
Abstract
Mild traumatic brain injury (mTBI), a common health burden among combat veterans, has been associated with alterations in brain structure. Moreover, post-traumatic stress disorder (PTSD), frequently comorbid with mTBI, is linked to smaller cerebellum volumes; however, little is known about whether mTBI (absent comorbid psychiatric symptoms) similarly affects cerebellar structure. The cerebellum may play a central role in common postconcussive symptoms due to its contributions to cognitive and emotional functions. In a sample of 122 combat veterans, we examined whether total cerebellum volumes differed among those with a remote history of mTBI with (n = 29) or without (n = 42) comorbid PTSD and healthy controls (n = 51). An automated cerebellum parcellation protocol was applied to T1-weighted anatomical scans to derive volumetric estimates of the cerebellum (and 28 subregions). Hierarchical regression analysis (adjusting for total intracranial volume, age, sex, and combat exposure) revealed that, compared with controls, participants with comorbid mTBI-PTSD had a significantly smaller volume of the total cerebellum (p = 0.010). There was no significant effect of mTBI-only on total cerebellum volume (p = 0.165). Follow-up exploratory analyses of subregional cerebellum volume differences suggested that volume differences in comorbid mTBI-PTSD were primarily localized to the posterior lobe (crus I, lobules VIIB, VIIIB). In sum, in a sample of combat veterans, mTBI was associated with a smaller volume of the cerebellum, but only when comorbid with PTSD. Consistent with recent work, exploratory subregional analyses indicated that volume differences were primarily attributable to regions of the cerebellum most prominently involved in cognition and emotion. These results underscore the profound effects of PTSD on brain health in military veterans and suggest that mTBI may not produce long-lasting structural damage to the cerebellum. Future work is needed, as it remains possible that subtle cerebellar volume changes may emerge in specific subgroups or as a function of injury-related factors (e.g., mechanism of injury, time since injury) not fully captured in the present study.
Introduction
Approximately 19–49% of military service members sustain a head injury during deployment, with most traumatic brain injuries (TBIs) classified as mild TBI (mTBI).1,2 mTBI is a brain insult from an external force that results in (typically temporary) impairment of cognitive, physical, or psychosocial function. Despite the expectation of full recovery following uncomplicated mTBI, 3 a history of mTBI is often associated with persistent cognitive impairment4,5 and/or chronic psychiatric distress, including post-traumatic stress disorder (PTSD),2,6 depression,1,7 and suicidal thoughts/behaviors.8,9 Notably, mTBI is associated with widespread structural brain changes to cortical gray and white matter and subcortical structures,10–13 which perhaps contributes to these persistent functional outcomes.
The cerebellum has recently emerged as a potential neural correlate of mTBI, as this region seems to be especially vulnerable to injury. 14 Long known for its role in orchestrating coordinated movements and maintaining balance, research has begun to illuminate the cerebellum’s contributions to diverse cognitive and affective processes.15–18 This is perhaps unsurprising, given the cerebellum is an anatomically complex and dense brain region. Specifically, the majority of the brain’s neurons are contained within the cerebellum, 19 which consists of a narrow, central column (vermis) and two lateral hemispheres divided into 10 lobules. Functionally, the cerebellum plays a central role in both cognitive and emotional processes,20–23 wherein cognitive functions are most prominently represented in lateral swaths of the posterior lobe16,24 and affective functions in the midline. 25
Considering how extensively the cerebellum supports cognition and emotion, it is possible that damage to the structural integrity of the cerebellum consequent to injury may explain many of the persistent difficulties TBI patients have in these domains.1,4 Indeed, structural, volumetric changes to the cerebellum have been observed after moderate-to-severe TBI.26–29 Recent work in pediatric samples has also revealed evidence of smaller cerebellum volumes following complicated mild to severe brain injury, particularly in the posterior lobe. 30 Yet, precisely how injury impacts cerebellum volumes after less severe forms of TBI remains unclear. Critically, human and animal models of mTBI injury suggest that—in addition to direct mechanical injury of the region—indirect damage to the cerebellum can result from these mechanical forces producing metabolic changes and Purkinje cell loss subsequent to presynaptic hyperexcitability. 31 In light of the high prevalence of mTBI,1,2 it is imperative to determine whether these injuries contribute to volumetric changes to the cerebellum to gain insight into veterans’ functional recovery following brain injury.
In combat veterans, however, brain injury is also deeply intertwined with psychological trauma. PTSD and mTBI are marked by profound neurobiological overlap, with both disorders characterized by disruption of neural circuits involved in emotion regulation and higher-order cognition.32,33 Clinically, this manifests in many shared features and symptoms across mTBI and PTSD, including executive dysfunction,34,35 emotion dysregulation,36,37 mood disruption,7,38 and sleep disturbance.39,40 Recent evidence has revealed prominent links between PTSD and smaller cerebellar volumes 41 ; however, it remains unclear whether mTBI exerts independent effects on the cerebellum, above and beyond PTSD. Comorbid mTBI-PTSD is also associated with poorer clinical outcomes and greater effects on cortical gray matter compared with singular diagnoses of mTBI or PTSD13,42; thus, disentangling potentially dissociable or exacerbating effects of mTBI on the brain is likely to point to improved pathophysiological models and better treatment outcomes.
To this end, the current study aimed to unpack the potentially unique effects of mTBI on cerebellar volumes in a sample of 122 combat-exposed military veterans with a remote history of mTBI, with or without current PTSD. We hypothesized that, compared with veterans without a history of brain injury, both comorbid mTBI-PTSD and mTBI-alone groups would have smaller cerebellum volumes. Notably, our inclusion of a non-PTSD mTBI group enabled us to directly test whether any observed volume differences could be attributed to a history of brain injury independent of PTSD. Due to the limited extant evidence for mTBI’s effects on cerebellar structure, our primary analyses focused on total cerebellar volumes; however, in follow-up, we conducted exploratory analyses to examine whether the effects of mTBI and/or mTBI-PTSD could be localized to specific cerebellar subregions. Based on recent work in PTSD, 41 we expected that comorbid mTBI-PTSD would be associated with smaller volumes of several lobules in the vermis and posterior lobe (e.g., lobule VIIB) compared with controls. We did not have specific subregion hypotheses for differences between the mTBI only and control groups. In addition, combat veterans are frequently exposed to blasts whose percussive forces may result in subtle neurological damage that accumulates over time, even if the acute injury does not meet clinical diagnostic thresholds for mTBI.43,44 Although emerging research strongly suggests that repetitive head impacts (below the clinical threshold of mTBI) can result in persistent changes to brain structure and neuropsychological functioning,45,46 in general, the neurobiological effects of this exposure are poorly understood. In our sample, many veterans were exposed to repetitive blast injuries (but did not have any history of mTBI based on acute symptom presentation). Thus, we followed up our total cerebellum analysis by repeating our primary analyses by subdividing the control group into those with a history of repetitive blast exposure (RBE) but no mTBI and those without any reported head injury.
