
Abstract
Invasive intracranial pressure (ICP) monitoring provides essential guidance for the treatment of patients with suspected head injuries; however, it remains incompatible with prehospital use. While several noninvasive ICP-measuring methods exist, previous studies have not adequately addressed their potential in a prehospital setting. In this systematic review and meta-analysis of diagnostic test accuracy, we explore the accuracy of existing noninvasive methods for ICP monitoring and assess their potential usefulness in prehospital screening for elevated ICP. This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses guideline. Embase, Scopus, PubMed, CENTRAL, and Cochrane databases were sought for relevant articles on June 23, 2025. All studies evaluating minimally invasive and transportable methods for ICP assessment were included. Animal studies, in vitro studies, reviews, and meta-analyses were excluded. Study selection was performed by two independent reviewers, and conflicts were resolved by a third reviewer. Potential for prehospital use of each method was evaluated using four predetermined criteria. Summary receiver operator characteristic curves and summarized sensitivity and specificity were reported if multiple studies investigating the same method were eligible for meta-analysis. The applicability and risk of bias of the included studies were assessed using the Quality Assessment of Diagnostic Accuracy Studies 2 tool for diagnostic test accuracy studies. Fifty-five articles were included. Ultrasound of optic nerve sheath diameter (ONSD) was the method with the highest potential for prehospital use. We found a summarized sensitivity of 92.6% (95% confidence interval [CI]: 87.0; 95.9%) and a summarized specificity of 85.1% (95% CI: 74.1; 92.0%) for detecting increased ICP through ONSD measurement. Other methods for diagnosing elevated ICP diagnosis showed poor diagnostic accuracy or low potential for prehospital use. We found ultrasound estimation of the ONSD to show the highest potential for prehospital use. Prospective studies are needed to verify their diagnostic capability in the prehospital setting.
Introduction
Intracranial pressure (ICP) monitoring is an established component in monitoring patients with severe hemorrhagic stroke and severe traumatic brain injury (TBI). It serves as a guide for therapeutic interventions and the detection of intracranial mass lesions. 1 Elevated ICP can lead to cerebral ischemia, brain herniation, and death when left untreated and is associated with considerable morbidity and mortality. 2 The insidious onset and nonspecific symptoms complicate early detection. 3 Early diagnosis of elevated ICP in a prehospital setting, which could enable direct transportation of patients to a neurosurgical center and earlier intervention, may decrease the risk of secondary injury.1,4 Accurately measuring ICP requires the placement of invasive pressure monitors by experienced neurosurgeons in a highly specialized setting. Previous research has shown that in-field detection of elevated ICP relies on clinical tools that tend to have low accuracy. 5 However, ultrasound-based methods have shown potential for noninvasive detection of intracranial pathology. 6 While several techniques for noninvasive ICP estimation have been proposed, an in-depth analysis of the available options and their compatibility with prehospital ICP screening is essential to strengthen the development of these noninvasive technologies. In this review and meta-analysis, we aim to find the most reliable noninvasive modalities for exploring the feasibility and accuracy of ICP monitoring modalities with potential for prehospital use.
Methods
Search strategy
The study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses criteria. 7 Embase, Scopus, PubMed, CENTRAL, and Cochrane databases were sought for relevant articles on June 23, 2025, using a search strategy containing keywords identifying the cohort, keywords identifying emergency or prehospital settings, and terms defining the intervention of measuring intracranial pressure, without filters or limits. The full search strategy can be found in Supplementary Data. Original articles cited in systematic reviews and meta-analyses that were identified through the initial literature search were included in the abstract screening process equally to other search results. Articles found this way were categorized as citation-searched results, and the systematic reviews and meta-analyses from which they were found were later excluded during the abstract screening process.
Eligibility criteria and study selection
We included all studies evaluating methods of ICP assessment with potential use in a prehospital setting, defined as noninvasive or minimally invasive methods performed with transportable devices. Studies were excluded if the full text in English language was not available. We also excluded in vitro studies, animal studies, reviews, and meta-analyses. Articles were managed using the web-based software Covidence. 8 All articles were initially assessed for eligibility by two investigators (A.N.R.L., M.H.K.) based on abstract and title. The selected articles were then full-text screened for eligibility by the same investigators (A.N.R.L., M.H.K.). Disagreements were resolved by a third investigator (M.F.G.). Data were extracted by one investigator (A.N.R.L.) and validated by a second investigator (V.H.).
Data extraction and outcomes
Data describing each method for ICP estimation were collected, including the reference standard test used, standard cutoff values for a positive index test, and technical details on the devices used.
Data describing the population in each study were extracted, including patient characteristics, number of participants, study design, and clinical setting of the study.
Data on index test accuracy were collected, including the number of true-positive (TP), false-positive (FP), true-negative (TN), and false-negative (FN) test results, reported sensitivity, specificity, positive predictive values, negative predictive values, and area under the curve (AUC) for receiver operating characteristic (ROC) curves.
Data were extracted as available from articles and supplementary material. Studies were not excluded based on the availability of data. All studies meeting the inclusion criteria were included in the systematic review. Meta-analysis was performed for methods where diagnostic test accuracy was tested in multiple studies with invasive ICP monitoring as a reference test. Only studies reporting TP, FP, TN, and FN, or reporting sufficient data to calculate these, were included in the meta-analysis.
Invasive ICP measurement was considered the gold standard test, and measurements of >20 mmHg were considered elevated. 2
Quality assessment
The quality of the included studies was assessed using the Quality Assessment of Diagnostic Accuracy Studies 2 tool. 9 Quality assessment was performed by two independent investigators (A.N.R.L., V.H.), and conflicts were solved through consensus.
Statistical analysis and evaluation
Analyses were performed using RevMan 5.4 software 10 and MetaDTA software,11,12 designed for meta-analysis of diagnostic test accuracy studies. For studies included in the meta-analysis, we report forest plots of sensitivity and specificity of each study with 95% confidence intervals (CIs) and summary ROC curves using a bivariate model with a 95% confidence area.
