
Abstract
Falls are the primary cause of mild traumatic brain injury (mTBI) among older adults, yet limited research has examined patterns of clinical care, mobility, and subsequent fall risk in this population. The objective of this study was to evaluate outpatient physical or occupational therapy (PT/OT) referral patterns and assess physical function and fall risk status of older adults with mTBI. We analyzed acute care and 2-week post-mTBI assessment data from a prospective cohort study of adults aged 65 and older with mTBI treated at a level 1 trauma center and six affiliated hospitals 2023–2025 and meeting eligibility criteria. Of 625 that were confirmed eligible, 155 consented to participate in the study. Of these, five were missing the 2-week assessment and nine were missing PT/OT referral information, leaving 141 in the current study. The exposure of interest was referral to PT/OT at discharge, obtained from medical records. Two-week post-mTBI assessments included the Short Physical Performance Battery (SPPB) and the Four-Square Step Test (FSST). Statistical comparisons between exposure groups were made using Fisher’s exact test, Student’s t-test or the Wilcoxon rank-sum test. Participants (n = 141) were on average 76.1 (standard deviation 7.3) years old and 56.0% female. Falls were the primary cause of mTBI (89%). At the 2-week assessment, participants demonstrated poor physical performance: 53% had impaired SPPB (<10), 62% had impaired FSST (>15 sec), and 65% had slow gait speeds (<0.80 m/s), all indicative of elevated fall risk. Only 34 (24%) were referred to PT/OT at discharge. Those referred were more likely to have received an inpatient PT/OT consultation (97% vs. 22%, p < 0.001). Among participants not referred to PT/OT, 46% had impaired SPPB, 58% had impaired FSST, and 60% had slow gait speed, indicating high fall risk. Less than a quarter of older adults with primarily fall-related mTBI received any discharge PT/OT referral despite clear mobility and balance deficits. This critical gap in post-discharge rehabilitation underscores a disconnect between fall-prevention guidelines and clinical practice, leaving many older adults at high risk of recurrent falls and injuries.
Introduction
Older adults experience more traumatic brain injuries (TBI) than any other age group, with falls being the leading cause. Each year in the United States, over 2.8 million TBIs—ranging from mild to severe—result in emergency department visits, hospitalizations, or deaths, and 22% occur in adults aged 65 and older. 1 Among older adults, TBI incidence has risen by 7.2% annually over the past decade, the highest increase of any age group.1,2 Mild TBI (mTBI), characterized by brief loss of consciousness (LOC), post-traumatic amnesia, or neurological deficits,3–5 accounts for over 80% of TBI in older adults. 6 In contrast to younger adults where motor vehicle accidents and sports are the dominant mechanisms of TBI, over 79% of TBIs in older adults are a result of a fall.1,2
Falls not only cause most TBI but also increase mortality risk and the likelihood of recurrent falls, particularly in older adults with prior mTBI. 7 The best predictor of fall risk in older adults is having fallen within the past 12 months, which increases the risk of a future fall more than 4-fold. 8 For older adults with mTBI, this fall risk may be even greater based on the detrimental effects of mTBI on gait and balance that have been well-documented in younger adults. For example, mTBI decreases postural stability, gait speed, dual-task ability, and turning ability in young adults,9,10 and these changes are associated with increased fall risk in older adults.11,12 Recent empirical evidence supports this association; older adults with mTBI are at a 97% greater risk for future falls compared to matched peers without mTBI. 7 Since recurrent fallers (more than one fall over 12 months) have a 50–100% higher mortality risk than single fallers,13,14 effective care for older adults with mTBI should include interventions to reduce fall risk and prevent individuals from progressing from a single fall to recurrent falls.
