
Abstract
Sport-related concussion (SRC) is a significant public health concern, warranting exploration of neuroimaging and fluid-based biomarkers as objective measures for diagnosis and prognosis. Sex differences in concussion outcomes may be influenced by the menstrual cycle, hormones, and hormonal contraceptives. Equitable representation of female athletes in emerging biomarker research is critical, but existing literature may not meet this need. This scoping review assessed neuroimaging and fluid-based biomarker research in SRC for inclusion and analysis of female athletes and to summarize female-specific and sex-difference results. Searches in MEDLINE, Scopus, Cochrane, and PsycInfo from January 2001 to July 2025 identified original research published in English and focused on SRC with neuroimaging or fluid-based biomarker assessment within 6 months after injury. Studies were then classified based on study sample sex/gender, and studies with female-specific and sex-difference results were further summarized. Literature review revealed underrepresentation of concussed female athletes in biomarker research, with over three times more concussed male athletes studied than concussed female athletes and approximately 19 times more male-only than female-only studies. Most mixed-sex studies did not explicitly investigate female-specific results. The 29 summarized reports indicate potential sex differences and different results for female athletes than those in the broader existing literature, although small sample sizes make definitive conclusions difficult. Addressing the knowledge gap in SRC in female athletes requires future biomarker research to include sufficient numbers of female athletes, analyze data to identify potential sex differences, and collect relevant data, including hormone levels and detailed menstrual cycle and hormonal contraceptive use information.
Keywords
Key Points
Female athletes are underrepresented in concussion research on emerging neuroimaging and fluid-based biomarkers. Analyses designed to detect female-specific or sex-difference results are needed in addition to incorporating more female athletes.
Introduction
Sport-related concussion (SRC) is a significant public health concern, with growing recognition of its acute and potential long-term consequences.1,2 As more females engage in organized sports at youth, collegiate, and professional levels, it has become increasingly important to understand sex-specific injury mechanisms and recovery trajectories. 3 Research has repeatedly demonstrated that females are more likely to sustain an SRC than males playing the equivalent sport.4–6 Emerging evidence also suggests that SRC presents differently in female athletes compared to their male counterparts, with females often reporting a greater number and severity of symptoms and potentially experiencing longer recovery times.7,8 Numerous sex-specific biomechanical and biochemical factors such as head and neck anatomy, menstrual cycle phase, and hormonal contraceptive use have been proposed to explain differences in concussion susceptibility, recovery trajectories, and biomarker profiles.9,10 While some of these differences may reflect a greater willingness to report symptoms, recent research also suggests underreporting persists among women, complicating reliance on self-report measures.7,11,12
Evidence from the broader neuroscience literature demonstrates the existence of fundamental anatomic and physiological differences between males and females.13–16 The National Institutes of Health (NIH) now requires consideration of sex as a biological variable in funded research, a policy that has improved inclusion of female subjects in neuroscience. Nevertheless, much of the neuroscience research to date has still not been designed to discover sex differences. 17 Moreover, appropriate analysis depends on the nature of the sex difference, with qualitative differences (i.e., due to differential mechanisms) requiring split-by-sex analyses while quantitative differences (i.e., different means of a dependent variable) can be analyzed with sex as a factor. 18 Reports that “control” for sex or include sex as a covariate without first establishing the nature of (or lack of) a sex difference essentially assume that “sex differences are quantitative, linear, and without interactions,” 18 and that subsequent findings apply to both sexes. These considerations are particularly consequential for traumatic brain injury (TBI, including concussion) biomarker research, where neuroimaging signals and fluid biomarker concentrations may reflect fundamentally different pathophysiological processes across sexes, not merely mean-level differences, yet sex-stratified analyses remain rare.
Sex differences in TBI have received growing attention, with several reviews synthesizing their scope and complexity. Prior work has documented that females with TBI generally experience worse outcomes than males in clinical settings, and has highlighted the role of gonadal hormones, neuroanatomical variation, and pharmacokinetic differences as potential mediating factors, noting a need for greater methodological consistency.19–22 Notably, less attention has been given to SRC, and existing research on sex differences related to SRC has been primarily focused on clinical outcomes. Despite higher rates of SRC in females participating in sex-comparable sports, research focused on female athletes remains limited with persistent underrepresentation in studies that include both sexes and minimal inclusion of female-specific analyses. 23 These limitations, if perpetuated, are especially concerning given the emergence of novel imaging and serum biomarkers. Advanced neuroimaging and fluid-based assays are being increasingly used to elucidate the pathophysiology and long-term effects of SRC. 24 Given the foundational role of biomarkers in advancing objective diagnostic and prognostic tools for SRC, it is critical to understand how these biomarkers have or have not been applied in female populations. Without adequate inclusion of female athletes in novel biomarker research, these powerful tools are at risk of being less accurate or applicable across sexes.
