
Abstract
Keywords
Latinos currently comprise 17% (50.5 million) of the total U.S. population; projections estimate that the percentage will grow to 25% (98 million) by 2030 (U.S. Census Bureau, 2015). Persons of Mexican heritage constitute more than 66% of all Latinos in the United States, with their population expanding faster than that of other Latino groups (Passel, 2011; U.S. Census Bureau, 2015). In particular, California, Texas, and Arizona have the largest population of persons of Mexican origin in the United States (Gonzalez-Barrera et al. & Lopez, 2013), and Mexican-origin Latinos comprise 87% of all Latinos living along the U.S.-Mexico border.
Latino Americans experience higher rates of behavioral health and substance use issues with 30% lifetime incidence versus 20% incidence for Anglos and substance addiction rates of 10% versus 8% for Anglos (González et al., 2010; Lai et al., 2015; López et al., 2012). Alegría, Canino, et al. (2008) showed that Latino Americans were the least likely of all minorities to utilize behavioral health services in their study of 8,000 subjects. Of those persons reporting behavioral health illness, only 5.9% of Latino Americans received any type of treatment versus 7.2% of African Americans and 11.8% of Anglos. Subsequent studies continue to show that Latino Americans are the least likely of minorities to receive behavioral health or substance use treatment (Alegría, Chatterji, et al., 2008). The purpose of this article is to highlight how culturally based care might be integrated into treatment programs to produce better outcomes for Latino patients. In addition, this article also emphasizes the importance of having the National Center for Complementary and Integrative Health (NCCIH) provide official recognition of Mexican traditional medicine (MTM) to facilitate its integration into Western health care for Latino patients.
Issues such as access to care, preferred language of the patient, stigma regarding behavioral health, and potential treatment preferences serve as ongoing factors in the limited utilization of behavioral health services. To alleviate these social determinants of health and the resulting behavioral/substance use disorders that may occur as a result, researchers postulate that specific comprehensive, multifaceted, culturally based methods of care might ameliorate these issues (González-Guarda et al., 2011; Guerrero et al., 2013). Addressing this issue through implementation research to identify potential treatment preferences and best practices is of paramount importance for addressing this ongoing disparity. With increasing rates of opioid use disorder in Latinos in the past 2 years, finding methods to address this issue is of the utmost importance (Bebinger, 2018).
While research shows that culturally based care systems enhance minority utilization of health care services (Wood & Newbold, 2012), a number of factors continue to set barriers to health equity for Latino immigrants (Betancourt et al., 2003). One factor is that immigrants are often rural Mexicans with traditional values and beliefs about health and illness (Brown et al., 2015). In addition, those of Latino descent are more likely to use traditional and folk medicine than Western medicine, especially for their initial inquiries regarding health or illness treatment-related services (Ho et al., 2015). This reluctance only increases when immigrants consider mental health or substance use treatment services because the increased stigma, lack of access to language/culturally congruent services, and other issues in treatment seeking result in lower utilization rates among Latinos for mental health and substance use services than other groups (Alegría et al., 2010; Cook et al., 2014). Decreased rates of treatment seeking combined with the recent rise in synthetic opioid availability and other factors have resulted in new challenges to addressing the opioid epidemic for minority groups, with opioid use and overdose rates rising faster for Latinos (52.5%) than for White, non-Hispanics (45.8%) from 2014 to 2016 (Bebinger, 2018).
MTM originates from pre-Columbian Mexican culture and shares similar characteristics with other Central and Latin American traditional healing practices. MTM has served as the basis for indigenous healing practices for more than 400 years (Martinez, 2009). An important component of successfully working with Latinos is understanding the belief structure, theoretical underpinnings, and healing/curing strategies associated with traditional and folk medicine of Mexican American immigrants. MTM remains an important part of Mexican immigrant health care today. Studies estimate that 45% to 65% of Mexican immigrant families use this traditional healing model (Dinallo et al., 2017; Ho et al., 2015; Lopez, 2014). Mexican American participants who seek this treatment identify the differing healing approach of MTM as an important part of their treatment (Lopez, 2014; Luquis & Castillo, 2016; Valdez, 2014). MTM can serve as both a standalone medical system or as complimentary therapy of traditional and complementary medicine (T&CM) practices integrated with Western medicine. Health services that validate a person’s culture and health beliefs are empowering to minorities and can improve care and treatment outcomes. This article provides evidence to support MTM as an emerging whole medical system as classified by the NCCIH (formerly known as the National Center for Complementary and Alternative Medicine, NCCAM) that, given its widespread influence among Latinos of Mexican descent and Western medicine’s increasing tendency toward holistic health care, has significant potential to address disparities in health care access among Latinos. The use of culturally accepted and clinically evidenced T&CM practices could be an effective method to increase Latino utilization of opioid use treatment methods and to decrease stigma for treatment engagement in other substance use treatments.
Practice Model: MTM as an Emerging Whole Medical System With Practice Evidence in Traditional and Complementary Medicine
Whole medical systems are characterized as “complete systems of theory and practice that have evolved independently over time in different cultures and apart from conventional medicine or Western medicine” (Baars & Hamre, 2017, p. 1). Inherent in these systems are presentations and symptom definitions, diagnostic methods and criteria, interventions, and outcome evaluation. Additionally, whole medical systems are based on a theoretical framework situated deep within a particular cultural context. Whole medical systems focus not only on a person’s symptoms and individualized treatment, but also see the whole person. As a result, whole medical system treatment models also address also mood, lifestyle, exercise, and emphasize balance among these areas within an individual’s cultural framework. As Western medicine works to provide more culturally sensitive care to patients, the terminology used to discuss traditional healing systems continues to evolve. This next section will explain how these approaches have changed in the past two decades as well as how MTM as a holistic system and T&CM as particular treatment practices of MTM, fit into the current model.
