
Abstract
Leading highly functional health care teams in all practice settings is sustained through the identification of a conceptual framework to guide education and practice. This article presents an interdisciplinary framework for palliative and hospice education and practice. The framework builds on theoretical caring to convey elements of relational, holistic and compassion; articulates interprofessional tenets for guiding values; and aligns with constructs for palliative and hospice best practices. The framework invites those at the bedside and in leadership to be intentional in attending to education and the necessary activities that address the day-to-day operations of palliative and hospice care, as well as, honoring all interdisciplinary collaboration that supports quality outcomes and inspires actions that transform.
Keywords
Introduction
Health care teams are reminded regularly that no matter the practice setting, the collective purpose is to provide a transformative patient experience, rich in artfully skilled holistic caring. Regardless of the role one holds on a health care team, having a clear conceptual framework for guiding practice and education is useful. The framework is accessed to continually guide education of health care providers. Once understood, it is subconsciously referenced to guide the intimate relationship between health care team and patient and families during palliative and hospice care. Its’ usefulness for palliative and hospice care is unmeasurable, yet there is a dearth of literature that advocates important conceptual linkages within a holistic caring lens. Therefore, the purpose of this article is to present a conceptual framework for palliative and hospice education and practice that conspicuously aligns caring theory with interprofessional tenets and clinical practice guidelines. The framework may be used to guide interdisciplinary education and practice encounters for all who are affiliated with palliative and hospice organizations.
Background
The terms palliative and hospice are often used interchangeably; however, that interchange is not completely accurate. Palliative is a term used to denote care that prioritizes the assessment and management of symptoms, caregiver needs, and care coordination (National Quality Forum, 2018). Palliative approaches can be accomplished at any time across the lifespan, but they seemingly increase when caring for those experiencing serious illnesses. Hospice is a term used to denote a specialized type of palliative care. Hospice approaches are directed toward care provision at the end of life, commonly within a 6-month or less prognostic timeframe. For this article, the terms are paired (palliative and hospice) to reflect distinct but interconnected care approaches. The framework was developed to intentionally guide education and practice for a large nonprofit hospice organization, but the application of the framework in palliative settings is plausible.
Palliative and hospice practice settings are complex, diverse, and constantly changing. There is focused attention on quality patient outcomes, dependent on interdisciplinary support for patient and family. Specifically, for hospice, federal regulations mandate an interdisciplinary team (IDT) approach for the provision of care (Centers for Medicare & Medicaid Services, 2017). Further guidance from experts is found within documents published by the Centers for Medicare & Medicaid Services (2017), the National Quality Forum (2018), and the National Consensus Project for Quality Palliative Care (NCPQPC, 2018), and the documents state that patient (and family) care be provided by interprofessional team. Careful examination of these documents helps health care teams gain a comprehensive appreciation of the complexities associated with palliative and hospice care. Still, the guidance dictates neither the conceptual foundations nor the exact way in which the interprofessional team should function.
There are, in fact, national guidelines that articulate team competencies to recognize and validate the IDT approaches (Interprofessional Education Collaborative, 2016). The competencies were foundationally developed to assure that multidisciplinary teams innovate solutions to complex health care challenges. Furthermore, evidence exists that indicates that IDTs enhance care provision, reduce lengths of stay, minimize costs, and decrease medical errors (Green & Johnson, 2015). Despite guidelines and evidence presupposing interprofessional practice and education, there are barriers to developing and implementing activities (Blacker et al., 2016.) This commitment to caring from an interdisciplinary perspective is enhanced by a framework that can be used by all members of a team to guide professional education and support excellent practice outcomes for palliative and hospice care.
