
Abstract
The Integrated Neurological Change Score (INCS) combines changes in sensory and motor subscores from the International Standards for Spinal Cord Injury Classification (ISNCSCI) into a composite measure. We evaluated the INCS sensitivity to therapeutic outcomes, robustness against ceiling effects, and association to functional improvement in patients with acute cervical spinal cord injury (SCI). To this end, we conducted a retrospective analysis of data from the Nogo Inhibition in Spinal Cord Injury (NISCI) clinical trial alongside a matched cohort from the European Multicenter Study about Spinal Cord Injury (EMSCI). The NISCI trial assessed the safety and efficacy of the anti-Nogo-A antibody (NG-101) in acute cervical SCI, reporting a potential therapeutic effect in motor incomplete patients. Our findings show that the sensitivity of INCS to the effect of NG-101 is comparable to that obtained employing the changes in the Upper Extremity Motor Score (the primary outcome in the NISCI trial). Moreover, the INCS is less susceptible to ceiling effects compared to measures of upper and lower extremity or total motor scores, as observed in the NISCI trial and in the matched EMSCI cohort. This robustness may facilitate the design of more inclusive clinical trials without compromising statistical power. Finally, INCS correlates strongly with functional outcomes in self-care and walking ability, outperforming ISNCSCI motor scores. In conclusion, the INCS represents a sensitive measure of neurological change corroborating the value of ISNCSCI standards for use in SCI trials.
Keywords
Introduction
Spinal cord injury (SCI) imposes a profound impact on patients’ lives, leading to neurological impairments that reduce independence and quality of life. The substantial health consequences and economic burden associated with SCI underscore the urgent unmet need for effective therapeutic interventions. In the last decades, significant advances in preclinical research have led to the identification of potential targets to enhance neurological recovery. However, translating these promising preclinical findings into meaningful clinical recovery remains challenging. In addition to economic, technical, and medical hurdles, the choice of primary outcome plays a crucial role in shaping trial design and influences its inclusiveness and ability to reliably assess therapeutic effects.1–4
The most common clinically meaningful outcome measure in neurorestorative SCI clinical trials is the improvement in neurological function assessed according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI).5,6 The choice of ISNCSCI classification or motor or sensory subscores to select as primary outcomes should consider not only the type of intervention being tested but also its target population. Once a primary end-point is selected, the high variability in neurological deficits and recovery trajectories among patients requires a careful patient stratification to balance natural recovery across experimental groups. While ISNCSCI reliably standardizes neurological function assessment, relying on a single measure presents limitations: first, a single ISNCSCI subscore cannot fully capture the multifaceted nature of neurological recovery, which often involves diverse combinations of motor and sensory gains at various spinal cord levels. Second, these subscores frequently exhibit ceiling effects, particularly in individuals with motor incomplete injuries, where spontaneous recovery is more common. Excluding those individuals and, therefore, reducing clinical trial inclusiveness, is the consequent trade-off to reliably assess the true effect of an intervention.
To address these challenges, we introduced the Integrated Neurological Change Score (INCS), 7 a composite score designed to provide a more holistic and robust measure of change in neurological function. Briefly, INCS integrates changes in motor and sensory function, as assessed by the ISNCSCI exam, into a single value. INCS ranges between −1 and + 1, where −1 indicates complete loss of the sensorimotor function that was preserved at the baseline and + 1 indicates full recovery of the sensorimotor function absent at the baseline. This approach offers a comprehensive representation of a patient’s overall neurological progress and has been proven to align more closely with expert assessments of recovery than individual ISNCSCI subscore changes (ΔUEMS, ΔLEMS, ΔTPP, and ΔTLT), American Injury Association Impairment Scale (AIS) grade conversion, or change in the Neurological Level of Injury. 7 The INCS has been applied in acute SCI to explore novel blood biomarkers that predict recovery,8,9 but its utility as an outcome for clinical trials has not yet been evaluated.
Here we present a retrospective analysis using data from the Nogo Inhibition in Spinal Cord Injury (NISCI) clinical trial alongside matched historical controls from the EMSCI study. The NSICI trial tested the safety and efficacy of an anti-Nogo-A antibody (NG-101) on patients with cervical SCI by selecting as the primary outcome the difference in the Upper Extremity Motor Score (UEMS) from baseline to 168 days post-baseline between NG-101 and placebo groups.10,11 Patients were stratified according to the expected outcome, and those predicted to be affected by a ceiling effect on UEMS were excluded. The full cohort analysis resulted in no statistically significant effects of NG-101 treatment, but post hoc analysis of motor incomplete patients uncovered a significant improvement in UEMS compared to the placebo that was paralleled by an increase in spinal cord injury independence measure (SCIM) of self-care. In this study we aimed to evaluate the ability of the INCS to capture neurological changes in patients with cervical motor-incomplete SCI as well as its resistance to ceiling effects. We also assessed its association with functional independence to further demonstrate the potential value of INCS as an outcome measure for future SCI trials.
Materials and Methods
Data sets
Two different datasets were analyzed: (1) the NISCI clinical trial (NCT03935321) database and (2) the European Multicenter Study about Spinal Cord Injury (EMSCI, NCT01571531).
The NISCI trial has been described in detail. 10 Briefly, it was a multicenter, placebo-controlled, randomized phase 2b clinical trial to test the efficacy and safety of NG-101, a Nogo-A-blocking antibody. Patients aged 18–70 years with a cervical SCI at 4–28 days after injury were eligible. The primary end-point was the difference in UEMS from baseline (1 day before the intervention starts) to 6 months post-baseline between NG-101 and placebo groups. Patients were assigned to placebo or NG-101 in a 1:2 ratio and stratified according to the expected UEMS recovery based on unbiased recursive partitioning (URP).12–14 Patients with UEMS > 28 at screening were excluded due to predicted ceiling effects. Placebo (phosphate-buffered saline, PBS) or NG-101 dissolved in PBS (45 mg/injection) were administered intrathecally six times every 5 days. Neurological function was assessed according to the ISNCSCI at the screening exam, the day before beginning the intervention (baseline exam), and once completing the treatment, at 30-, 84-, and 168 days post-baseline. Functional independence was also assessed according to the SCIM15,16 at the same time points. The final sample size of the NISCI trial is equal to 126 participants.
EMSCI (www.emsci.org), a network of SCI centers located primarily across Europe, prospectively collects data from patients with acute traumatic SCI using a standardized protocol. 17 This protocol includes ISNCSCI, SCIM, and additional assessments of functional independence, including the 6-min walking test, the Walking Index for Spinal Cord Injury (WISCI), and the Timed-Up and Go test (TUG). For the analysis in this study, we selected the scheduled EMSCI assessments that corresponded to the timepoints aligned with the NISCI follow-up timepoints (Supplementary Fig. S1): very acute (≤15 days after injury, aligned with the NISCI screening and baseline exams), acute I (4 weeks, 16–40 days, aligned with the NISCI screening and baseline exams), acute II (12 weeks, 70–98 days, aligned with NISCI exam at 84 days), and acute III (24 weeks, 150–186 days, aligned with NISCI trial end of follow-up). As of December 2024, the database used in this study includes 6702 patients.
Patient selection and characteristics
Among the 126 patients included in the NISCI full analysis set, we selected the 55 who sustained a motor incomplete SCI, that is, AIS C or D, at the baseline assessment and had complete ISNCSCI data both at the baseline and end-of-follow-up assessments. Patient demographic and clinical characteristics are shown in Table 1. A flowchart showing the patient selection process is shown in Supplementary Figure S2A.
Clinical and Demographic Characteristics of the Selected Patients with Motor-Incomplete Spinal Cord Injury
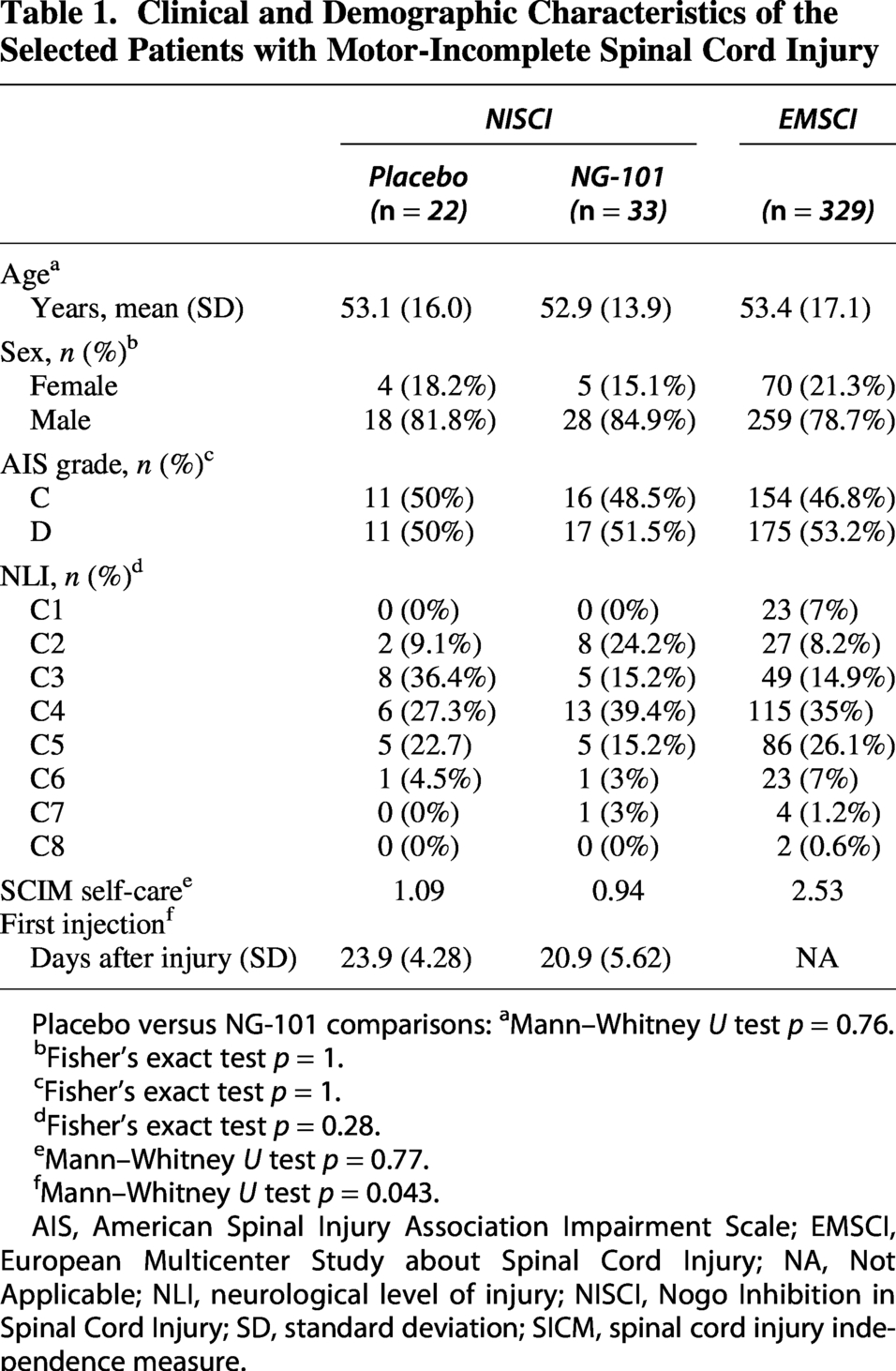
Placebo versus NG-101 comparisons: aMann–Whitney U test p = 0.76.
