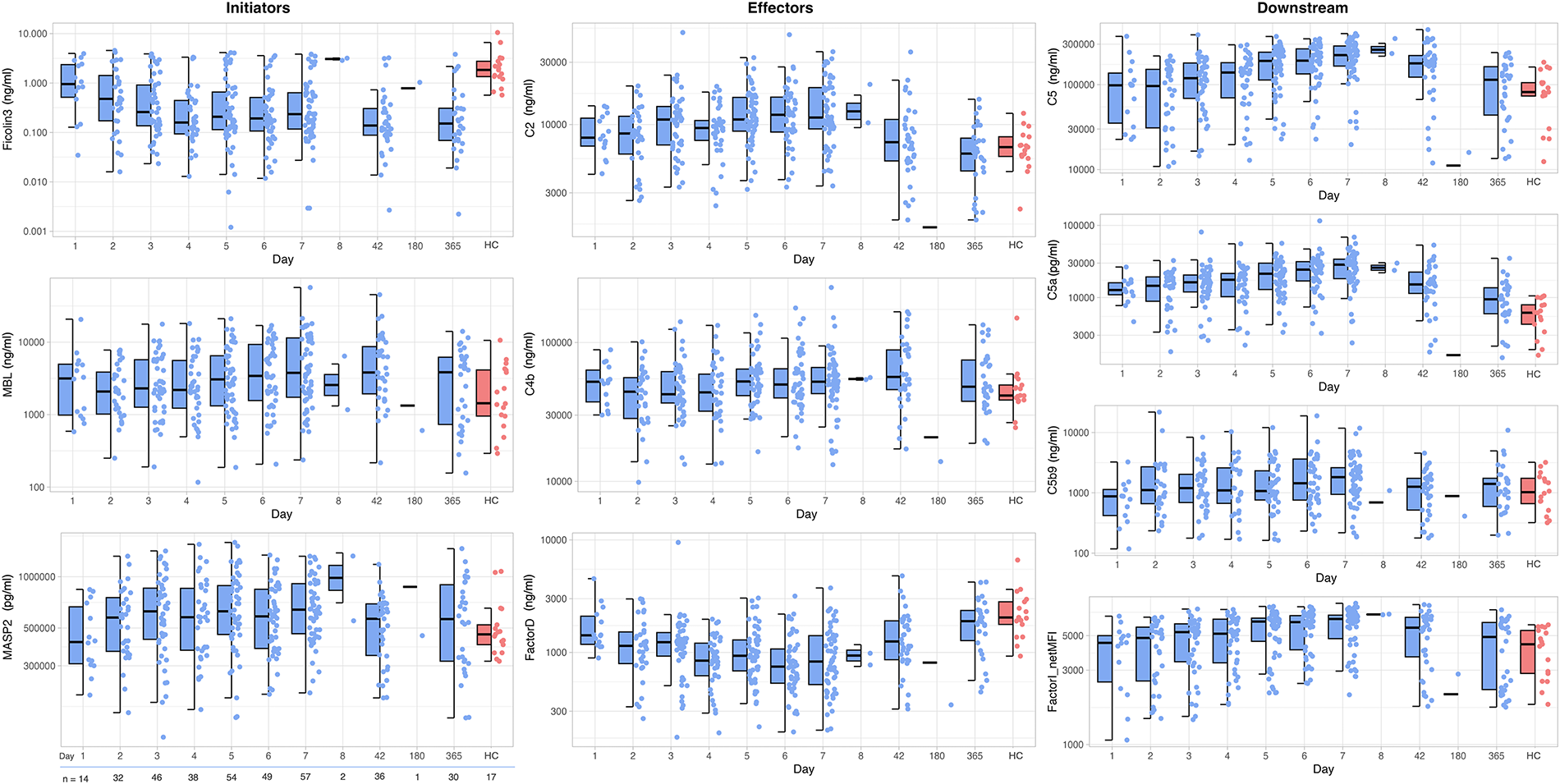
Complement analytes over time, including the later timepoints of days 42, 180, and 365 post-injury. Concentrations are shown as box and whisker plots with corresponding jitter distribution to demonstrate the protein concentration variation for the cohort per day. Note that net MFI levels are used for factor I. HC, healthy control timepoint.
Factor D and I act antagonistically in the complement Cascade
In our TBI cohort, we see a consistent rise in factor I within the first week post-injury, and a simultaneous decrease in factor D levels (Fig. 4). Note that we refer to MFI trends over time with this visualization, as concentration retrieval via extrapolation for all factor I samples was not possible. Notably, proteins contribute to PC analyses in opposite directions (Supplementary Data S3).
