
Abstract
Traumatic brain injury (TBI) frequently results in long-term cognitive deficits due to traumatic axonal injury and disruption of structural brain connectivity. Computerized cognitive remediation (CCR) has shown promise for improving cognitive outcomes in chronic TBI; however, diffusion imaging studies evaluating its effectiveness have often relied on tensor-based metrics that are limited in their ability to detect subtle treatment-related changes. This study used correlational tractography, a diffusion magnetic resonance imaging (dMRI) connectometry method sensitive to localized, fiber-specific changes, to investigate the effects of CCR on white matter microstructure in adults with chronic TBI and to further examine the relationship between white matter changes and improvements in cognitive function. Seventeen adults with chronic mild to severe TBI were assigned to an experimental group (n = 10), who received 40 hours of CCR over 14 weeks, or a nonintervention control group (n = 7). All participants underwent dMRI scans and cognitive assessments at pre- and postintervention visits. Correlational tractography was used to assess differences in longitudinal change of normalized quantitative anisotropy (QA), a tensor-free metric associated with axonal density and plasticity, across whole-brain white matter between CCR and nonintervention control groups. Following the intervention period, increased QA was observed in the CCR group, relative to the nonintervention control group, and changes in QA in the CCR group were related to improvements on objective measures of processing speed, attention, and working memory. These results provide preliminary evidence that CCR may promote white matter plasticity in relation to improved cognitive function in individuals with chronic TBI. Furthermore, by leveraging QA and correlational tractography, we were able to detect regionally specific changes that may have been overlooked using traditional tensor-derived diffusion metrics or tract-averaged approaches. Overall, our findings support the potential of CCR as a scalable intervention to facilitate structural and functional plasticity in adults with chronic TBI.
Keywords
Introduction
Approximately 50–60 million people globally suffer from a traumatic brain injury (TBI) each year, causing substantial health and economic burdens worldwide.1,2 Of those who survive a TBI, roughly 43% experience chronic functional disability, 3 and in the United States alone, approximately 5.3 million individuals are currently living with long-term disability due to their TBI.4,5 A common consequence of TBI is traumatic axonal injury (TAI), which is characterized by morphological changes to axons, ion imbalance, and impeded axonal transport. 6 Furthermore, TAI-induced disruption to cerebral white matter leads to a cascade of impairments 7 in processing speed, attention, memory, and executive function.8,9 These cognitive deficits profoundly affect daily functioning, impacting employment, social interaction, and overall quality of life.10,11
The injury-induced alterations to structural connectivity observed after TBI reflect a combination of primary and secondary damage in the acute/postacute stages of recovery and the adaptive and maladaptive neuroplastic changes that occur in the postacute and chronic recovery periods. 12 These neuroplastic processes also underlie the brain’s capacity for recovery, wherein repeated, coordinated neural activity strengthens co-activated synapses, forming the foundation for functional restoration and structural recovery.13,14 This capacity for experience-dependent neuroplasticity forms the theoretical foundation of restorative cognitive training approaches, which engage top-down, Hebbian mechanisms of network plasticity,15–17 including activity-dependent myelination, oligodendrocyte proliferation along frequently co-activated pathways, more efficient signal transmission through axonal remodeling and synaptic strengthening stimulated by high-frequency repetition, and enhanced neural synchronization that improves functional connectivity and promotes structural plasticity across distributed networks.15,16,18–20 As opposed to compensatory training, which involves adaptive strategies to minimize the impact of deficits, 21 restorative, plasticity-based training leverages these Hebbian principles to reverse the maladaptive neuroplastic changes that often characterize the chronic stages of TBI and improve cognitive functioning by targeting neuromodulatory processes that promote neurological renormalization across various system levels of recurrent brain networks via top-down biasing.15,16,19 Such interventions rely on the notion that adaptive neuroplastic changes may be stimulated through focused training exercises targeted toward systematic engagement of specific functional domains and suppression of neurological distractors that disrupt sensory processing, learning, and memory.16,22,23 These principles are supported by the results of investigations into the biological mechanisms underlying restorative training-related brain changes in animals and humans, which have demonstrated long-term potentiation and synaptic strengthening,24,25 enhanced neurogenesis, 26 increased blood flow and neurovascular coupling,24,27 and reduced neuroinflammation. 24
Growing evidence has demonstrated the efficacy of neuroplasticity-based, computerized restorative interventions, such as computerized cognitive remediation (CCR) programs that target foundational cognitive skills, including processing speed, attention, and working memory across healthy aging, TBI, and other clinical populations.18,21,28–32 CCR programs that target processing speed have shown particular benefit in TBI, as slowed information processing is a common consequence of TAI, and inefficient processing constrains higher-order cognitive functions. 33 Large-scale CCR trials utilizing processing speed training have demonstrated long-term maintenance of near transfer effects for up to 5 years,28,29,34 and these benefits have been shown to broadly extend to everyday quality of life,35,36 resilience to depression, 36 confidence for independence, 37 and enhanced brain health34,37 in older adults for up to 10 years.34,38,39 In TBI, studies employing CCR have demonstrated more generalized improvements to cognitive function,31,40–42 and we have recently shown improvements to resting-state functional connectivity in the present TBI sample following CCR. 43
Diffusion magnetic resonance imaging (dMRI) has also demonstrated sensitivity in detecting training-related structural plasticity in healthy44,45 and neurological populations;32,46,47 however, inconsistent results have been observed using diffusion tensor imaging (DTI) in TBI, despite observable cognitive improvements.46,48,49 Inherent limitations of the tensor model50–53 reduce its sensitivity to subtle microstructural changes typical of intervention studies. To address the limitations of DTI, generalized q-sampling imaging (GQI) 54 was developed as a model-free diffusion reconstruction technique that accurately quantifies free, restricted, and anisotropic diffusion contributions within each voxel. GQI-derived normalized quantitative anisotropy (QA) is a measure of anisotropic diffusion density that is calculated by sampling the peak orientation of the spin distribution function (SDF) at each voxel and measuring the amount of anisotropic diffusion along that direction. 55 QA is robust to the confounding effects of edema, inflammation, partial volumes, and crossing fibers,54–56 providing a fiber-specific metric with improved accuracy, particularly in regions with complex fiber architecture and low signal-to-noise environments.55,57 Thus, QA is a more sensitive and accurate measure of microstructural integrity than tensor-derived fractional anisotropy (FA), and higher QA is associated with axonal density and plasticity.55,58
The full potential of advanced diffusion metrics like QA is realized through analytical approaches that can detect subtle, localized changes in white matter. Historically, dMRI studies have relied on diffusion metrics averaged across entire white matter tracts. However, this approach may mask region-specific variations, thereby reducing the sensitivity and precision of the findings. 59 Diffusion connectometry is an advanced analytical technique capable of identifying these subtle variations by quantifying local connectivity patterns along the most affected segments of fiber pathways. 60 Unlike traditional approaches that examine global structural connectivity between anatomical endpoints, connectometry centers on the local connectome, which represents the degree of connectivity between adjacent white matter voxels, defined by the density of diffusing spins along specific fiber orientations. This enhances sensitivity to region-specific changes that may reflect neuroplasticity, degeneration, recovery, and other characteristic features of TBI, particularly in mild cases where conventional diffusion analysis may yield normal results. 58 Correlational tractography builds on this method by applying permutation testing on the local connectome with false discovery rate (FDR) correction to identify areas along white matter pathways that express variability in relation to a particular variable of interest, allowing for detailed mapping of brain–behavior relationships, even in clinical populations where diffuse or heterogeneous patterns of white matter pathology are expected.61–63 Recent feasibility research has effectively utilized correlational tractography to track changes in white matter microstructure in chronic mild TBI, implicating QA as a potential biomarker for evaluating axonal injury and repair.58,64
Given these methodological advantages and prior evidence supporting the efficacy of CCR to improve cognitive function and functional connectivity, the current study aims to use correlational tractography to evaluate the effects of CCR on microstructural changes in the white matter in chronic TBI. The relationship between changes in white matter microstructure and improvement on objective and subjective measures of cognitive performance is also explored. It is hypothesized that increased QA will be observed in individuals who undergo CCR, relative to those in a nonintervention control group, and that increased QA will be associated with improved scores on cognitive measures within the CCR group.