Effective fall-prevention strategies exist, such as the U.S. Centers for Disease Control and Prevention Stopping Elderly Accidents, Deaths, & Injuries initiative, which emphasizes screening, risk assessment, and targeted interventions.11,15,16 Specifically, the world guidelines for fall prevention and management recommend screening for falls in the past 12 months, assessing previous fall severity, and assessing gait and balance impairments (i.e., gait speed < 0.8 m/s or timed up and go > 15 sec) to stratify people as low, intermediate, or high fall risk. 11 Subsequently, anyone classified as intermediate or high risk should receive tailored physical therapy interventions that focus on balance, gait, and strength. 11 Clinical trials confirm that this approach reduces falls in older adults, 17 but it is unclear if older adults with mTBI receive care consistent with these guidelines. Instead, TBI-based rehabilitation is biased towards severe TBI by emphasizing gaining independence and improving gross motor function.4,18 While older adults with fall-related mTBI should be considered high risk for future falls, the “mild” misnomer and lack of obvious motor impairments may make clinicians less likely to refer patients for further follow-up or treatment.19,20 Consequently, subtle deficits in the integration of the sensory information critical for postural control (vision, somatosensation, vestibular) or the muscle coordination used to control the body’s center of mass that can increase the risk for future falls may go untreated in older adults with mTBI.
Despite the high prevalence of mTBI among older adults, research on the allocation of clinical treatment, mobility, and fall risk in this population is scarce, as most studies focus on younger adults with moderate-to-severe TBI in inpatient rehabilitation settings.4,6,20,21
The objective of this study was to evaluate discharge referral patterns for outpatient rehabilitation (physical or occupational therapy [PT/OT]) in a cohort of older adults with mTBI to determine if consultations and referral patterns align with current fall prevention guidelines. We also explored clinical factors from the acute care episode and 2-week post-mTBI measures of physical functioning associated with PT/OT referral.
Methods
Study design and population
We analyzed acute care and 2-week post-mTBI assessment data from RETRO-TBI (ClinicalTrials.gov registration number NCT07569354), a prospective cohort study of older adult mTBI that enrolled its first participant in May 2023. RETRO-TBI conducts assessments at 2 weeks, 3 months, 6 months, and 12 months post-injury. Adults aged 65 years and older who were treated for mTBI within 72 h of injury at the R Adams Cowley Shock Trauma Center or at one of six affiliated University of Maryland Medical System Hospitals with 2-week data available at the time of analysis (October 2025) were eligible for the current study. Individuals evaluated in the emergency department or admitted to the hospital were eligible for RETRO-TBI. Consistent with American Congress of Rehabilitation Medicine diagnostic criteria, inclusion criteria were a history of head trauma with an admission Glascow Coma Scale (GCS) score of 13–14 or a GCS of 15 plus one of the following criteria: a period of observed or self-reported transient confusion, disorientation, or impaired consciousness; LOC ≤30 min; post-traumatic amnesia <24 h; or CT positivity. 3 Individuals with GCS <13, LOC >30 min, post-traumatic amnesia ≥24 h, pre-existing dementia, no permanent address or phone number, living >55 miles from the trauma center, who did not speak English or would not be ambulatory at 2 weeks post-TBI were excluded.
Selection of participants
Enrollment for RETRO-TBI proceeded as follows. Participants evaluated in the trauma center or emergency room and meeting study criteria were offered an informational pamphlet on the study by trauma center research assistants and were told that they could refuse participation immediately, contact the study coordinator directly for more information, or wait for the study coordinator to contact them, typically within 48 h. Participants admitted to affiliated hospitals with possible TBI were identified using International Classification of Disease, version 10 codes based on the Centers for Disease Prevention and Control surveillance definition 22 and screened for study inclusion using information in the medical record. These participants were mailed an informational pamphlet and phoned 6 days later to confirm inclusion criteria and determine interest. All participants provided their own written informed consent at the 2-week assessment and were given a $50 gift card. This study was approved by the University of Maryland School of Medicine Institutional Review Board (HP-00100973).