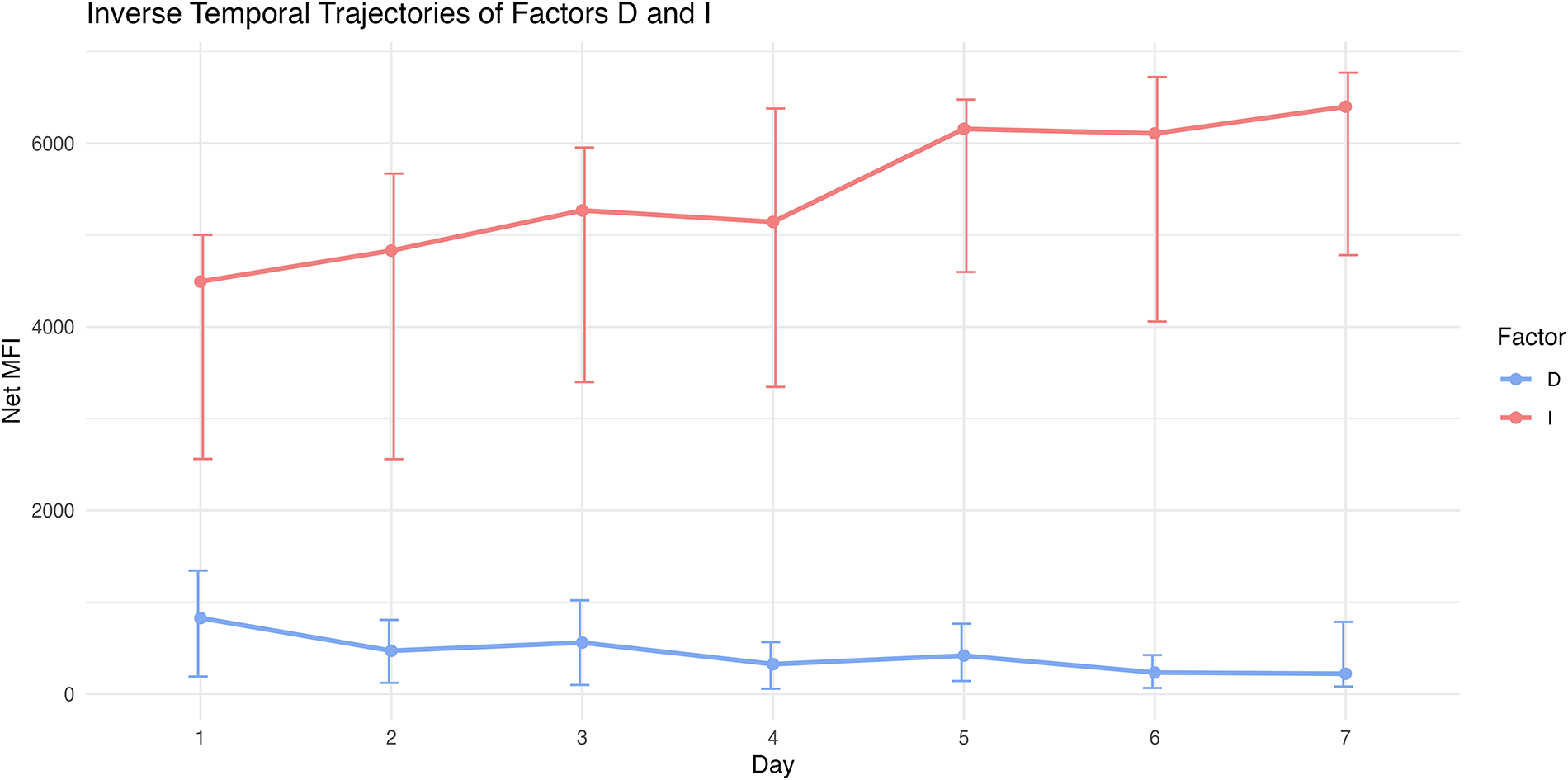
The median net MFI is plotted over time for factor D and factor I, with shading representing the interquartile range. While factor D increases over time, factor D moderately decreases.
Association between acute complement response (first week post-injury) and patient outcome
Table 3 shows the median complement protein concentration for the first week post-injury for the entire cohort, as well as for the outcome groups. Notably, effector protein C4b, and downstream proteins C5 and factor I are higher in patients who had an unfavorable outcome, compared with their favorable counterparts. Furthermore, PCA analyses informed by patient outcome suggest higher complement concentrations for patients that did poorly (Supplementary Data S3).