Method
Participants
Approval was obtained from the New York University Grossman School of Medicine Institutional Review Board prior to beginning the study, and this research was completed in accordance with the Declaration of Helsinki and its later amendments. All participants were screened for eligibility before enrollment and provided written informed consent prior to participation. Sixty-four adults with chronic mild to severe TBI (n = 50) or stroke (n = 14) were recruited from outpatient brain injury rehabilitation centers and clinics in the New York metropolitan area as part of a larger acquired brain injury (ABI) study. The inclusion criteria were ages between 18 and 70 years and a history of ABI occurring at least 12 months prior to participating in the study. Medical records were used to verify the history of ABI, and the mechanism of injury was self-reported. Exclusion criteria included any history of other neurological disorder; any history of bipolar disorder, schizophrenia, or alcohol or substance use disorder; and current use of benzodiazepine, anticonvulsant, or neuroleptic medications. TBI severity was determined in accordance with the American Congress of Rehabilitation Medicine 65 and Mayo Classification System for TBI severity. 66
A quasi-randomized approach was used for CCR or nonintervention group assignment. Participants who were randomized to the CCR group were reassigned to the nonintervention control group if they were unable to meet the demands of in-person training (four participants with TBI were reassigned to the nonintervention control group for this reason). If a participant chose to be reassigned, the vacated CCR group assignment was randomly applied to a future eligible participant. Participants in the CCR group were compensated through the provision of 30-day unlimited-use MTA MetroCards (valued at $114 each) for every month of training. These cards could also be used for personal travel throughout the city, thereby offsetting the time and cost of commuting to the laboratory. Participants assigned to the nonintervention control group were contacted weekly by telephone during the 14-week period between baseline and follow-up assessments and asked to report the amount of time spent engaging in cognitively stimulating activities (e.g., reading, exercising, completing puzzles) over the previous week, which was documented. The final sample resulted in 31 (22 TBI; 9 stroke) individuals assigned to the CCR group and 33 (28 TBI; 5 stroke) assigned to the nonintervention control group. Due to the requirement for supervised, in-person training, neither investigators nor participants were blinded to group assignment. An illustration of the 16-week timeline of participation is provided in Figure 1.
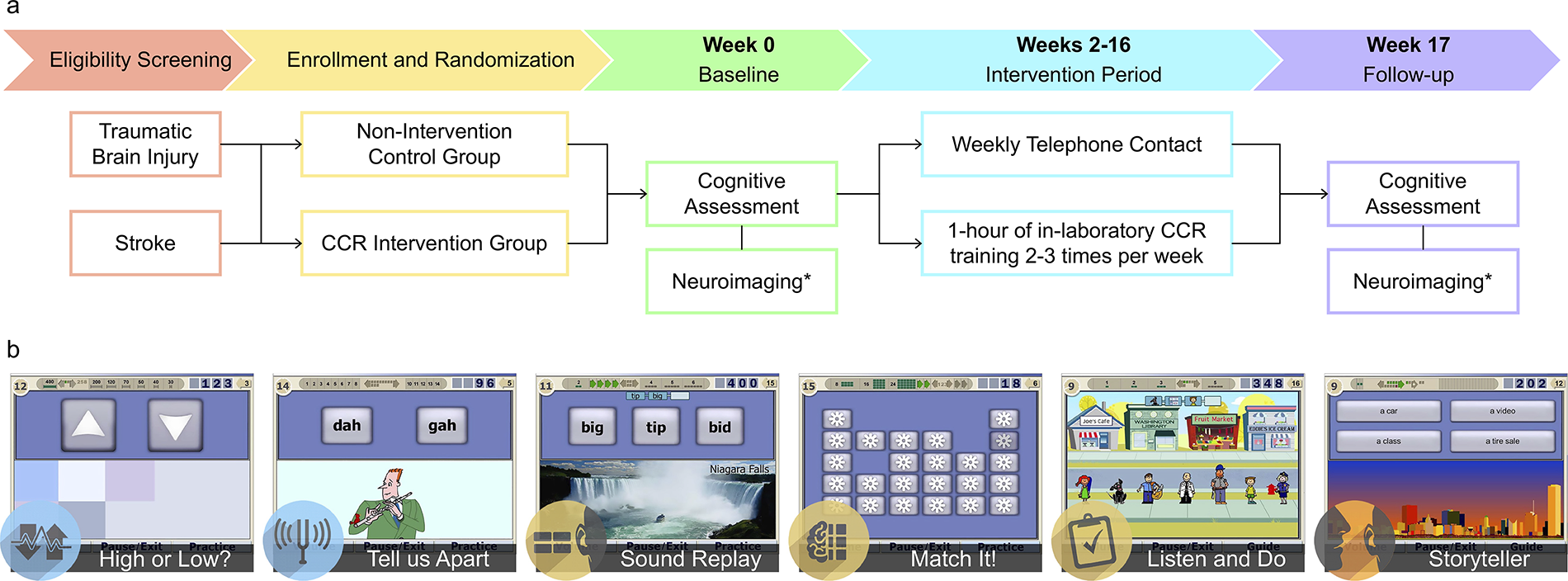
Timeline of participation and intervention. The progression of participation through the study is illustrated along with individual components of each phase
The present study focused on a subset of the original sample that included 23 individuals with TBI who were willing and able to complete the optional neuroimaging component of the study. A comparison of baseline demographic and injury characteristics between the present subset and individuals with TBI from the larger sample who opted out of neuroimaging (n = 27) is provided in the Supplementary Table S1. No significant differences were observed across baseline characteristics between those with and without neuroimaging data.
Cognitive intervention
The CCR intervention implemented was the Brain Fitness Program (BFP) version 2.0.1b (Posit Science, San Francisco, CA). The BFP targets auditory information processing speed and has been effective for long-term maintenance of improved cognitive functioning and structural integrity in healthy older adults.18,29,67,68 It was specifically designed to harness well-established principles of neuroplasticity, including Hebbian learning and activity-dependent myelin plasticity, to accelerate neural conduction.18,20 Exercises are structured to drive synaptic strengthening and structural remodeling through repeated, precisely timed auditory stimulation. 69 Difficulty adapts in real time to maintain ∼85% accuracy, creating optimal conditions for spike-timing dependent plasticity and engagement of neuromodulatory systems essential for long-term potentiation.15,18 This biologically grounded design distinguishes the BFP from general cognitive training interventions by targeting circuit-level remodeling through temporally precise, adaptive, high-repetition tasks. 41
The BFP comprises six 15-minute exercises (Fig. 1b) that involve the time order judgment of pairs of frequency-modulated sweeps (High or Low?), discrimination of confusable syllables (Tell us Apart), recognition of sequences of confusable syllables (Sound Replay), matching pairs of confusable syllables (Match It!), reconstruction of sequences of verbal instructions (Listen and Do), and identification of details in a verbally presented story (Storyteller).18,29 Each of the cognitive exercises becomes progressively more difficult through the systematic reduction of the inter-stimulus interval, stimulus duration, or increased auditory complexity. Participants completed four of the cognitive training exercises at each of the 40 one-hour training sessions. Participants were expected to complete 3–4 training sessions each week for 14 weeks, and all training sessions took place in a private laboratory space under the supervision of a research assistant to ensure compliance. As the intervention involves both visual and auditory modalities, participants were provided with noise-canceling headphones to wear during each training session.
Neuropsychological assessment
The cognitive measures included in the present analysis were selected based on prior work 42 that demonstrated significant improvements in these outcomes following CCR in the larger TBI sample, from which the current subsample was drawn. A comprehensive list of assessments administered at both visits and the aforementioned results are reported previously. 42 The Wechsler Test of Adult Reading (WTAR) 70 is a 50-item word-reading task used to estimate premorbid intelligence. The Trail Making Test, part A (TMTA) 71 is a widely used measure of visual attention, processing speed, and psychomotor ability, where examinees are required to draw a line connecting randomly placed circles numbered 1–25 in order and as quickly as possible. The Understanding Directions (WJUD) subtest of the Woodcock Johnson–III (WJ-III) Tests of Achievement battery 72 measures auditory attention and working memory where the examinee is asked to point to objects in a picture after listening to increasingly more complex sets of oral instructions. The 25-item Cognitive Self-Report Questionnaire 73 is a subjective measure of one’s everyday cognitive functioning, on which participants indicate the presence and extent to which they have suffered from cognitive, social, and hearing difficulties over the previous 2 weeks; the Cognitive subscale (CSR-C) is based on the 10 items related to perceived cognitive abilities. Demographically corrected T-scores (M = 50 ± 10) were used for the TMTA and CSR-C, and raw scores were used on the WJUD (total correct range = 0–57). As such, lower scores on the CSR-C indicate fewer symptoms, and higher scores on the TMTA and WJUD indicate better performance.