To highlight this gap and begin to synthesize current knowledge, this scoping review maps the extent of female athlete inclusion in existing SRC biomarker research. The primary objective of this review is to assess the current literature on neuroimaging and fluid-based biomarkers in SRC for inclusion and analysis of female participants. Research with female-only subjects, split-by-sex analyses, or analyses that address concussion-related sex differences (e.g., included sex-related interaction terms) will be summarized and evaluated for inclusion of relevant factors such as ovarian hormones, hormonal contraceptive use, or menstrual cycle data. While this review focuses on cisgender female athletes, we emphasize the importance of future research that is inclusive of transgender and nonbinary individuals to ensure that concussion science benefits all athletes. This work will inform future study design and promote equity in SRC biomarker research by advocating for intentional inclusion of female subjects and sex-specific methodological approaches.
Methods
Protocol registration
The review protocol was drafted and revised by the research team using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses: Extension for Scoping Reviews (PRISMA-ScR) for guidance. The protocol was registered prospectively with the Open Science Framework on May 22, 2024 (https://doi.org/10.17605/OSF.IO/XQ2US).
Eligibility criteria
To be included in the primary outcome, research was (1) peer reviewed original research (i.e., no case studies, conference papers or abstracts, reviews, preprints, dissertations, study protocols, editorials, or commentaries) published or e-published in English between January 2001 and July 2025; (2) focused on SRC or mild traumatic brain injury (mTBI); and (3) included at least one neuroimaging or fluid-based biomarker assessment within 6 months after injury. Research was excluded if it did not include concussion/mTBI with sport as the mechanism or if sport-related cases were not analyzed separately when other mechanisms were also included. Sample size and sex/gender information were collected from all included reports. Research results were additionally summarized when reports included female athletes and must have analyzed them separately or addressed concussion-related sex differences (e.g., included sex-related interaction terms). While sex and gender are separate concepts, reports screened for this review did not often make a clear distinction on how their data were collected. Therefore, for the purposes of this review, the terms female and woman were treated as designating female athletes.
Information sources
Potentially relevant research was identified through searching MEDLINE, Scopus, Cochrane, and PsycInfo from January 2001 to July 2025. These data sources were chosen to reflect readily available information. An experienced reference librarian (O.O.) drafted the search strategies, which were revised by the research team. The final search strategy for MEDLINE (via Ovid) is provided in the Supplement. The initial search was conducted on May 20, 2024, with a second search on July 22, 2025, and results were exported into Rayyan and deduplicated by O.O. and B.D.G.
Process for selecting evidence
Screening of articles was conducted in two stages. In a rapid screening step, titles and abstracts of each record were screened by a single reviewer (either B.D.G. or E.M.). Articles lacking abstracts were by default included in the second stage of screening. The second stage, conducted by B.D.G., E.M., T.B.M., H.M.F., E.F., and M.J.A., involved two reviewers blinded to the decisions of others screening the full text. Any conflicts were resolved by a third reviewer. Reviewers with authored reports included in the search results were not involved in the screening, data extraction, or synthesis of reports for which they are co-authors.
Articles were excluded if they were published before January 2001, not peer-reviewed original research, non-human studies (e.g., animal samples or computer model simulations), had a total sample size less than 10 participants, did not include concussion/mTBI 6 months or less from injury (e.g., sub-concussive, contact sport exposure, repetitive head injuries, mTBI/concussion not analyzed separately from moderate/severe TBI, only timepoints outside 6 months post-injury), did not include sport as a mechanism analyzed separately, or did not include at least one neuroimaging/fluid-based biomarker. Screeners coded the first recognized reason for exclusion, which may underestimate the actual frequency of the reasons for exclusion if multiple reasons could be applied to a report.
Synthesis of results
Included articles were classified based on study samples as female-only, male-only, sex/gender not specified, mixed-sex without female-specific results, or mixed-sex with female-specific or concussion-related sex-difference results. Information readily available from the reports or their supplements was collected in standardized forms with any missing data labeled as unspecified or unclear. Numbers of concussed and control subjects were collected from male-only and sex/gender not specified reports. Mixed-sex reports were examined for numbers of male and female concussed and control subjects, matching of participants by sex, inclusion of sex as a covariate, and inclusion of a sex-related interaction term in analyses. Reports with female-only samples and mixed-sex samples that analyzed female samples separately or addressed concussion-related sex differences (e.g., included sex-related interaction terms) were included in the summary. Additional collected information included biomarker modalities, sport(s) represented, age and level of athletes, the number and sex of participants with a description of controls and exclusion criteria, time points included in the report, ovarian hormone or menstrual cycle information, and a summary of the results focusing on female athletes or sex differences. A second team member verified all collected information.
Results and Discussion
Study characteristics
Records were identified from four databases (Ovid MEDLINE, Scopus, PsycInfo and Cochrane) resulting in 4,881 reports screened of which 1,141 were assessed for eligibility. Reasons for exclusion for reports not meeting the review criteria are detailed in Figure 1. Two hundred ninety-one reports met our inclusion criteria, with 29 meeting our criteria for summaries.
Modified Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. Details the identification, screening, and inclusion/exclusion of articles at each stage of the review process.