Median Protein Concentrations for the First Week Post-Injury Presented for Dichotomized Outcome Groups
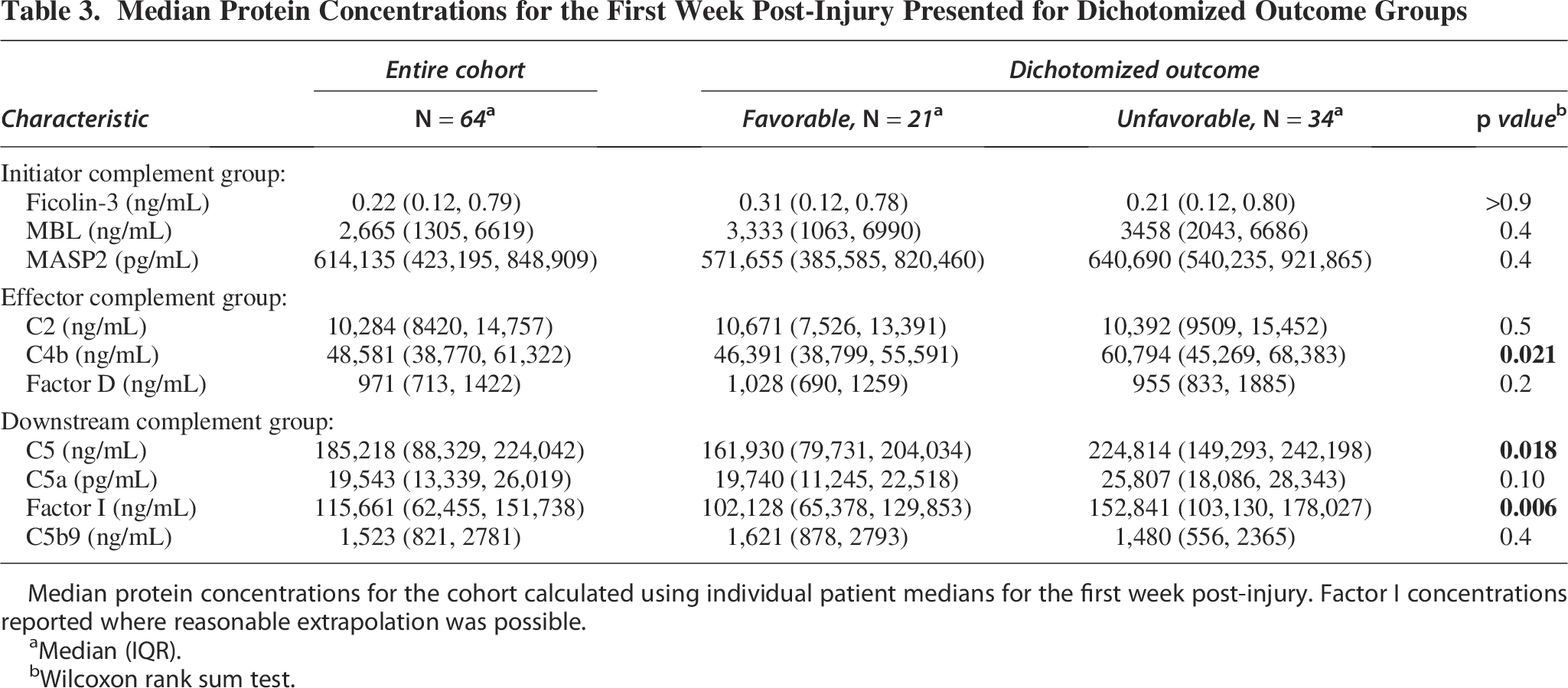
Median protein concentrations for the cohort calculated using individual patient medians for the first week post-injury. Factor I concentrations reported where reasonable extrapolation was possible.
Median (IQR).
Wilcoxon rank sum test.
Logistic regression modelling
All variables were modelled as predictors for dichotomized outcome; however, only C5 was significantly associated with dichotomized outcome. C5 is significantly positively associated with dichotomized outcome in univariate regression, where a median value for the patient’s first week of protein concentration was used (Odds ratio 1.98, with 95% confidence interval 1.11–2.86, p value = 0.029), such that patients with above-median C5 concentrations had nearly twice the odds of a poor outcome. Further, C5 remained significantly associated with outcome in a generalized linear mixed effect modelling where patient and time from injury were random effects (OR: 1.53 [1.52–1.53], p value < 0.001). Trends in C5 concentrations over time for the outcome groups are visualized with a LOESS (Fig. 5). C5 concentrations are distinct between outcome groups: C5 concentrations for patients with unfavorable outcome are consistently elevated in the first week following injury, compared with their favorable counterparts.
