
Abstract
Anxiety and depression are associated with high symptom burden, functional limitations, and poor quality-of-life. Understanding the prevalence and risk factors for mental health symptoms after concussion is essential for early identification and targeted treatment. The objective of this study was to estimate the prevalence and risk factors associated with moderate-to-severe anxiety (msANX) symptoms and depression (msDEP) symptoms after concussion. This prospective observational study recruited participants from three specialty concussion clinics within the TRANSCENDENT Concussion Research Program. Adolescents and adults aged 13 years and older diagnosed with a physician-confirmed concussion who presented for routine care within a learning health system were eligible if they completed mental health measures at intake assessment between April 2024 and July 2025. Primary outcomes were msANX (Generalized Anxiety Disorder-7 [GAD-7] ≥10) and msDEP (Patient Health Questionnaire-9 [PHQ-9] ≥10) symptoms at intake assessment. Multivariable logistic regression assessed the association between symptoms and patient-related and injury-related factors. Models were adjusted for known predictors. Of 1,639 participants (n = 1,051 [64%] female; median [interquartile range, IQR] age, 28 [17–45] years; median [IQR], 21 [12, 42] days since injury), 45.2% (95% confidence intervals, CI, 42.8–47.7) had msANX (median [IQR] score, (15 [12–18]) and 60.7% (95% CI, 58.3–63.0) had msDEP (median [IQR] score, (16 [12–19]). Risk factors included injury setting (motor vehicle collision [msANX: OR, 3.68; 95% CI: 2.56–5.30; p < 0.001; msDEP: OR, 3.15; 95% CI: 2.11–4.74; p < 0.001], workplace [msANX: OR, 2.85; 95% CI: 1.90–4.30; p < 0.001; msDEP: OR, 2.73; 95% CI: 1.74–4.35; p < 0.001], and assault [msANX: OR, 2.24; 95% CI: 1.07–4.82; p = 0.03] compared with playing sports, having preinjury anxiety (msANX: OR, 1.97; 95% CI, 1.41–2.75; p < 0.001; msDEP: OR, 1.87; 95% CI: 1.31–2.70; p < 0.001), sleep difficulties (msANX: OR, 1.44; 95% CI: 1.36–1.52; p < 0.001; msDEP: OR, 1.62; 95% CI: 1.53–1.73; p < 0.001), being female (msANX: OR, 1.38; 95% CI: 1.08–1.77; p = 0.01; msDEP: OR, 1.34; 95% CI: 1.04–1.72; p = 0.03), and time since injury (msANX: OR, 1.16; 95% CI: 1.07–1.26; p < 0.001; msDEP: OR,1.10; 95% CI: 1.01–1.20; p = 0.03). Leveraging data collected during routine care, this study suggests that existing prevalence estimates likely underestimate the high levels of anxiety and depression symptoms at specialty clinic intake that warrant active treatment. Clinicians should routinely screen for mental health conditions and prioritize higher-risk patients for closer monitoring, including those injured in a motor vehicle collision or at work, female patients, and those with preinjury anxiety or postinjury sleep difficulties. Timely referral to mental health professionals is needed to prevent chronic mental health problems and optimize recovery.
Introduction
A total of 1 in 10 people in Ontario, Canada, reported experiencing a concussion between 2008 and 2016, with prevalence rates increasing across Canada and the United States during that time.1,2 Growing evidence shows that anxiety and depression symptoms are more common several months after concussion than in the general population or after orthopedic injury.3–6 Those with anxiety and depression are more likely to experience prolonged symptom recovery and functional limitations and take longer to return-to-sport after concussion.7–10
Existing prognostic models show that preinjury patient and injury characteristics are linked with adverse mental health outcomes months to years following traumatic brain injury in adults.11–13 These studies have predominantly recruited adults from the emergency department with all severities of traumatic brain injury, some with structural injury on CT imaging or who had been hospitalized, and excluded patients with preexisting neurological disorders. What’s unknown is how often anxiety and depression symptoms are severe enough in adolescents and adults to recommend active treatment early after concussion and whether the prevalence differs based on similar factors. Understanding how many patients meet clinical threshold for anxiety and depression symptoms and who is most at risk before symptoms become chronic is essential for precision healthcare to support timely referrals to mental health specialists, optimize treatment, and improve patient outcomes.
Therefore, the primary objective of this study was to estimate the prevalence of moderate-to-severe anxiety (msANX) symptoms and depression (msDEP) symptoms at intake assessment in a specialty concussion clinic. The secondary objective was to identify risk factors across age, sex, injury setting/mechanism, and preinjury mental health conditions.
Methods
Design and setting
This multicenter observational study was a planned analysis of data collected in the prospective TRANSCENDENT Concussion Research Program 14 based on priorities identified through patient and public involvement 15 to determine the prevalence of anxiety and depression symptoms after concussion. Participants were recruited from three specialty concussion care clinic in three major cities in Ontario, Canada (Ottawa, Toronto, and Mississauga), between April 1, 2024, and July 17, 2025. 16 360 Concussion Care clinics are designed as a learning health system, whereby data are generated from routine care to advance knowledge and applied back into practice to improve outcomes.17,18 Patients are primarily referred from emergency departments or community physicians. Patients with lived experience and the public actively participate on a Community Advisory Committee to inform study design, conduct, and knowledge translation activities. The study was approved by the Children’s Hospital of Eastern Ontario Research Ethics Board and adheres to the Strengthening the Reporting of Observational Studies in Epidemiology reporting guideline. 19
Study population
We screened consecutive adolescent and adult (13 years and older) patients who presented for a concussion intake assessment at a participating clinic. Patients were eligible if they received a physician-confirmed diagnosis of concussion (definite, probable, and possible) within one year since injury. In the rare event that a physician deemed the patient to not have sustained a concussion (unlikely, none), they were considered eligible if they met American Congress of Rehabilitation Medicine (ACRM) diagnostic criteria for a definite or suspected mild traumatic brain injury (Supplementary Box S1). 20 Patients were ineligible if they were unable to provide consent or assent in English, French, or via a translator.