Figure 2 shows the breakdown by the sex/gender of samples for the included reports. Eighty-two reports (28.2%) on imaging or fluid-based biomarkers in SRC were determined to include only male subjects, some of which did not explicitly state the sex of participants in the methods or results sections but mentioned the inclusion of only male subjects as a limitation and were thus classified as male-only. Of the 14 reports in which sex/gender was not specified, 12 were of American football or professional ice hockey, which likely included exclusively male subjects. In total, at least 94 reports (32.3%) likely included only male athletes. In contrast, five reports (1.7%) were focused exclusively on female athletes. Most reports (190 reports, 65.3%) were on mixed-sex samples. Some attempted to account for potential sex differences by matching participants by sex (61 reports) or including sex as a covariate (47 reports), but few of these reports (15 reports) performed split-by-sex analyses that evaluated results for female athletes separately. An additional 9 mixed-sex reports addressed female-specific results or concussion-related sex differences by including interaction terms of concussion-by-sex in models, indicating sex differences, and/or normalizing outcomes by sex. In total, 29 reports (10.0%) provided results specific to female athletes. (Note: three research groups generated 11 reports that may have within-group sample overlap—see Table 1 “related reports.”) Figure 3 shows the breakdown of sex/gender for studies by publication year.
Sex/gender breakdown of included reports. Chart shows the peer-reviewed neuroimaging and fluid-based biomarker reports on SRC published January 2001 through July 2025 broken down by sex/gender of sample populations.
Sex/gender breakdown of reports by publication year. Chart shows the sex/gender breakdown of reports included in this review by publication year.
Additional Study Characteristics for Summarized Reports
Reports published by the same research group with potentially overlapping samples are noted in parentheses. Numerical data are reported as mean (SD) or median [Q1, Q3] whenever these data were available in the original manuscripts. Blood-based biomarkers are labeled as serum or plasma as listed is reports or as blood when unspecified.
Modality: 4-HNE, 4-hydroxynonenal; ASL, arterial spin labeling; BLBP, brain lipid-binding protein; DTI, diffusion tensor imaging; DWI, diffusion weighted imaging; eBFI, enhanced brain function index; EEG, electroencephalogram; GFAP, glial fibrillary acidic protein; HMGB1, high mobility group box protein 1; IFN- γ, interferon- γ; IGF-1, insulin-like growth factor 1; IGFBP5, IGF binding protein 5; IL, interleukin; LPS, lipopolysaccharide; MAPT, microtubule-associated tau protein; MCP, monocyte chemoattractant protein; miRNA, micro ribonucleic acid; MPO, myeloperoxidase; MPRAGE, magnetization prepared rapid gradient echo; MRS, magnetic resonance spectroscopy; MRI, magnetic resonance imaging; NfL, Neurofilament Light; PEA15, phosphoprotein enriched in astrocytes 15; QSM, quantitative susceptibility mapping; R848, resiquimod; rs-fMRI, resting state functional MRI; SWI, susceptibility weighted imaging; UCH-L1, ubiquitin C-terminal hydrolase L1; TNF-α, tumor necrosis factor- α; t-tau, total Tau; vWF, von Willebrand factor.
Sports: AF, American football; AU, Australian rules football; BB, baseball; BK, basketball; CH, cheerleading; CW, crew; CC, cross country; DN, dance; DV, diving; FH, field hockey; FS, figure skating; GL, golf; GY, gymnastics; HK, hockey (unspecified); IH, ice hockey; LC, lacrosse; MB, mountain biking; RW, rowing; RG, rugby; SL, sailing; SC, soccer; SB, softball; SQ, squash; SW, swimming; TN, tennis; TF, track and field; VB, volleyball; WP, water polo; WR, wrestling.
General: ACC, anterior cingulate cortex; AD, axial diffusivity; ADC, apparent diffusion coefficient; AUROC, area under the receiver operating characteristic curve; BOS, beginning of season; CBF, cerebral blood flow; CorpCal, corpus callosum; Cr, creatine; CST, corticospinal tract; Ctrl, control; Cx, concussion; d, days; dlPFC, dorsolateral prefrontal cortex; EOS, End Of Season; F, female; FA, fractional anisotropy; Gln, glutamine; Glx, glutamate + glutamine; h, hours; HC, HORMONAL CONTRACEPTIVE; HOC, history of concussion; ILF, inferior longitudinal fasciculus; IQR, interquartile range; LOC, loss of consciousness; LV, latent variables; m, months; M, male; MD, mean diffusivity; mI, myo-inositol; min, Minutes; MIP, macrophage inflammatory protein; MSK, musculoskeletal injury; MTG, medial temporal gyrus; NAA, N-acetyl aspartate; PTA, post-traumatic amnesia; rCBF, regional cerebral blood flow; RD, radial diffusivity; rec, recreationally active; ROI, region of interest; RTP, return to play; RTP45, 45 days after RTP; SCAT, sport concussion assessment tool; SLF, superior longitudinal fasciculus; SPL, superior parietal lobule; SRC, sport-related concussion; STG, superior temporal gyrus; TBI, traumatic brain injury; w, weeks; w/, with; w/i, within; w/o, without; WM, white matter; yr, year.