Measurements
RETRO-TBI obtains information on PT/OT consultations while in the emergency department or inpatient wards, PT/OT post-discharge referrals, and discharge location from the participant’s medical record after enrollment into the study. Information on LOC, GCS, and whether the visit resulted in a hospital admission is collected using a standard form from the medical record when available. Demographic and social variables are obtained via self-report at the 2-week assessment. TBI history is obtained using a modified version of the Ohio State University TBI Identification Method. 23 CT scans are conducted during the TBI admission visit according to the protocol of the hospital where they occurred. CT positivity is obtained from the radiologist report of the first CT scan during the acute TBI episode.
In addition to clinical information, RETRO-TBI collects physical performance measures of gait and balance at the 2-week assessment post-mTBI. RETRO-TBI maintains strict quality control protocols with two independent checks quarterly. Extreme or unexpected values are flagged and corrected at data entry. Unexpected values making it through this process are corrected if possible or set to missing if not. The Four-Square Step Test (FSST) was used to assess dynamic balance and coordination. The FSST is a timed test of multidirectional stepping motions requiring participants to step over canes forming four quadrants on the floor in a specific order and without touching a cane. The FSST quickly assesses the ability of an individual to dynamically maintain an upright posture while changing directions and weight shifting and has excellent predictive ability to identify individuals at risk of falls. 24 In older individuals without neurological disorders, scores >15 sec have been found to be valid predictors of falls.25,26 The Short Physical Performance Battery (SPPB) was used to assess lower extremity function. The SPPB measures balance, repeated chair stands, and a timed 4-meter walk and is associated with disability and mortality in older adults. 27 It ranges from 0 to 12 with lower scores indicative of increased dysmobility and scores <10 associated with increased fall risk. 27 Self-selected 4-m gait speed was extracted from the SPPB as an independent measure of physical performance. Slow gait speed has been linked to fall and mortality, with the latest world guidelines for falls prevention and management establishing a cut-off of 0.80 m/s as indicating impaired gait with increased fall-risk. 11
Analysis
We inspected all variables for missingness, distribution, outliers, and implausible values. Continuous values were described using means, standard deviations, medians, first quartiles, and third quartiles. Categorical values were described using frequencies and percentages.
To evaluate referral patterns for outpatient rehabilitation (physical or occupational therapy), we calculated the proportion of RETRO-TBI participants who received PT/OT referrals. We then stratified our sample into two groups based on referral status and compared demographic, clinical, and social variables using Fisher’s exact test for categorical variables and Student’s t-test for age (Table 1). Next, we compared measures of physical performance from the 2-week assessment between groups using Fisher’s exact test for categorical variables and the Wilcoxon rank-sum test for continuous variables (Table 2). All statistical analyses were conducted using Stata MP Version 17.
