
Abstract
Background:
Stress resulting from intimate partner violence (IPV) on pregnant women causes and sustains poor health and contributes to poor pregnancy and birth outcomes. Appropriate interventions to reduce stress in this population of women are warranted.
Objective:
To present a systematic review and the state of the science of evidence on alternate nostril breathing (ANB) as a holistic intervention for stress reduction for pregnant survivors of IPV, framed by complex adaptive systems theory and psychoneuroimmunology.
Data Sources:
Eight databases and reference lists of potential articles.
Study Eligibility Criteria:
Randomized controlled trials published between January 2013 and July 2019.
Participants:
Adults.
Intervention:
ANB.
Study Appraisal and Synthesis Method:
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Results:
ANB is effective in reducing stress, as measured by psychological and biological indicators.
Limitations:
Studies were limited in ethnic and gender diversity, most of the populations being Asian Indian and predominately male.
Conclusions:
Use of ANB as a safe and effective holistic intervention for stress reduction shows promise, but research in pregnant survivors of IPV is limited.
Implications:
Stress reduction benefits may be significant for pregnant survivors of IPV and their fetuses, with minimal risk.
Nurses providing holistic care benefit from understanding how multiple factors (individual, environmental, societal, physiological, psychological) interact to cause illness and disease and play a role in enhancing health by promoting well-being (Daruna, 2012; Yan, 2012).
Slow yogic breathing interventions, such as alternate nostril breathing (ANB), have been useful in decreasing stress across a range of populations. ANB is an accessible, easy-to-perform, and safe controlled breathing exercise that has some support for safety and efficacy in a broad demographic of individuals (Chandla et al., 2013; Chen et al., 2017; Dabhade et al., 2012; Franzblau et al., 2008; Goyal et al., 2014; Joshi et al., 2016; Joshi et al., 2017; Ma et al., 2017; Naik et al., 2018; Perciavalle et al., 2017; Peterson et al., 2017; Seppala et al., 2014; Sharma et al., 2013; Sinha et al., 2013; Turankar et al., 2013; Twal et al., 2016; Van Diest et al., 2014).
ANB may be useful in reducing stress in women survivors of intimate partner violence (IPV). Examples of IPV include physical and/or sexual violence, psychological aggression, and stalking (Centers for Disease Control and Prevention [CDC], 2019b). One factor contributing to poor health outcomes in survivors of IPV is excessive stress (Taillieu et al., 2016; Van Parys et al., 2015). The literature is lacking in stress-reducing interventions for women survivors of IPV in general (Sabri & Gielen, 2019). IPV also is a serious problem affecting pregnant women and their fetuses, with general prevalence rates estimated at 2.2% (Pregnancy Risk Assessment Monitoring System, 2017). Even less is known about stress reduction in pregnant women suffering with IPV. This article presents the state of the science of ANB to reduce stress and a systematic review (SR) of the literature to provide evidence for ANB as a holistic stress reduction intervention for pregnant survivors of IPV.
Two theories that resonate with holistic nursing guided this inquiry: complex adaptive systems (CAS) theory and psychoneuroimmunology (PNI). CAS theory views the individual as a complex, whole system, irreducible to its parts, with the whole greater than the sum of its parts (Bell & Koithan, 2006; Bell et al., 2012; Koithan et al., 2012; Rickles et al., 2007). CAS theory focuses on the individual as a complex system interacting with other complex systems and the environment. Ultimately, this interaction affects the occurrence of illness or health (Bell & Koithan, 2006; Bell et al., 2012; Koithan et al., 2012; Rickles et al., 2007). PNI is useful for explaining how holistic body–mind interventions, such as ANB, result in complex interactions between multiple organ systems to improve health (Daruna, 2012; Yan, 2012). PNI provides a holistic context to describe (1) the impact of stress resulting from the experience of IPV on women, (2) the pathways by which IPV causes and sustains poor health and contributes to poor pregnancy and birth outcomes, (3) the effects of maternal stress on the fetus, and (4) the mechanisms of action of ANB.
ANB is a type of controlled breathing derived from yoga, a holistic body–mind practice that originated in India more than 3,500 years ago (Cameron, 2010; Carter & Carter, 2016; Gard et al., 2014; Sharma et al., 2013). Yogic breathing consists of regulating breathing using various fast or slow techniques (Cameron, 2010; Gard et al., 2014; Goyal et al., 2014; Naik et al., 2018; Peterson et al., 2017; Sharma et al., 2013; Twal et al., 2016; Van Diest et al., 2014). Every yogic breathing technique involves voluntary breathing and incorporates conscious use of the diaphragm (Chandla et al., 2013; Gard et al., 2014; Goyal et al., 2014; Joshi et al., 2016; Joshi et al., 2017; Peterson et al., 2017; Pramanik et al., 2009; Sharma et al., 2013; Sinha et al., 2013). Yogic breathing purportedly optimizes the stress response (Van Diest et al., 2014) and downregulates arousal (Gard et al., 2014). Owing to these characteristics, yogic breathing has been used to promote relaxation and reduce stress by enhancing parasympathetic nervous system (PNS) function (Brown et al., 2013; Turankar et al., 2013; Twal et al., 2016).
State of the Science
Stress and Its Impact on Pregnant Women
Pathways by Which IPV Causes and Sustains Poor Health
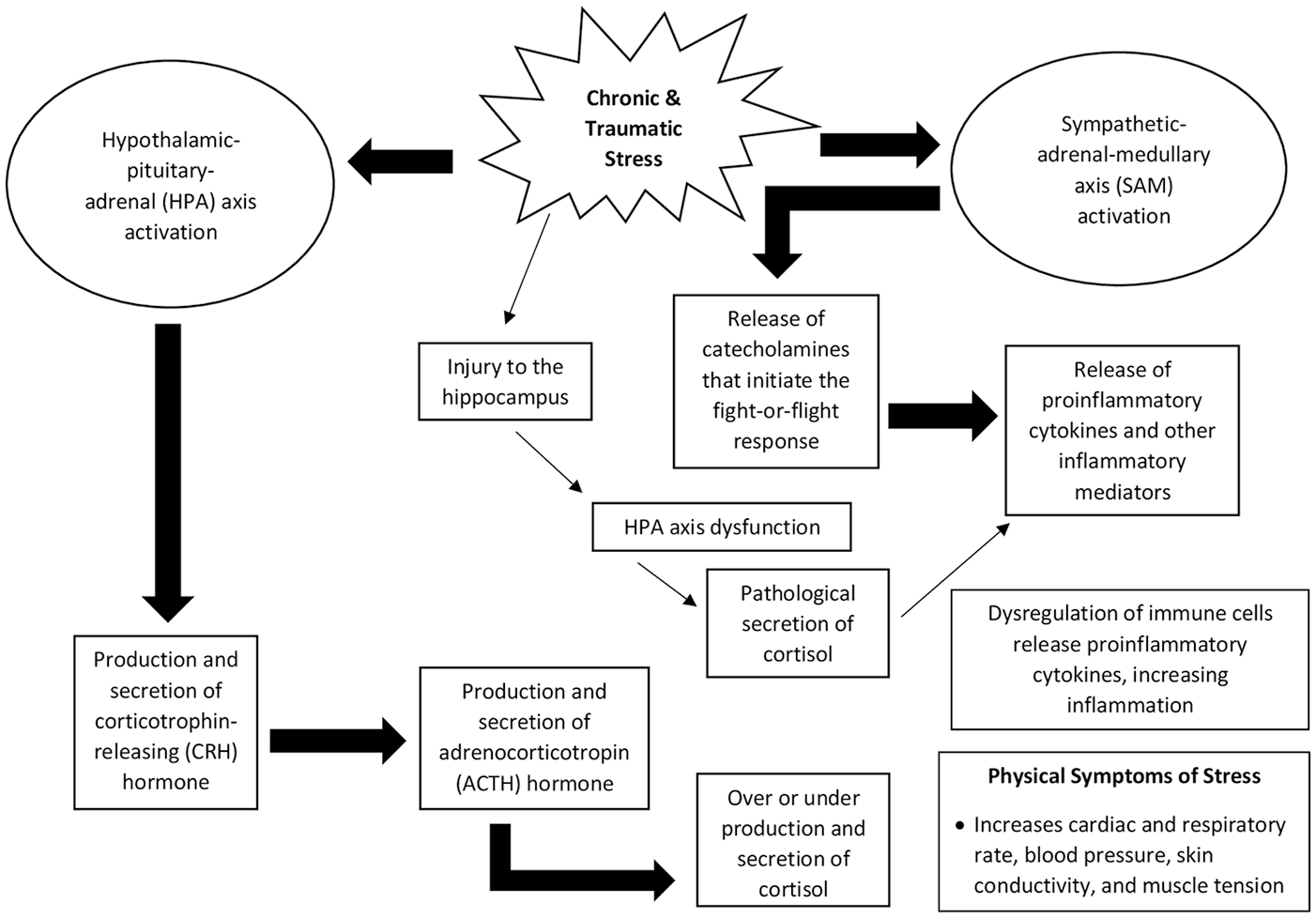