Suitability for prehospital use of each method was assessed by evaluation of the following four properties: (1) The device is sufficiently mobile, that is, small in size or based on equipment already widely used in ambulances or helicopters. (2) The method can provide a valid assessment of ICP in <5 min. (3) The device has minimal or no sterilization requirements. (4) ICP assessment can be performed by one person with minimal training requirements (<7 h, equivalent to 1 day). Studies were deemed of high potential for prehospital use, if they fulfilled ≥3/4 evaluation criteria.
Results
Study selection and quality assessment
We identified 2603 studies, and 1713 duplicates were removed. The remaining 965 studies were screened by title and abstract, and 124 studies were selected for full-text review. Twenty-two articles were excluded due to the unavailability of the full-text study in English. In total, 55 studies were included in the review and meta-analysis (Fig. 1). An overview of study characteristics and quality assessment for each study is found in Table 1 and Supplementary Table S1.
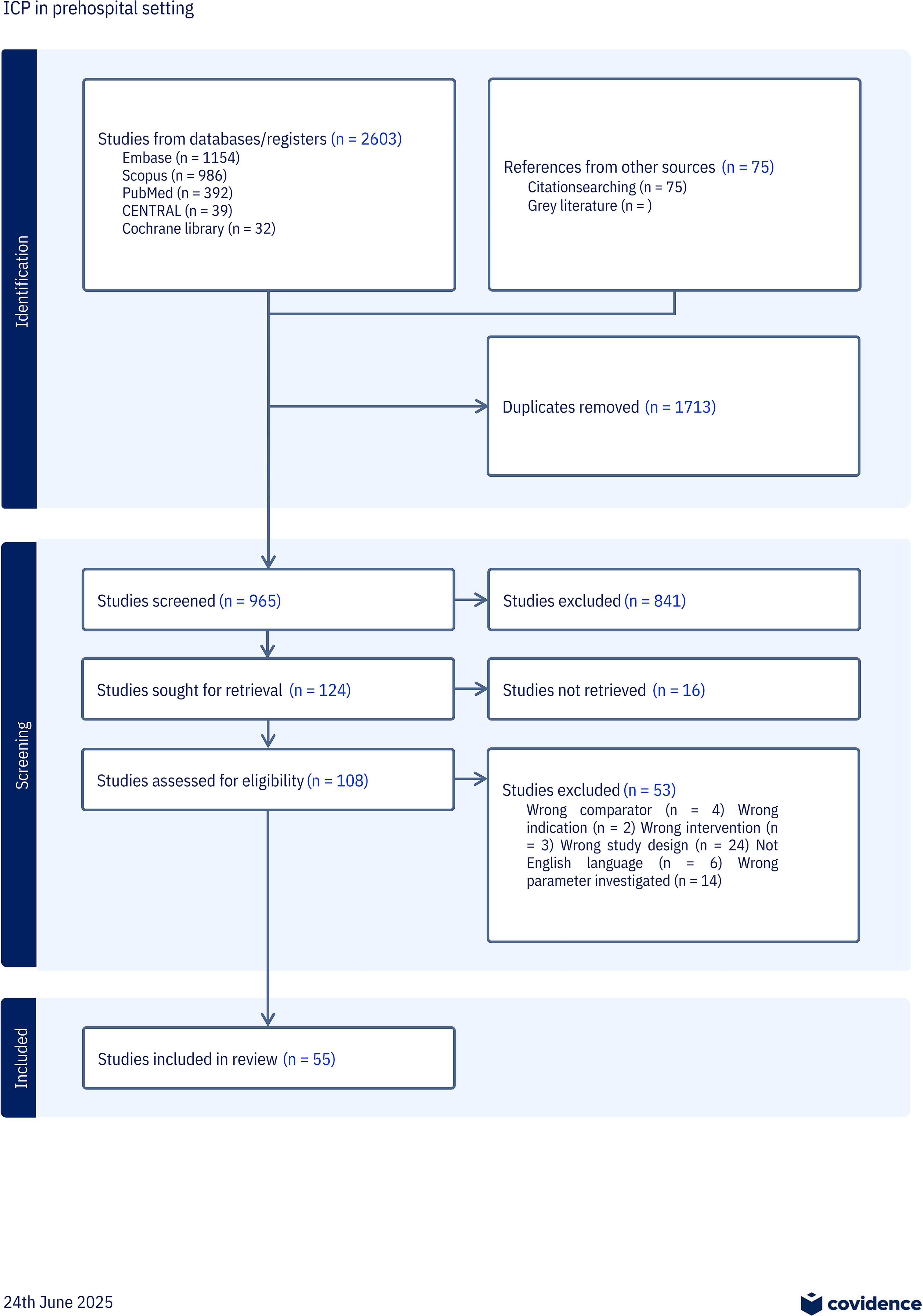
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Characteristics of Included Studies
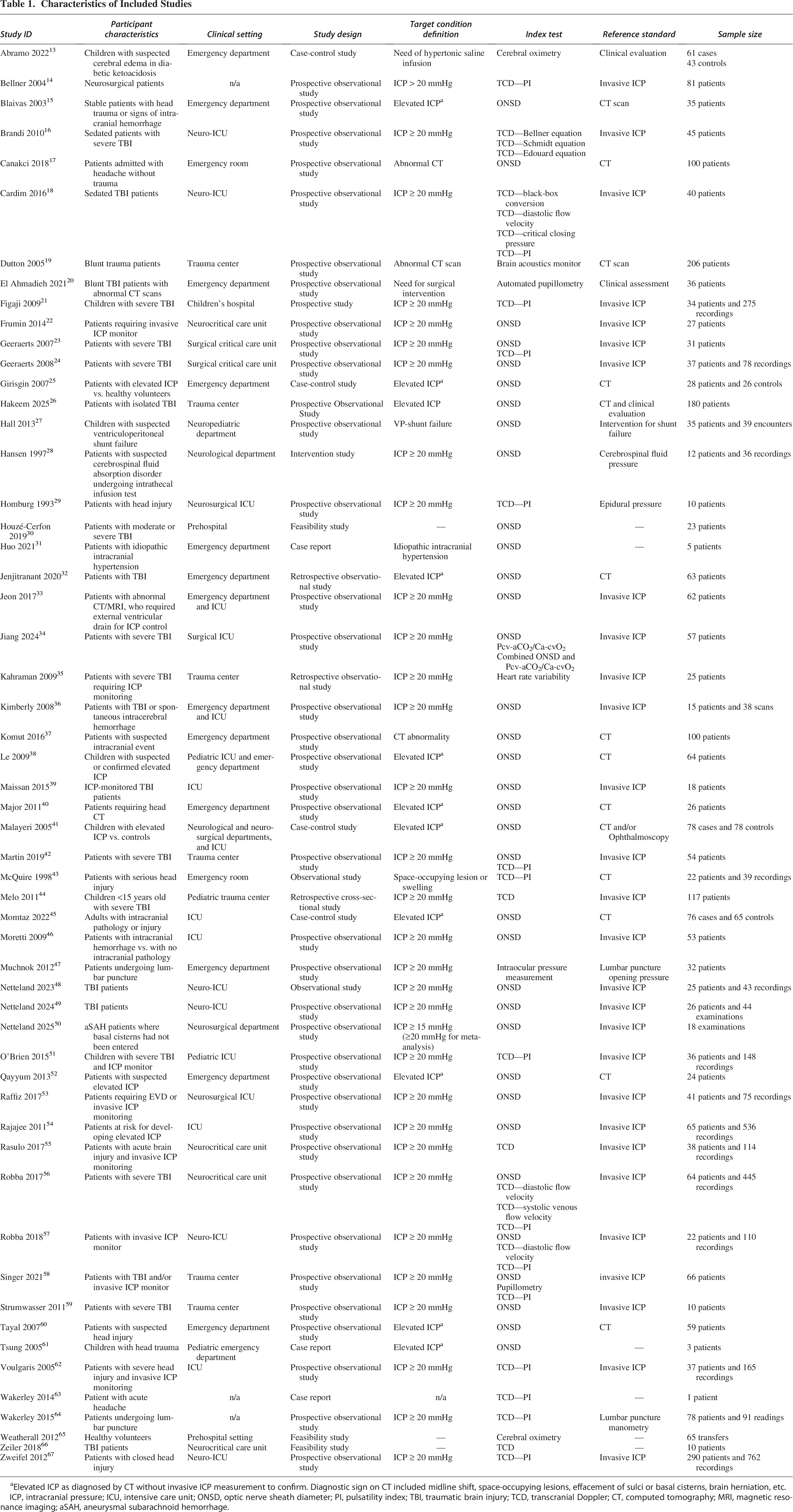