Study protocol
The TRANSCENDENT protocol has been previously published. 14 Briefly, participants completed online surveys using standardized intake questionnaires embedded within the Electronic Health Record (Telus CHR) and Research Electronic Data Capture (REDCap; Vanderbilt University) 16 prior to and during their in-person intake assessment with a physician. Participants provided information on demographics, injury setting/mechanism, and self-reported preinjury mental health diagnoses or treatment. All participants provided written consent or assent as appropriate via a REDCap 16 e-consent form as a pre-visit link or in-person discussion.
Outcomes and measures
We used freely accessible standardized anxiety and depression screening tools based on recommended concussion-specific common data elements21,22 and administered them in-person at the intake assessment.
Anxiety
We measured anxiety symptoms using the seven-item Generalized Anxiety Disorder-7 (GAD-7) screening and severity tool that demonstrates strong criterion and construct validity in both the general population and in those with concussion (Supplementary Table S1).23,24 Participants rated how often they have been bothered by symptoms over the previous two weeks, or if their injury is more recent since then, on a four-point Likert scale from 0 (not at all) to 3 (nearly every day). Higher GAD-7 scores (range 0–21) indicate higher anxiety symptoms. A score of 10 or greater is a common clinical threshold that indicates an anxiety disorder that requires further assessment by a mental health professional.23,24
Depression
We measured depression symptoms using the nine-item Patient Health Questionnaire-9 (PHQ-9) screening and severity tool which has strong diagnostic accuracy for depression in the general population and in those with concussion (Supplementary Table S1).24–26 Participants rated how often they have been bothered by symptoms over the previous two weeks, or if their injury is more recent since then, on a four-point Likert scale from 0 (not at all) to 3 (nearly every day). Higher PHQ-9 scores (range 0–27) indicate higher depression symptoms. A score of 10 or greater is a common clinical threshold that is consistent with a major depressive episode that requires further assessment by a mental health professional.24,25
Statistical analysis
We summarized participant characteristics and GAD-7 and PHQ-9 scores using medians and interquartile ranges (IQRs) for continuous variables and frequencies and percentages for categorical variables. To categorize participants as having msANX or msDEP, we used a cut-off score of ≥10 since further clinical evaluation of symptoms is typically recommended at or above a score of 10.23,25 All analyses were done using complete cases.
We estimated the overall prevalence of msANX and msDEP using Wilson 95% CIs and also stratified by sex (male, female), age category (13.00–17.99, 18.00–29.99, 30.00–59.99, >60.00 years), injury setting/mechanism (assault, fall, motor vehicle collision [MVC], workplace injury, playing sports), and preinjury mental health conditions.
We assessed factors associated with the odds of reporting msANX and msDEP using multivariable logistic regression models based on prognostically important clinical risk factors:27–29 age, sex (male as the reference), time since injury, injury setting/mechanism (playing sports as the reference), postinjury sleep difficulties (yes, no), preinjury depression diagnosis or treatment(yes, no), preinjury anxiety diagnosis or treatment (yes, no), prior concussion (yes, no), and physician-diagnosed concussion (definite, probable, possible). To allow for nonlinearity in continuous variables (age and time from injury) within the regression model, we used restricted cubic splines using three knots placed at fixed 10th, 50th, and 90th percentiles. Statistical significance was set at p < 0.05. We performed all analyses using R Project for Statistical Computing (R version 4.4.1; 2024-06-14). 30
Results
Participant characteristics
The analytic sample included 1,639 participants (n = 1,051 [64%] female; median [IQR] age, 28 [17, 45] years) who completed the GAD-7 and PHQ-9 a median (IQR) of 21 (12, 42) days since injury (Fig. 1). Participants reported most frequently being injured during sports (n = 546; 34%), MVC (n = 322; 20%), or falls (n = 301; 18%). The most commonly reported preinjury mental health or behavioral conditions included anxiety (n = 551; 34%), depression (n = 320; 20%), and attention deficit/hyperactivity disorder (n = 275; 17%). Table 1 summarizes participant characteristics, injury setting/mechanism, and preinjury mental health conditions stratified by age.
