
Abstract
Though various authors have refined and described the concept of compassion fatigue (CF), the overarching features, predisposing factors, and potential consequences remain relatively consistent. Available literature demonstrates that caregivers caring for patients who are chronically ill and/or traumatized are at highest risk for developing CF. Potential consequences for unmitigated CF include physical, emotional, and work-related consequences, all of which can have negative effects on the quality and safety of care and degree of engagement with one’s employer. CF is further exacerbated by exposure to cumulative, unresolved stress and neglect of one’s own emotional needs over time. Caregivers must be knowledgeable on CF’s risk factors, symptoms, and management strategies to decrease its incidence and negative impacts. This article details the creation, execution, and evaluation of an evidence-based practice change project implemented with the goal of increasing knowledge needed to prevent, identify, and alleviate CF in high-risk nurses. The project involved a series of educational workshops containing information on CF’s risk factors, symptoms, and consequences, with a strong emphasis on self-awareness, self-care, and stress management. Pre- and postknowledge tests showed a significant increase in knowledge was achieved via the workshops, and qualitative surveys indicated a high level of participant satisfaction with the program contents, format, and impact.
Keywords
Introduction
The term compassion fatigue encompasses the emotional, physical, and work-related effects of expending one’s energy in providing compassionate, empathic care to others over any length of time (Worley, 2005). After prolonged exposure to traumatic experiences of patients, “caregivers begin to integrate the emotions, fears, and grief of their patients, ultimately increasing their own stress and emotional pain” (Bush, 2009, p. 25). The term burnout has been used across multiple disciplines and described in various manners throughout the literature, though there is no single, universally accepted definition. For the purposes of this article, burnout will be defined as “a prolonged response to chronic emotional and interpersonal stressors on the job” (Maslach, Schaufeli, & Leiter, 2001, p. 397). The phenomenon of compassion fatigue was originally identified within the literature by Joinson (1992) as a form of burnout, and later described by Stamm (1999) as “the natural, predictable, treatable, and preventable unwanted consequence of working with suffering people” (p. 18). The purpose of this article is to review the creation and implementation of an Evidence-Based Change Project completed in the spring of 2014 at a large public hospital in New England.
Though various authors have refined and described the concept of compassion fatigue, the overarching features, predisposing factors, and potential consequences remain relatively consistent. The term was defined initially in nonnursing disciplines and has only recently been explored within the nursing literature. Regardless of specialty or discipline, caregivers who care for those with chronic illness and their families have been shown to be at highest risk for experiencing compassion fatigue (Figley, 2002; Maytum, Heiman, & Garwick, 2004; Yoder, 2010). Those caregivers who work with traumatized patients have also been identified as high risk for compassion fatigue (Boyle, 2011; Lombardo & Eyre, 2011; Stewart, 2009), though the two are interrelated as some form of previous traumatization is inherent in individuals and families struggling with chronic illnesses. Based on the experiences of this project manager, and in line with the above-mentioned notion that compassion fatigue is related to providing empathic and compassionate care over time, nurses who care for chronically mentally ill patients (many of whom are often traumatized) may also be particularly at risk for the onset and consequences of compassion fatigue, as empathic emotional support is one of the primary nursing interventions used in caring for this patient population (Bush, 2009; Stamm, 1999; Worley, 2005).
Compassion fatigue can have negative consequences in multiple aspects of a caregiver’s professional and personal life. These consequences categorically include physical consequences, emotional consequences, and work-related consequences, all of which can have negative effects on the quality of patient care, patient safety, and level of engagement with one’s employer (Coetzee & Klopper, 2010; Jenkins & Warren, 2012). Physically, compassion fatigue can present as an increase in somatic complaints, including (but not limited to) headache, sleep disturbances (one of the first signs of compassion fatigue), concentration problems, fatigue, and muscle tension, all of which can contribute to missed work days, increased accident proneness and errors, and decreased performance and/or endurance for job-related activities (Coetzee & Klopper, 2010; Jenkins & Warren, 2012; Lombardo & Eyre, 2011). Emotionally, consequences of compassion fatigue may include anxiety, depression, losing the ability to remain objective, mood lability, resentment, anger, and poor judgment. Excessive complaining, emotional outbursts, and tendency to place blame on others are some of the hallmark emotional manifestations of those suffering from compassion fatigue (Smith, 2009). Each of these has the potential to negatively impact not only the quality of patient care but also the employee–employer relationship (Coetzee & Klopper, 2010; Jenkins & Warren, 2012).
Job satisfaction can be negatively affected in individuals suffering from compassion fatigue, given that these individuals often “feel as though they have failed at their profession” (Stevens-Guille, 2003, p. 18). Other work-related consequences include reduced compassion and empathy for patients and families or avoidance or dread in working with a particular patient population (Lombardo & Eyre, 2011). These phenomena, among several others, can contribute to decreased employee retention (i.e., increased turnover), decreased productivity, increased work-related errors, and decreased employee engagement—all of which can contribute to significant, yet avoidable, costs for an organization.
A multiyear analysis of over 3 million U.S. employees concluded that employee disengagement can cost the U.S. economy as much as 350 billion dollars per year (Sanford & Coffman, 2002). “Employee engagement consistently affects key performance outcomes, regardless of the organization, industry, or country” (Gallup, 2013, p. 2). Increased organizational costs related to disengaged employees include (but are not limited to) increased use of sick days, decreased productivity, and decreased staff retention (Coffman, Gonzalez-Molina, & Gopal, 2002). Several studies, including large-scale meta-analyses from a variety of disciplines, demonstrate that employers who have employees who are engaged have significantly better profitability, patient and/or consumer satisfaction, and employee retention than those who do not (Coffman et al., 2002; Gallup, 2013). In one particular large-scale study, engaged employees scored 37% higher on measures of overall well-being than disengaged employees. In fact, engagement was found to be a significantly stronger predictor of overall well-being than number of hours worked, amount of personal or “flex” time available for use, and even amount of vacation time taken (Harter & Agrawal, 2012). Results from the 2011 annual employee engagement survey at one of Connecticut’s largest hospitals showed some of the poorest employee–employer engagement existed among inpatient staff from pediatric oncology and pediatric psychiatry.