A Framework for Palliative and Hospice Education and Practice
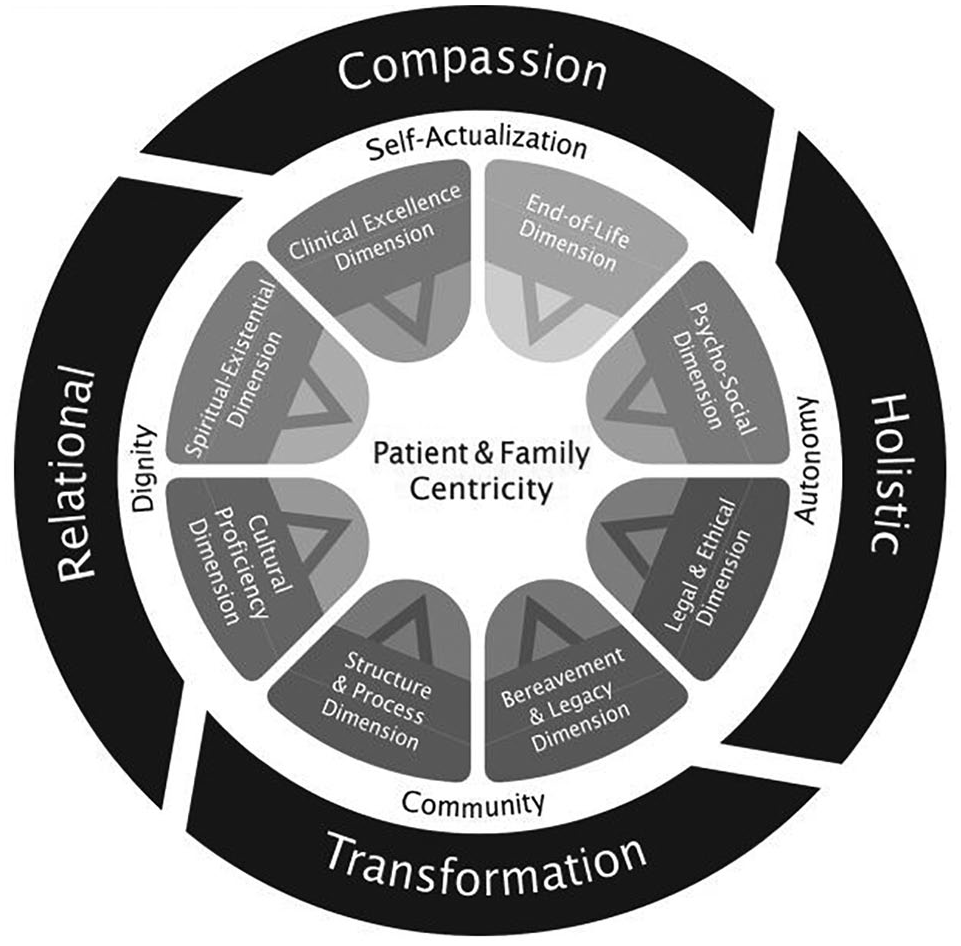
While interdisciplinary care is an objective for palliative and hospice practice, there is a shortcoming of literature illustrating how to conceptually frame for an IDT within a holistic caring lens. Parahoo (2006) declared that the term conceptual framework is appropriate when drawing on ideas from various theories to guide education, and practice. Henceforth, the conceptual framework being presented for palliative and hospice care foundationally builds on theoretical caring to articulate compassion and relational and holistic underpinnings, incorporates interprofessional tenets for guiding values and competencies; and aligns with constructs for palliative and hospice best practices. The framework is illustrated in Figure 1 and is elaborated below in three sections corresponding with elements of caring, guiding values, and best practices.
Interdisciplinary Framework for Palliative Care and Hospice Education and Practice
The framework is iterative and invites professional reflection but holds caring as its basic principle. Inspired by figures and ideas shared by Reed (2010) and Anderson et al. (2018), the conceptual framework provides a holistic and relational view that honors the interdisciplinary journey of personal health and illness within a palliative and hospice care perspective. Transformation is recognized; therefore, curing or fixing are not the ultimate aims. The practice and education framework is essential for leading successful IDTs as it enables a shared and integrated practice model and guidance for education.
While the image in Figure 1 is presented one dimensionally, the dynamic and interactive nature of the model is paramount and explained further. The circular design of the framework denotes the unending nature of the interdisciplinary palliative and hospice approach. The layers of the framework are not impermeable; rather, there is multidirectional movement among all elements. The outer ring of the framework reflects caring and is represented by the compassion and holistic and relational features that surround all encounters enabling transformation for all involved. The next ring of the framework represents the guiding interprofessional values of autonomy, self-actualization, dignity, and community that guide IDT practice. The framework’s inner ring represents the orchestration of complex caring best practices that unfold while holding the patient and the family in the center. Furthermore, the framework ideally is suited for the IDT members who provide direct care but certainly can be useful to educate and guide employment practices for all who are affiliated with palliative and hospice service.