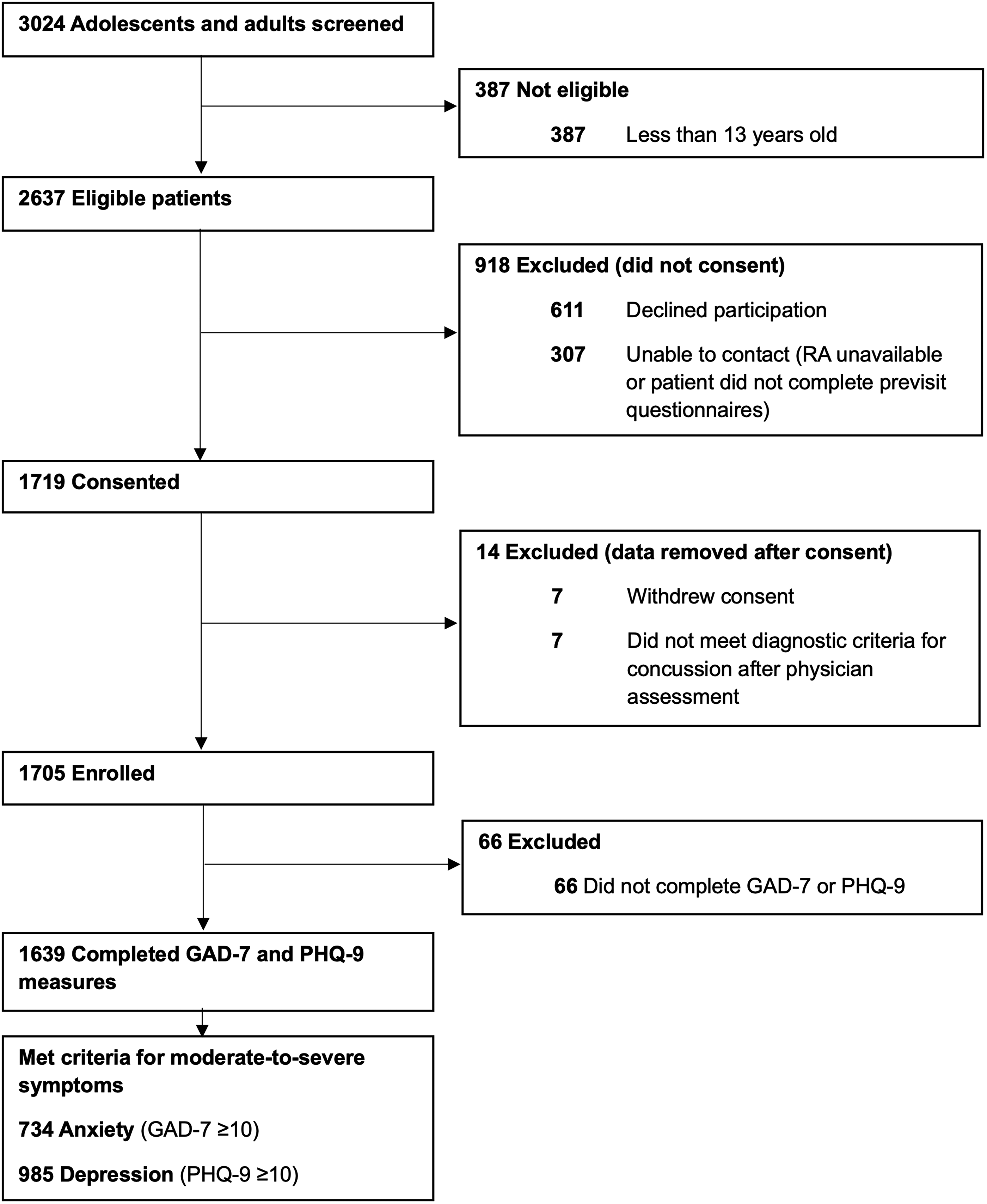
Flow Diagram of Participants with Post-Concussion Anxiety and Depression. aParticipants could have screened positive for both anxiety and depression.
Participant Characteristics at Initial Assessment
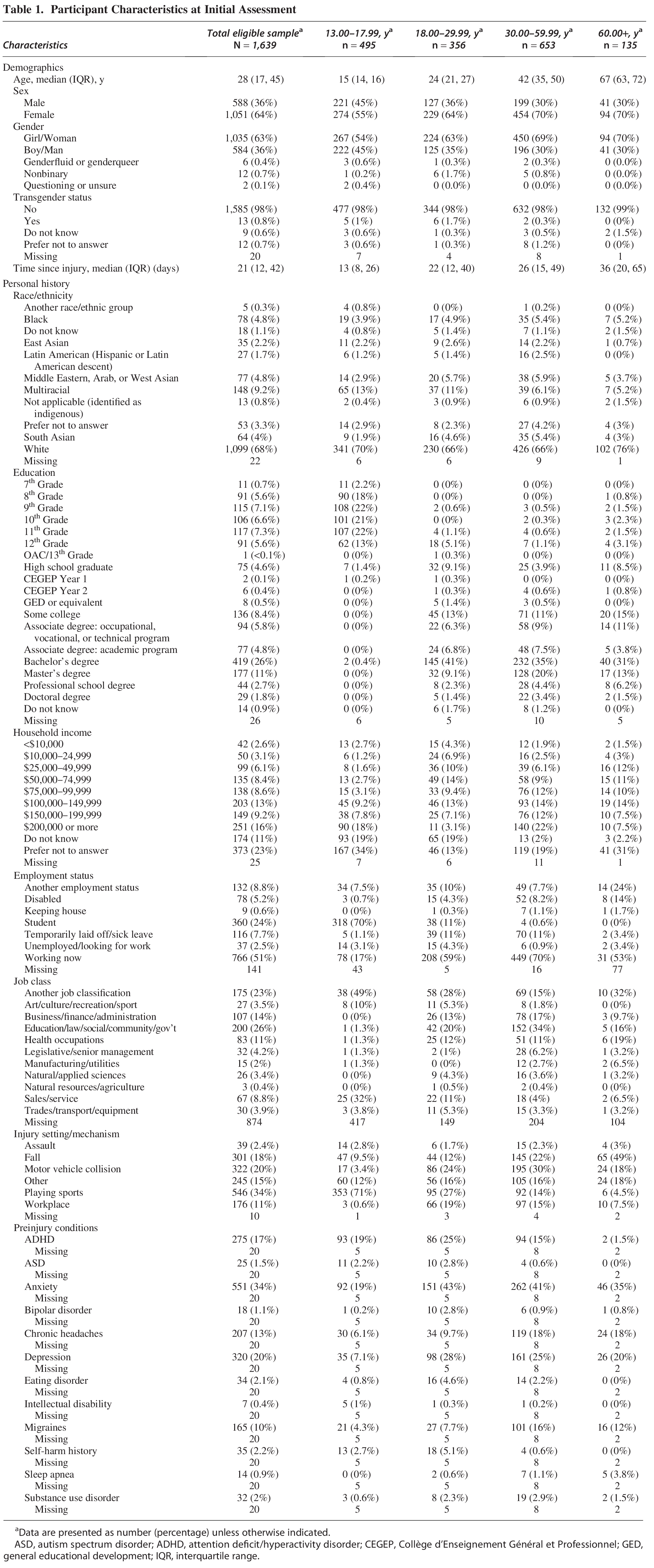
Data are presented as number (percentage) unless otherwise indicated.