Whole medical systems are characterized by a complex range of healing modalities including nutrition, herbal products, physical movement activities, and mental/spiritual activities (Fischer et al., 2014; NCCIH, 2017). Specifically, they include approaches to health care in which practitioners apply bodies of knowledge and associated practices in order to maximize the patient’s capacity to achieve mental and physical balance to restore [their] own health, using individualized, non-reductionist approaches for diagnosis and treatment. (Ritenbaugh et al., 2003, p. 32)
By definition, the patient–practitioner relationship, a therapeutic environment, and interaction form an integral part of the healing process over the course of treatment in whole medical systems (Baars & Hamre, 2017).
More recently, as NCCAM shifted to NCCIH, the focus on traditional and indigenous practices has shifted from the study of the whole medical system in practice to the incorporation of particular evidence-based practices with traditional Western medicine (Hoogasian & Lijtmaer, 2010; Xu & Chen, 2011). This has led to changes and additions to the nomenclature of complementary practices and medicines. Current terminology includes T&CM, traditional, complementary and alternative medicine (TCAM), and traditional, complementary, and integrative medicine (TCIM). Because T&CM is used consistently by the World Health Organization in the publication Traditional Medicine Strategy: 2014-2023 as their wording of choice, this article also uses T&CM practices to refer to applications of MTM, while reserving the term whole medical system to refer to the NCCIH classification. This article also prefers the T&CM terminology because it best reflects the topic of this article: How evidence-based practices from MTM can be incorporated into Western medicine for opioid treatment (Burton et al., 2015).
Mexican Traditional Medicine: Overview of the Whole Medical System
MTM is an indigenous whole health system developed in Mexico. Its roots can be traced to pre-Colombian Aztec, Mayan, and Incan healing traditions, coupled with African and Spanish-Catholic influences (Maduro, 1983). MTM, like many indigenous healing systems, uses the principle of physical, emotional, and psychic balance manifested in the body. MTM also utilizes therapeutic healers to treat ailments (Figure 1). These healers exist in a number of categories, ranging from healers available for familial consultation at the lower end to societal specialists at the upper end.
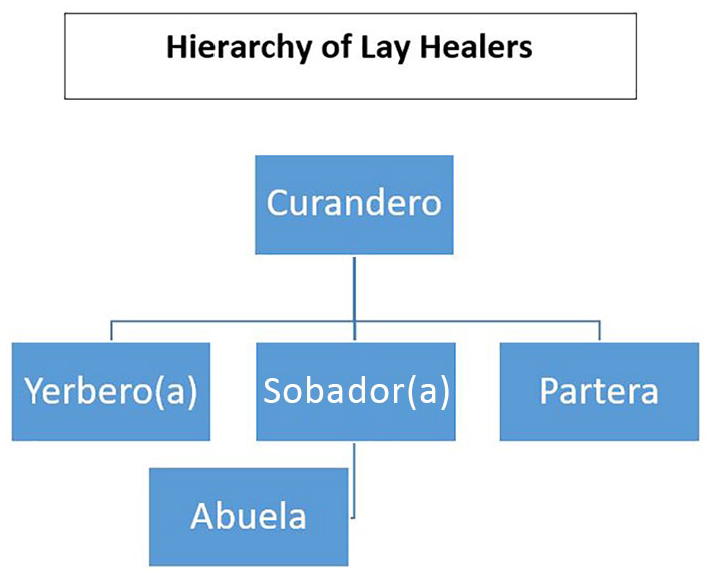
Hierarchy of Lay Healers.
At the lower level of familial consultation is the Señora/abuela or learned grandmother/female elder of the community. She is typically consulted initially for matters of the household, common illnesses, and marital/childrearing advice. Abuelas function as a cultural broker to treatment and MTM health services and often are the first step a person takes to seek help for a health condition. In some ways, abuelas are similar to a peer counselor, but also bring notable recognition, respect, and acceptance in the community. They provide a cultural link that decreases stigma and increases engagement for the client, provide knowledge-based information on a topic or issue based on traditional values and treatments, and in the United States, also serve as a bridge to the use of other more traditional Western medical services (Galvez & Silva, 2010).
In addition, the use of abuelas and similar cultural peer services has been documented for several decades as a fundamental part of substance use treatment. Interviews with Latino women specifically mention how abuelas served as counselors, referral agents, and sometimes as translators as they provided an entry point to medical services that resulted in increased access and utilization of substance use treatment (Trepper et al., 1997). Individual and particularly family interventions using an abuela as a peer counselor for a client and the client’s family were shown to increase involvement in rehabilitation treatment and outcomes in sobriety. The study noted that the abuela’s function paralleled the traditional Western arrangement in which people are encouraged to follow “older grandmother advice” as part of the treatment process (Engstrom, 2008).
Health lay workers, or promotores de salud, function at a level of support worker. They are not necessarily a peer, but have training in health care issues, basic assessment, and serve as an additional link between the Latino community and Western health care and mental health centers (Stacciarini et al., 2012; WestRasmus et al., 2012). Mental health promotores serve as additional cultural brokers with more advanced training in mental health assessment, mental health first aid, substance use assessment, brief intervention and referrals to treatment (SBIRT), and motivational interviewing to encourage help-seeking services for minorities with traditionally decreased access to care (Baars & Hamre, 2017; Barnett et al., 2018). This care provider serves as an additional bridge to services, provides educational presentations in the community, and decreases the anxiety typically reported in the initial help-seeking process by Latinos (Stacciarini et al., 2012).
