
Abstract
A Caring Arts Program (CAP) was inspired and carried out by the vision of an in-resident nurse-artist and the chief nursing officer in a private, not-for-profit health system. Together they envisioned a program that would impact family, patients, and staff while improving patient/family care practices. The impact of the CAP was evaluated through mixed methods which included stories, fieldnotes, comments, and the Listen360(R) which rates patient satisfaction scores. The synergy between the evaluations and the attempt to understand what creates patient satisfaction using creative arts was a prime objective of this article. The qualitative results represented by field notes and written patient comments revealed a positive impact on participants. The quantitative results demonstrated an improvement in patient satisfaction scores during the time of the project. The positive trend in the scores combined with the qualitative stories and interviews suggests that the CAP contributed to the improvement in patient satisfaction at Baptist MD Anderson Cancer Center. During a worldwide pandemic, supporting human caring and self-expression was more critical than ever.
Keywords
The purpose of this paper is to identify the benefits of a Caring Arts Program (CAP) in a health care system. As this article was being written, the world changed with the COVID-19 pandemic. Everything in healthcare changed in weeks, and competing priorities took on an amplified meaning. How can one consider an art program when only essential patients can be cared for, and families cannot accompany them? This challenging question brought to life the investigation of retroactive data which measures the impact of the CAP. The patients' subjective and personal outcomes were used in the form of a programmatic evaluation.
The power of the arts to heal is hardly a new concept. The history of healing arts describes ancient rituals that involved creating images that told healing stories. Ancient cultures included drums, music, dance, prayer, meditation, and artistic expression in their healing work (Rockwood Lane, 2005). Humans have been drawn to artistic expression in healing practices for millennia. Science was often narrowly defined as medical and bench research and seldom included the science of caring and healing. Florence Nightingale (A Conversation with Florence Nightingale 2019) saw nursing as an art: “It is one of the Fine Arts: I had almost said the Finest of Fine Arts.”
For several decades, some healthcare practitioners and administrators have partnered formally with the arts community to advance the arts in healthcare. Many of those early organizations evolved into the Arts, Health, and Well-Being in America and created a white paper, commissioned by the National Organization for Arts in Health [NOAH] (2017). The white paper is a living document as NOAH seeks to bring together and elevate the arena of arts, health, and well-being with a commitment to unifying. “Arts in Health is a maturing field dedicated to using the power of the arts to enhance health and well-being in diverse institutional and community contexts” (NOAH, 2017, p. 5). The white paper summarized research and empirical evidence indicating improvement in clinical and holistic outcomes. “In medical/clinical settings, patients’ family members and medical staff can benefit from the restorative and relaxing experience that can result from art-making” (NOAH, 2017, p. 21). Medical schools are partnering with professional artists and arts organizations focusing on the education of physicians; similar programs are lacking for nurses and other health science professionals (NOAH, 2017). As medical diagnostic and treatment skills advance, connection to the power of art to speak to the spirit and help heal continues to resurface. The duality of the medical scientific model and alternative or complementary care models is sought with more frequency as we see a revival in the nursing paradigm viewing nursing care as both an art and science (Delaney & Moore, 2017).
Literature Review
Patients report both positive and negative situations in clinical environments reflected in the service satisfaction scores. Rahmqvist and Bara (2010) mention that satisfaction scoring is a good reflection of the patient's attitude. In creating the patients’ experiences, sometimes making the family caregiver an afterthought is a missed opportunity in cancer care (Berry et al., 2016; Rahmqvist, 2001). “It is time to move beyond the concept of merely patient-centered care and place both the patient and the family caregiver at the center of care that benefits all stakeholders in the complex task of serving patients with cancer” (Berry et al., 2016, para.37).
Stuckey and Nobel (2010) mention the therapeutic effects and benefits of arts in healing. Additionally, Sadler et al. (2009) advocated that visual art demonstrates caring and empathy in hospital settings. Creative individuals and healthcare systems explored the impact of including the arts in healing approaches. When the arts become a part of the healing space's atmosphere, it can be perceived as more compassionate and humanistic to the patient and visitors (Sadler et al., 2009).
Researching this structured duality, Stuckey and Nobel (2010) noted that most of the early publications on art and healing were theoretical. The authors reviewed systematic and controlled studies that examined the therapeutic effects and benefits of arts and healing. Stuckey and Nobel (2010) found that the use of visual arts helped patients in many ways to make sense of or create meaning for what they were experiencing; to deal with negative emotions or anxiety; to reduce the physical and emotional impact of stress; and to improve physiologic metrics. “The use of the arts complements the biomedical view by focusing on not only sickness and symptoms themselves but the holistic nature of the person. The more we understand the relationship between creative expression and healing, the more we will discover the healing power of the arts” (Stuckey & Nobel, 2010, para.65).