ASD, autism spectrum disorder; ADHD, attention deficit/hyperactivity disorder; CEGEP, Collège d’Enseignement Général et Professionnel; GED, general educational development; IQR, interquartile range.
Prevalence of msANX and msDEP symptoms
Preinjury, 34% (551/1,639) of participants reported being diagnosed or treated for anxiety, and 20% (320/1,639) reported a diagnosis or treatment of depression (Table 1). After concussion, 45.2% (95% CI: 42.8–47.7; 734/1,623) of participants scored above the cut-off for msANX (15 [12–18]) on the GAD-7, and 60.7% (95% CI: 58.3–63.0; 985/1,623) of participants scored above the cut-off for msDEP (16 [12–19]) on the PHQ-9. A total of 42.0% (95% CI: 39.6–44.4; 681/1,623) reported co-occurring msANX and msDEP.
msANX and msDEP were more common in females than males. For anxiety, 49.4% of females (95% CI: 46.4–52.4; 519/1,051) versus 36.6% of males (95% CI: 32.8–40.5; 215/588). For depression, 64.6% of females (95% CI: 61.7–67.4; 679/1,051) versus 52.0% of males (95% CI: 48.0–56.1; 306/588).
Adults reported msANX and msDEP more often than adolescents and older adults. For anxiety, 55.1% (95% CI: 49.9–60.1; 196/356) of 18.00–29.99-year-olds and 52.5% (95% CI: 48.7–56.3; 343/653) of 30.00–59.99-year-olds compared to 27.5% (95% CI: 23.7–31.6; 136/395) of 13.00–17.99-year-olds and 43.7% (95% CI: 35.6–52.1; 59/135) of adults over 60.00 years of age. For depression, 71.1% (95% CI: 66.2–75.5; 253/356) of 18.00–29.99-year-olds and 68.8% (95% CI: 65.1–72.2; 49/653) of 30.00–59.99-year-olds compared to 42% (95% CI: 37.7–46.4; 208/495) of 13.00–17.99-year-olds and 55.6% (95% CI: 47.1–63.7; 75/135) of adults over 60.00 years of age.
msANX were more common in those injured in an MVC (69.9%; 95% CI: 64.7–74.6; 225/322), at work (59.1%; 95% CI: 51.7–66.1; 104/176), or by assault (56.4%; 95% CI: 41.0–70.7; 22/39) versus playing sports (26.9%; 95% CI: 23.4–30.8; 147/546). msDEP showed a similar pattern: MVC (81.1%; 95% CI: 76.4–85.0; 261/322), work (75%; 95% CI: 68.1–80.8; 132/176), or assault (69.2%; 95% CI: 53.6–81.4; 27/39) versus playing sports (42.7%; 95% CI: 38.6–46.9; 233/546).
Among participants with preinjury conditions, msANX were most common in those with bipolar disorder (77.8%; 95% CI: 54.8–91.0; 14/18), eating disorders (73.5%; 95% CI: 56.9–85.4; 25/34), and self-harm history (71.4%; 95% CI: 54.9–83.7; 25/35), as well as those with preinjury anxiety (59.7%; 95% CI: 55.6–63.7; 329/551) and depression (64.7%; 95% CI: 59.3–69.7; 207/320). msDEP were highest among those with self-harm history (88.6%; 95% CI: 74.0–95.5; 31/35), autism (88%; 95% CI: 70.0–95.8; 22/25), and substance use disorder (87.5%; 95% CI: 71.9–95.0; 28/32), as well as preinjury anxiety (74.2%; 95% CI: 70.4–77.7; 409/551) and depression (79.7%; 95% CI: 74.9–83.7; 255/320) (Table 2).