Fisher’s exact test p = 1.
Fisher’s exact test p = 1.
Fisher’s exact test p = 0.28.
Mann–Whitney U test p = 0.77.
Mann–Whitney U test p = 0.043.
AIS, American Spinal Injury Association Impairment Scale; EMSCI, European Multicenter Study about Spinal Cord Injury; NA, Not Applicable; NLI, neurological level of injury; NISCI, Nogo Inhibition in Spinal Cord Injury; SD, standard deviation; SICM, spinal cord injury independence measure.
Among the 6702 patients included in the EMSCI study, we selected those with cervical, motor incomplete (AIS C or D) injuries at the very acute stage. Among these patients, we selected those with complete ISNCSCI assessments at the very acute, acute I, acute II, and acute III stages. The demographic and clinical characteristics of the 329 selected patients, matched to those selected from the NISCI trial, are shown in Table 1. A flowchart illustrating the patient selection process is shown in Supplementary Figure S2B.
INCS calculation
There are two INCS estimation procedures: for tetraplegia, differences between two ISNCSCI assessments in UEMS, Lower Extremity Motor Score (LEMS), Total Pin-Prick score (TPP), and Total Light Touch score (TLT) are incorporated; for paraplegia, UEMS is excluded since upper extremity motor function is preserved and therefore does not change. INCS for the patients analyzed in this study (tetraplegia) was calculated as previously described.
7
Briefly, the changes in the ISNCSCI subscores—ΔUEMS, ΔLEMS, ΔTPP, and ΔTLT—were individually relativized to the margin of maximum improvement or maximum worsening, depending on whether changes are positive or negative. INCS were then calculated as the linear combination of the relativized changes –ΔUEMSr, ΔLEMSr, ΔTPPr, and ΔTLTr—according to the formula:

The INCS original article 7 includes an Excel-based INCS calculator that automates the steps described above, requiring only UEMS, LEMS, TPP, and TLT data from baseline and follow-up (URL link). Code implemented in R and examples of use to calculate INCS can be found at the Zenodo repository, DOI 10.5281/zenodo.20325012.
Since INCS is an integrative measure of the overall neurological change between two given examinations, its value at the baseline was set as zero. At all other time points, INCS was calculated as the change from the baseline.
Validation of INCS loadings
The loadings for each relativized difference within the INCS for tetraplegia (Eqn. 1) were estimated based on neurological changes between 4 and 52 weeks in 312 patients from the Sygen clinical trial. 7 To assess the robustness of these loadings, we re-estimated them using data from the EMSCI trial, aligning the time interval with the original study (31.5–343 days post-injury; Supplementary Table S1). Tetraplegia was defined as the presence of UEMS deficits at either the baseline or the second time point. Patient demographics are summarized in Supplementary Table S1.
Loadings were estimated following the original methodology. Briefly, differences in UEMS, LEMS, TPP, and TLT were relativized to the margin for maximum improvement (for positive changes) or worsening (for negative changes). Subsequently, a Principal Component Analysis based on singular value decomposition—without centering or scaling—was applied to the relativized changes. Principal Component 1 loadings were then estimated using 100,000 bootstrap iterations using the boot package 18 for R statistical software. 19 The mean bootstrapped loading estimates for each relativized difference (ΔUEMSr, ΔLEMSr, ΔTPPr, and ΔTLTr) were divided by their sum to obtain the final re-estimated INCS loadings.
Stratification of patients according to the expected ceiling of UEMS or LEMS
The NISCI trial excluded patients with an UEMS > 28 at the screening exam, a cut-off established by URP to separate those predicted to be affected by a ceiling effect on UEMS at the end of follow-up. 10 In addition, two subgroups with different UEMS expected recoveries were established by URP within the UEMS > 28 group: 28 < UEMS ≤ 38 and UEMS > 38. These cut-offs have been applied where indicated to the EMSCI data used in this study.
Ceiling may also occur in other secondary outcomes, such as LEMS, which were not considered in the initial stratification for the NISCI trial. While the focus was on recovery of UEMS in cervical SCI, a comprehensive assessment of motor recovery in both upper and lower extremities in cervical motor incomplete patients is also relevant. To account for a potential ceiling of the LEMS, URP was applied to patients included in the EMSCI study using the party package 12 for R statistical software. 19 A cut-off at LEMS > 36 was established to separate patients predicted to be affected by ceiling effects on LEMS and applied where indicated to NISCI and EMSCI data.
Statistical analysis
All statistical analyses were done using R statistical software (version 4.4.2, macOS). 19
Linear mixed-effects models
Linear mixed-effects models (LMMs) were adjusted using the lmer function from the lme4 package in R. 20 To ease interpretation of results, time was standardized so baseline was equal to zero and the end of NISCI trial follow-up, 168 days post-baseline, equal to 1. LMMs were adjusted to estimate (1) the effect of the interaction of time and NG-101 treatment on UEMS, TMS and LEMS trajectories, (2) the effect of the interaction of time and stratification according to expected ΔLEMS ceiling on LEMS, TMS, or UEMS trajectories, and (3) the effect of the interaction of time and stratification according to expected ΔUEMS ceiling on UEMS trajectories. The fixed-effect structure included the stratification group, time, and their interaction to test whether the rate of recovery over time is dependent on the initial UEMS or LEMS. Random intercepts and time slopes were included for each subject.
Nonlinear mixed-effects models
To estimate the effect of time and treatment on INCS, a nonlinear mixed-effects model was adjusted using the nlme function from the nlme package
21
in R. The INCS reflects overall neurological change between two time points, rather than the neurological status at a single time point. Given this and the fact that INCS trajectories start at zero at baseline regardless of treatment or stratification group, we fitted exponential asymptotic mixed-effects models with intercept values equal to zero, according to:

Where b0 represents the asymptote, 
Exponential asymptotic mixed-effects models were used to study the effect of (1) treatment, (2) stratification according to expected LEMS ceiling, and (3) stratification according to expected UEMS ceiling on INCS. The effect of treatment or stratifications were incorporated in their corresponding models as fixed-effect covariate both on the logarithm of rate constant (
Effect size and power estimation
The effect size of NG-101 treatment on INCS, ΔUEMS, ΔLEMS, ΔTLT, ΔTPP, ΔTMS, and ΔSCIM self-care from baseline to end of NISCI trial follow-up was estimated according to Cohen’s d using the effectsize R package. 22
The effect size of ΔUEMS, ΔLEMS, ΔTLT, ΔTPP, ΔTMS, and ΔSCIM self-care was compared to that of INSC by bootstrapping 1000 times their differences with resampling stratified by treatment group using the boot R package. 18 Then, bias corrected and accelerated 95% confidence intervals were estimated.
Power was estimated using the pwr.t2n.test function from the pwr R package. 23
Correlation analysis
Nonparametric Spearman’s rho was calculated to study the association of different measures of change in the neurological function –INCS, ΔUEMS, ΔLEMS, ΔTLT, and ΔTPP– with changes in functional independence –ΔSCIM self-care–, and mobility outdoors –ΔSCIM Section 14. The correlations of the ΔUEMS, ΔLEMS, ΔTLT, and ΔTPP with measures of functional recovery were compared with that of INCS by bootstrap as described above, using the boot R package.
Statistical tests for group comparison
Comparison of median raw ΔUEMS, ΔLEMS, ΔTMS and INCS between treatment (NG-101 vs. placebo) or stratification groups (LEMS > 36 vs, LEMS ≤ 36 or UEMS > 28 vs. UEMS ≤ 28) was done applying the Mann–Whitney U test both for NISCI and EMSCI data.
Comparison of ΔUEMS or INCS across UEMS ≤ 28, 28 < UEMS ≤ 38 and UEMS > 38 groups was done by the Kruskal–Wallis test after rejecting the normal distribution of ANOVAS’ residuals by a Shapiro–Wilk test. Post hoc comparisons were performed by the Dunn’s test.