Patient and Family Centricity
The notion of patient and family centricity celebrates care design in a manner that is meaningful and valued to the individual patient and family. There is a recognition and involvement of patient and family in all aspects as the centricity focus obliging that the IDT collaborate with, listen to, and include them in the plan of care. Moreover, the centricity focus creates a more intentional, and empathetic encounter that can be transformative for patient, family, and members of the IDT.
Everyone represented within the framework are supported in their own continuum of living and healing; patient and family member; nurse caregiver, nurse leader, physician, social worker, nursing assistants, chaplain, bereavement specialist, volunteers, and music therapist. The IDT collaborative contributions are void of “who did what” labels. Caring contributions flow freely, the shared effort of which creates synergy and ultimately results in a unified approach to patient care (Cote & Correoso, 2016).
To be sure, IDT collaboration and communication are at the core of patient and family centricity. The IDT can be described as a group of collaborating professionals who collectively advocate for, share information, set goals with, and coordinate strategy in order to yield best patient and family outcomes (Green & Johnson, 2015). The interconnectedness of the human experience is realized by honoring the centrality of patients and families. In palliative and hospice practice, the team calls on each other to respond with compassion, which benefits not only the patient and family but also the collective “we.” Patient, family, and health care providers transform as a result of operationalizing this framework.
Outer Circle of Framework: Transformation, Compassion, and Holistic and Relational Features
The outer circle is representative of caring as a basic principle that guides the IDT approach. Caring within health professions is acknowledged by many disciplines. Caring is a humanistic and intentional approach to health care that honors the whole person, family unit, and members of the team associated with the continuum of health and healing. The basic components of caring such as honesty, understanding, humility, hope, patience, trust, communication, and authenticity create a safe environment from which the team functions optimally (Mayeroff, 1970; Nancarrow et al., 2013; Parola et al., 2018). It is within this context of caring that this framework is offered. There is not one theorist or theory that is selected.
Roach (1992), an esteemed caring nursing scholar, asserts that caring is “not unique to any particular profession” (p. 4). Caring is ascribed to expressing humanness. Still, the articulation of what is associated for caring to be rendered within an IDT palliative and hospice framework is essential. The framework implicitly identifies caring expressed through knowing, responding, and interacting. Also, implicit to this framework are alternating rhythms of dialogue, hopeful decision making, and trusting caring leadership within a team approach that supports transformation (Mayeroff, 1970).
Transformation
The notion of transformation is a vital element of the framework, yet it is challenging to describe. Transformation is uniquely experienced in moments of emotional reflection, through powerful breakthroughs of symptom management or in subtle existential shifts. Transformation occurs for and with patients and families and IDT members. The transformation seems to happen as a result of caring intention to work with and care for others while simultaneously deepening a connection to the human experience of health and healing and living and dying. Experiences of transformation are anecdotally observed with noted remarks such as “I’ll never be the same again,” Something within my loved one is at peace,” “All of a sudden everything made more sense,” or “This experience of death gave me life.” Contemplating the human experience of life, death, suffering, love, and hope may be transformative for anyone. More research is warranted to fully analyze the nuances of transformation; however, within this education and practice framework, it is an element of caring that surrounds all encounters.
Compassion
Compassion is defined as the conscious awareness of and desire to alleviate another’s suffering (Merriam-Webster, n.d). Compassion in palliative and hospice care may appear self-evident, but it is important to acknowledge its theoretical foundation in caring. Researchers fully articulate elements of compassion as ways of being and inspiring action (Boykin & Schoenhofer, 2001a; Watson, 2005). Compassion honors respect for persons, prioritizes knowing other, advocates for ethical engagement, and celebrates presence. Compassion may be what unites an IDT because it is an underlying professional core value (Dyess, Prestia, & Smith, 2015).