Elevated ICP as diagnosed by CT without invasive ICP measurement to confirm. Diagnostic sign on CT included midline shift, space-occupying lesions, effacement of sulci or basal cisterns, brain herniation, etc.
ICP, intracranial pressure; ICU, intensive care unit; ONSD, optic nerve sheath diameter; PI, pulsatility index; TBI, traumatic brain injury; TCD, transcranial Doppler; CT, computed tomography; MRI, magnetic resonance imaging; aSAH, aneurysmal subarachnoid hemorrhage.
Prehospital suitability
Optic nerve sheath diameter for diagnosing elevated ICP
A total of 31 studies investigated the use of optic nerve sheath diameter (ONSD) for predicting elevated ICP15,17,22–26,28,30–34,36,37,39,40,42,45,46,48–50,52–54,56–60 in adult patients. ONSD was measured by ocular ultrasound through a closed eyelid using a linear probe. The diameter was measured 3 mm proximally to the optic disc perpendicular to the optic nerve. As a standard, ONSD was considered normal if <5 mm and increased if ≥5 mm.
Ultrasound of ONSD was performed using standard ultrasound equipment, taking a median of 4 min to obtain a valid measurement, 30 in a noninvasive manner, and after 4 h of training. 30 Thus, the method fulfilled 4/4 of the evaluation criteria for prehospital suitability (Table 2).