The next level of practitioners involves a number of practitioner specialists in different areas. The most common medical intervention involves consultation with herbal medicine specialists, known as herbolaria or yerbero/a). Yerberos use different herbal remedies, alone or in combination, in much the same way as practitioners do in Chinese herbal medicine (Neff, 2002). More than 2,000 herbal preparations are included as part of herbolaria (Tafur et al., 2009). Here also, yerberos can also play a role in addressing substance abuse issues. Many of the herbals used in MTM have been studied for substance use treatment properties, including the anxiolytic effects of Passiflora in weaning from benzodiazepines or opioid reversal use (Akhondzadeh et al., 2001; Dhawan, 2003).
Sobadores are a second type of specialist. Specifically, sobadores are lay healers who use muscular manipulation and massage with a focus on body pressure points and muscle/tendon connections. This form of healing functions similar to the work done by chiropractors or acupuncturists (Martinez, 2009). Sobadores place importance on direct manipulation of the body and provide whole body massage (Figure 2) for ailments, including muscle soreness, tension, and general aches (Graham et al., 2016). A person would seek a sobadora for physical pain, muscle, or joint issues such as back pain or strains. The work of sobadores has been studied as part of holistic treatment models for chronic pain, particularly for Latino patients (Hinojosa, 2008; Mielenz et al., 2016). A recent study illustrated how Western medicine could align with sobadores to provide appropriate treatment of chronic pain while limiting the risk of opioid addiction (Sandberg et al., 2018).

Nursing Students at the Autonomous University of the State of Morelos (UAEM) Are Learning the Mexican Traditional Medicine (MTM) Massage Technique for “Angina Tronada,” 2019.
A partera is another kind of MTM specialist. Parteras function as traditional midwives who participate in the birthing of a child, but their role is not limited to medical attendance and assistance with birth (Maduro, 1983). The partera also uses herbal treatments, massages, and other treatments to aid the woman through the pregnancy, labor, and delivery.
Occupying the highest level of MTM practice is the curandero or curandera. The curandero’s overall goal is to assist in the recovery of the participant by restoring balance and order, thereby preserving the participant, family, community, and culture (Neff, 2002). The curandero, with extensive knowledge about the treatment of mental and physical ailments, uses herbs and plants, prayers, chants, and rituals to rebalance an individual’s physical, emotional, and spiritual realms.
Interactions with the curandero are unique and involve the use of narrative descriptions of health and illness (Tafur et al., 2009). The initial consultation begins as the platica or initial assessment session, when the participant seeks consultation. The platica session allows the curandero to review symptoms, discuss a person’s history and beliefs about healing and spiritual change, and to describe lessons learned from the illness experience (Valdez, 2014). This narrative, story-gathering format enables the curandero to see which areas of the person’s life are out of balance through a process termed an “opening of the many biological, psychological, and spiritual doors” or the 13 doors technique (Hoogasian & Lijtmaer, 2010; Kennedy et al., 2016). For example, if a patient were to seek a curandera for lingering symptoms as a result of a scorpion sting, the platica will include a discussion of the types of issues the sting has caused and how best to start the curar, or treatment (Neff, 2002). From information gathered from the platica, the curandero prepares individualized treatment regimens for the participant, including use of humor, spiritual rituals, herbal medicines, cleansings (limpias), and ritual ceremonies (Figure 3).

Autonomous University of the State of Morelos (UAEM) Nursing Students Learn the Mexican Traditional Medicine (MTM) Massage Technique “Entonación,” 2017.
Certification and/or licensure, developed to set a standard of practice and serve as a safeguard for providers and clients, has been an ongoing discussion with regard to traditional medicine and its use in Western medicine. For example, the National Indigenous Institute maintains training and certification standards in Mexico for MTM practitioners and programs, and many U.S. providers have received training in these programs in Mexico (Vogt, 1997). However, no such direct registry exists in the United States where it might serve as a form of certification or licensure (World Health Organization, 2001). Meanwhile, some MTM practices have certification and licensure of the particular practices involved, such as acupuncture, herbal medicine, and massage therapy, and many MTM providers hold certifications those specific MTM practices. Likewise, some curanderos have received education and certification as Naturopathic Physicians or other types of alternative care providers, which allows a level of practice consistency and some potential for credentialing and reimbursement for practices and procedures (Cohen & Nelson, 2011). Certification generally occurs at the higher levels of MTM practice, and some herbalists and sobradores have completed education and certifications complementary to their practicing fields in the past 20 years.
MTM: Theories of Health and Illness
MTM also includes theories of hot and cold, similar to those found in other theories of illness such as traditional Chinese medicine (TCM). Harwood first discussed hot and cold in aspects of Latin American folk medicine in 1971 when studying Puerto Rican folk healing. The overall premise of hot–cold or humoral medicine is based on “avoiding extremes” and “the selective use of opposites” (Harwood, 1971). The body maintains a state of health or equilibrium by balancing hot–cold forces. The hot–cold balance moves beyond merely taste or temperature, instead “connot[ing] an intrinsic property thought to be found in or associated with most natural substances, particularly foods and medicinal agents, as well as with states of illness” (Logan, 1977, p. 88). Body imbalances of hot–cold are believed to cause illness in humans, with treatment focused on restoring balance (Logan, 1977). In MTM, illnesses believed to be caused by excessive cold include arthritis, common indigestion, constipation, menstrual pain, and stomachache. These “cold” illnesses would be treated with “hot” foods, for example, chocolate, allium plants, ginger, or chilies (Linares et al., 2005). Illnesses from excess heat include diarrhea, fever, muscle spasm, pregnancy, rash/hives, and ulcers (Ortiz et al., 2007). If the curandero identifies excess heat as the cause of illness during the platica, cold treatments (plants, herbs, cheeses, etc.) to rebalance the energy would be used (Neff, 2002). If excess earth elements are identified as problematic, preparations of air and water treatments (which the participant ingests/bathes in) are used to restore balance. In addition, herbal remedies, such as baths in creosote tea (a natural sapofonic used in Mexican cleansings) and sage (a neural, spirit cleanser) are used for cleansing in an attempt to regain balance in the patient’s physical, emotional, and spiritual realms (Harwood, 1971).