However, scholars do not unanimously agree on a definition for interdisciplinary compassion (Klaver et al., 2014; Leget et al., 2017). Still, meaningful understanding of compassion and collaboration exists. One definition offered by Pfaff and Markaki (2017) focuses on compassionate collaboration that is a process through which caregivers from different professional and non-professional backgrounds work together with patients and families to deliver care that recognizes, understands and responds to concerns, pain, distress, or suffering, with the aim to promote positive patient-family, team, and organizational outcomes across healthcare settings. (p. 3)
Compassion is often framed by processes associated with quality health care, perspectives associated with intention, and purposes associated with interventions inside a patient-centered practice setting. Within this interdisciplinary framework, compassion is acknowledged as a guiding basis for every professional encounter, as are holistic and relational mind-sets.
Holistic
Holistic caring respects diversity, honors presence, and addresses professional and ethical obligations of ontology. Holistic ways of being are grounded in knowing the wholeness of individuals. Knowing wholeness necessitates a lens of possibility not a lens of deficit (Boykin & Schoenhofer, 2001a). Rather than focus only on the physical, the mind, spirit, emotions, body, and environmental context are considered and synthesized to determine the best approaches to care.
Members of the IDT skillfully cocreate with patients and family an evidence-based integrative approach that respects life, supports palliative health, and nurtures efforts for dying well (Dossey & Keegan, 2016). As holistic professionals, intuitive thinking advances care while multiple modalities are considered to ensure the best options for symptom management. Kindness, trust, peacefulness, and unconditional positive regard encourage the patients/families and the IDT members. The holistic intention or the ability to consciously potentiate the integration of mind, body, and spirit begins with establishing relationship.
Relational
Relational establishment within any palliative and hospice situation demands sensitivity to the gravity of the decisions being contemplated. Relational elements include creating presence or a manner of being with, knowing, active listening, and meaningful interpersonal connection, which will advance compassion in patient and family and IDT encounters (Costello, 2017; Doona et al., 1999; Ferguson, 2018). At the same time, the relational communication invites reciprocal interactions that demand authenticity for and from IDT members.
Authenticity can be cultivated and often is evidenced by simplistic displays of human kindness. Spichiger (2010) asserts that IDT members should proudly acknowledge their intentional inclusion of “friendliness, cheerfulness, and good manners as indispensable conditions” (p. 200) that are foundational to any health care. However, the relational elements often demand deepening connections with patients, families, and IDT members as situations vary greatly. Ferguson (2018) identifies “vivid descriptions” of nurses “knowing and caring” within a “special relationship” that accentuates “person centered comfort care” (p. 76). For palliative and hospice care, relational elements are inclusive of vigilant attention to the physical welfare, personal safety, and emotional strength of patients and family, as well as the IDT.
Middle Circle of Framework Guiding Interprofessional Values
The synergies created by a caring IDT are enhanced by interprofessional values that are conscientiously identified, shared, and lived. The interdisciplinary framework recognizes four guiding interprofessional values that are embedded in every encounter; autonomy, self-actualization, dignity, and community (Canadian Palliative Care Association, 2013). These values can be actualized by professionals, patients, and families.
Values expressed are meant to assure that caring occurs. The values reflect the relational context of the patient and family. While values may be individual in some cases, there are times when they are collective. When these values are viewed through varied lens, their importance to IDT cohesion and patient well-being is recognized (Table 1). The interactions supported by guiding interprofessional values in the framework benefit not only the patients/families but also the IDT as autonomy, self-actualization, dignity, and community manifest themselves through actions.
Foundational Values Expressed for Patient/Family and Interdisciplinary Team

Autonomy
Patient autonomy is consistent with what some would label an essential element of bioethical principles in Western hemisphere cultures but not across all cultural variations (Kara, 2007). Autonomy is a value that encompasses the freedom to make individual choices and decide on a course of action for those who are capable (Beauchamp & Childress, 2013; Cheon et al., 2015). The amount of autonomy is wholly governed by the patient and family acknowledging their cultural/religious preferences. Within this framework, there is an expectation that the IDT will endeavor to promote informed decision making for patients and families as they collectively define a quality palliative or end-of-life experience. The freedom to determine how one is cared for while facing serious illness leaves a lasting impression on all those involved. Similarly, the autonomy of IDT members is valued and demonstrated as communication occurs within meetings to develop and contribute to the patient’s plan of care. Ideally, communication that supports autonomy should occur early and often as plans for care are considered.