Subjects in mixed-sex reports were often unbalanced, with more male than female participants and more female controls than concussed female athletes. Not including the 26 mixed-sex reports with unclear sex breakdown (lacking enough detail to determine the breakdown by sex of controls and concussed athletes in the report or supplement), the mixed-sex reports included almost 5,100 concussed male athletes and just over 2,400 concussed female athletes. Sixty-four mixed-sex reports had a ratio of concussed males to concussed females greater than 2:1, and five mixed-sex reports did not include any concussed female athletes (i.e., only control subjects were mixed-sex). This inequality between male and female subjects in imaging or fluid-based biomarkers SRC research is even more evident when looking at all included studies that specified sex of controls and concussed athletes, with roughly 16,800 males (7,600 with SRC, 9,200 controls) and 5,900 females (2,500 with SRC, 3,400 controls) (see Fig. 4).
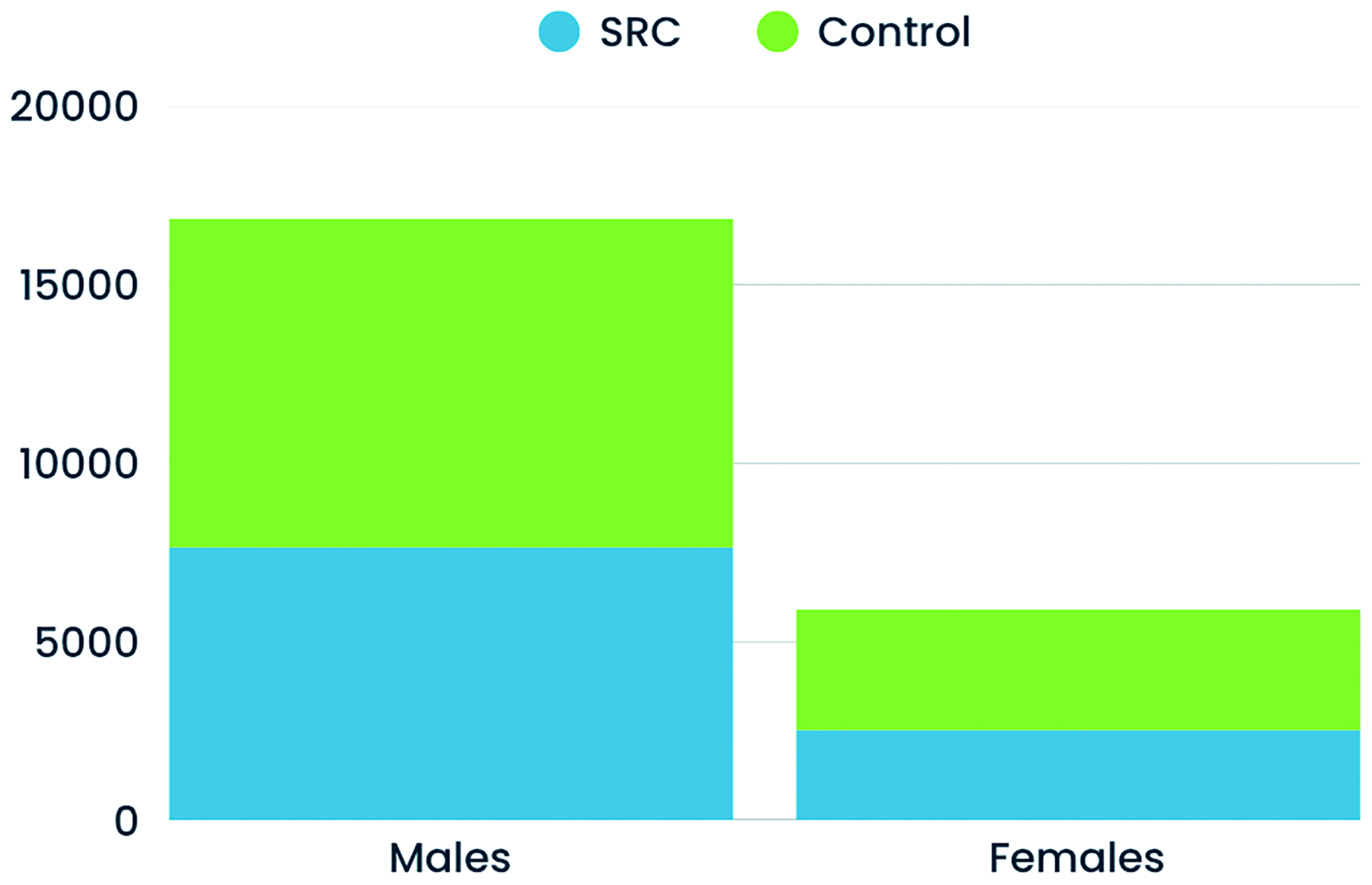
Sex/gender breakdown of participants. Graph shows the male and female subjects from all mixed-sex, male-only and female-only reports that provided enough detail to determine sex of controls and concussed athletes (SRC).