According to Berry et al. (2016), a lack of rehearsal for the severe turn of life events, such as a cancer diagnosis, also places the family caregiver in a high anxiety state regarding the patient's situation. Northouse et al. (2012) wrote “when the patient-caregiver dyad is treated as the unit of care, important synergies are achieved that contribute to the well-being of both patients and caregivers” (p. 1229).
Watson (2005) speaks to the many ways connections can be made between caregivers and patients to create a caring field that will open new possibilities that allow each person to be present in the moment. Watson's work addresses the need to combine medical science with the scientific impact of human caring and provide support for the caregiver which reflects as beneficial to the patient. This transpersonal connection is defined by Watson as the caring moment when “two individuals are both in the process of being and becoming” (Watson, 2010, p. 115). Watson (2008) has written extensively on the ethics of caring and the use of multiple ways of connecting with and knowing each other, including touch, color, and visual arts. The conceptual framework in nursing is described by Watson's Theory of Human Caring as a “moral ideal that involves mind, body, and soul engagement with another” (Malek, 2015, p. 14). The caring exemplar was further postulated by Malek (2015) as a moral responsibility to patients. “The ethics of care considers three distinct elements that not only involve actions, but also a focus on relationships between power and caring practices” (Malek, 2015, p. 14). “Caring and love ultimately become one … we are all called to care, and it is through the energy of Love that we reach out to the universe of possibilities to connect with Other, nature, and that which is greater and more magnificent than our isolated separate, physical-ego existence alone” (Watson, 2005, p. 54).
Theoretical Framework and Factors Influencing Project
Applying creative outlets for stress reduction in all persons who surrounded the patient appeared to be a significant place to begin this project. Being attentive to the patient, family, and staff's needs is imperative in the patient's perception and satisfaction with treatment. To make a difference in the patient's perception of care by supporting those who support the patient is essential.
The history of CAP and the study of its impact on patient satisfaction started in 2004 when a multihospital health system began its Magnet Recognition® journey. A committee of nurses from education, clinical practice, and leadership selected Watson's Theory of Human Caring as the theory most closely aligned with the culture of nursing and care-giving in the system. The adoption of the theory led to the incorporation of caring science as the delivery model for nursing practice. Watson's encouragement and her extensive work on the importance of love, compassion, human connection, and allowing the space for possibilities of healing and wholeness to emerge Watson (2008) led the system to engage further with the work by educating nurses more fully in the theory. Nurses applied to the Watson Caring Science Institute for Caritas Coach TM education over 6 months, which included reading, reflecting, and experiencing the theory via online assignments and faculty retreats. Caritas is Latin for the love of humankind and charity. The journey was a professional and personal one as each nurse was immersed in the science of caring and the art of embracing the humanity of self and others. Poulious (2018) mentions this process as not just a study of Caring Science imposing competencies. “Rather, it is an inward journey of winding roads that lead to new ways of thinking, feeling, and becoming. The journey invites an exploration of previously held ideas about self and the world” (Poulious, 2018, p. 174). The evolution of behavioral changes allows one to see the environment in a new or different way. Poulious (2018) postulates the experience will ultimately affect the nurse's spirit.
Experienced critical care and behavioral health practitioner, the author (PM) had professional and life experiences in which the power of connection and the power of artistic expressions impacted patients. Maturing in an understanding of caring science and the difference the practice could have on the caregivers and the patients, PM approached the chief nursing officer (CNO) about the possibility of using her skill and talent to create a program that would support the organization's journey in caring science and use the arts as a way of bringing a deeper connection to the human spirit and encouraging healing and wholeness for patients.
Visual Arts Imagined
“Caritas Coaching provides nurses and other caregivers a deep, intimate look at how to infuse their practice with Caring Science, a scientific and philosophical context to explore, describe, and research human healing. By integrating Caring Science into their practice, nurses can balance information and technology with the human side of healthcare” (Poulious, 2018, p. 175). PM joined a team of both Caritas Coaches and chaplains in the system, all working to advance caring science and support the caregivers and patients. PM's role was unique as a nurse artist who intentionally created connections with staff and patients through expressive art.
With the help of foundation dollars, the health system supported PM in a part-time position to focus on Caritas Coach work. PM's role evolved over the next decade from helping colleagues understand why artistic experiences would help patients and staff (“what exactly do you do?”) to being sought after on multiple campuses to provide patient and team-member consultations and interventions. Building trust with health care workers is essential to promoting art interventions with patients. The Caritas Coach learns to be authentically present with the patient and reads patterns in the environment that positively and negatively influence health and well-being. For example, upon scanning the patient's room with intentional presence, there are questions to ask oneself. What is the mood or intensity surrounding the patient? The patient's unease may be pain management, well-meaning guest, lighting, or room temperatures. The Caritas Coach acknowledges the physical healing environment and attunes self to the spiritual needs of the patient. According to Casterline (2018), “the only way nurses can be authentically in right relation with the spiritual needs of another is to be intimately aware of their own spiritual maturity” (p. 8).