Given the aforementioned evidence-based risk factors for its development, compassion fatigue among employees was assumed to have likely been contributing to these low scores in some manner(s). Exhaustion, the most thoroughly analyzed and frequently reported component of burnout, may also be a contributing factor to the low engagement scores, based on the notion that “exhaustion is not something that is simply experienced—rather, it prompts actions to distance oneself emotionally and cognitively from one’s work, presumably as a way to cope with the work overload” (Maslach et al., 2001, p. 403; see also Maslach & Leiter, 2008). Bush’s (2009) findings demonstrated that compassion fatigue is exacerbated by exposure to cumulative, unresolved stress and a neglect of one’s own emotional needs over time. Given the myriad potential costs—both financial and safety/quality based—to an organization that have consistently been associated with poor employee engagement, it is in an organization’s best interest to provide assistance to its employees geared toward reducing stress and improving employer–employee engagement. At the time of inquiry, there did not exist a means within the state’s largest teaching hospital system to aid and educate nurses in the identification and/or prevention of compassion fatigue nor were there any available interventions or trainings available for those who were affected by it.
Review of the Literature
The phenomenon of compassion fatigue, a form of burnout, has far-reaching emotional, physical, and employment-related consequences across multiple domains of a caretaker’s life. Each of these consequences has the potential to negatively affect the quality and safety of patient care, physical and emotional health of a caregiver (with subsequent costs to the employer), job satisfaction, and level of employee–employer engagement (Akkus, Karacan, Goker, & Aksu, 2010; Anderson, 2000; Lombardo & Eyre, 2011; Stevens-Guille, 2003). A comprehensive literature review was completed to find evidence-based interventions for preventing and alleviating compassion fatigue in nurses in order to guide this evidence-based change project (EBCP). This section details the methodology and findings of this systematic literature review.
A thorough review of available literature was completed by the project manager using multiple databases, including PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Clinicaltrials.gov, Medical Subject Headings (MeSH), Cochrane Database of Systematic Reviews, Google, and Ovid. Key search terms included compassion fatigue, burnout, nursing self-care, compassion fatigue rating scale, employee engagement, employee disengagement, and ProQOL. Search filters used were English language, published within the past 10 years, and nursing (where applicable, such as in CINAHL). The search was then opened up to all years as well as removing the “nursing” filter, so as to gather additional, generalized data for the purpose of defining the concept of compassion fatigue and its remedies. A Google search using the full term compassion fatigue was also completed for additional resources.
The review of literature highlighted several studies that demonstrate that many of the components of compassion fatigue including (but not limited to) emotional exhaustion, stress, burnout, anxiety, fatigue, somatic complaints, and job disengagement can be prevented and/or combated through stress-reduction, self-awareness, and self-care (Edmonds, Lockwood, Bezjak, & Nyhof-Young, 2012; Marine, Ruotsalainen, Serra, & Verbeek, 2006; Radley & Figley, 2007). Current literature provides rationale for emotional exhaustion to be one of the primary symptoms targeted by a compassion fatigue prevention intervention (Craig & Sprang, 2010; Edmonds et al., 2012; Gunusen & Ustun, 2010; Kravits, McAllister-Black, Grant, & Kirk, 2010). Self-awareness and stress reduction should also be target objectives of any compassion fatigue intervention, given Bush’s (2009) findings that the compassion fatigue is exacerbated by exposure to cumulative, unresolved stress and a neglect of one’s own emotional needs over time. Additionally, those experiencing personal stress outside of work have been shown to be at higher risk for the development of compassion fatigue (Meadors & Lamson, 2008). Several studies highlight stress-reducing activities that promote emotional release and relaxation as having positive effects on preventing and alleviating compassion fatigue and its related sequelae (Edmonds et al., 2012; Goodman & Schorling, 2012; Gunusen & Ustun, 2010; Kravits et al., 2010; Lemaire & Wallace, 2010; Marine et al., 2006; Radley & Figley, 2007). Stress reduction will also help combat nurse burnout, which, if left unmitigated, can indirectly increase the risk for development of compassion fatigue (Figley, 1995).
Identification of compassion fatigue and burnout symptoms has been reported to be helpful in promoting caregiver awareness and reflection as well as in highlighting the need for interventions to prevent or alleviate these symptoms and their negative effects on work performance and emotional and physical health (Hooper, Craig, Janvrin, Wetsel, & Reimels, 2010; Maytum et al., 2004; Meadors & Lamson, 2008). “The first step in preventing or ameliorating compassion fatigue is to recognize the signs and symptoms of its emergence” (Bride, Radey, & Figley, 2007, p. 155). Mindfulness as a form of self-awareness and reflection has been demonstrated to be helpful in reducing stress levels and identifying the need for such preventative and alleviating activities (Cohen-Katz, Wiley, Capuano, Baker, Deitrick, et al., 2005; Cohen-Katz, Wiley, Capuano, Baker, Kimmel, et al., 2005; Cohen-Katz, Wiley, Capuano, Baker, & Shapiro, 2004; Goodman & Schorling, 2012; Vilardaga et al., 2011).
Based on Figley’s (1995) research, “Compassion fatigue can be manifested in the physiological, psychological, spiritual, and emotional issues that people who have posttraumatic stress disorder also experience” (as cited in Bourassa, 2012, p. 1700). Though the compassion-fatigued caregiver is not directly experiencing a primary traumatic event, he or she is constantly being exposed to the trauma and stress of others in his or her caregiver role, thereby experiencing what some call secondary traumatic stress. Mind–body techniques including (but not limited to) meditation, imagery, movement, and other forms of self-care have been shown to have significant beneficial effects on symptoms of posttraumatic stress disorder (Gordon, Staples, Blyta, & Bytyqi, 2004; Gordon, Staples, Blyta, Bytyqi, & Wilson, 2008; Staples & Gordon, 2005).