Results
Validation of INCS loadings
We validated the INCS loadings initially derived from the Sygen database (clinical trial in acute traumatic SCI spanning from 4 to 52 weeks post-injury) by comparing them with EMSCI data that were selected for the same time interval after injury, while not adjusting patient profiles such as age and frequency of incomplete lesions (Supplementary Table S1). Despite these differences, the EMSCI-based loadings were remarkably similar to the original INCS estimates (0.3492 for ΔUEMS, 0.2938 for ΔLEMS, 0.1699 for ΔTPP, and 0.1870 for ΔTLT; Fig. 1). Indeed, the Tucker’s congruence coefficient between the two sets of loadings is 0.9961. According to established criterion, 24 this value confirms that both composite scores are virtually identical and, consequently, represent the same phenomenon. This robustness in loading estimation ensures that applying the EMSCI-based loadings yields composite values and changes over time (recovery profiles) nearly identical to those of the original INCS across the different severity categories of acute SCI (AIS A-D, Fig. 1C).
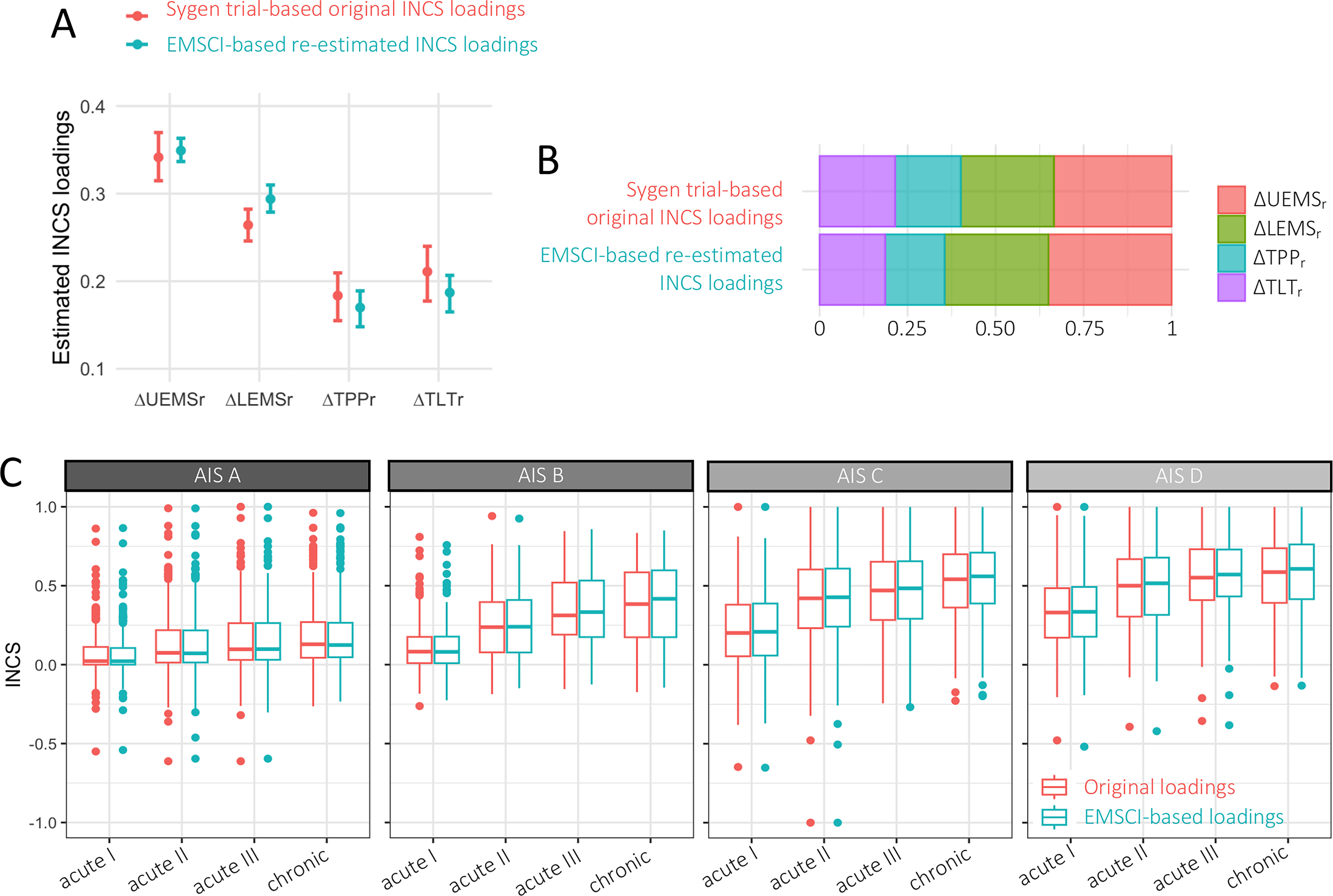
External validation of INCS loadings.
Sensitivity of INCS to reveal NG-101-treatment effects
The NISCI trial did not meet its primary end-point in the full cohort analysis, but a significant therapeutic effect of NG-101 treatment was observed by post hoc analysis of the motor-incomplete participants (4.40 points higher ΔUEMS in NG-101-treated compared to the placebo group, n = 63). 10 In agreement, a linear mixed-effects model fitted to the sample of NISCI’s motor-incomplete patients used in this study (n = 55, complete ISNCSCI assessments at baseline and end of follow-up) shows that change in UEMS from baseline to 168 days was 4.28 points higher among patients treated with NG-101 (95% CI: 0.5234 to 8.0376; Fig. 2A and Supplementary Table S2). Comparing the median raw difference in UEMS (ΔUEMS) between placebo and NG-101-treated groups failed to reach statistical significance (p = 0.059; Fig. 2B).
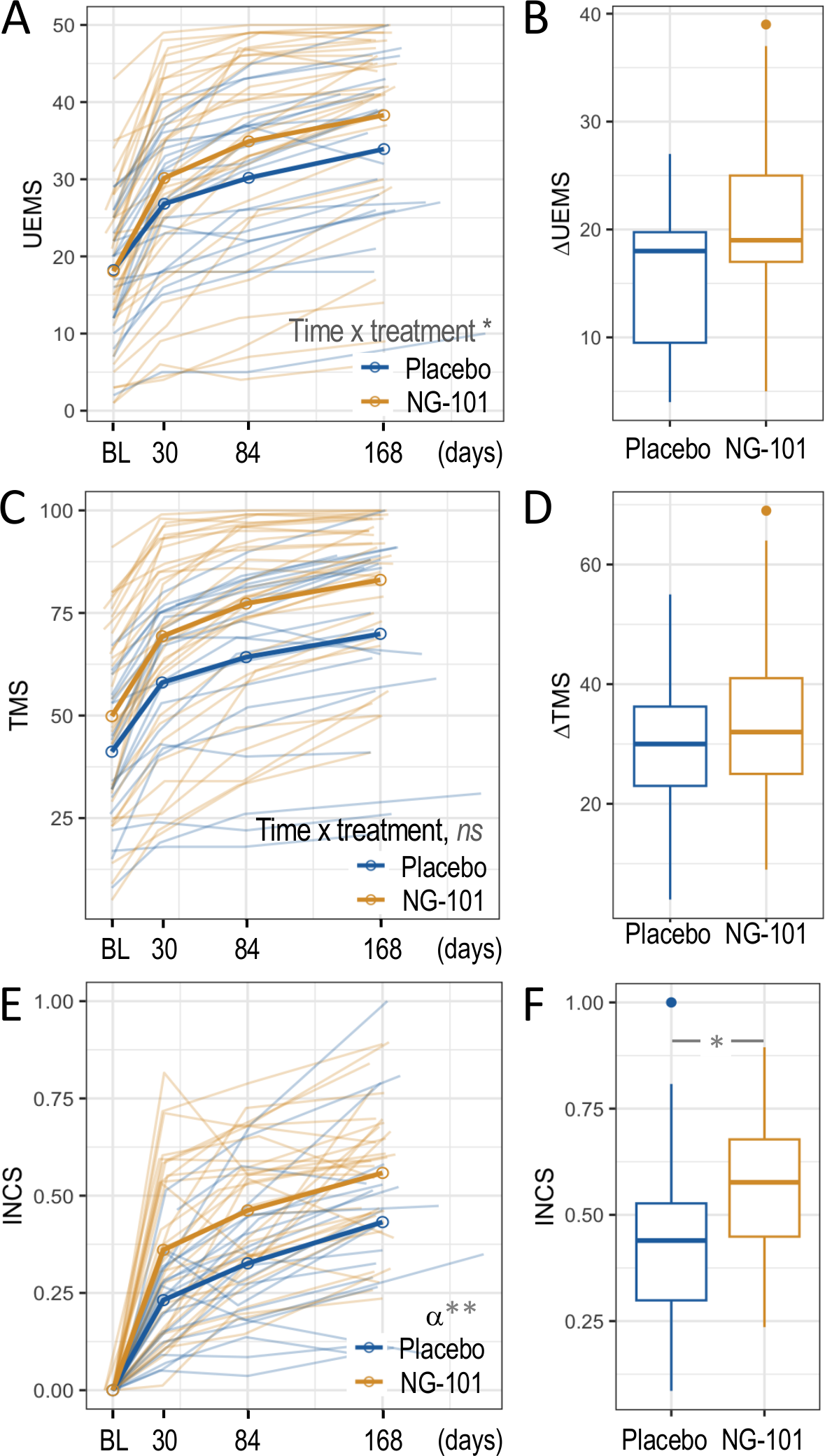
Sensitivity of INCS assessments to reveal NG-101 treatment effects using clinical trial data (NISCI data set).
A linear mixed-effect model failed to reveal any difference in TMS from baseline to 168 days between NG-101 and placebo groups (Fig. 2C and Supplementary Table S2). Also, no difference was observed in the ΔTMS between NG-101 and placebo patients (Fig. 2D).