Methods
Participants
Veterans were recruited from the VA Mid-Atlantic Mental Illness Research, Education, and Clinical Center (MIRECC) postdeployment mental health repository. 47 Eligible participants were between the ages of 18 and 65 years old, served during or after September 11, 2001, fluent in English, and capable of providing informed consent. As part of the current study, 162 veterans were recruited to complete a structural MRI of the brain and clinical and self-report assessments of TBI and PTSD. Participants were excluded for missing/incomplete PTSD assessments (n = 9), TBI assessments (n = 4), or MRI scans (n = 14). Participants were also excluded for failed/poor cerebellar parcellation (n = 9). Several subjects inadvertently participated in the study more than once (n = 4); for these individuals, only data from their first visit were retained for analysis. This resulted in an analyzable sample of 122 participants. Study procedures were approved by the Institutional Review Boards at Duke University Medical Center and Durham VA Medical Center.
Image acquisition and processing
Scanning was conducted on a GE Discovery MR750 3.0 Tesla MRI scanner, and T1-weighted anatomical images were acquired using a 3D Fast Spoiled Gradient-Recalled (FSPGR) sequence (repetition time [TR]/echo time [TE] = 7.53/2.9 ms, flip = 12°, FOV = 240 mm, 256 × 256 × 162 matrix, 1 mm slices). The ENIGMA cerebellum volumetric pipeline 48 —based on the Automatic Cerebellum Anatomical Parcellation using U-Net with Locally Constrained Optimization (ACAPULCO)—was applied to high-resolution T1-weighted anatomical scans. 49 This automated procedure parcellated the cerebellum into 28 anatomical regions, including bilateral hemispheric lobules (I-III, IV, Crus I, Crus II, VI, VIIB, VIIIA, VIIIB, IX, X), vermal lobules (VI, VII, VIII, IX, X), and the corpus medullare (see Fig. 1). Images were corrected for intensity inhomogeneity using N4, blurred with a 3D Gaussian kernel (SD = 3 mm) and transformed to Montreal Neurological Institute (MNI) template space. The segmentation protocol was followed by visual inspection of cerebellar segments for quality control purposes.41,48 Consequently, each subject’s segmentation was scored by a minimum of two trained raters on a scale from 1 (good) to 3 (poor/failed). In the event of a discrepancy between raters, the parcellation was examined by a third rater to reach consensus. Subjects with a three rating (n = 9) were excluded from all analyses. Examples of representative scans of different quality ratings are included in Supplementary Data.
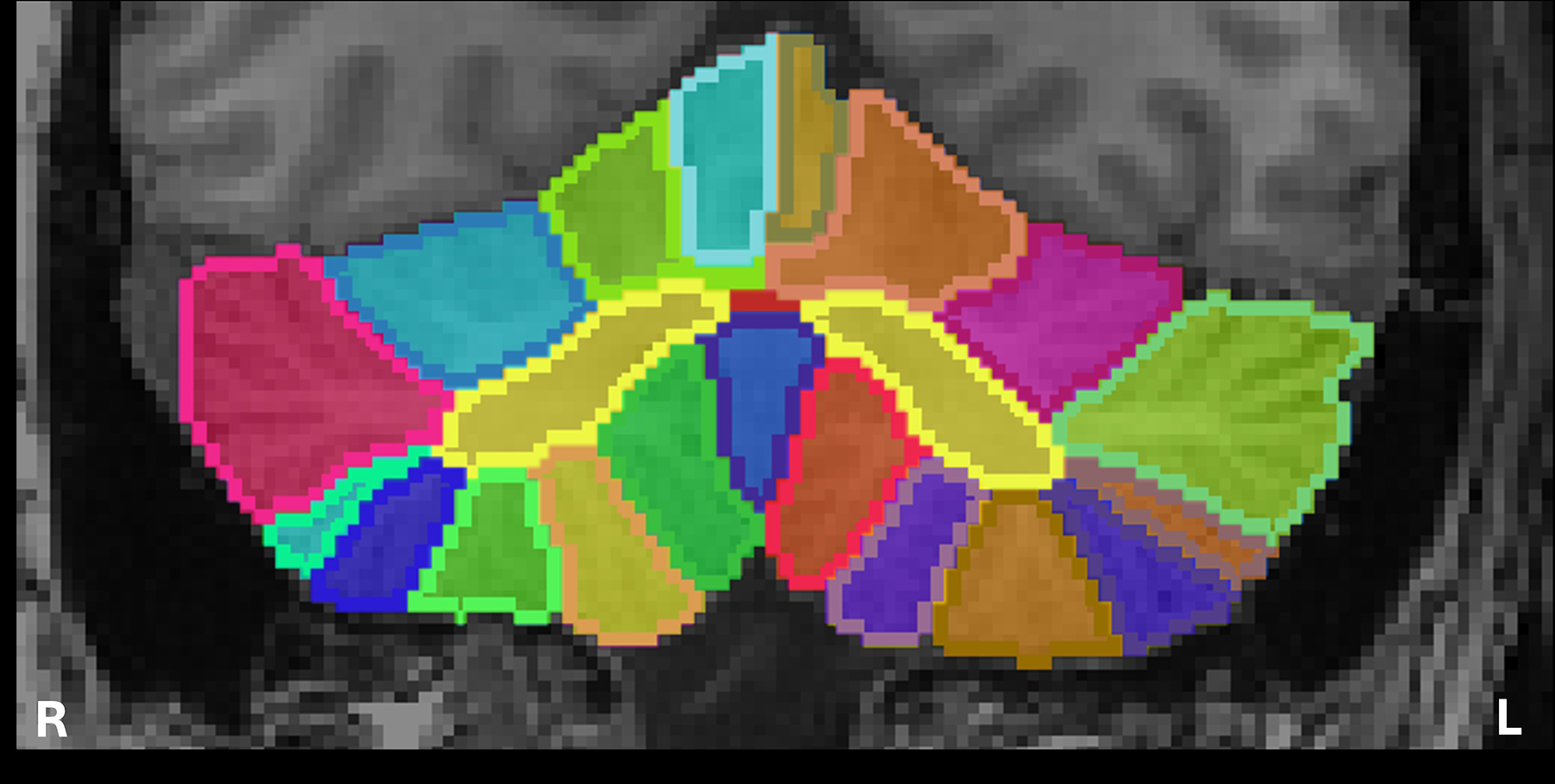
Example of cerebellum parcellation output mask from Automatic Cerebellum Anatomical Parcellation Using U-Net with Locally Constrained Optimization (ACAPULCO). Mask is presented in subject-space in coronal orientation. ACAPULCO produces a measurement of total cerebellum volume, along with estimates for 28 subregions.
TBI assessment
History of mTBI was measured using the Quantification of Cumulative Blast Exposure (QCuBE), 50 a semistructured interview used to assess the presence and severity of TBI, with an emphasis on blast-related exposures. The QCuBE provides a detailed assessment for up to five individual blast exposures, rank-ordered by severity. Blast-relevant details, including device type, tamping forces, distance from the blast, context of the explosion, and acute neurobehavioral (i.e., postconcussive) symptoms, were also collected. In addition, we assessed the history of nonblast mTBIs (i.e., blunt force/impact) veterans may have experienced from combat exposure or other circumstances (e.g., motor vehicle collision, assault, sports injury, fall), with up to five impact-related events evaluated in order of severity.
