
Abstract
Introduction
Infertility has been known to adversely affect psychological, marital, and social distress of couples, including depression, stigma, sexual dysfunction, marital dissatisfaction, and withdrawal from their family and friends (Casu & Gremigni, 2015; Greil, Slauson-Blevins, & McQuillan, 2010; Kim & Shin, 2013; Onat & Beji, 2011; Sherrod, 2004). One approach to assessing the impacts of infertility is to measure the quality of life (QoL; Aart et al., 2011; Boivin, Takefman, & Braverman, 2011). QoL is a conceptual indication of physiological, psychological, and social health (WHOQOL Group, 1995) and is a holistic approach to complex health conditions (Aart et al., 2011); it has been used frequently to examine the status of infertile patients (Aart et al., 2011; Boivin et al., 2011; Kim & Shin; 2013; Valsangkar, Bodhare, Bele, & Sai, 2011). Although infertility affects the QoL of couples, gender differences in QoL within a couple have also been identified (Monga, Alexandrescu, Katz, Stein, & Ganiats, 2004; Onat & Beji, 2011). Many studies have found that infertile women reported more extensive QoL impairments compared with the QoL reported by infertile men (Kissi et al., 2014; Ragni, Mosconi, & Baldini, 2005; Rashidi et al., 2008). In addition, published research reported that main factors influencing the QOL were infertility-related distress (Kim & Shin, 2013; Min, Kim, & Cho, 2008), the marital relationship (Chachamovich, Chachamovich, Zachia, Knauth, & Passos, 2007; Gamerio, Moura-Ramos, Canavarro, Santos, & Dattilito, 2011; Kim & Shin, 2013; Monga et al., 2004; Onat & Beji, 2011; Peterson, Newton, & Rosen, 2003; Valsangkar et al. 2011), and depression (Chachamovich et al., 2009; Chachamovich, Chachamovich, Ezer, Cordova, et al., 2010; Kim & Shin, 2013).
However, most of these studies have focused on the infertile individual’s response (Chachamovich et al., 2007; Chachamovich, Chachamovich, Ezer, Cordova, et al., 2010; Kim & Shin, 2013; Valsangkar et al., 2011), and even though some research has been conducted using a dyadic approach, it has been found that specific factors affect only the infertile individual, not the spouse (Chachamovich et al., 2009; Gamerio et al., 2011; Peterson et al., 2003). As infertility is a common problem within couples, distress and well-being could be affected not only by the individual perceptions of infertility but also by the partner’s perceptions (Benyamini, Gozlan, & Kokia, 2009; Berg & Upchurch, 2007; Peterson et al., 2003). Family systems theory also proposes that individuals are better understood through their relationship with family members rather than through studying individuals independently (Peterson et al., 2003). Therefore, a dyadic approach may be suitable for use in studies of infertility.
Recent studies of couples suggested that studies of infertility should take into account the partners’ appraisal of the situation, also known as the partner effect (Benyamini et al., 2009; Peterson, Pirritano, Christensen, & Schmidt, 2008). These authors also emphasized the need for statistical methods that focus on the dyad as the unit of analysis (Berg & Upchurch, 2007). One of the statistical methods used to analyze dyadic data is the actor–partner interdependence model (APIM) developed by Kenny (1996), which has been used in studies of couples’ interactions. The APIM examines the influence of a causal variable on individual outcomes (called the “actor affect”) and on spousal outcomes (called the “partner effect”; Kenny & Ledermann, 2010). The APIM also emphasizes that dyadic data are likely to be correlated. If such correlations are ignored, interdependent data can bias significance (Kenny, 1996). Because infertile couples have interacted for a long time, the dyadic data may be interdependent. Therefore, studies of infertility should be conducted using a dyadic approach in data collection and analysis.
This study was conducted to compare the level of infertility stress, marital adjustment, depression, and the QoL between couples and to examine actor and partner effects of these variables on the QoL. The results may help nurses be aware of such effects and can be used as a baseline data in the development of nursing interventions for infertile couples.