When employing INCS as the outcome of interest, an asymptotic exponential mixed-effects model shows that NG-101 treament increased the logarithm of rate constant by 0.527 compared to the placebo group (standard error (se), 0.16; p value, 0.0019: Figure 2E). In other words, the growth rate was 1.6 times higher in the NG-101 compared to the placebo group. The adjusted model did not result in a significantly higher effect in the long term (p = 0.091 for the difference between the asymptotes of the NG-101 and placebo groups; Supplementary Table S3). However, the median raw INCS from baseline to 168 days was significantly higher among the NG-101-treated compared to the placebo group (0.57 vs. 0.44; p = 0.019; Fig. 2F). Therefore, the results show that the therapeutic effect of NG-101 assessed by change in UEMS is well detectable by using INCS.
Estimation of treatment effect size by INCS
Effect sizes were estimated by Cohen’s d for INCS and its constituent variables (Table 2). Only Cohen’s d for INCS and ΔUEMS were significantly different from zero. For all other variables (ΔLEMS, ΔTPP and ΔTLT, and ΔTMS), the confidence interval included zero, so a reliable treatment effect could not be estimated. Effect sizes of INCS and ΔUEMS were similar, a medium effect size of 0.63 vs. 0.62, corresponding with an achieved power of 0.61 and 0.60, respectively (Table 2). Differences between the effect sizes achieved by INCS and ΔUEMS were not found to be significantly different when estimated by bootstrapping. Also, bootstrap estimates of the difference between INCS and ΔTMS, ΔLEMS, ΔTPP or ΔTLT were not found to be statistically significant (Table 2). Therefore, our results show that sensitivity of INCS to the effect size of NG-101 treatment is similar to that of ΔUEMS, the individual ISNCSCI subscore exhibiting the maximum sensitivity.
Effect Size and Achieved Statistical Power of Anti-Nogo-A Antibody Treatment by Means of Integrated Neurological Change Score Compared to International Standards for Spinal Cord Injury Classification Subscores and Spinal Cord Injury Independence Measure Outcomes
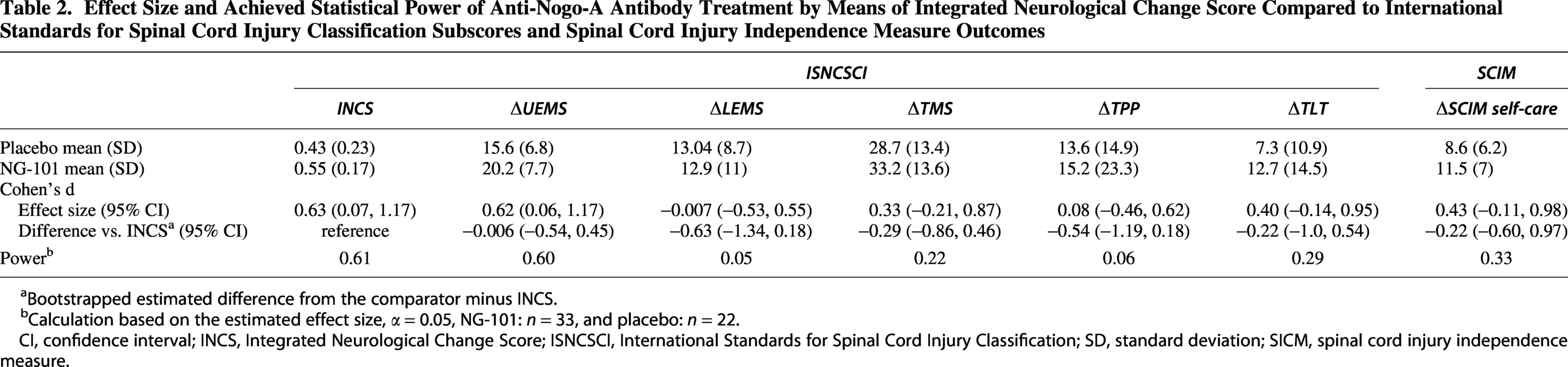
Bootstrapped estimated difference from the comparator minus INCS.
Calculation based on the estimated effect size, α = 0.05, NG-101: n = 33, and placebo: n = 22.
CI, confidence interval; INCS, Integrated Neurological Change Score; ISNCSCI, International Standards for Spinal Cord Injury Classification; SD, standard deviation; SICM, spinal cord injury independence measure.
We also aimed to compare the sensitivity of INCS to NG-101 treatment with a measure of functional recovery, ΔSCIM self-care, since it was found to be significantly enhanced by NG-101 treatment during the NISCI trial. 10 In our study, the effect size when comparing ΔSCIM self-care between NG101 and placebo (small effect size of 0.43) was lower than that for INCS, but the difference was not found to be significantly different when estimated by bootstrap (Table 2).
INCS to account for ceiling effects
The NISCI trial excluded patients with an UEMS > 28 at the screening exam, predicted to be affected by a ceiling effect when applying UEMS scores at the end of follow-up, since this would challenge the analysis of the total benefit obtained from the intervention. 10 Using historical controls from the EMSCI study, we observed the expected ceiling effect of UEMS among patients with UEMS higher than 28 at baseline (Fig. 3). A linear mixed-effects model estimated a difference of 5.74 UEMS points from baseline to 168 days (95% CI: 4.77 to 6.72; Fig. 3A; Supplementary Table S2) between the group with UEMS ≤ 28 at baseline compared to that with UEMS > 28. Also, the median ΔUEMS was higher in the UEMS ≤ 28 group (20 vs. 10 for the UEMS > 28 group; p < 2·10−16; Fig. 3B).
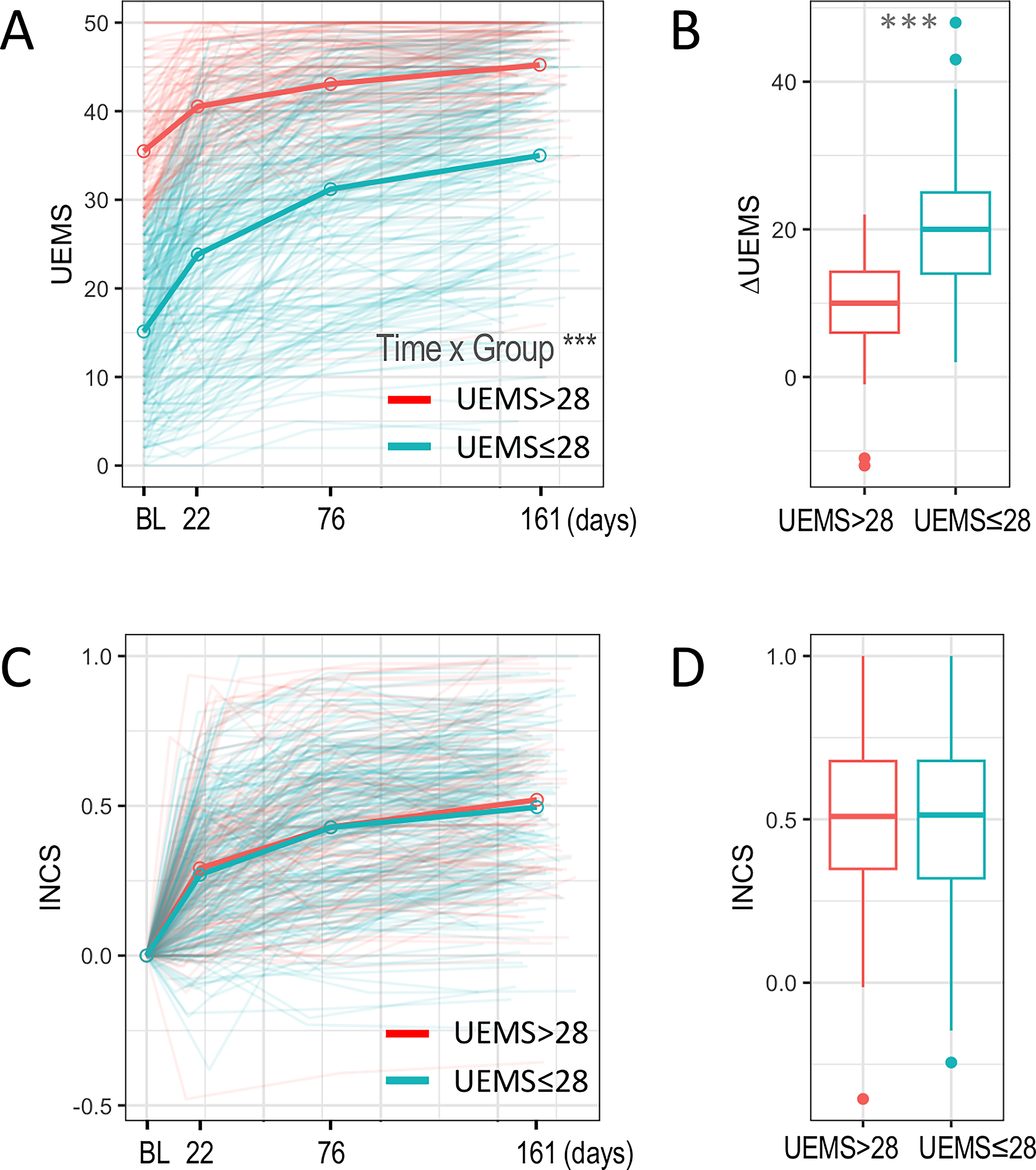
Comparison of ceiling effects using UEMS and INCS in historical controls (EMSCI data set).
However, we did not observe a ceiling effect for the INCS outcome in patients with UEMS > 28 at baseline. There was no significant difference in the rate constant (ratio between UEMS ≤ 28 and UEMS > 28 groups, 0.96; p value = 0.57; Fig. 3C; Supplementary Table S3) nor in the estimated asymptote for each group (difference between UEMS ≤ 28 and UEMS > 28, −0.017; p value, 0.54; Fig. 3C). Median INCS between baseline and end of follow-up did not differ between both groups (0.513 for the UEMS ≤ 28 group and 0.508 for the UEMS > 28 group; p value = 0.50; Fig. 3D).