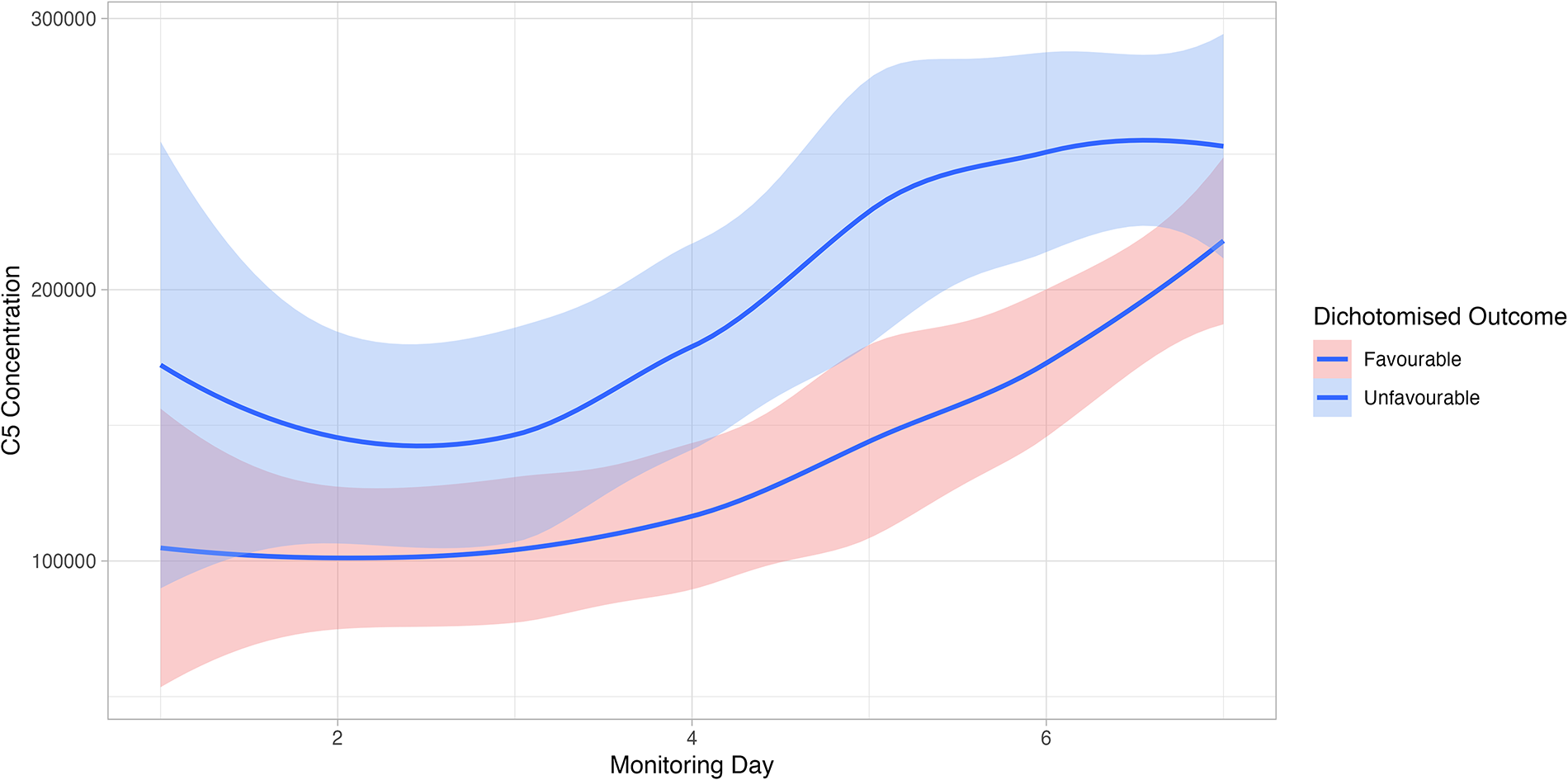
C5 concentrations plotted for the first week post-injury for each outcome group using a nonparametric smoothing function, locally estimated scatterplot smoothing function (LOESS).
Furthermore, to explore the potential prognostic benefit of C5 over and above clinical predictors, we investigated two models for outcome prediction. The base mixed model had the IMPACT-Core clinical predictors age, GCS Motor, and pupil reactivity score (with day as a random effect). The adjusted mixed model included these clinical predictors, with C5 concentration as an added co-variate. In the adjusted model, C5 was significantly associated with dichotomized outcome (OR: 1.99 [1.49–2.66], p < 0.001), suggesting an independent prognostic effect. Comparing the base and adjusted models: adding C5 resulting in an improved model fit (χ2 = 24.50; p < 0.001). The AIC was 329.93 for the base model and 307.44 for the C5-adjusted model, supporting a better fit when C5 was included. Figure 6 shows the added prognostic effect of C5, with an AUC of 0.76 (as compared with the base model AUC of 0.68).