We developed a hypothetical model based on the APIM (Kenny, 1996) and previous research before conducting this study (Figure 1). The hypotheses are as follows: Wife’s infertility stress, marital adjustment, depression, QoL interacts with husband’s infertility stress, marital adjustment, depression (4 hypotheses). Wife and husband’s variables (infertility stress, marital adjustment, and depression) affect wife and husband’s QoL (12 hypotheses). The former hypotheses represent how infertility stress, marital adjustment, depression, and QoL of the wife interact with those of husband, while the latter hypotheses demonstrate the influence of these variables in the wife and husband influence their own and spouse’s QoL.
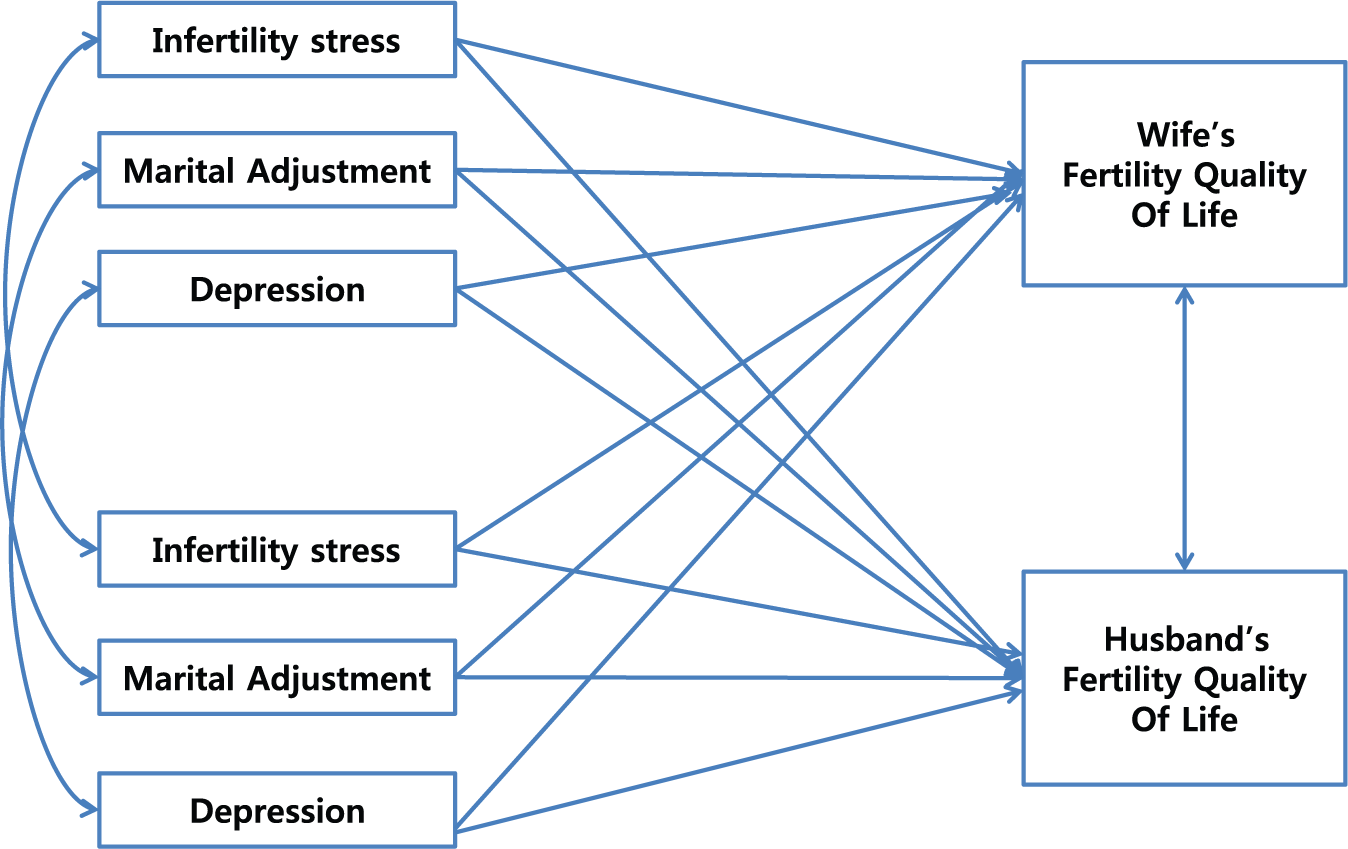
Hypothetical Model: Effects of Infertility Stress, Marital Adjustment, and Depression on the Quality of Life in Infertile Couples.