Creating a relationship with the care-giving teams provided a better understanding of PM's presence and the impact art interventions could have on the staff, patient, and family. Over the years, PM was sought by leaders and team members for team building or support activities. Often this manifested as group art projects where the team could focus for a brief time on the beauty and expressions of their spirits. Just beneath the surface of these projects was the need of the caregivers for self-healing.
As the understanding of a Caritas Coach artist's role grew, PM partnered with many units and saw numerous patients. Design consultations were requested for Caritas Rooms in the hospitals where staff could go for respite. PM saw patients in intensive care, palliative care, oncology, and outpatient settings such as the Age-Well Senior Center. Following a patient consultation, PM brought artistic expression methods and skills to manage individual anxieties, such as practicing intentional breathing and meditation. PM was a listener, an encourager, and a caring partner for the patient and family.
PM developed relationships with grateful patients who helped finance art supplies and even named the art cart “Eleanor” after a patient who donated funds. PM led a nomadic existence within the system, going where she was most needed. PM multiplied her influence by creating arts kits that unit staff could use to engage patients when she was unavailable. This project emerged from the history and success of the Caritas Coach nurse artist's experiences throughout the system.
Stories of Program Development
From experiences in the hospital environment, the reflective stories below tell the program development story that preceded this project.
Story One
The patient referral was from a nurse regarding a particularly challenging man. The nurse believed him to be consumed with his family responsibilities and business, which interfered with his care. The field notes reflect he was very withdrawn and inhibited during the first visit with only brief eye contact. During the second visit, a conscious effort was made to be present with him and to listen as he talked about his many financial concerns. On the third visit, he began to be more receptive to other topics. The question of vacation came up, and his response was, “No, I have never been on vacation.” PM encouraged him to pretend he had no financial obligations and was free to travel. Where would he go? He responded by saying, “I have never been on a cruise.” “If you draw a cruise ship,” explained PM, “we could go together.” Accepting the offer from PM, the patient drew a very tight, precise image of a ship (see Figure 1) while PM asked questions like “doesn't the salt air smell good”? and “did you see that dolphin”? When he completed his drawing, it was attached to the wall where he could see it from his bed. PM asked him to take deep breaths and repeat the visual imagery whenever he looked at his drawing.

The Cruise Ship.
On the next visit, his wife was present in his room, and PM reached out to introduce herself. The wife said, “I already know you. You are the only woman I would let my husband go on a cruise with.” The wife was filled with tearful gratitude and hoped to make the cruise a reality. She reported framing the drawing and said she would always treasure it. This was the last visit before his death. Contemplating this experience with a terminally ill patient, PM viewed this art intervention as permitting him to let go at the end of his life and enter uncharted waters, while leaving his wife with a wonderful memory of his departure.
Story Two
A charming couple married for 50+ years and devoted to each other beyond measure, cocreated an interesting art project. Painting a birdhouse was chosen for the collaborative art intervention (see Figure 2). The patient orchestrated the design and color scheme. PM helped with the art execution because the patient's hands were too shaky. Enthusiasm and eagerness were abundant about this little wooden birdhouse. Her condition improved, and she was discharged from the hospital. Nurses reported she was sitting in a wheelchair carrying her birdhouse project as though it was a newborn baby.

The Birdhouse.
After 3 days at home, it became necessary to call rescue for her and return to the hospital. Her caretaker communicated that the patient said, “I’m not going anywhere without my birdhouse.” The impact of doing small things for others is often underestimated. This example demonstrates how a small act of kindness can make a big difference in someone's struggle for wellness.
Story Three
Caring for staff caregivers with art interventions is as important as caring for the patients. One poignant story of lessening caregiver suffering occurred at a hospital where a beloved young nurse leader was diagnosed with terminal cancer. Her goal was to work if her strength would permit. Her colleagues surrounded her with love and support.
During one of the leader's hospitalizations, PM was asked to work with the team to help them cope with the impending loss of their friend. A workshop experience was created where the staff painted beautiful silk scarves to give their friend as she lost her hair. The other nurses also wore scarves in support. This collective expression of grief and beauty gave the nursing staff a way to process pain and focus love on a dear colleague (see Figure 3).

Silk Scarves.
Story Four
A bond was created among team members in an art project called The Fan Club. This project was a group activity for team collaboration called “Tell Me Something About Yourself.” Each staff member was given a miniature white paper and colored pencils. Participants were asked to draw a symbol that represented who they were. A collage was created with examples of drawings ranging from golf clubs to family members to religious icons (see Figure 4). One of the symbolic reasons for choosing the fan is the understanding that until the fan is fully opened, a breeze cannot occur, so it is with open team communication. Closed fans are not as effective as open ones.

