
Abstract
Obesity is considered a complex chronic disease with multiple causative factors, including social, economic, genetic, behavioral, physiologic, psychological, and metabolic components (Apovian, 2010). Obesity and overweight conditions have reached epidemic levels in America with more than 60% of adults meeting the criteria for being overweight or obese (Flegal, Carroll, Ogden, & Curtin, 2010). Nearly 80% of obese persons have diabetes, coronary artery disease, hypercholesterolemia, hypertension, gallbladder disease, or osteoarthritis, and 40% of these obese adults have two or more of these conditions (Gabel et al., 2009).
During menopause, women have an increased risk of weight gain (Keller et al., 2010; Simkin-Silverman, Wing, Boraz, & Kuller, 2003). Because of decreasing estrogen levels and other hormonal changes, additional weight gained during menopause is more likely to be stored centrally, increasing the amount of abdominal fat, which is associated with an increased risk of diabetes and cardiovascular disease (Crawford, Casey, Avis, & McKinlay, 2000; Keller et al., 2010; Lovejoy, 1998, Sternfeld et al., 2004). Weight gain, even in normal weight women, increases the risk of cardiovascular disease 3.1% with every kilogram of weight gained in adulthood (Colditz, Willett, Rotnitzky, & Manson, 1995; Crawford et al., 2000; Willett et al., 1995). Despite these risks, Deeks, Zoungas, and Teede (2008) found that only 11% of perimenopausal women in their study perceived heart disease to be a risk associated with menopause, when the actual mortality figure for this population is 41%. Preventing weight gain in perimenopausal women is of primary importance in preventing chronic health conditions and requires a holistic approach.
Possible factors that may contribute to weight gain in perimenopausal women are nonpurge binge eating, emotional eating, and low diet-related self-efficacy. Nonpurge binge eating is the uncontrolled consumption of a large amount of food in a specific period of time without subsequent purging (e.g., vomiting, laxatives, diuretics, excessive exercising, or fasting; American Psychiatric Association, 2013; Timmerman, 1998). The binge eater’s perception of being out of control while eating is what distinguishes nonpurge binge eating from overeating (Fairburn & Wilson, 1993).
Emotional eating can be defined as eating in response to a variety of negative emotional states (e.g., anger, anxiety, depression, and loneliness) in an attempt to cope with negative feelings (Ricca et al., 2009). Emotional eating and binge eating often occur simultaneously with negative emotional events or stressors often preceding binge episodes (Masheb & Grilo, 2006). Heatherton and Baumeister (1991) theorized that binge eating is motivated by a desire to escape from oneself or from self-awareness; by focusing attention on the immediate environment (food), one can escape emotional distress and temporarily avoid negative feelings. Eating behaviors that occur independent of hunger, like binge eating and emotional eating, can contribute to the consumption of excess calories, which will eventually result in weight gain.
Self-efficacy is an individual’s belief in one’s ability to perform a behavior in a specific situation (Bandura, 1977). Since the performance of many behaviors is, in part, determined by self-efficacy (McAlister, Perry, & Parcel, 2008), it is reasonable to assume that the degree of one’s diet-related self-efficacy may also be linked to other eating behaviors such as binge eating and emotional eating.
Preventing weight gain and the subsequent increase in abdominal fat in perimenopausal women need to be addressed from a holistic perspective in order to reduce the risk of heart disease, diabetes, and other health problems. Little research has been conducted to determine to how emotional eating, nonpurge binge eating and diet-related self-efficacy are related in healthy women without diagnosed eating disorders, such as Binge Eating Disorder (BED).
The purpose of this study is to examine the potential relationships among emotional eating, nonpurge binge eating behavior, and diet-related self-efficacy. These factors represent a facet of individuals’ emotional response (emotional eating) and mental experience (perceived diet-related self-efficacy), which may affect behavior (binge eating) and subsequently the body (weight gain). Thus, the study addresses the problem from a perspective consistent with holistic nursing practice that recognizes the interconnectedness of the mind, body, emotions, and spirit within the context of one’s environment and how this interconnectedness affects the individual’s well-being (Thornton, 2014). Understanding these relationships may better inform the development of holistic interventions to help perimenopausal women with weight management and promoting wellness.