Numerous deleterious effects of traumatic stress on physical and emotional well-being have been identified through PNI (Bennett et al., 2013; Jaremka et al., 2013; Kendall-Tackett, 2009; Payne & Crane-Godreau, 2015). Composite interactions link the immune system to behavior and health outcomes (Bennett et al., 2013). Available evidence suggests that traumatic stress such as that resulting from IPV activates the immune and inflammatory systems, initiating responses that increase the concentrations of stress hormones and inflammatory mediators in the bloodstream (Bennett et al., 2013; Jaremka et al., 2013; Kendall-Tackett, 2009). Recurrent exposure to trauma conditions the immune and inflammatory systems to react to potential or impending stress-inducing incidents rapidly and persistently (Kendall-Tackett, 2009; Payne & Crane-Godreau, 2015). Elaborate interactions between the sympathetic and parasympathetic branches of the autonomic nervous system (ANS), the ANS and the immune system, and the cortical and subcortical regions of the brain initiate the stress response (Payne & Crane-Godreau, 2015). Evidence further suggests that chronic stress can injure the hippocampus, resulting in hypothalamic–pituitary–adrenal (HPA) axis dysfunction that results in pathological secretion of cortisol (Sapolsky et al., 1985). Persistently elevated cortisol concentrations can impair sensitivity of glucocorticoid receptors, resulting in dysregulation of immune cells that release pro-inflammatory cytokines, and thus increase inflammation (G. Miller et al., 2002; Webster et al., 2002). Chronic stress has been shown to increase release of the excitatory neurotransmitter glutamate within the amygdala, and this neuronal hyperactivity has been linked to depression, anxiety, and other stress-induced conditions (Zhang et al., 2019). Communication between the neurologic, immune, and endocrine systems is multidirectional, which generally permits a cohesive response between them (Maier & Watkins, 1998; Wrona, 2006). Yet the bidirectional communication between these systems also heightens risk for dysfunction to occur if one system is compromised (Bennett et al., 2013).
Several adverse health outcomes can result with abnormally elevated and chronic inflammation, including cardiovascular disease, type II diabetes, cancer (Bennett et al., 2013; Jaremka et al., 2013; Kendall-Tackett, 2009), neurodegenerative diseases (Bennett et al., 2013; Jaremka et al., 2013), gastrointestinal disorders, and chronic lung diseases (Kendall-Tackett, 2009). These adverse health outcomes are common in women exposed to IPV (CDC, 2019b; Chisholm et al., 2017; World Health Organization [WHO], 2017). Other common outcomes of IPV such as depression, anxiety, insomnia, smoking, and poor nutrition elevate inflammation (Bennett et al., 2013; Jaremka et al., 2013; Kendall-Tackett, 2009). Women exposed to IPV are often isolated from friends and family by their abusers; lack of social support is also linked to abnormal elevations in inflammation (Bennett et al., 2013; Jaremka et al., 2013; Kendall-Tackett, 2009). These stressors can interact, resulting in exponential increases in inflammation (Bennett et al., 2013; Jaremka et al., 2013).
Marital discord itself increases stress and depression in individuals, in part through psychoneuroimmunological mechanisms (Jaremka et al., 2013). Depression has been linked to amplification of the inflammatory response to acute stressors (A. H. Miller et al., 2009; Pace et al., 2006). It has also been suggested that the association between depression and inflammation is bidirectional: Depression increases inflammation, and inflammation fosters depression (A. H. Miller et al., 2009). Even physiological stressors such as giving birth are amplified in women who are depressed: Women diagnosed with major depression had higher concentrations of IL-6 (interleukin 6) postpartum than those who were not diagnosed with major depression (Maes et al., 2001). Depression is a common adverse psychological outcome in women exposed to IPV, especially during pregnancy (Brownridge et al., 2011; Chambliss, 2008; Van Parys et al., 2015).
Effects of Maternal Stress on the Fetus
Multiple studies have examined the effect of maternal prenatal psychosocial stress on the developing fetus and its implications for the health of offspring during their lifetime. Although the pathways by which maternal prenatal stress affects fetal development and health outcomes for offspring are multifactorial, complex, and not completely understood, these studies implicate the effect of the maternal physiological stress response (e.g., HPA axis function, stress hormones, and inflammatory mediators) on fetal growth and development, DNA, and/or HPA axis function (Blaze et al., 2017; DeSocio, 2018; Gilles et al., 2018; Huizink & de Rooij, 2018; Kuzawa et al., 2017; Murray et al., 2020; Rakers et al., 2020; Schepanski et al., 2018; Van den Bergh et al., 2018; Zucchi et al., 2013), which ultimately alters stress reactivity in offspring and increases their susceptibility to physical, psychological, and behavioral disorders (DeSocio, 2018; Huizink & de Rooij, 2018; Murray et al., 2020; Rakers et al., 2020; Zucchi et al., 2013). The synergistic interaction of maternal stress, mental illness, substance abuse, infection, poor maternal nutritional intake, inadequate maternal antenatal health care utilization, and poor maternal–fetal attachment is cited to lead to poor health outcomes in children whose mothers experienced prenatal IPV (Murray et al., 2020). The synergistic impact of these pathways must be considered when developing interventions for pregnant women experiencing stress, especially those who are survivors of IPV (Alhusen et al., 2015; Bailey, 2010; Chambliss, 2008; Taillieu et al., 2016; WHO, 2011). A holistic intervention such as ANB has the potential to address this synergistic impact more readily than traditional interventions alone (Carter & Carter, 2016; Daruna, 2012; Jerath et al., 2015; Yan, 2012), thus resulting in improved health outcomes for both mother and fetus. Pregnant women who are survivors of IPV have undoubtedly experienced toxic stress that threatens their health and the health of their fetuses. Development of feasible, portable interventions with demonstrated effectiveness to reduce their stress levels is warranted for improving their pregnancy and birth outcomes.
Mechanisms of Action of Alternate Nostril Breathing
ANB is believed to assist in balancing the sympathetic and parasympathetic branches of the ANS—particularly in mitigating the sympathetic nervous system (SNS) dominance associated with sustained stress (Peterson et al., 2017). Multiple studies have demonstrated the effects of ANB in enhancing PNS function, promoting relaxation, and reducing stress (Chandla et al., 2013; Goyal et al., 2014; Joshi et al., 2016; Naik et al., 2018; Peterson et al., 2017; Sharma et al., 2013; Sinha et al., 2013; Turankar et al., 2013; Twal et al., 2016).