INCS to facilitate inclusive clinical trial designs
Among the 329 patients included in the analysis of historical EMSCI controls, 108 (32.8%) presented with UEMS > 28 (Fig. 4A). Of them, 74 (22.5%) presented with 28 < UEMS ≤ 38, and 34 (10.3%) presented with UEMS > 38 (Fig. 4A). Applying measures of ΔUEMS as a readout of recovery is already showing significant ceiling effects in patients with 28 > UEMS ≤ 38 that become extensive in UEMS > 38 (Fig. 4B). 10 In contrast, there was no difference in INCS between participants with UEMS > 38, 28 < UEMS ≤ 38, and UEMS > 38 (Fig. 4C).
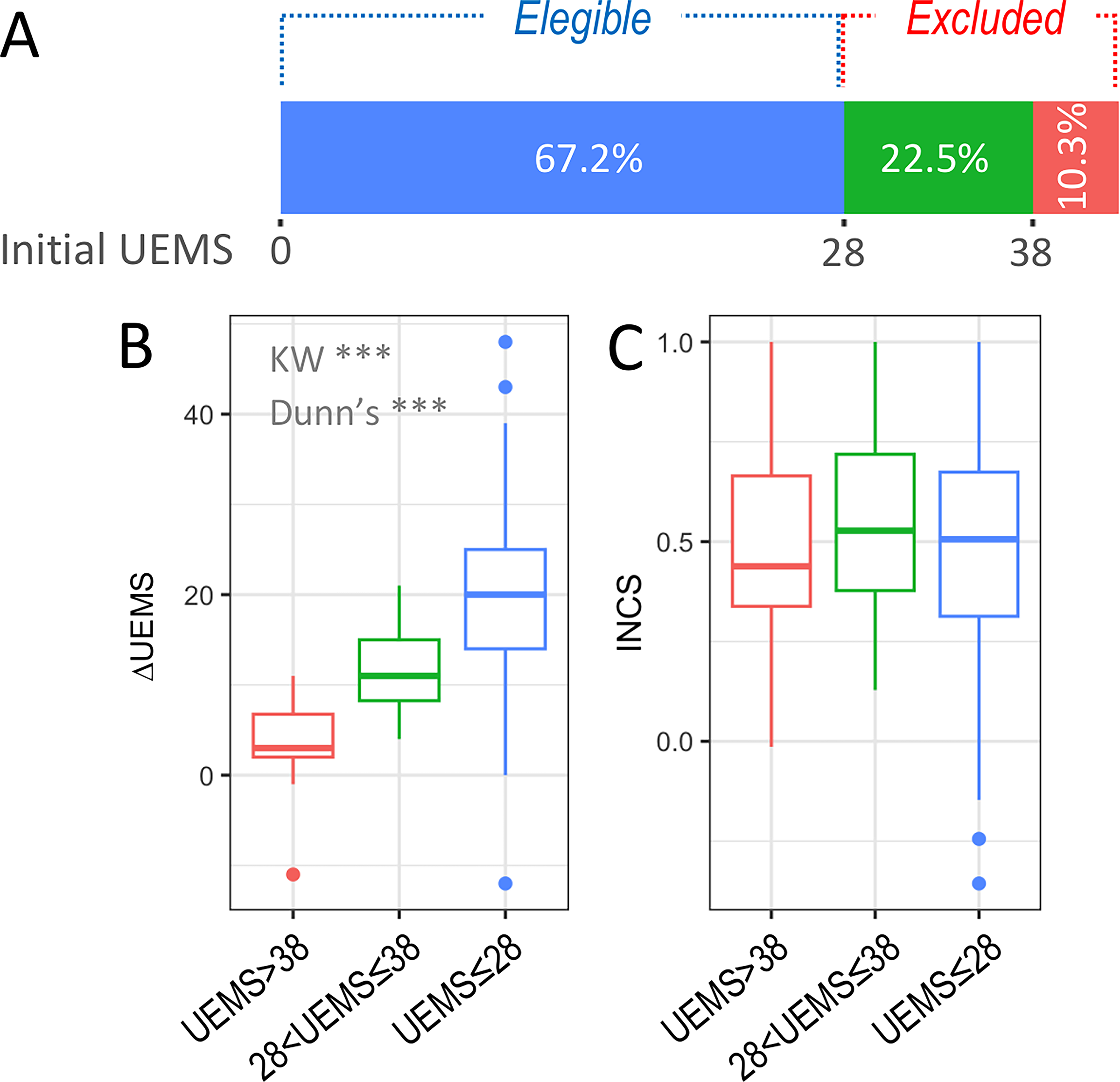
Evaluation of inclusiveness of INCS using EMSCI historical controls (EMSCI dataset).
Relation of INCS to LEMS outcomes
To reveal ceiling effects of LEMS outcomes, URP was applied to EMSCI data (n = 525) to predict LEMS outcomes and predefine cohorts of patients with a likely ceiling effect of LEMS. In patients with LEMS > 36 at the acute stage (representing 29.9% of total patients), a ceiling effect was seen in 73% (n = 115/157) of patients (EMSCI acute III stage; Fig. 5A). Moreover, LEMS trajectories differed between those with LEMS ≤ 36 and LEMS > 36 (linear mixed-effect model estimated difference between groups: 7.3; 95% IC 6.2 to 8.4; Fig. 5B; Supplementary Table S2). Lastly, raw median ΔLEMS was significantly lower in patients showing a significant ceiling effect (LEMS > 36; Fig. 5C).
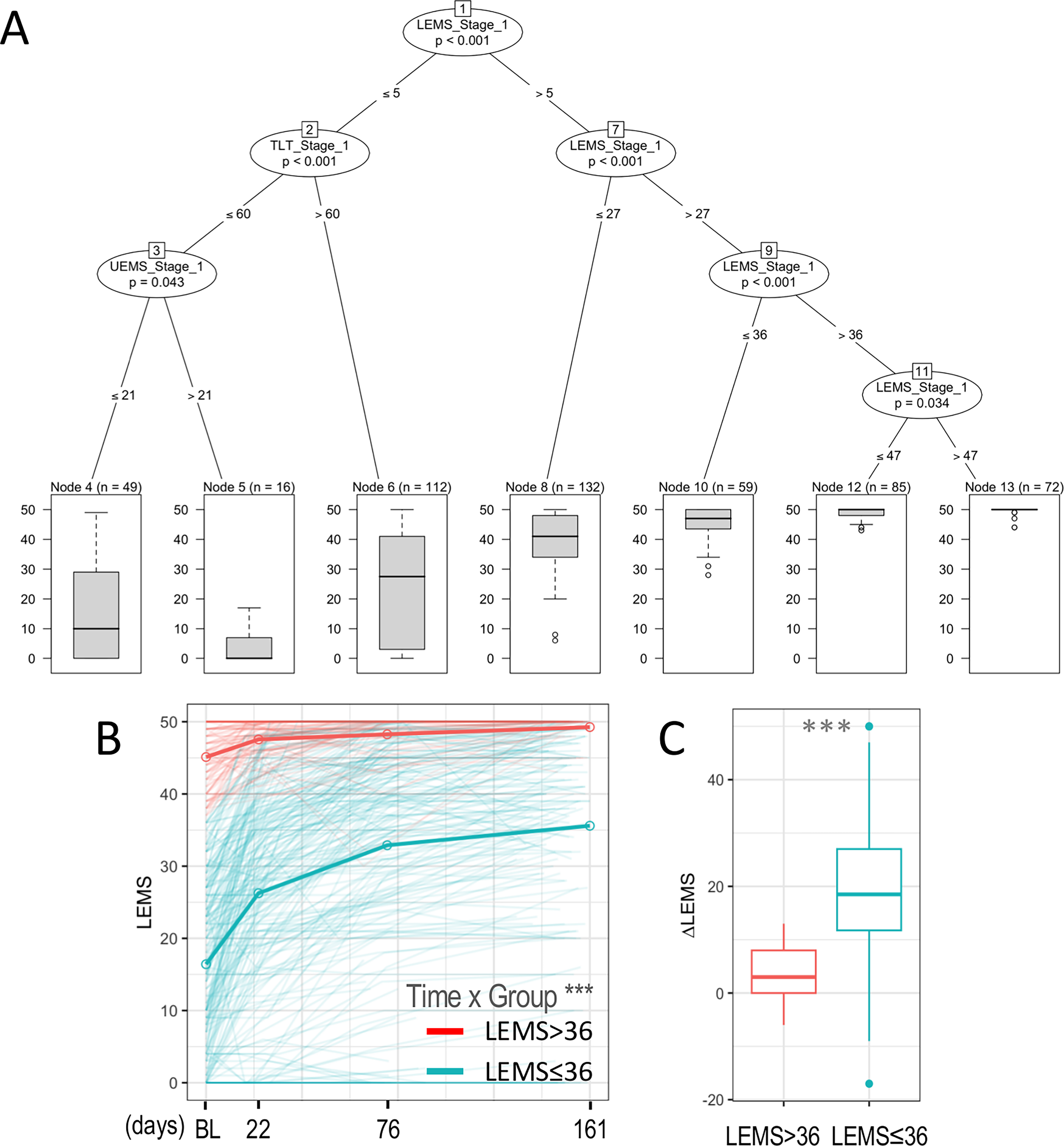
Stratification of LEMS outcomes in acute SCI (EMSCI dataset).