Research Questions
The research questions for this secondary data analysis are the following:
Literature Review
Research on emotional eating and binge eating has primarily focused on individuals diagnosed with BED. BED involves persistent and recurrent binge eating episodes accompanied by marked distress without subsequent purging (American Psychiatric Association, 2013). BED has been identified as a significant risk factor for future weight gain (Yanovski, 2003). The relationship between the presence of binge episodes, binge eating severity, and negative emotions in persons with BED has supported by numerous studies (Brown, Smith, & Craighead, 2010; Eldredge & Agras, 1996; Goodrick et al., 1999; Kenardy, Arnow, & Agras, 1996; Masheb & Grilo, 2006; Noli et al., 2010; Pinaquy, Chabrol, Simon, Louvet, & Barbe, 2003; Ricca et al., 2009; Zeeck, Stelzer, Linster, Joos, & Hartmann, 2011). Fewer studies have investigated binge eating in individuals who engage in nonpurge binge eating but do not meet the criteria for BED.
Restaurants have been identified as a high-risk environment for those who engage in nonpurge binge eating, with about 50% of randomly selected binge episodes occurring in restaurant settings (Allison & Timmerman, 2007). In a study examining restaurant eating in nonpurge binge eating women, the frequency of binge episodes had significant, positive correlations with frequency of eating out (r = .27; p < .05; Timmerman, 2006). The number of binges that occurred at restaurants was significantly correlated with daily calorie (r = .41; p < .01) and fat (r = .29; p < .05) intake. These findings indicate that women who binged more frequently also ate out more often and had difficulty with controlling their calorie intake, which supports the decision in the present study to look at binge eating in a sample of women who ate out frequently.
Self-efficacy is an important predictor of behavior; if a person believes he or she can successfully perform a behavior, then that individual is more likely to do so. Researchers have found relationships among binge eating behavior, emotional eating, and low levels of eating self-efficacy (Annesi, 2011; Brown et al., 2010; Cargill, Clark, Pera, Niaura, & Abrams, 1999; Clark, Forsyth, Lloyd-Richardson, & King, 2000; Linde et al., 2004; Miller, Watkins, Sargent, & Rickert, 1999; Presnell, Pells, Stout, & Musante, 2008). Treatment interventions aimed at decreasing binge eating behavior (Wolff & Clark, 2001) or increasing weight loss self-efficacy have shown favorable results, but essentially no long-term follow-up has been conducted to determine whether the behavior change was maintained (Dennis et al., 2001; Linde, Rothman, Baldwin, & Jeffery, 2006; Presnell et al., 2008; Warziski, Sereika, Styn, Music, & Burke, 2008). While these studies support the interconnectedness of emotional eating, binge eating, and self-efficacy, few studies have investigated these factors in healthy, perimenopausal women without BED; a gap in the literature addressed by this study.
Method
This study is a secondary analysis of the Mindful Restaurant Eating intervention, designed to prevent weight gain in women who eat out frequently (Timmerman & Brown, 2012). The Mindful Restaurant Eating study was developed using Pender’s Revised Health Promotion Model (Pender, Murdaugh, & Parsons, 2006). The data utilized in this study were from both the intervention and control groups prior to the intervention. Institutional review board approval by the university was received prior to data collection.
Participants and Recruitment
The target population were healthy, perimenopausal women (40-59 years old) who ate out at restaurants regularly. The exclusion criteria included (1) eating out less than three times per week; (2) currently using appetite suppressants, weight loss medications, or hormone replacement therapy; (3) concurrently being treated for eating disorders or obesity; (4) reporting newly diagnosed or unstable chronic health problems that affect eating, weight, or metabolism; and (5) reporting surgical menopause (Timmerman & Brown, 2012). Participants were recruited from a metropolitan area of central Texas using advertisements placed in various locations (i.e., newspapers, radio, television, email, the Internet, and bulletin boards). Participants were given a $20 gift card at the completion of baseline data collection.