Reports including female athletes did not generally include data on hormones, hormonal contraceptives, or the menstrual cycle. Two reports focused on progesterone as an outcome, measured in serum by Chen et al. 28 and in plasma by Ott et al. 43 Chen et al. 28 also matched SRC athletes with controls based on either menstrual cycle phase or hormonal contraception use. Naturally cycling athletes scanned in days 1–7 of the menstrual cycle were matched. Oral contraceptive and NuvaRing users were categorized as being in active or inactive phases and were matched within 2 days of their pill pack or NuvaRing days. Ott et al. 43 also incorporated menstrual cycle phase into their analyses. They collected oral contraceptive use data and found no significant difference in use between the SRC and control groups, but these data were not used further in analyses. Mac Donald et al. 38 evaluated the potential influence of menarche status (yes/no) on volumetric data. No other reports collected hormone or female-specific data.
Literature review results
Table 1 provides the following information: sport, age and level of athletes, number of subjects, control descriptions, time between SRC and biomarker measurements, and a summary of results for each report. 15 summarized reports included a neuroimaging component, and 15 included a fluid-based biomarker component, with one report overlapping both areas of research.
In the following sections, we synthesize the results from these reports, but we caution that the limitations of the existing literature make it difficult to draw definitive conclusions. Heterogeneity in experimental methods (scanning equipment, acquisition parameters, assays), statistical methods, sample characteristics, and the timing of post-injury visits all likely contribute to differences in results. In addition, small sample sizes and the preliminary nature of many of the reports may limit generalizability.
Neuroimaging results
Diffusion MRI (two female-only reports, five mixed-sex reports)
The most common neuroimaging modality studied was diffusion MRI, as it was in a recent review of biomarkers and emerging technologies in SRC by Tabor et al. 24 Diffusion MRI is thought to reflect subtle microstructural changes that occur as a result of concussion, with research to date suggesting edema, axonal damage, and demyelination as possible pathological sources for diffusion differences.54,55 Overall, diffusion MRI reports did identify some consistent areas of the brain as vulnerable to concussion, but varied in the nature of their findings. Multiple reports found diffusion differences in the corpus callosum at acute and subacute timeframes,29,39,44,52 and two of those also saw differences in the corona radiata.29,52 For female athletes, either separately or within a mixed-sex group, higher fractional anisotropy (FA),39,44,52 lower mean diffusivity (MD) and axial diffusivity (AD),39,44 and lower radial diffusivity (RD)44,52 were the most common finding across studies, though lower FA 29 and lack of significant changes to various diffusion metrics29,37,45 were also seen. Two reports that included the sex-by-group interaction in analyses did not find it significant37,44; however, Churchill et al. 29 found lower FA and nonsignificantly lower MD for SRC females relative to controls while male SRC athletes had higher FA and MD than controls, suggesting the existence of sex-specific diffusion differences in response to injury. In addition, white matter features from diffusion MRI were important in classifying athletes with post-concussive syndrome and the predictive index was associated with the number of prior concussions for female but not male athletes. 50 Variation among the reports with respect to direction of diffusion metric differences is consistent with findings in a systematic review by Lindsey et al. 56 and may be partially attributed to timing of visits with respect to injury, variation in region of interests (ROIs), and differences in scanners and scanning parameters.
Summary: Diffusion data highlights the sensitivity of corpus callosum in female athletes following concussion, most typically characterized by higher FA and lower diffusivity, though variation across studies was observed. There was limited investigation of sex-dependent effects of injury on diffusion metrics, with one study identifying different effects in female athletes compared to male athletes.
MR spectroscopy (two female-only reports)
Magnetic resonance spectroscopy (MRS) can quantify metabolite concentrations that may change following concussion as a result of mitochondrial dysfunction and altered metabolism due to ionic flux and glutamate release. 57 Among the most common metabolites measured are: N-acetyl aspartate (NAA), a neuronal marker synthesized by neurons; creatine (Cr), involved in energy homeostasis; glutamate (Glu), an excitatory neurotransmitter, and glutamine (Gln), an amino acid precursor to glutamate, which are often reported as Glx = Glu + Gln; and myo-inositol (mI), a neurotransmitter precursor involved in calcium signaling. 58 Only two reports that utilized MRS met our study criteria and they had diverging results. One found higher Glx/Cr in the primary motor cortex and dorsolateral prefrontal cortex at 6 months post-injury, 27 while the other reported lower Gln and Gln/Cr in prefrontal white matter acutely and around 3 months post-injury which resolved by 6 months. 45 Both studies observed no differences in NAA 45 and NAA/Cr 27 in female athletes with SRC. Interestingly, these results conflict with those of a meta-analysis of MRI in all severity TBI where decrease in NAA and no effects for either Cr or Glx across brain regions were observed. 58 The differences between these reports themselves and with the meta-analysis may be somewhat explained by regional variation of MRS results. 58
Summary: Only two studies investigated MRS differences following concussion, both with a limited number of injuries. While this makes definitive conclusions difficult, it is noteworthy that results varied across studies and were inconsistent with a meta-analysis of MRS results from all severity TBI.