Consistent with criteria established by the American College of Rehabilitation Medicine 51 and the Veterans Administration/Department of Defense Clinical Practice Guideline for Management of Concussion and Mild Traumatic Brain Injury, 52 mTBI was defined as any blast- or blunt force-/impact-related injury to the head that resulted in immediate manifestation of (1) loss of consciousness less than 30 min; (2) alteration of consciousness/mental state, for example, confusion, disorientation, slowed thinking, up to 24 h; and/or (3) post-traumatic amnesia less than 24 h. Participants who endorsed multiple combat-related blast exposures without accompanying signs or symptoms of mTBI were designated as having RBE.
Available data for the current study reported diagnostic status (i.e., mTBI, RBE, or control). Detailed characteristics about head injury exposure from the QCuBE are reported for a subset of participants in Supplementary Table S1.
PTSD assessment
Current and lifetime PTSD diagnosis and severity were assessed using a semistructured clinical interview, the Clinician-Administered PTSD Scale (CAPS-5 53 ). Diagnostic interviews were administered by trained research staff. The CAPS-5 is considered the “gold standard” in the assessment of PTSD, demonstrating high internal consistency and good test–retest reliability.
Grouping
Veterans were categorized into non-mTBI, non-PTSD controls (n = 51), mTBI (n = 42), and comorbid mTBI-PTSD (n = 29) groups. A binary classification was used to group those with (1+ event) or without (0 events) a history of mTBI. Notably, individuals in all groups, including the control group, may have been exposed to noncombat blasts during training exercises; virtually all military personnel are exposed to noncombat blasts during basic training or other training exercises and therefore could not feasibly be excluded.
Exploratory analyses further subdivided the non-mTBI, non-PTSD control group into participants with or without RBE. The RBE category (n = 26) was assigned to veterans who reported blast-related head injury exposure without acute signs or symptoms that met criteria for mTBI. 54 The remainder of the control group (n = 25) reported no history of either mTBI or RBE.
Additional clinical and sociodemographic covariates
Outcomes from the following clinical assessments or self-reported measures were examined and/or included as covariates in the analyses. Veterans completed the Beck Depression Inventory–II (BDI-II 55 ), the Alcohol Use Disorders Identification Test, 56 the Combat Exposure Scale (CES 57 ), and the Brief Symptom Inventory (BSI 58 ) to measure self-reported depression, alcohol use, combat exposure, and global psychological distress, respectively.
Analytic strategy
Data were analyzed using R Version 4.3.1 using an alpha level of 0.05 for all statistical tests. We employed a stepwise hierarchical regression to examine differences in total cerebellum volume based on a three-level mTBI group classification: mTBI-only, comorbid mTBI-PTSD, and non-mTBI, non-PTSD controls. Covariates—including intracranial volume (ICV), age, sex, and combat exposure—were controlled for in step 1. Continuous covariates were mean-centered. Participants with missing CES data (n = 5) had their scores mean-imputed. Next, mTBI group was entered in step 2, with the control group as the reference. Models were compared using Analysis of Variance (ANOVA) to assess for significant change from step 1 to step 2.
Exploratory analyses examined the effects of (1) mTBI group status on subregional cerebellum volumes and (2) RBE on total cerebellar volumes. Regressions were modified from those described above but included the same covariates. To test subregional specificity, we replaced the original dependent variable (total volume) with each of the 28 cerebellar subregion volumes. To test for potential effects related to RBE, we substituted the mTBI grouping variable with a new four-level grouping that separated the controls into those with RBE (n = 26) and those without (n = 25). Prior research suggests that effects of PTSD 41 and (complicated) mTBI 30 are quite small; in the context of our small sample size (N = 122), we did not correct for multiple comparisons in these exploratory analyses and intended them to support prior findings and inform future, more well-powered work examining the cerebellum in mTBI and PTSD.
Results
Participant characteristics
Sample characteristics are reported in Table 1. Correlations among variables of interest are reported in Table 2. Chi-square tests were used to test whether mTBI groups differed in categorical variables. There was a significant difference in sex between groups, χ2 = 8.888, df = 2, p = 0.012, with more female veterans in the control group. A series of ANOVAs compared continuous sample characteristics between mTBI groups. Groups significantly differed on the CES, F(2,119) = 30.74, p < 0.001; comorbid mTBI-PTSD and mTBI-only participants both reported significantly more combat exposure compared with controls (p < 0.001) but did not significantly differ from each other (p = 0.109). There was also a significant difference in symptom severity scores on the CAPS-5, F(2,119) = 104.40, p < 0.001; BDI, F(2,119) = 37.35, p < 0.001; and BSI, F(2,119) = 28.52, p < 0.001. Comorbid mTBI-PTSD participants reported significantly higher PTSD (p < 0.001), depression (p < 0.001), and BSI (p < 0.001) symptom severity compared with both control and mTBI-only groups. Participants with mTBI-only also reported significantly higher PTSD (p = 0.016) and depression (p = 0.019) severity—but not neurobehavioral symptoms (p = 0.363)—compared with controls.
Sample Demographics (N = 122)
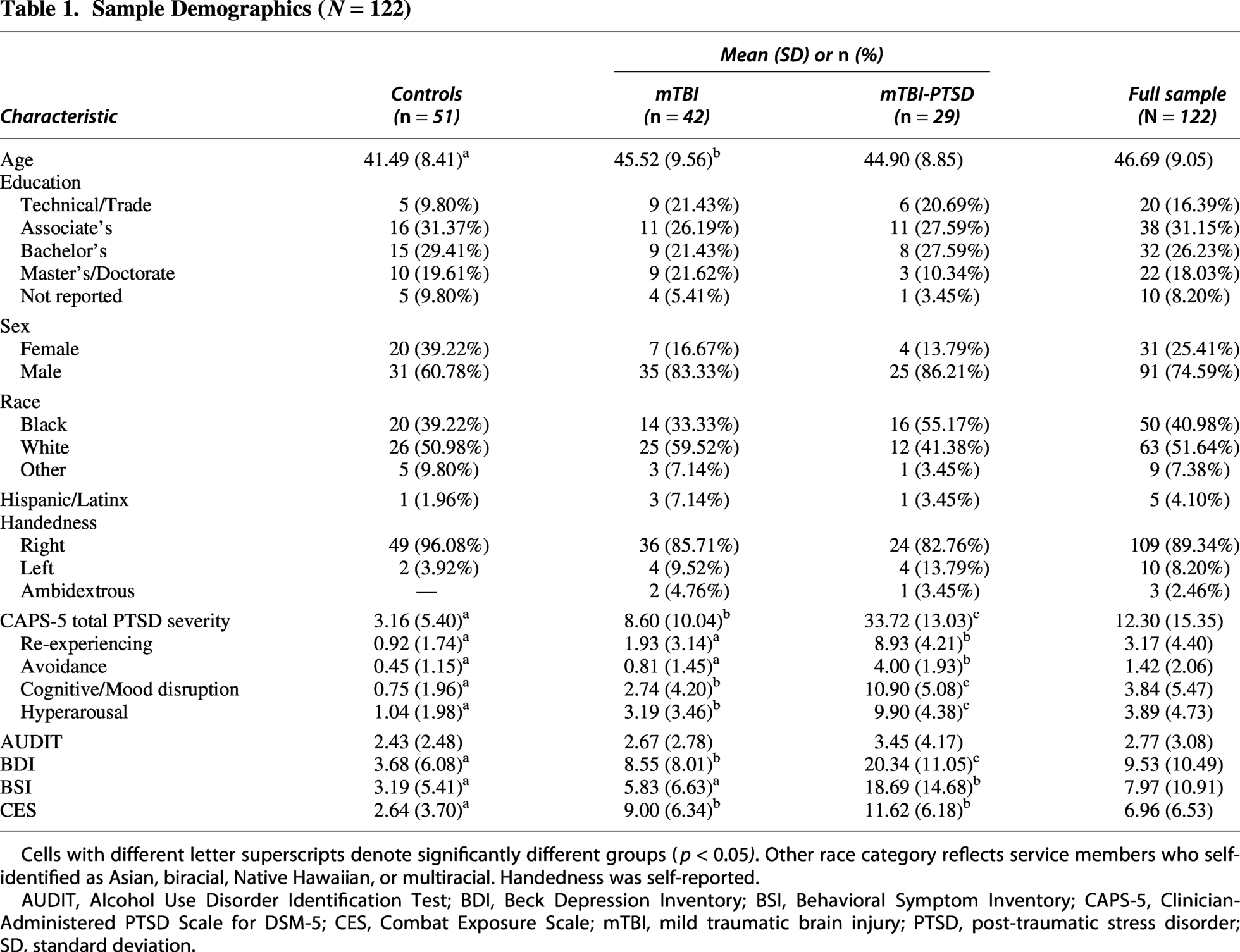
Cells with different letter superscripts denote significantly different groups (p < 0.05). Other race category reflects service members who self-identified as Asian, biracial, Native Hawaiian, or multiracial. Handedness was self-reported.