Method
Design
This study used a cross-sectional research design and a dyadic approach to examine the actor and the partner effects of infertility stress, marital adjustment, and depression on QoL in infertile couples.
Sample, Setting, and Ethical Consideration
The study was conducted between November 2012 and March 2013 in Cheil General Hospital in Seoul, South Korea. This is one of the largest infertility hospitals that performs approximately 400 artificial reproduction procedures per month. Infertile couples visiting the infertility clinic for medical treatment formed part of the study sample. Inclusion criteria were (a) a diagnosis of infertility by an obstetrician or medical doctor, (b) primary or secondary infertility without history of parity, and (c) and one or more infertility treatments.
One hundred and thirty couples were recruited and invited to participate in the research; complete data for 121 couples were obtained (93.1%). Two couples refused because they were unwilling to expose their infertility, and seven couples were excluded due to incomplete questionnaires by the wife or husband, which limited the dyadic analyses. The final sample comprised 121 husbands and wives. The optimal sample size for path analysis varies, but Hair, Black, Babin, Anderson, and Tatham (2006) classified five factors affecting sample size and proposed that 100 to 150 participants were acceptable for path analysis. Based on their study, our sample size was adequate.
This study protocol was approved by the Institutional Review Board of the hospital where the research took place (No. CGH-IRB-2011-83). All the respondents were informed of the objectives of the study. They were also assured that the data that they provided would be confidential and used in this study only and that a decision to withdraw from the study would not compromise the standard of care that they received at the clinic. All the participants signed informed consent forms before this study began.
Measures
General Characteristics
General characteristics of the participants included age, educational level, employment status, religion, and monthly family income. Infertility-related characteristics were the length of marriage, infertility treatment period, number of infertility treatments, financial burden of infertility treatments, and the cause of infertility.
Infertility Stress
Infertility stress was measured using the Fertility Problem Inventory (FPI), developed by Newton, Sherrard, and Glavac (1999) and translated into Korean by Kim and Shin (2014). The FPI is a 46-item, self-report, multidimensional measure that identifies infertility-related problems in five homogeneous domains: social concerns, sexual concerns, relationship concerns, the need for parenthood, and the rejection of a childfree lifestyle. A composite score is derived by summing the five domain scores, which results in a global measure of perceived infertility-related stress. The FPI requires respondents to indicate their degree of agreement with statements on a 6-point Likert-type scale ranging from 1 = strongly disagree to 6 = strongly agree. The overall score ranges from 46 to 276; a high score is associated with high fertility-related stress. Cronbach’s alpha was .92 in this study.
Marital Adjustment
Marital Adjustment was measured using the Revised Dyadic Adjustment Scale developed by Spanier (1976), but modified and translated into Korean by Choi (2004). This 14-item questionnaire has three subscales: marital satisfaction, marital cohesion, and marital consensus. A high score is associated with positive marital adjustment. Cronbach’s alpha was .84 in this study.
Depression
Depression was measured using the Beck Depression Inventory developed by Beck (1967) and translated into Korean by Lee and Song (1991). The Beck Depression Inventory is a 21-item self-report instrument with items rated on a 4-point Likert-type scale; a higher score is associated with greater depression. Cronbach’s alpha was .80 in this study.