Characteristics of Adults Aged 65 and Older Treated for Mild Traumatic Brain Injury (TBI), by Referral to Physical and/or Occupational Therapy (PT/OT) at Discharge from Care, n = 141
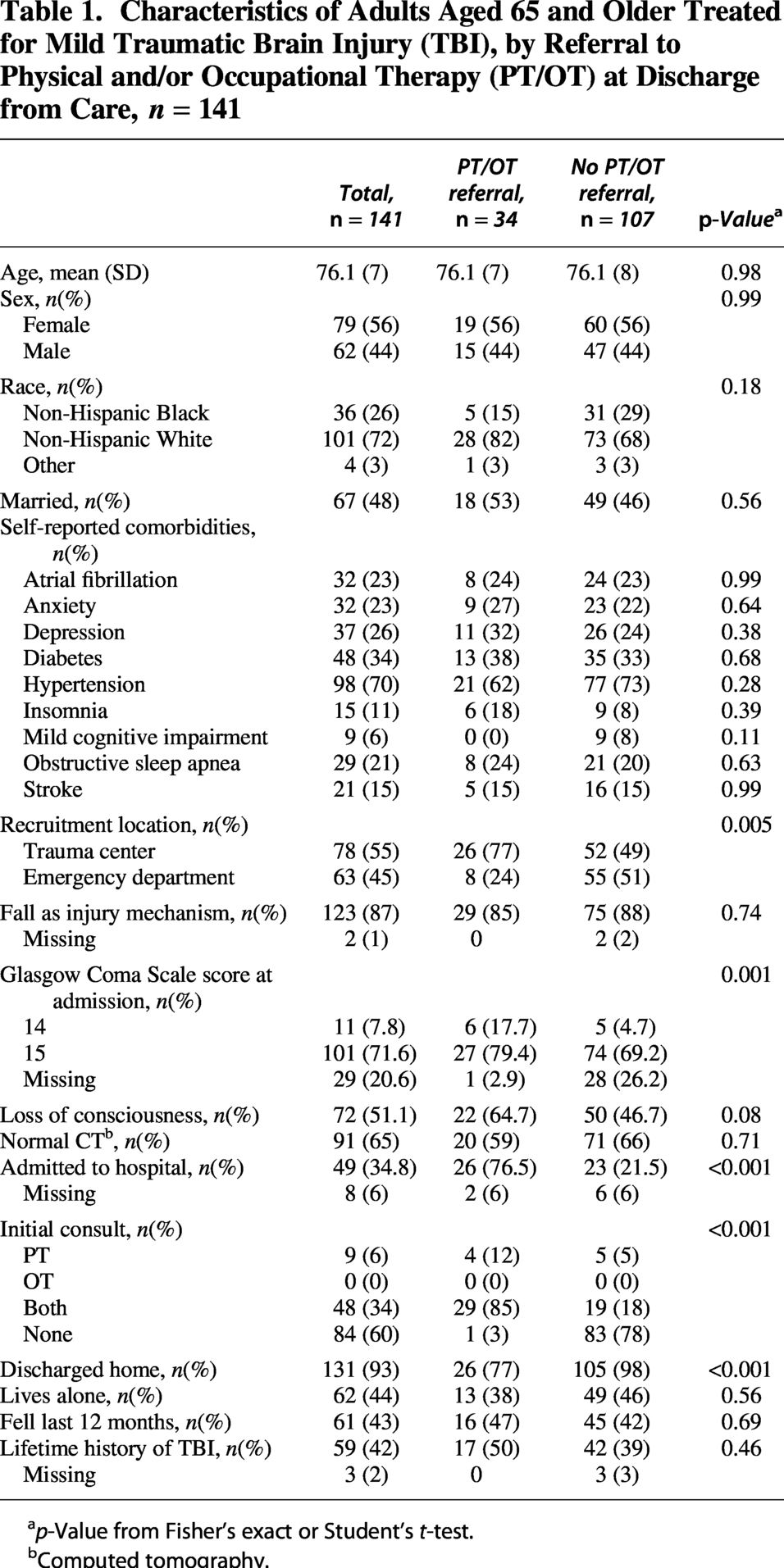
ap-Value from Fisher’s exact or Student’s t-test.
bComputed tomography.