Health care professionals have reportedly responded positively to group educational activities that teach self-care, self-awareness, and mind–body skills (Cohen-Katz et al., 2004; Cohen-Katz, Wiley, Capuano, Baker, Deitrick, et al., 2005; Edmonds et al., 2012; Kravits et al., 2010; Staples & Gordon, 2005). A systematic review completed by Edwards and Burnard in 2003 indicated that “relaxation techniques, training in behavioral techniques, stress management workshops, and training in therapeutic skills were effective stress management techniques for mental health nurses” (p. 169). Results of a study at a large children’s hospital demonstrated statistically significant improvement in emotional exhaustion in nurses who completed a 4-hour stress management workshop versus those who did not (Meadors & Lamson, 2008).
In summary, the phenomenon of compassion fatigue has far-reaching consequences across multiple domains of a caretaker’s life, many of which directly or indirectly affect his or her work performance, engagement with his or her employer, and ability to continue providing the empathy required within their patient care roles. Though there is not an overabundance of research on the subject of compassion fatigue and its remedies and/or preventability, much of the literature thus far has shown that self-care—including (but not limited to) stress reduction, self-awareness, and mindfulness—may be an effective intervention in reducing the emotional exhaustion inherent in those who provide care for traumatized individuals and their families. The results of this comprehensive, integrative literature review provided strong rationale for an EBCP to be implemented at one of the state’s largest hospital settings in the spring of 2014. The project—a series of educational workshops with the goal of preventing and reducing compassion fatigue related symptoms in high-risk nurses—was determined to likely be an appropriate and effective intervention, given that “educational sessions can enhance the capacity of human service professionals to cope with the demands of their jobs” (Maslach et al., 2001, p. 419).
Purpose of Project
The purpose of this evidence-based change project was to increase awareness of risk factors, causes of, and symptoms of compassion fatigue so as empower nurses to be able to identify and prevent its onset. An additional goal of the project was to provide nurses with demonstrations and recommendations of self-care activities that may have been beneficial to them in preventing and/or counteracting the effects of compassion fatigue. These objectives were accomplished via an educational workshop for nurses that will be held at the host hospital on multiple dates and times throughout the spring of 2014. Nurses received education on the syndrome of compassion fatigue itself (including risk factors, causes, and preventative strategies); learned to self-administer and score the Professional Quality of Life (ProQOL) Scale in order to monitor their symptoms of compassion fatigue over time; and received suggestions, recommendations, and interactive demonstrations of self-care activities and stress management techniques that may have been helpful to them in preventing, identifying, and remedying symptoms of compassion fatigue in the future. A long-term, indirect goal of preventing and/or reducing compassion fatigue among these nurses is to increase the quality and safety of patient care, improve job satisfaction and nurse retention rates, and lower compassion-fatigue related costs to the hospital.
Project Design and Description
The evidence-based change project was implemented within a large urban hospital setting in New England. The hospital allows for room reservations at several of its campus buildings that can be booked several months in advance. The 1-hour workshops were scheduled around mealtimes to incorporate nurses’ 30-minute meal break into their attendance, so as to minimize potential effects on patient care.
The participants who were notified about and participated in the workshop were nurses, age 18 and older, and actively employed by the hospital in either the Department(s) of Psychiatry and/or Pediatrics, including the Psychiatric and Emergency Department(s). In order to implement this project, a detailed e-mail was sent to all nurse managers of the above-mentioned hospital units at least 2 months in advance in order to notify them of the purpose of the workshop, gauge their interest in supporting staff members to be able to participate in the workshop, and allow for adequate time for any preparations they may need to make to allow staff to leave the units to attend the workshops. Patient Service Managers were then be asked to forward an e-mail announcement of the workshops, created by the project manager, to all their nurses along with a customized message from the PSM that indicated whether or not the workshop could be scheduled by the nurses as part of their regular work shift and how they could go about signing up starting in January 2014 if interested.
The 1-hour educational workshop was offered multiple times during the first 8 weeks of 2014 to allow for as much staff participation as possible. It was offered at various times throughout the day (almost all of which were scheduled around mealtimes as meal was provided) to accommodate nurses who work the four most common shifts at the hospital. Groups were limited to 10 participants to allow for a personalized and intimate experience and to increase the number of feasible locations based on capacity.
The project manager facilitated the workshop. It began with a breathing exercise to promote relaxation and centering of participants. There was then a brief introduction of the project manager, the purpose of the project, and a brief description of the agenda. The participants were then given the ProQOL Scale along with instructions on completing the scale with adequate time allowed for to do so. After this they were taught to self-score the scale and had some time for discussion and for sharing of results, purely voluntarily. Educational information on compassion fatigue was then shared and elaborated on with all participants, in an interactive discussion format, led by the project manager.
The remainder of the workshop was dedicated to the project manager demonstrating and discussing various self-care and stress management activities and techniques in order to promote prevention and management of compassion fatigue. These involved breathing exercises, discussion and demonstration of passive and active meditation methods, and several other stress-relieving activities, as well as suggestions for individualizing self-care techniques based on one’s preferences and lifestyle. This discussion highlighted the importance of not only self-care activities that could be done on one’s own time in his or her home or community but also those that could be completed while actively working his or her job(s) as a registered nurse. Examples of the latter were described and/or demonstrated to participants, including breathing techniques, using or smelling essential oils (in the break room), taking breaks outside of the unit for meals or walking meditations, and using certain herbs and teas that promote relaxation. Participants were also led through a meditative exercise involving listening to one’s own heartbeat with a stethoscope—something that can be done for a few seconds or minutes throughout one’s busy day to re-center, relax, and recharge. Participants were then given a healthy meal that they were free to enjoy while filling out the requested forms. The workshop ended with the same breathing exercise with which it began.