The Fan Club.
The art intervention helped the staff to open collaboration and talk to each other. The tension which arose from poor departmental communication and lack of connection with coworkers was reduced. The single submissions represented the individuality of each employee. Together all the artwork illustrated a strong team. Some staff went right to work on this project; others needed some time to process this concept. Over time, the small renderings appeared and were assembled into a collage now hanging in the nursing station.
Financial Constraints
The CNO worked with the system foundation to secure more generous funding for the CAP with inconsistent success. The CAP is broad in scope and collaborative in nature, making specific measurements of impact a challenge. Building a financial case for the program involved improved quality outcomes or improved patient satisfaction scores. The reality of budgeting for positions that were not direct patient care was a challenge each budget cycle, despite the evidence in the literature and patient feedback that this work positively impacted the patients’ and staff’ experiences. It became clear that funding for the broader vision of building a systemic CAP was not possible in the foreseeable future, and it was time to focus PM's efforts in one area to measure the impact of creative arts.
A New Cancer Center and a New Opportunity
The need to create this focus coincided with building a new multispecialty cancer center that would provide outpatient treatment and partner with the hospital oncology units for inpatient care. Baptist Health, a Magnet® designated system located in Northeast Florida, is one of three systems in the United States who have partnered with MD Anderson Cancer Center at the University of Texas, Houston. Together they created Baptist MD Anderson Cancer Center (BMDACC) in Jacksonville, Florida (see Figures 5 and 6). The goal of the partnership was to replicate MD Anderson's multidisciplinary philosophy of care and cancer research. BMDACC provides world-class care in the prevention, diagnosis, and treatment of adults with cancer. Medical and surgical specialties are complemented with nursing, social work, pastoral and psychological care, pharmacy services and nutrition, and genetic counseling. The center was created to provide architectural aesthetics and a humanitarian environment of hope and healing for patients when they need it most.

Baptist MD Anderson Cancer Clinic.

Baptist MD Anderson Cancer Center First Floor Lobby.
Project Evaluation-Methodology and Results
The purpose of the project was to evaluate the impact of the CAP using mixed methods including field notes, artwork, patient stories, comments, and the Listen360® which rate patient satisfaction scores. The investigation focused on synergy between the evaluations to understand what creates patient satisfaction. The infusion department was chosen for score comparisons because it is where the most frequent rounds and art interventions by the Caritas Coach nurse artist occurred. Weekly documentation of art attendance records (both group and individual) was kept throughout the evaluation process. The participation reflected art visits for family, patients, and staff when attending an art studio workshop in the infusion department. Sign-in sheets were used in the voluntary art studio workshops. Participant recruitment was done through flyers advertising the art groups (see Figure 7), and personal invitations. The participant involved with an individual art visit was accounted for by writer field notes. Comments, photos, and the number of participants in group visits were also recorded daily in field notes.

Marketing Flyer.
Qualitative Examples
For this programmatic development project, the qualitative component is the study of field notes of patients’ stories and artwork, and the impact this program has on the participant's outcomes. There are many examples and stories from this caring practice. The following stories were collected from field notes and illustrate the impact that one Caritas Coach nurse artist can have while connecting to family, patient, and staff. The practice of art interventions at BMDACC was established to complement the clinic's operational flow, meaning days and hours of visits were designed to maximize the program's impact. Two examples of qualitative data used in this history are storytelling through art projects and personal comments from patients.
Art Projects Tell the Story
For the individual patient receiving chemotherapy, the focus was a 1:1 art intervention in the infusion department. Intravenous pole (IV) art is an example of a typical art intervention. The IV pole art is a colorful image made with mixed media that resonates with a patient's positive emotions during treatment. The patient takes the art home as an affirmation or an art piece to hang on the wall. Figure 8 represents the heart focus of a single word. The word courageous, taken from a scripture in the Bible, is what this patient called upon during her cancer struggle. The true measurement of success using IV pole art is to view it as a catalyst to awaken a patient's passion and hope. Individualization is a priority when caring for a patient and encouraging creativity.