Two-Week Post Mild Traumatic Brain Injury Assessments of Adults Aged 65 and Older Treated for Mild Traumatic Brain Injury, by Referral to Physical and/or Occupational Therapy (PT/OT) at Discharge from Care, n = 141
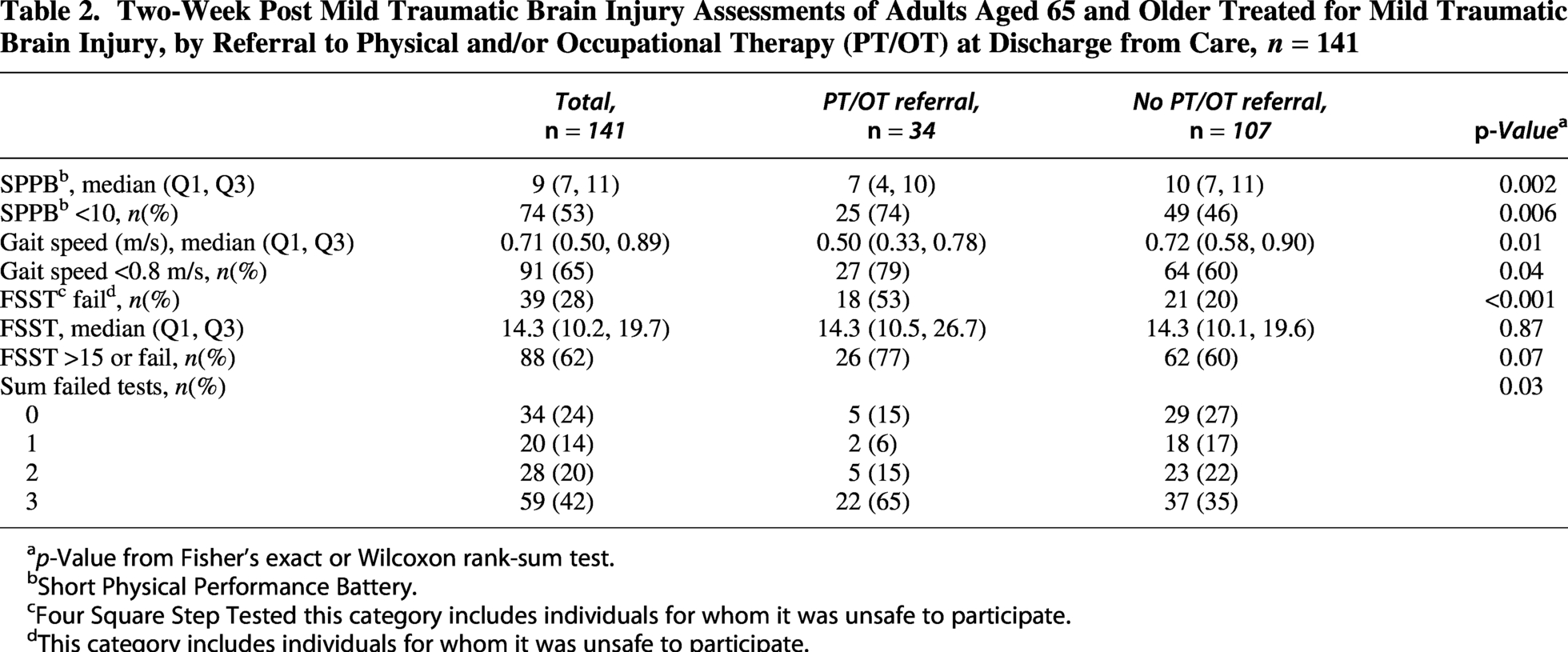
ap-Value from Fisher’s exact or Wilcoxon rank-sum test.
bShort Physical Performance Battery.
cFour Square Step Tested this category includes individuals for whom it was unsafe to participate.
dThis category includes individuals for whom it was unsafe to participate.
Results
We screened 1,460 older adults with possible TBI for eligibility. Of these, 625 were confirmed eligible (324/625 from the trauma center), and 155 consented to participate (25% of eligible participants). Of 155 RETRO-TBI participants, 5 were missing the 2-week assessment, and 9 were missing discharge PT/OT referral information, leaving 141 in the current study. Of the 141, 5 (4%) completed the 2-week assessment in a rehabilitation facility. Participants were 56% female and 72% non-Hispanic White with an average age 76.1 (SD 7) years (Table 1). The majority had a GCS of 15 (71.6%), with 29 (20.6%) missing GCS and 51.1% reported LOC. CT scans were negative for 64%, and 35% were admitted to hospital. The primary cause of TBI was a fall (89%), and most participants were discharged home (93%). Falls in the last year were reported by 43%, and prior history of TBI was reported by 43%. Small amounts of missing information are noted in Table 1.