Project Evaluation
Measurement Tools
Data were collected using both qualitative and quantitative means.
Quantitative Indicators
On arrival to the educational workshop, participants were given a demographic questionnaire as well as a (separate) 12-question knowledge test on compassion fatigue that they were requested to immediately complete. The same knowledge tests (identical contents to pretest, though labeled posttest) were given immediately after the intervention, to obtain scores for comparison to evaluate the effectiveness of the educational intervention. Prior to the workshop, pretests were coded with sequential alphabet letters, which the participants were then asked to transcribe onto their posttests after completion, to allow for pairing of the results of pre- and posttests for each individual participant for future analysis by the project manager. The demographic surveys were collected separately and were not paired or linked with knowledge tests in any way to preserve anonymity. The quantitative knowledge test contained the following questions.
Compassion Fatigue Knowledge Test
Please circle what you believe to be the correct answer for each of the following 12 questions:
Compassion Fatigue is a. A set of symptoms b. A disease c. A disability d. All of the above
Compassion Fatigue has been described as a. A posttraumatic stress disorder b. A secondary traumatic stress disorder c. An acute stress disorder d. All of the above
Organizational symptoms of Compassion Fatigue include a. High turnover rates b. Increased worker’s compensation claims c. Chronic absenteeism d. All of the above
Caregivers who are volunteering (unpaid) are more at risk for Compassion Fatigue than caregivers who are paid for their work. a. True b. False
Symptoms of stress manifested in sufferers of Compassion Fatigue are chronic in nature. a. True b. False
In a Compassion Fatigue sufferer, a constant need to express excessive complaints verbally stems from a. A high level of frustration b. A lack of awareness as to the origin of one’s symptoms c. The chronic experience of one’s symptoms d. All of the above
An evidence-based risk factor for developing Compassion Fatigue is a. Working shifts greater than 8 hours b. Working without pay (volunteering) c. Caring for chronically ill persons d. Job dissatisfaction
The natural consequences of stress resulting from caring for and helping traumatized or suffering people or animals is a. Posttraumatic stress disorder b. Burnout c. Compassion Fatigue d. None of the above
A psychological term for the experience of long-term exhaustion and diminished interest, especially in one’s career, is a. Burnout b. Compassion Fatigue c. Posttraumatic stress disorder d. Secondary traumatic stress disorder
One of the first signs of Compassion Fatigue is often decreased a. Appetite b. Restful sleep c. Personal boundaries d. Concentration
_________ is “too much”—that is, too much work, too much pressure, too many expectations; whereas _________ is “not enough”—feelings of depletion, emptiness, apathy, lack of motivation. a. Burnout, stress b. Stress, burnout c. Compassion Fatigue, burnout d. Stress, compassion fatigue
_________ is a form of _____________. a. Compassion Fatigue, burnout b. Burnout, Compassion Fatigue c. Burnout, secondary traumatic stress disorder d. Secondary traumatic stress disorder, burnout
Qualitative Indicator
At the end of the workshop, the participants were given a data collection worksheet that they were told they could use to record their self-care and stress-management activities over the next several weeks post workshop. They were told that this particular worksheet would not be collected, but that it may be helpful to keep written record, as they will be asked in a general manner about their self-care practices 1 month after the workshop. Participants also received a qualitative survey with instructions for the participants to either send the survey back via U.S. mail (with preaddressed, stamped envelope included) or place in boxes located on their unit 2 to 4 weeks post workshop. This qualitative survey, composed of combination of a Likert-type scale and free text questions, was created by the project manager and was approved by the institutional review board prior to implementation. The survey did not contain any demographic info, so as to encourage honest answers on workshop effectiveness, quality, and participant satisfaction via anonymity. The qualitative survey contained the following questions:
In what way(s) has your professional practice been affected by your attending the workshop?
Have you used the Professional Quality of Life Scale since completing the workshop? ___ Yes ___ No a. If yes, was your score different than the score you calculated during the workshop? ___ Yes ____ No Please explain: b. If no, please explain why you did not use the Professional Quality of Life Scale
Since completing the workshop, tell me how your self-care practices have or have not changed? Please be specific about your changes in self-care in terms of the quality and quantity of your self-care activities.
What was the MOST helpful part of the workshop for you personally and professionally? Why?
What was the LEAST helpful part of the workshop, and how would you recommend improving this for future workshops?
How likely are you to recommend the 1-hour workshop you experienced to other nurses? (Please check one)
□ Likely □ Somewhat likely □ Neutral/unsure □ Somewhat unlikely □Unlikely
Why or why not? Please explain
Purpose
This qualitative measure was distributed at the end of the workshop to evaluate the participants’ subjective experience(s) and satisfaction with the workshop contents and structure and to assess the degree to which they had used the information that was discussed, modeled, and practiced during the educational workshop. Though some of its content would have been relevant to assess immediately postintervention, the project manager requested that participants send the survey back 2 weeks later in hopes that they would be able to report on whether or not they in fact used the workshop contents in their daily nursing practice and/or personal lives.
Limitations
Like with any measure, limitations are inherent. One particular study on Likert-type scales showed potential bias, as the findings “highlighted the role of participant’s frame of reference and indicate how questions can be interpreted in different ways according to what is salient to the individual” (Ogden & Lo, 2012, p. 360). The Likert-type scale questions in the qualitative survey were targeted toward measuring the level of satisfaction with the program, as well as the perceived applicability in their personal and professional lives.