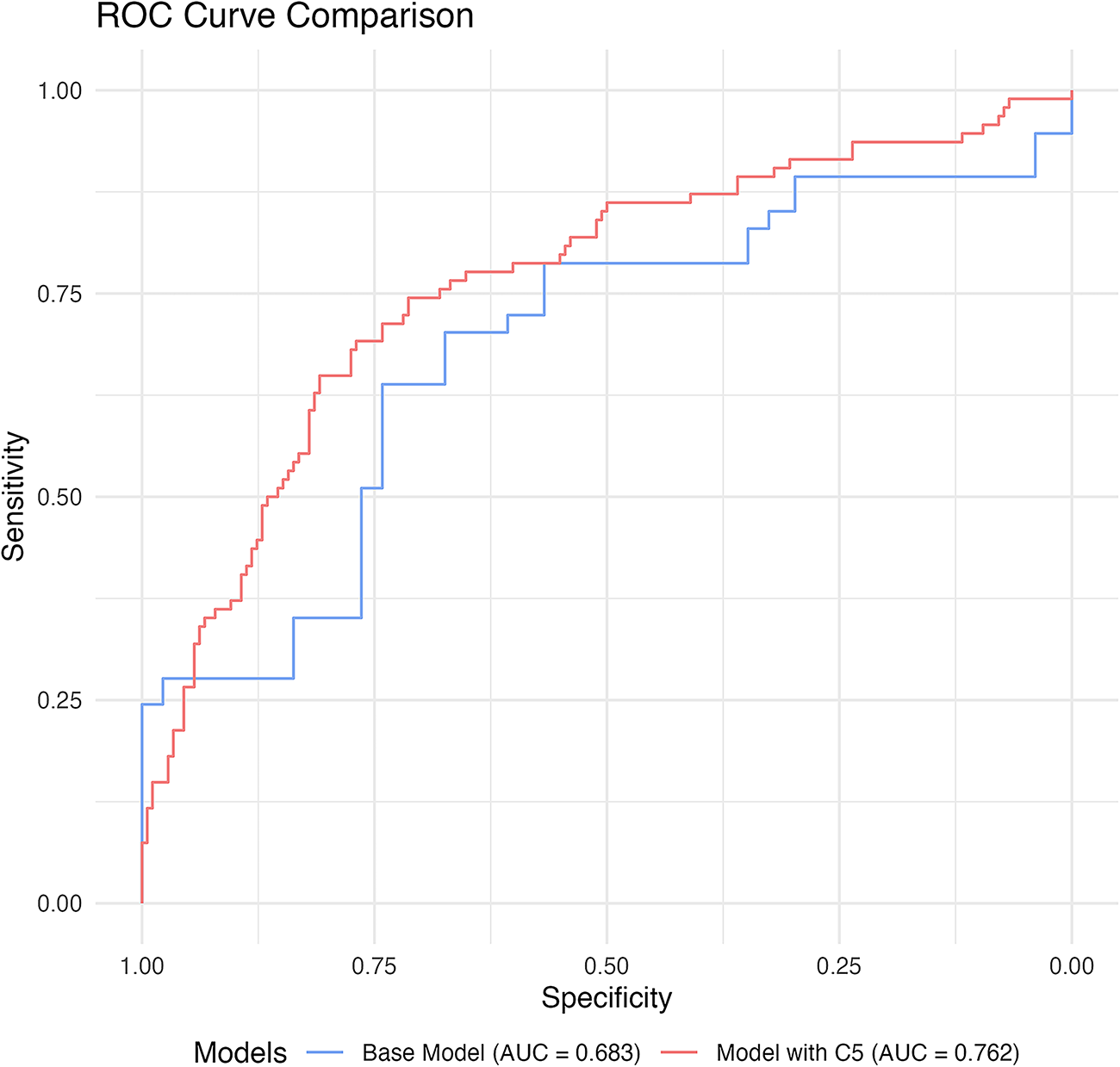
Receiver Operating Characteristic curves for the base model, and adjusted model with C5 concentrations used for outcome prognostication. The base model included age, GCS Motor score, and Total ISS. Areas under the curve (AUCs) are presented for each model.
Complement and clinical metrics
As expected with low mortality numbers, the complement analytes were more strongly correlated with dichotomized outcome than mortality, with positive correlations implying higher complement concentrations associating with unfavorable outcome (Fig. 7). Interestingly, the complement proteins did not correlate with markers of injury severity (GCS motor, AIS brain, and ISS). However, complement proteins correlated positively with age. Investigations of the influence of systemic trauma on complement proteins was done via the trauma categorization; however, complement concentrations were not different between isolated head trauma and polytrauma patients (Supplementary Data S2). Further, complement proteins did not show distinct clustering when informed by trauma category (Supplementary Data S3).