Participants demonstrated poor physical performance at 2-weeks post-injury (Table 2). Based on self-reported dizziness or inability to perform tasks, or investigator discretion, nine participants (6%) were deemed unsafe to participate in the FSST and SPPB. These individuals were placed in the high fall risk group for FSST, SPPB, and gait speed. The median (interquartile range [IQR]) SPPB score of 9 (7, 11) indicated poor physical performance, with 53% falling below a score of 10, indicating increased fall risk. A large number (28%) failed the FSST (i.e., were unable to complete or touched a cane), and among the completers, the median (IQR) time to complete was 14.3 (10.2, 19.7) seconds. Including those who could not complete the test, 62% of the sample fell above established FSST cutoffs (>15 sec) for high fall risk. The median gait speed was 0.71 (0.50, 0.89) m/s, with 65% having gait speeds <0.80 m/s, indicating increased risk for falls, morbidity, and mortality. Among those who fell above the cutoff or failed the FSST (n = 88), 59 (67% of 88) also fell below the SPPB and gait speed cutoffs. Only 34 (24%) participants had normal function based on exceeding fall-risk thresholds across all three physical performance tests, and of these, 27/34 (79%) incurred mTBI as a result of a fall.
Among the 141 participants, 34 (24%) were referred to PT/OT at discharge (Table 1). Among those who were in a rehabilitation facility for the 2-week assessment, 5/5 (100%) were referred to PT/OT at discharge from acute care. Few differences in baseline characteristics by PT/OT referral status achieved statistical significance. Individuals referred to PT/OT were more likely to have been recruited from the trauma center (77% vs. 49%, p = 0.005) and admitted to the hospital (77% vs. 22%, p < 0.001) than those without an PT/OT referral. Normal CT scan did not differ between groups (63% vs. 70%, p = 0.51). Notably, the proportion of participants who experienced mTBI as a result of a fall did not differ by group (85% with PT/OT referral vs. 90% with no PT/OT referral, p = 0.54). Participants referred to PT/OT were more likely to have received an inpatient PT/OT consultation (97% vs. 22%, p < 0.001) and less likely to be discharged home (77% vs. 98%, p < 0.001) than those without a PT/OT referral.
Comparing participants by PT/OT referral status, those who received a referral to PT/OT had worse median SPPB scores 7 (4, 10) vs. 10,7,11 (p = 0.002), slower median gait speed 0.50 (0.33, 0.78) vs. 0.72 ([0.58, 0.90] m/s, p = 0.01), and were more likely to fail the FSST (53% vs. 20%, p < 0.001) at 2-weeks post-mTBI compared to those without a referral to PT/OT. Of the group that did not get an PT/OT referral, 46% had impaired SPPB, 58% had impaired FSST, and 60% had impaired gait speed, indicating high fall risk.
Discussion
This study sought to evaluate referral patterns for outpatient rehabilitation (physical or occupational therapy) in a cohort of older adults with mTBI to determine if basic screening and referral patterns align with current fall prevention guidelines. Current fall prevention guidelines state that any individuals with a fall-related injury should have a multifactorial fall risk assessment, an individualized exercise intervention to prevent falls, 28 and follow-up within 90 days to assess fall-risk status. 11 Despite 89% of individuals in this sample meeting fall risk criteria based on their mechanism of injury (fall-related mTBI), less than a quarter (24.1%) received any PT/OT referral. The notable lack of referral for PT/OT services post-discharge among this population of older adults with mTBI highlights a critical gap between current fall reduction recommendations and routine practice and leaves these individuals at high risk of another fall with potentially more serious consequences.