Arterial spin labeling (one female-only report, five mixed-sex reports)
Although the mechanism is not entirely understood, cerebral blood flow (CBF) may be affected by mTBI through decoupling from neuronal metabolism, disruption to the blood–brain barrier, and impaired autoregulation. 59
ASL can be used to quantify CBF and potentially identify changes to the cerebrovascular system occurring as a consequence of concussion. Included ASL reports had varying results. Three found higher (or trending higher) CBF,29,44,47 while two found lower (or trending lower) CBF post-SRC.28,53 In addition, athletes reporting physical symptoms at 6 weeks post-SRC had higher CBF in the left dorsal ACC than asymptomatic athletes and controls. 47 Other regions with significant differences for post-SRC female athletes included the caudate, 44 left dorsal ACC, 47 left insula, 47 left superior and middle temporal gyri, 28 and left superior parietal lobule, 28 with no overlap between studies, although regions investigated across studies had little overlap. Higher CBF being slightly more common here is somewhat in contrast with the reports in a recent systematic review of ASL in mTBI, although their findings also varied between increased and decreased CBF. 59 In terms of differing effects of injury on CBF based on sex, most studies found no sex difference 47 or nonsignificant sex-by-group interactions,44,53 though Churchill et al. 29 found nonsignificantly higher CBF for female SRC athletes but lower CBF for post-SRC males versus controls. Similarly, male athletes had decreased occipital CBF during selective head cooling post-SRC, while females had stable or increased CBF, 51 though the sex-by-group interaction was not significant.
Resting-state functional MRI (one female-only report, two mixed-sex reports)
Resting-state functional MRI (rs-fMRI) measures changes to the blood–oxygen-level dependent (BOLD) signal to evaluate the functional connectivity within the brain which could be disrupted by SRC. Included rs-fMRI studies showed that recently concussed athletes had altered functional connectivity.37,39,44 Lower caudate connectivity to the pallidum and thalamus was present post-SRC, as well as a negative relationship between symptom severity and activity in the cerebellum and a positive relationship between days since injury and cerebellar-parietal connectivity. 44 In a female-only report, altered connectivity (higher and lower) between the whole brain and the default mode, cerebellar, and executive networks was linked with diffusion tensor imaging (DTI) changes along with symptom severity. 39 While one rs-fMRI report did not see a significant sex-by-group interaction, 44 another found lower frontoparietal-visual association and default mode-visual II network connectivity for concussed males than for controls, with no group difference for females. 37
Summary: Female athletes have altered functional connectivity post-SRC in various brain regions, with some evidence of potential sex differences.
Other neuroimaging modalities (five mixed-sex reports)
A handful of reports used other neuroimaging metrics, ranging from volumetric MRI to electroencephalography (EEG), with some evidence of sex-specific concussion effects across studies. For example, a study of EEG, which measures electrical currents to quantify neuronal function via electrodes on the scalp, found that the enhanced brain function index (eBFI; a percentile assigned based on EEG, neurocognitive measures, and clinical signs/symptoms of concussion) was lower for female versus male athletes overall. 30 Moreover, split-by-sex analyses demonstrated that while SRC athletes had lower eBFI than controls in both sexes, effects were stronger in females (though no interactions with sex were significant). 30 Similarly, sex differences in white matter hypointensity burden following concussion (higher in male vs. female) were observed using susceptibility weighted imaging. 36 Using quantitative susceptibility mapping (QSM), researchers found a trend towards a significant sex-by-injury interaction driven by lower susceptibility in the straight sinus (a measure of cerebral venous oxygen saturation) in female SRC athletes versus controls. 53 In contrast, another group saw higher susceptibility in the cerebellum post-SRC across a mostly male cohort, with no sex interaction observed. 44 Finally, an analysis of adolescent female athletes post-SRC versus controls grouped by menarche status did not find any significant differences in volumetric measures. 38
Fluid-based biomarker results
Fifteen summarized reports had a fluid-based biomarker component, with one of these also including a neuroimaging component. All but one report focused on blood-based biomarkers, which aligns with Tabor et al. 24 finding blood to be the most common fluid analyzed for biomarkers. Furthermore, our review demonstrates that only one report has evaluated non-blood-based (urinary) biomarkers, with no saliva biomarkers studied, in female-only cohorts or in cohorts that completed sex-stratified analyses.