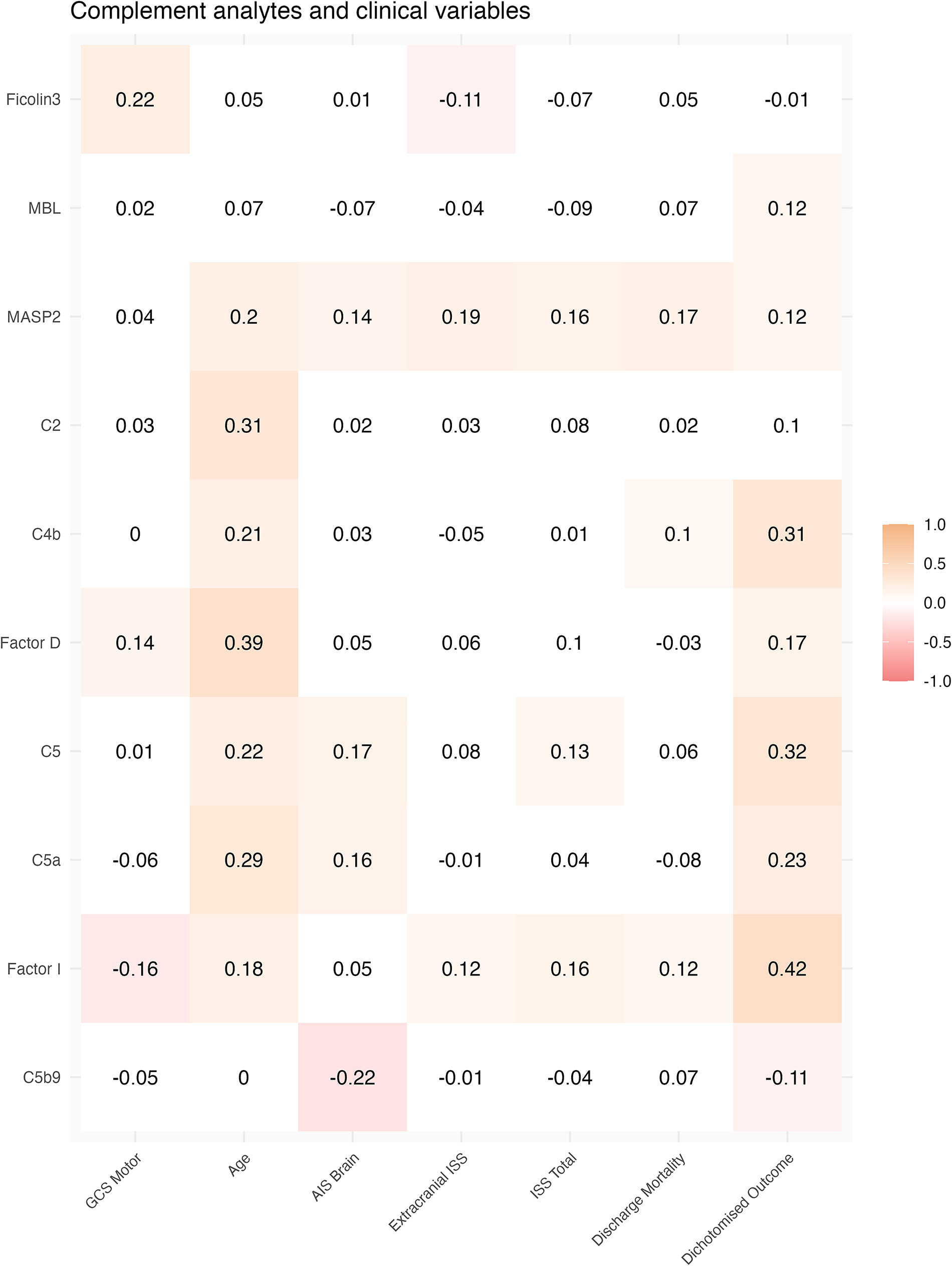
Patient medians of complement concentrations were correlated with baseline clinical characteristics and patient outcomes. The Spearman’s correlation coefficient is shown, with the color of the rectangle indicating positive (orange) or negative (pink) relationships. Median protein concentrations of the patient’s first week post-injury were used.
Discussion
In this prospective analysis of 382 plasma samples from 64 TBI patients and 17 healthy controls, we have characterized the complement cascade as represented by select initiator, effector, and downstream subgroups. We have demonstrated that:
Complement analytes are significantly different in traumatic brain injury patients compared with controls. Notably, factor D and ficolin-3 were significantly lower in patients compared with controls. All other analytes were elevated after brain injury. Temporal profiles of the complement analytes showed dynamic changes within the first week from injury. MBL, MASP2, C2, C4b, C5, C5a, and C5b9 experience steady increases within this first week. Notably, ficolin-3 is consistently lower in patients with TBI compared with healthy controls and remains depressed 1-year following injury. Our clinical results align with biologically plausible: factor D and I are thought to act antagonistically, and we see suggestions of this in the temporal profiles of these proteins. Complement analytes C4b, C5, and factor I are associated with dichotomized outcome at 6 months. Specifically, C5 has a robust association with outcome in both univariate and linear mixed regression, where a higher C5 concentration was associated with unfavorable outcome. Further, C5 adds prognostic benefit over and above known clinical variables. Complement proteins did not correlate with markers of injury severity (GCS motor, AIS brain, and ISS). However, complement analytes correlated positively with age.
