
Abstract
Background
The daily life of the working nurse has been shown to be a stressful one (van Wyk & Pillay-Van Wyk, 2010), and the stressors that nurses feel can affect patient care (Laschinger & Leiter, 2006; van Wyk & Pillay-Van Wyk, 2010). The link between nursing burnout and lack of self-care has been recognized (McElligott, 2013). In her text on Caring Science, Jean Watson (2008) emphasizes the importance of self-care for nurses:
Nurses often become pained and worn down by trying to always care, give, and be there for others without attending to the loving care needed for self. This model invites, if not requires, nurses to attend to self-caring practices that assist in their own evolution of consciousness for more fulfillment in their life and work. (p. 47)
Self-care is a core value of the American Holistic Nurses Association (AHNA), which describes how nurses can care for themselves: “The nurse has a responsibility to model health care behaviors. . . . Holistic nurses strive to achieve harmony in their own lives and assist others striving to do the same” (AHNA, 2012, p. 21). The American Nurses Association’s (2013) Scope and Standards of Practice also states that the registered nurse “demonstrates a commitment to practicing self-care, managing stress, and connecting with others” (p. 137).
This study reports on the method employed by a community hospital to offer a self-care management tool to its nurses. Nursing officers in a Northern California hospital desired to support nurses in stress reduction. A small pilot study extended Jin Shin Jyutsu® (JSJ) self-care training to 20 nurses as a model to potentially reduce their stressors. The purpose of this research was to conduct a pilot study to assess whether we could identify a relationship between training in a self-care practice and self-reported stress measures in a group of nurses. Additionally, we wanted to measure the relationship, if any, between self-care and the nurses’ perceived caring efficacy. There is a paucity of research on this topic.
In this study we chose the intervention of JSJ© self-care training. JSJ is a time-honored, comprehensive healing art similar to acupressure, which uses hand contact at specific locations to harmonize the flow of vital energy circulating through the body in organized pathways. All traditional healing systems are founded “on the principle that in order to heal the body, the person must strengthen and harmonize the flow of vital energy within” (A. Burmeister, 1997, p. 13). JSJ self-care is a readily learned and easily applied energy-balancing method.
Literature Review
The literature relevant to this study includes the topics of work-related stress in nurses, self-care in nurses, and JSJ. Several large reviews of the literature have been undertaken on nurses and work-related stress (Applebaum, Fowler, Fiedler, Osinubi, & Robson, 2010; Jennings, 2008; Laschinger & Leiter, 2006; Ruotsalainen, Serra, Marine, & Verbeek, 2008). Nursing stress has been measured and sources of stress identified. How to minimize and moderate these stressors was less clear (Edwards & Burnard, 2003, van Wyk & Pillay-Van Wyk, 2010). An integrative review of the quality of work life for nurses (Vegharseyyedin, Vanaki, & Mohammadi, 2011) advised nurse managers to work at removing mental stress from the workplace. In a Cochrane-sponsored systematic review of interventions for reducing health care workers’ occupational stress (Marine, Ruotsalainen, Serra, & Verbeek, 2009), interventions such as training programs on communication and stress (Delvaux et al., 2004) provided by the organization were successful in reducing stress symptoms. Wanjiku (2011) also found in a systematic review of methods to reduce stress for nurses that interventions offered by the organization were key determinants for change. Tourangeau, Cummings, Cranley, Ferron, and Harvey (2010) found organizational support also to be essential.
A lack of self-care by nurses has been documented in the literature (McElligott, Siemers, Thomas, & Kohn, 2009). Lawrence and Kear (2012) studied caring in an interventional cardiac unit nursing staff and found that nurses in this unit “may not be tending to self-caring and mind-body-spirit renewal practices” (p. 39). Training was revised for new nurses to emphasize modeling self-care and caring for others. The authors conclude that for an organization to embody Watson’s Caring Science, “there must be a culture in which the practice of loving kindness to self and co-workers is not merely a theory [italics added] but the normative behavior of all nurses who practice within the organization” (p. 39).
Nelson et al. (2012) studied 636 nurses in four countries and found that the lowest scores on a Caring Factor Survey were in “treating self with loving kindness.” Johnson (2012) found a statistically significant inverse relationship between self-care and compassion fatigue and self-care and burnout risk. She concluded,
The call to the leaders of today and tomorrow is to take care of the people who take care of people—to serve the servers—and to help the growth of their capacity to work compassionately and resiliently from their hearts. (p. 419)
Several self-care modalities and approaches have shown success in helping nurses cope with work-related stress. Brooks, Bradt, Eyre, Hunt, and Dileo (2010) used music imagery. Kravits, McAllister-Black, Grant, and Kirk (2010) used guided imagery, relaxation training, art exploration of coping strategies, and a personal wellness plan. Repar and Patton (2007) used massage, language, and visual art. Several studies have shown mindfulness-based stress reduction to be helpful (Bazarko, Cate, Azocar, & Kreitzer, 2013; Cohen-Katz et al., 2005; Mackenzie, Poulin, & Seidman-Carlson, 2006; Pipe & Bortz, 2009; Zeller & Levin, 2013). A study by McElligott, Capitulo, Morris, and Click (2010) found that an 8-hour holistic program (the collaborative care model), combined with development of a self-care plan, was associated with an increase in nurses’ self-care health promoting behaviors. A pilot study by Cuneo et al. (2011) found that a self–Reiki training intervention helped decrease perceived stress in nurses who practiced it regularly.