Instruments
Background Information Questionnaire
The Background Information Questionnaire assessed demographic information, frequency of eating out, and recent patterns related to weight change and dieting status.
Number of Binge Episodes
The actual number of binge episodes was determined from 24-hour dietary recalls, using the multiple-pass method, which provides a more accurate assessment of dietary intake (Conway, Ingwersen, Vinyard, & Moshfegh, 2003). Three days of dietary intake were collected including two week days and one weekend day, which are considered necessary for representative intake (St. Jeor, 2002). For each eating episode, participants were asked whether they had consumed an excessive amount of food and if they felt their eating was out of control, both considered essential components to the definition of binge eating based on the Diagnostic and Statistical Manual of Mental Disorders, 5th edition criteria (American Psychiatric Association, 2013). An eating episode was coded as a binge when participants answered yes to both questions.
Binge Eating Scale
The Binge Eating Scale (BES) measured binge eating severity using 16 items with half addressing the behavioral manifestations of binge eating and the other half addressing feelings and thoughts associated with binge eating (Gormally, Black, Daston, & Rardin, 1982). Concurrent validity was established with a sample of healthy women who engaged in nonpurge binge eating at least twice a month; the total BES score was significantly correlated (r = .48; p < .001) with the number of binge eating episodes (Timmerman, 1999). Two-week test–retest reliability was also significant for the total BES score (r = .87; p < .001; Timmerman, 1999). For this sample, the BES was internally consistent with a Cronbach’s α of .84.
Emotional Eating Scale
The Emotional Eating Scale (EES) measured eating in response to emotions using 25 items and a 5-point Likert-type scale with responses ranging from no desire to eat to an overwhelming desire to eat (Arnow, Kenardy, & Agras, 1995). Construct, discriminant, and criterion related validity was established in two studies with obese females being treated for binge eating and weight loss (Arnow et al., 1995). Based on a factor analysis, three subscales emerged: anger/frustration, anxiety, and depression (Arnow et al., 1995). For this sample, the EES was found to be internally consistent, with a Cronbach’s α of .93 for total score (Timmerman & Brown, 2012).
Self-Efficacy for Eating Behaviors Scale
Diet-related self-efficacy was measured by the Self-Efficacy for Eating Behaviors Scale (SEEBS; Sallis, Pinski, Grossman, Patterson, & Nader, 1988), using a 5-point Likert-type scale that rates participants’ confidence to motivate themselves to do things like these regularly for at least 6 months (Sallis et al., 1988). Criterion-related validity was supported by a significant correlation (p < .001) between the SEEBS and a health healthy dietary index derived from food frequency questionnaires with a sample of university students and staff (Sallis et al., 1988). Five subscales were identified using factor analysis: (1) Resisting Relapse, (2) Reducing Calories, (3) Reducing Salt, (4) Reducing Fat, and (5) Behavioral Skills (Sallis et al., 1988). The reducing salt subscale was not used for this study since it was not central to weight management. Additionally, four items were revised, using at a restaurant or eating out instead of at a party. The SEEBS was internally consistent with a Cronbach’s α of .93 for the 49 items used in this study (Timmerman & Brown, 2012).
Procedures
Respondents to the ads were screened by telephone to determine eligibility. A face-to-face meeting was set up to obtain written informed consent and collect data. During that meeting, participants completed the Background Information Questionnaire, the EES, the SEEBS, and the BES. Additionally, weight was measured on a calibrated scale in light clothing, and height was measured without shoes on a stadiometer (Timmerman & Brown, 2012). The first of three 24-hour dietary recall was collected at the meeting, and two more 24-hour dietary recalls were randomly collected by phone within the week, capturing a total of two weekdays and one weekend day (Timmerman & Brown, 2012).