Initiation of the stress response increases cardiac and respiratory rates, blood pressure, skin conductivity, and muscle tension (Jerath et al., 2015; see Figure 1). Various psychological states are known to influence the ANS and cardiorespiratory function (Kreibig, 2010). Negative or positive psychological states such as stress or calmness are believed to affect the ANS through SNS or PNS activity (Kop et al., 2011). Jerath et al. (2015) suggested that negative affective states stimulate the SNS. Stimulation of the PNS is suggested to result in universal inhibition and hyperpolarization (Jerath et al., 2015). Deep, slow breathing techniques such as ANB are proposed to stimulate the PNS, which increases synchronization of cardiorespiratory function, resulting in inhibition and hyperpolarization of cells in the amygdala and thalamus, and transference to PNS control (Jerath et al., 2012). Deep breathing techniques such as ANB have demonstrated effects in optimizing heart rate variability, a positive indicator of enhanced PNS functioning and improved stress response (Chandla et al., 2013; Van Diest et al., 2014). Additionally, the improvement in PNS activity through breathing techniques like ANB is presumed to target the stress response by increasing the action of the inhibitory neurotransmitter GABA (gamma amino-butyric acid) system within the brain, including through stimulation of the vagal nerves, and ultimately decreasing allostatic load (Brown et al., 2013; Streeter et al., 2012). Multiple outcomes of PNS stimulation also include effects on the HPA axis through its conduits to the hypothalamus, amygdala, and hippocampus, which facilitates an increase in GABA levels in the hippocampus and decreases cortisol concentrations (Brown et al., 2013). Stimulation of the vagal nerves through deep, diaphragmatic breathing may increase release of oxytocin, vasopressin, and prolactin—hormones believed to be associated with increasing emotions of love, bonding, and empathy, and improving feelings of general well-being (Brown et al., 2013).
Feedback Loops of the Stress Response
Respiration is the only autonomic function that is readily managed through voluntary control, and it can therefore be used to influence the PNS toward adaptive responses to stress (Streeter et al., 2012). Research suggests that body–mind interventions such as ANB may directly affect the subcortical brain and may be potentially more effective than conventional therapies in managing stress-related maladaptive behaviors (Jerath et al., 2015; Payne & Crane-Godreau, 2015). ANB assists in bringing the user to a state of calmness and relaxation by shifting focus from existing or potential challenges (Payne & Crane-Godreau, 2015). The concerted focus of the mind while practicing ANB may be the mechanism by which the mind and respiration interact (Carter & Carter, 2016; Goyal et al., 2014; Payne & Crane-Godreau, 2015; Sharma et al., 2013; Twal et al., 2016). A state of relaxation is induced through recursive feedback loops by decreasing excitability of muscle and other tissues, stimulating stretch receptors in the lungs, and in neural tissues and processes within the cardiorespiratory and neurologic systems (Carter & Carter, 2016; Goyal et al., 2014; Payne & Crane-Godreau, 2015; Sharma et al., 2013; Twal et al., 2016).
Physical and psychological functioning may improve with regular practice of ANB through appropriate PNS stimulation, which balances the influence of the SNS on immune/inflammatory responses (Carter & Carter, 2016; Payne & Crane-Godreau, 2015; Sharma et al., 2013; Twal et al., 2016). The potential for ANB to restore balance between the sympathetic and parasympathetic branches of the ANS is believed to promote positive psychological states by reducing anxiety and stress (Streeter et al., 2012) safely and effectively.
Examination of novel interventions that may alleviate stress, anxiety, and depression in pregnant women is essential and warranted (National Center for Complementary and Integrative Health, 2016). Reducing stress associated with IPV may be helpful in overcoming psychosocial dysfunction and health disparities that are prevalent in pregnant survivors of IPV.
Impact of Intimate Partner Violence on Women’s Health
IPV is a pervasive and insidious issue affecting the health of millions of U.S. citizens (CDC, 2019a). The incidence of IPV is demographically widespread in the United States, occurring in all states (Smith et al., 2017), subcultures, religions, and socioeconomic groups (E. Miller & McCaw, 2019). For women in abusive relationships, pregnancy does not necessarily offer protection from physical and psychological violence (Alhusen et al., 2015; Bailey, 2010; Brownridge et al., 2011; Chambliss, 2008; Chisholm et al., 2017; Taillieu et al., 2016; WHO, 2011).
Women exposed to IPV are at risk for a wide range of injuries resulting from physical violence. This includes increased risk for a multitude of chronic diseases and conditions affecting body systems (CDC, 2019b; Chisholm et al., 2017; WHO, 2017). They are also at considerable risk for many psychologic conditions, including anxiety disorders, depression, posttraumatic stress disorder, and insomnia (CDC, 2019b; WHO, 2017). Consequences to women’s health can endure despite termination of violence (CDC, 2019b; Chisholm et al., 2017). Women exposed to IPV at any point in their lifetime, even if it ended years prior, assessed their physical and mental health as poor twice as often as those who were never exposed to IPV (WHO, 2012). Physical and psychological stress resulting from exposure to IPV is a factor implicated in the adverse health outcomes common to this population of women (Taillieu et al., 2016; Van Parys et al., 2015). In addition to increased risk for several adverse outcomes with regard to their general health (CDC, 2019b; WHO, 2017), pregnant women who experience IPV face additional risk for poor pregnancy and childbirth outcomes (Alhusen et al., 2015; Brownridge et al., 2011; Taillieu et al., 2016; Van Parys et al., 2015; WHO, 2017).
Adverse pregnancy and birth outcomes experienced by pregnant women exposed to IPV include preterm labor and birth, placental abruption, uterine rupture, low birth weight, infection, poor maternal nutrition/weight gain, pregnancy-induced disease, and fetal demise (Alhusen et al., 2015; Bailey, 2010; Brownridge et al., 2011; Chambliss, 2008; Taillieu et al., 2016; Van Parys et al., 2015; WHO, 2011). Exposure to IPV can severely affect the health and development of the fetus (Taillieu et al., 2016; Van Parys et al., 2015; WHO, 2017). Poor physical and mental health during pregnancy has implications for children’s health after birth, including physical, cognitive, and emotional problems and impaired maternal–child attachment (Bailey, 2010; Chambliss, 2008; Izaguirre & Calvete, 2014; Taillieu et al., 2016; WHO, 2011).
Women are vulnerable during pregnancy because of the physical and psychological adaptations they undergo during this period (Brownridge et al., 2011; Van Parys et al., 2015). Evidence has demonstrated that IPV affects the health of pregnant women because the stressors experienced from the trauma of IPV intensify the normal stressors of pregnancy (Brownridge et al., 2011; Van Parys et al., 2015). The combined exposure to stressors of IPV and those of normal pregnancy increases the vulnerability of pregnant women exposed to IPV even further.
In summary, ANB reduces stress by enhancing PNS function and has demonstrated effectiveness in stress reduction in several populations. It is a safe, easy to learn and perform intervention, and it may be useful in alleviating stress in pregnant survivors of IPV. Reducing stress levels in these women has great potential to improve their physical and psychological health, pregnancies, and birth outcomes.
Systematic Review
The question guiding this SR was “Does the evidence on ANB support its use as a holistic intervention to reduce stress in pregnant survivors of IPV?” The SR followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (Moher et al., & The PRISMA Group, 2009).
Search Strategies and Information Sources
The first search determined the prevalence of the use of yogic breathing as an intervention for stress reduction. Search terms reflected the known variations of name and technique of yogic breathing interventions (Van Diest et al., 2014). The search limits were publication dates between 01/2013 and 07/2019, and English language and peer-reviewed articles. The selection criterion was randomized controlled trials (RCTs). This initial general search yielded too many unspecific results, so a second search narrowed articles to those most relevant to stress reduction.
Eight databases (see Table 1) were explored in the second search (studies conducted in the general population). Reference lists of the selected articles were examined for relevant articles using the same search terms, limits, and selection criterion. A search was then performed on Google Scholar by entering the titles of these potentially relevant articles. In the third search (studies conducted in pregnant survivors of IPV), four databases (see Table 1) were explored. Reference lists of the research articles selected for consideration in this search were also examined for articles meeting the selection criterion. Then a search was performed on Google Scholar by entering the titles of these potentially relevant articles. This search yielded several articles that were duplicates or were minimally/nonrelevant to the purpose of the search.