There is a growing body of literature regarding the uses of JSJ in health care. JSJ intervention in direct patient care has been shown to be beneficial in patients with a wide variety of conditions, including heart transplants (Sempell, 2000), breast cancer (Searls & Fawcett, 2011), and multiple myeloma (Shannon, 2002). The Markey Cancer Center at the University of Kentucky is using JSJ to assist patients in coping with pain, stress, and nausea. In a study of 111 patients, 51% had decreases in pain, 62% reported decreased stress, and 67% reported decreased nausea after their JSJ sessions (Markey, 2012). The Integrative Medicine Department at Morristown Medical Center, a large Magnet-designated facility, offers multiple complementary therapies, including JSJ. Analysis of 1,667 treatment interventions to 1,219 patients showed consistent reduction in patient’s reports of pain, stress, and nausea after sessions (Atlantic-Department of Integrative Medicine, 2010).
Dr. Kristina McFadden and colleagues at the University of Colorado at Boulder have conducted several studies using JSJ to reduce physiological and emotional stress. McFadden and Hernandez (2010) used a randomized, placebo-controlled single-blind design to evaluate the effects of a series of eight JSJ acupressure treatments on heart rate and blood pressure in stroke patients (n = 16). The authors found significantly greater and faster heart rate reduction in the active treatment compared to the placebo group. Because decreased heart rate is an indicator of autonomic nervous system modulation and can be an indicator of the relaxation response, the authors propose that this modality could help reduce risk of further cardiovascular disease in this population. McFadden et al. (2011) conducted a randomized, placebo-controlled, single-blind study to assess the effects of a series of acupressure (JSJ) treatments on cognitive function following traumatic brain injury (n = 42). The authors found that the treatment group showed improvements, suggesting “an enhancement in working memory function.” McFadden, Healy, Hoversten, Ito, and Hernandez (2012) found significant reduction in college student stress using JSJ acupressure, but not more reduction than with the use of a matched relaxation compact disc.
The use of JSJ with nurses has been less studied, Updike, Cleaveland, and Nyberg (2000) incorporated JSJ training as one of several complementary modalities in a caring-healing curriculum for 25 nurses on a pediatric hematology/oncology unit. At the end of a 6-month period, the nurses reported becoming more intentionally present with patients and their families. A master’s thesis by Lamke (1993) explored the effects of a series of JSJ treatments on stress symptoms in 34 nurses. The treatments included self-help instruction in the use of four exercises for general harmonizing. After a series of six treatments, the nurses had decreases in perceived stress and somatic symptoms (p < .05). The nurses who practiced self-help were more likely to have persisting positive changes 6 to 8 weeks after the treatments. Subjective responses included feeling relaxed (62%), improved coping/decreased stress (44%), and feeling calm, at peace, and integrated (38%).
Theoretical Framework
The nursing model followed by Kaiser Permanente is based on Jean Watson’s theory of human caring. Caring Science is based on 10 caritas processes that provide a unifying framework for nursing based on human caring, compassion, and authentic interrelationships. This model posits that caring for self is a prerequisite for authentic caring for others. By offering a self-care healing modality to nurses in an acute care hospital, the nurses’ abilities to care for themselves and others may be affected.
Research Design
A quasi-experimental, pre-, post-, and 30-day posttest design was used. This was a pilot test of a single group of 20 nurses who were trained over a month’s time how to use JSJ self-care. The Personal and Organizational Quality Assessment–Revised (POQA-R) instrument and the Coates Caring Efficacy Scale (CES) were used to measure stressors and caring efficacy prior to, after, and 1 month after the intervention.
