
Abstract
Problem and Significance
Nurses are often responsible for performing medically necessary invasive procedures that produce pain, fear, sadness, discomfort, and anxiety. These negative experiences may be more traumatic in the pediatric population due to a child’s developmental level and sometimes his or her limited ability to communicate needs. Appropriately managing these uncomfortable invasive procedures is essential in all age groups. Children, however, may not receive adequate procedural comfort interventions despite modern knowledge, availability of treatments or interventions, and the ability to significantly reduce or avoid these discomforts (American Academy of Pediatrics, 2001). The American Society for Pain Management Nursing refers to comfort management as more holistic and incorporating the use of pharmacological and nonpharmacological procedural interventions, which can enhance patient comfort and overall procedural management (Czarnecki et al., 2011). However, there is minimal data demonstrating how a child perceives holistic comfort related to nursing procedures.
Based on the pediatric procedural pain literature, providing pediatric holistic procedural comfort measures are superior to strictly managing pain. Nurse theorist Katharine Kolcaba (1994) contends that comfort is holistic and should not be confused with pain because it involves more than physical ailment or suffering. Holistic comfort is more clearly defined in the adult population but poorly defined in children. Limited research exists on the perceptions of comfort related to procedures as described by a child. The majority of extant research on pediatric comfort or comfort measurement is defined by the absence of pain, fear, anxiety, and distress (Bice & Wyatt, 2016). Whereas comfort during invasive procedures certainly includes lower levels of these feelings, it may not represent the concept of procedural holistic comfort completely. In order to measure procedural holistic comfort in children, it was necessary to gain an understanding of the concept from the child’s perspective. Otherwise a child’s comfort needs are strictly interpreted by adults rather than provided according to a child’s insights.
There is extant literature that separately measures outcomes of pediatric pain interventions (Bice, Gunther, & Wyatt, 2014). Extensive literature also exists on measuring components of comfort in children during invasive procedures by providing interventions such as music, caregiver facilitation, the use of toys, screen time, or play and pharmacological intervention (Bice & Wyatt, 2016). This study moves away from strictly focusing on pain and aimed to explore perspectives of children and their caregivers regarding procedural holistic comfort.
Literature Review
Holism
In this study, comfort was examined from a holistic perspective. The Oxford dictionary describes holism as an understanding that all parts of a whole are constantly connected; that treating a person holistically means to consider not only physical elements but also social and mental factors (Oxford Dictionaries, 2014b). The American Holistic Nurses Association (2016) recognizes that holistic care is a collaborative relationship between the patient and their provider and incorporates treating the whole person. Another author simply states, “A single holistic approach to care is oxymoronic” because holism involves numerous remedies (Freeman, 2005). In a concept analysis, Tjale and Bruce (2007) indicated that holistic nursing incorporates two dimensions: the whole person and the mind–body–spirit. Tjale and Bruce argue that together these include emotional, social, physical, mental, and spiritual well-being.
Holism is considered essential to best spiritual nursing care practice: “Holistic nursing asserts the balance between mind, body, and spirit, and is necessary for optimal health” (Dell’Orfano, 2002, p. 380). A “return to a more holistic approach” to child health care is needed, involving not only the treatment of diseases but also special attention to well child care, child development, and health promotion (Schor, 2004, p. 210). Additionally, holism has been recognized as the core of the well-known concept of family-centered care, which has been defined as “a way of caring for children and their families within health services which ensures care is planned around the whole family” (Shields, 2007, p. 893). For the purpose of this study, the definition of holistic was inspired by the literature and is understood as an approach to caring that includes acknowledging and treating the whole child, with careful consideration of physical, psychological, social, cultural, spiritual, and environmental needs.
Comfort
No predetermined understanding of comfort for children was brought to this study. However, it is important to examine the description of comfort in research to date. The Oxford Dictionary defines comfort as physical ease and a lack of pain; a pleasant feeling, the state of well-being, or richness, and a relief of sorrow or distress (Oxford Dictionaries, 2014a). In an early understanding, Rankin-Box (1986) added that comfort is a “state of both mind and body” (p. 340) encompassing social, environmental, and cultural care and bound by influencing variables such as noise, sleep, warmth, communication, sight, lighting, and smell. Markham (1962) describes comfort as including provision of appropriate health information in order to alleviate fear and pain in language the patient comprehends. Morse, Bottorff, and Hutchinson (1994) argue that comfort is a state of embodiment that extends beyond human consciousness; it is more than just the relief of pain. Hamilton (1989) claimed comfort is distinctive and defined by each person differently. Kolcaba (2013) has theoretically analyzed comfort, defining it as “the immediate experience of being strengthened by having needs for relief, ease, and transcendence met in four contexts (physical, psychospiritual, sociocultural, and environmental); much more than the absence of pain or other physical discomforts” (p. 193). Note that many definitions of comfort in the literature are in fact holistic. We sought to capture how children describe being comforted, from a holistic perspective.
Procedural Comfort
A very recent systematic review of 33 studies revealed procedural comfort interventions for children existed in four major themes: music therapy, amusement and entertainment, caregiver facilitation, and a multifaceted approach of various interventions (Bice & Wyatt, 2016). The review also showed younger children experience higher levels of pain, anxiety, fear, and distress—demonstrating a likelihood of increased procedural comfort needs in children of younger age. In an earlier study, Hodgins and Lander (1997) examined children coping with fear and pain before and after venipuncture and found that in order to cope with these negative emotions, children reported looking away from the procedure, thinking of something else, wanting medications, tolerating the pain, seeking moral support, seeking an inanimate comfort source, trusting in the health care professional, or seeking physical comfort. Carnevale and Guadreault (2013) interviewed children in critical care and found that parents, food, entertainment, and hospital staff were reported comfort sources. A gap in the knowledge base was identified as a lack of understanding of procedural holistic comfort from the child and caregiver perspective, thus indicating a need for theory-building qualitative research.
Method and Theory
Study Design
A qualitative descriptive design was used in this study as this type of research is conducted by scientists who seek to understand descriptions of a natural phenomenon, particularly research related to human behavior (Sandelowski, 2000, 2010). Qualitative descriptive research, like all qualitative inquiry, is interpretive (Sandelowski, 2010). But it is typically less interpretive than other forms of qualitative research such as phenomenology, ethnography, or grounded theory (Sandelowski, 2000). A summary of accounts and occurrences as Sandelowski describes it, summarized by the participant, is relative to this type of approach. The researcher must stay close to the data or “data-near” (Sandelowski, 2010, p. 78) in order to best generate findings in line with participant imageries. In this study, descriptions of procedural holistic comfort were captured and interpreted as caregivers and children explained them.