Search Strategy
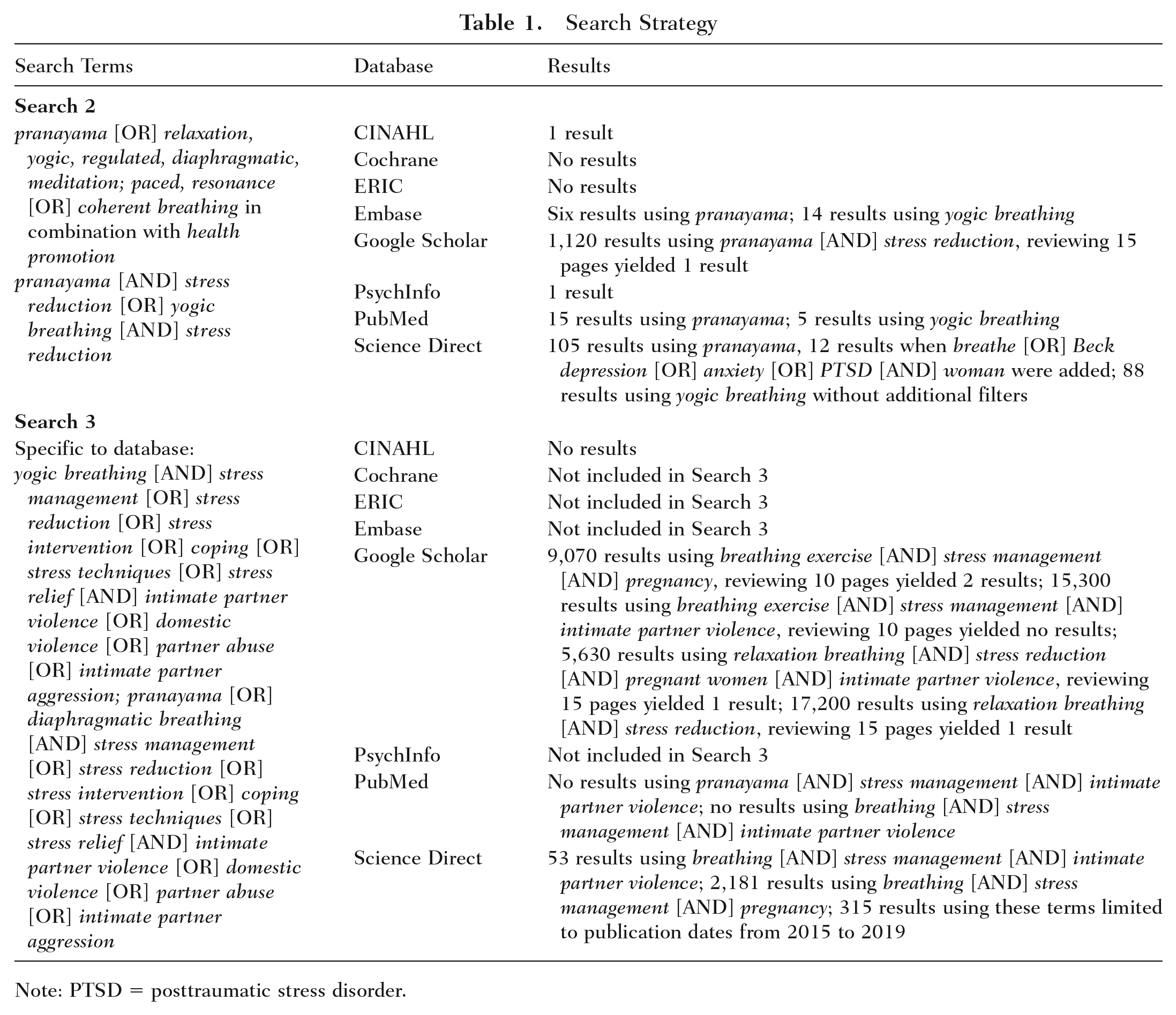
Note: PTSD = posttraumatic stress disorder.
A third search targeted databases that yielded the most results from the second search, using similar search limits but narrowed to pregnant survivors of IPV. In the third search, four databases (see Table 1) were explored. Reference lists of research articles were also examined using the procedure described above. This search only yielded studies conducted in women survivors of IPV who were not pregnant or pregnant women who did not experience IPV, and it generated many duplicates or minimally/nonrelevant articles. Thus, the search yielded no studies specifically targeting pregnant survivors of IPV.
Study Selection
Studies that met the selection criterion from the second database search (those conducted in the general population) were screened for inclusion in the SR. Studies using reference lists of these articles that met the selection criterion were also considered in the final evaluation. After reviewing the abstracts of these articles, those studies that were not RCTs were removed from inclusion. The remaining studies (i.e., RCTs) obtained from the databases and reference lists were reviewed for use of ANB as an intervention. Searches for studies that met the criteria from the third database search (those conducted in pregnant survivors of IPV) only yielded studies conducted in populations of women survivors of IPV who were not pregnant and those who were pregnant but did not experience IPV. Unfortunately, none of these studies used ANB, but they did use a type of relaxation breathing. Thus, the studies using a form of relaxation breathing in these two subpopulations were examined.
Data Collection Process and Data Items
The first author extracted data from the study articles independently; the extraction was confirmed by a second member of the team. The studies were examined for similarities and dissimilarities in several study characteristics.
The specific variables examined were study purpose, study population, sample size, sample demographics, type of ANB used, measurement scales for stress and/or other psychological states, measurement of biological indicators of stress, intervention duration, study duration, study results, and risk of bias.
Risk of Bias in Individual Studies and Across Studies
Risk of bias in individual studies and across studies was assessed by carefully examining the study article for potential sources of bias. The Revised Cochrane Risk-of-Bias tool for randomized trials (RoB 2) was used to assess risk of bias in individual studies and across studies (RoB 2 Development Group, 2019).
Results
Study Selection
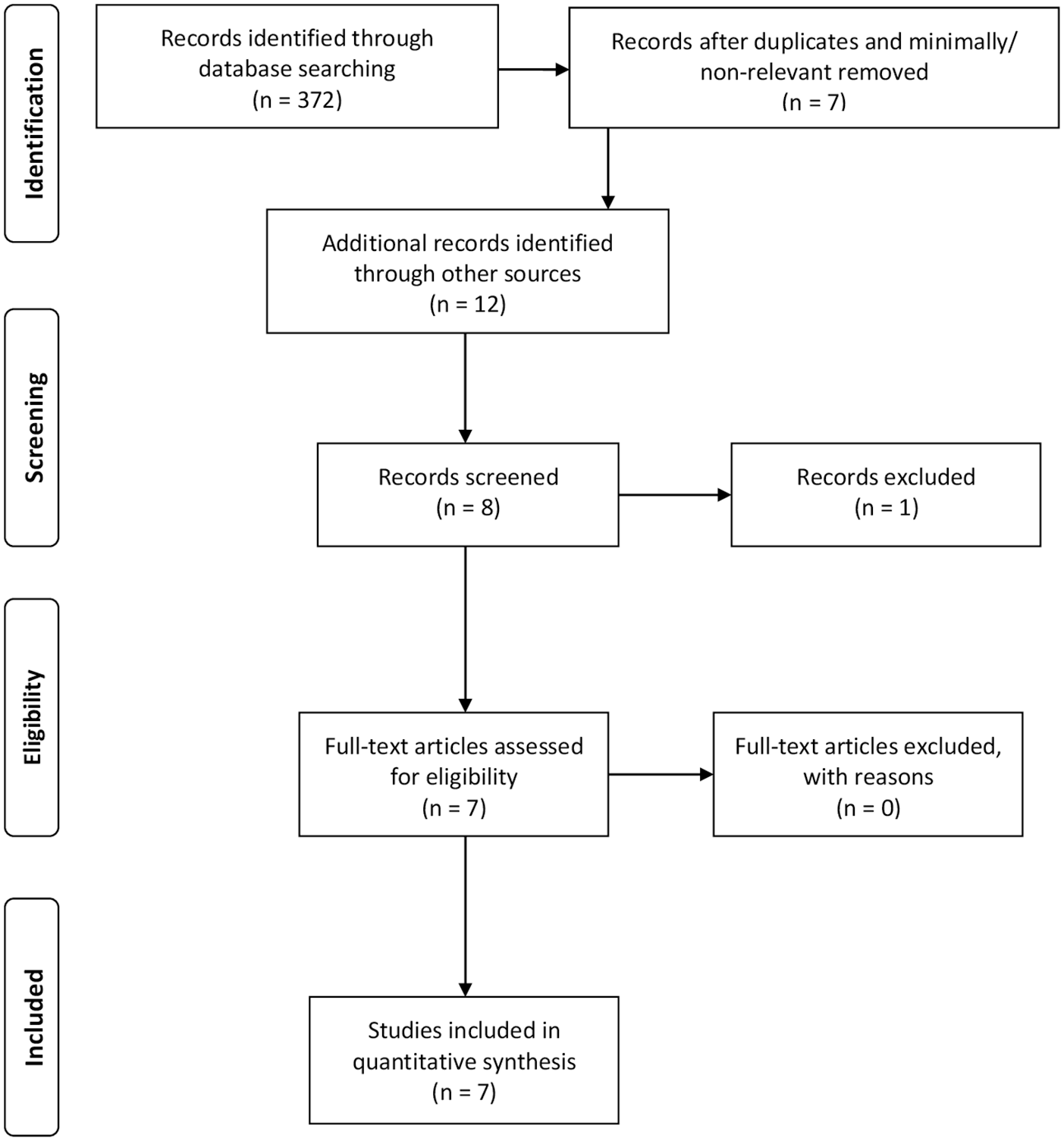
In the second database search, of studies conducted in the general population, relevant studies were assessed for eligibility, and additional articles were identified by examining the reference lists of the relevant studies. Studies that met the selection criterion were considered in the final evaluation. After reviewing the abstracts of these articles, those that were not RCTs were removed from inclusion. The remaining RCTs were reviewed for use of ANB as an intervention, and those that used ANB were included (see Figure 2 for details).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Flow Diagram: General Populations (Second Search)
In the third database search, of studies conducted in a population of pregnant survivors of IPV, no studies relevant to the purpose of the SR were found. Studies conducted in pregnant women or women who experienced IPV were assessed for eligibility. Additional articles were identified from examining the reference lists of the studies selected from this search. Studies that met the selection criterion were considered in the final evaluation. After reviewing the abstracts of these articles, those studies that were not RCTs were removed from inclusion. Seven studies from this search that met the criteria of interest were identified for inclusion: three RCTs in populations of women survivors of IPV and four RCTs in those who were pregnant. None of these studies used ANB, demonstrating that no studies to date have used ANB as an intervention to reduce stress in pregnant survivors of IPV (see Figure 3 for details).