Research Questions
Definition of Terms
Sample
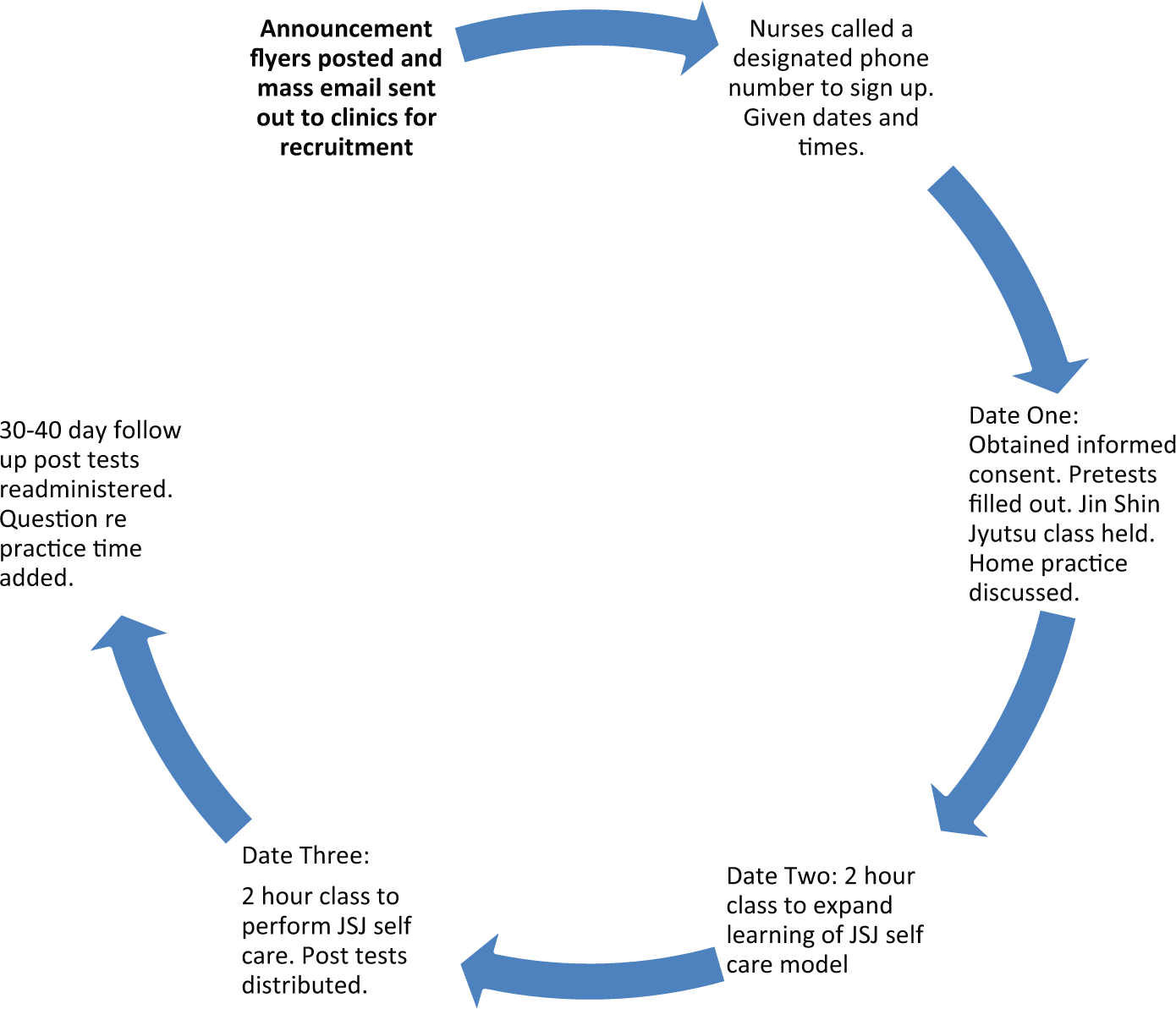
We used a sample of convenience of nurses employed at the health care clinics and hospital in a small Northern California community. The recruited sample was smaller than anticipated due to labor union requirements that all nurses in work-related activities be paid in full for their time. These nurses worked in both the outpatient clinics and the hospital and included both registered nurses and licensed vocational nurses. Recruitment was through general e-mail blasts throughout the clinics and posters hung within the outpatient facility (Figure 1). Interested parties were asked to call a confidential designated phone line to express interest. After a 1-month period, remaining spaces were opened within the hospital. The first 25 persons calling were accepted into the study and told where and when the trainings would take place. A total of 20 nurses came to the first session, consented to the study, and attended the three sessions. The 20 nurses completed the study.
Design Pictorial
Human Subjects Review
The Northern California Institutional Review Board (IRB) approved the study. Nurses recruited understood that participation or nonparticipation had no effect on their employment at the organization and that they could withdraw from the study at any time. Each participant was assigned a code number known only to the primary investigator. The surveys had no names on them, and the consent forms were collected and stored separately from the data collection sheets. All materials were stored in a locked cabinet. No interfacility e-mail was used. The nurses’ supervisors were kept blind as to who participated in the study. Because nurses were considered vulnerable populations, the IRB asked that complete confidentiality be maintained. After the initial consent signing, managed by the third researcher, the primary investigator and the JSJ trainer remained blinded to the identity of the participants throughout the study and no names were exchanged during the classes. Employee Health Services were made available to any participant in need of mental or physical attention as a result of the study but none was needed.
Instruments
The POQA-R is a self-report inventory created by the Institute of HeartMath in 1999 and revised in 2009 to reflect key psychological and workplace elements that contribute to the overall quality of an organization. There are 85 individual questions, which are categorized into two primary scales: Personal Quality and Organizational Quality. The primary scales are further categorized into 24 subscales generally made up of 2 to 4 questions each. The subscales of the Personal Quality Scale are Positive Outlook, Gratitude, Motivation, Calmness, Fatigue, Anxiety, Depression, Anger Management, Resentfulness, and Stress Symptoms (six specific symptoms are rated). The subscales of the Organizational Quality Scale are Strategic Understanding, Value of Contribution, Manager Support, Goal Clarity, Job Challenge, Work Intensity, Time Pressure, Freedom of Expression, Communication Effectiveness, Confidence in the Organization, Work Attitude, Morale Issues, Productivity, and Intention to Quit. Additionally, there are 2 separate questions rating general health and general stress in the past month. Each item consists of a 7-point scale ranging from 1 (not at all or strongly disagree) to 7 (always or strongly agree). Validity was established based on theories of organizational climate that affect job performance. The instrument underwent reliability verification with 2,540 respondents. Cronbach’s alphas established were .76 for Organizational Stress, .92 for Emotional Vitality, .92 for Emotional Stress, and .76 for Physical Stress.