AUDIT, Alcohol Use Disorder Identification Test; BDI, Beck Depression Inventory; BSI, Behavioral Symptom Inventory; CAPS-5, Clinician-Administered PTSD Scale for DSM-5; CES, Combat Exposure Scale; mTBI, mild traumatic brain injury; PTSD, post-traumatic stress disorder; SD, standard deviation.
Correlations Between Study Variables
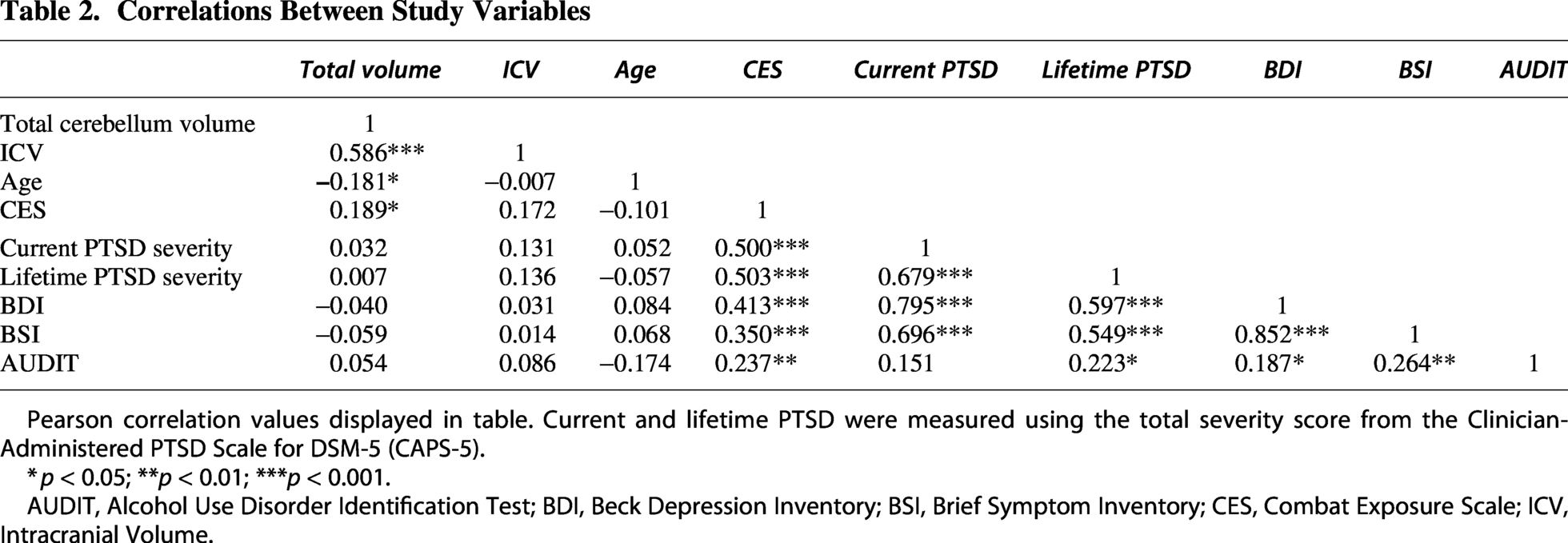
Pearson correlation values displayed in table. Current and lifetime PTSD were measured using the total severity score from the Clinician-Administered PTSD Scale for DSM-5 (CAPS-5).
*p < 0.05; **p < 0.01; ***p < 0.001.
AUDIT, Alcohol Use Disorder Identification Test; BDI, Beck Depression Inventory; BSI, Brief Symptom Inventory; CES, Combat Exposure Scale; ICV, Intracranial Volume.
Total cerebellum volume differences
Results of hierarchical linear regressions examining the effects of mTBI group on total cerebellum volume are reported in Table 3. Covariates were entered in step 1, with mTBI grouping added in step 2, resulting in a statistically significant model, F(6,115) = 13.83, adjusted-R2 = 0.389, p < 0.001. There was a significant increase in the model fit from step 1 to step 2 (model change F = 3.42, p = 0.036, R2 change = 0.035). Compared with controls, participants with comorbid mTBI-PTSD had a significantly smaller volume of the total cerebellum, b = −8108.59, SE = 3103.16, t = −2.613, and p = 0.010. There was no significant effect of mTBI-only on total cerebellum volume compared with controls (p = 0.165). Group differences in total cerebellum volume are plotted in Figure 2.