Results
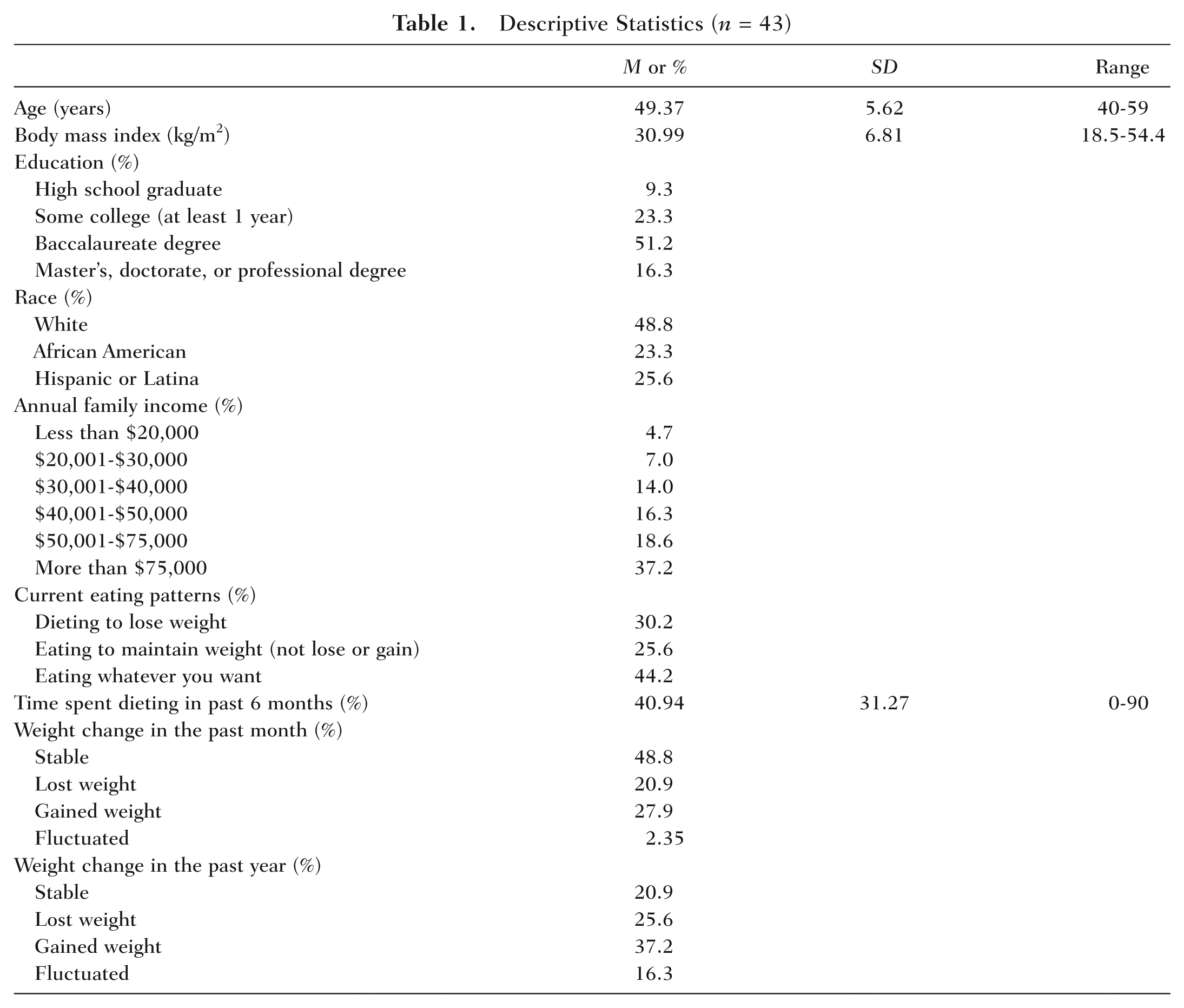
A total of 43 participants were recruited for the pilot study. See Table 1 for complete demographic information. The mean age of the participants was 49.37 (SD = 5.61) with a range of 40 to 59 years. The sample was triethnic: 48.8% were Caucasian, 23.3% African American, and 25.6% Hispanic. The majority of the sample had at least a baccalaureate degree (51.2%) and reported earning more than $50,000 annually (55.8%). The average calculated body mass index was 30.99 kg/m2 (SD = 6.81). Of the women who reported no dieting behaviors at the time of the survey (69.8%), 25.6% stated they were eating to maintain (not lose or gain) current weight and 44.2% were eating whatever they wanted. Almost all the participants reported some dieting behavior within the past 6 months, with the percentage of time spent dieting over the past 6 months ranging from 0% to 90%. Approximately half (48.8%) of the women surveyed reported a stable weight over the past month; however, the number of women who reported that they maintained a stable weight over the past year dropped to 20.9%. The number of nonpurge binge eating episodes ranged from 0 to 5 over the 3 days sampled and the average number of binges was 1.1 (SD = 1.2).