The CES was developed by Dr. Carolie Coates in 1995 (Coates, 1997). The tool was established in order to relate nurses’ understanding of their own caring behaviors to the Jean Watson caring theory. Validity was established based on caring concepts from Watson and other nurse theorists and on concepts of self-efficacy from the social learning theory of Bandura (1997). The initial reliability was established on 47 novice nurses and further supported by additional applications of the instrument with populations including graduating nurses, alumni, and clinical preceptors. Cronbach’s alpha was between .84 and .88 on the various formats of the questions (Coates, 2009, pp. 163-166). The Coates instrument was recommended as a caring measurement tool that offers content validity with references to the carative factors in Watson’s theory (Coates, 2009, p. 165).
Permission was obtained to use both instruments through correspondence with the authors. Both instruments required a small charge for purchase and the POQA-R required an analysis fee.
Intervention
A researcher not involved in the training obtained informed consent and then administered the POQA-R and CES instruments. The 20 nurses were then introduced to the certified JSJ trainer, who was also a registered nurse. Because the IRB asked for anonymity, the participants were not introduced and each was given a code number to use for their pre- and posttesting. JSJ self-help Books 1 and 2 (M. Burmeister, 1981, 1985) and handouts were distributed to each participant. The trainer instructed nurses in JSJ methods. Participants practiced locating specific body points on themselves and on each other. The trainer observed each person as she practiced a return demonstration. The participants were asked to practice any of the class exercises at home for 20 minutes daily between classes. The classes met three times over a 1-month period. After the third class, the two instruments were given again by the nonteaching researcher. The two instruments and a third question about time spent practicing were given again after 30 to 40 days.
Data Analysis
The HeartMath Institute scored the POQA-R in individual and group responses for the three time periods. Individual groups of answers are grouped by the Heartmath Institute and reported in subscales. The subscale means were compared between the pretest and posttest, and the pretest and 30- to 40-day follow-up using paired t tests.
Responses on the Coates CES were recorded by the nonteaching researchers. All scores were checked twice for reliability by the two nonteaching researchers. The comparison means were assessed between the pretest and posttest, and the pretest and 30- to 40-day follow-up with paired t tests. This analysis was done by biostatisticians provided by the health care system.
Additionally, the amount of time the individual nurse was practicing the self-care model at home was assessed at the 30- to 40-day follow-up. Participants were asked, in a question added by the researchers, whether they were practicing JSJ at home daily, occasionally, rarely, or not at all. Participants were not asked to record their home practice sessions.
The biostatistician ran t tests, Spearman correlation coefficients, and Pearson correlation coefficients on these three pilot data sets to answer three questions: (a) Did the pre- and posttests of the POQA-R and CES reflect any significant changes after the intervention, and if so, in what areas? (b) If there were significant changes in the pre- and posttests on either of the measures, was there any relationship between the significant changes of the POQA-R with the significant changes of the CES? (c) Did the individual amount practiced at home influence the individual Caring Efficacy results?
Results
Personal and Organizational Quality Assessment–Revised
Demographics
Limited demographic data were collected as part of the POQA-R. The 20 nurses were all female and 80% worked over 36 hours per week. The respondents (80%) had worked within the health care system for over 20 years and many (60%) had worked in their same jobs for over 10 years. The nurses came from clinics throughout the county and had varied levels of nursing education (licensed vocational nurses through master’s).