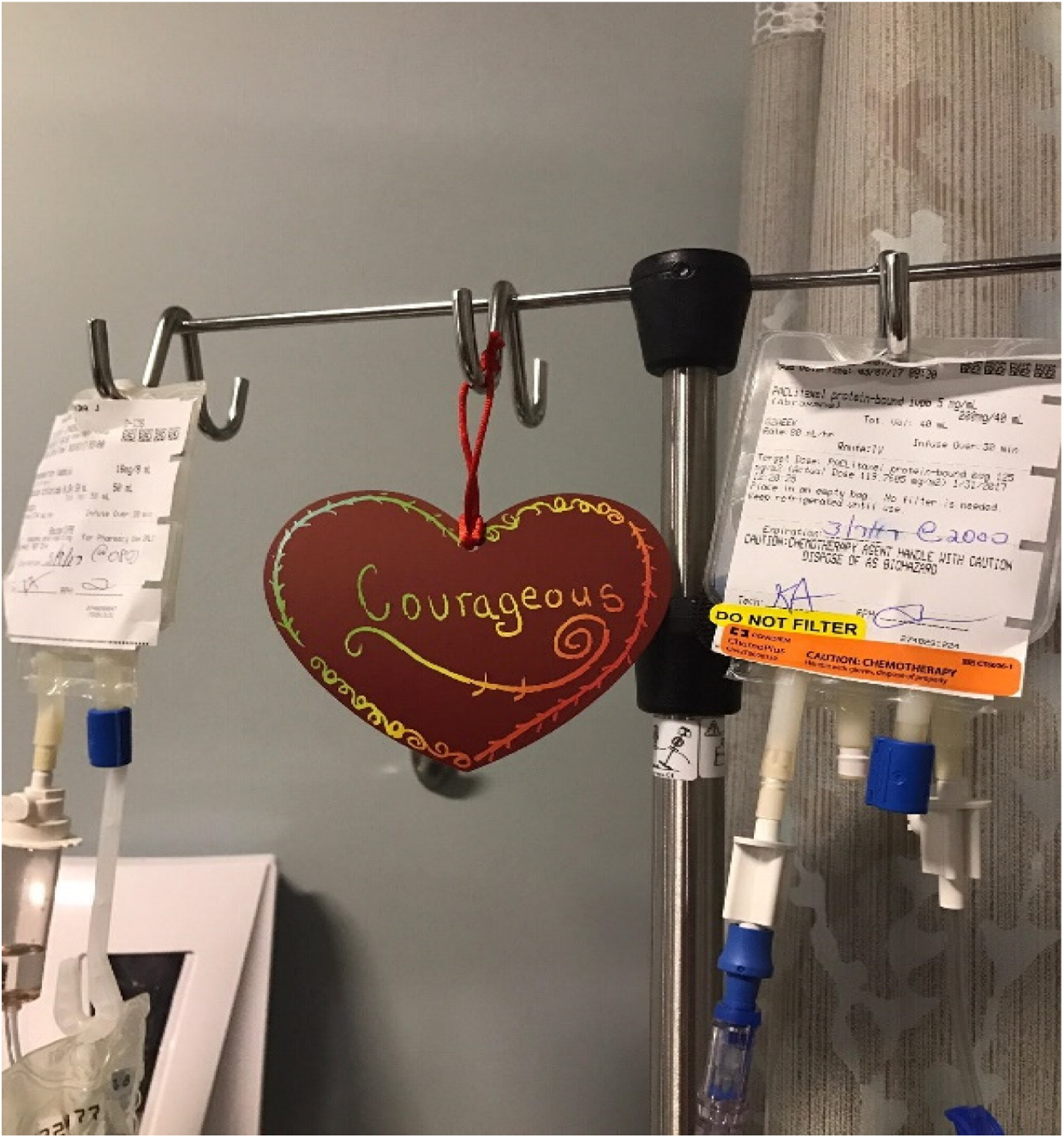
IV Pole Art.
The Cancer Awareness Topiary was created to educate and increase awareness of the many types of cancer. Cancer awareness always comes with ribbon colors and recognition of specific cancers. Figure 9 represents the many cancer diagnoses and the designated colors for those diagnoses. All disciplines at BMDACC were involved in making the topiary. Materials used consisted of a white gallery wrapped canvas measuring 12″ × 36″ and colorful pharmaceutical bottle caps supplied by nursing. Each color correlated with a type of cancer. Infusion nurses were a remarkable resource in collecting and saving pharmaceutical caps for this project. The art piece was assembled over several weeks by family, patients, and staff. It has found a home in the nursing staff lounge on the ninth floor as a reminder of why this cancer team is committed.

Cancer Awareness Topiary.
Comments From Patients
Comments from patients demonstrate additional elements for qualitative evaluation. The following notes are comments from patient art participants.
Example 1. “I have battled cancer since 2007. This is the first time I enjoyed going to the doctor. When I walk out of the building, my spirit is lighter.”
Example 2. “The arts and crafts are a great relief for any type of illness. It relieves what you are dealing with and just relieves your mind.”