The low PT/OT referral rates are not confined to our trauma center and health care system. Similarly low referral rates have been reported in other samples, with only 21% of middle-aged adults with mTBI receiving rehabilitation within 3 months post-injury. 29 While people with CT-positive mTBI may receive follow-up care from a neurologist, this gap in care is even more important among the group of patients with CT-negative mTBI because these patients likely have no follow-up visit with a health care provider yet are at high risk for a subsequent fall with potentially more serious injury. In the current study, CT status had no bearing on referral to PT/OT.
While this study cannot elucidate the causes for low rehabilitation referrals in older adults with mTBI, we speculate that clinical care pathways and the perception of a “mild” injury contributed to this gap in care. While overall referral to PT/OT was low, individuals who received a referral were more likely to have been treated at a trauma center (77% vs. 49% of those without a referral to PT/OT). They were also more likely to have been admitted to hospital (77% vs. 22% of those without a referral to PT/OT). This finding is consistent with results from a prior study that reported that adults with concussion who were treated in the ED were less likely to receive a referral to PT/OT relative to those treated in primary care and sports medicine clinics. 30 These differences in hospital admission rates across referral groups suggest factors that co-occur with mTBI in older adults may be driving the referrals. For example, injury to body regions other than the head or face can co-occur with mTBI as consequences of falls, and these orthopedic or tissue injuries may be more likely to result in hospital admission and PT/OT referral based on the overt, visible injuries. Future research should explore factors that influence PT/OT referrals in older adults with mTBI. Notably, referral to PT/OT was much more common among those who received an initial PT/OT consultation. This study included a single, level 1+ trauma center; whether similar results would be found at other trauma centers should be investigated. However, a burden on clinicians’ and patient’s time may play a role in getting necessary referrals for follow-up care.
A surprising result of this study was the low level of physical performance across the entire sample at 2 weeks post-mTBI, especially in people who did not receive PT/OT referral. In addition to meeting high fall-risk classification based on an injurious fall (the fall-related mTBI that qualified them for the study), over 75% of these patients also exhibited impaired balance and gait on at least one of the FSST, SPPB, or gait speed. Additionally, over 40% of patients were recurrent fallers. It should be noted that individuals who received a referral to PT/OT were lower functioning relative to those without a referral. However, even for individuals without a fall-related TBI or a previous fall history, the slow gait speeds and low level of physical performance, had they been assessed, would indicate intermediate fall risk that should prompt referral for tailored gait and balance exercises. 11 This would align with the American College of Surgeons Best Practice Guidelines in geriatric trauma management that call for a multifactorial fall risk assessment. 31
To our knowledge, our study is the first to report rates of PT/OT referral among older adults with mTBI and to objectively assess mobility using validated measures of both dynamic balance (FSST) and lower extremity function (the SPPB) among older adults within a short time after mTBI. One previous study using participants from the Health and Retirement Study found that individuals with a history of TBI (average time since injury: 33 years) reported greater difficulty with physical activities. 32 Although its findings generally align with ours, the study differed substantially in both population and methodology. Our study population reflects the diversity of the population treated at our trauma center and participating hospitals. Other strengths of the current study include well-defined TBI criteria and CT assessment results.
Limitations of the study should also be considered. We focused on PT/OT referral, but we do not know the nature of the referral (e.g., was it balance-related or orthopedic related), whether the referral was related to the TBI, or whether the patients acted upon the referral. Therefore, the rates reported here reflect the upper bound; it is likely that the percentage of older adults that receive appropriate fall-prevention interventions after mTBI is much lower than the already low referral numbers reported here. Second, we focused on direct referrals from the ED/trauma center, it is possible that patients received intermediary referrals (e.g., referred to a geriatrician or primary care provider who then provided fall-prevention guidance or referred the patient to PT/OT). However, these efforts are likely to be infrequent, and intermediary referrals, even if modestly increasing the number of referrals, create delays in beginning necessary fall-prevention interventions. Typical delays in receiving a PT/OT evaluation after TBI are already lengthy, taking on average 60 days. 33 Given the high fall risk, both by mechanism of injury (fall-related TBI) and the low levels of physical functioning, immediate intervention is recommended. Generalizability of study findings to individuals who were excluded, including those with dementia, severe injury to other body regions, and non-English speakers, is unknown. The current study is limited to a single health care system in the mid-Atlantic region of the United States but does include a range of hospitals from a Level 1 trauma center to suburban community hospitals. Finally, we lack measures of balance and lower extremity function pre-TBI and during the acute period. However, despite these limitations, our results suggest that PT/OT referrals are likely being underutilized.