Quality of Life
QoL was measured by the fertility-related quality of life (FertiQoL) measure developed by the European Society of Human Reproduction and Embryology and the American Society of Reproductive Medicine. This measure has been translated into several languages, including Korean. The measure consists of 36 items that collectively assess the impact of fertility problems on the QoL. In addition, there is a core section related to personal and interpersonal QoL (“Core FertiQoL”) and an optional section relating to treatment (“Treatment FertiQoL”). The core FertiQoL is a 24-item self-report measure consisting of 6 items of each 4 domains: emotional, mind–body, relational, and social. The Treatment FertiQoL assesses QoL during treatment, including any medical inventions or consultations according to the treatment environment (6 items) and treatment tolerability (4 items). The FertiQoL items are rated on a 5-point Likert-type scale; higher scores are associated with a lower fertility-related QoL (Boivin et al., 2011). This study used only the core and treatment sections of the FertiQoL (24 items). Cronbach’s alpha was .93 in this study.
Procedures
Pilot Study
Before the data collection, a pilot study was conducted with couples with infertility to identify and resolve any potential problems. The pilot study participants included 10 couples meeting the inclusion criteria. The respondent confused the meaning of Item 22, “Having sex is difficult because I don’t want another disappointment.” That item was modified and supplemented. It was confirmed that estimated time for completing the questionnaire was between 20 and 40 minutes.
Data Collection
From November 2012 to March 2013, couples with infertility were invited to participate voluntarily in our study through a hospital announcement of poster. Those who agreed to participate were given letters explaining the purpose of the study, providing the researcher’s affiliation and contact information, and clearly stating that responses would be confidential and anonymity would be guaranteed. The couples agreeing to participate completed the questionnaires in a private counseling room. The average completion time was 30 minutes, and each participant received a coupon for a book as a gift for participating in the study.
Data Analysis
Statistical analyses were performed with SPSSWIN, 20.0, and AMOS 20.0 software (SPSS, Chicago, IL). Descriptive statistics, chi-square tests, t tests, and Pearson correlations were used to analyze respondent characteristics and variables. The APIM (Kenny, 1996) was used to assess the couple as the unit of analysis. The independent variables in this study were infertility stress, marital adjustment, and depression, and the dependent variables were the QoL of the wife and husband. The analyses evaluated interactions between variables affiliated with the wife and husband (4 paths) and for each combination of independent and dependent variables (12 paths). This resulted in 16 paths (Figure 1). To identify the actor and partner effects of infertility stress, marital adjustment, and depression on the QoL, path analysis was conducted, and the fitness of the model was identified by the goodness of fit index (GFI), normed fit index (NFI), comparative fit index (CFI), Tucker–Lewis index (TLI), and the root mean square error of approximation (RMSEA). Generally, the model is a good fit if the values of GFI, NFI, CFI, and TLI are higher than 0.9 and the RMSEA is lower than .05 (Hong, 2000).
Results
General and Infertility-Related Characteristics
The general and infertility-related characteristics of the participants are presented in Table 1. Wives aged 35 years and older accounted for 48.8% of the participants, and the percentage of husbands aged 35 years and older was 66.9% (χ2 = 8.20, p = .006). Regarding employment status, 72.7% of the wives and 98.3% of the husbands were employed (χ2 = 3.43, p < .001). The financial burden of infertility treatment was felt by 84.3% of the wives and 94.2% of the husbands (χ2 = 6.21, p = .021), in spite of government subsidies. More than half of the couples were married for more than 3 years (57.4%), and most couples (84.3%) had been treated for infertility for more than 2 years.
General and Infertility-Related Characteristics of Respondents (N = 242).