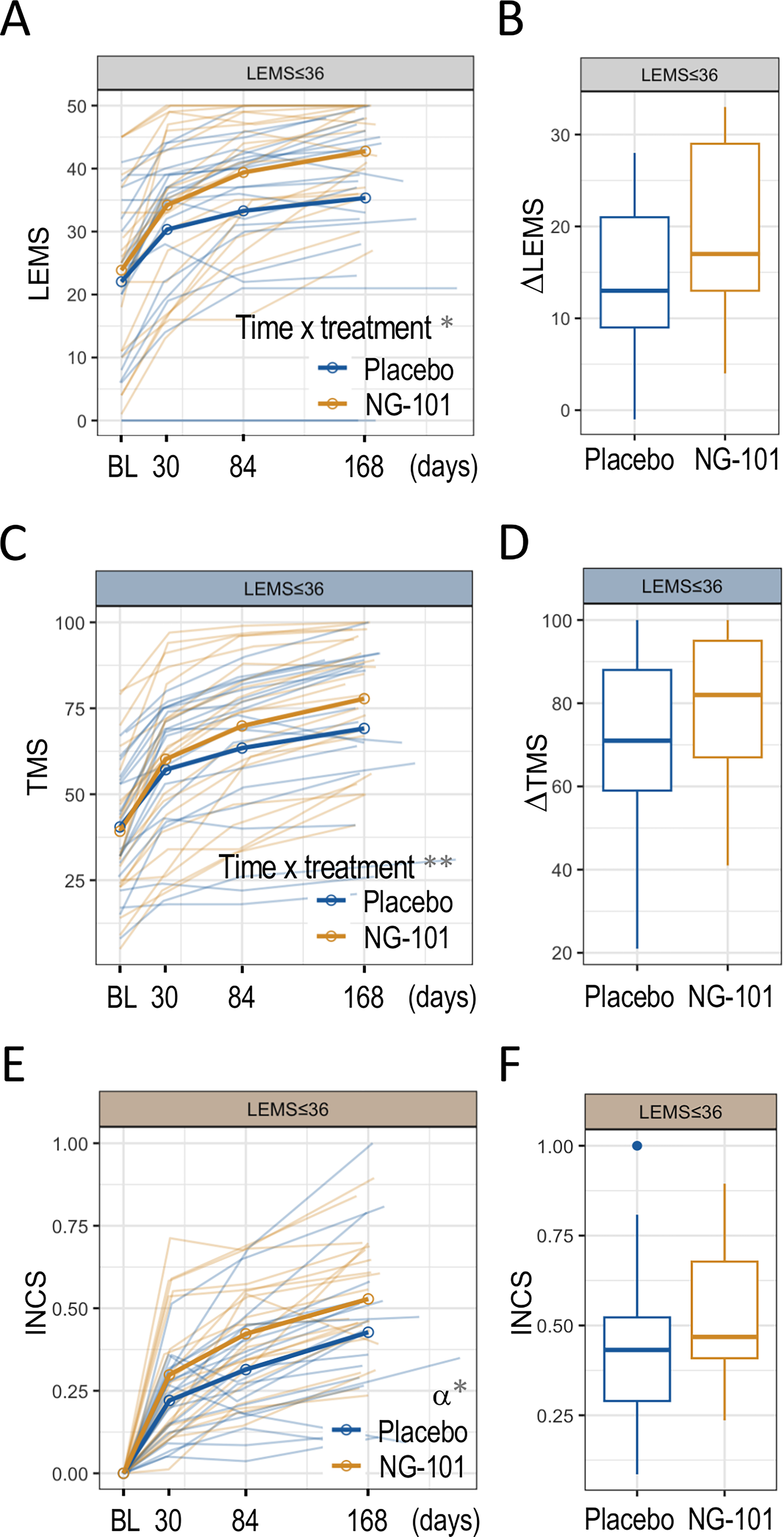
Accordingly, in the NISCI trial, 77% (n = 10) of motor incomplete patients with LEMS > 36 at screening reached the maximum LEMS (50 points) by the end of follow-up. In those with LEMS ≤ 36 at screening, 19% (n = 8) reached the maximum by the end of follow-up. (Fig. 6A). A linear mixed-effects model of the NISCI trial data showed a significant difference in LEMS along the follow-up period between LEMS ≤ 36 and LEMS > 36 groups (difference, 12; 95% CI: 7 to 17.1; Fig. 6A; Supplementary Table S2). In addition, median raw ΔLEMS between baseline and end of follow-up was significantly lower in the LEMS > 36 group (Mann–Whitney p = 0.00003; LEMS ≤ 36 median values: 16; LEMS > 36 median values: 2; Fig. 6B).
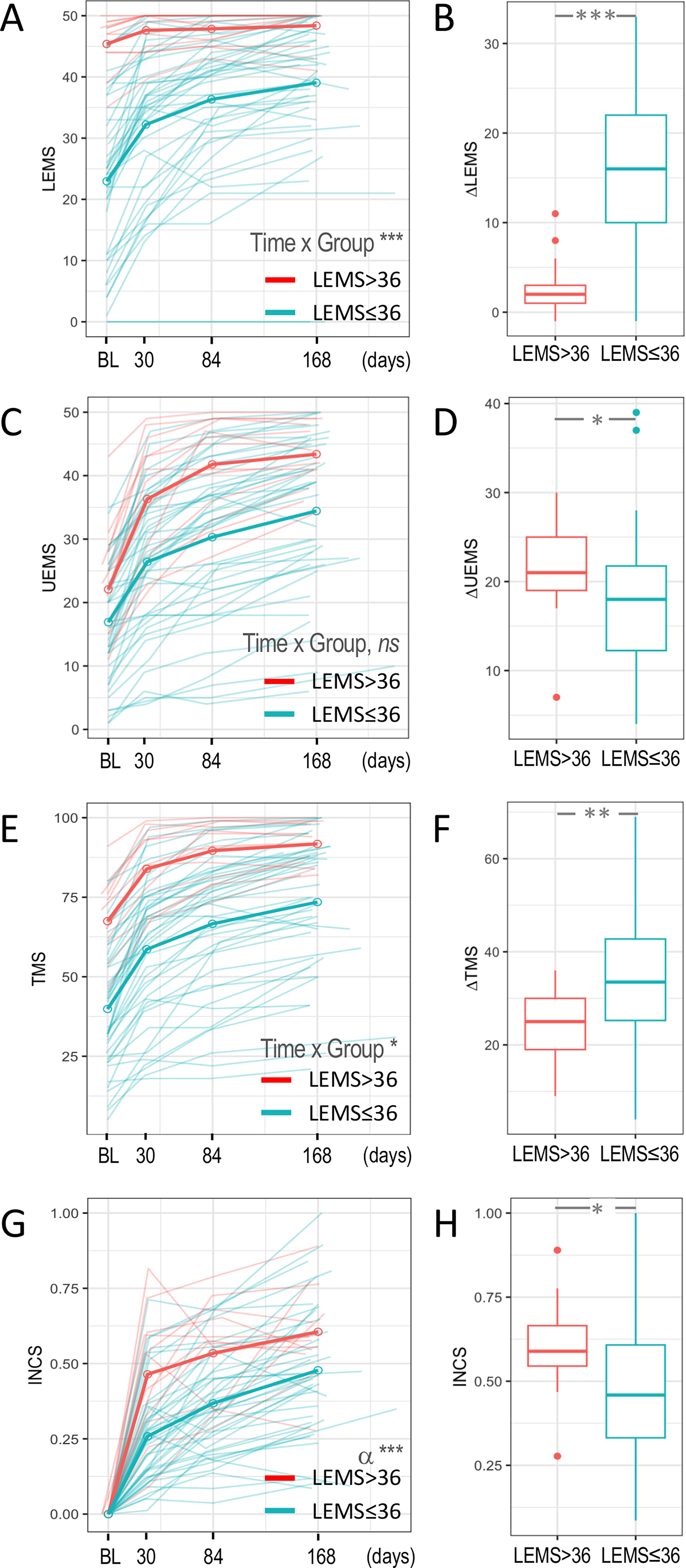
INCS is robust to the ceiling effects on ΔLEMS in the NISCI trial.
A linear mixed-effects model estimated a nonsignificant difference of −2.3 UEMS points from baseline to 168 days (95% CI: −7.12 to 2.3; Fig. 6C; Supplementary Table S2) between the group with LEMS ≤ 36 at baseline compared to that with LEMS > 36. However, median ΔUEMS from baseline to end of follow-up was significantly higher among patients with LEMS > 36 (21 vs. 18 for the LEMS ≤ 36 group; Mann–Whitney p = 0.038; Fig. 6D).
In motor incomplete cervical SCI patients, some preservation of both upper and lower limbs is expected, and therefore looking at the total motor score (TMS) or INCS may be applicable to estimate overall motor recovery and potentially compensate for LEMS ceiling effects.
When looking at the TMS changes, a significant ceiling effect was also observed for the LEMS > 36 group (difference between LEMS ≤ 36 and LEMS > 36, 9.5; 95% CI 1.48 to 17.5; Fig. 6E; Supplementary Table S2). The median ΔTMS from the baseline to the end of follow-up was lower in the LEMS > 36 group (33.5 for LEMS ≤ 36 and 25 for LEMS > 36; Mann–Whitney p = 0.009; Fig. 6F).
However, when integrating sensorimotor function into INCS, a nonlinear mixed-effects model showed that the rate constant was significantly lower in the LEMS ≤ 36 group (rate constant ratio, 0.53, p value 0.0003; Fig. 6G; Supplementary Table S3). These results were paralleled by lower median INCS from baseline to end of follow-up in the LEMS ≤ 36 compared to the LEMS > 36 group (0.46 vs. 0.59; Mann–Whitney p = 0.017; Fig. 6H). Therefore, INCS is not affected by the ceiling effect on ΔLEMS among patients with LEMS > 36 at the screening.