Neuroimaging
Acquisition
Diffusion data were acquired at the Center for Biomedical Imaging of New York University’s Langone Medical Center on a 3T Siemens Tim Trio or Prisma Fit whole-body scanner using a 12-channel head coil. The diffusion acquisition included a high-angular resolution, single-shot echo planar imaging (EPI) sequence with 55 slices and a GRAPPA factor of 2, which was applied at a b-value of 1000 s/mm2 across 64 noncollinear diffusion-weighted directions and three nondiffusion b0 images. The following additional parameters were used: TR/TE = 7000/85 ms, in-plane field of view (FOV) = 220 × 220 mm, matrix = 100 × 100, voxel size = 2.2 mm isotropic, and flip angle = 90°. To correct for EPI distortions, field maps with matching geometry were acquired using a dual-echo spoiled gradient recall echo sequence with the following parameters: TR/TE1/TE2 = 843/8/10.46 ms, FOV = 230 × 230 mm, matrix = 104 × 104, voxel size = 2.2 mm isotropic, and flip angle = 70°. All participants were scanned on the same scanner at baseline and follow-up.
Preprocessing and reconstruction
Preprocessing included the initial extraction of an individual b0 volume, which was then fed into the brain extraction tool 74 from the FMRIB Software Library (FSL) 75 to generate a skull-stripped brain mask for each subject. Susceptibility-induced EPI distortions were corrected from field maps using prelude (unwrapping) and fugue (unwarping) tools in FSL. The estimates produced from the brain mask and the EPI-corrected diffusion data were then fed into FSL’s eddy tool for eddy-current and motion distortion correction.
To minimize the risk of false positive results, the following quality control protocol 76 was applied to all preprocessed data prior to reconstruction: (1) the consistency of image acquisition parameters between pre- and postintervention scans was verified; (2) DWI contrast estimates were calculated, with an exclusion threshold of values falling below 1.1; (3) the neighboring diffusion-weighted correlation coefficient was calculated, with an exclusion threshold of r ≥ 0.10 differences for any between-subject scans; (4) each slice of each diffusion image was assessed for signal dropout, and a threshold for inclusion set at < 1% of slices affected (one subject was excluded based on this criterion); and (5) the correct b-table orientation was confirmed using the fiber coherence index. 77 To obtain the SDF, all data that passed the quality checks were then reconstructed in MNI space using q-space diffeomorphic reconstruction 53 with a diffusion sampling length ratio of 1.25 and an isotropic output resolution of 2 mm. The goodness-of-fit for the transformation to template space was assessed, and dataset(s) were excluded if the R2 value fell below 2.5 standard deviations from the sample mean (one subject was excluded based on this criterion). All remaining data were inspected visually to confirm quality. Subject-specific local connectome fingerprints 78 in template space were then compiled into a local connectome matrix in DSI Studio 79 for group analysis. Longitudinal change in QA was calculated as the absolute difference (time 2–time 1) to provide a more stable estimate of change across subjects,80,81 as percent change can produce inflated or spurious fluctuations when baseline QA values are near the noise floor.82–84 No filter was applied for the directionality of results (i.e., two-tailed hypothesis test).
Statistical analysis
All statistical analyses for demographic and cognitive data were completed using StataBE 18.0. Homogeneity of variance between groups was confirmed via Levene’s test prior to each between-group comparison of continuous data, and normality was tested using Shapiro–Wilks tests. Between-group differences in demographic and injury characteristics were analyzed using Wilcoxon’s rank-sum and Pearson’s chi-squared tests for continuous and categorical variables, respectively. Wilcoxon’s rank-sum or Welch’s t-tests were used to test differences in scores on cognitive measures at baseline. For all analyses, statistical significance was thresholded at an α = 0.05. Baseline to follow-up change scores were computed for the investigation of change in performance on cognitive and self-report measures over time by subtracting baseline scores from follow-up scores. Welch’s t-tests were also used to confirm that our original findings of significant improvements in the CCR group, relative to the nonintervention control group, on the TMTA, WJUD, and CSR-C in the larger sample 42 are also present in the current subsample. Appropriate effect size estimates are provided for all between-group comparisons, and they are interpreted according to the definitions provided by Cohen. 85
Diffusion MRI connectometry
Connectometry was used to perform correlational tractography in DSI Studio 79 (“Hou” March 4, 2025, qt6 build for Mac; http://dsi-studio.labsolver.org) to investigate longitudinal changes in QA in participants who underwent CCR compared to those who did not. Given significant between-group differences in QA, relationships with improvements on TMTA, WJUD, and CSR-C were performed within each group separately using correlational tractography. For the initial between-group analysis, a rank-based multiple linear regression model was used, with the effects of mechanism of injury and premorbid intelligence (i.e., WTAR) removed. Spearman’s correlations were used for within-group correlations between QA and cognitive function, where no covariates were included to avoid overfitting the models. Correlational tractography was obtained using a deterministic fiber tracking algorithm 54 with a T-statistic threshold of 3.0, a length threshold of 20 voxels (40 mm), and 16 iterations of topology-informed pruning to remove false tracts. 86 To account for cases where the inferior cerebellar region was excluded from the field of view, a region of avoidance was applied to exclude the cerebellum at the level of Crus II and below. To estimate the FDR while preserving independence of observations at the subject level, a total of 10,000 randomized permutations were applied to the group label to obtain the null distribution of the track length, and 128,000 whole-brain seeds were placed per permutation. 60 Statistical significance of results was determined using the FDR, where an FDR < 0.05 (i.e., 5% of tracts may be false positives) is interpreted as highly confirmatory. 60 Finally, subject-level data were extracted from significant tractography results and plotted with 95% confidence intervals generated through 1,000 iterations of bootstrapping.
To identify the most affected tracts, significant correlational tractography results were segmented into individual tract clusters using DSI Studio’s built-in tract recognition function. Each cluster then underwent visual assessment and manual refinement by a neuroanatomist with expertise in white matter anatomy and tractography (H.M.L.). All bundles were carefully inspected for accuracy, with misclassified fibers reassigned to the appropriate tract cluster, and any false continuations or looping streamlines were trimmed and excluded from the final segmentation.
Results
Of the 23 participants initially included in the present subsample, two were lost to follow-up, one was excluded due to a later diagnosis of amyotrophic lateral sclerosis, one participant received the baseline and follow-up MRI scans on different scanner models, and two participants’ diffusion data did not pass the quality control procedures described above; thus, a total of 17 subjects (10 CCR, 7 control) were included in the present analysis. Participants (47% female) were between 24 and 56 (M = 42.35 ± 11.19) years of age, with 9–19 (M = 15.76 ± 2.79) years of education, and a history of most recent TBI occurring between 12 and 459 (M = 114.24 ± 135.85) months prior to participation in the study. Participants within the CCR group began training between 1 and 9 (M = 4.22 ± 2.44) days of the completing baseline assessments and returned for the follow-up assessment between 3 and 20 (M = 7.89 ± 5.84) days after completing the CCR intervention; all CCR participants completed the required 40 hours of training over the course of 9–14 (M = 11.40 ± 1.33) weeks. Demographic and injury characteristics for each group are reported in Table 1, and subject-specific characteristics are reported in Supplementary Table S2. Mechanism of injury was significantly different between the two groups (exact p = 0.014), with more motor vehicle accidents in the nonintervention control group, while falls, being hit by a motor vehicle as a pedestrian, and blunt force trauma were more common in the CCR group. No other significant group differences across demographic or clinical variables were found between the two groups. Additionally, no significant between-group differences were present in baseline scores on cognitive measures. Welch’s t-tests confirmed previous findings 42 that the CCR group improved across all cognitive measures, relative to the nonintervention control group, in the present subsample, and subject-specific percent change scores are shown in Figure 2.