Prehospital Suitability of the Included Methods
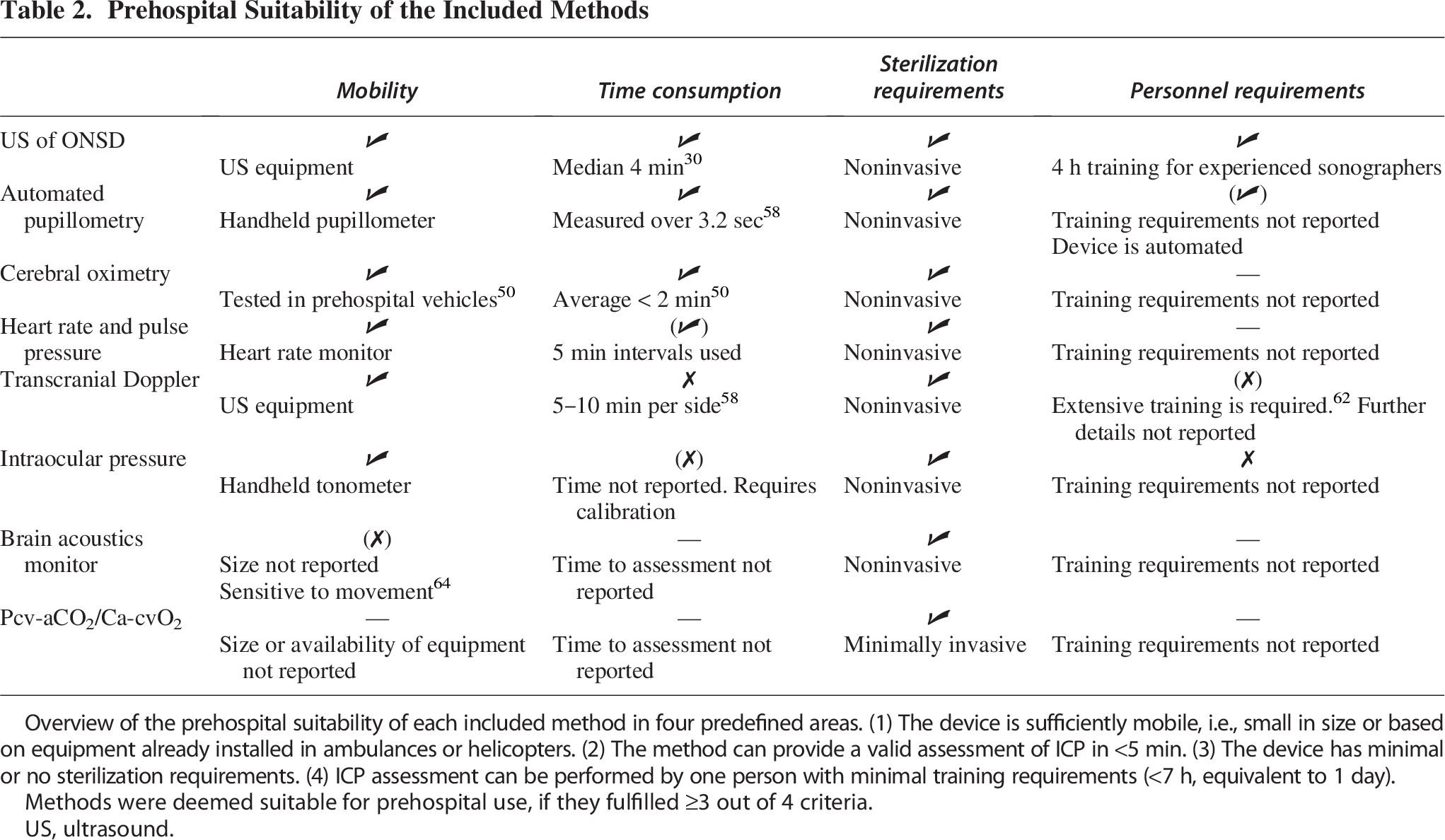
Overview of the prehospital suitability of each included method in four predefined areas. (1) The device is sufficiently mobile, i.e., small in size or based on equipment already installed in ambulances or helicopters. (2) The method can provide a valid assessment of ICP in <5 min. (3) The device has minimal or no sterilization requirements. (4) ICP assessment can be performed by one person with minimal training requirements (<7 h, equivalent to 1 day).
Methods were deemed suitable for prehospital use, if they fulfilled ≥3 out of 4 criteria.
US, ultrasound.
Pupillometry
Two studies investigated the use of neuropupillary index (NPI) score and the correlation to elevated ICP.20,58 Both studies used an infrared pupillometer, which automatically measured pupil size, response latency, and constriction and relaxation velocity, and computed these measures into the NPI score between 0 and 5 for each eye.
Pupillometry-based estimation of ICP was performed using a handheld automated pupillometer, evaluating the NPI over 3.2 sec, 58 in a noninvasive manner with unknown training requirements. Thus, the method fulfilled 3/4 of the evaluation criteria for prehospital suitability (Table 2).
Cerebral tissue oximetry
Noninvasive cerebral tissue oximetry was investigated in two of the included studies.13,65 Two cerebral oximetry probes were placed on the forehead of the patients, and regional cerebral oxygen saturation (rcSO2) was recorded at short time intervals by near-infrared spectroscopy. Cerebral oximetry was performed using portable cerebral oximetry probes, tested during transport in a prehospital setting, taking on average <2 min to obtain a valid measurement, 65 in a noninvasive manner, with unknown training requirements. Thus, the method fulfilled 3/4 of the evaluation criteria for prehospital suitability (Table 2).
Heart rate and pulse pressure
One study investigated the correlation between heart rate and pulse pressure and ICP 35 in 25 patients with severe TBI. Heart rate and pulse-pressure-based estimation of ICP was performed using a standard heart monitor, for 5-min intervals, in a noninvasive manner with unknown training requirements. Thus, the method fulfilled 3/4 of the evaluation criteria for prehospital suitability (Table 2).
Transcranial Doppler
A total of 19 studies investigated the use of transcranial Doppler (TCD) for estimating elevated ICP14,16,18,21,24,29,42–44,51,55–58,62–64,66,67 patients with confirmed or suspected head injury or other intracranial pathology; of these, 13 studies investigated the use of pulsatility index (PI) to predict elevated ICP in adult patients.14,18,23,29,42,43,56–58,62–64,67
PI was found through TCD examination of the middle cerebral artery and calculated as the ratio between the difference in systolic flow velocity (FVs) and diastolic flow velocity (FVd), and the mean flow velocity (FVm);
Intraocular pressure
One study investigated the use of intraocular pressure (IOP) measurement for diagnosing elevated ICP. 47 IOP measurement was performed using a handheld tonometer in a noninvasive manner, with unknown requirements for time and personnel training. Thus, the method fulfilled 2/4 of the evaluation criteria for prehospital suitability (Table 2).
Brain acoustics monitoring
One study investigated the use of the brain acoustics monitor (BAM) for diagnosing elevated ICP. 19 The BAM records sound waves from the skull through a sensor placed on the patient’s forehead.
The BAM was used to estimate ICP noninvasively, with unknown requirements for space, time, and training. However, the BAM was reported sensitive to patient movement. Thus, the method fulfilled 1/4 of the evaluation criteria for prehospital suitability (Table 2).