INCS to account ceiling effects of secondary outcomes
In addition to underestimating the true effect of an intervention, a ceiling of secondary outcomes may mislead one to conclude a lack of therapeutic effect when the ceiling is more prominent among the treatment group. In this regard, a lack of effect of NG-101 on LEMS trajectory is observed among the 55 patients studied (Supplementary Table S2). When the effect of NG-101 treatment is assessed only in the subgroup of patients predicted with no ceiling effect (LEMS ≤ 36 at the screening), a statistically significant effect of NG-101 on LEMS is observed (difference between NG-101 and placebo: 6.35, 95% CI: 1.28 to 11.43, Fig. 7A,B; Supplementary Table S2). Again, when using TMS as an outcome, no significant effect of treatment was observed among all the 55 patients (Fig. 2C; Supplementary Table S2). However, a significant effect of NG-101 is detected when only the subgroup free of ceiling effect (LEMS ≤ 36) is considered (linear mixed-effect model difference between NG-101 and placebo: 11.3; 95% CI: 3.77 to 18.72; Fig. 7C,D; Supplementary Table S2). In contrast, INCS detects the effect of NG-101 treatment among patients with LEMS ≤ 36 at the screening (Fig. 7E,F; Supplementary Table S3) but not among the whole sample of 55 motor incomplete patients (Fig. 2E–F).
Treatment effects on LEMS in the NISCI trial.
Statistical analysis was not performed for patients with LEMS > 36 at screening, as the inclusion of only 1 placebo patient in this subgroup precluded meaningful comparisons.
Correlation of INCS with functional outcomes
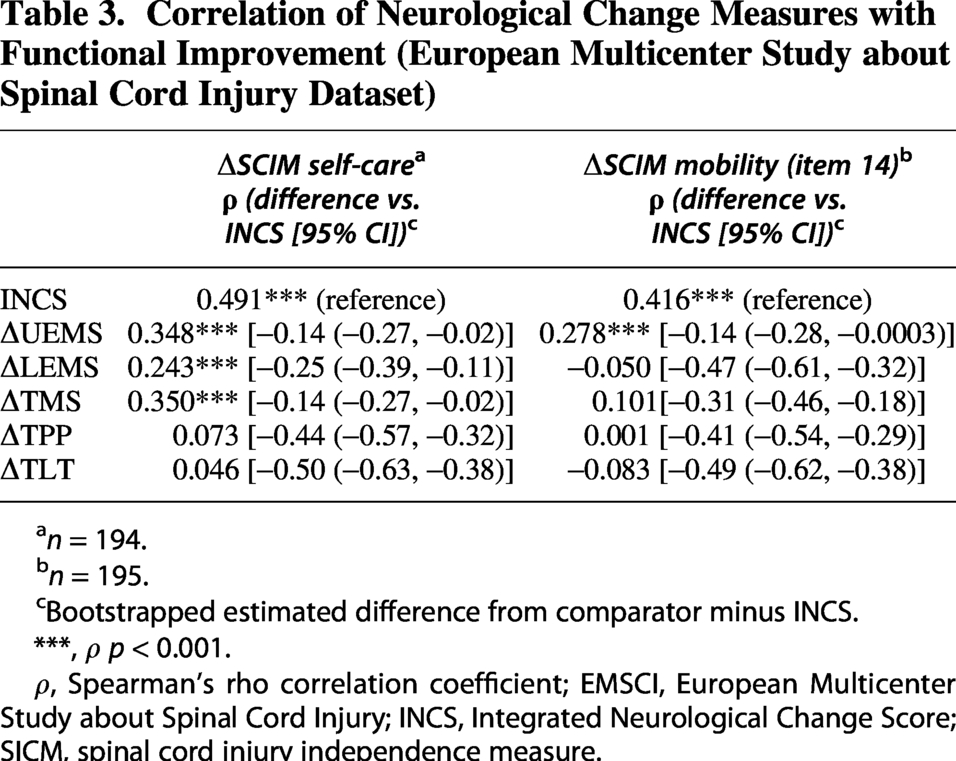
To estimate the relation of INCS with functional outcomes by means of SCIM-self-care and SCIM-mobility (item 14), the changes of neurological outcomes using ISNCSCI standard scores were compared to the measures of INCS using the EMSCI dataset. SCIM outcomes (self-care and mobility) correlated best with INCS outcomes, but less with ΔUEMS, ΔLEMS, and ΔTMS, and showing no relation to ΔTPP or ΔTLT (Table 3). Differences between the correlation of functional recovery with INCS and with all other ISNCSCI delta scores were estimated to be significant by bootstrap (Table 3).
Correlation of Neurological Change Measures with Functional Improvement (European Multicenter Study about Spinal Cord Injury Dataset)
n = 194.
n = 195.
Bootstrapped estimated difference from comparator minus INCS.
***, ρ p < 0.001.
ρ, Spearman’s rho correlation coefficient; EMSCI, European Multicenter Study about Spinal Cord Injury; INCS, Integrated Neurological Change Score; SICM, spinal cord injury independence measure.
Discussion
The definition of a specific clinical trial primary end-point has proven essential for the development of targeted interventions. However, many interventions in regenerative trials may affect several domains of neurological functions. We analyzed whether the application of the INCS for acute cervical SCI patients can improve an early translational trial. Our results indicate that INCS exhibits high sensitivity to neurological changes while demonstrating superior resistance to ceiling effects compared with UEMS, LEMS, and TMS, which enables the design and execution of more inclusive clinical trials.
The assessment of recovery after SCI and selection of the primary end-point have commonly relied on the changes in the subscores and classifications obtained according to the ISNCSCI protocol. In patients with tetraplegia, the assessment of UEMS is the clinically most relevant outcome to evaluate the effect of a therapeutic intervention, as recovery of upper limb function has the highest priority in these patients. 25 However, focusing on a single subscore may fail to capture other changes (both for subtle and strong changes) that in combination may better reflect the overall effect of the tested intervention. Consequently, integrative measures such as the Integrated Neurological Classification System (INCS) represent a viable alternative, provided (1) they rely on already well-established neurological items, that is, the INSCSCI protocol, (2) they robustly capture the relative contribution of each ISNCSCI subscore to global recovery, and (3) they do not artificially over or underestimate the effect of an intervention. Regarding the first requisite, our results demonstrate that the original INCS loadings estimated for patients with tetraplegia are remarkably consistent with re-estimated loadings derived from an independent cohort. To assess the second requisite, we compared recovery profiles and treatment effects when using INCS with differences in ISNCSCI motor and sensory subscores. As shown in Table 2, ΔUEMS is the only ISNCSCI-derived subscore achieving a significant treatment effect size based on its confidence interval; a reliable effect size could not be estimated for the three other variables integrated into INCS (ΔLEMS, ΔTPP, and ΔTLT). Applying the INCS in a retrospective analysis of the NISCI trial, the effect size remained almost identical to that of ΔUEMS. Therefore, in this specific setting, INCS effect size seems to reflect that of its unique constituent achieving a significant effect, rather than artificially overestimating the overall effect of the therapeutic intervention by including three other variables where an effect was not actually observed. And the contrary is also true: INCS is not underestimating the effect of the intervention, since INCS sensitivity compared to that of ΔUEMS is not burdened by a lack of treatment effect in ΔLEMS, ΔTPP, and ΔTLT. It remains to be explored how interventions with significant treatment effects in more than one motor or sensory subscore will affect the sensitivity of INCS.
A major strength of INCS is its reduced susceptibility to ceiling effects compared to conventional UEMS or LEMS outcomes. In the NISCI trial, patient stratification was performed based on predicted UEMS outcomes, which led to the exclusion of patients with UEMS > 28 at the screening, who are likely to show a ceiling effect. This resulted in 171 patients who did not meet eligibility for the NISCI trial, 37% of all the patients screened. 10 Our analysis suggests that using INCS instead of UEMS could have potentially allowed for the inclusion of these patients, rejected during the screening exam in the NISCI trial. EMSCI historical controls show similar numbers: using INCS instead of UEMS might increase the sample size by 33%. Employing INCS could thus facilitate more inclusive clinical trial designs (enrollment of less severely affected patients), potentially improving trial efficiency and enhancing the generalizability of findings. Alternatively, if UEMS were selected as the primary outcome and patients with an initial 28 < UEMS ≤ 38 were included to accelerate the recruitment, INCS as a secondary outcome might provide an alternative insight in case that modest residual ceiling effect on UEMS blurs the therapeutic effect being tested.
Given that patient stratification in the NISCI trial was performed based on UEMS, 23.6% (13/55) of enrolled patients with motor incomplete SCI showed a ceiling effect for LEMS (LEMS > 36 at the screening). In these patients, potential improvements in lower extremity motor function may be masked, underestimating the effect of NG-101 treatment and therefore challenging the interpretation of a relevant secondary outcome. Using the TMS instead is not more sensitive since it is also affected by ceiling effects, and it only detects a significant effect of treatment on the group predicted to be free of ceiling effects (LEMS ≤ 36 at the screening). By contrast, INCS is not affected by this ceiling phenomenon, offering a more accurate reflection of the change in the neurological function, and may represent a more favorable secondary outcome in clinical trials.
INCS may be less susceptible to ceiling effects for two reasons: (1) INCS is a composite score, so changes in subscores other than the one that reaches a ceiling can still influence the final score and (2) INCS integrates the relative changes in UEMS, LEMS, TPP, and TLT. Regarding this last point, differences in the ISNCSCI subscores are individually relativized to the margin of maximum possible improvement or worsening, depending on whether differences are positive or negative. Thus, when using relative delta scores, a patient’s recovery is not penalized when a subscore reaches its maximum. INCS therefore reflects overall recovery relative to full restoration of sensorimotor function as measured by ISNCSCI (INCS = 1) or the overall worsening relative to the hypothetical loss of all preserved function (INCS = −1) and is, by definition, less susceptible to ceiling effects.
The clinical meaningfulness of therapeutic intervention that boosts neurological recovery depends on whether it translates into functional improvement. The NISCI trial showed that NG-101 in motor incomplete SCI, in addition to significantly increased ΔUEMS, significantly improved the self-care subscores of the SCIM, which evaluates the ability of patients to accomplish feeding, bathing, dressing, and grooming activities.15,16 Our study shows that INCS exhibits stronger associations with SCIM self-care than did the individual ISNCSCI motor and sensory subscores. Improvement in self-care outcomes, which are critical for independence in daily living, requires the integration of motor and sensory changes into coordinated upper limb movements. Therefore, it is not surprising that INCS correlates more strongly with self-care than do individual neurological changes. Subtle changes in sensory function may also contribute to the higher correlation between INCS and an activity requiring hand dexterity.