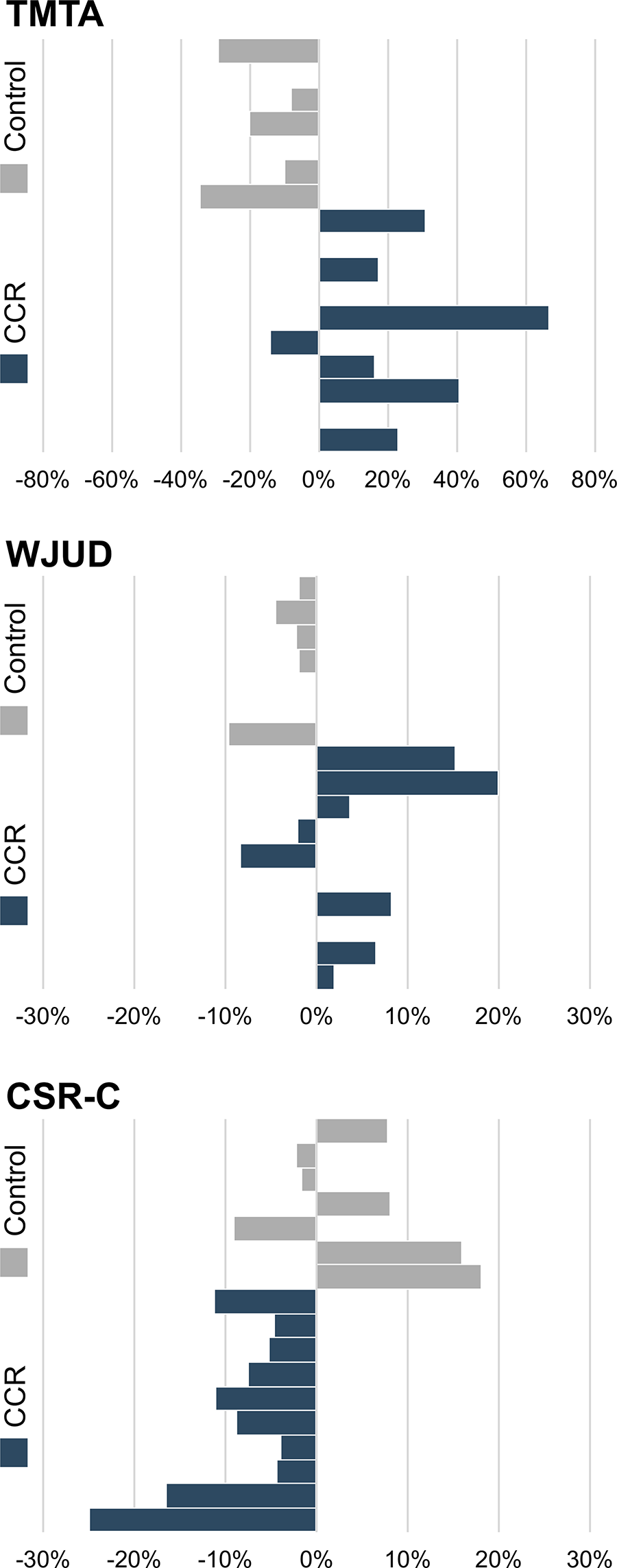
Subject-level percent change scores across cognitive measures. Percent change from baseline scores is shown for each participant. Participants in the nonintervention control group are represented by gray bars, and participants in the CCR group are represented by blue bars. Increased scores on the TMTA and WJUD indicate improved score, and decreased scores on the CSR-C indicate fewer self-reported cognitive symptoms. CCR, computerized cognitive remediation; TMTA, Trail Making Test Part A T-score; WJUD, Woodcock-Johnson III Tests of Achievement, Understanding Directions subtest raw score; CSR-C, Cognitive Self-report Questionnaire Cognitive subscale T-score.
Sample Characteristics
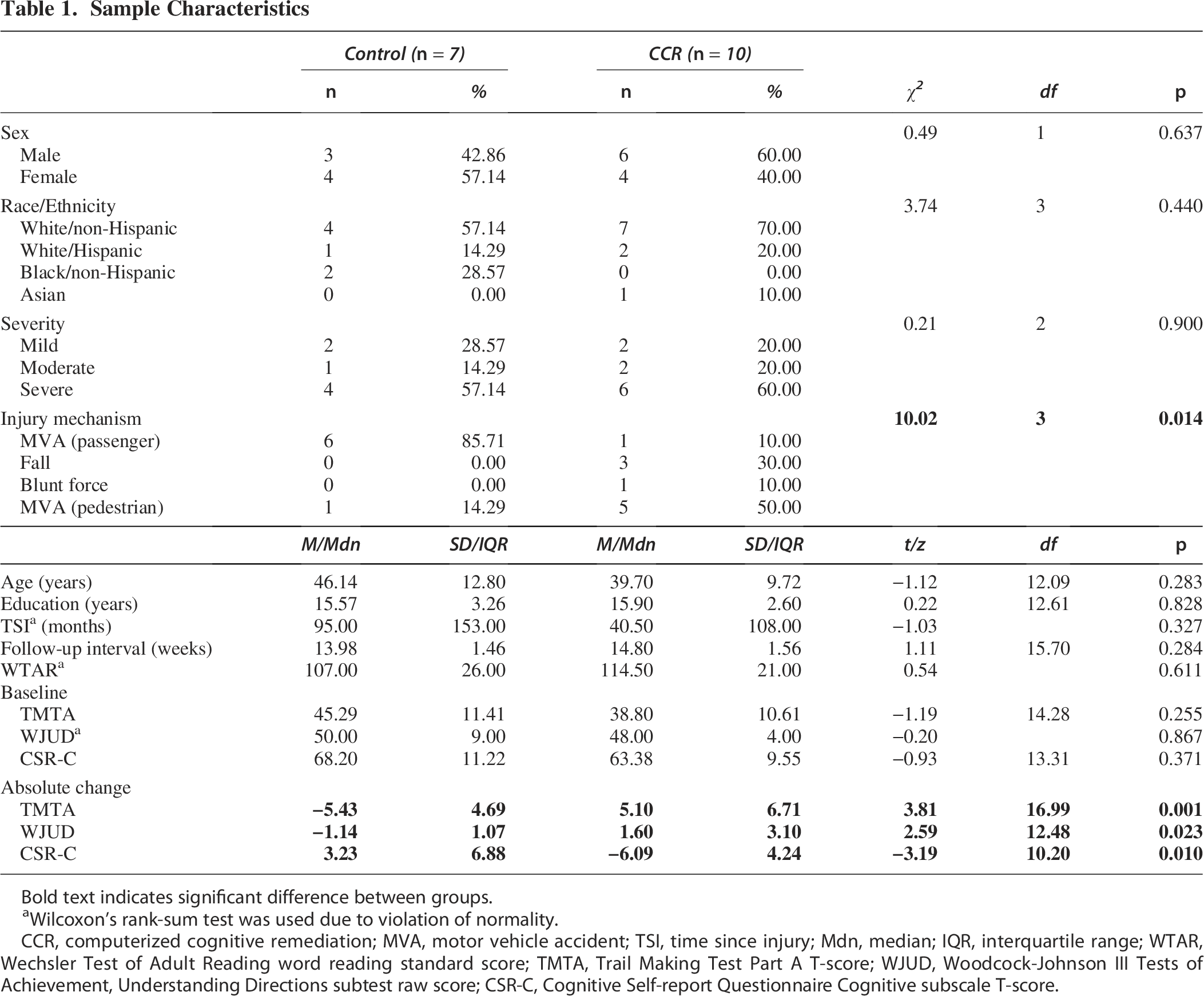
Bold text indicates significant difference between groups.
Wilcoxon’s rank-sum test was used due to violation of normality.
CCR, computerized cognitive remediation; MVA, motor vehicle accident; TSI, time since injury; Mdn, median; IQR, interquartile range; WTAR, Wechsler Test of Adult Reading word reading standard score; TMTA, Trail Making Test Part A T-score; WJUD, Woodcock-Johnson III Tests of Achievement, Understanding Directions subtest raw score; CSR-C, Cognitive Self-report Questionnaire Cognitive subscale T-score.