Self-Actualization
Perceptions of life for those facing serious illness are multidimensional. Still, in palliative and hospice care settings, self-actualization is a goal. The value of self-actualization was made universal by Maslow (1970), the need to be fulfilling one’s individual unique potential. The journey toward attaining that potential within a life is often hastened with the eminence of death. According to Maslow, self-actualization can be achieved if the other hierarchy of needs are met. Applied within this palliative and hospice care framework, the hierarchy prioritizes the ease of maladaptive symptoms such as pain, or shortness of breath, and directs efforts toward experiences of sensing safety and belonging; before there could be potential self-actualization (Zalenski & Raspa, 2006). Assisting patients to review how love, time, and faith have intersected to create meaning within an individual’s life may support the important journey toward self-actualization.
Dignity
Dignity is recognized as a complex multifaceted value. According to one group of scholars, “dignity in care means the kind of care, which supports and promotes, and does not undermine or erode, a person’s self-respect regardless of any difference” (Tauber-Gilmore et al., 2018, p. 3). As humans experience the process of serious illness, loss of dignity or loss of self-respect becomes a concern. Relieving this worry is an IDT priority for those who are living and those who are dying (Namendys-Silva, 2017). The IDT works to knowingly bring honor and respect to the individual’s time on earth through remembrance and discussion. Respecting and appreciating is the basis of palliative and hospice care as dignity is preserved.
Community
Death is universal. Its unique expression, although honored, cannot mask the collective experience. Death is the final experience in life, yet it does not need to be filled with pain, suffering, or solitude (Kessler, 1997). Community denotes the interconnectedness and caring ethos of professionals, patient, and family working together. As a value, community represents the dedicated principles associated with developing and improving palliative and hospice care worldwide (De Lima & Radbruch, 2018). A collective goal is for “universal access to high-quality palliative care, integrated into all levels of health care systems in a continuum of care with disease prevention, early diagnosis, and treatment, to assure that any patient’s or family caregiver’s suffering is relieved to the greatest extent” (De Lima & Radbruch, 2018, p. 96). Community can also point to the importance of one’s social community within any palliative or hospice situation. Meeting the needs as a community to benefit the “collective we” inspires the use of this caring interdisciplinary framework.