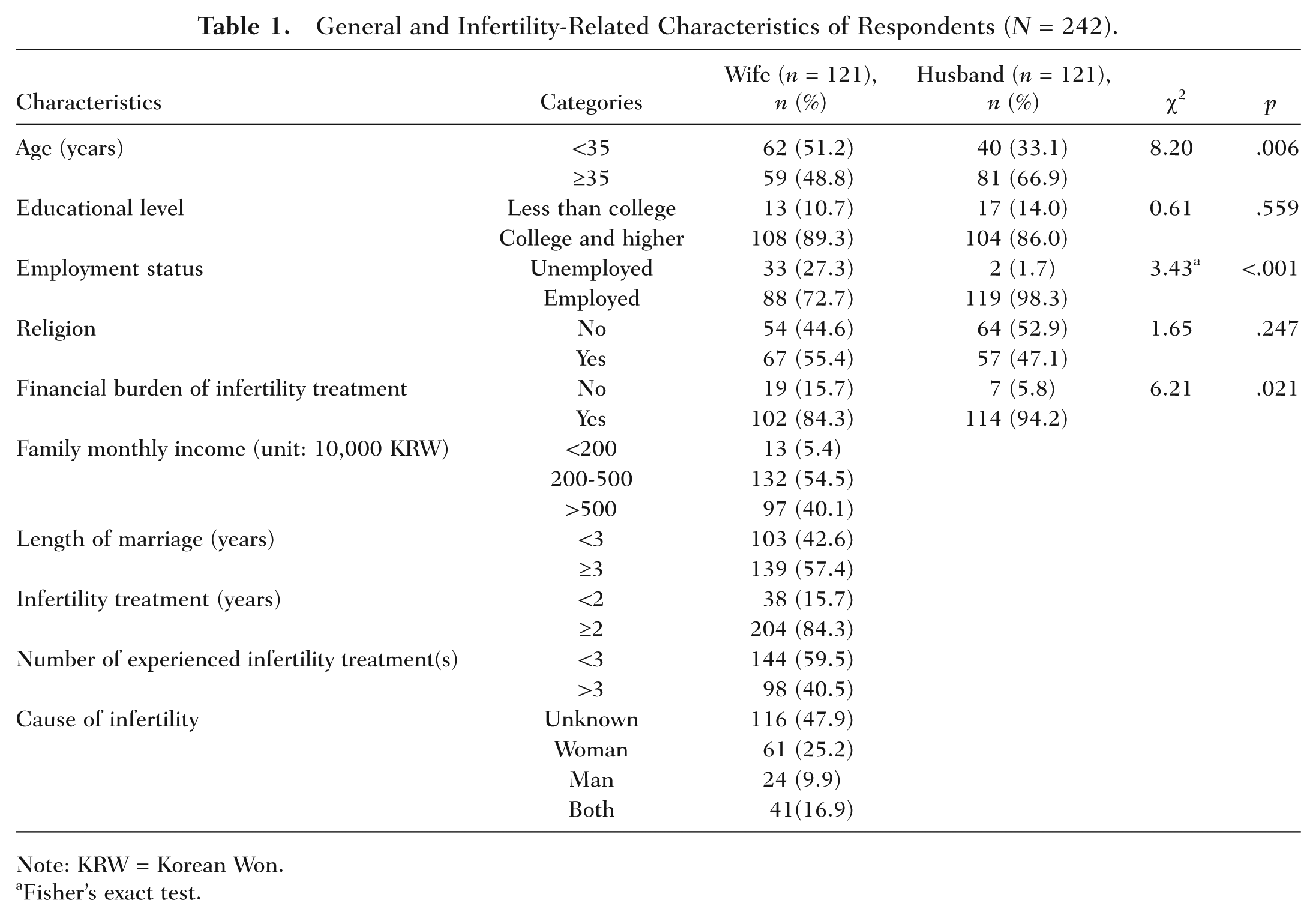
Note: KRW = Korean Won.
Fisher’s exact test.
Gender Difference in QoL, Infertility Stress, Marital Adjustment, and Depression
The gender differences in QoL, infertility stress, marital adjustment, and depression of wives and husbands are presented in Table 2. Wives reported higher levels of infertility stress (t = −3.61, p < .001) and depression (t = −6.83, p < .001) and lower levels of QoL (t = 7.24, p < .001) compared with their husband’s reports. However, wives reported lower values of marital adjustment than their husbands did, but this difference was not significant (t = 0.82, p = .414).
Gender Differences in QOL, Infertility Stress, Marital Adjustment, and Depression (N = 242).