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Flow Diagram: Women Survivors of Intimate Partner Violence (IPV) or Pregnant Women (Third Search)
Study Characteristics and Risk of Bias Within and Across Studies
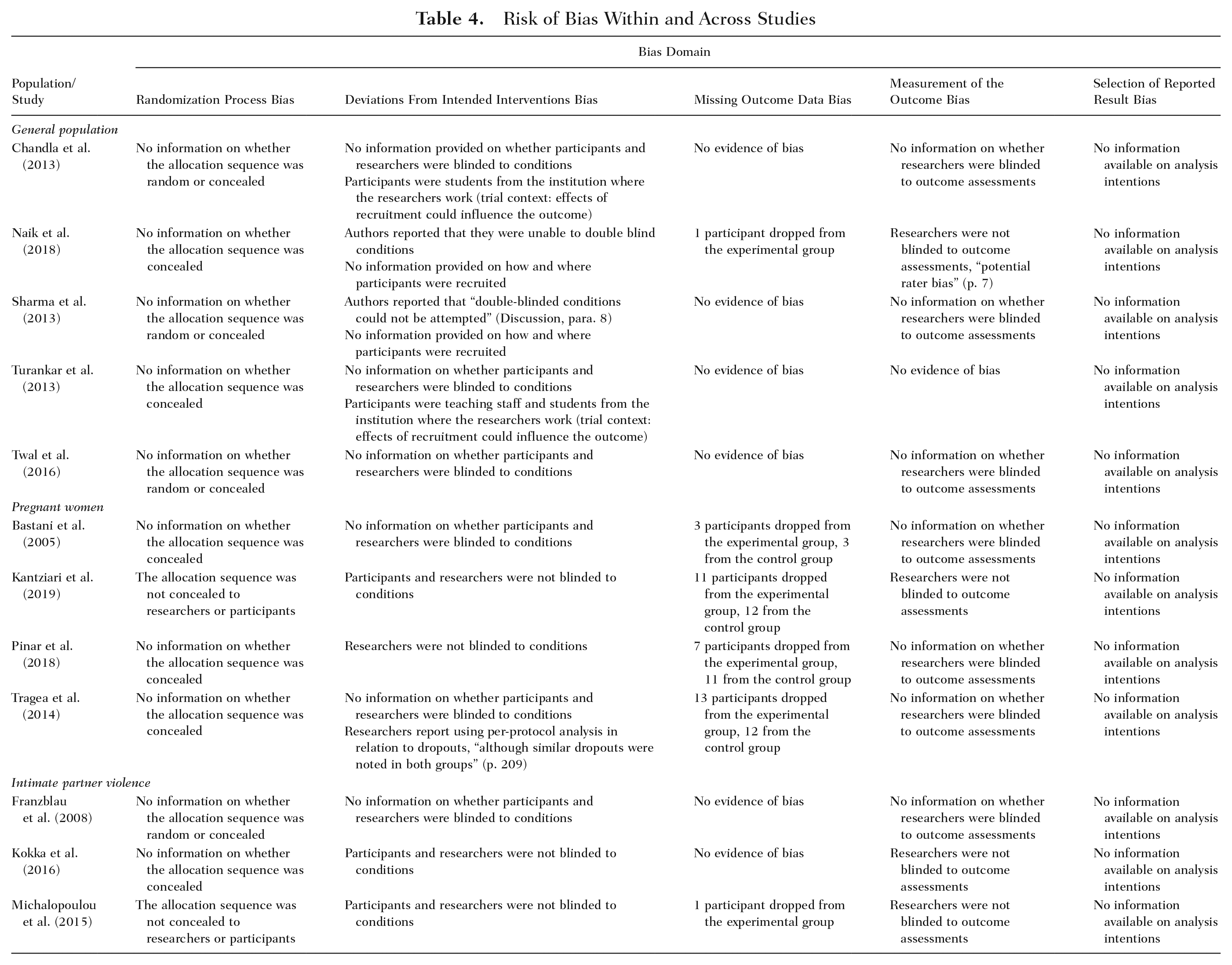
Study characteristics are listed in Tables 2 and 3. The most frequently occurring risk of bias across studies that may affect cumulative evidence was bias due to deviations from intended interventions. Other types of bias that may affect cumulative evidence were randomization process bias, measurement of the outcome bias, and missing outcome data bias (see Table 4).