Pcv-aCO2/Ca-cvO2
One study investigated the use of the ratio between central venous (cv) minus arterial (a) CO2 pressure and arterial minus central venous O2 (
Diagnostic accuracy
In the following, we present a review and meta-analysis of the diagnostic accuracy of the methods with high potential for prehospital use, that is, fulfilling ≥3/4 evaluation criteria for prehospital suitability. A review of the remaining methods can be found in Supplementary Data.
ONSD for diagnosing elevated ICP
In 24 studies, the optimal cutoff value in adult patients was found to be 4.7–6.3 mm.15,17,22–24,26,28,31,33,34,36,37,39,40,42,45,46,50,52,54,56,57,59,60 One study found an optimal cutoff value of 3.15 mm. 32
Twenty studies reported ROC curves of ONSD for diagnosing elevated ICP (>20 mmHg). Nineteen studies26,33,34,36,37,39,42,45,48–50,52–54,56,57 found a good diagnostic accuracy, with an AUC of 0.72–1.00, while one study 59 found the test to be insufficient with an AUC of 0.36.
Two studies evaluated mean ONSD in patients with elevated ICP compared with patients without. One study found no correlation between ONSD and elevated ICP, 58 while the other found a significantly higher mean ONSD in patients with elevated ICP compared with patients with normal ICP. 25
One study tested the quality of ONSD measurements performed in a prehospital setting by physicians experienced in sonography, who received 4 h of training in ocular ultrasound prior to the study. 30 ONSD measurements were obtainable and validated by experts in 80% of cases during ambulance transportation, 71% in the field, and 43% during helicopter transportation.
The sensitivity and specificity of ultrasound of ONSD for detecting elevated ICP in adults found in each study included in the meta-analysis are summarized in Figure 2. We found a summarized sensitivity of 92.6% (95% CI: 87.0; 95.9%) and a summarized specificity of 85.1% (95% CI: 74.1; 92.0%) across 15 studies evaluating the diagnostic accuracy of ultrasound of ONSD for detecting elevated ICP on invasive monitoring22–24,28,33,34,36,42,46,50,53,54,56,57,60 (Fig. 3A). Risk of bias and applicability concerns in the included studies are illustrated in Figure 4. Furthermore, summary ROC curves for different cutoff values are shown in Figure 3B. Studies using 5.2 mm as a cutoff value showed the highest summarized diagnostic odds ratio of 92.2 (95% CI: 20.8; 407.9) across three studies.
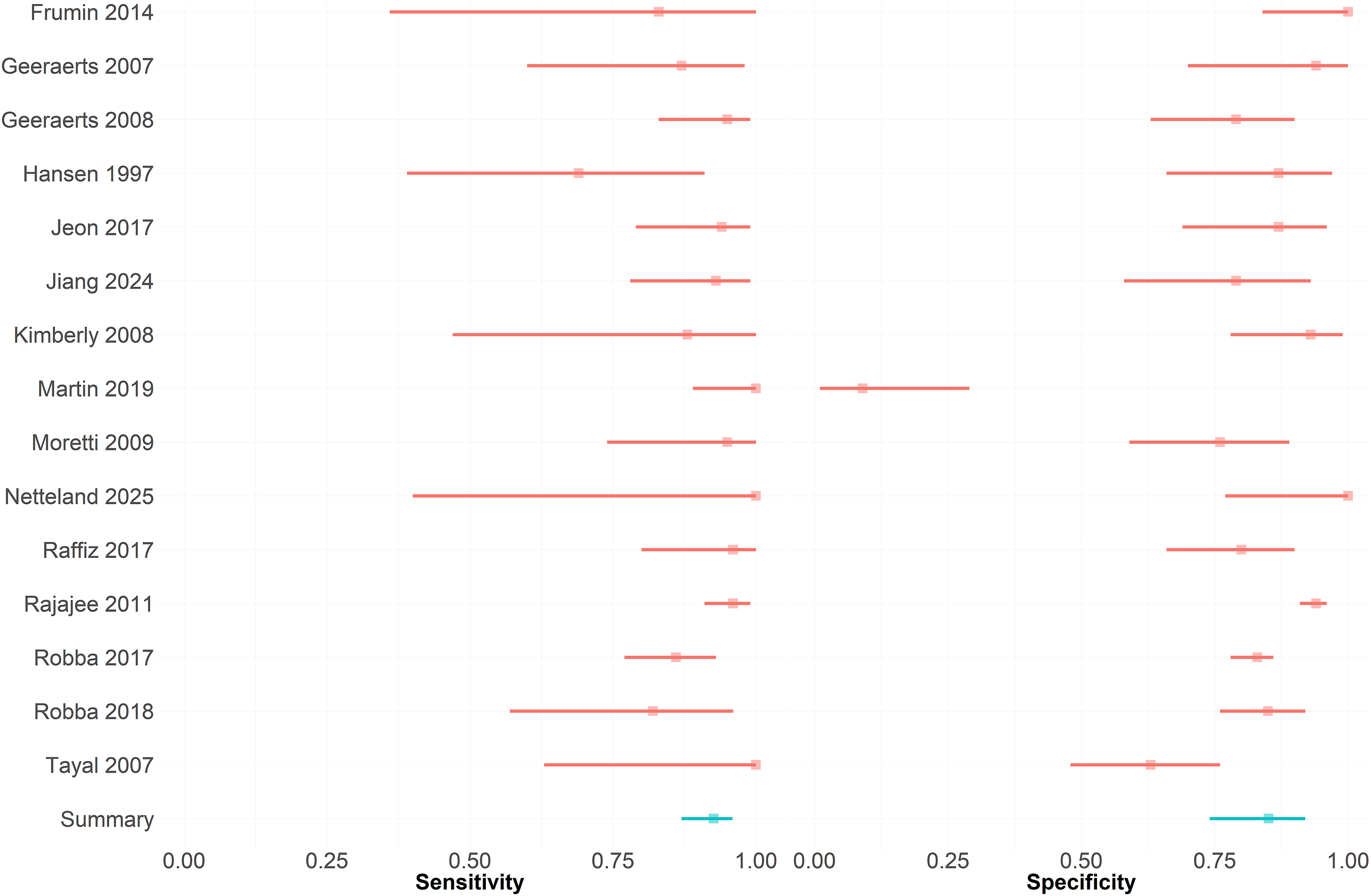
Forest plot for studies evaluating optic nerve sheath diameter. Forest plot of sensitivity and specificity of optic nerve sheath diameter for diagnosing elevated ICP for studies included in the meta-analysis.