Professional Quality of Life Scale
Background
The ProQOL scale is the most frequently used test to measure the effects of working with people in distress, with over 200 published studies citing its use. Developed initially by Charles Figley in 1980, the ProQOL—called the Compassion Fatigue Self-Test—at the time—encountered a variety of revisions, coauthoring (by Stamm as of 1988), modifications, and title changes until the late 1990s when it was renamed to the ProQOL. Initially written in English, it has since been translated into Finnish, French, German, Hebrew, Italian, Japanese, Spanish, and Croatian. The tool measures Compassion Satisfaction, Compassion Fatigue, and two of the components of Compassion Fatigue, Burnout, and Secondary Traumatic Stress. High scores of Compassion Satisfaction have generally been correlated with positive engagement with one’s employer.
Purpose
The benefit of the scale for some is that the components are individually identified and can be categorized easily during scoring; however, the scale has consistently been shown to be best used over time by comparing all components, noticing the balance between negative and positive ones to highlight need for intervention and/or management (Xie, Wang, & Chen, 2011). Administering the scale prior to the workshop and then by the participants on their own in regular intervals would serve this purpose over time.
Limitations
A potential limitation in using this scale is that it was determined not be appropriate to be used as both a pre- and posttest measure in the traditional research sense, given that the workshop is not designed to fully eradicate all symptoms of burnout and compassion fatigue within this limited workshop time frame (though ideally these symptoms showing some improvement would of course be a favorable secondary gain), but instead to empower nurses with the tools needed to achieve this outcome as a long-term goal of the educational session. The purpose of the workshop was to teach the nurses how to identify and prevent these syndromes on their own through self-awareness and self-care techniques. Therefore, administering and measuring this scale pre and immediately post workshop would have likely given a false implication that the scales should have shown a significant reduction in scores from the beginning of the day to the end, which is not the intention of this project.