Inner Circle of Framework Best Practices for Palliative and Hospice Dimensions of Care
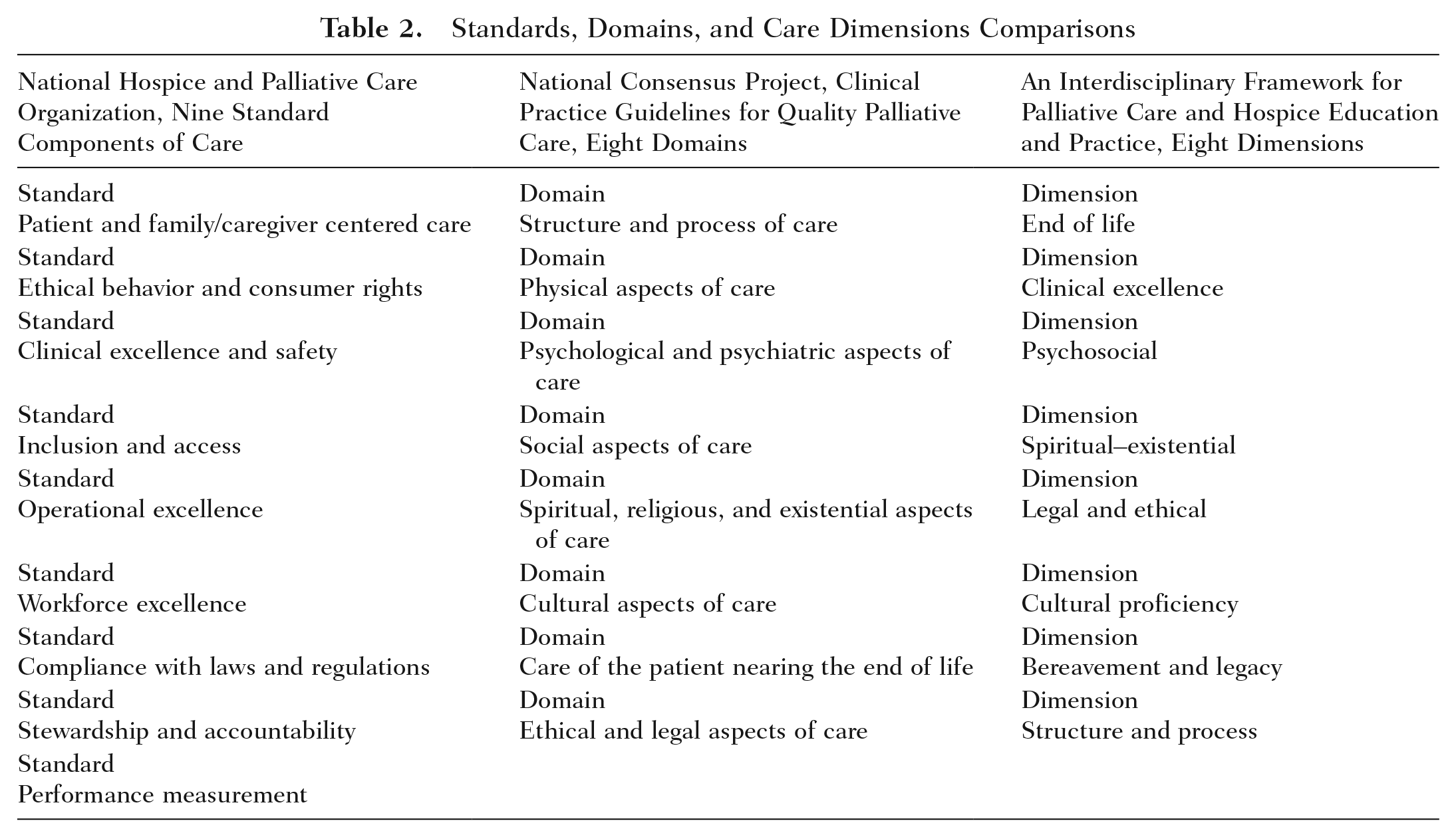
The presented dimensions of care within the interdisciplinary framework align with the National Hospice and Palliative Care Organization’s (NHPCO) Standards of Practice for Hospice Programs (2018) and the NCPQPC Guidelines (2018). Both of the aforementioned practice documents promote high-quality palliative and hospice care. Collaborative organizations embracing these guidelines exhibit a commitment to organizational excellence, foster consistent standards, and encourage continuity of care across settings. The dimensions of care within Figure 1 mirror and amalgamate the nine standard components determined by NHPCO and the eight domains identified by the NCPQPC.
Table 2 lists the NHPCO standards, the NCPQPC domains, and the dimensions chosen for the framework. Each dimension is deemed essential to the interdisciplinary framework and creates continued opportunity to review the evidence for best practices that influence exceedingly compassionate care in practice settings. For a better understanding of these best practices, please refer to Clinical Practice Guidelines for Quality Palliative Care (NCPQPC, 2018).
Standards, Domains, and Care Dimensions Comparisons
End-of-Life Dimension
All agree that patients and families ought to receive optimal self-defined care within palliation and at the end of life. In fact, the Institute of Medicine (2014) recommends that competent palliative and hospice health care professionals be proficient in communication skills, interprofessional collaboration, and symptom management. The National Institutes of Health (2018) acknowledge the term end-of-life care as a conundrum to predetermine because individuals experience it differently and likely require vastly different approaches to compassionate caring. The NCPQPC rephrased end-of-life care as care nearing the end of life. It is the care and support provided in the period before death, inclusive of weeks or months prior to the heartbeat stopping. This focused care dimension supports patients and families so they experience ease during dying. The IDT actions within the framework incorporate evidence-based interventions that are tailored to patient and family preferences for comfort and serenity at the end of life with a quest for clinical excellence.