Philosophical Perspective
The tenets of qualitative descriptive research are most closely associated with a naturalistic paradigm (Sandelowski, 2000). Blumer (1969) stated that investigators who are looking at a problem found in its natural form use naturalist inquiry. This philosophy embraces an “exploration of human life” (Blumer, 1980, p. 413). In a naturalistic approach, “the researcher does not search for data that fit his or her theory but develops a theory to explain the data” (Guba & Lincoln, 1982, p. 235). In this study, procedural holistic comfort was explored in the natural environment of the child immediately after a venipuncture procedure.
Procedures
This study was conducted after institutional review board approval was received from both the university and hospital where participants were recruited. The principal investigator (PI) and all those closely affiliated with the study signed a confidentiality agreement before the study began. Written informed consent from parents and verbal child assent was obtained. Risks associated with participating in this study for both the children and caregivers were relatively low. The research interventions were commensurate to those already in place for the venipuncture procedure, which was ordered by the child’s physician/practitioner. Children were asked to draw two pictures during their interview: (a) what it was like to get the needle poke today and (b) whatever he/she thought would make him/her feel better when they were receiving the needle poke. The child was given the choice to keep the picture. All drawings were digitally photographed and password-protected after the interview.
Rather than relying solely on adults’ descriptions, interviewing young participants directly allows them to give voice to their experiences (Eder & Fingerson, 2002). A basket of toys and activities was given to each child participant as a gift for their time. These items were chosen based on the existing evidence to support their alleviation of pain, fear, and distress (Bice & Wyatt, 2016). The value of each basket was approximately $20. Caregiver participants were also given a $20 VISA gift card for their time and inconvenience. Various toys were also provided on a carpet tile for the child to play with during the interview.
Sample
The sample included 13 child participants between 5 and 7 years and 15 primary caregiver participants. The researchers originally sought to recruit children age 4 to 7 years, but no 4-year-old children were recruited. Caregivers were mainly parents but also included grandparents or adopted parents. Both child and caregivers were recruited as dyads, but one caregiver wishing to participate alone (whom gave consent) was also independently eligible. This situation was noted once in the course of the study when a child did not assent but a mother still wished to participate. One married mother and father wished to participate but only if they were interviewed together due to time constraints. They were included, and they were interviewed together.
Participant Recruitment and Setting
Child and caregiver participants were recruited from August 2014 to November 2014 using purposive and convenience sampling. Participants were purposefully chosen in this study because each child was in need of an invasive venipuncture procedure ordered by a licensed medical provider. Additionally, participants were conveniently selected from a population of many pediatric patients who were in an outpatient laboratory. Recruitment for this study took place in a freestanding children’s hospital in the Southeastern United States, specifically in the clinical laboratory. Both child and caregiver interviews were held approximately 15 minutes after the procedure to help prevent recall bias and in the same location: a quiet room across from the clinical laboratory in the hospital. Caregiver participants also completed a demographic questionnaire.
Data Collection
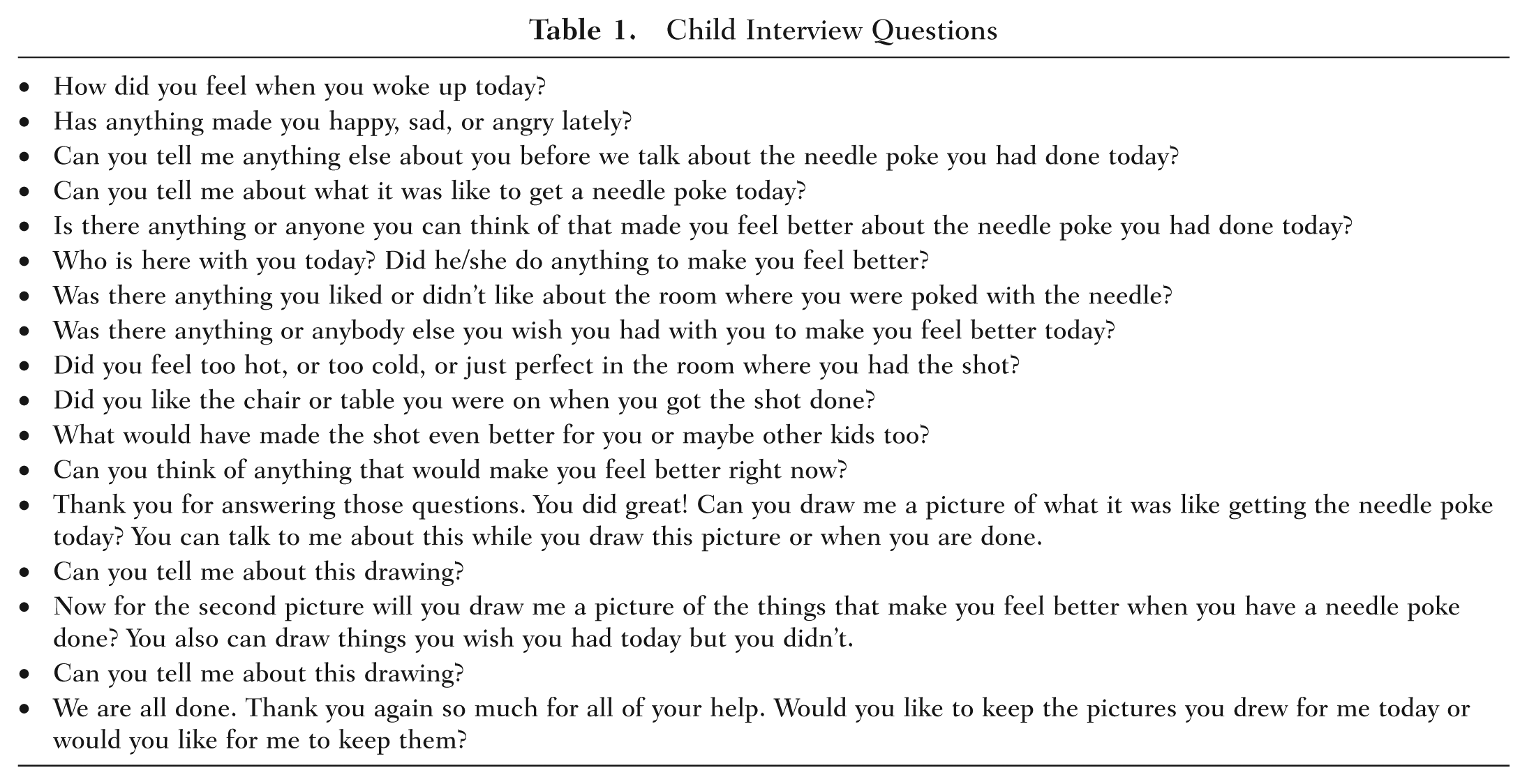
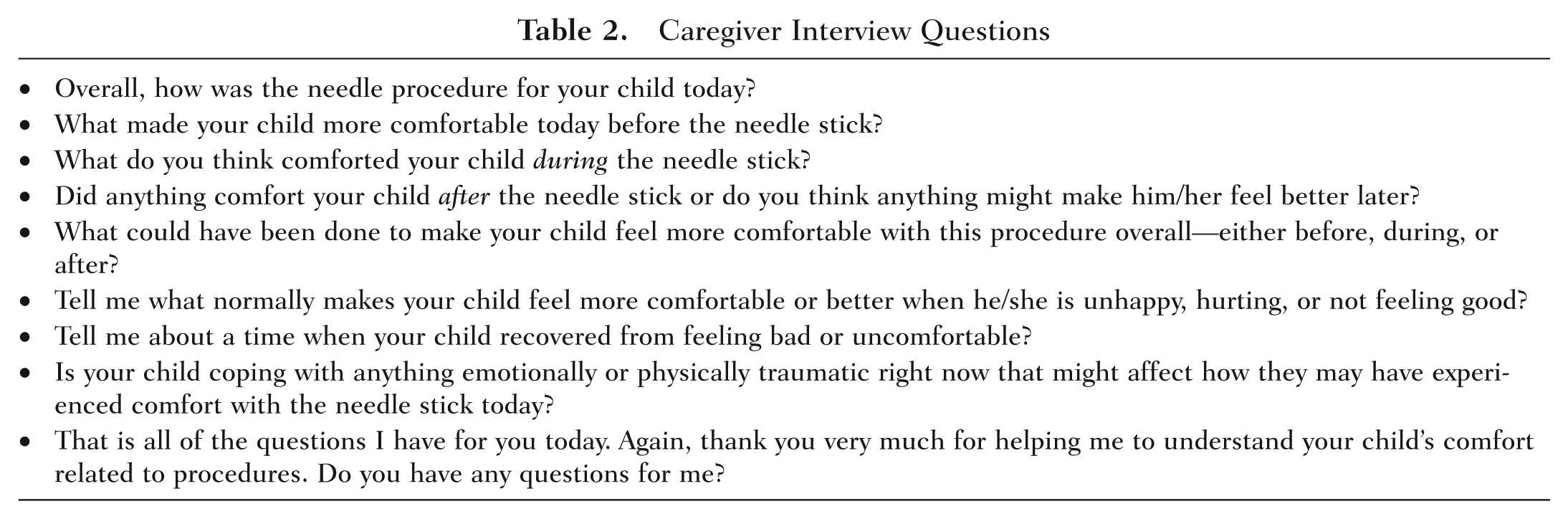