As changes occur with treatment, the person reestablishes balance in a dynamic, changing course. Ongoing treatments with additional remedies focus on altering the status of the person to invoke additional change at different levels of healing. As the person arrives at a new state of healing, the balances between hot/cold, light/dark, and self/others regain equilibrium to manifest a healthier overall state (Logan, 1977). Treatments continue as needed, with differing limpias, chants, herbal use, and other treatments prescribed by the curandera. Notably, improvements in spiritual health would likely occur before changes in other areas of health. The pace and duration of the healing process is highly individualized as participants seek equilibrium of their physical, emotional, spiritual, and social systems (Ortiz et al., 2007). This holistic approach is designed to repair the body, soul, and spirit of the participant by perturbing the bodily forces (body, soul, and spirit) to move toward a different state of balance or equilibrium (Martinez, 2009).
MTM: A Nonlinear Dynamical System of Healing
To better understand MTM as a whole medical system, it is important to understand the science of nonlinear dynamical systems (NDS). NDS science relies on an evolving perspective used to explain and understand treatment resolution in alternative and complementary health care such as TCM. The system maintains that change is not only unidirectional, but also multidirectional and dynamic (Higgins, 2002). NDS is defined as “a system consisting of an extremely large and variable number of component parts, where the individual components display marked variability over time, and are characterized by a high degree of connectivity or interdependence between variables” (Higgins, 2002, p. 248).
NDS principles allow for a more thorough integration of the sciences and a better understanding of how physical, social, and metaphysical sciences can interact and be interdependent (Pincus et al., 2017). Through NDS, change can occur continually over time (Guastello & Gregson, 2016) as a person interacts with the outside world. The NDS process differs from a concept of change as a linear progression from beginning to end, and instead takes into account other factors that may impact the system during transformation (Higgins, 2002). Although Western medicine focuses on the process of reductionism, seeing the cure or resolution of illness as the only notable goal (Ahn et al., 2006), the NDS approach, with its emphasis on nonlinear change, forms the basis of complementary and alternative medicine practice. Nonlinear change allows for multiple areas of growth, alteration in the person and their experience, a step-back to make two steps forward, and the overall holistic improvement of the person and their quality of life as the goal, not just a cure.
The NDS model of change also provides a meta-theoretical explanation of MTM. MTM strives for systems balance to maintain optimal health. Imbalances are treated with a variety of strategies, including spiritual rituals, herbal medicines, chants, limpias, prayers, and massage as a way to “perturb” the body to move toward a different state (Valdez, 2014). Change occurs in either direction along the healing trajectory (“cure” or “wellness”) and is acknowledged as a dynamic state in both traditional and Western medicine. Western medicine, however, maintains that “cure” or “absence of illness” is the treatment goal (Guastello & Gregson, 2016). MTM seeks the holistic healing and wellness of the individual. In contrast to Western medicine, MTM’s goal is a “re-establishing of balance,” and hinges on the notion that a level of “wellness” entails more than just the “absence of disease” (Luquis & Castillo, 2016). This belief in wellness as a higher level of being is consistent with whole person healing methods (Salazar & Levin, 2013). The use of nonlinear systems in MTM explains the changes that occur within the individual and that move them from a state of imbalance to balance (Neff, 2002).
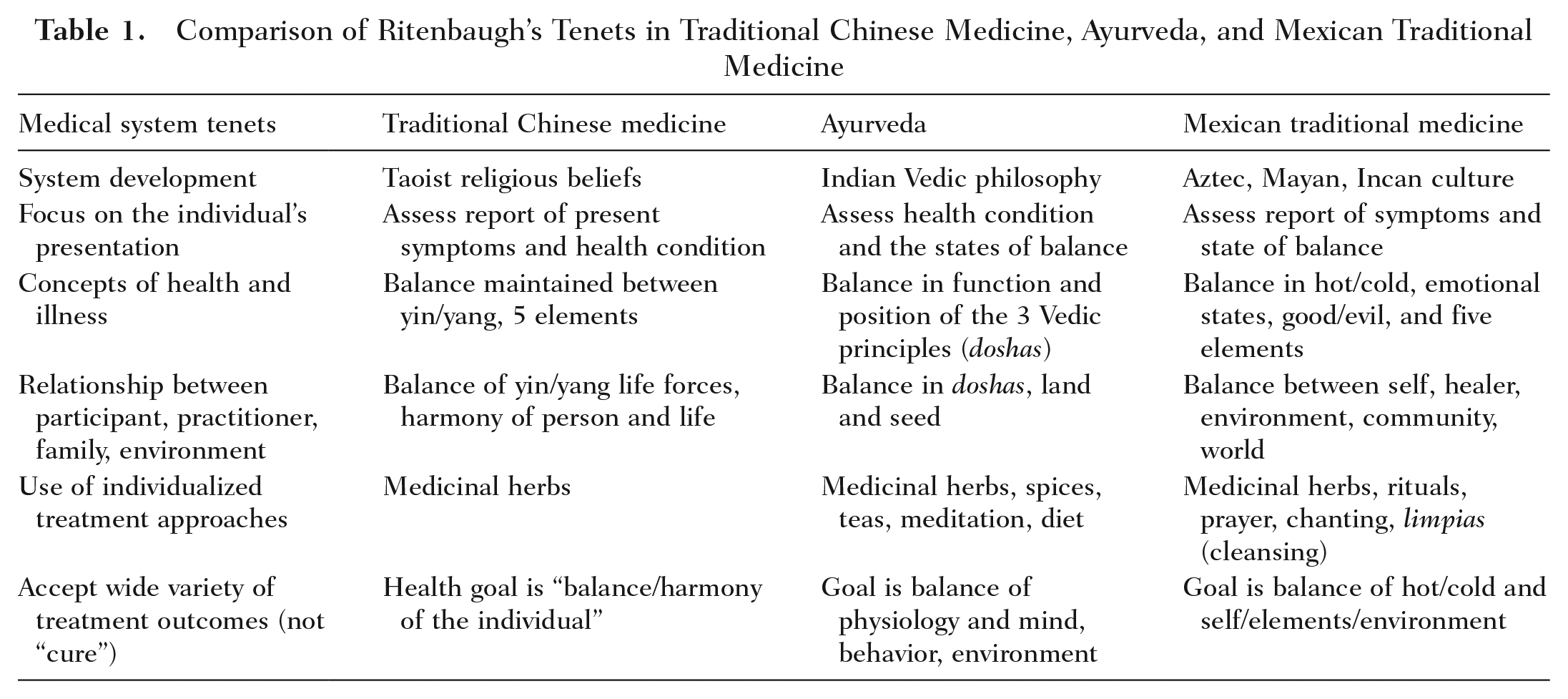