Prevalence of Moderate-to-Severe Anxietya and Depressionb After Concussion, Stratified by Demographics, Injury Setting/Mechanism, and Preinjury Conditions
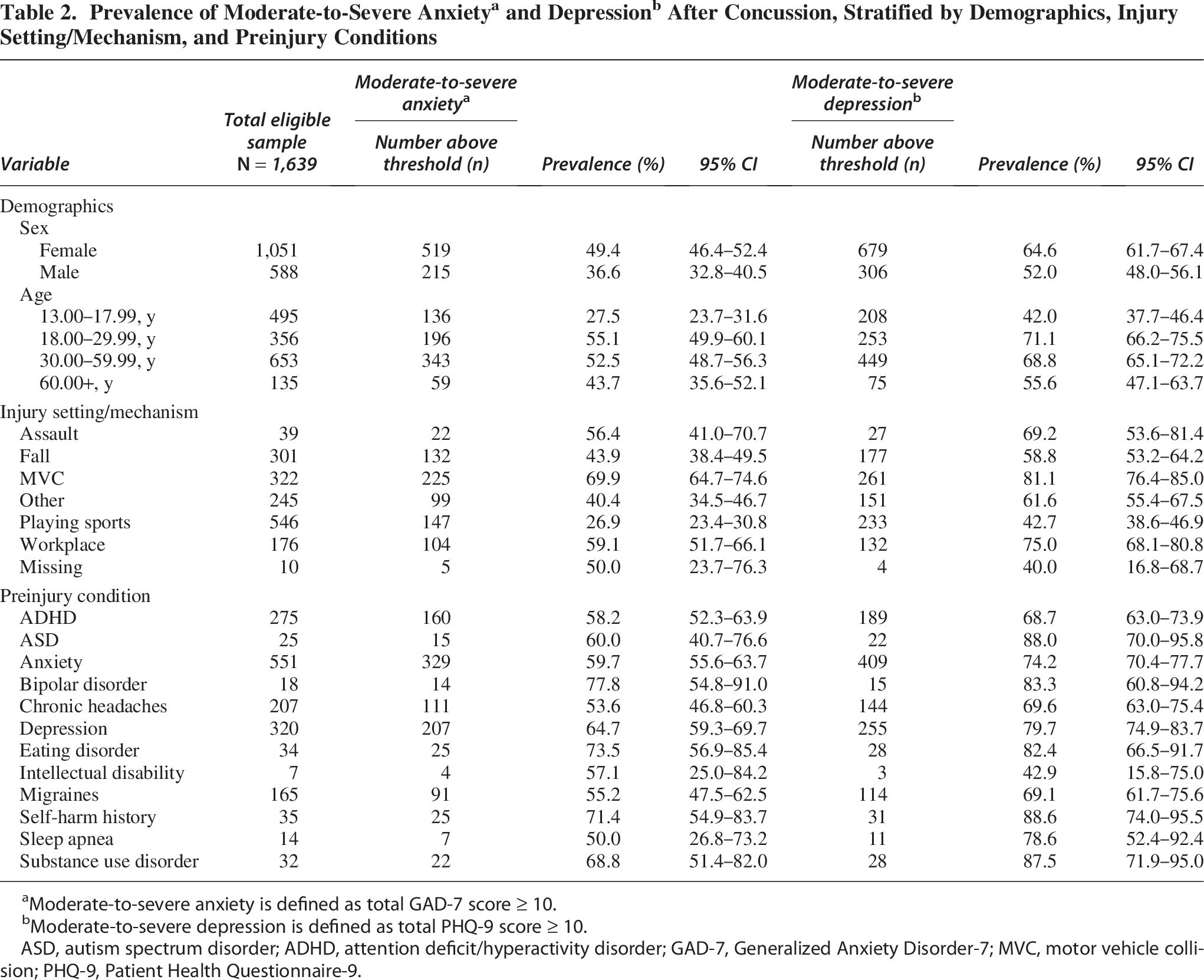
Moderate-to-severe anxiety is defined as total GAD-7 score ≥ 10.
Moderate-to-severe depression is defined as total PHQ-9 score ≥ 10.
ASD, autism spectrum disorder; ADHD, attention deficit/hyperactivity disorder; GAD-7, Generalized Anxiety Disorder-7; MVC, motor vehicle collision; PHQ-9, Patient Health Questionnaire-9.
Associations of msANX and msDEP symptoms with demographics, injury setting/mechanism, and preinjury condition
Adjusted models (Table 3) showed that females were more likely to have msANX (OR, 1.38; 95% CI: 1.08–1.77; p = 0.01) and msDEP (OR, 1.34; 95% CI: 1.04–1.72; p = 0.03) than males.
Adjusted Odds of Moderate-to-Severe Anxietya and Depressionb After Concussion (N = 1,623)
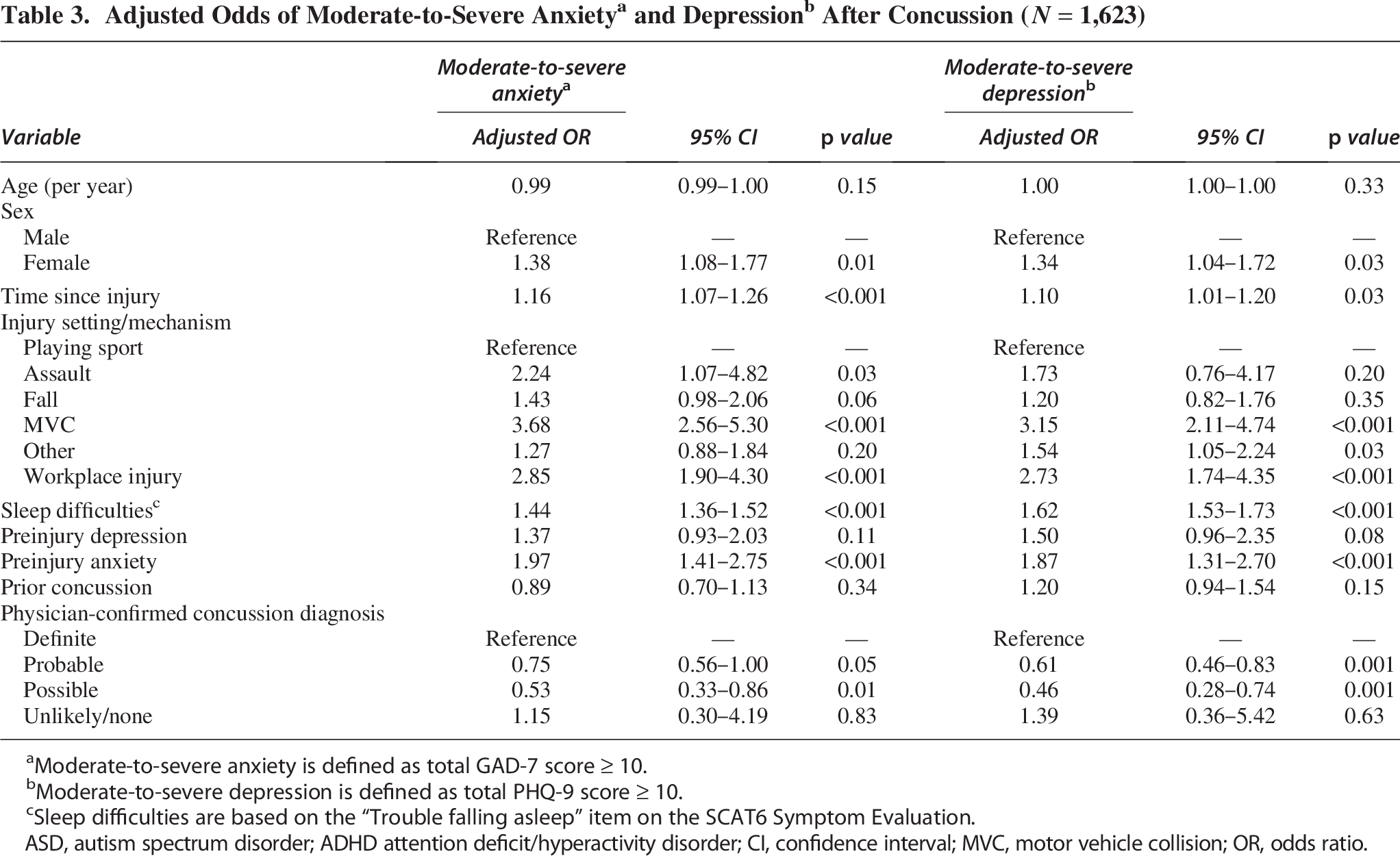
Moderate-to-severe anxiety is defined as total GAD-7 score ≥ 10.