Significant Actor and Partner Effects on QoL
Descriptive Statistics for Variables
Before conducting the path analysis, we examined the descriptive statistics of the variables in the hypothetical model. The values of skewness and kurtosis of all variables were within critical range (±1.96) for all variables at the .05 significance level (Hair et al., 2006), and we concluded that the model met normal distribution standards. In addition, we evaluated the correlation of variables; if the correlation is higher than .90, there is multicollinearity between variables (Hair et al., 2006). In this study, the Pearson correlation coefficients of all variables were lower than 0.9, which indicated no multicollinearity.
Testing and Modifying of Hypothetical Model
The values of the statistics used to evaluate model fitness were GFI = 0.91, NFI = 0.90, CFI = 0.91, TLI = 0.83, and RMSEA = 0.10; the indexes of TLI and RMSEA were low. Based on previous research (Kim & Shin, 2013; Peterson et al., 2003) and modified indexes, we added four paths from infertility stress and marital adjustment to depression for both the wife and husband (Figure 2). Values of fit statistics for the modified model were GFI = 0.95, NFI = 0.92, CFI = 0.91, TLI = 0.94, and RMSEA = 0.04; these indexes were within recommended levels. Therefore, the modified model was accepted.
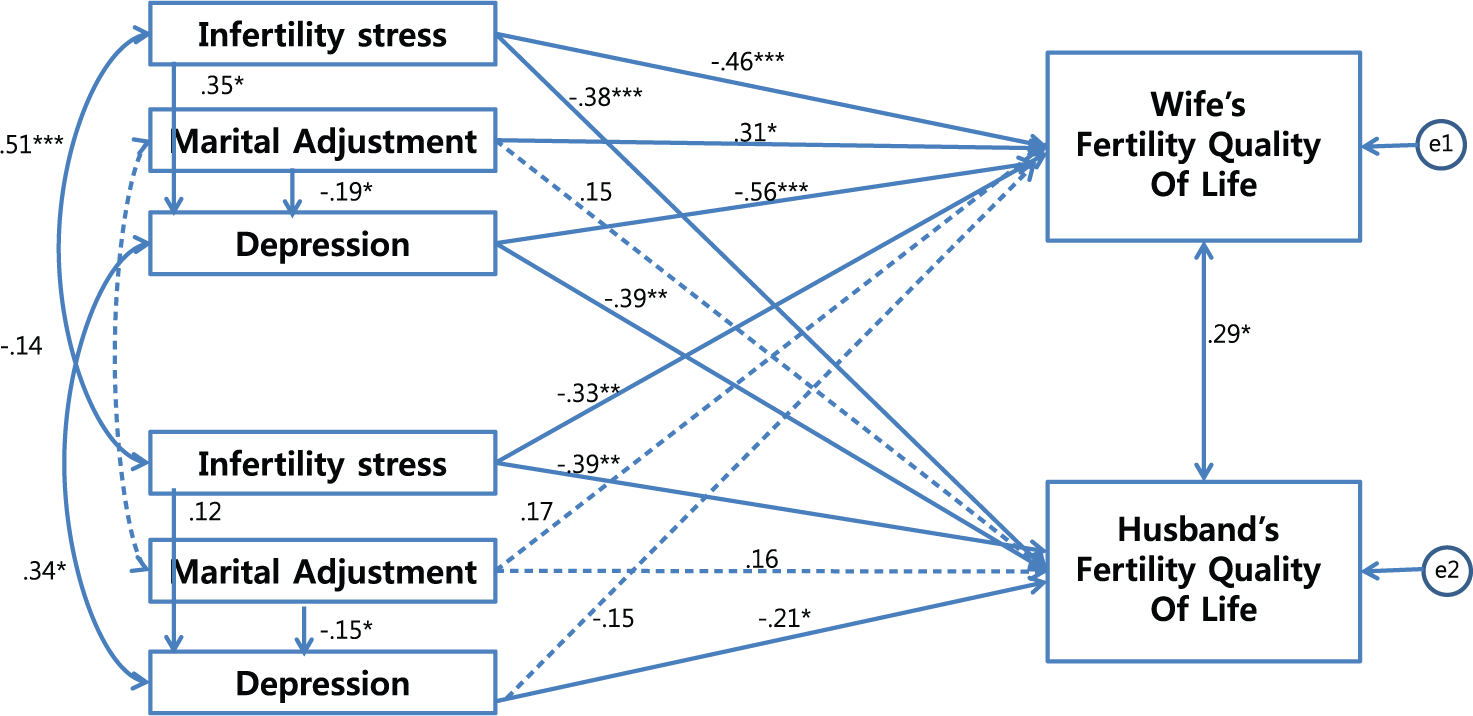
Effects of Infertility Stress, Marital Adjustment, and Depression on the Quality of Life in Infertile Couples.