Interview questions with children and caregiver participants were conducted in a semistructured format (see Tables 1 and 2). Questions were focused on actual or missing holistic comfort sources for the child before, during, and after the procedure. An interview protocol was used for both children and caregivers as Creswell (2009, 2013) recommends. Notes were taken during all interviews. Following child and caregiver interviews, a more detailed summary of field notes were also written. These field notes included only pseudonyms for identification and were used in conjunction with transcripts to help elucidate the most rich and accurate descriptions and to note any discrepancies between verbal and nonverbal behavior. Interviews took, on average, 15 to 30 minutes and this included the drawing time.
Child Interview Questions
Caregiver Interview Questions
Data Management
All interview data, including drawings, were transcribed then digitalized into a password-protected computer as soon as possible. No real names appear anywhere except on the original consent and on a roster that matched pseudonyms to the consent. All interviews with both child and caregivers were audio-recorded with a small digital recorder. Transcripts and other pertinent data were also stored in the computer software program NVivo for Mac. This program could not be accessed without the digital access code on the PI’s computer.
Data Analysis
Data analysis began during the process of data collection. With recurring child and caregiver perceptions and a lack of new descriptions, the PI determined that data saturation had been reached. Child and caregiver interviews were initially analyzed separately as two different populations, but child interviews were lined up with caregiver interviews to assess similarities and differences in perception of events. After analysis of data for child and caregiver participants, results from both groups were compared for content. The process of data analysis recommended by Sandelowski (2000, 2010) and the more specific descriptions of conventional content analysis by Hsieh and Shannon (2005) were used. All interviews were transcribed verbatim and each transcript was read and reread line-by-line. As Hsieh and Shannon recommend, the PI started analyzing with no preexisting theory, categories, or codes. Field notes taken were used to capture environmental conditions and nonverbal behaviors—this assisted in data analysis. Codes were created from the existing data and then sorted into categories of meaningful clusters and descriptions. In some cases “in vivo” codes and categories were used. These were generated from like phrases, words, and meanings, which were developed carefully and interpreted into themes.
Maintaining Rigor
Stepped procedures recommended by Guba and Lincoln (1981), Creswell (2013), Sandelowski (1986), and Beck (2009) were employed to enhance trustworthiness and validity in this study. The goal of these steps was to help maintain what the aforementioned researchers call credibility (truth-value), dependability (stability of data over time), and confirmability (objectivity of findings). First, rich descriptions of procedural comfort from both child and caregiver participants were evoked. Additionally, a reflexivity statement was completed to openly recognize and share researcher views and potential biases related to the phenomenon under study. Peer debriefing was also conducted with four individuals familiar with study. A clear audit trail was maintained. Last, external auditing was completed with an experienced researcher who was not affiliated with the study to verify whether the interpretations were supported by the data. Transferability/fittingness is another aspect of trustworthiness and essentially represents the stability of findings for application across contexts. This element of rigor is more difficult to maintain given the population of young children and the specific focus on invasive nursing procedures. However, children in this study were outpatient (like the majority of pediatric patients who receive venipuncture procedures) and they were similar in demographic diversity to the state where the research took place. This increases fittingness of findings. Additionally, some generalized and broad comfort findings may be elicited among children, which would, in fact, be more transferable.