Personal Quality Scales
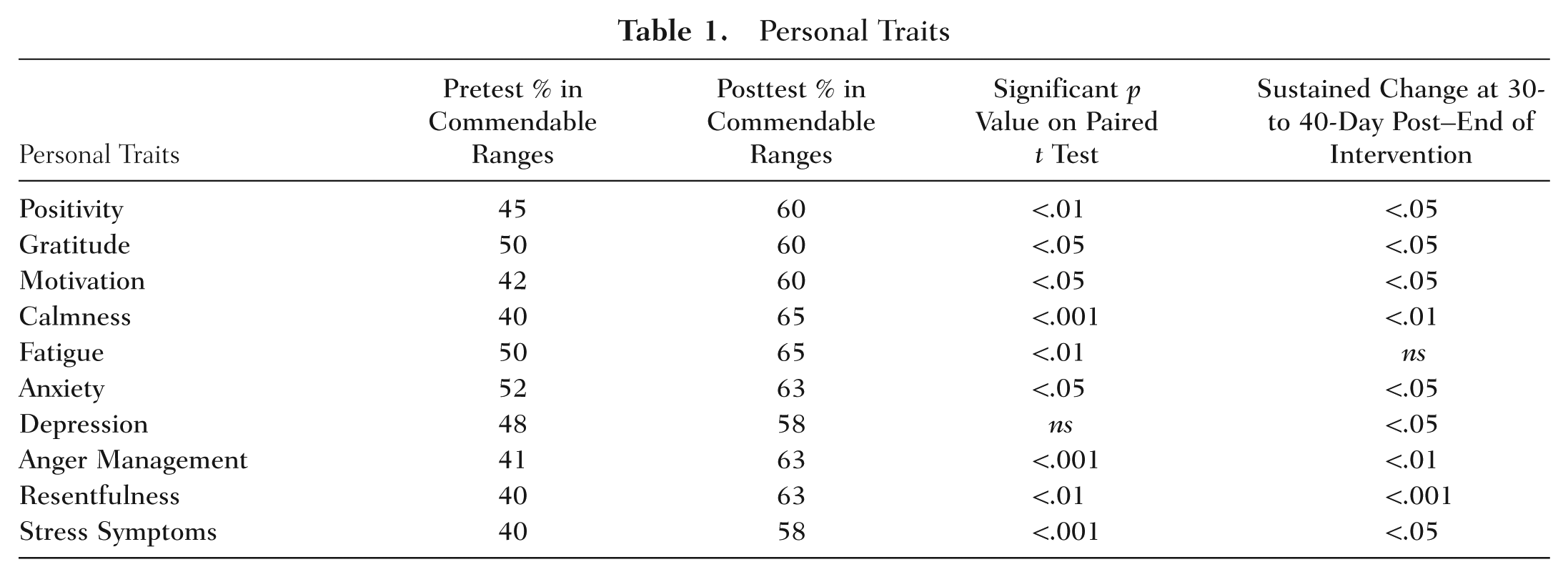
The POQA-R Personal Quality subscales examine personal traits, moods, and attitudes of the participants. In analysis of the study data, individual and group scores are compared to nationally established averages of similar populations, in this case 5,900 other health care workers (Institute of HeartMath, 2011). The POQA-R then assessed whether our 20 nurses scored higher or lower than nationally established averages. In pretest measures, the 20 nurses scored below national norms in positive outlook, motivation, and calmness and above the national norms in feelings of depression, anger, resentfulness and stress. They were at the average for gratitude, fatigue, and anxiety. After the 6 hours of JSJ training, on post test, all subscale measures improved. This improvement sustained in the 30-day follow-up in all areas except fatigue. Table 1 shows the statistical values.
Personal Traits
Organizational Quality Measures
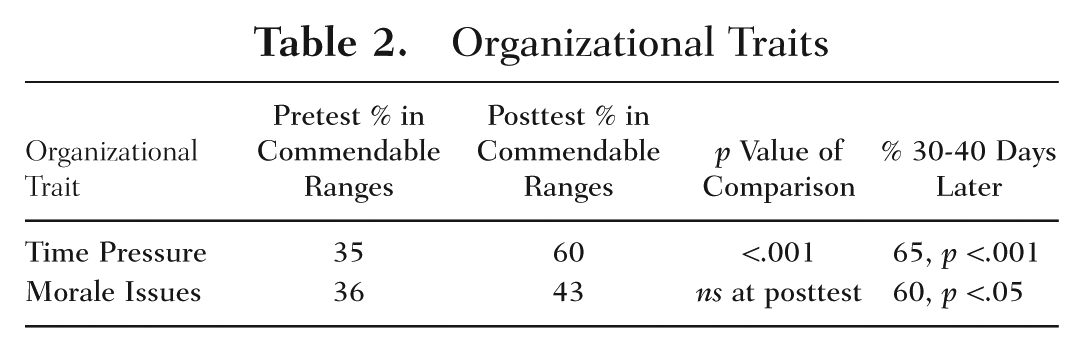
How the nurses felt about their organization was measured. In general, nurses felt good about the organization (higher than the average national score) in 9 of the 11 measurement areas and these positive feelings sustained to the 30- to 40-day postintervention. On the pretest, only two subscales, time pressure and morale issues, found participants reporting lower than average scores. On posttest these scores improved and were higher at Time 3 measurement 30 days later (see Table 2).