Correlational tractography
Group connectometry was used to correlate the change over time in local connectome matrix with group assignment (CCR vs. control) in a rank-based multiple linear regression model, while controlling for premorbid intelligence and mechanism of injury (Fig. 3). Relative to the nonintervention control group, the CCR group demonstrated significantly greater increases in QA over time, with a moderate effect size (T = 1.48, FDR = 0.000, r2 = 0.14; additional details are provided in Table 2). After trimming (0.52% of streamlines removed), approximately 90% of the affected tracts consisted of portions of the body of the corpus callosum (CC), forceps minor (FMin), left and right paracentral U-fibers, left superior longitudinal fasciculus (SLF), left arcuate fasciculus (AF), left superior thalamic radiation (STR), and left and right corticospinal tracts (CST). Group assignment was most strongly associated with increased QA in the left hemisphere U-fibers (T = 1.80), SLF (T = 1.65), and STR (T = 1.63). Details for these and all other tracts implicated in this relationship are provided in Table 3, and images of each tract cluster are provided in Figure 3c.
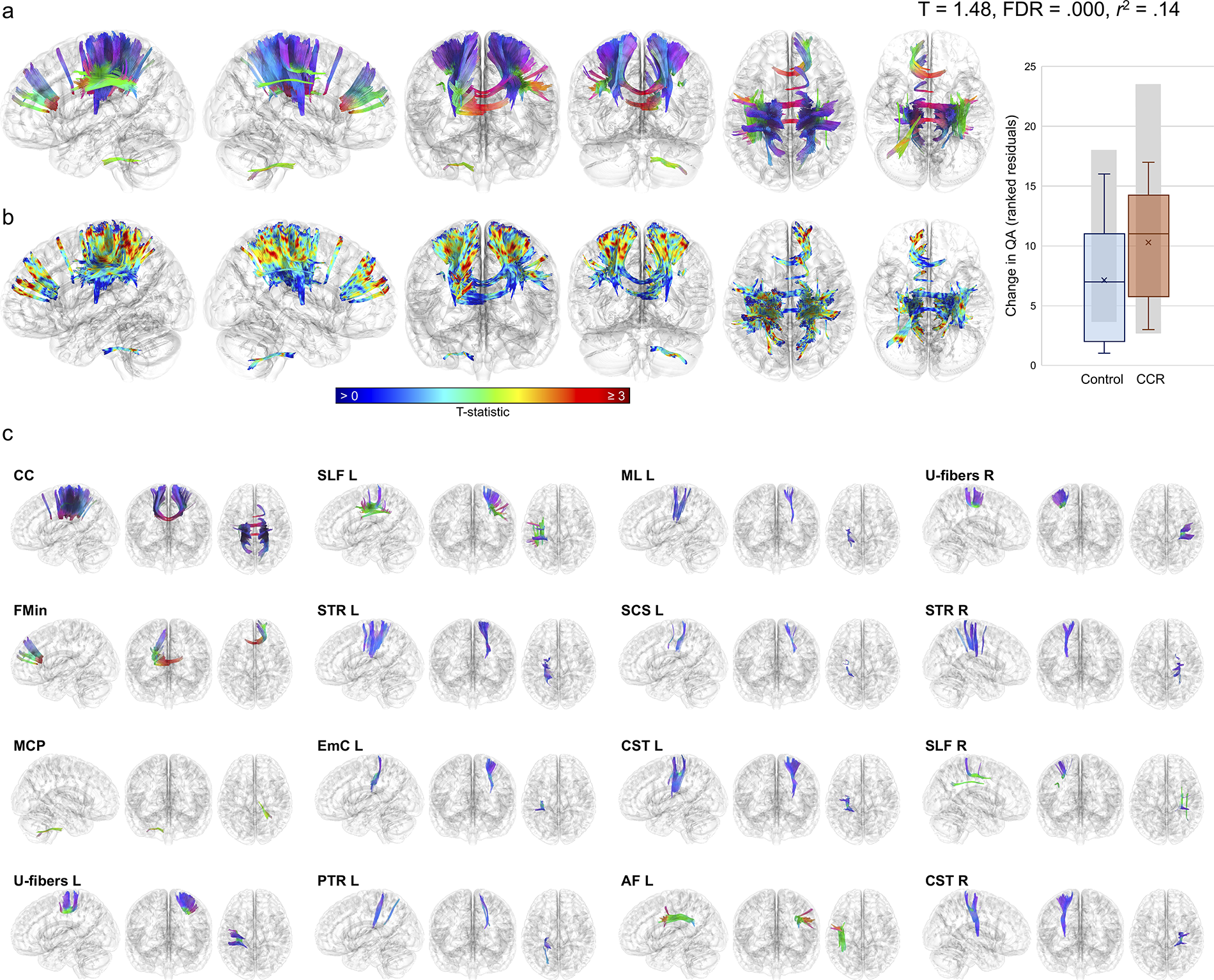
Tract segments with significantly greater increases in QA in the CCR group over time, relative to the nonintervention control group. Correlational tractography results are shown in glass surface renderings with tracts rendered using a directional color map
Overall Results of All Correlational Tractography Analyses
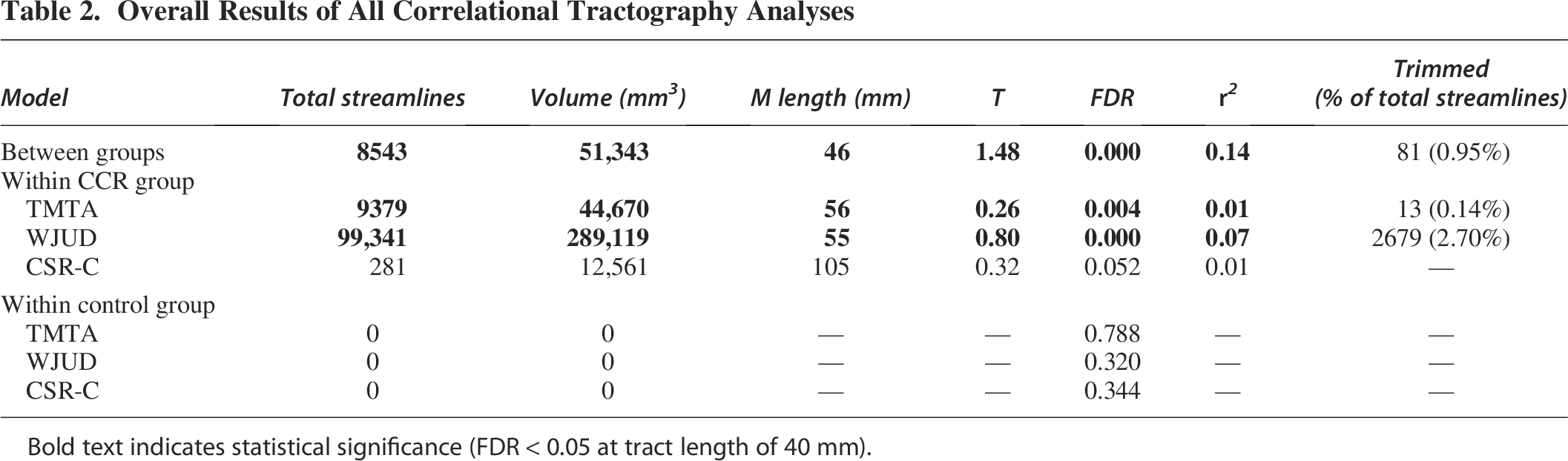
Bold text indicates statistical significance (FDR < 0.05 at tract length of 40 mm).