Path Analysis
The results of the path analysis are presented in Figure 2. The infertility stress of the wife had a negative effect on her QoL (β = −.46, p < .001) and the QoL of her husband (β = −.38, p < .001). The marital adjustment reported by the wife positively affected her QoL (β = .31, p = .016), but did not affect the QoL of her husband (β = .15, p = .617). However, there was an indirect effect on the QoL of her husband with depression as the mediator (β = −.20, p = .041). The wife’s depression negatively influenced her QoL (β = −.56, p < .001) and the QoL of husband (β = −.39, p = .006). Infertility stress reported by the husband had a negative effect on his QOL (β = −.39, p = .009) and the QoL of his wife (β = −.33, p = .005). Marital adjustment reported by the husband did not affect his QoL (β = .16, p = .891) or the QoL of wife (β = .17, p = .214), but had an indirect effect on his QoL through the mediator of depression (β = −.30, p = .046). Depression reported by the husband negatively influenced his QoL (β = −.21, p = .026), but not the QoL of wife (β = −.15, p = .297). The infertility stress, depression, and QoL reported by the wife interacted with the infertility stress (β = .51, p < .001), depression (β = .34, p = .043), and QoL (β = .29, p = .012) of her husband. The model accounted for 42% and 33% of the variance in the QoL of wife and husband, respectively.
Discussion
The purpose of this study was to compare infertility stress, marital adjustment, and depression in wives and husbands and to examine the actor and partner effects of these variables on the QoL of infertile couples.
Gender Difference in Variables
This study found that the QoL of infertile women was significantly lower than their husbands’ QoL, which supports previous research (Chachamovich, Chachamovich, Ezer, Fleck, et al., 2010; Greil et al., 2010; Kissi et al., 2014; Ragni et al., 2005; Rashidi et al., 2008). However, some studies (Chachamovich et al., 2009; Onat & Beji, 2012) reported that the QoL of the wife and husband did not differ significantly. The reason for discrepancy of findings is likely due to the sensitivity of the QoL measurement instrument. Unlike infertility-specific instruments, general QoL instruments have no questions specific to infertility. Therefore, general instruments lack specificity for infertility stress and may not be sensitive enough to access the specific effects of infertility on QoL (Aart et al., 2011; Boivin et al., 2011; Newton et al., 1999; Mousavi, Masoumi, Keramat, Pooralajal, & Shobeiri, 2013). The use an infertility-specific QoL measurement tool is recommended for studies assessing factors related to infertility (Aart et al., 2011; Mousavi et al., 2013). In this study, we used the FertiQoL, whereas Onat and Beji (2011) and Chachamovich et al. (2009) used the WHOQOL, a general QoL measure, to measure the QoL of infertile couples.
This research showed that the scores of infertility stress and depression of the wife were statistically higher than the scores of the husband. These results correspond with the results of earlier studies that reported women suffered significantly higher levels of infertility-related stress and depression (Kissi et al., 2013; Peterson et al., 2003; Wichman, Ehlers, Wichman, Weaver, & Coddington, 2011). It is likely that women generally experience a more complex process of infertility treatment and may have a stronger drive to have a child (Greil et al., 2010).