Organizational Traits
Physical Stress
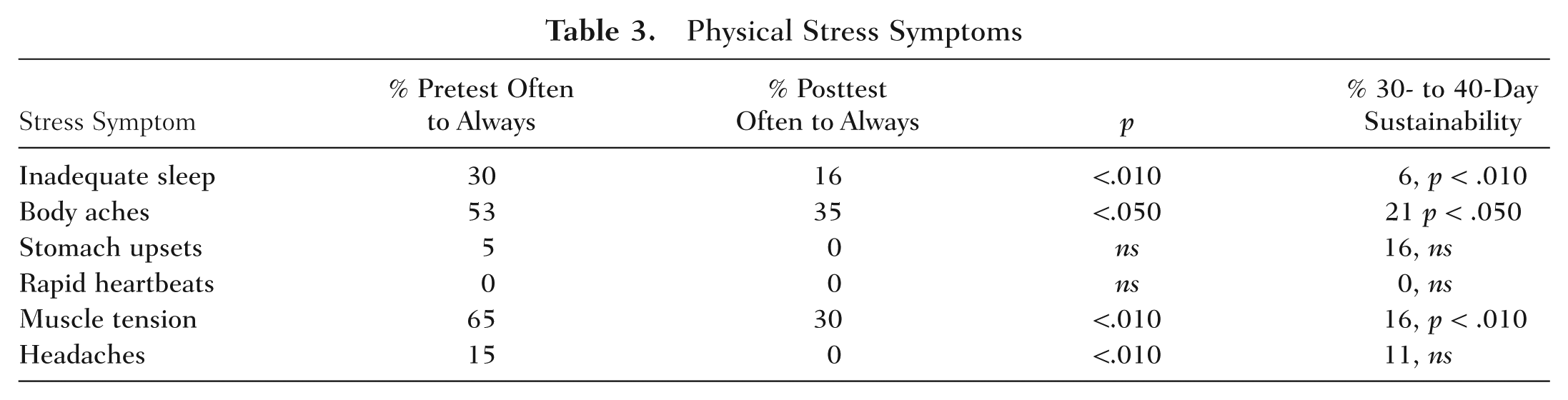
Physical stress symptoms were also measured by the POQA-R. Respondents were asked about their sleep, body aches, stomach upsets, rapid heartbeats, muscle tension, and headaches. All negative symptoms decreased at the posttest measurement. Sleep problems, body aches, and muscle tension stayed decreased after 30 to 40 days (see Table 3).
Physical Stress Symptoms
Coates Caring Efficacy Scale
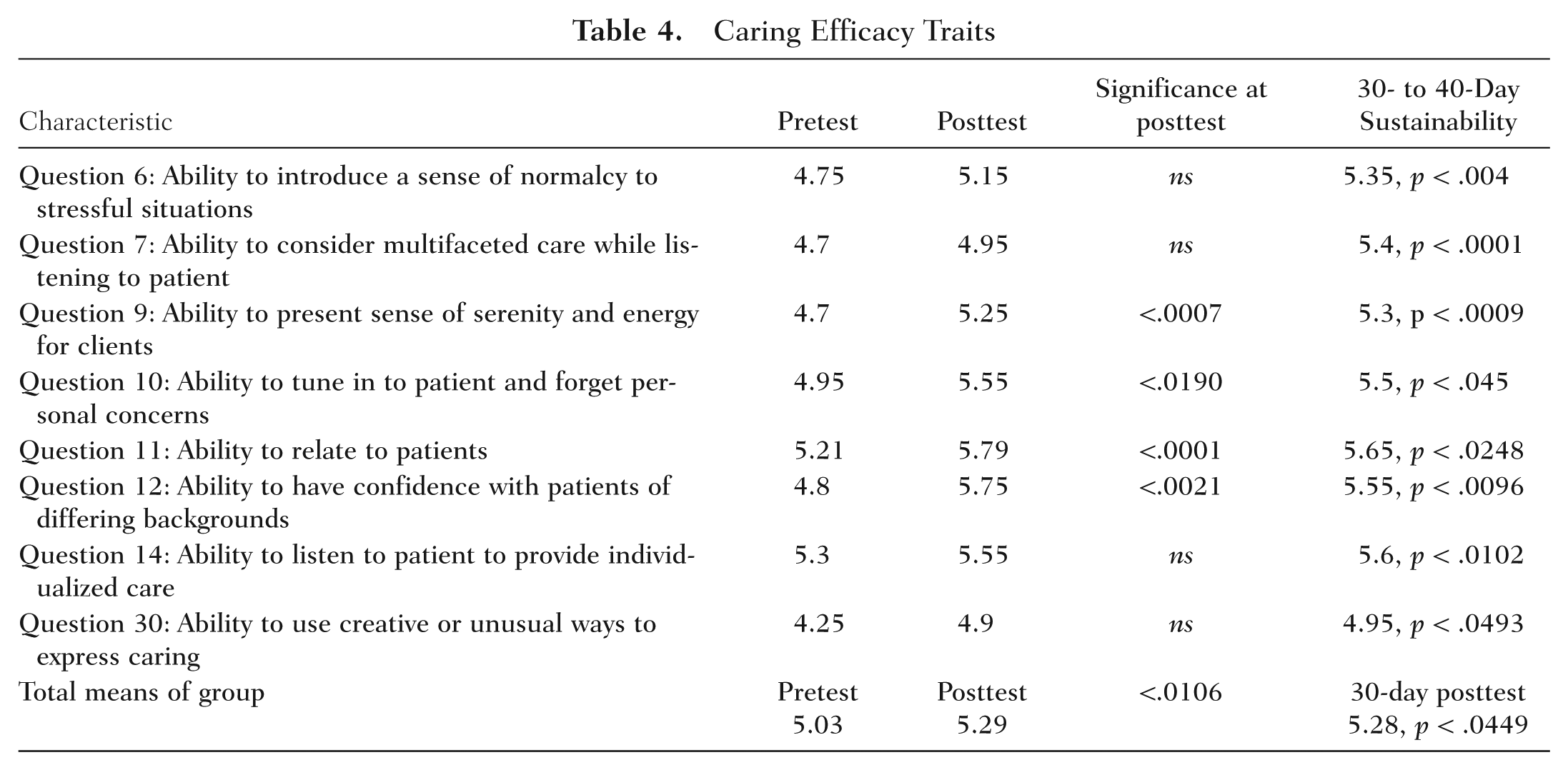
The CES measured participants’ confidence in their ability to show caring for their patients by self-report. Thirty items that measured caring attitudes, skills, and behaviors were assessed. The scale ranged from 0 to 6 with a score of 6 exhibiting the highest level of caring efficacy. Negative characteristics were reversed for analysis. The mean preintervention scores on all items ranged from 4.25 to 5.65, showing a high level of caring efficacy to start. At the end of the intervention, mean scores increased significantly (p = .01), and remained increased 30 days postintervention (p = .045). Specific questions showed statistically significant changes at posttest and/or 30-day posttest (see Table 4; note: questions not showing significant changes are not shown in Table 4).