Example 3. This note corresponds to Figure 9. “Hi, PM! It was a pleasure meeting you yesterday. I believe your art is part of God's ministry. I believe this because I was a benefactor of one of your ‘signs’ two weeks ago. I was diagnosed with pancreatic cancer and have held on to the scripture Joshua 1:9, which reads, ‘This is my command-be strong and COURAGEOUS! Do not be afraid or discouraged. For the Lord, your God is with you wherever you go.’ As I have done many times before, I walked into Baptist MD Anderson Infusion Center to receive my eighth chemotherapy. My nurse escorted me to my assigned chair, chair number 17. Imagine my surprise when I looked up and noticed a gold, sparkly red heart with the word courageous written, hanging from my IV pole. I believe that there is no such thing as a coincidence, and this was simply a God wink! I know without a doubt that this was an affirmation for me from God that he has heard my prayer and is with me wherever I go. Thank you for your ministry and for being such an obedient servant to Christ our Lord. God bless you.”
Example 4. “I understand the healing benefits sewing gives me, and I am using this creative healing activity as a mission to create quilts for others who are also in treatment for cancer. Textile arts have always been a comforting and healing experience for me, now I get to pass it on to others.”
Example 5 “Thank you for making me smile today.”
Quantitative Evaluation
The focus of the programmatic development project was to examine patient satisfaction preimplementation and postimplementation of the CAP in the infusion department at BMDACC. The quantitative component was the use of three examples of data collection. Data collected included the number of participants, the identity of participants (family, patient, or staff), and the Listen360® scores which is the tool used to rate patient satisfaction scores.
Participant Categories
The number in attendance and diversity of participants were measured to understand the broader engagement in the arts offerings. The participants in the art program self-identified “in Figure 10” as family, patients, or staff.
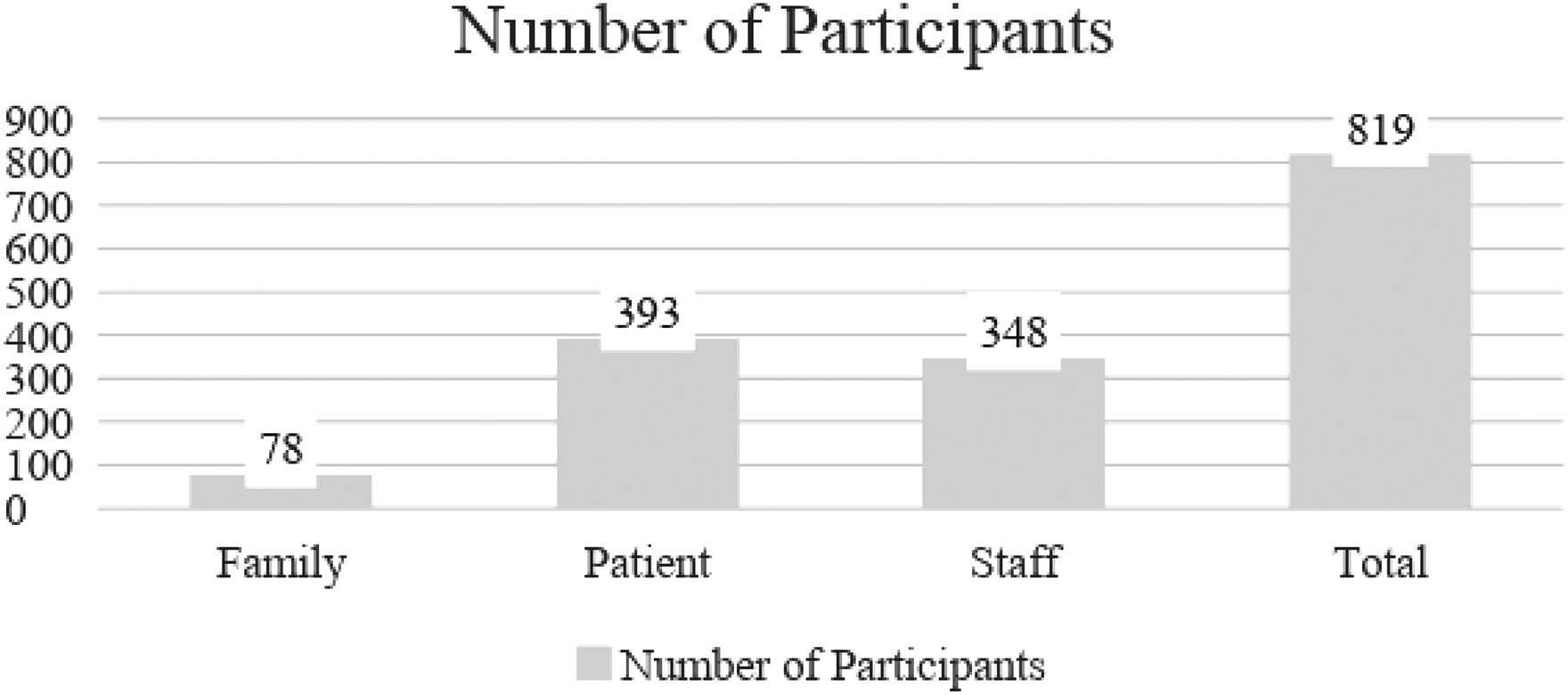
Number and diversity of participants in Caring Arts Program February 1, 2017 to October 31, 2017.