The influence of NDS thinking also helps to clarify how MTM is a T&CM distinct from Western medicine, rather than an additive set of techniques. Although Western medicine focuses on the process of reductionism (Verhoef et al., 2005), the NDS approach emphasizes nonlinear change as the basis of complementary and alternative medicine practice. The nonlinear approach to health care change and the MTM approach are delineated in Table 1 (Guastello & Gregson, 2016; Higgins, 2002; Pincus et al., 2017; Ritenbaugh et al., 2003). The nonlinear approach comprises five elements of change: attractor, chaos, perturbance/entropy, perturber, and fractals (Kirshbaum, 1998). The attractor is the area in which change takes place. For MTM, this is the participant. Chaos represents the uncontrollable life situations or activities that pertain to the attractor/participant. Perturbance is the amount of change over time in the person or system. The perturber facilitates change, and for MTM, this is represented by the curandero. Fractals are the minute, nonlinear dimensions of change that occur in the participant’s path of life as they move toward a new equilibrium. MTM addresses each of these elements in its approach to healing (Kirshbaum, 1998).
Comparison of Ritenbaugh’s Tenets in Traditional Chinese Medicine, Ayurveda, and Mexican Traditional Medicine
MTM and NCCIH Requirements for a Whole Medical System
MTM meets both the terminology and requirements that NCCIH outlines as necessary for a whole medical system. The NCCIH tenants include system development (philosophical or religious basis); a focus on a participant’s presentation; defined concepts of health and illness; defined relationships between participants, practitioners, family, and environment; use of individualized treatment approaches; and acceptance of a wide variety of treatment outcomes rather than a focus simply on a cure. To assess the validity of a healing tradition for inclusion as a whole medical system, NCCIH would review theoretical and evidenced-based data submitted on a particular type of therapeutic practice to assess the validity of the data for inclusion. The data are largely provided by anthropologists, who observe the utilization of these therapies and supply data regarding the healing tradition’s system development, patient presentation, concepts of health and illness, and nonlinear trajectories of treatments. To date, NCCIH has classified four other systems as whole health medical systems: TCM, Ayurveda, homeopathy, and naturopathy. Other traditional healing systems that might also meet NCCIH whole medical system standards include variations of American Indian, African, and South American healing traditions (Baars & Hamre, 2017). Table 1 outlines these NCCIH tenets and compares MTM to two other NDS-based traditional systems: TCM and Ayurveda (Kim et al., 2011; Loera et al., 2009; Lopez, 2014; Luquis & Castillo, 2016; Maduro, 1983; Martinez, 2009; Park et al., 2012).
As noted in Table 1, TCM is based on Taoist religious beliefs, Ayurvedic medicine is based on Indian vedic philosophy, and MTM is based on Aztec, Mayan, and Incan cultural beliefs, incorprating not only Mexican but much of Central American variations of traditional medicine. Likewise, MTM’s focus on an individual’s symptom presentation and on providing individualized treatments meets the same NCCIH criteria as TCM and Ayurveda. In addition, MTM focuses on the concept of maintaining balance as the backbone of health and prevention of illness, just as the other NCCIH-classified whole medical systems do (Kleinman, 1978; Luquis & Castillo, 2016; Park et al., 2012).
While the older NCCAM terminology focused more on whole medical systems as unique wholes, the newer NCCIH terminology has focused on how T&CM practices from whole medical systems can be successfully incorporated into traditional Western medicine to improve outcomes in health care using evidenced-based assessment methods (Ijaz et al., 2019). Likewise, the focus of NCCIH is moving away from the complete utilization of a whole medical system apart from Western medicine to researching which aspects of these whole medical systems have clinically based evidence for their use and incorporation into Western medical treatments. As a result, the evidence-based nature of T&CM becomes the focus in patient-centered medicine. It also strengthens the argument for the inclusion and integration of MTM practices into health care practices for a particular illness or ailment as clinical evidence of improved outcomes is demonstrated by research (Xu & Chen, 2011).