We found no gender differences in marital adjustment; this finding is consistent with the results of previous research, which reported that total scores on the Dyadic Adjustment Scale indicated no difference between men and women (Peterson et al., 2003). However, a systematic review of the marital relationship in infertility reported that infertile men reported greater marital satisfaction than their wives did (Tao, Coates, & Maycock, 2012). This seemingly contradictory finding may be related to the use of the marital satisfaction variable, which is only one of the three subscales of marital adjustment and does not represent the full complement of marital adjustment factors. In this study, marital satisfaction reported by the husband was significantly higher than reported by his wife (p = .043), but there was no gender difference in marital adjustment.
Significant Actor and Partner Effects on QoL
Tests of our modified model indicated that infertility stress of spouses had both actor and partner effects on QoL. Infertility stress negatively affects not only the individual’s QoL but also affects the QoL of his or her spouse. It is difficult to compare these results with previous studies because there is little previous research on infertility stress in dyads. Nevertheless, this result supports the findings of previous studies that infertility stress had a main effect on the QoL (Kim & Shin, 2013; Min et al., 2008). Some research has emphasized the importance of partner effects in infertility stress; one study reported that a partner’s psychological adjustment was related to their perception of infertility (Benyamini et al., 2009), and another study demonstrated that congruence of infertility stress between partners was related to marital adjustment and depression (Peterson et al., 2003).
This study also found that a wife’s depression had both actor and partner effects, but husband’s depression had only actor effects. In accordance with previous studies, researchers have found that the QoL of infertile women was affected by depression (Kim & Shin, 2013; Min et al., 2008) and that psychological distress, including depression, was main predictor of QoL in infertile men (Chachamovich, Chachamovich, Ezer, Fleck, et al., 2010). Dyadic research has indicated that older women with husbands with high levels of depression may be particularly at risk for depression (Ayotte, Yang, & Jones, 2010). As seen in our study, there was a reciprocal relationship in depression between spouses. In addition, depression mediated infertility stress and marital adjustment; this finding is in accordance with that of previous research (Kim & Shin, 2013). Therefore, to enhance the QoL for infertile couples, evidence-based intervention and counseling to reduce infertility stress and depression should be provided to the couples rather than each individual.
In the case of marital adjustment, the wives reported an actor affect, but husbands had neither actor nor partner affects. This finding corresponds with those of previous studies, which reported that marital conflict reduced the QoL of women and that higher marital satisfaction was related to higher QoL ratings (Gamerio et al., 2011, Kim & Shin, 2013; Monga et al., 2004; Onat & Beji, 2011; Valsangkar et al., 2011). On the other hand, our finding for the husbands’ ratings of marital adjustment differed from previous research, which found that low marital relationship scores were associated with lower QoL scores (Drosdzol & Skrzypulec, 2008; Lau et al., 2008). The reason for this discrepancy may be due to the contribution of sexual functioning, which was not included in our study. Published studies reported that sexual functioning was the most important predictor of the QoL in men (Drosdzol & Skrzypulec, 2008; Shindel, Nelson, Naughton, Ohebshalom, & Mulhall, 2008). The marital adjustment measurement tools used in our study included marital satisfaction, cohesion, and consensus, but not sexual functioning.
Conclusion
This study found gender differences and actor and partner effects on emotional aspects of infertility such as infertility-related stress, depression, marital adjustment, and QoL in infertile couples. These findings suggest nurses who take care of infertile couples must take into account gender difference and partner effects on emotional aspect during physical intervention and counseling. And this result can be used as a baseline data in the development of nursing knowledge for infertile couples.
There are several limitations to our study. First, although the sampled hospital is one of the largest infertility hospitals in Korea, participants in this study were limited to the clinic-based couples seeking treatment for their infertility. Because the participants of this study do not represent the entire range of infertile couples, future studies should include infertile couples not seeking treatment. Second, this study focused on the effect of infertility stress, marital adjustment, and depression; other studies have reported that sexual functioning variables and interpersonal variable such as social support also affect the QoL (Chachamovich et al., 2007; Kim & Shin, 2013; Shindel et al., 2008). Therefore, future studies should include those variables.