Tract Clusters with Significantly Increased QA in the CCR Group Relative to the Control Group
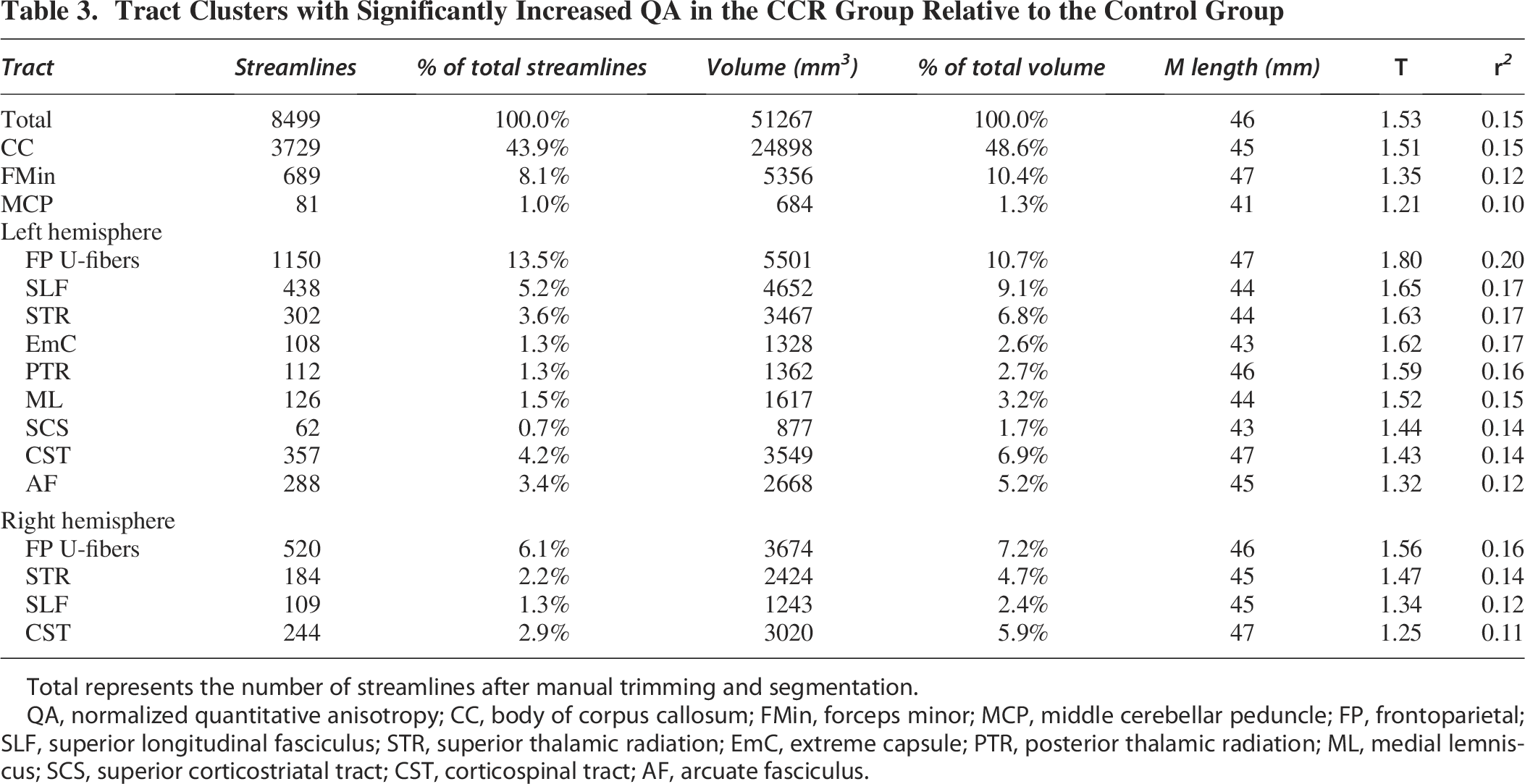
Total represents the number of streamlines after manual trimming and segmentation.
QA, normalized quantitative anisotropy; CC, body of corpus callosum; FMin, forceps minor; MCP, middle cerebellar peduncle; FP, frontoparietal; SLF, superior longitudinal fasciculus; STR, superior thalamic radiation; EmC, extreme capsule; PTR, posterior thalamic radiation; ML, medial lemniscus; SCS, superior corticostriatal tract; CST, corticospinal tract; AF, arcuate fasciculus.
Given the significant finding of increased QA in the CCR group, relative to the nonintervention control group, correlational tractography was further used to map associations between changes in QA and changes in measures of cognitive function within each group separately using Spearman’s correlations (Table 2). Within the CCR group, correlational tractography revealed a significant positive association between increased QA and improvement on TMTA (Fig. 4a), with a small effect size (T = 0.26, FDR = 0.004, r2 = 0.01). After trimming (0.14% of streamlines removed), approximately 90% of the affected tracts included the FMin, left and right inferior fronto-occipital fasciculi (IFO), and right inferior longitudinal fasciculus (ILF; details of all clusters are provided in Supplementary Table S3 and Supplementary Fig. S1). The tracts with the largest associations between increased QA and improved TMTA were the middle cerebellar peduncle (MCP; T = 0.92) and right middle longitudinal fasciculus (MdLF; T = 0.52). Increased QA was also significantly positively associated with improved WJUD score within the CCR group (Fig. 4b), with a small effect size (T = 0.80, FDR = 0.000, r2 = 0.07). After trimming (2.64% removed), portions of the forceps major (FMaj), FMin, body of CC, tapetum, left and right SLF, left AF, left and right CST, left and right IFO, left posterior thalamic radiation (PTR), and MCP made up approximately 70% of the affected tracts; all other tracts each made up < 2% of the total affected streamlines (details of all clusters are provided in Supplementary Table S4 and Supplementary Fig. S2). Improved WJUD score was most strongly associated with increased QA in the MCP (T = 1.25), left (T = 1.22) and right (T = 1.13) inferior cerebellar peduncles (ICP), and left frontal U-fibers (T = 1.14). No significant correlation was observed between increased QA and change in CSR-C score within the CCR group (Supplementary Fig. S3), and no associations were found between change in QA and change in score across the TMTA, WJUD, and CSR-C within the nonintervention control group (Supplementary Fig. S4).
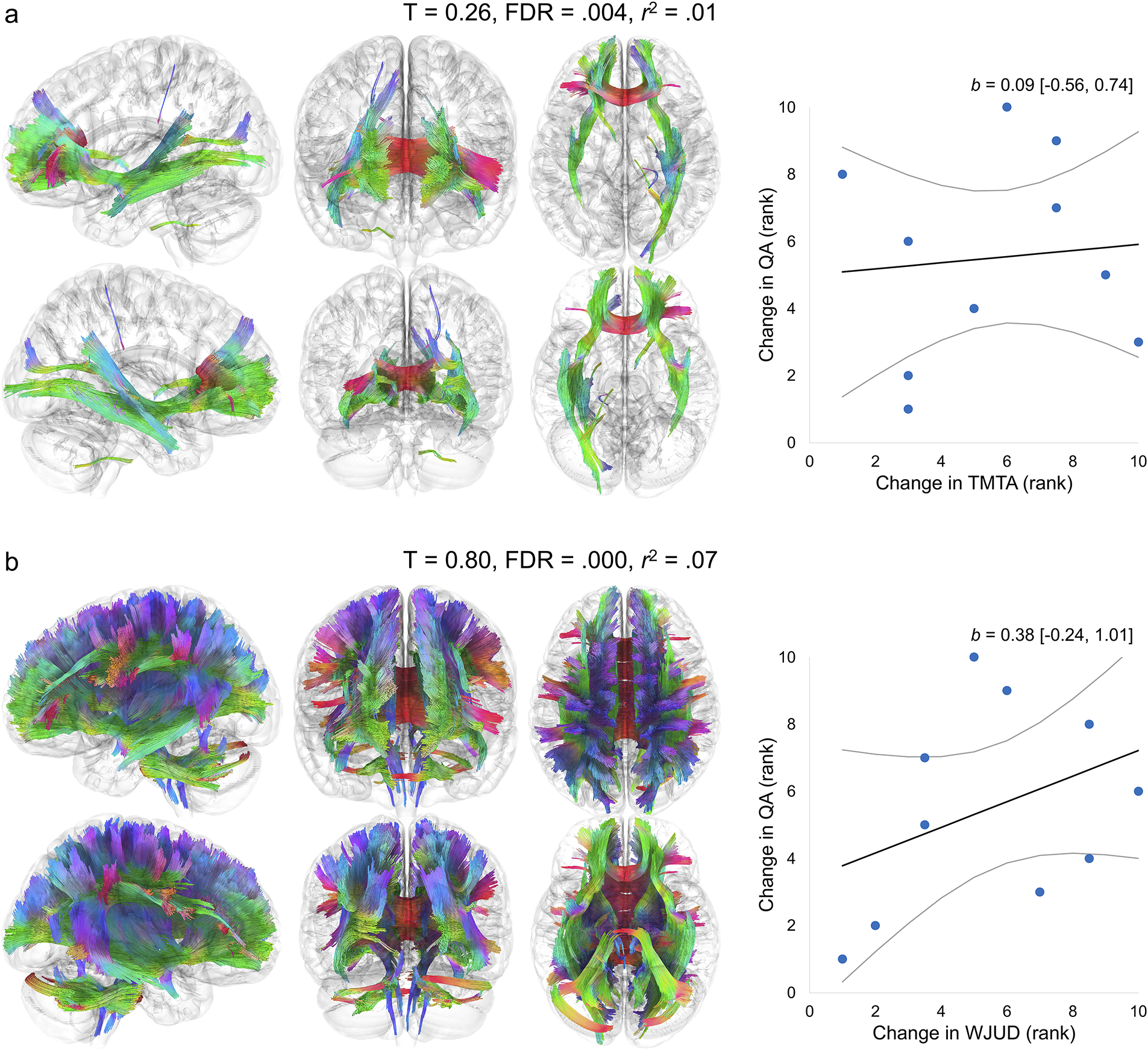
Tract segments with significant correlations between increased QA and improvement on cognitive measures within the CCR group. Correlational tractography results demonstrate significant associations between increased QA and improved TMTA T-score
Discussion
This study investigated the effects of auditory processing speed CCR on white matter plasticity in adults with chronic TBI using correlational tractography. In support of our hypothesis, we found increased QA in the CCR group, relative to nonintervention controls, suggesting that CCR may improve axonal density and promote neuroplasticity years postinjury. These findings support those of prior dMRI studies demonstrating increased FA and decreased mean diffusivity, suggesting improved white matter organization following cognitive training32,47,87 and other CCR programs88–90 in various clinical populations. Specifically, longitudinal correlational tractography revealed increased QA in the CC, MCP, bilateral SLF, CST, and STR, and left AF, medial lemniscus (ML), superior corticostriatal (CS) tracts, PTR, and extreme capsule (EmC) in those who underwent CCR relative to the nonintervention control group. Increased QA across the CC, SLF, CST, and STR suggest systemic microstructural changes in pathways commonly implicated in TAI91–95 consistent with activity-dependent myelination and synaptic strengthening that enhance neural conduction velocities and overall transmission efficiency.20,96