Clinical Excellence Dimension
Quality patient outcomes centered on patient and family implies clinical excellence. Clinical excellence demands symptom management that is predicated on a comprehensive assessment and is an element of care within the framework (NCPQPC, 2018; NHPCO, 2018). Decline in health at the end of life may be filled with a sundry of clinical indicators, and the IDT is obligated to recognize and fully address all of these. Currently, there is a large and growing body of evidence focusing on the management of physical symptoms for palliative and hospice care. Researchers acknowledge that there is a global need for a wider understanding, measurement, and response to multidimensional symptoms (Wilkie & Enzenwa, 2012). The pinnacle of clinical excellence occurs when opportunity is found in crisis and the IDT cocreates innovative treatment plans. The patients and/or families relate the “lived” symptoms. It is the IDT that expertly translates them into something recognizable, creating accurate modalities of care. This also extends to the psychosocial dimension.
Psychosocial Dimension
Many efforts in palliative and hospice care address symptom management, emotional support, spiritual care, provider communication, and reducing aggressive treatments that contribute to suffering (Wilkie & Enzenwa, 2012). There are fewer efforts that focus on the patient and family social needs that may be important to the experience of dying well. In this framework, the psychosocial dimension is recognized as essential and conspicuously includes the dynamic of family/loved ones as caregivers (NCPQPC, 2018; NHPCO, 2018). “Appropriate end-of-life discussions can promote healthy coping” and if done appropriately fosters “open discussion of treatment desires, feelings, and fears” (Vazquez & Santone, 2011, p. 321). The psychosocial dimension accounts for coping and mental stability as vital for dying well. It is closely linked to the spiritual–existential dimension.
Spiritual–Existential Dimension
The IDT is called to address the spiritual-existential dimension of patients and families in a compassionate caring manner (NCPQPC, 2018). Addressing this dimension demands that palliative and hospice professionals hold in perspective the values, beliefs, and convictions of others before self. No single definition of the spiritual-existential dimension exists within the literature although its importance is accepted (Koenig et al., 2001). For this framework, the dimension combines attributes of beliefs; meaning for life; interrelating with self, others, and/or Divine; offering love and relatedness; including hope; and the need for forgiveness (Dyess, 2011). It is the essence of one’s being that encompasses living and provides the awareness of what purpose is and how inner resources shape life (Burkhardt & Nagai-Jacobson, 2002). “Current spiritual care interventions, such as employing compassionate presence, bearing witness, deep listening, centering prayer, reading scripture, and connecting to community, are all crucial to the art of tending spirit” (Rosa et al., 2019, p. 101). This dimension may or may not involve a traditional religious denomination, but ritual may be significant, nonetheless.
Cultural Proficiency Dimension
A multiethnic and multigenerational inclusive perspective with an aspiration for cultural proficiency is requisite to the interdisciplinary framework. This dimension of inclusive aspirational cultural proficiency emphasizes that the IDT hold abilities to care for patients, families, and team members representing varied cultural contexts and respond appropriately (NCPQPC, 2018). The responses include but are not limited to LGBTQ (lesbian, gay, bisexual, transgender, queer) inclusive care, bilingual professionals in conjunction with language lines, awareness of ethnically diverse practices at the end of life, recognition of barriers that may exist in IDTs, and intentional leadership initiatives to promote proficiency (Acquaviva, 2017; Reese & Beckwith, 2015). The aspiration of cultural proficiency enables important conversations with patients and families at the end of life and breaks down barriers for quality outcomes (Periyakoil et al., 2016). The culturally proficient IDT supports unique caring for “individualized patient care, which demonstrates respect for a patient’s health care beliefs and acknowledges that these beliefs play a role in effective health care delivery” (Saccomano & Abbatiello, 2014, p. 24) at the end of life.
Legal and Ethics Dimension
There are a number of features that constitute this legal and ethics dimension of care in the framework that include internal compliance, advance directives, advance care planning, wills, financial concerns, and communications involving decisions related to medically futile treatment (NCPQPC, 2018; NHPCO, 2018; Dyess, Tappen & Hennekens, 2014). Fear and uncertainty often surround unpreparedness for palliative and hospice services. In an effort to educate and support the family unit, members of the IDT may review consumer rights, explain eligibility requirements for the levels of care, and provide options for decision making (NHPCO, 2018). Within this dimension of the framework, patients and families are assisted to navigate legal and ethical perspectives of healthy dying, thereby alleviating fear and uncertainty.