Alternate Nostril Breathing Studies in General Populations: Main Findings Related to Stress
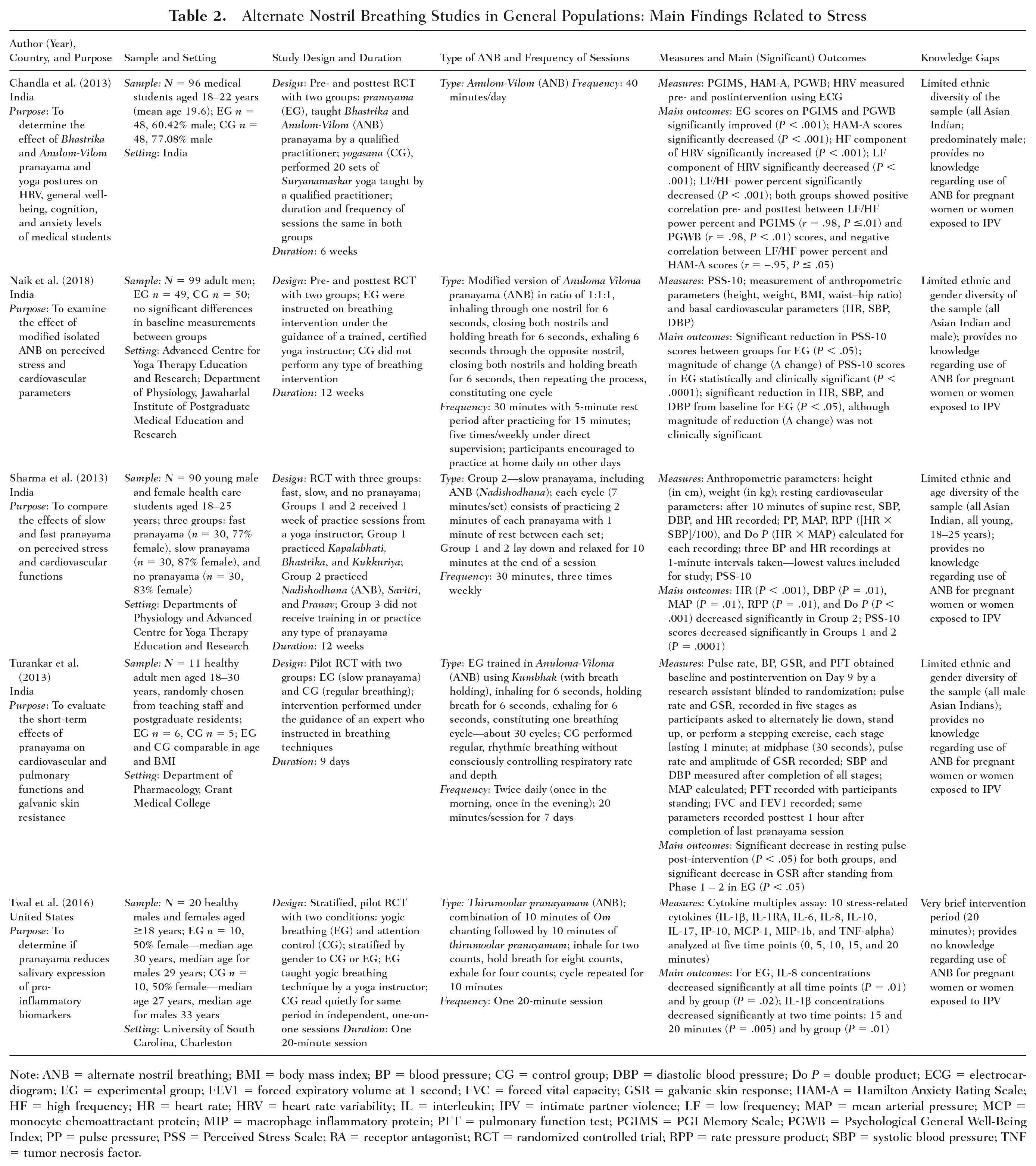
Note: ANB = alternate nostril breathing; BMI = body mass index; BP = blood pressure; CG = control group; DBP = diastolic blood pressure; Do P = double product; ECG = electrocardiogram; EG = experimental group; FEV1 = forced expiratory volume at 1 second; FVC = forced vital capacity; GSR = galvanic skin response; HAM-A = Hamilton Anxiety Rating Scale; HF = high frequency; HR = heart rate; HRV = heart rate variability; IL = interleukin; IPV = intimate partner violence; LF = low frequency; MAP = mean arterial pressure; MCP = monocyte chemoattractant protein; MIP = macrophage inflammatory protein; PFT = pulmonary function test; PGIMS = PGI Memory Scale; PGWB = Psychological General Well-Being Index; PP = pulse pressure; PSS = Perceived Stress Scale; RA = receptor antagonist; RCT = randomized controlled trial; RPP = rate pressure product; SBP = systolic blood pressure; TNF = tumor necrosis factor.
Breathing Intervention Studies in Women Survivors of IPV or Pregnant Women: Main Findings Related to Stress
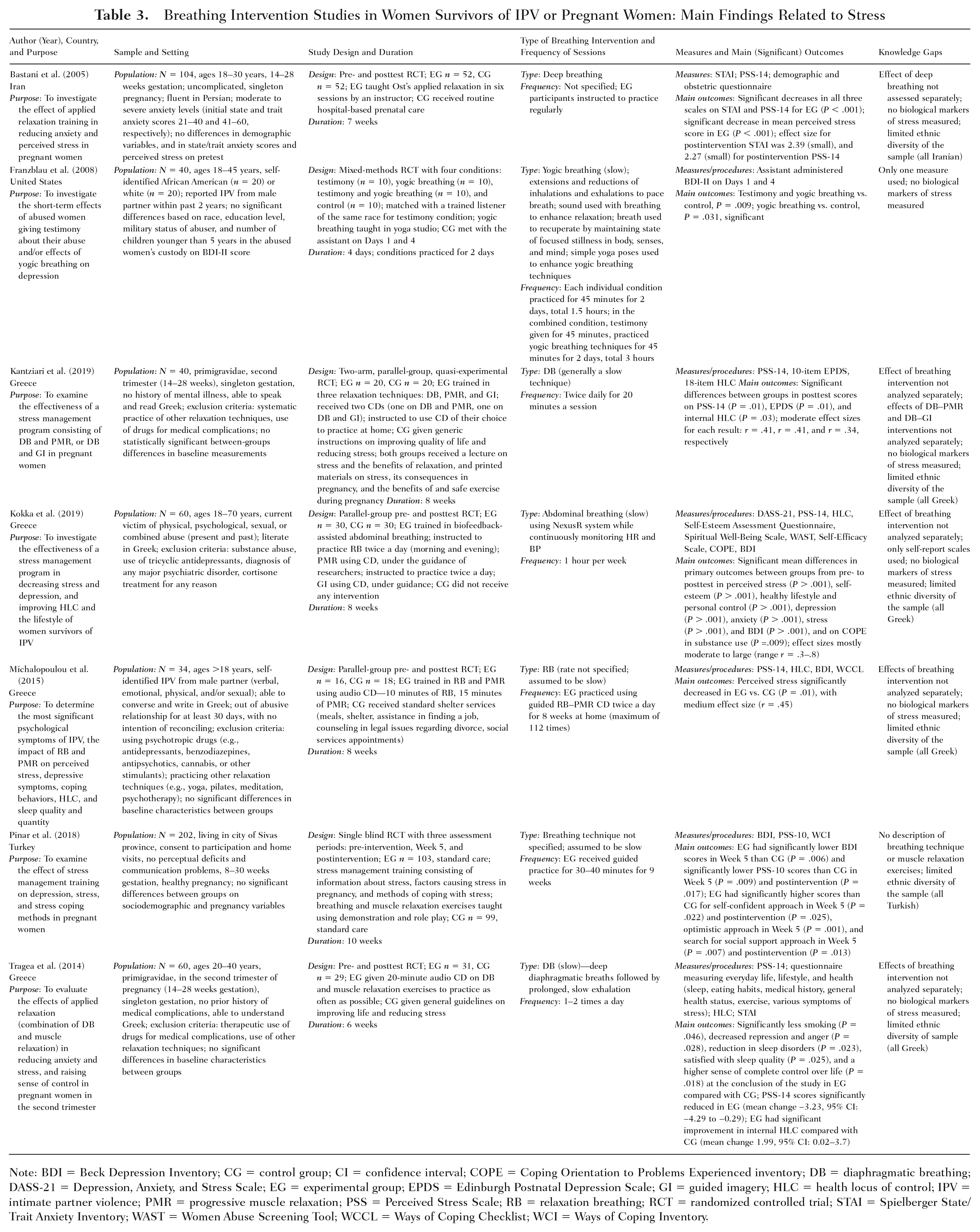
Note: BDI = Beck Depression Inventory; CG = control group; CI = confidence interval; COPE = Coping Orientation to Problems Experienced inventory; DB = diaphragmatic breathing; DASS-21 = Depression, Anxiety, and Stress Scale; EG = experimental group; EPDS = Edinburgh Postnatal Depression Scale; GI = guided imagery; HLC = health locus of control; IPV = intimate partner violence; PMR = progressive muscle relaxation; PSS = Perceived Stress Scale; RB = relaxation breathing; RCT = randomized controlled trial; STAI = Spielberger State/Trait Anxiety Inventory; WAST = Women Abuse Screening Tool; WCCL = Ways of Coping Checklist; WCI = Ways of Coping Inventory.