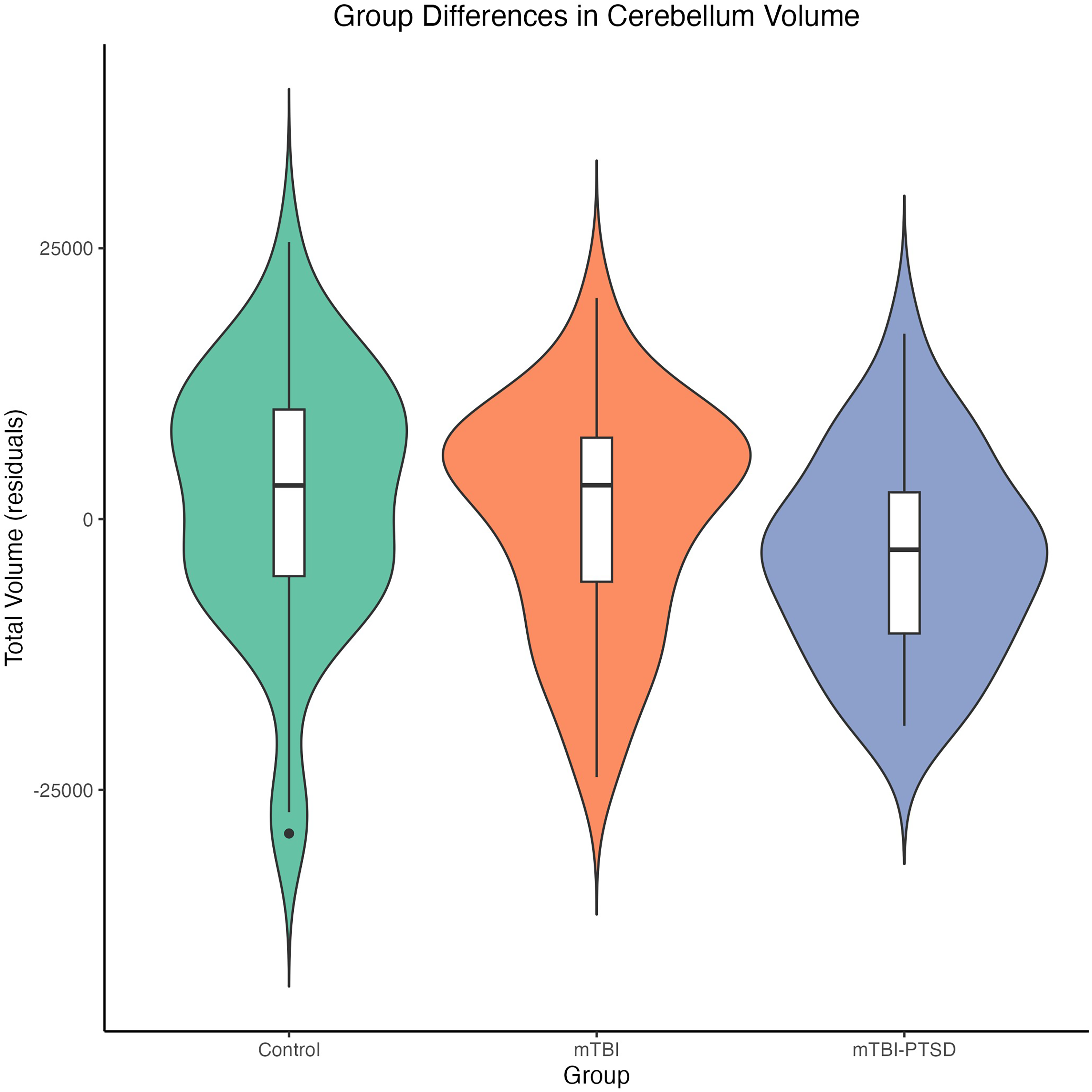
Group differences in total cerebellum volume. Violin plot depicts distributions of residualized total cerebellum volumes accounting for total intracranial volume, age, sex, and combat exposure between comorbid mTBI-PTSD (n = 29), mTBI-only (n = 42), and healthy non-mTBI, non-PTSD control (n = 51) groups.
Results of Hierarchical Regression Analyses for Total Cerebellum Volume Differences (N = 122)
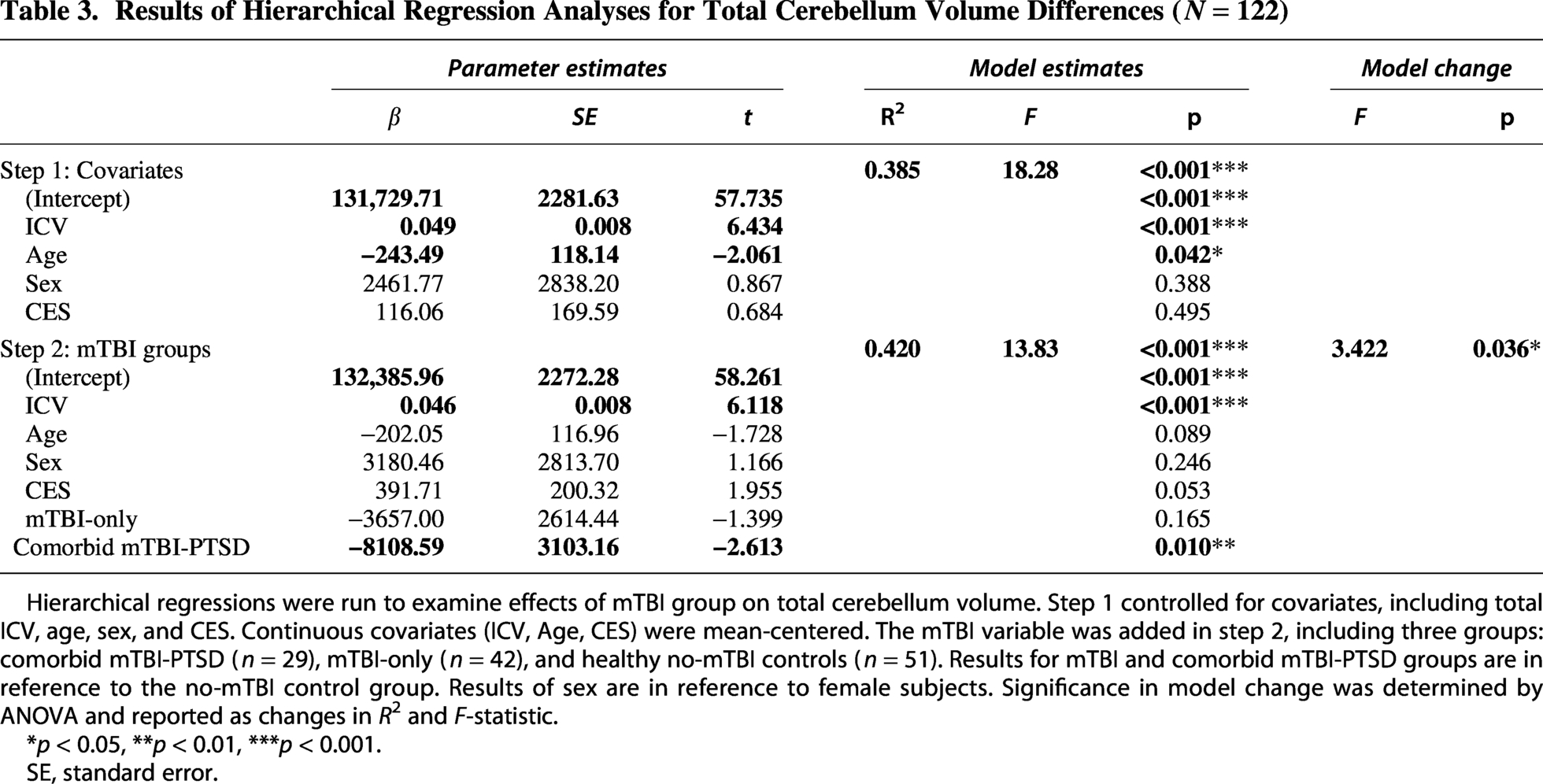
Hierarchical regressions were run to examine effects of mTBI group on total cerebellum volume. Step 1 controlled for covariates, including total ICV, age, sex, and CES. Continuous covariates (ICV, Age, CES) were mean-centered. The mTBI variable was added in step 2, including three groups: comorbid mTBI-PTSD (n = 29), mTBI-only (n = 42), and healthy no-mTBI controls (n = 51). Results for mTBI and comorbid mTBI-PTSD groups are in reference to the no-mTBI control group. Results of sex are in reference to female subjects. Significance in model change was determined by ANOVA and reported as changes in R2 and F-statistic.