Moderate-to-severe depression is defined as total PHQ-9 score ≥ 10.
Sleep difficulties are based on the “Trouble falling asleep” item on the SCAT6 Symptom Evaluation.
ASD, autism spectrum disorder; ADHD attention deficit/hyperactivity disorder; CI, confidence interval; MVC, motor vehicle collision; OR, odds ratio.
Injury setting/mechanism was a strong risk factor. Compared with playing sports, odds of msANX were higher for MVC (OR, 3.68; 95% CI: 2.56–5.30; p < 0.001), workplace injury (OR, 2.85; 95% CI: 1.90–4.303; p < 0.001), or assault (OR, 2.24; 95% CI: 1.07–4.82; p = 0.03). msDEP risk showed a similar pattern for MVC (OR, 3.15; 95% CI: 2.11–4.74; p < 0.001) and workplace (OR, 2.73; 95% CI: 1.74–4.35; p < 0.001).
Preinjury anxiety (OR, 1.97; 95% CI: 1.41–2.75; p < 0.001), postinjury sleep difficulties (OR, 1.44; 95% CI: 1.36–1.52; p < 0.001), and time since injury (OR, 1.16; 95% CI: 1.07–1.26; p < 0.001) were associated with msANX. Similarly, preinjury anxiety (OR, 1.87; 95% CI: 1.31–2.70; p < 0.001), postinjury sleep difficulties (OR, 1.62; 95% CI: 1.53–1.73; p < 0.001), and time since injury (OR, 1.10; 95% CI: 1.01–1.20; p = 0.03) were associated with msDEP. Prior concussion history or preinjury depression was not significantly associated with either msANX or msDEP.
Compared with a physician-confirmed “definite” concussion diagnosis, the odds of msANX were 47% lower for a “possible” concussion (OR, 0.53; 95% CI: 0.33–0.86; p = 0.010). Similarly, msDEP odds were 39% lower for “probable” concussion (OR = 0.61; 95% CI: 0.46–0.83; p = 0.001) and 54% lower for “possible” concussion (OR = 0.46; 95% CI: 0.28–0.74; p = 0.001). Age showed a nonlinear pattern, with msANX and msDEP risk increasing through early adulthood and then decreasing in one’s early thirties (Supplementary Figs. S1 and Figs. S2). Supplementary Table S3 summarizes anxiety and depression scores according to participant characteristics.
Discussion
In this cohort study of 1,693 adolescents and adults referred to a specialty concussion clinic, nearly half reported msANX and two out of three experienced msDEP at intake assessment. Nearly all those with anxiety also had co-occurring depression, underscoring the clinical complexity and need for early specialty care. Among those with moderate-to-severe symptoms, anxiety scores met and depression scores exceeded common clinical severity thresholds above which referral to a mental health professional for further assessment and active treatment is recommended.23,25 High levels of anxiety and depression symptoms were more common amongst females, adults between 18 and 60 years of age, non-sport-related settings/mechanisms, and those with preinjury psychiatric conditions in addition to commonly recognized clinical predictors, such as preinjury anxiety and depression. 28 MVC, workplace injuries, and assault were associated with between one and a half and four times greater odds of msANX and msDEP compared with playing sports, as were being female and having postinjury sleep difficulties. Time since injury was also associated with an increased risk of msANX and msDEP. This aligns with previous evidence that earlier care after concussion promotes faster recovery, likely through timely active rehabilitation, education, and specialty interventions.31,32 Since our participants presented on average three weeks after injury, this may partly explain the elevated symptom prevalence observed, although other predictors in our model had stronger associations.