Neurological injury markers (six mixed-sex reports)
Biomarkers with connection to neurological injury have gained attention for their potential in aiding diagnosis and prognosis for concussion. 24 These include glial fibrillary acidic protein (GFAP), a marker of glial damage; neurofilament light (NfL) and tau, both axonal cytoskeletal proteins; and ubiquitin carboxyl-terminal esterase L1 (UCHL1), an enzyme found in neurons involved in protein degradation.35,60,61
While post-SRC male athletes have high GFAP with respect to baseline 40 or uninjured levels, 49 female athletes either respond similarly 49 or show no significant difference. 40 Furthermore, an underlying sex difference exists for GFAP with higher levels for female subjects than males. 49 Although baseline UCHL1 is lower in females,25,40,49 post-SRC females and males may have similar levels of UCHL1.35,49 While three studies indicated UCHL1 was not promising for distinguishing those with SRC from controls,25,35,40 Tabor et al. 49 found females had high post-SRC UCHL1 compared to uninjured levels, while males showed no significant difference. Sex differences appear to exist in the trajectory of NfL post-SRC with increases for male athletes, but no significant differences for female athletes.40,49 Additionally, Bui et al. 26 observed that a high percentage of female athletes with SRC had low NfL at baseline that remained low following injury, a trajectory that was less likely to be associated with loss of consciousness or post-traumatic amnesia, features which are less common for females than males.62–64 Finally, reports on post-SRC trajectories of tau found evidence for sex differences, though the direction of these effects varied (e.g., no consistent pattern in elevated tau in either sex).40,41,49
Cytokines/chemokines (four mixed-sex reports)
Inflammation has been shown to result from mild TBI and is suggested as a possible root of many concussion symptoms.57,65 Measuring peripheral inflammatory cytokines and chemokines may offer a way to evaluate the effects of concussion and to identify possible mechanisms for these effects. 33 Three of the four reports examining various cytokines and chemokines (three are from the same group) are suggestive of sex differences. Symptom severity was negatively correlated with interferon (IFN)-γ, myeloperoxidase (MPO), and tumor necrosis factor (TNF)-α and positively correlated with monocyte chemoattractant protein (MCP)-4 for female athletes, but in male athletes symptoms positively correlated with IFN-γ. 33 In addition, MPO, macrophage inflammatory protein-1β, and eotaxin were lower, and IFN-γ-induced protein-10 was higher in female versus male SRC athletes, although these differences did not survive correction for multiple comparisons. 33 Analyzing results with sex-controlled z-scores, Di Battista et al. 32 found higher post-SRC MCP-4 and MIP-1β compared to healthy controls and a positive relationship between days to recovery and higher subacute MCP-1 and MCP-4 in athletes with SRC, but not musculoskeletal injury. When examining immunoreactivity through stimulation of blood samples separately with lipopolysaccharide (LPS) and resiquimod (R848), significant effects of SRC on LPS reactivity were seen in male but not female athletes. 34 Furthermore, the effects of history of concussion on post-SRC immunoreactivity also differed between male and female athletes in the same study. In contrast, O’Brien et al. 42 did not find a main effect of time, sex, or a sex-by-time interaction for IL-1β or IL-18 levels post-SRC.
Other fluid-based biomarkers (two female-only reports; three mixed-sex reports)
The only fluid-based biomarker examined in female-only reports was progesterone. Sex hormones have been theorized to potentially play a role in the possible menstrual cycle influence on concussion vulnerability or outcomes and in sex differences in concussion.19,67,68 Additionally, progesterone has been shown to provide a degree of neuroprotection in animal models and phase II clinical trials, but failed phase III trials indicate its role is not so straightforward. 19 Chen et al. 28 found associations between progesterone, CBF, and perceived stress in female athletes, while perceived stress symptoms negatively correlated with progesterone in the SRC group. However, Ott et al. 43 saw no significant associations between SRC and progesterone.
Research into other fluid-based biomarkers primarily showed no evidence of sex differences. One study found no significant findings or sex-by-time interactions for several markers including phosphoprotein enriched in astrocytes 15, von Willebrand factor, claudin-5, fibrinogen, high mobility group box protein 1, and 4-hydroxynoneal, though a decrease in brain lipid binding protein (BLBP) was seen for female athletes post-SRC compared to pre-injury baseline but not for males (no significant sex-by-time interaction). 48 Similarly, no significant sex-by-time interactions post-SRC were found in an analysis of multiple microRNA in plasma, but plasma levels of miR-221-3p and miR-27a-3p were decreased post-SRC compared to baseline and were inversely correlated with symptom severity across the whole cohort. 46 Finally, urinary insulin-like growth factor (IGF) 1 and IGF binding protein 5 were lower post-SRC compared to controls with no significant sex-specific differences. 31
Summary of sex effects across modalities
Evidence for influence of SRC on the brains of female athletes existed in each of the modalities included in this review to varying degrees. For imaging studies, common brain areas affected included the corpus callosum,29,39,44,52 limbic system,37,39,44,47 cerebellum,39,44 corona radiata,29,52 and prefrontal white matter and cortex.39,45 Combined with effects on neurological injury markers (e.g., NfL), injury to white matter is the most common finding, consistent with white matter damage being considered one of the hallmarks of concussion.61,69 In addition, the sensitivity of a wide array of other biomarkers to the effects of concussion in female athletes is consistent with the known heterogeneous physiological response to concussion, which has been extensively documented elsewhere. 57 Interestingly, while a variety of biomarkers have been investigated, very few reports explicitly investigated cross-modal relationships among biomarkers. Given that relationships between perceived stress and progesterone were 100% mediated by CBF, 28 and there were links between DTI differences, functional connectivity, and the number of SCAT3 symptoms, 39 cross-modal investigations may prove useful in further research.