Together, the body of the CC and FMin accounted for 60% of the affected white matter volume. Increased QA in the CC is particularly meaningful given its role in interhemispheric functional integration, which is essential to efficient information processing.97,98 Slowed processing speed constrains higher-order cognitive processes,33,99–102 and cognitive training that targets speed of processing and attention has likewise shown both near and far transfer to episodic and working memory, executive function, fluid reasoning, and daily functioning.103–107 The BFP intervention used presently specifically targets processing speed and attention through auditory-based, millisecond-level adaptive training designed to optimize neural synchrony through Hebbian plasticity.17,108 The largest between-group differences were observed in the left hemisphere U-fibers, with bilateral U-fibers comprising 17.9% of the affected volume. These short-range association fibers, which connect adjacent gyri, support rapid local information transfer. We specifically observed increased QA in the superior fronto-parietal U-fibers connecting the hand-knob regions of the pre- and postcentral gyri, 109 which may reflect localized neuroplasticity in cortico-cortical networks that support functions known to predict recovery outcomes in neurological conditions,110,111 including sensorimotor integration, fine motor control, and precision and power grip.112–114 The integrity of fronto-parietal U-fibers has been implicated as indicators of motor and cognitive reserve following stroke 115 and as a potential target for neuromodulatory therapies in neurological populations. 116 Furthermore, U-fibers are highly sensitive to experience-dependent plasticity109,117,118 and are thought to undergo rapid myelination in response to temporally precise, repetitive co-activation, 118 which are core principles of Hebbian learning that the BFP was explicitly designed to elicit.20,91,96 We also observed increased QA in long-range projection fibers surrounding the hand-knob region, including the CST, ML, STR, PTR, and superior CS, which further suggests training-related plasticity in sensorimotor and thalamo-cortical circuits, facilitating more efficient integration of sensory input and motor output. 109 Increased QA in the SLF and EmC supports improved connectivity between frontal, temporal, and parietal regions that are essential for language comprehension, phonological processing, auditory processing, verbal attention, and working memory,119,120 while the lateralized QA increase in the left AF aligns with the auditory processing emphasis of the intervention, as the left AF is implicated in the localization of sound in space.120–122 Finally, the MCP is the primary conduit for cortical input to the cerebellum, which plays a critical role in auditory information processing. Increased QA in the MCP may therefore reflect enhanced cortico-cerebellar communication supporting auditory function, aligning with the cerebellum’s emerging role in sound recognition, phonological processing, and auditory working memory. 123 Taken together, the distributed pattern of QA increases in the CCR group offers neurobiological support for the BFP’s mechanism of action, demonstrating that repeated engagement of precise auditory discrimination tasks may drive structural remodeling in chronic TBI, potentially restoring microstructural properties of white matter pathways that support processing speed, auditory and language functions, and sensorimotor integration.
To assess functional relevance, we performed correlational tractography within each group to further investigate associations between QA changes and change in performance on cognitive measures that were shown to be improved within the CCR group in a previous study. 42 Increased QA was associated with improvements on objective measures of attention, working memory, and processing speed (TMTA, WJUD) within the CCR group; however, no associations were observed with self-reported cognitive symptoms on the CSR-C. The BFP has been shown to improve cognitive function in TBI 42 and other clinical populations,29,124 and there is growing evidence that CCR can induce functional and structural changes in the brain that are associated with these cognitive improvements. 32 The correlations observed presently between increased QA of various white matter tracts and improved attention, working memory, and processing speed provide further support for this, suggesting that CCR may positively impact the microstructural properties of white matter tracts relevant to the specific cognitive processes targeted by the intervention.