Our use of validated mental health measures provides novel insight into the high prevalence of clinically important levels of anxiety and depression symptoms early on in concussion recovery. Since similar research has not been published, we are unable to directly compare our results with the current body of evidence. Nonetheless, our findings of msDEP (60.7%) at intake assessment are higher than previously reported at long-term follow-up after concussion. Other large-scale emergency department studies have reported 7% to 21.2% of adults hospitalized for traumatic brain injury, many with positive neuroimaging findings, met the criteria for major depressive disorder 6-months after concussion.7,12,33 On long-term follow-up of one of those studies, 34 rates of clinically significant depression and anxiety symptoms were double for those with versus without a preinjury psychiatric disorder and persisted at various time points over the following seven years. This reinforces the need for early screening and mental health referral to prevent persisting mental health problems after concussion. Likewise, the prevalence of msANX (45.2%) in our study was higher than the pooled estimate of 17.5% reported in a systematic review of anxiety symptoms and disorders following varying severities of traumatic brain injury.35,36 Rates of msANX and msDEP in the general population are estimated at 7.5% and 6.7%, respectively. 35
While our study does not speak directly to whether high levels of anxiety and depression symptoms early after concussion worsen long-term outcomes, they do highlight the need for early psychological care. This is especially important given gaps in follow-up care. Roughly only 7% of patients with moderate to severe persisting symptoms after concussion seen in the emergency department were seen by a psychologist or psychiatrist within 3 months after injury. 37 Even though we expect that follow-up rates from a specialty concussion clinic would be higher, cost of specialty care could nonetheless represent a barrier to mental health treatment. 38 Psychological treatments using existing best practice guidelines are critical, as they can decrease long-term mental health complications after concussion. 39 As aerobic exercise as “medicine” is considered best-practice for time to recovery and persisting symptoms after concussion, playing sports may also be protective of mental health symptoms after concussion.40,41 One small-scale study showed that high volumes (≥150 min/week) of early aerobic exercise may also be an effective treatment for anxiety and depression symptoms. This represents a promising opportunity for future research.
Age, sex, and preinjury mental health conditions are known clinical risk factors for persisting symptoms after concussion.29,42 Our study sheds light on additional risk factors for high levels of anxiety and depression symptoms at initial assessment. An important contribution of our study was that injury cause involving a MVC, workplace, or assault was independently associated with msANX and msDEP at initial assessment. Although Stein 12 found injury resulting from assault or violence to be a risk factor for posttraumatic stress disorder but not major depressive disorder 3–12 months after mild traumatic brain injury, the study cohort included 30.7% who had an intracranial injury on CT scan and 24.5% who were admitted to the intensive care unit. This cohort was more severely injured than those in our study. Being injured in an MVC or by assault are risk factors for persisting symptoms after concussion in those assessed in an emergency department, although its effect on early mental health symptoms has not been studied. Although previous prognostic models have compared falls (individually or combined with MVCs) with assault as risk factors for anxiety and depression after concussion, they did not consider broader causes of injury.12,13 Our study adds granularity to the evidence base by using sports-related concussions as the reference and including multiple settings/mechanisms as independent variables in our model.43–45 This suggests that clinical guidelines that are primarily based on sport-related concussion research may underestimate the mental health burden of concussion in those resulting from different causes of injury.
Our findings reinforce clinical guideline recommendations to routinely screen for mental health symptoms after concussion. Relying solely on global symptom evaluations (such as in the Sport Concussion Assessment Tool 6) to identify mental health problems, however, may result in underdiagnosis or inadequate care if validated anxiety and depression measures are not used. Diagnostically accurate screening tools, such as the GAD-7 and PHQ-9, can be used to assess symptom severity, monitor progress over time, and identify those who could benefit from further evaluation. Given the high mental health burden among adolescents and adults at initial assessment, there is an urgent need to better understand the natural progression of symptom change, potential biopsychosocial vulnerabilities, and the effectiveness of early, targeted mental health support on concussion recovery.
Key clinical takeaways from this study include (1) the cause of concussion should be taken into consideration to identify those at risk for high anxiety and depression symptoms; (2) symptoms at intake assessment are often severe enough to warrant referral to a mental health professional and active treatment.
Strengths and limitations
Our study has several strengths. We enrolled a large sample across a broad range of age, sex, injury setting/mechanism, and preinjury mental health conditions, and we used translators when necessary, enhancing generalizability. We used diagnostically accurate, validated screening tools as part of routine clinical care at three concussion clinics within a learning health system across Ontario (Canada), which optimizes applicability and ecological validity.
This study has limitations. First, although there is no objective biomarker of concussion, we used the ACRM diagnostic criteria that were developed by an interdisciplinary expert panel using the Delphi method. Second, we screened for anxiety and depression symptoms using validated self-report questionnaires rather than a comprehensive clinical interview. While they are not a substitute for a physician-confirmed mental health diagnosis, the GAD-7 and PHQ-9 are standardized measures widely used in clinical practice and research that are recommended by the National Institute of Neurological Disorders and Stroke and Department of Defense Sport-Related Concussion Common Data Elements and Common Measures in Mental Health Science Initiative.22,46 Third, because we did not collect data on preinjury anxiety and depression symptom severity (i.e., mild, moderate, severe) using a standardized clinical interview, we are unable to determine the directionality of any symptom change after concussion. However, the higher prevalence of msANX and msDEP after concussion compared to preinjury diagnosis or treatment suggests symptom worsening or new onset rather than improvement or stability. Fourth, while our findings provide valuable insight into the high prevalence of anxiety and depression symptoms after concussion, the observational study design and lack of control group did not allow us to establish causality or symptom trends over time. Fifth, our intake system was not set up to determine the proportion of participants who were referred from emergency departments versus primary care versus self-referred. Certainly, patients seen in specialty concussion clinics are at greater risk of persisting symptoms after concussion.47,48 As such, participants in this study may not represent patients who first present to acute care points of entry. To enable equitable healthcare access, 360 Concussion Care clinics require only a concussion diagnosis, regardless of injury setting or mechanism, and this may improve generalizability within this population. Sixth, our participants were predominantly university/college-educated patients with a household income of at least $100,000. Since higher education level and family income are associated with lower rates of anxiety and depression symptoms in the general population, 35 our results may not be generalizable to those with lower levels of health literacy or who are financially unable to access specialty care with out-of-pocket fees. Seventh, we only included participants with complete GAD-7 and PHQ-9 measures. Missing data may have introduced selection bias; however, we have confidence in our findings, as only 16/1,639 (1%) of participants were excluded for incomplete data, and participant characteristics were similar between groups (Supplementary Table S2). Eighth, since concussion is, by definition, 20 the result of a traumatic event, participants may have experienced symptoms of posttraumatic stress disorder, which we did not account for in this study. Finally, participants may have accessed other concussion services before presenting for specialty care, which may have affected their symptoms at intake assessment.