Caring Efficacy Traits
Relationship Between POQA-R Stress Factors and Coates CES Paired t Tests
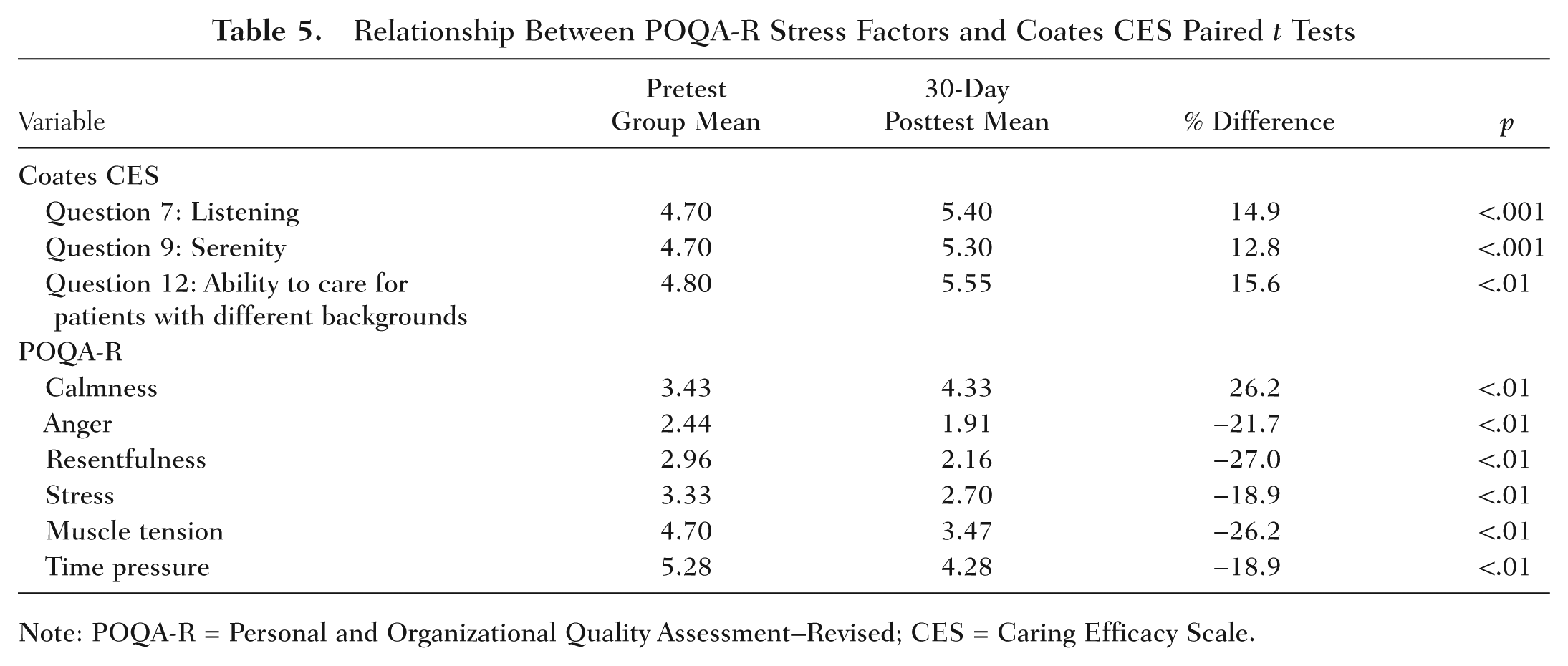
Note: POQA-R = Personal and Organizational Quality Assessment–Revised; CES = Caring Efficacy Scale.