*p < 0.05, **p < 0.01, ***p < 0.001.
SE, standard error.
Exploratory analyses examining RBE
Results of hierarchical linear regressions with a separate participant group for RBE are reported in Table 4. As in the primary analyses, after covarying for total ICV, sex, age, and combat exposure, participants with comorbid mTBI-PTSD had significantly smaller volume of the total cerebellum compared with controls, b = −8898.30, SE = 3680.47, t = −2.418, and p = 0.017. There were no significant differences in total cerebellum volume related to either the mTBI-only (p = 0.174) or RBE participant groups (p = 0.688).
Results of Exploratory Regression Analyses for Total Cerebellum Volume Differences Related to Repeated Blast Exposure (N = 122)
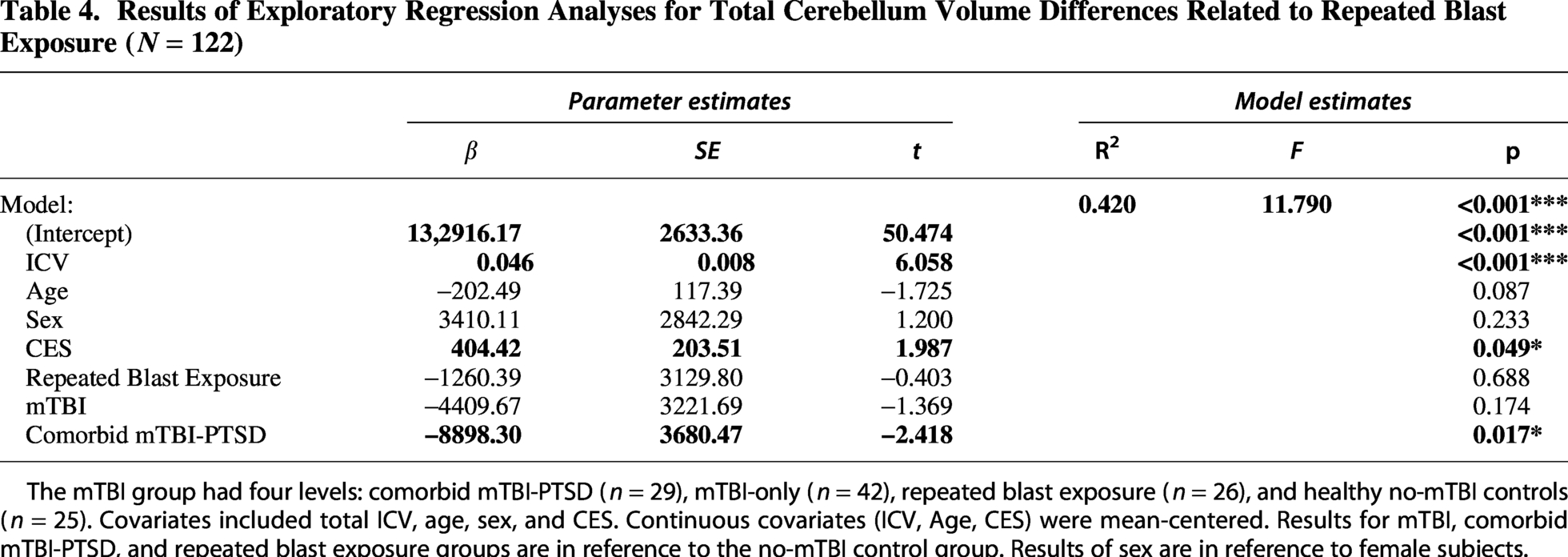
The mTBI group had four levels: comorbid mTBI-PTSD (n = 29), mTBI-only (n = 42), repeated blast exposure (n = 26), and healthy no-mTBI controls (n = 25). Covariates included total ICV, age, sex, and CES. Continuous covariates (ICV, Age, CES) were mean-centered. Results for mTBI, comorbid mTBI-PTSD, and repeated blast exposure groups are in reference to the no-mTBI control group. Results of sex are in reference to female subjects.
Exploratory analyses on all cerebellar regions
To explore whether mTBI and/or comorbid mTBI-PTSD were associated with localized volume reductions of the cerebellum, we performed a series of regressions on each cerebellar substructure to examine associations with the volumes of cerebellar subregions. After controlling for ICV, sex, combat exposure, and age, we found significant differences in several lobules including right lobule IV, bilateral crus I, left lobule VIIB, and left lobule VIIIB when comparing the comorbid mTBI-PTSD group to controls (uncorrected p < 0.05). The mTBI-only group was also associated with a smaller volume of right lobule IV (p-unc = 0.012). Results of these exploratory analyses are reported in Table 5.
Results of Exploratory Regression Analyses on Subregional Volume Differences in the Cerebellum (N = 122)
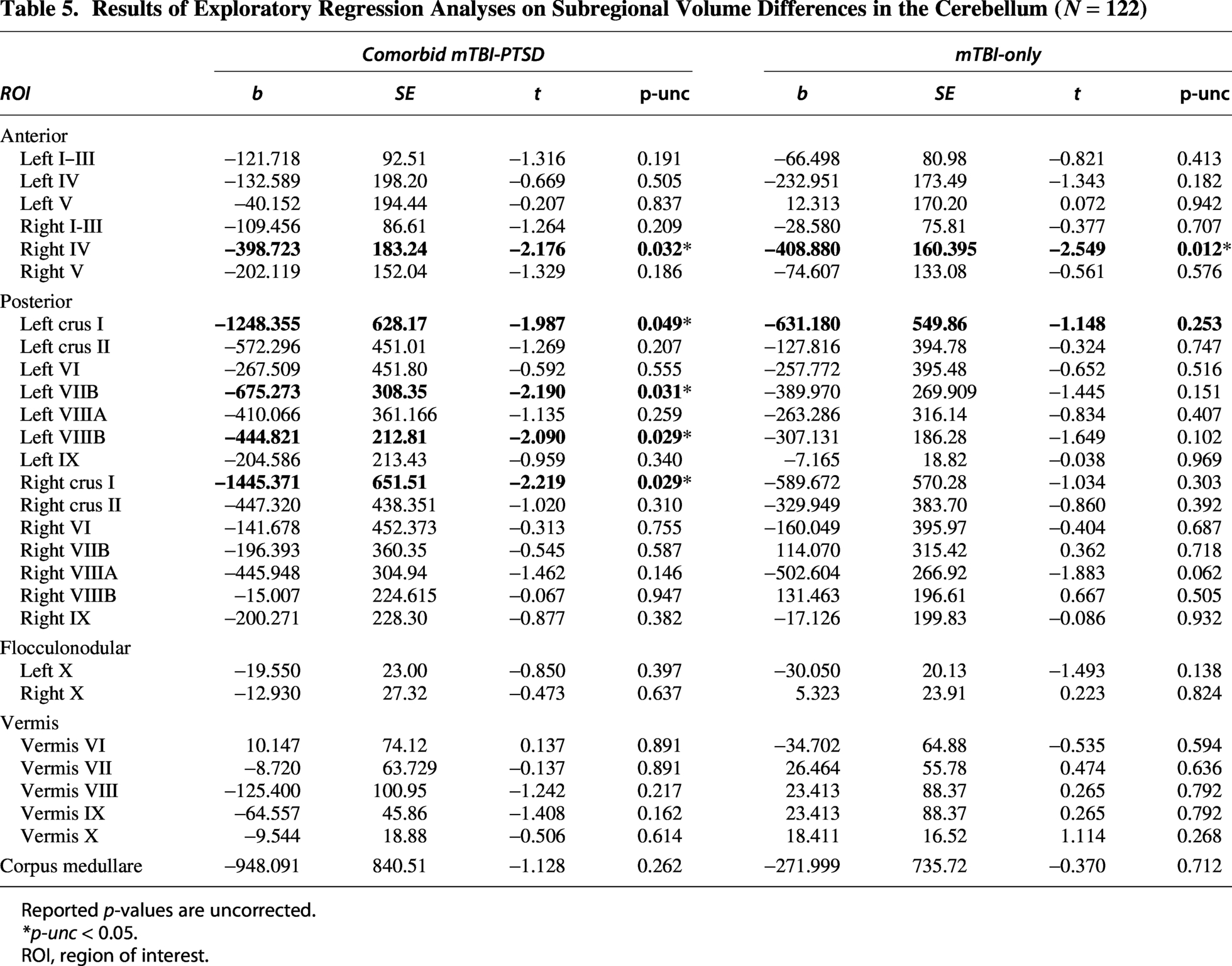
Reported p-values are uncorrected.