This study provides the first known investigation of multiple components of the complement cascade in the context of human TBI. The temporal profiles of our proteins show clear activation of the complement system in human TBI as compared with healthy controls.
Interestingly, ficolin-3 is consistently lower in patients, both as summary values for the first week post injury, and when investigated over time. This finding is consistent with that of Pan et al., whose study of 256 severe TBI patients and healthy controls concluded that serum ficolin-3 levels were lower in patients compared with controls, and that ficolin-3 levels were independently associated with GCS and plasma C-reactive protein levels. They conclude that ficolin-3 could be an independent marker of prognostication in sTBI due to its high predictive value. 30 As ficolins bind to apoptotic and necrotic cells, the decreased level of ficolin-3 in blood is likely due to consumption: ficolin-3 is recruited to the site of destruction during the acute period of sTBI.30–32 Hence, the level of detectable, free-floating ficolin-3 in blood is decreased. Further, decreased ficolin-3 levels are associated with increased complement activation. 33
Of all the proteins investigated in our study, ficolin-3 has a relatively weak association with GCS motor (Spearman’s coefficient of −0.22). Other studies (including those in ischemic stroke, 34 and aneurysmal subarachnoid hemorrhage 35 ) suggest the use of ficolin-3 as a biological marker of injury severity because of their strong correlation findings.
Factor I is a crucial regulatory protein of the complement system. It functions to regulate complement activation, specifically, it is known to act at the C3 level by degrading activated complement components C3b and C4b in the presence of its cofactors. 36 C3 is activated by factor D, 37 and hence, factor I acts antagonistically to factor D, and we see suggestions of this relationship in the clinical TBI setting.
We demonstrate significantly elevated levels of MASP2 in TBI compared with controls (609,130 vs. 458,936 pg/mL, p = 0.049). While MBL concentration in TBI is higher than that of controls, it fails to reach statistical significance in our cohort (2672 vs. 1434 ng/mL, p = 0.059). However, other clinical TBI studies support the use of MBL as a strong prognostic marker of head trauma. 5 As our work included several markers of the lectin-activated pathway (ficolin-3, MBL, MASPs), we can specifically comment on this pathway in human TBI. The elevation of MBL and MASP2 in TBI compared with controls and the temporal profiles of these lectin markers imply activation of the lectin pathway of complement. Our findings, taken in context with that of De Blasio et al. who confirm the direct presence of lectin pathway components in cerebral contusions and association with injury severity and outcome, 6 suggest a central role for the lectin complement pathway in the pathophysiology of human TBI.
We show that C5, a protein common to the lectin, alternative and classical pathways of the complement system, has a strong association with outcome. Patients with unfavorable outcome have higher concentrations of C5 compared with their favorable counterpart (224,814 vs. 161,930 ng/mL, p = 0.018), and this trend is demonstrated over time (OR: 1.53 [1.52–1.53], p < 0.001). Further, C5 concentrations are not only independently associated with outcome, but improve prediction of outcome over and above known clinical variables (AUC of 0.75 as compared with the base model AUC of 0.69). C5 concentrations may act as a biomarker for general complement activity in TBI. However, the complexity and nuances of the cascade’s activation pathways are particularly relevant in the heterogeneous TBI population, with the lectin system showing promise in injury pathophysiology.
Limitations
While we show consistent differences in complement proteins in TBI versus controls, we do not show direct pathway activity. To show evidence of complement activation, one would need to do an activation assay, which was out of the scope for this analysis. Notably, analyses did not adjust for multiple comparisons. Factor I results should be interpreted in the confines of the methodological considerations mentioned. For future studies, we recommend that researchers consider this limitation of multiplexing given the analytical range available.
As we measured complement proteins in the blood of patients with TBI, we cannot comment on whether the proteins originate from the brain or the systemic circulation/tissues. As TBI patients often experience simultaneous systemic injury that triggers an inflammatory reaction, the overlap of brain- versus systemically derived inflammatory markers is yet to be understood. While the liver is a known production site for complement, there have been several studies showing evidence of complement deposition in the brain.6,38–40 In fact, complement is present even in healthy cerebrospinal fluid and is thought to play a role in cerebral immunosurveillance. Complement is produced intracerebrally, by resident cells of the brain.40–42 After injury, it is likely that complement is produced locally, as well as occurring as part of passive leakage across a leaky blood–brain barrier. We have attempted to investigate this in patients who had isolated, minor or major polytrauma (based on extracranial ISS score categorization) and show no clustering in PCA analyses nor difference in complement concentrations. While we recognize this “trauma categorization” is an oversimplification, it allows for preliminary investigations of the influence of systemic complement in TBI. However, we cannot differentiate origin/production in the brain versus the systemic circulation based on our data.