Practice At Home
Participants were asked to practice the JSJ self-care at home for 20 minutes daily. At 30- to 40-day follow up, participants were asked how often they were practicing the measures. The language was converted to numerical form: “Using Daily” or “Using Often” was given 4 points, “Occasionally Using” was given 3 points, “Rarely Using” was given 2 points, and “Not Using” was given 0 points. About half of the nurses were still practicing the self-care daily or often. Results were as follows: using daily or often = 45%, using occasionally = 25%, using rarely = 25%, and not using = 5%. This score was then correlated with the participants’ individual scores showing statistically significant changes on the CES. The relationship between amount practiced and normalcy (Question 6), listening (Question 7), serenity (Question 9), forgetting personal concerns (Question 10), ability to relate (Question 11), ease with cultures (Question 12), individualized care (Question 14), and creativity (Question 30) were analyzed. We were unable to find any relationship between amount practiced and caring variables and had no statistically significant findings.
Relationship Between POQA-R and CES
Variables with the highest amount of statistical in the pre- and posttest means on the POQA-R and CES were compared to evaluate the relationship between stress levels and caring efficacy levels. Paired t tests were run on the group means in pre- and 30-day post POQA-R for the subscales of Calmness (increases in) and Anger, Resentfulness, Stress, Muscle Tension, and Time Pressure (decreases in). These results were then correlated with the mean increases in caring efficacy on the Coates Scale in Listening (Question 7), Serenity (Question 9), and Backgrounds (Question 12). We were able to see some relationship between the results on the two instruments. Increases in group means in calmness and decreases in group means of negative characteristics were associated with increases in variables in caring efficacy. Although the group means were statistically related at the .001 to .01 levels, on scatter plots for individual scores we were unable to establish correlations. This was possibly due to the small number of subjects and insufficient power.
Limitations
This pilot study was small, and we were unable to do the planned control group due to budgetary reasons. The study sample was very homogeneous in that all were female, most were longtime employees, and all worked at the same health care facility. The participants self-selected, and their reasons for participation are unknown. It is uncertain whether payment for time in the classes influenced the findings. The generalizability of the findings of the study are limited by these factors.
Discussion
The response to JSJ self-care training was positive. JSJ appears to have been helpful to the participants. Each instrument is discussed below.
POQA-R
According to Maslach and Leiter (1997), symptoms of stress and burnout include physical problems such as headache, gastrointestinal symptoms, elevated blood pressure, muscle tension, and fatigue and symptoms of mental distress including anxiety, depression, sleep disturbances, frustration, and anger. Statistically significant decreases on the POQA-R tool in several of these symptoms were reported by the study group, suggesting that the JSJ self-care may have helped reduce physical stress. Additionally, the increases in positivity, gratitude, motivation, and calmness are indicative of a less stressed state, suggesting that JSJ self-care may have helped with improving the respondents’ emotional state.
CES
The degree of positive changes on the CES scale measures seemed important. In Updike et al.’s (2000) study, nurses verbally reported being more intentionally present after being trained in several complementary modalities, which included some self-care tools such as relaxation and mindfulness. Our small pilot study shows a statistically significant relationship between a holistic self-care practice and increased caring efficacy in nurses. Several of the items as measured by the CES (see Table 3) indicate an improved sense of being authentically present with the patient. Being authentically present is a prerequisite to establishing a caring relationship in the context of Watson’s Caring Science. The authors are aware of only one other study that showed a positive correlation between self-care and caring efficacy: a pilot study (n = 10) by Brathovde (2006). Brathovde also showed significant (p = .028) increases in the CES scores after a training of nursing in Reiki self-care and felt, too, that increased authentic presence could increase the caring relationship.
Pipe, Bortz, Dueck, Pendergast, and Buchda (2009) and Turkel and Ray (2004) also discuss the importance of the nursing leader’s involvement with self-care. They advise leaders to practice self-care measures and to facilitate self-care, renewal, and healing in the organizational culture. Our small study had the support of nursing leaders and may have the potential to improve the caring environment. An example of the improved environment came to us in an anecdotal comment from one of the participants after the study. She stated,
Two of us who had done the training were at a meeting where tensions were running very high. Our manager was escalating in stress. I looked at my colleague. We both went into a Jin Shin Jyutsu measure and calmed ourselves. We smiled. We knew. Afterwards, my manager came up to me. “I saw you doing that Jin Shin stuff. You better teach me how.”
Recommendations
Conclusion
Given that the CES measures attitudes, skills, and behaviors that reflect nursing in the framework of Caring Science, JSJ self-care training appears to be useful to nurses or organizations working to incorporate Watson’s caring theory into practice. For the researchers, the results of this pilot study indicated that the relationship between self-care, decreased stress, and greater caring efficacy is “not just a theory” but rather a reality worth further investigation for the potential benefit of nurses, patients, and organizations.
Footnotes
Acknowledgements
The authors thank Dr. Gretchen Summers for funding statistical analysis from the Northern California Kaiser Nursing Research Fund and Jeanne Darbinian, MPH, analyst with the Biostatistical Consulting Unit of the Kaiser Permanente Division of Research, for her concentrated efforts on our behalf. The authors thank the anonymous reviewers for their excellent suggestions.
The authors express appreciation to the Nursing Leadership of the Kaiser Santa Rosa Organization for funding of this study and to the Nursing Research Council for their support.