Findings
Demographic Characteristics
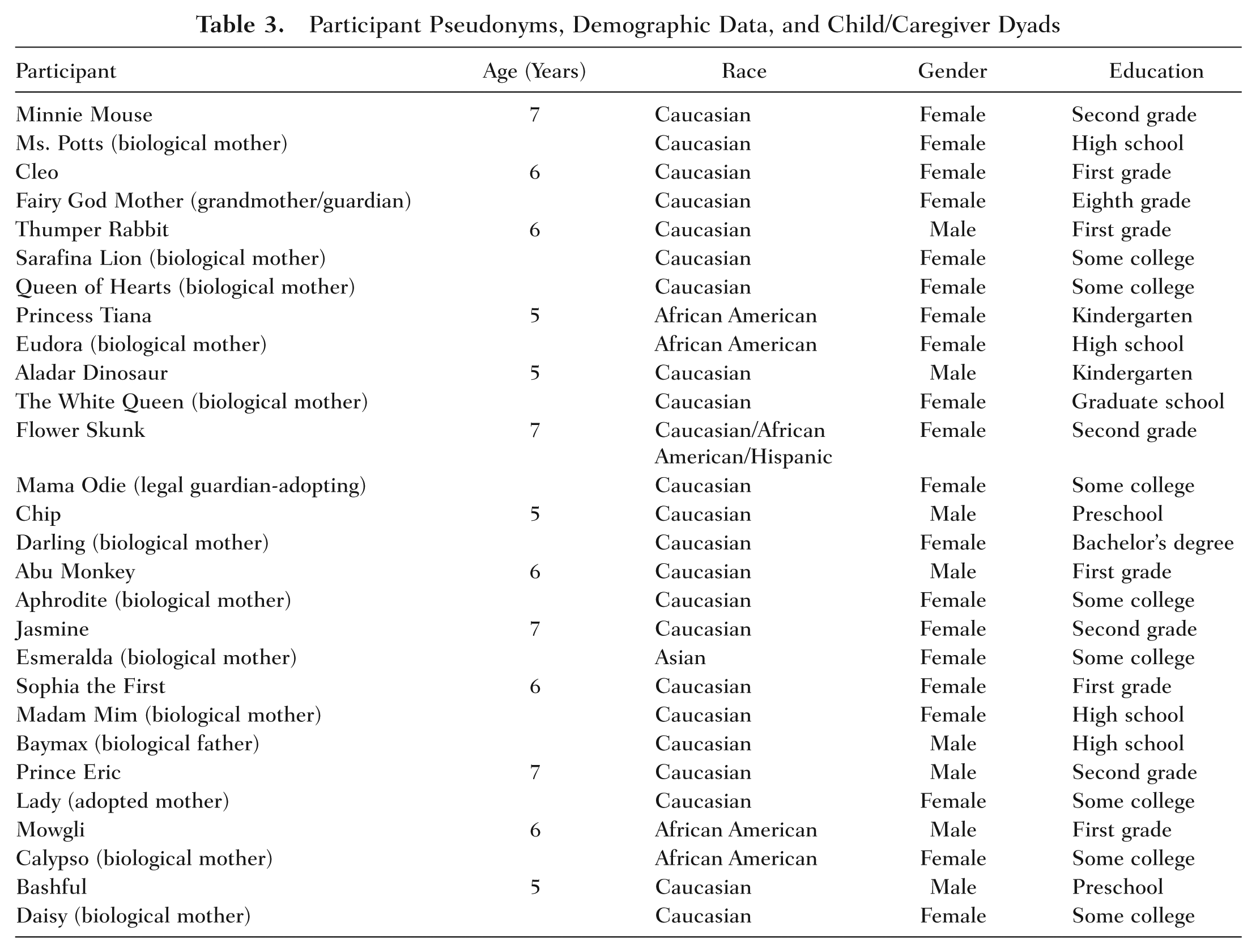
Twenty-eight participants were interviewed in this study: 15 adult caregivers and 13 children. Two of the caregivers who participated were the biological mother and father of the same child participant. One child did not assent to participation and therefore was excluded. A summary of demographic characteristics with each caregiver and their corresponding child is found in Table 3.
Participant Pseudonyms, Demographic Data, and Child/Caregiver Dyads
Holistic Comfort Descriptions
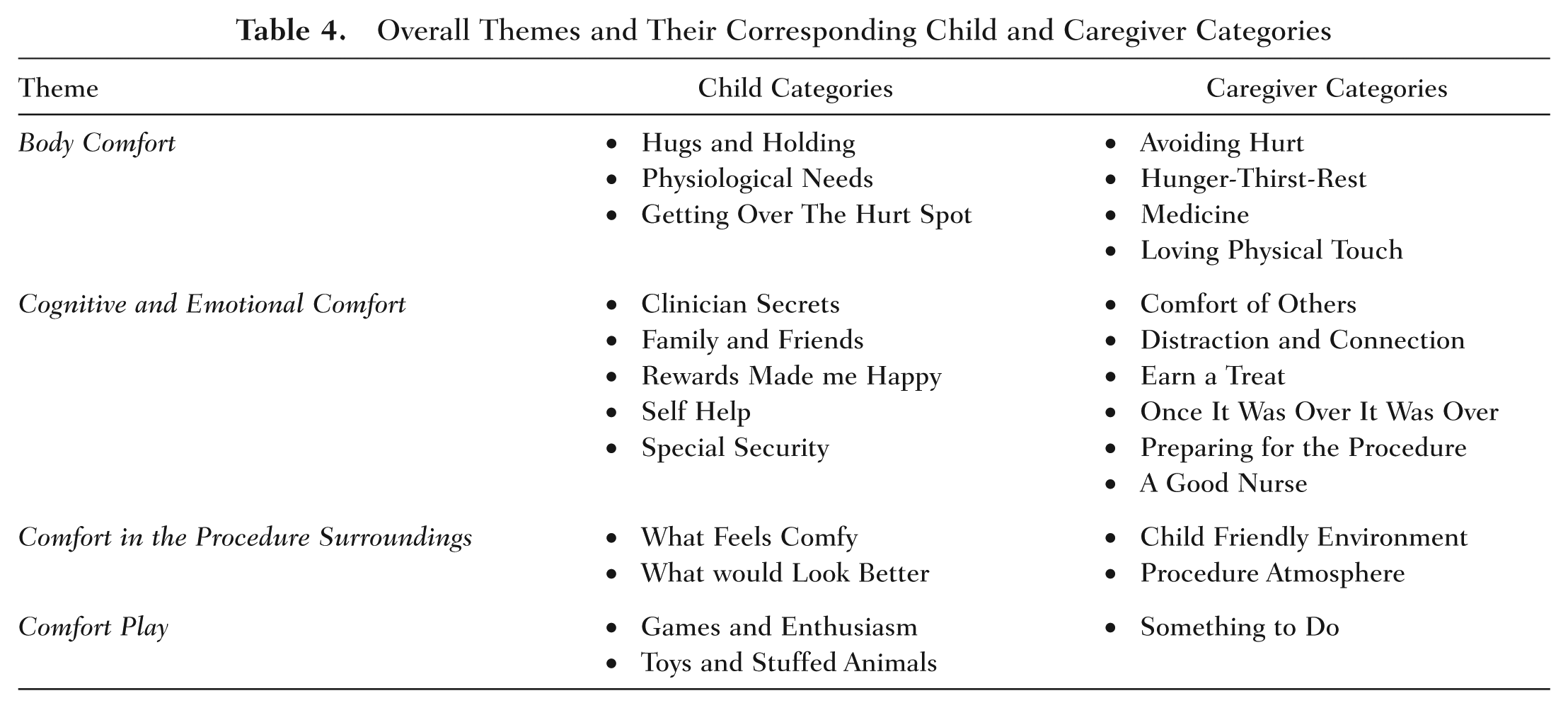
As previously explained, caregivers and children were originally analyzed separately. After this separate analysis, it was evident that comfort descriptions between the two groups were extremely similar, resulting in identical overall holistic comfort themes. There were four overarching themes of holistic comfort related to venipuncture procedures: Body Comfort, Cognitive and Emotional Comfort, Comfort in the Procedure Surroundings, and Comfort Play. Table 4 outlines all the overarching themes and their corresponding categories among child and caregiver descriptions. Many were in vivo categories, in the tradition of staying data-near. The overall themes are presented individually with explanation and supporting references to the data.
Overall Themes and Their Corresponding Child and Caregiver Categories
Body Comfort
The theme body comfort related to the child’s somatic needs involving the venipuncture procedure. Children and caregivers described body comfort as an experience that was desired or necessary related to the human body system, structures or parts of the body, or improvement/satiation in body function or needs, sensation, and feelings. Children and caregivers were detailed in explaining the positive effects of various types of body comfort while additionally describing the negative aspects of missing these desired comforts such as pain or “hurt.”
Being held anywhere on the body, touching, and giving or receiving hugs were sources of body comfort for children. Children experienced this kind of comfort from a primary caregiver, immediate family member, or extended family member. Children and caregivers mentioned this physical touch during the venipuncture procedure or in preparation of the procedure. One child spoke of holding her mother’s hand and one mother described the importance of physical touch for comfort to all of her children.
Yeah. I holded her [mother’s] hand and it didn’t even hurt because I, I was holding still . . . holding my moms hand . . . she was holding onto mine . . . I’m gonna draw my mom holding my hand . . . that made me feel better . . . (Jasmine, 7-year-old female) I mean I think that’s all my children, comforted either sitting in my lap with some, you know something uneasy coming, yeah . . . kisses and holding is usually the path, physical touch. (Darling—Mother)
Another source of body comfort described by children and caregivers was in relation to various physiological body needs. Descriptions and discussion focused on eating or drinking, sleep/being tired, and elimination habits were noted. One child stated his need to use bathroom before his procedure:
I need . . . I need, well when I was waiting in the room, I had to go potty . . . I did go potty before I had the shot. (Aladar Dinosaur, 5-year-old male)
Caregivers also spoke of these physiological needs. One mother described her child’s hunger while NPO (fasting from food and water) for her blood test.
I just discussed with her and told her you know she can’t eat or drink anything. . . . She didn’t really like that. She was complaining all the way down here I’m hungry, I’m hungry. (Fairy God Mother—Mother)
Many children talked about materials used on their body by the clinician when initiating and completing the blood sampling. These materials and supplies were discussed as both positive and negative aspects of the procedure. One child expressed his specific positive feelings about Band-Aids and gauze.
That little wash cloth . . . um they put a Band-Aid over it . . . because the, they [gauze dressing with a Band-Aid] get over the hurt spot. (Aladar Dinosaur, 5-year-old male)
Caregivers additionally described their child’s distressing actions, refusal to cooperate with the procedure, and the comfort of avoiding hurt associated with the procedure. One mother described her daughter’s pain experience that could have been avoided with the venipuncture.
They went from arm to arm and tried to figure which arm to get it out of and then they had to wiggle around the needle a little. Um, that was probably the worst part, the hunting . . . but they just kept, you know going, trying to figure out which arm and then she did have to call um somebody else in there to figure out what’s the minimum (blood) she could get . . . the thing they use on her arm (tourniquet), she did, it started to hurt cause it had to be left on so long. (Ms. Potts—Mother)
Caregivers were the only participants to describe the comforting effects of “medicine.” Only one caregiver participating in the study reported the use of procedural pain prophylaxis with topical analgesia—a standard of care recommended for children by various medical and nursing experts. This analgesic cream was provided by her child’s doctor’s office.
We went by our pediatrician’s office and they gave me the numbing . . . the lotion . . . and I think without that, it would not have been perfect. . . . But I was really really shocked because of the numbing medicine. I mean he sat there and watched it and didn’t flinch. (The White Queen—Mother)
It is clear by the aforementioned descriptions that a child’s body is an important part of procedural holistic comfort. Contrast is certainly noted between (a) the experience of the child requiring a lengthy procedure with increased needle probing and tourniquet use and (b) the child who “sat there and watched” the procedure after given anesthetic cream for the needle stick.
Cognitive and Emotional Comfort
Another overarching theme of procedural holistic comfort described was cognitive and emotional comfort. This theme was found to have the most frequently occurring codes and categories between both participant groups. One type of comfort described was in relation to the clinician performing the procedure. One child associated his clinician’s performance with an even higher level of cognition—helping in finding the source of his “itching” eczema.