Distinct white matter correlates with TMTA and WJUD performance within the CCR group align with prior literature. Improved TMTA score was associated with increased QA of tracts previously implicated in TMTA performance, given their role in visual-motor integration and attentional control, including the CC, ILF, and IFO.125–130 TMTA improvements were also associated with increased QA in the MCP, anterior and superior CS tracts, and left ATR, consistent with literature linking these pathways to attention, timing, processing, and motor control.131–138 In contrast, more widespread white matter associations were observed with improved WJUD performance, which may reflect the task’s greater cognitive complexity and its close overlap with the neural systems targeted by the BFP. Successful performance on the WJUD requires the integration of auditory working memory, linguistic comprehension, sequential processing, and goal maintenance—functions that are subserved by a distributed network of frontotemporal, frontoparietal, temporoparietal, subcortical, and cerebellar pathways, including the CC, AF, SLF, IFO, EmC, MdLF, frontal aslant tracts (FAT), cingulum bundles (CB), uncinate fasciculi (UF), thalamic radiations, MCP, and ICP.120,122 Improved WJUD performance within the CCR group was associated with increased QA across these and other pathways (see Supplementary Table S3), with the strongest associations occurring with the MCP and bilateral ICPs. The cerebellum plays a role in various functions required for successful WJUD performance, including sound recognition and processing,139,140 phonological storage,141,142 sequential learning, 143 and auditory working memory,144,145 and the cerebellar peduncles serve as the primary afferent pathways for auditory information passing into it.123,146 To our knowledge, no prior studies have directly examined the effects of CCR on cortico-cerebellar connectivity, making these findings, along with the between-group differences demonstrating increased QA of the MCP in the CCR group, especially noteworthy, as they implicate the cerebellum as a potentially critical, yet underexplored, locus of cognitive training-induced structural changes and suggest that cerebellar circuits may represent a promising target for future interventions. Lastly, improved WJUD performance in the CCR group was associated with increased QA in short-range paracentral (right), parietal (bilateral), and frontal (left) U-fibers. As previously mentioned, superior fronto-parietal (paracentral) U-fibers play a role in sensorimotor integration, fine motor control, and precision and power grip.112–114 Direct investigations of the functional correlates of parietal U-fibers spanning the intraparietal sulcus is limited; however, the superior and inferior parietal gyri may play roles in verbal working memory and auditory spatial attention,147–150 and the intraparietal sulcus has been implicated in auditory perceptual organization.151,152 Finally, our observations of increased QA in left frontal U-fibers connecting the middle and inferior (operculum) frontal gyri and spanning the inferior frontal sulcus suggest plasticity in short-range pathways connecting critical regions for language processing, speech production, and verbal working memory. 109
Overall, the brain-behavior findings are consistent with the concept of near transfer, wherein training effects generalize most strongly with tasks that share cognitive demands and neural substrates with the intervention. This is demonstrated by the widespread white matter associations observed between QA increases and WJUD performance within the CCR group, which closely align with the core neural targets of the BFP intervention. The shared emphasis on verbal working memory and auditory processing likely contributed to QA increases across auditory and language-related pathways, such as the AF, SLF, CB, EmC, FAT, MdLF, and UF. 120 In contrast, TMTA measures more distally related functions, which may account for its more circumscribed white matter associations. However, the observed QA increases in tracts supporting these broader functions, including the FMaj, IFO, ILF, and CS pathways, raise the possibility of far transfer effects, whereby improvements in core cognitive capacities like processing speed extend to support untrained cognitive domains. 153 Together, these findings reinforce established evidence that cognitive training is most effective when engaging overlapping neural circuits, 153 while also suggesting that BFP may promote system-wide improvements that generalize beyond the speed of processing.103,139–145
Notably, no significant associations were observed between changes in QA and cognitive performance in the nonintervention control group, likely reflecting the absence of targeted stimulation to drive neuroplasticity. In chronic TBI, white matter integrity tends to remain stable or decline in the absence of intervention,154–156 and any minor fluctuations in performance are not likely to correspond to meaningful structural remodeling. These findings reinforce the specificity of the observed brain-behavior relationships in the CCR group and suggest that cognitive improvements following CCR are supported by targeted white matter plasticity, rather than nonspecific or spontaneous changes over time. The overall findings of this study are particularly notable given the chronic stage of injury in our sample, where neuroplasticity is often diminished due to ongoing maladaptive processes, such as disrupted neuromodulation and increased neurological noise.157,158 The region-specific QA increases following CCR, particularly in frontal, temporal, callosal, short-range, and cerebellar pathways, suggests that targeted cognitive interventions may partially reverse or mitigate maladaptive microstructural changes in chronic TBI. Moreover, these findings build upon those of prior studies by providing additional evidence of neuroplastic changes, complementing tensor-derived metrics that are less specific in characterizing underlying microstructural alterations. Through correlational tractography, we were further able to demonstrate region-specific changes in QA along affected tracts, supporting the sensitivity of connectometry-based approaches for detecting subtle microstructural changes and anatomical variability in the presence of neuronal injury and recovery. 76
Limitations and future directions
Despite these promising findings, several limitations should be considered when interpreting the results of the present study. First, the small and unequal sample sizes between the CCR and nonintervention control groups, along with the absence of a healthy control group, limit the generalizability of the findings and increase the risk of both Type I and Type II error, particularly in subgroup analyses. Although our use of advanced connectometry techniques improved sensitivity to subtle and regionally specific white matter changes, this approach remains observational in nature and cannot establish causal relationships between CCR, structural changes, and cognitive improvements. Additionally, the use of a single-shell diffusion scheme constrained the accuracy of QA estimates and precluded examination of free and restricted diffusion compartments and more advanced diffusion models, such as neurite orientation dispersion and density imaging (NODDI), which may provide further insight into axonal, dendritic, and glial contributions to the observed microstructural changes.
Furthermore, while increases in QA were associated with improvements on objective measures of attention, working memory, and processing speed, no significant relationship was observed between QA changes and self-reported cognitive symptoms. This discrepancy suggests that subjective symptom reporting may be influenced by other factors, such as mood, metacognitive awareness, or other psychosocial variables, which were not directly assessed in the present study. Notably, these domains have previously been shown to improve following CCR in individuals with mild TBI,35,36,41,159 indicating that CCR may impact self-perceptions of cognitive function through mechanisms not captured by QA alone. Supporting this, resting-state fMRI research 160 suggests that brain regions associated with improved confidence in one’s cognitive abilities overlap with those we previously observed to increase in functional connectivity following CCR in this same sample. 43 Future studies incorporating broader assessments of functional, affective, and quality-of-life outcomes will be important to more comprehensively characterize the clinical significance of CCR-induced neural changes and to clarify the pathways through which CCR may influence both objective and subjective cognitive outcomes. Finally, longitudinal designs incorporating multiple imaging and assessment time points will also be essential to determine the time course and durability of CCR-induced neuroplastic changes, as the present study only examined outcomes at 2 weeks posttraining.
While these limitations warrant consideration, the present findings implicate the potential of CCR as a low-risk, scalable intervention to promote neuroplasticity and cognitive recovery in individuals with chronic TBI. Given the observed associations between microstructural white matter changes and objective cognitive improvements, CCR may be particularly valuable as an adjunct to traditional rehabilitation approaches, supporting long-term maintenance of cognitive functioning in this population. Future larger-scale randomized controlled trials are warranted to confirm these findings and explore the durability of CCR-induced neuronal and cognitive changes over extended follow-up periods. Additionally, integration of multimodal imaging techniques, including functional connectivity, NODDI, and neurometabolic measures, may provide a more comprehensive understanding of the mechanisms underlying CCR efficacy and inform the development of personalized rehabilitation protocols targeting specific neural systems affected by TBI.
Conclusion
The present findings offer preliminary evidence that an auditory information processing CCR may induce microstructural white matter changes in adults with chronic TBI. Furthermore, these observed changes are associated with improvements in attention, working memory, and processing speed, suggesting that CCR may facilitate neuroplasticity at both functional and structural levels many years postinjury. Together, these findings implicate CCR as a scalable intervention to engage mechanisms of cognitive recovery and neural plasticity in individuals with chronic TBI and underscore the importance of incorporating sensitive neuroimaging biomarkers, such as QA and diffusion connectometry, in future intervention studies.
Transparency, Rigor, and Reproducibility Statement
The study was retrospectively registered at clinicaltrials.gov (NCT02507271), without formal preregistration of the analysis plan. A sample size of 70 was planned, and 64 participants were enrolled. The imaging component of the study was optional, and imaging data were only collected from 23 participants. Of these, one participant in the nonintervention control group was lost to follow-up, and two participants in the nonintervention control group and one participant in the intervention group were excluded due to excessive head motion, later diagnosis of amyotrophic lateral sclerosis, and pre- and postimaging occurring on different scanner models, respectively. Additionally, one subject from each group was later excluded due to failure to pass quality control criteria applied to diffusion imaging data. Participants were not told the results of their cognitive evaluations but were provided with a clinical report of their MRI from a licensed medical doctor with a specialty in radiology. Imaging quality control decisions and analyses were performed by investigators who were aware of relevant characteristics of the participants. All cognitive data were collected with standardized clinical neuropsychological measures. The equipment and software used to perform imaging and preprocessing are widely available from FSL (http://fsl.fmrib.ox.ac.uk/) and DSI Studio (http://dsi-studio.labsolver.org/). The inclusion criteria and outcome evaluations are established standards. No replication studies have been planned at this time. De-identified data from this study will be made available upon request by emailing the corresponding author as of June 3, 2025. The analytic code used to conduct the analyses presented in this study is not available in a public repository, but it will be made available upon request by emailing the lead author. The authors agree to provide the full content of the article on request by contacting the corresponding author.
Authors’ Contributions
H.M.L.: Data curation, formal analysis, investigation, methodology, software, validation, visualization, writing—original draft, and writing—review and editing. J.F.R.: Conceptualization, methodology and writing—review and editing. T.B.: Conceptualization, methodology, and writing—review and editing. S.F.: Conceptualization, resources, and writing—review and editing. M.L.: Data curation, software, and writing—review and editing. G.T.V.: Conceptualization, funding acquisition, investigation, methodology, project administration, supervision, writing—original draft, and writing—review and editing.
Footnotes
Acknowledgments
The authors recognize and greatly appreciate Giulia Mercuri’s contribution to data collection.
Author Disclosure Statement
The authors declare no financial disclosures or potential conflicts of interest regarding the research, authorship, and/or publication of this article.
Funding Information
This study was supported by the New York University Research Challenge Fund (R8740).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.