While the general physiological consequences of concussion may be largely similar between male and female athletes, summarized reports, though limited, suggest that sex-dependent effects likely exist. Potential post-SRC sex differences were identified in diffusion MRI metrics,29,52 CBF,29,51 hypointensity burden in susceptibility weighted imaging, 36 QSM susceptibility, 53 connectivity, 37 and eBFI measured with EEG, 30 among imaging metrics. For fluid biomarkers, sex differences post-SRC were seen in GFAP, 40 UCHL1, 49 NfL,26,40,49 tau,40,41,49 and various cytokines and chemokines.32–34 Given the nature of the differences and the underrepresentation of female athletes in many of the studies, we cannot clearly say that female athletes fare better or worse post-SRC, just that differences likely exist and warrant more investigation.
It is important to note the great variability observed across studies. Some of the aforementioned sex-effects were limited to a single report and there was a lack of evidence for sex differences or significant sex-by-group interactions in these same metrics in other studies.35,37,42,44,47,49,53 Interestingly, many of the sex-related effects observed were from studies that conducted a priori split analyses or exploratory analyses even when the sex-by-injury interaction was not technically significant. Given the modest sample sizes for most studies, this could simply reflect limited power to identify significant interactions, and we discuss the utility of conducting planned split-by-sex analyses below. Besides discrepancies driven by limited sample sizes between studies, additional differences between reports within this review, and compared to existing literature, may be explained in part by differences in methodology such as using different MRI sequences, scanners, ROIs, assays for biomarker measurement, and statistical approaches, as previously discussed. Nevertheless, the current review highlights probable sex-dependent effects of concussion in athletes that merit further study.
Limitations
While this review highlights an important knowledge gap, its tight focus on neuroimaging and fluid-based biomarkers in recent SRC means that other important areas of concussion research were not included. Broadening our scope to incorporate concussion by other mechanisms would have allowed for more reports to be included in our review and in our summary. Likewise, expanding to research on those with a history of concussion would also result in more information specific to female participants. Additionally, while female athletes are understudied, our literature search did not turn up any reports that included results for transgender or nonbinary athletes, two additional groups that are also underrepresented.
Conclusions
The underrepresentation of female athletes, recently highlighted by D’Lauro et al.
23
in the research informing concussion consensus and position statements, also exists in the neuroimaging and fluid-based biomarker research. While 67.0% of reports in our review were either mixed-sex or exclusively focused on female athletes, the majority of these (85.1%) did not include female-specific or concussion-related sex-difference results. Moreover, <2% of the identified studies were exclusively in female athletes, compared with 32% exclusively male studies. Not only are there few reports that appropriately analyze results for female athletes, but those that do tend to be small. Only five reports that included a female-specific or sex-difference analysis had over 25 female SRC athletes, with an average of just over 18 subjects (532 subjects over the 29 reports). Overall, our results demonstrate that there are >3 concussed male athletes studied for every concussed female athlete (7,600 male vs. 2,500 female athletes total). Given that effect sizes for neuroimaging and fluid-based biomarker changes resulting from SRC are typically small, these studies are likely underpowered to find effects of SRC. Thus, we cannot rule out that the lack of significant findings, including interactions, across the biomarker studies we summarized might be driven by the small sample sizes. In fact, 3 of the 29 reports included “preliminary” in the title. While conducting studies that include a focus on female athletes is a step in the right direction, novel biomarkers or biomarker thresholds developed without adequate female inclusion might lead to misinterpretation of diagnostic or prognostic information. Thus, we provide the following recommendations related to the inclusion and study of female athletes for concussion research moving forward.
Transparency, Rigor, and Reproducibility Statement
The protocol for this scoping review was registered through Open Science Framework (https://doi.org/10.17605/OSF.IO/XQ2US). PRISMA-ScR guidelines were used in designing and conducting the review. Searches conducted in MEDLINE, Scopus, Cochrane, and PsycInfo used standard search methods (see Supplement for sample search strategy). Two reviewers verified inclusion of studies and data extraction, with conflicts resolved by a third reviewer.
Authors’ Contributions
R.M., T.B.M., B.D.G., and E.M. contributed to the conceptualization of this study. O.O. was responsible for data curation. B.D.G., E.M., H.M.F., E.F., M.J.A., and T.B.M. were involved with investigation and validation. B.D.G. and E.M. prepared the original article draft. B.D.G. also conducted the formal analysis and was project administrator. All authors assisted with review and editing of the article.
Availability of Data and Material
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Footnotes
Acknowledgments
The authors thank Saishreyans Beeram and Nicholas Weyenberg at the Medical College of Wisconsin for assistance in the screening process.
Author Disclosure Statement
R.M. reports funding from Abbott Laboratories, the National Football League, the Department of Defense, and the National Institutes of Health. T.B.M. reports in-kind research support from Abbott and has previously received compensation as a member of the Clinical and Scientific Advisory Board for Quadrant Biosciences Inc. All other authors have no conflicts of interest to declare.
Funding Information
There was no funding provided for this research.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.