Um, a lady with ah um, a Halloween shirt on . . . Um, well she made me better because I didn’t, we didn’t know what, made me like, made me like you know like what it was when I was itching to death. (Chip, 5-year-old male)
Caregivers also described the clinician performing the procedure. Summative descriptions from caregivers regarding a “good nurse” revolved around comfort from clinician demeanor, rapport, skill, and talk. One grandmother shared her perception of clinician personality. Another caregiver, a mother, described the “sweet” comfort of clinicians.
It just wasn’t you know like some one went in there [procedure room] and didn’t say anything and just poked her [child] and went on . . . I think they think some people thinks kids don’t have feelings but I think the personality on the nurses is a . . . it’s good . . . for our kids. (Fairy God Mother—Grandmother/Guardian) The lady was real sweet talking to her . . . you know . . . the sweeter they are, the, that comforts em. (Ms. Potts—Mother)
Children and caregivers also reported people as a source of comfort surrounding the venipuncture procedure. Primary caregivers, immediate family, friends, and extended family were discussed multiple times. In terms of providing comfort, children focused on having a significant interpersonal relationship with the described individual. One child described the comfort of her brother and sister.
I think of my baby sister and it made me feel good . . . my brother but he’s at school . . . because I wished he was with me . . . because he’s my brother. (Cleo, 6-year-old female)
A mother explained the comfort that her sister provides to her daughter in times of need.
She was calling out for my sister. . . . Auntie ah Jackie yeah. She’s, she’s like real, more I guess like calmer. . . . Yeah, that’s her [the child’s] favorite auntie so she [child] was mainly looking out for her [during the procedure]. . . . But, she’s [the child], she’s just like, she’s real sensitive and emotional so that extra type of comfort and love from the ones that she love the most, that’s probably what you know, that would um, help her out, as far as, being comfortable in the room. (Eudora—Mother)
Children and caregivers also described the comforting effects of receiving rewards or treats before or after the venipuncture procedure. One child described, in great detail, how his reward of various stickers received after the procedure made him feel better.
Well after [the procedure], I got some stickers but I got some, hang on, let me clean my back pocket. . . . See I got Monster [Jam], these were the first ones and then I had Crusher what even it was my other one . . . and then these were my 2nd ones right here, Swamp Force [another Monster Jam truck name]. (Thumper Rabbit, 6-year-old male)
One mother described the importance of her son earning a treat after the venipuncture because of his bravery with the procedure.
You know when they’re having to do extra stuff. . . . You want to get enough that you know they feel they’ve earned it and he definitely earned it. He was so brave. You know you earn a treat when you’re brave. (Lady—Mother)
Both children and caregivers described cognitive strategies and thought processes that represented comfort surrounding the procedure. Children described various acts of their own will such as holding “still” leading to the provision of cognitive and emotional comfort. Caregivers frequently described ways children were comforted through distraction away from the procedure. One child described how his “table” could provide him a “hiding” place.
My table . . . ah, I will push it up like this . . . and then nothing . . . where people can’t give me a shot! A whole bunch of table surrounding me . . . and then I’d be hiding. (Mowgli, 6-year-old male)
One mother described her anticipation of what the day would be like and the comforting effects of counting beads as a distraction to her son before the procedure.
I mean walking in, I already knew that he would already tense up knowing that it was a doctor’s atmosphere. . . . With the distraction of this [counting beads], we did pretty good. . . . We honestly were completely distracted by this [working with the beads] . . . all the way up to the moment [the procedure began] so. (Darling—Mother)
Caregivers alone described the cognitive comfort of preparing or not preparing his/her child for the procedure as well as descriptions that explained the importance of his/her child no longer enduring the discomforts associated with the venipuncture. One mother explained the conflict of watching her child in distress but described the relief of seeing him manage well after the venipuncture was over.
As soon as the shots are you know done and administered you know then he’s fine. . . . Oh I think as soon as the needle’s out and once that bandage is on there, wrapped up, he knows he can go . . . yeah cause he’s . . . he knows he gets to go out. (Queen of Hearts—Mother)
Another mother described the comforting effects of providing a more explanative and informative form of preparation.
I tried to explain it to her. You know they’re gonna have to take some blood out . . . you have to try to prepare her for anything new. (Mama Odie—Mother)
Children described cognitive and emotional comfort received through special security. Many children described belongings that provided them a unique kind of emotional comfort. They were communicated and interpreted as being extraordinary and meaningful to the child. One boy, on several occasions, described his stuffed penguin “Poofy” who made him feel “so much” better.
My penguin named Poofy. . . . Yeah look look, and he’s a stuffed animal and he is ah from the Aquarium . . . cause he’s so fluffy. . . . Watch this it’s my best buddy Poofy’s feet [child telling PI to look at his drawing of the stuffed penguin] . . . he always makes me feel better. . . . Next time when I come here I’ll bring Poofy . . . this, my friend right here [Poofy] will make me more than anything feel better. . . . You know why I’m wanting you to have that picture and keeping it [child asks PI]? Cause I want you to remember what Poofy is. (Thumper Rabbit, 6-year-old male)
Another child described the emotional comfort he received during his venipuncture from a blanket that he has had since he was born. The blanket is called his “Bee Bee.” The child was holding and caressing the “Bee Bee” at the time of the quote.
My Bee Bee. . . . Well I use it at night and it’s snuggly. . . . It’s a blanket . . . I can snuggle the hurt spot . . . I can put my Bee Bee over the hurt spot. (Aladar Dinosaur, 5-year-old male)
Well-being through self-help, special security objects, knowing the procedure was over, rewards or “treats,” preparation, distraction, and a “good nurse” were all described as essential aspects of procedural holistic comfort.
Comfort in the Procedure Surroundings
Another overarching theme of this study was comfort in the procedure surroundings. This type of holistic comfort was characterized by elements within the context of the child’s environment. Room temperature was described in detail. Some children also mentioned their views on the size of the procedure room. On numerous occasions children made references to what they would have changed about their environment to make it feel more “comfy.” One child described how a jacket would have made her feel better about the temperature of the room, and a mother also discussed how the room could have been “warmer.”
This whole building [hospital] is cold! . . . Ah, a jacket, like kind of like my moms [would have made me feel better]. Mmm, if I had my mom’s jacket [would make me feel better now]. . . . Cuz it’s still cold even in here. (Minnie Mouse, 7-year-old female) They could have made it warmer. . . . As a matter of fact, it’s kind of cold in here [interview room]. . . . Yeah and you know she has a shirt, she has an undershirt, and a jacket and then she has a coat too. . . . She’s a very cold natured child. (Mama Odie—Mother)
Children and caregivers described the procedure table in various ways. One child described his dislike for the noisy crunching sounds of the paper on the procedure table.