In conclusion, older adults with mTBI have impaired mobility and balance and are at high risk for future falls yet are not receiving guideline-concordant care. This study highlights an unmet need for fall prevention interventions, including referral to PT/OT. Future studies should consider expanding results to excluded groups, including individuals with dementia, and examine the effects of the allocation of guideline-concordant care on individual fall rates as well as health services outcomes, such as hospital readmissions and prospective health care expenditures.
Transparency, Rigor, and Reproducibility Summary
Study design and transparency
RETRO-TBI is an ongoing prospective cohort study designed to evaluate trajectories of recovery in four domains of functioning (i.e., physical function, cognition, sleep, and psychological symptoms) over the year following primarily mild traumatic brain injury among adults aged 65 and older. The present descriptive analysis focuses on receipt of a referral to physical or occupational therapy (PT/OT) at discharge from care and measures obtained at the 2-week assessment. Neither the study protocol nor the analytic plan for these analyses has been published or uploaded to a website. RETRO-TBI eligibility enrollment criteria are detailed in the methods section of this article. Follow-up, assessments, and information obtained from the medical record are similarly detailed. This article presents descriptive information on receipt of referral to PT/OT and bivariate analyses by PT/OT referral status using Fisher’s exact test to test differences in distribution of categorical variables for statistical significance and Student’s t-test or the Wilcoxon rank-sum test to test differences in distribution of continuous variables for statistical significance. De-identified data from RETRO-TBI will be made available upon request to Dr. Albrecht after completion of all planned analyses. Statistical code will be made available upon inquiry.
Authors’ Contributions
J.S.A. and O.A. made substantial contributions to the conception and design of the study, acquisition, analysis, and interpretation of data, drafting and approving the final version of the article and agree to be accountable for all aspects of the work. M.N. and D.S. made substantial contributions to the conception and design of the study, acquisition of data, drafting and approving the final version of the article and agree to be accountable for all aspects of the work. L.D., P.F., and Y.L. made substantial contributions to the analysis and interpretation of data, drafting and approving the final version of the article and agree to be accountable for all aspects of the work. J.M., E.M.W., R.K., A.G.B., D.O., and N.B. made contributions to initial design of RETRO-TBI, critically reviewed the draft and approved the final version of the article and agree to be accountable for all aspects of the work.
Ethical Considerations
This study was approved by the University of Maryland School of Medicine Institutional Review Board (HP-00100973).
Consent to Participate
All study participants provided written informed consent.
Data Availability
De-identified data from RETRO-TBI will be made available upon request to Dr. Albrecht after completion of all planned analyses. Statistical code will be made available upon inquiry.
Footnotes
Acknowledgements
The authors thank Mary Bahr-Robertson, BA, for recruiting study participants.
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This study was supported by National Institutes of Health (NIH) award R01AG076441 to the University of Maryland School of Medicine (JSA). JSA also acknowledges support from NIH awards P30AG028747 and R01AG079391. AGB acknowledges support from NIH grants. NB reports support from DOD awards (W81XWH-24-CCCRP1; HR001122S0043-RITMO-PA-006). LED and PCF acknowledge support from NIH R01HD114748, OA acknowledges support from VA I01RX003484 and I01CX002836.
This study was supported by National Institutes of Health award R01AG076441 and P30AG028747 to the University of Maryland School of Medicine.