MTM is also consistent with whole medical system principles delineated by Ritenbaugh et al. (2003). Ritenbaugh et al. defined a whole system of healing as “an approach in which practitioners apply bodies of knowledge and associated practices in order to maximize the patient’s capacity to achieve mental and physical balance and restore their own health, using individualized, non-reductionist approaches to diagnosis and treatment” (Ritenbaugh et al., 2003, p. 32). Using this foundation, T&CM interventions focus on helping patients to learn individualized new behaviors and fostering experiences and lifestyle approaches that promote disease prevention as well as healing (Ijaz et al., 2019). Review and assessment of whole medical systems include integrating a “whole person assessment of a patient’s physical, mental, emotional, and psychosocial wellbeing,” with a focus on patient preferences, priorities, and values in their treatment design (Ijaz et al., 2019, p. S22). The approach outlined by Ijaz et al. includes evaluating the healing traditions a conceptual model, diagnostic methods, and the treatment modes specific to each system as delineated in Ritenbaugh et al. Utilizing the principles discussed above as a guide, MTM meets the classifications and should be considered a whole medical system to provide more culturally sensitive and appropriate health care to Latino populations in the United States (see Table 1).
Application of MTM to Address Latino Health Disparities
Research studies consistently show a continued disparity in Latino access to allopathic healthcare services, in addition to low utilization rates and poor satisfaction (Betancourt et al., 2003; Vega et al., 2009). Satcher’s 1998 hallmark Surgeon General Report started the national discussion of health care disparities for minorities, including Latinos (McMorrow et al., 2015; Sondik et al., 2010; U.S. Department of Health and Human Services, 1998). Further studies showed the underutilization of health care services by Latinos, with a national study by the Centers for Disease Control and Prevention that posited that Latinos experience a disproportionate amount of disease, injury, death, and disability when compared with non-Latino Anglos. Latinos experienced increased incidence of chronic disease and trailed in the leading indicators of good health based on the national objectives of 2010 (Beckie, 2012; Chen et al., 2016; McMorrow et al., 2015). Bastida, Brown, and Pagán noted continued decreased Latino utilization of health care services, reporting issues with health insurance coverage, access to care in the community, and preferences for culturally based medical care as factors related to the decreased utilization of services (Bastida et al., 2008). Although there has been noted improvement since the advent of the Affordable Care Act, disparities remain for Latinos across all monitoring areas and types. Disparities in health care utilization persisted despite controlling for the variable of age, poverty, and health insurance coverage (Chen et al., 2016; McMorrow et al., 2015). These inequalities remain salient issues for Latinos particularly when it comes to culturally sensitive and effective opioid treatment (Vega et al., 2009).
T&CM Practices to address Latino Stigma and Treatment Engagement
When assessing mental health and substance use access and utilization of treatment, Latinos continue to show disparate service utilization. Latinos reports rates of mental illness incidence at 30% of their population, higher than the 20% of Caucasian U.S. residents (Alegría et al., 2007), and this disparity increases with substance use issues. However, only 20% of Latinos who report mental health or substance use issues also report utilizing available substance use treatments services (Guerrero et al., 2013; Mulvaney-Day et al., 2012). Mental health research has shown that including culturally relevant elements in treatment increases Latino utilization and satisfaction in mental health services (Rastogi et al., 2012; Villatoro et al., 2014). Likewise, incorporating similar culturally relevant treatment services in substance use treatment may increase service utilization and decrease stigma issues notably present in Latino access to mental health and substance use treatment.
In contrast, the use of T&CM practices by Latinos varied from 50% to 90% lifetime use (Ho et al., 2015). Of those, the majority of subjects utilize herbal medicines or remedies and integrative medicine providers, including herbalists, sobadors, and other MTM providers (Arcury et al., 2019; Dinallo et al., 2017; Sorrell, 2013). In the past several years, more research has been done regarding how providers can effectively incorporate integrative medicine and culturally related care to improve outcomes, but the literature remains sparse, with research focusing on specific herbals or curanderismo techniques (Favazza Titus, 2014; Holden et al., 2014; Hoogasian & Lijtmaer, 2010; Tran et al., 2014; Valdez, 2014). These articles show a consistent pattern of increased health care utilization, satisfaction, and treatment outcomes success with the incorporation of these types of treatments for Latinos. Although there clearly is increased utilization of integrative care practices by Latinos and studies documenting the clinical efficacy of MTM practices, MTM lacks official recognition as a whole medical system that would substantiate its incorporation into Western medical care particularly for Latino patients. Acknowledging and effectively incorporating MTM practices—for example, utilization of herbal medicines for anxiolytic treatment in opioid withdrawal, sobadores for chronic pain, and additional T&CM modalities with evidenced-based validation—could facilitate increased health care utilization and minimize health care disparities. Validating MTM as a whole medical system would pave the way for additional research to better understand how MTM integrative treatments could improve patient outcomes for opioid use, mental health issues, and additional issues.
Applying MTM Practices as a Holistic Approach to Opioid Treatment
Healthy People 2020’s (Office of Disease Prevention and Health Promotion, 2018) goals include improving access to culturally appropriate services for minority groups and eliminating health care disparities for vulnerable groups (Maduro, 1983). Disparities research shows Latinos are less likely to have access to appropriate health care services than any other minority group (Martinez, 2009). A focus on culturally congruent health care and access for those living in the United States serves as a key feature in improving health care access, utilization, and satisfaction (Ortiz et al., 2007). Specifically, incorporating treatments based in MTM as part of patient-centered opioid treatment for persons of Latino heritage could increase health care participation for this group (Maduro, 1983).