INCS also showed stronger association with mobility outcomes than did the ΔUEMS. SCIM item 14 evaluates outdoor mobility along 9 potential functional independence grades from wheeling to independent ambulation.15,16 Many of these grades may require some hand function and/or upper extremity strength (like moving independently in a wheelchair or walking with crutches). Therefore, not surprisingly, ΔUEMS significantly correlates with improvements in item 14, while no other single ISNCSCI Δsubscore showed a significant correlation. However, the stronger association of SCIM14 with INCS may reflect two factors: (1) the integration into INCS of subtle changes in other motor and sensory subscores that are not independently associated with changes in item 14, and (2) an underestimation of the true correlation of ΔUEMS with item 14 due to a ceiling effect in ΔUEMS. Supporting the second explanation, UEMS at the final time point correlates more strongly with ΔSCIM item 14 than ΔUEMS does (data not shown, final UEMS-ΔSCIM item 14 rho = 0.66; p < 2.2·10−16).
Noticeably, neither ΔLEMS nor ΔTMS correlates with improvements in item 14, which might indicate that gains in these scores only result in improved mobility when a critical threshold is reached. These findings suggest a nonlinear relationship between changes in ISNCSCI subscores and functional outcomes, highlighting the potential of INCS to better capture these complex recovery dynamics and warranting further investigation.
Our aim was to analyze INCS behavior in a clinical trial where a significant therapeutic effect could be detected to evaluate the feasibility of its implementation in future studies. Since the post hoc analysis of the NISCI trial showed differences between treatment groups only in motor incomplete cervical SCI, our study has been limited to this population of patients. Nevertheless, we also explored INCS behavior in NISCI’s motor complete patients. In agreement with previous post hoc analysis, no therapeutic effect was detected using INCS (Supplementary Fig. S3). However, INCS behaves in this population as in motor incomplete patients: INCS proved to be as sensitive as LEMS (the most sensitive outcome for this cohort; Supplementary Table S4) and correlated more strongly with functional improvement (Supplementary Table S5). In addition, a ceiling effect on UEMS was detected among AIS B patients with baseline UEMS > 28, but INCS proved to be unaffected by this (Supplementary Fig. S4). Generalization of the findings presented here to thoracolumbar injuries remains to be validated retrospectively on trials with a therapeutic effect detected.
Several limitations of this study should be acknowledged. First, the treatment effect analyses are post hoc in nature and focused on a selected cohort with a slight but statistically significant difference in the time at the first day of treatment. Therefore, while the findings on the therapeutic effect are clinically suggestive, they should be interpreted as hypothesis-generating rather than definitive. Second, the study’s generalizability may be influenced by layered selection criteria, including the original URP-based enrichment of the NISCI trial and our subsequent focus on motor incomplete patients with complete datasets. Third, despite NISCI and EMSCI cohorts being balanced on demographical characteristics, slight differences in the examination time points, clinical management strategies, and rehabilitation protocols might affect the use of the EMSCI cohort as historical controls. Finally, the modest statistical power achieved due to the selection of a relatively small sample from the NISCI study and the focus on acute cervical SCI within predominantly European centers may limit the generalizability of these results to more diverse populations.
In conclusion, INCS represents a promising outcome measure for SCI clinical trials. While it is not intended to replace established ISNCSCI subscores, it offers substantial complementary value by reducing ceiling effects and better aligning neurological improvements with functional independence. These features suggest that INCS could serve as an alternative measure to address the limitations of traditional outcome scales in the evaluation of novel therapeutic interventions in SCI.
Transparency, rigor, and reproducibility
The NISCI clinical trial was pre-registered at ClinicalTrials.gov (NCT03935321), and the EMSCI is registered at ClinicalTrials.gov (NCT01571531).
This work represents a retrospective secondary analysis of these previously registered datasets; therefore, the analytic strategy for this secondary analysis was not formally pre-registered.
The original NISCI trial planned a total sample size of 126 participants, powered to detect a between-group difference of 6 points in UEMS at 168 days after baseline, as reported in the primary trial publication. The present study analyzed 55 motor incomplete cervical SCI patients from NISCI and 329 matched patients from EMSCI. Therefore, the present study was not formally powered a priori for treatment effect, as its primary focus was the methodological validation of the INCS. Effect sizes and achieved power for primary and secondary outcomes are reported in the Results.
A flow diagram describing patient screening, inclusion, exclusions, deaths, and losses to follow-up is provided in the primary trial publication. Incomplete treatments and assessments are also reported in the same publication. A flow diagram describing selection of patients for the secondary analysis is shown in Supplementary Figures S2A and 2B.
In the original NISCI trial, participants, investigators, and outcome assessors were blinded to treatment allocation; ISNCSCI and SCIM assessments were performed by certified raters blinded to treatment.
For the present retrospective analysis, data analysts were aware of group allocation. All datasets were labeled using coded identifiers not linked to personal information.
Data for the NISCI clinical trial were acquired between Sept 2019 and Jul 2022 across multiple international sites. Data for the EMSCI trial were acquired since 2004. Neurological and functional assessments were collected using standardized ISNCSCI and SCIM protocols.
Data were analyzed using R statistical software (version 4.4.2) and the packages specified in the Material and Methods section.
All clinical assessment tools and statistical software used are widely available. ISNCSCI and SCIM are established, validated standards in the field of SCI. INCS is an emerging composite outcome, externally validated in this study against EMSCI data.
Linear and nonlinear mixed-effects models were used to account for nonindependence of repeated measures within participants. No imputation or complete-case filtering was applied to missing data for the 55 motor incomplete patients included from the NISCI dataset; analyses were performed using the available observations for each outcome and time point. As indicated in the Material and Methods, the 329 patients selected from the EMSCI dataset constitute a complete case subset, without ISNCSCI missing values. Statistical analyses were performed and discussed by researchers with formal training in biostatistics.
No formal correction for multiple comparisons was applied. Analyses of secondary outcomes were considered exploratory and interpreted in conjunction with effect sizes and confidence intervals.
External validation of INCS loadings was performed using an independent EMSCI cohort.
Deidentified data from NISCI and EMSCI are not publicly available due to consortium and ethical restrictions but may be requested through the corresponding author and the respective data governance bodies.
Analytic code used in this study is publicly available at the Zenodo repository (DOI: 10.5281/zenodo.20325012).
The authors will provide the full content of the article upon request.
Authors’ Contributions
Conceptualization and study design: A.A.-M., C.J., and A.C. Investigation: N.W., R.A., D.M., L.G., I.L., O.M., Klaus R., F.R., B.Z., M.H.-G., Y.B.K., J.B.-P., Kerstin R., M.A., A.B., J.K., M.S., P.F., M.E.S., and A.C. Data analysis: A.A.-M. and M.B. Critical revision and discussion of data analysis: A.A.-M., C.J., P.S.S., M.B., and J.L.K.K., and A.C. Drafting of the article: A.A.M. and A.C. Critical revision of the article for important intellectual content: C.J., D.G.-O., N.W., L.G., J.L.K.K., R.R., P.S.S., M.S., and PF. Interpretation of data and critical revision: All authors. All authors reviewed and approved the final article and agree to be accountable for all aspects of the work.
Ethical Considerations
This study is a retrospective secondary analysis of data obtained from the NISCI (ClinicalTrials.gov NCT03935321) clinical trial and the EMSCI (ClinicalTrials.gov NCT01571531). Both original studies were conducted in accordance with the Declaration of Helsinki and were approved by the appropriate local Ethics Committees and Institutional Review Boards at each participating center. The NISCI trial was approved by the Ethics Committees listed in the primary trial publication. The EMSCI study protocol was approved by the Ethics Committees of all participating institutions.
The present secondary analysis used fully deidentified data and did not require additional ethical approval.
Consent to Participate
Written informed consent to participate was obtained from all participants in both the NISCI and EMSCI studies prior to enrollment, in accordance with local regulatory requirements.
No additional consent was required for the present secondary analysis of deidentified data.
Consent for Publication
Not applicable. The article does not contain any individual-level identifiable data, images, or videos.
Data Availability
Deidentified data from NISCI and EMSCI are not publicly available due to consortium and ethical restrictions but may be requested through the corresponding author and the respective data governance bodies.
Supplemental Material
sj-tiff-1-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-tiff-1-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Supplemental Material
sj-tiff-2-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-tiff-2-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Supplemental Material
sj-tiff-3-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-tiff-3-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Supplemental Material
sj-tiff-4-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-tiff-4-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Supplemental Material
sj-docx-5-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-docx-5-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Supplemental Material
sj-docx-6-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-docx-6-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Supplemental Material
sj-docx-7-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-docx-7-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Supplemental Material
sj-docx-8-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-docx-8-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Supplemental Material
sj-docx-9-nrt-10.1177_08977151261467219 — Supplemental material for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials
Supplemental material, sj-docx-9-nrt-10.1177_08977151261467219 for The Integrated Neurological Change Score Is a Sensitive Neurological Composite Measure to Evaluate Cervical Spinal Cord Injury Trials by Angel Arevalo-Martin, Catherine Jutzeler, Daniel Garcia-Ovejero, Marc Bolliger, Norbert Weidner, Rainer Abel, Doris Maier, Lukas Grassner, John L.K. Kramer, Iris Leister, Orpheus Mach, Klaus Röhl, Frank Röhrich, Björn Zörner, Margret Hund-Georgiadis, Yorck B. Kalke, Jesús Benito-Penalva, Kerstin Rehahn, Mirko Aach, Andreas Badke, Jiri Kriz, Rüdiger Rupp, Paulina S. Scheuren, Martin Schubert, Patrick Freund, Martin E. Schwab, and Armin Curt
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
A.A.-M. and D.G.-O. are supported by grant
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.