Conclusions and Relevance
Leveraging data collected during routine care, this study suggests that existing prevalence estimates likely underestimate the high levels of anxiety and depression symptoms at specialty clinic intake that warrant active treatment. Clinicians should routinely screen for mental health conditions and prioritize higher-risk patients for closer monitoring, including those injured in an MVC or at work, female patients, and those with preinjury anxiety or postinjury sleep difficulties. Timely referral to mental health professionals is needed to prevent chronic mental health problems and optimize recovery.
Transparency, Rigor and Reproducibility Summary
The protocol for the TRANSCENDENT Concussion Integrated Discovery Program was published and is freely available at BMJ Open (e095292.full.pdf). This study prospectively enrolled patients as part of routine clinical care without a predefined sample size calculation. However, the final sample size exceeds those commonly reported in similar studies published in the literature, thereby providing a robust basis for analysis and interpretation. The inclusion of a larger-than-typical cohort without common exclusion criteria enhances the generalizability and reliability of the findings. A total of 3,015 patients were screened, 1,706 enrolled, and 1,639 completed the outcome measures. Clinicians informed participants of outcomes as part of routine care. The diagnostic criteria and selected outcome measures are established standards and recommended concussion-specific common data elements. The data collected for this study is stored and will be shared via the Ontario Brain Institute’s (OBI’s) Brain-CODE neuroinformatics platform.
Authors’ Contributions
Dr. Zemek had full access to all of the data in the study and takes full responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design: Zemek, Johnston, van Ierssel, Yeates, Ledoux, Liu, Lalonde, Master, Howell, Chintoh, Mikolic, Beauchamp, Silverberg. Acquisition of data: Zemek, Johnston, Lamoureux. Analysis, or interpretation of data: van Ierssel, Webster, Kutcher, Pham, Zemek, Johnston. Drafting of the article: van Ierssel. Critical review of the article for important intellectual content: All authors. Statistical analysis: Webster, Kutcher, Pham. Obtained funding: Zemek, Johnston, Yeates, Ledoux, Lalonde, Master, Howell, Mikolic, Beauchamp, Silverberg. Administrative, technical, or material support: Lamoureux, Dodd, Mullan. Supervision: Zemek.
Footnotes
Acknowledgments
Thank you to the clinical and research staff at 360 Concussion Care, where the TRANSCENDENT research program is integrated into the learning health system. A special thank you to the patients who participated in the study and whose contribution would not make this research possible.
Author Disclosure Statement
Roger Zemek’s (R.Z.) program of research has received financial support through competitively-funded research grants from Canadian Institutes of Health Research (CIHR), Ontario Neurotrauma Foundation (ONF), Physician Services Incorporated (PSI) Foundation, CHEO Foundation, Ontario Brain Institute (OBI), National Football League (NFL), Brain Heart Interconnectome Canada First Research Excellence Fund (BHI-CFREF), Ontario Ministry of Health (MOH), Public Health Agency of Canada (PHAC), Health Canada, Parachute Canada and Ontario SPOR Support Unit (OSSU). R.Z. is also supported by a Tier 1 Clinical Research Chair in Pediatric Concussion from University of Ottawa. All grant funding goes directly to the institution. R.Z. sits on the board of directors for North American Brain Injury Society (NABIS) which is a volunteer (unpaid) role. Finally, R.Z. is a founding partner and a minority shareholder of 360 Concussion Care (a learning health system and network of interdisciplinary concussion clinics in Ontario); no proceeds have been transferred to RZ.
K.O.Y. receives an editorial stipend from the American Psychological Association; is principal investigator on grants from the Canadian Institutes of Health Research and Canada Foundation for Innovation, and coinvestigator on grants from the Canadian Institutes of Health Research, Brain Canada Foundation, Ontario Brain Institute, and the National Football League Scientific Advisory Board; has paid research consultancies with University of California San Francisco, Pennsylvania State University, and Research Institute at Nationwide Children’s Hospital; receives book royalties from Guilford Press and Cambridge University Press; has been provide with travel support and honorariums for presentations to multiple organizations; serves on the Data Safety and Monitoring Board for the Concussion Health Improvement Program Trial, University of Washington, and on the National Research Advisory Council for the National Pediatric Rehabilitation Resource Center, Virginia Tech University.
C.L.M. has received research support from the Centers for Disease Control, National Institutes of Health (National Institute of Neurological Disorders and Stroke, National Eye Institute, National Institute of Nursing Research), Department of Defense, National Collegiate Athletics Association, American Medical Society for Sports Medicine Collaborative Research Network, Chuck Noll Foundation, Children’s Hospital of Philadelphia Frontier Program, Toyota Way Forward Foundation.
M.B. receives funding as part of a Canada Research Chair in Pediatric TBI, receives book royalties from Guilford Press, and is an unpaid board member of the International Brain Injury Association and International Pediatric Brain Injury Society.
Funding Information
This research was conducted with the support of the Ontario Brain Institute (OBI funding for period 2023–2026), an independent nonprofit corporation funded partially by the Ontario government. The opinions, results, and conclusions are those of the authors, and no endorsement by the Ontario Brain Institute is intended or should be inferred. Additional funding was provided by Canada First Research Excellence Fund for the Brain-Heart Interconnectome (CFREF-2022-00007).
Role of the Funder/Sponsor
The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Data Sharing Statement
The data collected for this study are stored and will be shared via the Ontario Brain Institute’s (OBI’s) Brain-CODE neuroinformatics platform.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.