Yeah um, it was, well um it wasn’t comfortable because of that paper on it. . . . Um, well first of all it um, it makes, it does, it’s not um like, it makes uncomfortable and it also and also when it makes that um those noises, it kind of hurts my ears. . . . Um um just like um like a like a soft sheet [would be better]. (Prince Eric, 7-year-old male)
One mother described how a “soft chair” might have been more comfortable to her child instead of a table.
Well she had to sit there for a for a little while since she was, you know, and her legs were danglin off the table . . . better to sit on than the, you know they might be more comfortable instead of just sitting out in the open on a table. I don’t know . . . little kids . . . um, a soft chair [would be better]. . . . I think a kid would feel better in a chair instead of just kind of feeling like they’re vulnerable up sitting on that table. (Ms. Potts—Mother)
Children and caregivers also described the visual aspects of their surroundings—those that were aesthetically pleasing and those that were not. Children talked frequently about color preferences and recalled colors in their surroundings. When one boy was asked what he liked about the exam room floors and walls, he lamented a lack of color, stating there was “nothing.”
There was nothing! . . . white, white, white, white. (Mowgli, 6-year-old male)
Another child described the colors on the floor in the laboratory and what colors he would have preferred while evoking an image of a figure that was captivating to him—a fire fighter/officer.
Nothing was on the floor there . . . only colors . . . I think it was just light blue and dark blue and all kinds of blue. [I Would have liked to see] red and orange and in yellow because I, I really like fire . . . like fi, like a fire cop! (Chip, 5-year-old male)
Caregivers described a “child-friendly environment” that a child would relate to or identify with.
One mother described the lack of décor in the procedure room and compared this to her child’s doctor’s office.
Our pediatrician’s . . . office is awesome. Every room is decorated . . . and it’s really great cause they [child patients] look at the . . . count the pigs on the wall . . . but that’s . . . it helps the child feel more secure in an area. . . . The white walls I think are probably not soothing. (The White Queen—Mother)
Descriptions of decorations (or lack thereof) in the exam room, waiting room, and laboratory were common. Also, commonly discussed were the aspects of the procedure experience that would feel more comfortable to the child such as room temperature, positioning, and the procedure table. It is clear that a child’s surrounding affects procedural holistic comfort.
Comfort Play
Comfort play is the final overarching theme. Comfort from “play,” with the objects described in this study, is related to recreation and hobbies that a child would likely enjoy. Children were far more detailed, specific, and varied in their descriptions of “play” in the procedure scenario than were the caregivers. This theme included descriptions of various activities and sources of amusement that could be used before, during, or after the venipuncture procedure. At times boys and girls seemed enthusiastic about different sources of play. Some boys mentioned things such as “brachiosaurus” or “Michael Jordan” while some of the girls described a “princess.” One child described his phone as a source of comfort play.
My phone . . . Ah, cause I like to play games on it. . . . I have angry birds and mind craft and stuff. (Mowgli, 6 year-old male)
Additionally, several caregivers described the comforting effects of passive television watching. One legal guardian described the beneficial effects of television.
Well, if they had given her a TV and turned it on, she’d had zoned out, probably wouldn’t even felt the stick [needle insertion]. (Mama Odie—Mother)
Children and caregivers also described comfort associated with novelty toys, action figure toys, and stuffed animals. Many children talked about enjoying the toys that were left for them to play with (provided by the PI) on the carpet tile during the interview. One boy described a stuffed toy at home similar to the action figure on the carpet tile in the interview room.
Um, um my Ninja Turtle. . . . I do have a stuffed animal Ninja Turtle. He’s Michelangelo crawling like this [Child picks up the ninja turtle action figure and gestures him crawling]. . . . And it has a button right here (child points to the back of the ninja turtle toy) and it, and it, and it lights up . . . at the, in the dark. (Bashful, 5-year old male)
When asked about things that may have been helpful or comforting in the laboratory or procedure room, one mother described how she recalls no activities her son would have enjoyed.
I don’t even remember if there was any toys or anything . . . in there . . . where we went and got the um, where you got the blood at [laboratory]. . . . No, there wasn’t anything in there . . . anything in there for him to do. (Calypso—Mother)
Many children and caregivers mentioned stuffed animals as a comfort source during and after the venipuncture procedure. Among these descriptions included children wishing for a stuffed animal they had not brought with them. One child described staff giving him a squeaking stuffed cat after the procedure and how he wished he had it during his venipuncture.
I wish I would have that with me when I was in my room today [Child points to stuffed animal in his mother’s arms and takes it from her hands]. . . . It’s a kitty who’ll squeak, squeak. (Bashful, 5-year-old male)
Children and caregivers expressed multiple realities of procedural holistic comfort within the context of their own life circumstances and personal values. The researcher and participants were directly influenced by one another on the basis of these shared realities. Children and caregivers described procedural holistic comfort as comfort to the body, comfort through cognition and emotions, comfort in surroundings, and comfort from play. Discoveries of pediatric holistic comfort related to a venipuncture procedure provides new evidence, leads to the support and question of existing evidence, and spearheads the implementation of various interventions to improve pediatric procedural care.
Discussion
Findings from this study support discoveries of previous investigators. Other findings seem to contradict the appropriateness of some comfort interventions that have been previously researched. This study additionally brings about new findings not yet reported in the literature and it expands on some of the already examined comfort measures.
Findings Related to Preceding Literature
In a very recent systematic review, Bice and Wyatt (2016) found procedural comfort interventions included music therapy, amusement and entertainment, caregiver facilitation, and a multifaceted approach—including mixed nonpharmacological and pharmacological interventions. Neither children nor caregivers described music therapy, music listening, or music intervention as a source of comfort related to venipuncture procedures in this study. This could be because no music was offered or playing at the time of the venipuncture procedure. Children and caregivers in this study did describe sources of amusement and entertainment for comfort. These sources included novelty toys, stuffed animals, screen time, games, and activities. As in this study, similar findings of coping with procedural fear and pain through the use of inanimate objects, moral support, and trusting clinicians was found by Hodgins and Lander (1997).