Substance use treatments incorporating MTM practices from a foundational level could include the utilization of an abuela or similar lay health advisor as an entry point to decrease barriers for those seeking treatment at a substance use treatment center (Ayala et al., 2010). Passiflora could be used as an anxiolytic to mediate withdrawal symptoms and cravings when clients begin medication assisted treatments (MAT) such as suboxone (Patkar et al., 2013). MTM integrations could also include the use of Latino-based acupuncture during Suboxone/Methadone induction (Sobralske et al., 2012). Curanderos could consult with patients at the rehabilitation center and help promote sobriety from a bio–psycho social–spiritual perspective (Kennedy et al., 2016; Ortiz & Torres, 2007). Sobadores could be incorporated into chronic pain programs for culturally appropriate massages and muscle manipulation to address chronic pain without opioid use. In addition, sobadores massages and muscle manipulation could decrease anxiety in those initiating and continuing in MAT services. Such prevention is important because anxiety is a known trigger in substance abuse relapses (Hinojosa, 2008; Villalobos, 2016). In summary, treating more persons of Latino heritage successfully for opioid use and other health care issues could decrease the economic losses that result from illness. Continued research into and incorporation of MTM practices for the Latino community will be necessary to adequately address the health care needs of this population (Valdez et al., 2018).
A Case Example of MTM for Opioid Use Disorder
This case example shows how MTM practices might be incorporated with a holistic approach to nursing that is more culturally sensitive. Oswaldo is a 45-year-old married Latino male who presents for referral. He reports he spoke with one of our abuelas at his local church who encouraged him to meet with us for an assessment regarding his prescription painkiller and heroin use. Doña Elisa, a local abuela and Sra. Alma, a mental health promotora, who has had SBIRT and Mental Health First Aid training with our facility (Ramos et al., 2018), attends his first substance assessment appointment, then sits with the psychiatric nurse practitioner, client, and the family as opioid use disorder and treatment options are explained to the client. A decision to start MAT is made using a family-based decision-making approach (Carman et al., 2013; Villatoro et al., 2014). As part of the work-up for physical health and mental health issues, Oswaldo meets with our curandera, who assesses the client using the MTM 13 doors technique and then develops a plan to assist in treatment with appointments, massages (massajes), and spirit/energy activities to help the lower back pain from a work injury that initiated the prescription opioid use and subsequent heroin addiction (Hoogasian & Lijtmaer, 2010; Kennedy et al., 2016; Ortiz & Torres, 2007).
The abuela and/or promotora meet with Oswaldo’s family at their home to review the MAT induction process and assist the nurse in reviewing questions about the treatment process. The abuela and/or promotora also attend the induction appointment with the client and assist the client and family with understanding the need for non-use prior to induction, as this is a critical time in the MAT process (Ornelas et al., 2015). Because the time between the initial assessment and Suboxone induction is a common dropout time for those seeking services, this additional contact can facilitate adherence to treatment and decrease dropout (Cucciare et al., 2015). An MTM variant of auricular acupuncture is used by our nurses as part of MAT induction with suboxone, and the client is instructed that he can use up to 400 mg of the Passiflora herbal preparation from a botanica for anxiety related to induction and the sobriety process (Akhondzadeh et al., 2001; Appel et al., 2011). The client participates in individual and group therapy for substance use, as well as appointments with the curandera and ongoing family interaction from the promotora to encourage and support the client and answer questions that can lead to stigma in treatment (Meza, 2013; Valdez et al., 2018). Because of the integrative care and support of prescribers, nurses, and MTM providers, Oswaldo is able to increase his days of sobriety from opioids, continue his engagement with his work and family, and as with other culturally based substance use treatment methods such as those that combine American Indian cultural practices with traditional Western treatments, increase the rates of continuance for minorities in substance use treatment (Saloner & Cook, 2013). Successfully addressing Oswaldo’s opioid use disorder with T&CM practices that embrace cultural competency increases the likelihood of his engagement in services, utilization of resources for increased days without use, and improves his treatment outcomes (Dickerson et al., 2016; Guerrero et al., 2013). The holistic aspects of MTM practices and nursing are utilized hand in hand to improve outcomes in opioid use disorder MAT treatments (Figure 4).