Results and Outcomes
Participant Demographics
A total of 24 nurses participated in the workshops—10 fewer than the target goal of 34 nurse participants, set by the project manager during the planning phase. Demographic surveys indicated that the majority of the nurses who participated were from the Pediatric Emergency Department, while the second majority were Advance Practice Registered Nurses from the Department of Psychiatry. Number of participants per workshop varied from zero (i.e., workshops that were held but that no participants attended) to seven at any given time. The majority of nurses indicated that they had participated in self-care activities in the past, though most of them had not had education on compassion fatigue in the past. Aggregate age and gender data as well as more detailed demographic data are available in Figure 1 and Table 1.
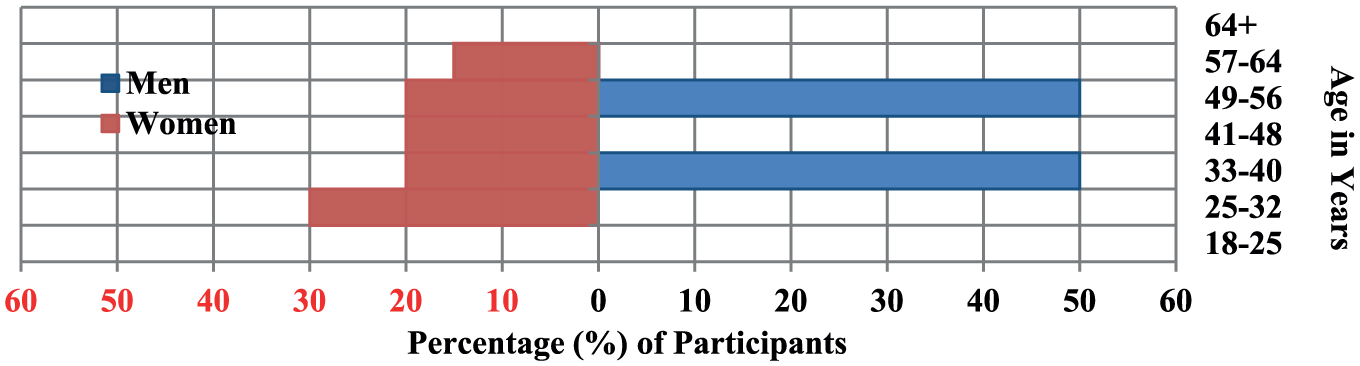
Demographic Data. Age of Participants by Gender.
Demographic Data. Participant Responses to Demographic Survey.
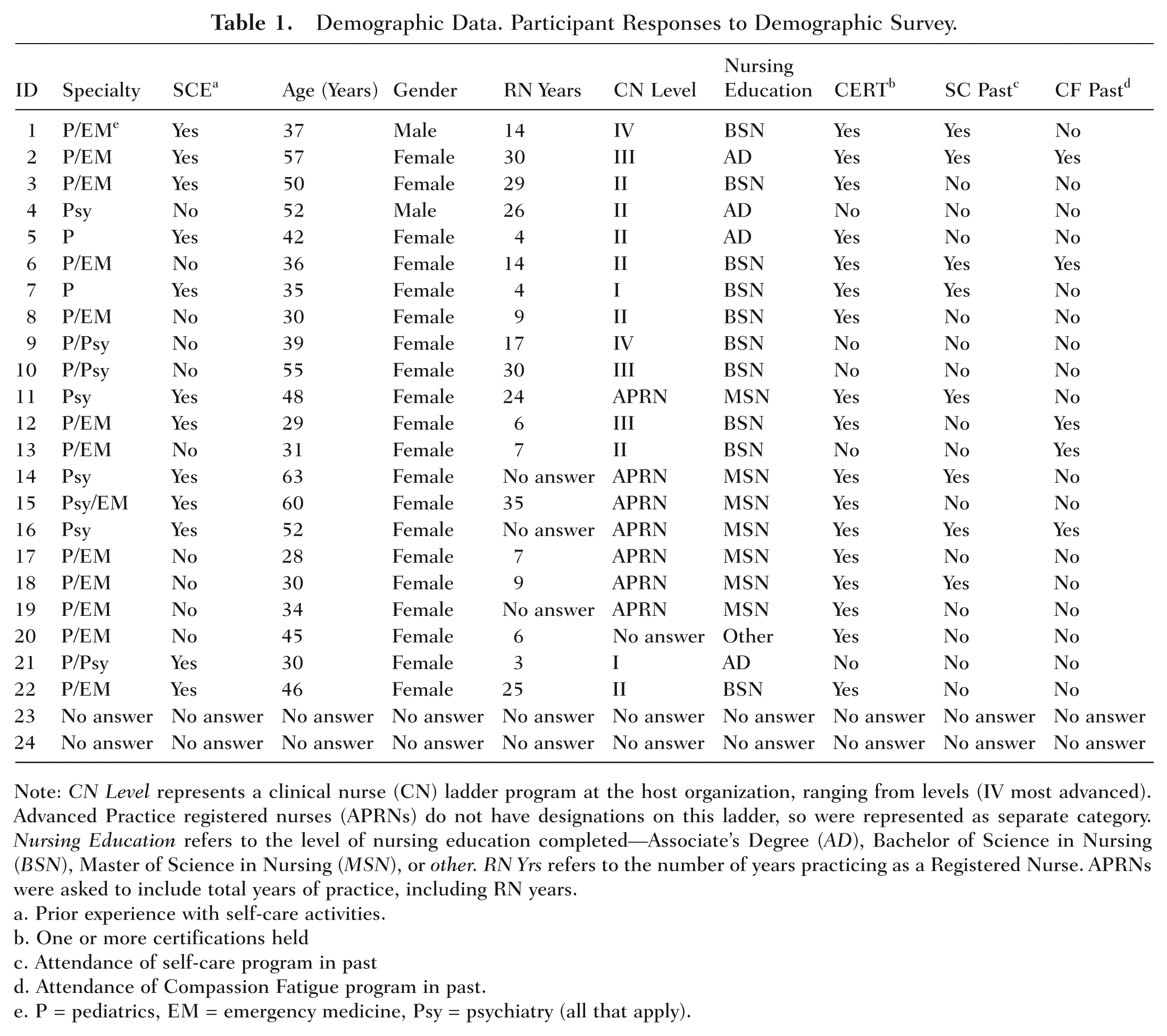
Note: CN Level represents a clinical nurse (CN) ladder program at the host organization, ranging from levels (IV most advanced). Advanced Practice registered nurses (APRNs) do not have designations on this ladder, so were represented as separate category. Nursing Education refers to the level of nursing education completed—Associate’s Degree (AD), Bachelor of Science in Nursing (BSN), Master of Science in Nursing (MSN), or other. RN Yrs refers to the number of years practicing as a Registered Nurse. APRNs were asked to include total years of practice, including RN years.
Prior experience with self-care activities.
One or more certifications held
Attendance of self-care program in past
Attendance of Compassion Fatigue program in past.
P = pediatrics, EM = emergency medicine, Psy = psychiatry (all that apply).
Quantitative Data
Pre- and postintervention knowledge tests were hand scored by the project manager, the results of which were coded and inputted into Excel spreadsheets so that they could then be compared with one another. Participant pre- and posttest percentage scores were calculated by dividing the number of correct responses by 12 (the total number of questions), the results of which are highlighted in Figure 2.
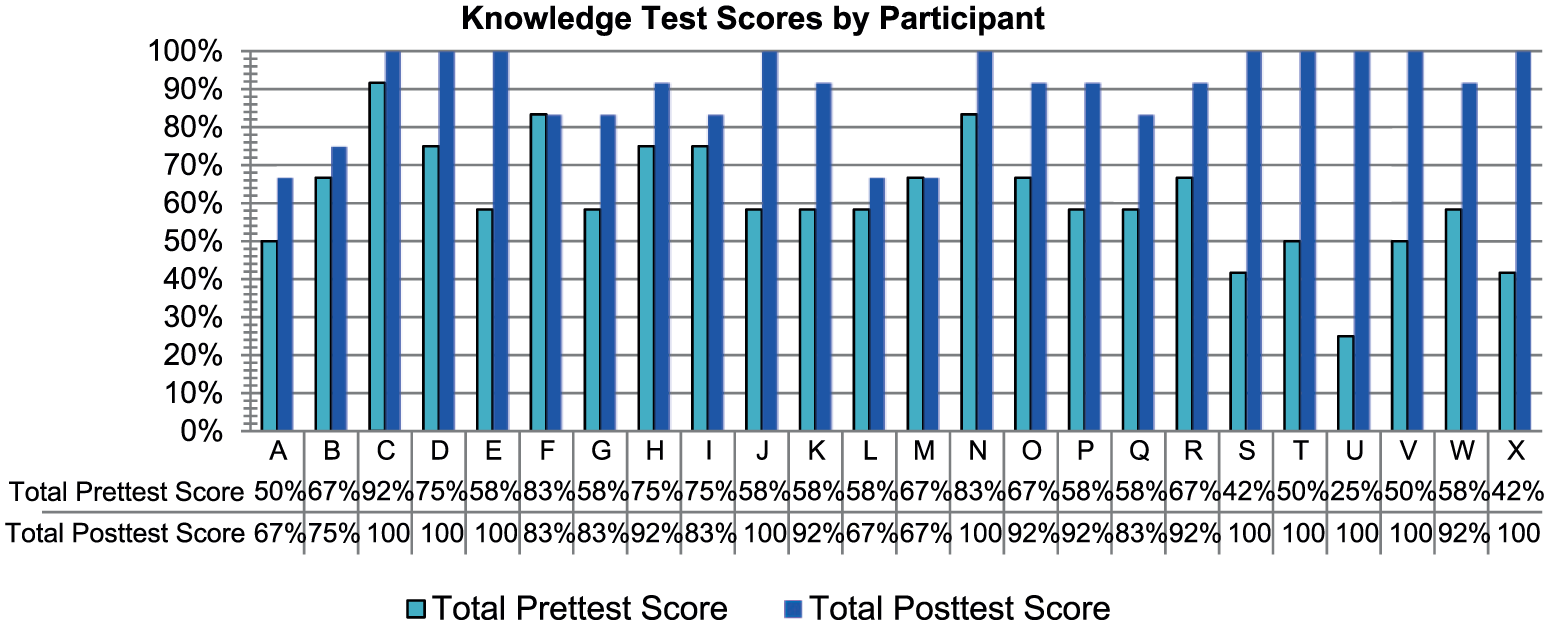
Knowledge Pre- and Posttest Scores, Paired by Participant.