p-unc < 0.05.
ROI, region of interest.
Discussion
In a sample of combat-exposed military veterans, the current study found that a history of remote mTBI was associated with reduced cerebellum volume, but only when comorbid with PTSD. In the absence of PTSD, mTBI was not significantly associated with total cerebellum volumes. These results underscore the profound effects of PTSD on brain health in military veterans and suggest that mTBI alone may not produce long-lasting structural damage to the cerebellum.
Accumulating research has identified consistent alterations of the cerebellum in PTSD across both structural41,59,60 and functional brain metrics,61–63 consistent with our findings. Moreover, these studies have specifically implicated aberrancies in the posterior41,61 and vermal41,59 regions of the cerebellum. Similarly, here we found evidence for localization of cerebellum volume differences primarily in the posterior lobe (crus I, lobules VIIB, VIIIB) in our exploratory subregion analyses, building on prior work. As the most evolutionarily recent part of the cerebellum, 64 the posterior lobe is typically considered part of the “cognitive” cerebellum and has unique contributions to various cognitive processes such as working memory, abstract reasoning, and problem-solving.65,66 In prior research, 41 structural differences have also been observed in vermal lobules in patients with PTSD, perhaps for the role of the vermis in modulating emotional processing and regulation,17,67 including acquired fear responses68–71 at the center of established translational models of PTSD. 72 Together, these findings suggest that reduced volume of the cerebellum may contribute to the distressing and debilitating cognitive and affective symptoms that burden patients with PTSD.
In contrast to our hypotheses, though, mTBI alone was not associated with smaller total cerebellar volumes in the primary analyses. However, subtle cerebellar volume differences following remote mTBI cannot definitively be ruled out, particularly in the context of a relatively modest sample size, the expectation of small effect sizes in the chronic phase of brain injury, and the absence of a PTSD-only comparison group. It is notable that there remained no effect of mTBI-only even when compared with a control group that excluded veterans exposed to subclinical thresholds of brain injury, further underscoring the subtlety of any potential mTBI-related effects on cerebellar structure.
Together, these findings suggest the cerebellum may be resilient to mTBI and that impacts to cerebellar structure may only result from more severe brain injuries. Alternatively, these findings may reflect substantial heterogeneity in injury characteristics and recovery trajectories following mTBI. Factors such as mechanism of injury (e.g., blunt impact versus angular acceleration or blast-related forces), number of injuries, and time since injury may critically influence whether long-term alterations of the cerebellum emerge. For instance, there is evidence of persistent cerebellar structural damage following moderate-to-severe brain injury,26,27,29 and pre-clinical animal work has also previously illuminated atrophy of the cerebellar peduncles following TBI.29,73,74 Although exploratory subregional analyses suggested mTBI-only could be linked to a smaller volume of right lobule IV (part of the anterior lobe), this effect would not withstand stringent statistical correction (p-unc = 0.012) and should be interpreted with caution. Moreover, lobule IV was also implicated in the context of PTSD in the current study, limiting conclusions regarding mTBI-specific subregional effects. 41 Thus, much uncertainty remains regarding the consequences of mTBI on cerebellar structure.
It is exceptionally challenging to disentangle both the symptoms and neurobiological markers of chronic mTBI in veteran samples. For example, comorbidity between mTBI and PTSD (as well as other psychiatric symptoms and chronic pain) in combat veterans is the norm, rather than the exception.75,76 And even in single-diagnosis cases (i.e., patients without comorbid psychopathology), patients with a history of mTBI frequently endorse greater symptom severity across the board compared with veterans without mTBI. 77 This effect was evident in our own sample, wherein participants with history of mTBI (but not PTSD) reported more severe psychiatric symptoms, including PTSD and depression, compared with controls. Conversely, prior work has also shown that psychiatric patients who have never had a head injury also frequently report concussive symptoms upon self-report.78,79 In addition to high comorbidity, there is profound symptom overlap between mTBI and PTSD as both disorders share features of cognitive impairment and emotional disturbance,32,33 posing further challenges for both clinical care and research. Thus, characterizing symptoms and tracing them to a particular cause is, to say the least, difficult.
Some of these challenges may be partially resolved through careful, thorough assessment of patients’ symptoms and their possible etiologies, which will always be an integral component of patient care (particularly in veteran populations frequently exposed to repeated psychological and head trauma). Identifying dissociable biological correlates of mTBI and PTSD, though, may prove to be a valuable tool in identifying root causes of symptoms and thus point to more targeted, efficient interventions. The current findings, for example, observed smaller cerebellum volumes only in veterans who had a comorbid diagnosis of PTSD along with their history of mTBI. Previous neuroimaging studies have often pointed to similar neural correlates between mTBI and PTSD, 33 but it seems the cerebellum may be uniquely impacted by PTSD. Identifying dissociable neurobiological correlates of mTBI and PTSD is likely to be advantageous, as brain-based markers could be considered more objective measures of assessment (and thus not be subject to patients’ reports that may miss or contain details that bias clinical impressions of patients’ symptoms and histories). When making treatment decisions, this could be especially valuable in the context of highly comorbid and often nonspecific symptoms frequently endorsed by both mTBI and PTSD patients.80,81 It is imperative for research to continue illuminating both shared and unique markers of mTBI and PTSD to support more effective interventions for combat veterans receiving care.