Descriptive Statistics (n = 43)
Research Question 1
Table 2 presents the partial Pearson correlations, controlling for age and BMI, among emotional eating, binge eating severity, diet-related self-efficacy, and the actual number of binges reported during the 3 days sampled. The total scores on the Emotional Eating Scale, along with the scores on Depression, Anger, and Anxiety subscales, were significantly related to binge eating scores. The SEEB scores were not significantly correlated to Emotional Eating scores, but there was a significant negative correlation between the total SEEB score and BES score (partial r = −.49; p ≤ .05). The total number of binges was significantly negatively correlated with the Resisting Relapse subscale of the SEEB scale (partial r = −.37; p ≤ .05) and positively correlated with the Anger subscale (partial r = .34; p ≤ .05). The correlations between emotional eating and binge eating suggests that eating excessive amounts and feeling out of control when eating are linked to eating in response to emotions. The correlation between the total number of binges and the Anger subscale suggests that binge eaters are more likely to experience binge eating behavior while feeling angry.
Partial Correlations of Emotional Eating, Binge Eating, Eating Self-Efficacy, and Total Number of Reported Binges, Controlling for Age and BMI (n = 43)
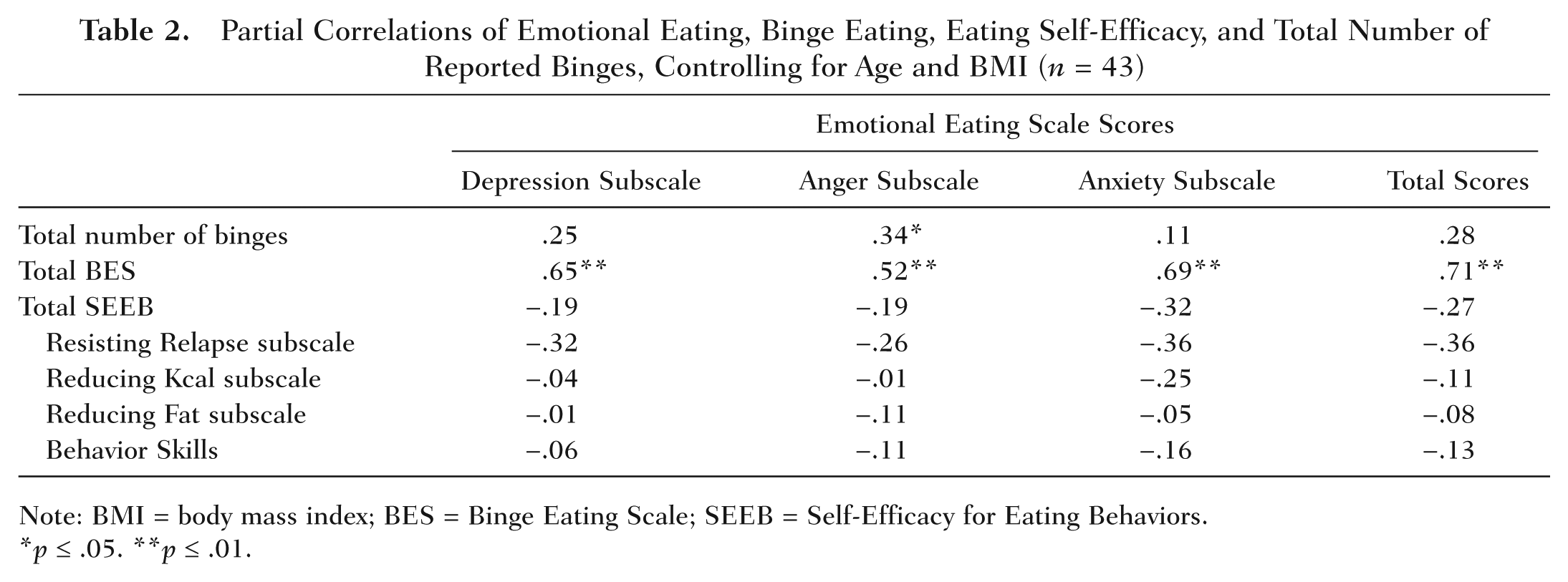
Note: BMI = body mass index; BES = Binge Eating Scale; SEEB = Self-Efficacy for Eating Behaviors.
p ≤ .05. **p ≤ .01.
Research Question 2