Data Analysis
Pre- and posttest results were paired by participant and compared via a paired t test model. Both a one-tailed (given that the project manager predicted an improvement in scores) and a two-tailed (in order to allow for adequate analysis) versions of the paired t test were completed for comparison. Individual score improvements were calculated, noted, and recorded, and the mean difference between the pre- and postscore averages were also scored and recorded.
Results
In reviewing the knowledge test scores, a significant difference between the pretest mean score(s) and the posttest mean score(s) was evident. This was determined via performing a paired t test, the results of which indicated a statistically significant difference between the pre- and posttest scores both when completed as a two-tailed analysis (p = 3.53373064809759E-07) and as a one-tailed analysis (p = 1.76686532404879E-07). The detailed results of these calculations, completed using the Microsoft Excel Tools Pack add-on, are available in Table 2.
Statistical Analysis: One-Tailed Paired t test.
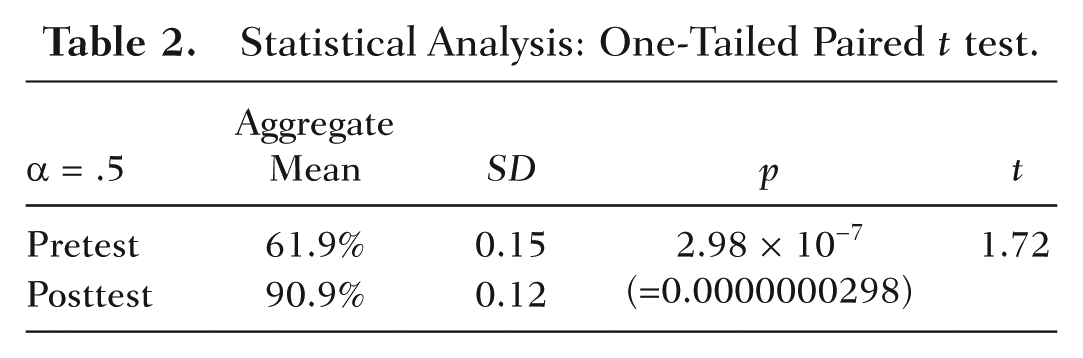
Participants scored a mean of 61.9% on the pretest version of the knowledge tests, indicating a serious knowledge deficit in the topics of interest. Postintervention, the mean knowledge posttest score was 90.9%—a mean difference of 47.5% from pre- to postintervention, indicating knowledge was in fact significantly increased during these workshops.
Qualitative Data
Postintervention qualitative surveys were returned to the project manager either via postal mail or via drop-boxes located on the patient-care units whose nurses were invited to participate in the intervention. Qualitative survey answers were transcribed by the project manager by hand into Microsoft Excel spreadsheets (available on request) and were then compiled and analyzed by the project manager. A total of 41.7% of qualitative follow-up surveys were received by their respective deadlines, dates that were set by the project manager to be at least 2 weeks post workshop attendance date to allow for adequate time for data analysis. These dates were indicated on the top of each qualitative survey and were adjusted accordingly for each workshop based on the date the workshop was held.
Results
Qualitative scores, indicated by free-text, open-ended questions as well as Likert-type scale responses that varied from “unlikely” to “likely,” indicated a generally positive response to the intervention and a high level of participant satisfaction. One benchmark goal set by the project manager was that at least 50% of participants would use the ProQOL scale post workshop. This benchmark goal was not met, however, as only 1 out of 10 of the respondents (or 10%) reported they had yet used the scale in the post workshop period. One hundred percent of participants reported that they were either Somewhat likely or Likely to recommend attendance of this workshop to a colleague in the future, which exceeded the project manager’s internal benchmark goal that 80% of responders would choose either one of these answers. Comments from participants were somewhat variable, though generally positive in nature. The majority of participants expressed the greatest satisfaction with the portions of the workshop that involved relaxation and/or stress-relieving exercises, especially those that could potentially be used while actively on duty. These exercises—not typically a part of a nurse’s workday—were reportedly highly beneficial and appreciated by participants based on survey responses. Three nurses commented to this writer (in person) that through the workshop, they realized they had suffered from compassion fatigue in the past while working in the pediatric intensive care unit and pediatric oncology units and left their jobs as a result of these symptoms. All three nurses endorsed that had they had this workshop prior to this decision, and had they known they could manage and alleviate these symptoms on their own, they may not have felt they had no choice but to leave these positions.
Discussion
The purpose of this evidence-based change project was to increase self-awareness as well as knowledge of the risk factors, causes of, and symptoms of compassion fatigue so as empower nurses to be able to identify and prevent its onset. An additional goal of the project was to provide nurses with recommendations and interactive demonstrations of self-care activities that may be beneficial tools for preventing and/or counteracting the effects of compassion fatigue in the future.
These objectives were accomplished via educational workshops for nurses that were held at the host hospital on multiple dates and times throughout the winter of 2014. Nurses received education on the syndrome of compassion fatigue itself (including risk factors, causes, symptoms, and preventative strategies), learned to self-administer and score the ProQOL Scale and how to access it in the future in order to independently self-monitor their symptoms of compassion fatigue intermittently, and received suggestions, recommendations, and interactive demonstrations of self-care activities and stress management techniques, which may have been helpful to them in preventing and/or remedying symptoms of compassion fatigue on their own. A long-term, indirect goal of preventing and/or reducing compassion fatigue among these nurses is to increase the quality and safety of patient care, improve job satisfaction and nurse retention rates, and lower compassion fatigue-related costs to the hospital.