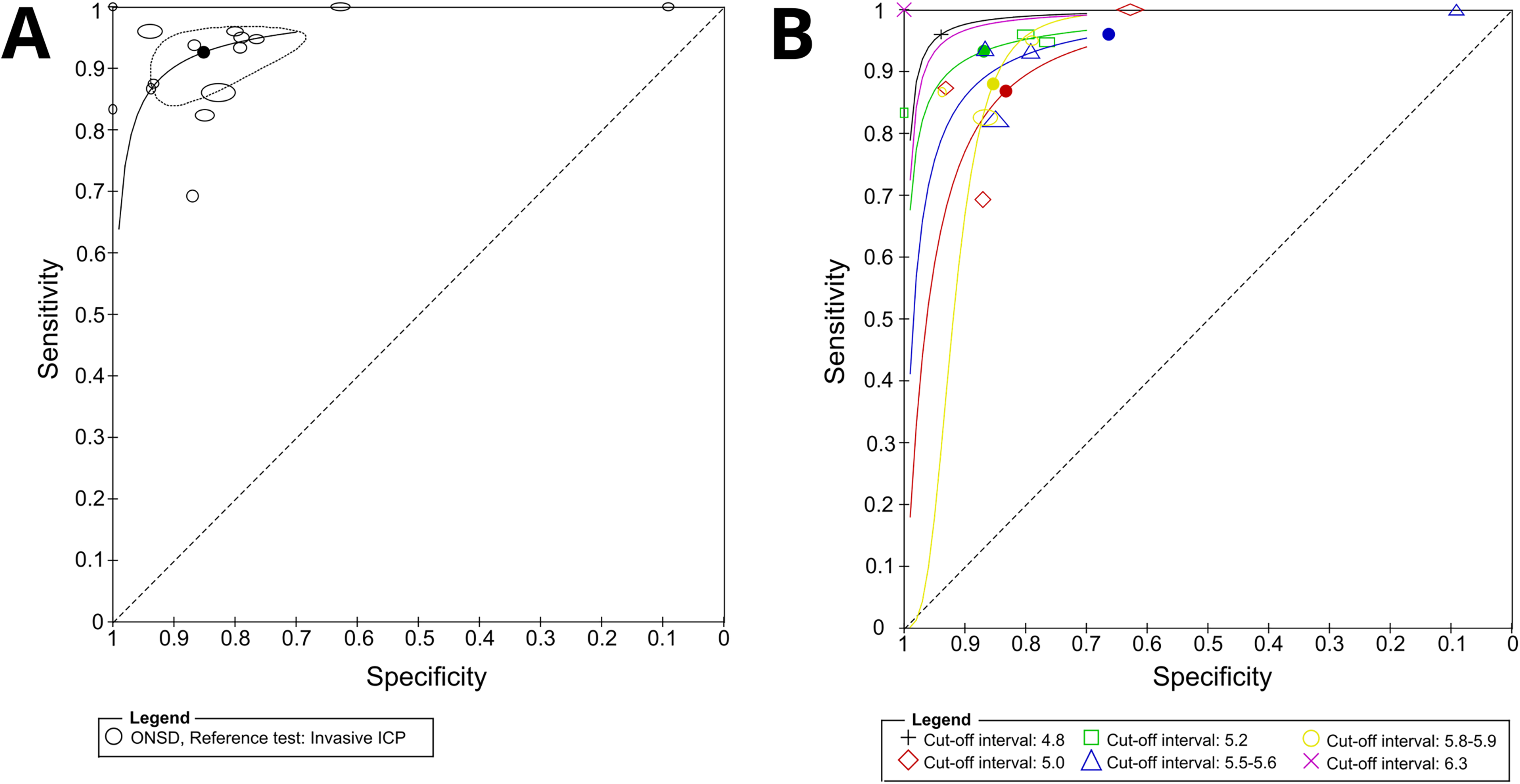
Summary receiver operator curve of ONSD for detecting elevated ICP.