Risk of Bias Within and Across Studies
Results of Individual Studies
Chandla et al. (2013) demonstrated a significant reduction in anxiety levels postintervention and significant improvement in the experimental group postintervention. Naik et al. (2018) demonstrated that ANB resulted in a significant reduction in PSS-10 scores, with a clinically significant magnitude reduction (Δ change) in PSS-10 scores for the experimental group. Sharma et al. (2013) demonstrated that ANB is effective in reducing perceived stress, and the ability of specifically slow yogic breathing to decrease cardiac indices indicative of stress response, including heart rate, diastolic blood pressure, mean arterial pressure, rate pressure product, and double product, thus showing that it is an effective intervention for reducing stress. Turankar et al. (2013) demonstrated that ANB is effective in reducing pulse rate and galvanic skin response, corroborating other studies that measured these parameters and found similar results. Twal et al. (2016) demonstrated that ANB is effective in decreasing some salivary cytokines (IL-1β, IL-8, and MCP-1 [monocyte chemoattractant protein]) that are increased during stress states.
Synthesis of Results for ANB as an Intervention to Reduce Stress
Slow yogic breathing techniques have shown effectiveness in several studies with demographically diverse populations in reducing multiple indicators of stress (Chandla et al., 2013; Chen et al., 2017; Ma et al., 2017; Naik et al., 2018; Perciavalle et al., 2017; Seppala et al., 2014; Sharma et al., 2013; Turankar et al., 2013; Twal et al., 2016), implying its broad applicability. Five of these nine RCTs (Chandla et al., 2013; Naik et al., 2018; Sharma et al., 2013; Turankar et al., 2013; Twal et al., 2016) used a version of ANB in their interventions and are included in this review (see Table 2).
The five RCTs using ANB measured one or more biological parameters of stress and demonstrated the efficacy of ANB in reducing stress as assessed by these parameters. The biological parameters measured included cardiorespiratory function (n = 3), skin conductivity (n = 1), heart rate variability (n = 1), and salivary pro-inflammatory cytokines (n = 1). Of the five studies that measured physiological parameters of stress, three also used psychological measures. Combined biological and psychological assessments showed overall improvements in stress, supporting the correlation between the intervention and the outcome of interest (Kazdin, 2017).
Two of the three studies that used psychological measures used the PSS-10 (Naik et al., 2018; Sharma et al., 2013). The third study (Chandla et al., 2013) used three different psychological scales to measure a variety of emotional states related to stress (i.e., anxiety, memory, and general well-being).
Risk of Bias Within and Across Studies in General Populations
Risk of bias due to deviations from the intended interventions, i.e., the effect of assignment to intervention bias due to lack of blinding of participants, researchers, and/or evaluators, was apparent in all of the reviewed RCTs (n = 5), and trial context: effects of recruitment that could influence the outcome (n = 4). All of the studies also demonstrated some form of risk from the randomization process. Most of the studies demonstrated risk in measurement of the outcome bias (n = 4). Risk of missing outcome data bias due to attrition was demonstrated in one of the five RCTs. Concerns regarding the potential for bias due to inadequate or selective reporting as a result of failure to disclose both funding sources and conflicts of interest were demonstrated in two of the five RCTs. Table 4 is a summary table with additional details of these studies. Taken together, the studies suggest that ANB can positively influence the stress response, thereby improving resistance to stressors and mitigating health risks (Carter & Carter, 2016; Goyal et al., 2014; Kendall-Tackett, 2009). The scientific base for yogic breathing, specifically ANB, as a potential intervention for pregnant survivors of IPV is subsequently examined.
Synthesis of Results Supporting an Intervention of ANB for Reducing Stress in Pregnant Women Survivors of IPV
The literature search yielded seven RCTs that used a yogic breathing intervention in samples of women who were relevant for pregnant survivors of IPV (see Table 3). Three of these studies investigated stress reduction in women survivors of IPV who were not pregnant (Franzblau et al., 2008; Kokka et al., 2019; Michalopoulou et al., 2015). The remaining four studies investigated stress reduction in pregnant women who were not exposed to IPV (Bastani et al., 2005; Kantziari et al., 2019; Pinar et al., 2018; Tragea et al., 2014). Although all of these studies used a form of yogic breathing in a combined intervention to reduce stress, none of them used ANB.
Franzblau et al. (2008) used three different interventions (giving testimony, yogic breathing, or giving testimony combined with yogic breathing) in a sample of American women exposed to IPV. Kokka et al. (2016) used a combination of relaxation breathing, progressive muscle relaxation, and guided imagery in a sample of Greek women exposed to IPV. Michalopoulou et al. (2015) used relaxation breathing and progressive muscle relaxation in a sample of Greek women exposed to IPV.
Bastani et al. (2005) used deep breathing and muscle relaxation in a sample of pregnant Iranian women. Kantziari et al. (2019) used diaphragmatic breathing and progressive muscle relaxation, or diaphragmatic breathing and guided imagery in a sample of pregnant Greek women. Pinar et al. (2018) used breathing and muscle relaxation exercises in a sample of pregnant Turkish women. Tragea et al. (2014) used relaxation breathing and progressive muscle relaxation in a sample of pregnant Greek women.
Only one study analyzed the yogic breathing portion of the combined intervention separately (Franzblau et al., 2008). None of the studies measured biological parameters of stress, relying only on psychological scales. All the studies except one (Franzblau et al., 2008) measured stress using the Perceived Stress Scale. Four of the studies reported effect sizes ranging from small to large (Bastani et al., 2005; Kantziari et al., 2019; Kokka et al., 2019; Michalopoulou et al., 2015), which supports the efficacy of the intervention. This literature review revealed that no intervention studies using ANB have been conducted to date to reduce stress in pregnant survivors of IPV, which reveals a gap in knowledge that should be addressed to provide a holistic and potentially beneficial, safe, and cost-effective intervention for pregnant survivors of IPV.
Risk of Bias Within and Across Studies in Pregnant Women and Survivors of IPV
All of the studies demonstrated some form of risk from the randomization process. Bias due to deviations from the intended interventions and bias in measurement of the outcome due to lack of blinding of participants, researchers, and/or evaluators were apparent in all of the reviewed RCTs, although Pinar et al. (2018) did blind the participants to conditions. Potential for missing outcome data bias due to attrition was evident in five of the seven RCTs. Some concerns regarding inadequate/selective reporting were apparent in most of the studies, with authors failing to disclose both funding sources and conflicts of interest (n = 3), funding sources (n = 2), conflicts of interest (n = 1), or aspects of the intervention (n = 2). See Table 4 for additional details.
Limitations
A limitation in conducting this SR was the dearth of literature on the use of ANB for stress reduction in pregnant survivors of IPV. In addition to the risks of bias previously discussed, most of the studies conducted in the general population were limited in ethnic and gender diversity—most of them using populations of Asian Indians (Chandla et al., 2013; Sharma et al., 2013) who were male (Naik et al., 2018; Turankar et al., 2013). There was no indication in two studies that a power analysis had been conducted (Chandla et al., 2013; Naik et al., 2018). Two studies did not provide reliability and validity data for the PSS-10 (Naik et al., 2018; Sharma et al., 2013). A potential limitation in two studies was lack of measurement of biochemical and/or physiological parameters of stress (Naik et al., 2018; Sharma et al., 2013). Chandla et al. (2013) reported that it was challenging to maintain subjects’ participation and motivation for the duration of the study, and they also noted that few studies have been conducted on yogic breathing. We observed that the researchers did not specify how participants were randomized to groups and did not provide information on whether the groups were demographically similar. Naik et al. (2018) reported that participants with psychological conditions were not excluded from participation. Sharma et al. (2013) reported that only one self-report measure was used to assess stress. We observed that age diversity of the sample was limited (all young, 18-25 years) and the researchers did not specify how participants were randomized to groups. Turankar et al. (2013) reported no limitations for their study. We considered this lack of discussion on potential limitations as itself a limitation, and the researchers did not specify how participants were randomized to groups. Twal et al. (2016) reported that cytokine concentrations at time 0 were obtained after the experimental group learned ANB, which may have influenced the cytokine concentrations and may not reflect the true baseline values. We observed that the intervention duration was very brief (20 minutes) and the researchers did not specify how participants were randomized to groups.