To compare the differences in emotional eating, diet-related self-efficacy, and number of binges between those individuals with a low and those with a high severity of binge eating, the participants were divided into two groups based on previously established cut off scores (Greeno, Marcus, & Wing, 1995; Timmerman, 1999). Those with a total BES score ≤17 constituted the low severity group (n = 28), and those with a total BES score ≥18 constituted the moderate combined with high severity group (n = 15).
There were significant differences between the low and high severity binge eating groups for total EES scores and the Depression, Anger, and Anxiety subscales (see Table 3). The difference between these two groups on the Resisting Relapse (p = .05) and the Reducing Calories (p = .09) subscales of the SEEBS approached significance. There were no other significant differences in the means of the SEEBS. There were no significant differences between the low and high severity binge eating groups for the total number of binges occurring for the 3 days sampled.
Comparisons of Emotional Eating, Eating Self-Efficacy, and Number of Binges for Low Severity and High Severity of Binge Eating Behavior
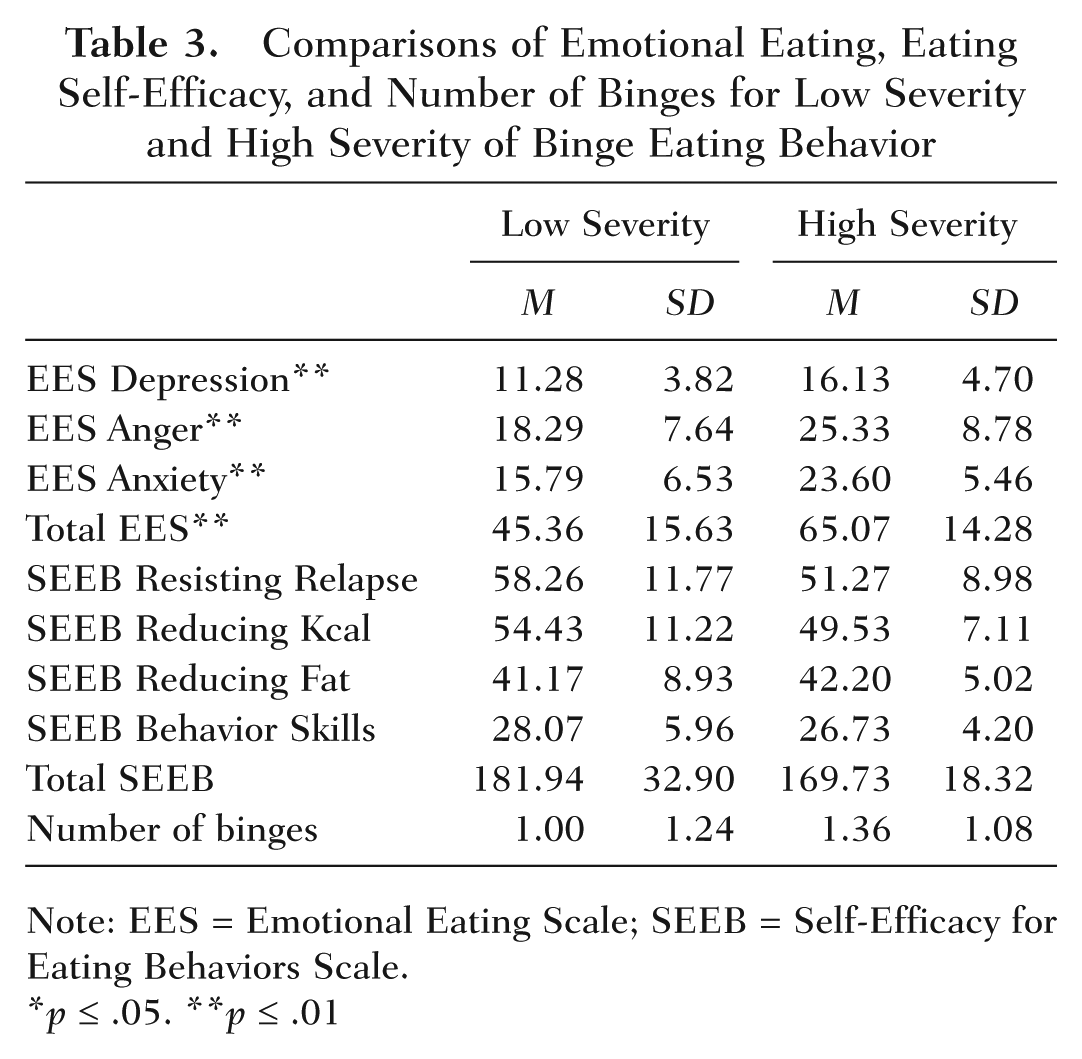
Note: EES = Emotional Eating Scale; SEEB = Self-Efficacy for Eating Behaviors Scale.
p ≤ .05. **p ≤ .01
Conclusions
Understanding the relationships between an individuals’ emotional responses (emotional eating), mental experiences (perceived diet-related self-efficacy), and eating behaviors (binge eating) may provide important insight to prevent weight gain. The bottom line for weight management is calories; to lose weight one needs to be in a caloric deficit (Jensen et