Group 1. The family category includes individuals who have a close social relationship with the patient, with or without a genetic association, or individuals working as caregivers outside the hospital to support the patient. The family participant in this project is limited to individuals affiliated with a patient in treatment at BMDACC.
Group 2. The patient category represents individuals who are participating in the treatment of cancer at BMDACC.
Group 3. The staff category includes all disciplines employed by BMDACC. In this scenario, the staff includes the housekeeper, admitting clerk, the nurse, the doctor, and others.
Listen360® Database Scores
BMDACC elected to incorporate patient feedback using the Listen360® database, allowing the capture of metrics and comments to address any performance issues or reinforce positive outcomes. The Listen360® survey was developed by Bain and Company over a decade to determine what drives companies’ success and growth. They determined that the most critical question to ask is, “Would you recommend us to friends and business associates?” The survey is designed to answer that question and explore any answers below nine on a 0–10 scale. A 9 or 10 answer is highly correlated with customer satisfaction and business success. People who rate the experience at a 9 or 10 level are referred to as net promoters (Listen360.com).
Every discharged patient received an email survey with the following questions:
How likely are you to recommend BMDACC to a friend or business associate (1–10 scale)? What did you like about your care (if responded with 9 or 10)? What could we do to improve (if responded with 7 or 8)? How did we disappoint you, and what can we do to make things right (if responded with 0–6)?
The follow-up questions depended on the answer to the first question.
The returned survey responses were anonymous unless the patient chose to be identified for follow-up. Surveys were returned to the Listen360® vendor via email for analysis and categorization. The Infusion Department scores are used in this analysis to measure patient satisfaction, both pre- and post-caring arts implementation.
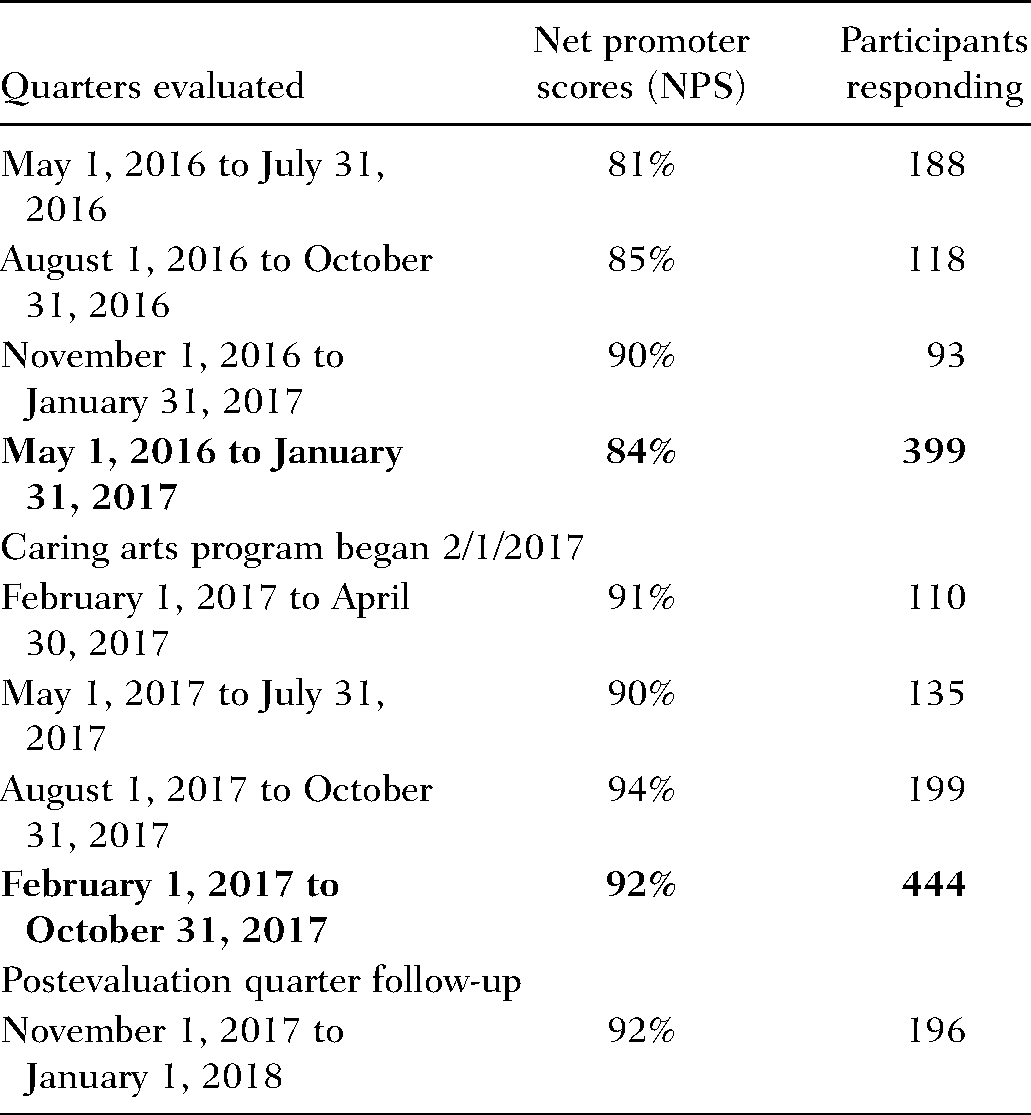
In this 18-month project, a retrospective analysis compared the infusion department's Listen360® (Table 1) with and without the CAP. Each duration of the analysis was 9 months. The preprogram and postprogram analyses were represented by three quarters of scores and a summary score. A fourth-quarter postimplementation score was also reviewed to determine if the positive changes continued. The score remained at 92%. During this period, an increase of 8 percentage points in the mean Listen360® scores occurred after the second measurement period. The returned surveys represented a nonrandom, biased voluntary response and are therefore not suitable for statistical comparisons.