Bereavement and Legacy Dimension
Bereavement is an undefined time period of grief and mourning subsequent to the death of a loved one. Patients and families can also bereave the memory of what was, in terms of independent function or an ability that contributed to life quality. Palliative care and hospice teams are called to support and even anticipate this bereavement experience whenever it appears. Patients require ongoing support in their “continued search for meaning, despite their impending mortality” (Anderson et al., 2018, p. 261). On patient death, ongoing engagement with families and loved ones ensure that grief work is supported. The legacy of life is acknowledged as the IDT aims to allow for a positive, conscious effort of identifying what matters most for patients and families.
Structure and Process Dimension
All palliative and hospice care practice settings acknowledge procedural process and policy that address compliance with regulatory standards and advancement of quality patient outcomes. In this framework, the structure and process of the organization are paramount to successful caring. Like other health care organizations, features of structure and process may apply the principles associated with lean businesses (Institute for Healthcare Improvement, 2005). These principles dismantle silos, point blame to processes not staff, integrate standardized work, empower frontline staff to eliminate productivity waste, and utilize visual systems for accountability. Recruitment, initial orientation education, and ongoing skill refinement are essential aspects for creating a successful palliative and hospice culture (Dudley et al., 2018). Within this culture, there is opportunity for celebrations of even the tiniest of successes. This framework allows for the devotion of time to acknowledge, praise, and reward collegiality.
Discussion and Conclusion
Hospice and palliative care is provided in many settings: within a patient’s home, assisted living facility, hospital, or specialized care unit where the IDT is not interfacing moment by moment. The authors offer this framework as a foundational tool to guide the IDT in achieving “high quality outcomes, improving patient quality of life and decreasing costs” (Blacker et.al, 2016, p. 329). Rosa et al. (2019) acknowledge that “the physical, mental, emotional, and spiritual responses to suffering are dynamic and require continual reassessment by providers to give appropriate care” (p. 105). This dynamic framework allows for the continual assessment and intervention response to support all connected to a palliative and hospice situation.
Innovative efforts can be used to ensure the use and evolution of the framework within any organization. One option is to encourage the sharing of patient and family stories within the IDT weekly meetings. The commitment to share stories yields many benefits albeit time consuming. The sharing of stories reveals the embedded expert practice knowledge displayed in day-to-day caring and utilization of the framework in practice (Boykin & Schoenhofer, 2001a). The stories remind the IDT of what matters most. All members of the team learn from this expert practice knowledge and are provided with an opportunity to inspire one another in living compassion with patients and families. Sharing of stories also fosters conceptual framework reeducation with the acknowledgement of the intensity of palliative and hospice work so that members of the team can be encouraged and affirmed. Compassion is bolstered and celebrated.
In this interdisciplinary framework, leaders “integrate, coordinate, and facilitate the interface of multiple dynamic and caring relationships from which positive outcomes ultimately emerge” (Dyess, Prestia & Smith, 2015, p. 114 ). This leadership requires intentional energy and takes time, commitment, and courage, to not only attend the necessary activities that address the day-to-day operations but also honor interdisciplinary collaboration supporting quality outcomes and inspire actions that transform (Boykin et al., 2005; Boykin & Schoenhofer, 2001b; Parola et al., 2018). The interdisciplinary collaboration will yield advancements in palliative and hospice care.
No doubt, all who practice palliative and hospice care can recall a patient and family situation that can illuminate the realities of the framework presented to acknowledge transformation. The transformation can be mutually experienced by all who are involved in any encounter throughout an organizational day. Previous researchers of health care practice settings suggest that when a caring practice is uniquely created, transformational changes occur that increases satisfaction and a sense of value for all involved (Boykin et al., 2005; Boykin & Schoenhofer, 2001b; Parola et al., 2018) The education and practice framework galvanizes a commitment to ongoing IDT collaboration and transformation in the practice setting, and the recruitment, retention, and sustenance of the leaders for palliative and hospice innovation.
Footnotes
Authors’ Note:
The authors wish to acknowledge the Trustbridge organization and team.