Results exceeded the benchmarks set by the project manager in some domains and matched the benchmarks in the remaining domains—an indication of overall effectiveness of the intervention. Knowledge increase from pre- to postintervention was an indication of effectiveness in terms of the mode of delivery of and content of the educational sessions, evidenced by significant difference in mean scores from preintervention to postintervention, increases as well as significant differences in paired pre- and posttest results for individual participants.
Qualitative surveys indicated that participants were the most satisfied with the portions of the workshop that involved relaxation and/or stress-relieving exercises—especially those that could feasibly be done during a nurse’s work day. These exercises—historically, not in any way a typical part of a nurse’s day—were reportedly highly beneficial and appreciated by participants based on survey responses and one-on-one feedback during the workshops. Interventions of this type promote relaxation, stress relief, and an outlet for participants to find reprieve from the potential consequences of caring for others. High levels of participant satisfaction with these activities as well as the frequency of positive comments about these activities on qualitative follow-up surveys should be seen as indications that these were among the most beneficial portions of the workshop and potentially the most needed and appreciated (albeit novel to a typical Registered Nurse workday) of all the components.
Positive outcomes of knowledge acquisition, increased understanding of compassion fatigue, and reinforcement of the purpose and practice of self-care were appreciated as a result of the educational workshop. Nurses reported a high level of satisfaction with the program via qualitative measures, and a significant increase in mean interest in knowledge tests scores from pre- to posttest indicated that the content and method of delivery of the intended knowledge were highly effective in increasing their knowledge on the subject matter. Though nurses who care for traumatized patients—including pediatric nurses, emergency room nurses, and psychiatric nurses—were the primary subjects invited to participate (as they are at highest risk for developing compassion fatigue), this intervention should be offered to nurses of all specialties as well as to nonnursing disciplines, as literature demonstrates that all caregivers carry some level of risk for developing compassion fatigue. An intervention of this type should be incorporated in all health care settings, as a means for helping to prevent combat the onset of and myriad negative consequences of compassion fatigue on organizations, employees, and patients.
Limitations
Limitations of an intervention of this type are minimal, though important to consider. One limitation is the physical space of the workshop, which should ideally be outside of patient care areas so as to promote relaxation and stress relief and to diminish external stimuli to allow for adequate concentration and focus during the learning and relaxation activities. Financial limitations also need to be considered, as nurses must be paid for attendance in order to maximize attendance to the program. At this particular institution, the workshop was initially approved as a 4-hour workshop, including more detailed and lengthy relaxation exercises as well as other components that promoted self-awareness, mindfulness, and stress relief. However, state budget cuts to hospitals that ensued the year of project implementation were hindrances to this initial approval, requiring adjustments to the workshop content and structure in order to consolidate its contents and purpose into a 1-hour session.
Electronic limitations also existed, one unforeseen limitation of which was the hospital policy restricting contacting employees via e-mail for any research project or study. Participant response rate on the follow-up surveys may have been higher than 65% if this limitation did not exist, given that the majority of persons use electronic communications at least once per day.
Ideally, to better assess the impact of this intervention, participants would have been retested 2 or more weeks after the educational session to evaluate their level of retention of the information presented on a longer term basis. However, given that this was a time-limited project as part of the author’s clinical dissertation, this was not feasible within the small time frame.
Future Implications
Given the positive feedback received from participants as well as the increase in knowledge seen postintervention, the workshop was effective in delivering education to nurses on preventing, identifying, and managing symptoms of compassion fatigue as intended. The high level of participant satisfaction in the content and effect of the intervention, evidenced by results of the qualitative and quantitative measures as stated above, further supports implementing a similar program in the future. Though this particular project was promoted to nurses in the Departments of Psychiatry and Pediatrics, future workshops should be inclusive of all specialties, education levels, and disciplines (including MD, ancillary staff, etc.) as caregivers of all types are at risk for compassion fatigue to some degree or another. Also, as referenced in the Limitations section, future interventions of this type would ideally allow for more time to be able to survey respondents several weeks postintervention to gauge their level of knowledge retention on a longer term basis to further weigh the intervention’s impact and effectiveness.
Conclusion
The primary quantitative measure of workshop effectiveness in achieving the outcome goal of improving the knowledge about the recognition, prevention, and management of compassion fatigue in high-risk nurses was a pretest–posttest measure. A 47.5% increase in mean scores was demonstrated from pretest (mean score of 61%) to posttest (mean score of 90%), indicating an impressive and significant increase in knowledge via the workshop. These results were deemed to be statistically significant using a Microsoft Excel–run paired t test analysis of pre- and posttest scores. The benchmark for mean scores, 80%, was not only achieved but also exceeded by 10%. Only 10 out of 24, or 41.7%, of qualitative surveys were received prior to the final deadline, which did not meet the benchmark goal of 50% that was initially set by the project manager. Qualitative survey responses were exceedingly positive, however, with all participants reporting a high likelihood of recommending this program to others and they themselves attending a similar program in the future. Comments from participants also indicated a high level of benefit from and satisfaction with the program contents and format, as well as positive changes in their self-care practices and professional nursing practice as a result of their attending the workshop(s).
Overall, positive outcomes were appreciated as a result of the educational workshop. Nurses reported a high level of satisfaction with the program and a mean interest in knowledge tests scores indicated that the content and method of delivery of the intended knowledge were effective. Though nurses who care for traumatized patients—including pediatric nurses, emergency room nurses, and psychiatric nurses—were the primary subjects invited to participate as they are at highest risk for developing compassion fatigue, this intervention should be offered to nurses of all specialties as well as to nonnursing disciplines, as all caregivers are at some level of risk for its onset.
Footnotes
Acknowledgements
A special note of thanks to Cynthia Bautista, PhD, for her guidance and support in facilitating and executing this project from start to finish.