al., 2013). However, to successfully manage caloric intake, a holistic approach is needed to address eating patterns that influence each individual’s calorie consumption (e.g., emotional eating, diet-related self-efficacy, binge eating). Prevention of weight gain during the perimenopausal years is especially important since it is a high-risk time for weight gain, and the weight gained is stored abdominally increasing the risk for chronic lifestyle diseases. Thus, there remains a critical need for effective interventions for weight gain prevention in this population.
In the present study, data from a sample of healthy overweight and obese women who ate out at least three times a week were examined to explore the relationships among number of binge episodes, binge eating severity, emotional eating, and diet-related self-efficacy. Consistent with past studies (Brown et al., 2010; Eldredge & Agras, 1996; Goodrick et al., 1999; Kenardy et al., 1996; Masheb & Grilo, 2006; Noli et al., 2010; Pinaquy et al., 2003; Ricca et al., 2009; Zeeck et al., 2011), participants who reported higher levels of emotional eating were more likely to also experience higher levels of binge eating severity. Since the majority of past studies on emotional eating and binge eating have focused on the BED population, the present study extends those findings by showing that emotional eating and binge eating appear to be linked even in women without eating disorders. This suggests that strategies needed to address binge eating behavior may need to include developing competencies in the area of stress management, including cognitive restructuring.