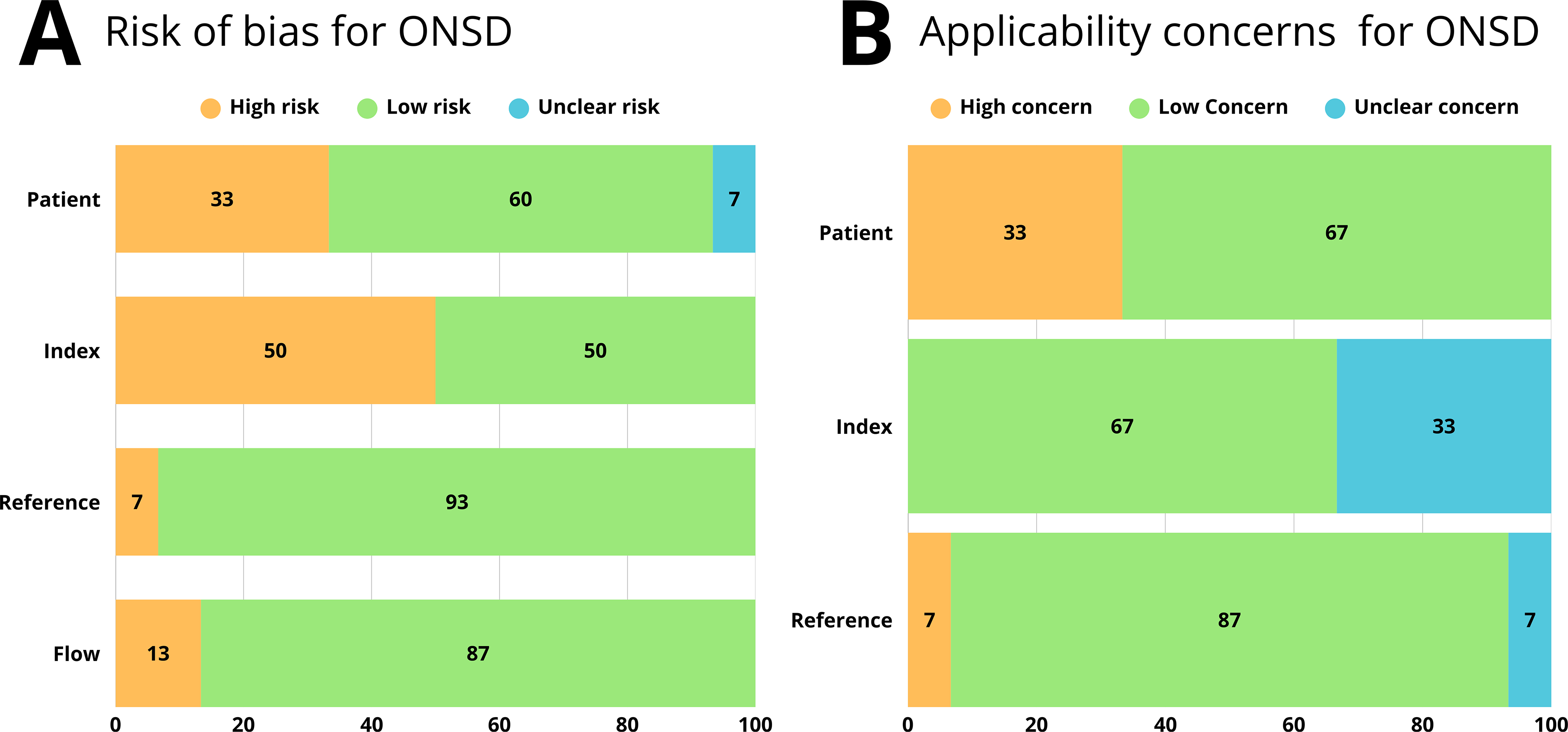
Summary of quality assessment of studies included in the meta-analysis. Summary of risk of bias and applicability concerns in each domain for studies included in the meta-analysis, assessed using the QUADAS-2 tool for diagnostic test accuracy studies.
Four studies evaluated the use of ONSD for diagnosing elevated ICP in pediatric patients, using the same measuring technique as for adults.27,38,41,61 All studies used cutoff values of ≥4.0 mm for children <1 year and ≥4.5 mm for children >1 year. One study found a significant difference in mean ONSD between cases with elevated ICP and a control group with normal ICP. 41 Two studies reporting sensitivity and specificity of ONSD for detecting elevated ICP 38 or neurosurgical intervention for shunt failure 27 found a sensitivity of 61.1–83% and a specificity of 22.2–38%.
Cerebral tissue oximetry
One study 13 investigated the use of cerebral tissue oximetry in pediatric patients with suspected cerebral edema diabetic ketoacidosis (SCEDKA), comparing readings before and after hypertonic saline solution (HTS) infusion as a proxy for elevated ICP. They found that rcSO2 was significantly lower after infusion of HTS. They also found a significant difference in rcSO2 between SCEDKA patients and controls, both before and after HTS infusion.
Another study 65 investigated the feasibility of cerebral tissue oximetry in a prehospital setting and during transportation in 33 healthy volunteers and found that the probes provided successful bilateral monitoring for over 70% of the monitoring period in 100% of volunteers during road transport and 85.7% of volunteers during helicopter transport. However, they also found that in 50% of cases, the probes could not provide monitoring when used in ambient light due to light contamination.
Pupillometry
One study 20 found a significantly lower NPI score in 9 TBI patients who later underwent neurosurgical intervention than in 27 TBI patients who did not. Three patients with bilaterally normal NPI (≥3) underwent invasive ICP monitoring and did not show elevated ICP. Two patients had a low NPI score (<3) in one or both pupils and were monitored with invasive ICP monitoring. Both patients had consistently increased ICP.
Another study 58 found no correlation between pupillometry-derived measures and ICP measurements in 36 severe TBI and 39 nontrauma patients with invasive ICP monitors.
Heart rate and pulse pressure
One study 35 found that pulse pressure, heart rate variability (HRV), and pulse pressure variability (PPV) increased with increasing ICP when cerebral perfusion pressure (CPP) remained stable and that HRV and PPV decreased significantly when CPP decreased to ≤60 mmHg.
Discussion
In this systematic review and meta-analysis, we have explored ICP measuring devices with potential for use in the prehospital environment. We found a range of different methods for noninvasive ICP estimation performed with transportable equipment, potentially suitable for prehospital use.
After evaluating each of the methods on four predefined criteria for prehospital suitability, we found that four of the seven identified methods fulfilled at least 3/4 criteria and thus showed high potential for prehospital use.
Of these, the most extensively researched method was the measurement of ONSD. One of the advantages of this method is that ultrasound equipment is inexpensive and readily available in most parts of the world. While the need for an experienced sonographic operator is a limitation, studies indicate a rapid learning curve for ONSD ultrasound for both experienced sonographers and novices. 60 Furthermore, automated modalities for monitoring ONSD are available, reducing the need for operator experience and limiting interoperator variability, 48 though these options have not yet been thoroughly tested.