Overall, though, much more targeted evaluation of neurobiological sequelae of head injury is needed to improve outcomes, as these injuries are highly heterogeneous. For instance, RBE is common in Operation Enduring Freedom (OEF)/Operation Iraqi Freedom (OIF) veterans and thought to kindle neurological damage over time.46,82 In exploratory analyses, there were no significant effects of RBE on cerebellar volumes. Considering there was no significant effect of mTBI-only in the primary analysis, this is perhaps unsurprising. RBE, though, has previously been linked to subtle neuroanatomical changes, particularly in the brain’s white matter microstructure.44,83 As neither mTBI nor RBE was associated with cerebellar volume, it may be that milder forms of brain injury do not exert observable macro-level changes in the cerebellum. This finding is consistent with the generally excellent clinical prognosis for complete and timely recovery from uncomplicated mTBI. 3 However, as mTBI is, by far, the most common form of brain injury in combat veterans, future research must continue delineating its neurobiological consequences. Future work, for instance, is needed to probe how RBE or mild brain injury impacts the cerebellum, as repeated head injuries could contribute to neuropathological changes over time. Other features of head injury—such as time or mechanism of injury—could have consequences for the cerebellum. The nature of the TBI assessment used in this study unfortunately precluded us from a more nuanced or dimensional characterization of brain injury. Moving forward, studies should aim to more eloquently investigate how various injury-specific factors (as well as psychological symptoms) relate to the structure and function of the cerebellum to better understand (and perhaps prevent or treat) negative outcomes of mTBI.
Limitations
There are several important limitations of this work. First, although our findings suggest that smaller volume of the cerebellum may be a unique feature of PTSD, all PTSD patients in the study had a history of mTBI. While we would hypothesize that a PTSD-only patient group would also exhibit smaller cerebellum volumes, 41 we were unable to test this empirically given the composition of our sample. Considering comorbid mTBI-PTSD is linked to poorer clinical outcomes compared with either mTBI or PTSD alone, 42 it is important for future work to examine whether cerebellum volume reductions in PTSD may be exacerbated for patients with a history of mTBI. In addition, our use of cross-sectional data limits our ability to make causal inferences; future work employing prospective, longitudinal designs is needed to assess whether smaller cerebellum volumes might predict risk for PTSD or if they are a consequence of chronic psychiatric symptoms. Such designs may also help improve our understanding of the functional correlates of the cerebellum in clinical samples, including how volumetric changes of this region correspond to changes in cognition and emotional functioning. In addition, the current findings may also not be generalizable to nonveteran samples, yet mTBI also frequently co-occurs with trauma exposure in civilian samples (such as motor vehicle collisions or physical assaults). There are also many additional characteristics of mTBI (such as mechanism of injury, features of blast exposure [e.g., distance]) that we were unable to assess in this study. Future studies leveraging continuous, item-level measures of blast exposure in larger samples will be critical for evaluating potential dose–response relationships between blast intensity, cumulative exposure, and cerebellar structure. Lastly, our sample size may have been insufficient to detect the small effects typically observed in PTSD and mTBI brain imaging studies.41,84 Our groups did also vary in several factors, further complicating our ability to determine the presence and strength of effects between mTBI, comorbid mTBI-PTSD, and control patients. Mega-analysis from data consortiums and multisite studies—including ENIGMA, 85 LIMBIC-CENC, 86 and TRACK-TBI 87 —will provide greater clarity and improve the generalizability of these findings.
Conclusions
In sum, comorbid mTBI-PTSD was associated with a smaller volume of the whole cerebellum in a sample of military combat veterans, though a history of mTBI, on its own, had no discernible effect on cerebellum volume. Overall, these findings are consistent with prior work demonstrating cerebellar alterations in PTSD, particularly in the posterior lobe, which may map on to the many cognitive and emotional features of the disorder. Despite the specificity of the current findings, brain injury remains a pressing health concern, as it is strongly linked to adverse cognitive and psychological outcomes for combat veterans. Understanding dissociable neurobiological correlates of PTSD and mTBI will illuminate the pathophysiology of these disorders and further efforts for targeted, effective treatments in the context of challenging comorbidity.
Transparency, Rigor, and Reproducibility
The analysis plan was not formally preregistered. The existing data included 162 subjects, and due to missing or incomplete data, only participants with complete data (N = 122) were included in analysis. Key inclusion criteria were based on information available in the repository and subsequent telephone screenings. All symptom reporting was based on self-report or clinical interviews, with all measures described earlier. All surveys and questionnaires used in the study are available from the authors and have demonstrated acceptable psychometric characteristics. Scanning was conducted on a GE Discovery MR750 3.0 Tesla MRI scanner, and T1-weighted anatomical images were acquired using a 3D FSPGR sequence. The ENIGMA cerebellum volumetrics pipeline was utilized to quantify local changes in cerebellar volume using structural MRI, and the ACAPULCO automated protocol was used to parcellate the cerebellum into 28 anatomical regions. Data were analyzed using R Version 4.3.1 using an alpha level of 0.05 for all statistical tests. Statistical results are reported using the beta coefficients, standard error, and t statistic where appropriate. No replication or external validation studies have been performed or are planned/ongoing at this time to our knowledge. Code for statistical analyses conducted via R can be obtained from the corresponding author (A.A.H.). The data that support these findings are available in deidentified format upon reasonable request from the corresponding author (A.A.H.) and permission of the VA Mid-Atlantic (VISN 6) MIRECC Workgroup. The authors agree to provide the full content of the article on request by contacting the corresponding author.
Authors’ Contributions
A.A.H.: Conceptualization, methodology, formal analysis, software, and writing (original draft; review and editing). B.S.M.: Conceptualization, methodology, formal analysis, writing (original draft; review and editing), and visualization. C.L.B.: Data curation, project administration, and writing (review and editing). A.H.: Data curation. A.N.C.: Data curation and writing (review and editing). Courtney Haswell: Data curation and software. Rajendra Morey: Supervision, funding acquisition, and writing (review and editing).
Footnotes
Acknowledgments
The VA Mid-Atlantic MIRECC Workgroup consists of the following: Pallavi Aurora, PhD; Patrick S. Calhoun, PhD; Eric Dedert, PhD; Eric B. Elbogen, PhD; John A. Fairbank, PhD; Tate F. Halverson, PhD; Robin A. Hurley, MD; Jason D. Kilts, PhD; Angela Kirby, MS; Anna T. Magnante, PsyD; Sarah L. Martindale, PhD; Christine E. Marx, MD, MS; Scott D. McDonald, PhD; Scott D. Moore, MD, PhD; Victoria O’Connor, PhD; Jennifer C. Naylor, PhD; Jared Rowland, PhD; Robert D. Shura, PsyD; Cindy Swinkels, PhD; Larry A. Tupler, PhD; and Elizabeth E. Van Voorhees, PhD.
Funding Information
One of the first authors (B.S.M.) was supported by the VA Mid-Atlantic (VISN 6) MIRECC and the Department of Veterans Affairs Office of Academic Affiliations Advanced Program in Mental Illness, Research, and Treatment. Research was supported by VA Merit Award I01 CX002293.
Disclaimer
The views, opinions, and/or findings contained in this article are those of the authors and should not be construed as an official Veterans Affairs position, policy, or decision, unless so designated by other official documentation.
Author Disclosure Statement
A.N.C. is a paid research consultant for Saint Vincent Hospital. The authors otherwise declare no conflicts of interest, financial or otherwise.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.