All of the studies conducted in pregnant women who did not experience IPV and most of the studies conducted in women survivors of IPV who were not pregnant were limited in ethnic diversity of the sample, and the breathing intervention was not evaluated separately from the other components of the intervention in all but one of these studies. None of these studies measured biological indicators of stress. Most of them did not include any type of blinding. Bastani et al. (2005) reported the following limitations: some aspect of the group sessions other than the relaxation technique itself may have reduced anxiety and perceived stress; socializing after training sessions (in person or over the phone) could have provided social support that influenced outcomes for experimental group participants; frequency of home practice was based on unverified, subjective self-reports; and long-term changes in anxiety and stress were not assessed. Potential limitations that Kantziari et al. (2019) reported were that self-report tools were used, the degree of compliance was not measured, and participants’ expectations of benefit could have biased the results. Pinar et al. (2018) did not report limitations. We observed this lack of discussion on potential limitations as a limitation. Pinar et al. (2018) also did not describe the breathing technique or the muscle relaxation exercises, effect sizes were not stated, and the researchers stated in their conclusion that pregnant women should be given a music CD to listen to in their home but did not discuss the use of a music CD in their report. Tragea et al. (2014) reported several limitations, including the following: (1) results may be partially differentiated in the experimental group due to the influence of the trainer-consultant; (2) more frequent phone and/or personal contact with the trainer in the experimental group may have assisted in reducing stress and anxiety independently of the intervention; (3) it was not possible to monitor and control adherence to the intervention, other than using a diary to record frequency of practice; (4) results may not be generalizable to all populations of pregnant women due to potential differences in demographics; (5) specific demographics of their sample of pregnant women may have influenced adherence to the intervention and expectation of an effect; (6) per-protocol analysis was used despite similar numbers of attrition in both groups; and (7) the scales used measured stress in general, not stress specific to pregnancy, since these are considered more predictive and reliable for assessing for premature birth.
Franzblau et al. (2008) stated that the sample size was small and the study duration was brief (4 days). Kokka et al. (2016) reported several limitations, including (1) the relatively small sample size, (2) the short duration of the study/intervention, (3) difficulty monitoring compliance, and (4) inability to determine if participants were receiving other interventions while participating in the study. We observed that the researchers did not specify how participants were randomized to groups. Michalopoulou et al. (2015) reported that all measures relied on self-report, the study duration was short (8 weeks), and the control group did not receive any form of stress reduction intervention, increasing the potential for differences in outcomes. We observed that the techniques used for relaxation breathing and progressive muscle relaxation were not described.
Discussion
Summary of Evidence for ANB in Stress Reduction
In conducting this SR, no nursing literature was found that focused on the intervention of ANB in pregnant survivors of IPV. One study using a combination intervention of relaxation breathing and muscle relaxation in pregnant women who did not experience IPV was conducted by nurses but was not published in a nursing journal (Pinar et al., 2018). The study by Bastani et al. (2005) conducted in the same population using a similar intervention was published in a nursing journal (Journal of Midwifery and Women’s Health), and one of the researchers was a registered nurse and midwife (Maryam Vafaei).
Five studies in general populations demonstrated the effectiveness of ANB in significantly improving multiple indicators of stress, including increasing the high-frequency component of heart rate variability (Chandla et al., 2013); decreasing heart rate (Naik et al., 2018; Sharma et al., 2013; Turankar et al., 2013); decreasing blood pressure (Naik et al., 2018; Sharma et al., 2013); decreasing double product, mean arterial pressure, and rate pressure product (Sharma et al., 2013); decreasing galvanic skin conductivity (Turankar et al., 2013); and decreasing the pro-inflammatory cytokines IL-8 and IL-1β (Twal et al., 2016). These parameters are appropriate to measure when evaluating an intervention for stress reduction, because all are involved in the stress response initiated by the immune system and SNS, and the HPA axis (Jaremka et al., 2013). One of these studies also demonstrated that ANB significantly improved psychological well-being and memory and significantly decreased anxiety (Chandla et al., 2013). Two of these studies also demonstrated that ANB significantly decreased perceived stress (Naik et al., 2018; Sharma et al., 2013). Turankar et al. (2013) blinded the research team member who collected data on biological parameters of stress to conditions, which strengthens confidence in these results. The study by Chandla et al. (2013) included women, which adds support for the effect of ANB in pregnant women; measured anxiety, which is a common condition in women survivors of IPV; and measured heart rate variability, which is a good biophysical indicator of stress. And the experimental intervention of ANB was compared with a control of yoga postures. This allowed for evaluation of the effects of ANB separately from those of yoga postures, demonstrating that ANB, compared with yoga positions, likely is the component in the practice of yoga that contributes most to stress reduction, providing support for the strength of an intervention of ANB as beneficial for stress mitigation. Half of the participants in the study by Twal et al. (2016) were women, supporting the potential to use ANB as an intervention to reduce stress in pregnant women. Of the three studies that used psychological measures, Chandla et al. (2013) used three different psychological scales to measure a variety of emotional states related to stress but did not use the PSS-10. Use of different psychological measures can make synthesis of the results challenging.
Seven studies conducted with survivors of IPV or with pregnant women and using a combined intervention that included a form of yogic breathing demonstrated improvements in psychological measures, including significantly decreased anxiety (Bastani et al., 2005; Kokka et al., 2019), significantly decreased depression (Franzblau et al., 2008; Kantziari et al., 2019; Kokka et al., 2019; Pinar et al., 2018), and significantly decreased perceived stress (Bastani et al., 2005; Kantziari et al., 2019; Kokka et al., 2019; Michalopoulou et al., 2015; Pinar et al., 2018; Tragea et al., 2014). All but one of these studies used a version of the Perceived Stress Scale to measure stress, which enhances synthesis of results.
Pinar et al. (2018) blinded participants to the allocation sequence, which likely strengthens confidence in the differences in results between groups. Franzblau et al. (2008) demonstrated that although the combined intervention of yogic breathing and giving testimony about the experience of IPV was the most significant of their four interventions, testimony alone was not significant, while yogic breathing alone was significant, indicating that the breathing component of the combined intervention contributed the greatest effect. However, none of the studies in survivors of IPV or in pregnant women used ANB.
Conclusions
The evidence on yogic breathing, specifically ANB, for stress reduction shows promise, but research using ANB as a holistic intervention for reducing stress in pregnant survivors of IPV is limited. Because of the insidious and profound implications of IPV for the physical and psychological health of affected pregnant women and their fetuses, further research on safe and effective interventions is warranted. Pregnant survivors of IPV are an exceptionally vulnerable group of women. Based on the findings of this SR, ANB may offer a feasible, safe, and effective holistic intervention for decreasing psychological and biological measures of stress in these women. ANB may also offer benefits for pregnant women’s emotional health and presents no known associated risks to mother or baby.
Research and Clinical Implications
Using ANB as an intervention to reduce stress in pregnant survivors of IPV supports the tenets of holistic nursing because it addresses the whole person through mechanisms of action that intersect the complexity of the conditions of pregnancy and IPV with the intervention itself.
The first step in investigating the use of ANB as an intervention to reduce stress in pregnant survivors of IPV is to determine its feasibility and acceptability within this vulnerable population. The authors are currently conducting this feasibility research. Knowledge gained from the feasibility study will determine how ANB can be incorporated into a stress mitigation program for pregnant survivors of IPV. Since the stress reduction benefits may be significant for these women and their fetuses, and the risks of an ANB intervention are very minimal, the benefit-to-harm ratio is likely to favor implementation (Friedman et al., 2015).
A feasible, holistic ANB intervention has the potential for important clinical applications. Because the incidence of IPV is likely greatly underreported (Bailey, 2010; Brownridge et al., 2011; Chisholm et al., 2017; Taillieu et al., 2016), stress reduction should be offered to all pregnant women in obstetric providers’ offices; prenatal classes; women’s shelters, including those providing outreach services, emergency shelter, or transitional housing; birthing centers; and labor and delivery, and mother–baby units of hospitals. Since ANB is easy to practice and does not require any special clothing or equipment, it can be practiced in practically any setting—home, work, school, or health care provider offices.
Footnotes
Authors’ Note:
This research received financial support in the form of a doctoral award, the McGaffic Memorial Endowment Scholarship, awarded to Ottilie Rung from the College of Nursing and the University of Arizona Foundation. Portions of this article were exhibited in part as a poster presentation at the Western Institute of Nursing (WIN) Conference in Portland, OR, on April 16, 2020.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.