As one of the main limitations of sonographic ICP estimation in a prehospital setting seems to be time consumption, 30 this is a crucial factor to consider. However, one of the included studies indicated that valid ultrasonic ONSD measurements were obtainable in 80% of cases during ambulance transportation, when performed by experienced sonographers, 30 limiting the time needed to perform this assessment on scene.
Our meta-analysis showed a summarized sensitivity of 92.6% (95% CI: 87.0; 95.9%) and a summarized specificity of 85.1% (95% CI: 74.1; 92.0%), indicating a high diagnostic accuracy of ONSD. While the overall accuracy of the test is important when used for prehospital screening for elevated ICP, a test with high sensitivity should be prioritized to ensure the identification of most cases with elevated ICP. It is likely that higher diagnostic accuracy and predictive value may be obtained by combining two or more ICP estimation methods; however, using multiple measures may also increase the time needed to assess ICP, thus limiting the use in acute situations.
Methods like heart rate variability and pupillometry showed poor correlation with ICP and limited potential for diagnosing elevated ICP, and the research on these methods was likewise limited. Thus, the value of these methods as a prehospital tool for diagnosing elevated ICP remains undetermined.
Finding and implementing an affordable and accessible noninvasive method for prehospital evaluation of increased intracranial pressure could be of great value, especially in low income or rural areas, where computed tomography scan or neurosurgical expertise may not be readily available. In these situations, a way of diagnosing early stages of increased ICP could mean both early prehospital intervention and a timelier decision to transport patients to a facility with neurosurgical capabilities.
Limitations
There was substantial heterogeneity in the specifics of the tested methods, the reference standard, the defined thresholds for a positive test, and the patient populations investigated in the included studies, reducing the generalizability. In a prehospital setting, the aim of measuring ICP would be to determine the need for neurosurgical intervention in patients without clear signs of intracranial pathology, while most of the included study populations consisted of patients with severe injuries, where clinical signs are typically more distinct.
In the absence of a validated method for assessing prehospital suitability, the potential for prehospital use was assessed through four major criteria formulated by investigators with extensive prehospital qualifications and experience. However, other factors, such as power requirements and durability when exposed to adverse conditions, including humidity, temperature changes, and dirt or dust, that could potentially influence the suitability of a device for prehospital use should be carefully considered and assessed before implementation.
The meta-analysis in this study was conducted based on a dichotomous evaluation of whether ICP was elevated. In a clinical setting, a more graded evaluation of the relation between ONSD and ICP across studies could be valuable; however, the reported data in the included studies were insufficient to perform a meta-analysis of this aspect.
In several studies, the index test was performed by one or a few trained physicians, limiting the ability to examine inter-rater variability. Most included studies were conducted in hospitals in emergency departments or intensive care units, further reducing the transferability to a prehospital setting. Quality assessment showed a high risk of bias in 50% of studies included in the meta-analysis in relation to the index test, primarily due to the lack of blinding during test result interpretation, and in 33% of studies in relation to the patient population, primarily due to a nonrandom inclusion process. The proportion of high risk of bias was low in the remaining domains. Between 14% and 33% of studies included in the meta-analysis were assessed to have high or unclear applicability concerns regarding patient population, index test, and reference standard.
Conclusion
Several portable, noninvasive methods for detecting elevated ICP are available; however, no single method has been sufficiently investigated. In this review, we found ultrasonic measurement of the ONSD to have the highest potential for prehospital use; however, most of the studies found through this systematic review and meta-analysis were performed in emergency departments and ICU settings with a very limited number of investigators performing the test. Further prospective studies evaluating the use of this method in a prehospital setting are needed to verify the value and diagnostic capability.
Transparency, Rigor, and Reproducibility Summary
This study was not formally registered. The analysis plan was not formally preregistered, but the team member with primary responsibility for the analysis certifies that the analysis plan was prespecified. Data were acquired between April 2023 and June 2025. Data were collected using Covidence. 8 Data were analyzed using RevMan. 10 All datasets were analyzed at the same time. All equipment and software used to perform acquisition and analysis are widely available from Covidence.org and Cochrane.org. The primary prehospital eligibility criteria have not been established as a standard in the field. The criteria were formulated by investigators with extensive prehospital qualifications and experience. The statistical tests used were based on the assumptions of independent measurements. The authors agree or have agreed to publish the article using the Mary Ann Liebert, Inc. “Open Access” option under appropriate license.
Authors’ Contributions
A.N.R.L.: Conceptualization, formal analysis, investigation, methodology, writing—original draft, writing—review and editing, and visualization; M.H.K.: Investigation and writing—review and editing; V.H.: Conceptualization, investigation, validation, and writing—review and editing; M.R.: Methodology and writing—review and editing; K.U.K.: Writing—review and editing; A.G.: Writing—review and editing; R.M.: Writing—review and editing; L.K.R.: Writing—review and editing; C.Z.S.: Writing—review and editing; M.F.G.: Investigation and writing—review and editing; A.R.K.: Conceptualization, validation, resources, writing—original draft, writing—review and editing, visualization, supervision, project administration, and funding acquisition.
Footnotes
Author Disclosure Statement
A.R.K. reports grants from IRRAS AB to Aarhus University Hospital to support the ACTIVE study and personal fees from IRRAS AB for a presentation at a scientific symposium describing his experiences with the IRRAflow technology during the conduct of the study; grants from IRRAS AB to Aarhus University Hospital to support the development of a neuromonitoring technology related to IRRAflow outside the submitted work. In addition, A.R.K. has a patent for a neuromonitoring technology pending with relation to the IRRAflow technology. The remaining authors have no conflicts of interest to declare.
Funding Information
A.R.K. is supported by grants from the Danish Cancer Society (R304-A17698-B5570 and R295-A16770), the Lundbeck Foundation (R325-2019-1490), and the Independent Research Fund Denmark (903900307B) unrelated to this study. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; and decision to submit the article for publication.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.