As shown by Bice and Wyatt (2016), numerous descriptions of caregiver presence, physical touch, hugs and holding, encouragement, and talk were described as sources of body comfort and cognitive or emotional comfort by caregivers and children. Carnevale and Guadreault (2013) found children who were hospitalized used food as a source of comfort as did participants in this study. Descriptions of nonpharmacological and pharmacological interventions for comfort were also interpreted in this study as recommended by Czarnecki et al. (2011). In this study, holistic comfort was described similar to definitions presented by the American Holistic Nurses Association (2016), Freeman (2005), and Tjale and Bruce (2007): representing the whole person and incorporating numerous remedies for the mind–body–spirit.
The qualitative evidence from this study provides new documented insights on procedural holistic comfort management for children age 5 to 7 years. This is the first study to investigate qualitative procedural holistic comfort evidence through descriptions of children and their caregivers. Findings from this study help bridge the gap of an unrecognized understanding of comfort from a holistic perspective related to invasive pediatric procedures including the body, emotions, cognition, surroundings, and play.
Implications
The implications from this qualitative study are multidimensional and include possibilities for innovation in procedural practice, organizational and administrative policy, nursing practice, and methodology. Many of these improvements and/or new developments can be implemented in various health care locations, in a timely manner, with low cost, ease of administration, and minimal duty burden to health care staff. Procedural implications include using topical analgesics for procedures, acknowledging child color preferences, offering food or drink to children, and using caregivers during the procedure. Next, offering warm blankets, giving stuffed animals to children prior to procedures (instead of after), and providing child-friendly décor and/or entertainment are all organizational implications. The main practice implication noted in this study revolves around early communication with clinicians: on referral for a procedure, caregivers should be informed to bring special objects and family members or friends who provide their child the most comfort. Last, methodology implications were noted: children as young as 5 years were successfully interviewed and were provided an opportunity to draw pictures. This can be replicated for studies in the future, and providing toys for the interview proved engaging not only for participants but also for siblings who accompanied caregivers but were not interviewed.
Future Research
Several areas for future research are still noted after conducting this study. More research addressing procedural holistic comfort with other invasive procedures including, but not limited to, urinary catheterizations, nasogastric tube insertions, port-a-cath central line access, IV cannulation, lumbar punctures, wound dressing changes, suture placement, and suture removal, is needed. In order to conduct intervention studies with children who experience invasive procedures a tool must be developed so outcomes research can be initiated. Narratives exploring the experiences of caregivers who witness invasive pediatric clinical procedures and children who experience frequent invasive procedures is also needed. Holistic comfort needs exist in many areas of a child health, across various age groups such as infants, toddlers, school-age children, and adolescents, and in various cultural groups, races, and ethnicities. Research focused on disparate groups and pediatric procedural holistic comfort outcomes is absent from the literature. Comfort connected to other areas of child experiences with health and health care also needs exploring. This includes ancillary or radiology testing such as magnetic resonance imaging, computed tomography, simple radiographs, electroencephalograms, polysomnography (sleep study), treadmill electrocardiograms, and nuclear medicine studies. Holistic comfort research is also needed for children with illnesses that require invasive procedures over many months, even years, such as cancer, cystic fibrosis, HIV, chronic kidney disease, diseases causing neurological impairment, congenital heart disease, trisomy 21, diabetes, juvenile rheumatoid arthritis, asthma, musculoskeletal disease, autism spectrum disorders, obesity, depression, and attention-deficit hyperactivity disorder. Additionally, the holistic comfort needs at the end-of-life is a significant area of research indicated for children to have a more peaceful death.
Study Limitations
Interpretation was used in the thematic content analysis process, which could have affected participant “pure descriptions.” Stabilization of this limitation was aimed for in the implementation of peer debriefing and the use of an external researcher audit. Another limitation in this study is the unknown transferability across different populations and different age groups. However, according to the U.S. Census Bureau, in 2013 the diversity of the state where the study took place is fairly similar to the demographics of the child and caregiver participants in this study. Additionally, varied child backgrounds could have affected descriptions of procedural holistic comfort in this study. The use of a single institution for recruitment restricts findings to those participants coming to one hospital in one city of a much larger region. Next, the VISA gift card and child toy basket offered for participation may have over-influenced willingness to participate. This is why a reasonable amount of $20 and nonextravagant toys were chosen as gifts for study involvement. Finally, the PI is a certified pediatric nurse practitioner who has previously performed many invasive procedures on children. For this reason, a reflexivity statement was completed prior to conducting the study so to separate the PI’s opinions, attitudes, and beliefs. Again, peer debriefing and external audit was also implemented in order to further support the interpretation of findings from this study.
Conclusion
Invasive pediatric clinical procedures are an unavoidable part of health care for many children. The negative aspects however related to these invasive procedures can be reduced or avoided through providing various comfort interventions. Many of these comfort interventions such as forms of entertainment, music therapy, caregiver facilitation, and a multifaceted approach to decreasing pain, distress, anxiety, and fear have been studied. Research in the area of holistic comfort related to invasive procedures in children was missing. Although comfort has been rigorously studied in the adult population, the definition and meaning of pediatric procedural comfort has been defined more by the absence of pain as opposed to a broader perspective focusing on the whole child. The significance of holism is unquestionable when nurses and other clinicians care for children. Findings from this study suggest that the process of experiencing an invasive clinical/nursing procedure introduces more comfort needs than relief from fear, pain, distress, and anxiety. Children and caregivers described holistic procedural comfort as including body comfort, cognitive and emotional comfort, comfort in the procedure surroundings, and comfort play. Findings from this study have implications in the areas of procedural practice, organizational policy and procedures, nursing practice, and methodology. There are however questions about pediatric holistic comfort that remain unanswered. With the findings from this study and future outcomes research, there is potential for enhancement of overall procedural holistic comfort in children. Adequate nurse and clinician-provided procedural comfort management is the right of every child. With this new knowledge and further research on holistic comfort, clinicians can avoid becoming metaphorically and mentally anesthetized, which has, in the past, rendered the problem of suffering during invasive pediatric procedures more difficult to manage. Most significantly, as a result of this study, beginning evidence exists with regard to care that focuses on ending associated anguish and enhancing holistic comfort related to invasive pediatric clinical procedures.
Footnotes
Acknowledgements
The authors would like to thank and acknowledge Sigma Theta Tau International for receipt of the 2013 Virginia Henderson Clinical Research Grant, without which this study could not have been completed.