The present findings indicate that women with higher binge eating severity also had less diet-related self-efficacy, especially with regard to resisting relapse and reducing calorie intake. This is of particular interest. Self-efficacy continues to be an important predictor of successful lifestyle change (McAlister et al., 2008), and the most effective mechanism for increasing self-efficacy is successful mastery experiences (Pender et al., 2006). Perhaps the very nature of binge eating, in which a perceived loss of control is central, negatively affects one’s ability to consistently feel like one is maintaining mastery or successfully attain dietary goals; thus, negatively affecting self-efficacy.
Participants in the Mindful Restaurant Eating intervention (Timmerman, 2011) had significantly reduced binge eating severity (p = .004) following the intervention, which focused on developing the skills needed to manage calories and fat intake when eating out. These skills included knowledge about managing weight along with the calories eaten at restaurants, mindful eating meditations, individualizing strategies, and theory-based behavior change strategies such as building self-efficacy by experiencing mastery (e.g., weekly goals and homework; Timmerman & Brown, 2012). Mean BES total scores were 15.4 (6.5) for the intervention group (n = 19) at Time 1 versus 9.5 (5.4) at Time 2, and 13.9 (7.6) for the control group at Time 1 versus 13.3 (7.9) at Time 2 (Timmerman, 2011). This further supports the relationships between binge eating severity, experiences of mastery, and diet-related self-efficacy and indicates that diet-related self-efficacy and reduced binge eating severity may be affected by planned interventions that incorporate experiences of mastery, even when regularly exposed to the high-risk food environment of restaurants.
Another possible explanation for the improvement in binge eating for intervention participants could be the use of mindful eating meditations. In a research study using the Mindfulness-Based Eating Awareness Training intervention, there was a decrease in number of binge episodes, reduced BES scores, and a decrease in depression in obese women with BED (Kristeller & Wolever, 2011). In a systematic review, mindfulness training contributed to positive changes in disordered eating, particularly emotional eating, but authors cautioned that mindfulness alone may not produce significant changes in weight without some other sort of weight loss strategy or program (Katterman, Kleinman, Hood, Nackers, & Corsica, 2014), such as the strategies incorporated into the Mindfulness-Based Eating Awareness Training. However, mindful eating meditations as an intervention component in a comprehensive, holistic approach to weight management may prove especially helpful in addressing binge eating behavior in women without BED.
The main limitation of this study is its small convenience sample; generalizing the findings to other samples should be done with caution. Additionally, the cross-sectional design with self-report measures precludes drawing conclusions about possible temporal relationships among the variables studied (Houser, 2012). Further research needs to tease out how binge eating behavior is related to diet-related self-efficacy. Despite these limitations, this study adds to the literature by examining the relationships between binge eating severity, emotional eating, and diet-related self-efficacy in a non–eating-disordered population. The study also provides support for the interconnectedness between emotions, thoughts, and behaviors.
This secondary analysis of the Mindful Restaurant Eating study had a sample that was limited to women who ate out at least three times per week. Since restaurants have been identified as a high-risk food environment that contributes to loss of control and excess consumption for those who binge eat (Timmerman, 2006), participants in this study who ate out regularly may have had greater binge eating severity and number of binge episodes as compared with women who ate out less. Further research is needed to determine potential differences in eating patterns (e.g., binge eating and emotional eating) between women who eat out frequently and those who do not.
Assessing eating patterns that contribute to weight gain in perimenopausal women may provide useful information for tailoring interventions. The complex nature of weight management mandates a holistic, patient-centered approach that recognizes the interconnectedness of the mind, body, emotions, and spirit within the context of one’s environment. Future interventions may need to address how to manage emotional eating and to increase diet-related self-efficacy in order to combat binge eating and to provide protection from weight gain in perimenopausal women.
Footnotes
Funding for this study was provided to Gayle M. Timmerman (the University of Texas at Austin) by the North and Central Texas Clinical and Translational Science Initiative (5UL1RR024982-03), National Institutes of Health.