In addition, there are other sources of complement in TBI patients in the days following injury that may arise not only from extra-cranial injuries but also from secondary infections (such as hospital-acquired pneumonia), surgical procedures, and systemic inflammatory response syndrome. These confounders may not be captured in our data. Notably, while most patients would represent severe brain trauma (median GCS total 3), the inclusion criteria did not exclude those of moderate severity, and subsequent stratification based on clinical severity was not possible.
Conclusion
To our knowledge, this is the first characterization of complement in human TBI, as represented by multiple proteins along various stages of complement in the first week post-injury. We describe the temporal profile of these proteins, and their association with outcome and clinical variables after TBI. Further, we have investigated levels of complement proteins up to 1 year after injury. Our analyses strongly suggest the involvement of complement in the first week post-injury in human TBI, and in the case of ficolin-3, this persists up to 1 year post-injury. Further, complement was consistently associated with unfavorable patient outcomes.
Transparency, Rigor, and Reproducibility Summary
The ICON-TBI technical summary, planned impact, and funding details are listed on the UK Research and Innovation website (https://gtr.ukri.org/projects?ref=MR%2FR005036%2F1#/tabOverview). The analysis plan was not formally pre-registered. The original trial included 175 patients, but the sample size of this study was determined by the amount of available biological samples and resulted in a considerable cohort of 64 patients. Handling of biofluid samples, and fluid biomarker measurements, were performed by investigators who were aware of characteristics of the participants. Patient samples were acquired once daily for the first 10 days following injury, and the study was active between 2017 and 2021. Details of processing are available in the methods, but samples were stored at −80°C until batch analysis. Samples were randomly assigned for analysis over 10 separate batches, all done using the exact same protocol (reagents, assay plates, laboratory conditions, etc.). Quantification quality control across assays is specified in Supplement A—in short, we confirm acceptable quantification according to the manufacturer standard. We encountered a challenge with Factor I quantification, details of which (and subsequent handling) are available in the methods section. All equipment and analytical reagents used to perform protein quantification are widely available from Luminex, Abexxa, and Abcam. The primary clinical outcome is an established standard in the field (dichotomized patient outcome at 6 months using the GOS-E version, with inclusion of additional clinical prognosticators). Statistical tests for non-parametric data were used, but multiple comparisons were not accounted for. Interquartile ranges and 95% confidence intervals are reported where possible. Statistical analyses were checked by all authors of this article. A prospective external validation study is planned, with patient recruitment currently underway. Deidentified data and analytical code from this study may be made available upon reasonable request to the corresponding author. All collected biofluid samples were used in this and other studies; hence, insufficient quantities remain for future research. The authors agree to publish this work using the Mary Ann Liebert Inc. “open access” option under the appropriate license.
Authors’ Contributions
A.H. and D.M. conceptualized and designed the study. A.J., V.D., and E.N. recruited patients as part of the ICON-TBI study and collected all biological samples. C.A.S. and A.S. did the proteomic analyses. C.A.S. did all data handling/processing. C.A.S. did the statistical analyses, with support from R.S. and E.N. C.A.S. wrote the article, with final approval from all authors.
Footnotes
Author Disclosure Statement
The authors have no competing interests and nothing to disclose.
Funding Information
The ICON-TBI study was funded by the Medical Research Council, while the Cambridge recruitment was funded by the TBIcare Grant (a European Commission Framework 7 projects; UK PI: DM). Further analyses were supported by Addenbrooke’s Charitable Trust (Grant no. 900404). Individual author funding as follows: C.A.S.—The Patrick and Margaret Flanagan Skye Cambridge Trust Scholarship; R.S.—NIHR Grant (NIHR304175); D.M.—Cambridge Biomedical Research Centre and NIHR Senior Investigator Awards and the British Oxygen Professorship of the Royal College of Anaesthetists; E.J.N.—Brain Research UK; A.H.—Medical Research Council/Royal College of Surgeons of England Clinical Research Training Fellowship (Grant no. G0802251), MRC Grants (MR/X021882/1, MR/Y008502/1) the NIHR Biomedical Research Centre and the NIHR Brain Injury Health Tech Research Centre and NIHR Grant (NIHR129748); The views expressed are those of the authors and are not necessarily those of the NIHR, the Department of Health and Social Care or of any of the other funding bodies.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.