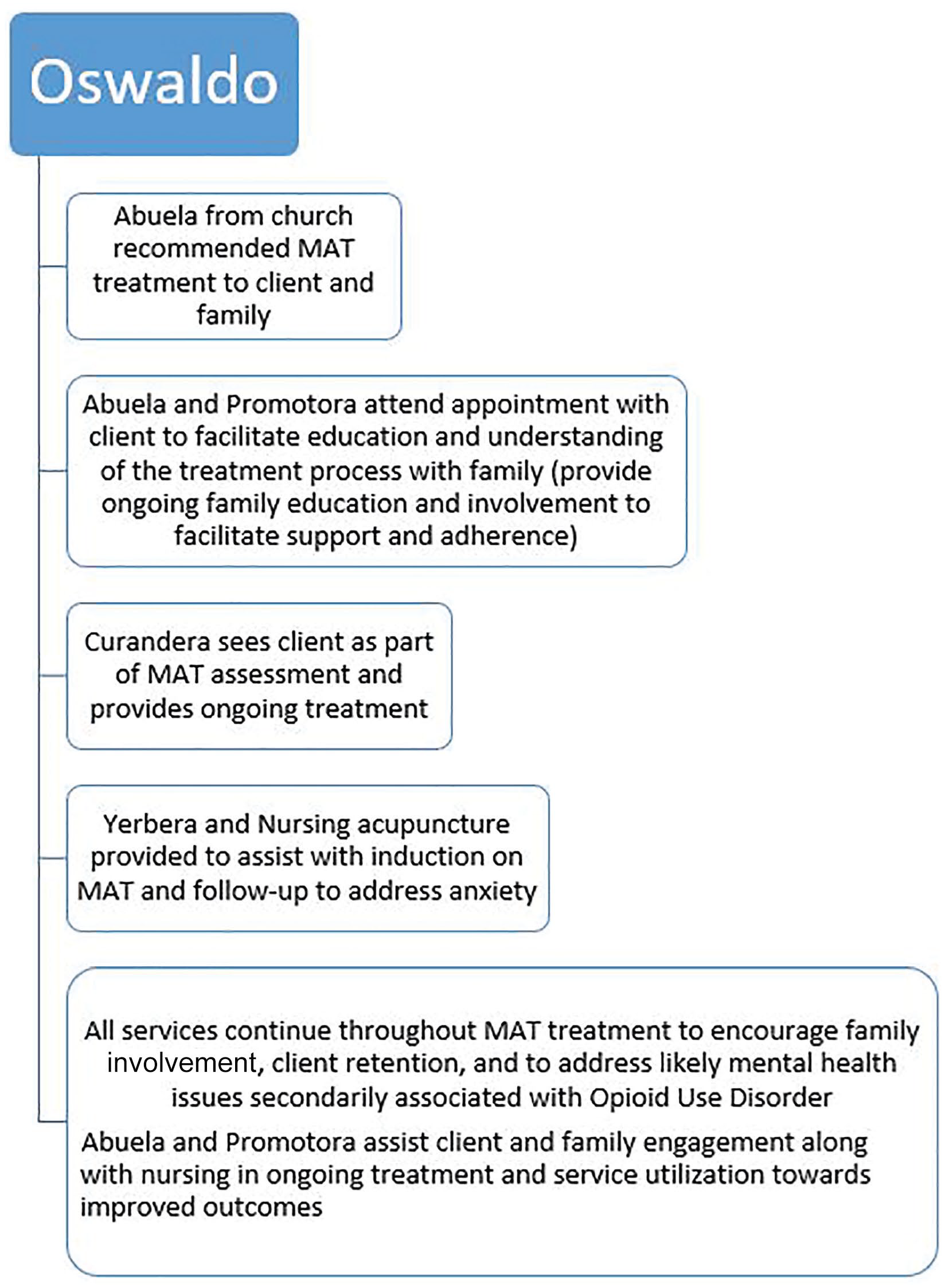
Mexican Traditional Medicine and Nursing Holistic Treatment Approaches.
Conclusion
Given the similarities of MTM with TCM and Ayurveda in principle, application, and etiological theory, MTM should be adopted as a whole medical system and its practices incorporated as T&CM practices by the NCCIH. MTM is used by a majority of Latinos in the United States and elsewhere. Integrating MTM with the Western medical system would serve this population as an entry point into the U.S. health care system, validate Latino culture, and provide an opportunity to address health disparities.
In addition, recognition of MTM as a whole medical system would provide the recognition that MTM providers need to provide optimal care to their patients. MTM providers need to be informed about the type of care individuals may be receiving through Western practitioners, and likewise, Western practitioners need to be informed about the MTM care their patients are receiving as happens with providers of recognized systems like TCM. NCCIH recognition would provide that visibility. Official NCCIH recognition would also encourage research to foster a better understanding of the principles of MTM and how the evidence-based practices currently used—as well as other potential T&CM practices—could be integrated to improve care for Latinos with opioid use disorder. Likewise, the NCCIH designation would encourage more research overall regarding the uses and benefits of MTM and T&CM practices to educate patients and providers alike to address the particular aspects of the Latino opioid crisis.
Based on current guidelines, MTM should be classified as a whole medical system, with its T&CM practices of clinical value by NCCIH to provide more culturally sensitive and effective substance abuse treatment to the Latino population. The use of T&CM treatments to decrease anxiety and triggers in maintaining sobriety, decrease risks of relapse during the course of substance use treatments, and to address chronic pain issues that may precipitate substance misuse are only some of the methods that could more effectively address issues for Latinos. Increasing Latino utilization of and satisfaction with mental health and substance use treatments will address the noted disparities seen despite recent efforts to increase access to behavioral health and substance use care. With known entry points to decrease stigma and empower Latinos in seeking treatment that is familiar and aligned with their cultural ideas, traditions, and values, MTM can serve as a bridge to improving outcomes in opioid use disorder treatment for this group. To close the health care gap, additional research is needed about how MTM care and treatment can improve Latino health care outcomes when integrated with Western medicine. Only then will we be able to deliver more effective, culturally competent and sensitive health care provision for Mexican immigrants in the United States.
Supplemental Material
permiso_derechos_tanya_r_orrell-_English_translation – Supplemental material for Mexican Traditional Medicine: Application of a Traditional and Complementary Medicine System to Improve Opioid Use Treatment in Latinos
Supplemental material, permiso_derechos_tanya_r_orrell-_English_translation for Mexican Traditional Medicine: Application of a Traditional and Complementary Medicine System to Improve Opioid Use Treatment in Latinos by Tanya R. Sorrell in Journal of Holistic Nursing
Footnotes
Authors’ Note:
This study was partially funded by a grant from the American Nurses Association—Minority Fellowship Program. The author thanks Dr. Mary Koithan, PhD, for initial support in the development of this topic. I would also like to acknowledge to Dr. Mario Rojas Alba, Director general at TlahuiEdu AC, Cuernavaca, Morelos, Mexico who encouraged my ongoing exploration of MTM techniques for mental health/substance use treatment and provided the photos for the article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.