Listen360® Net Promoters/Patient Satisfaction Scores for Infusion Department Pre- and Post-Caring Arts Program
Analysis
Surveys were sent out to all patients. The sample analyzed consisted of participants who chose to return the surveys, which created a self-selection bias, another limitation of the project. The inability to test statistical significance and the various confounding variables make it impossible to conclude that implementing the CAP improved patient satisfaction scores. The positive trend in the scores combined with the qualitative stories and interviews suggests that the CAP contributed to the improvement in patient satisfaction at BMDACC.
Summary and Concluding Discussion
The implementation of an art program is one of the initiatives chosen to increase patient experience scores. Other changes included revising the patient intake process and hiring an additional nurse, oncology sensitivity training, and establishing a medical records team for improved response to patient requests. These additional changes were confounding variables in the analysis of the impact of the CAP. While it can be said that providing caring arts was not the only factor that increased patient satisfaction scores in the Listen360® database, ruling out the importance of its contribution would be a mistake.
The effects the arts have on health and well-being have been well explored and demonstrate a positive outcome in most patients. The increased Listen360® scores and the qualitative patient responses after implementing the CAP align with these views. One could also consider as positive the high numbers of staff and patients who attended self-care art interventions. A commonly accepted interpretation of the Listen360® score is that a good score depends on a culture of teamwork and caring for everyone that surrounds the patient. Art interventions can be a significant catalyst to promote that culture and make a difference in patient satisfaction. The visual arts were noted to improve self-esteem, ability to cope, and an overall sense of well-being for many participants in CAP.
While many variables can influence the Listen360® scores, providing creative expression often produces a relaxed and confident spirit during high stress, which benefits the patient experience. Going beyond clinical treatment to create a more patient-centered individualized healthcare environment has proven beneficial to the patient and the supporting team. As noted, previous research demonstrates the physical and biological benefits which the arts have on the human body. A calming and soothing healthcare environment produces emotional and physical benefits for the patient (Sadler et al., 2009). This study supports Watson's caring science and the importance of creating a healing environment through the creative use of self and the artistry of caring-healing practices (Watson, 2005). The implications of the study results provided a focus to evaluate whether this environment made the patient feel more cared for, as evidenced by how patients rated the care experience through the Listen360® survey and their comments about the program.
Limitations and Recommendations
While the outcomes suggest an influencing relationship between the CAP and patient satisfaction, an exact cause and effect cannot be made due to the survey limitations and the multiple actions taken to improve the patient experience. It is likely that not all patients taking the survey participated in the CAP and inversely that not all patients participating in the program took a survey. In addition to limitations that prevented statistical analysis, a halo effect that the awareness of an arts program positively influenced the center's patient perceptions even if they did not participate, could not be measured.
Space, time, and staffing also proved to be limitations. If staffing is less than optimal, it is challenging for team members to participate in self-care activities. If there is no convenient, dedicated location or process, the program can lose visibility and participation. Moreover, if leaders do not support self-care at all levels, staff feel less free to participate. These are everyday realities of healthcare and present a challenge to any program. When the staff does not take time for self-care, it is not just the patient’s experience that is affected. The staff becomes more vulnerable to stress-related illnesses, which creates absenteeism and feeds the cycle of burnout (Khamisa et al., 2013).
Funding has been a limitation from the inception of the program over a decade ago. While healthcare practitioners and patients are open to a more holistic view of what constitutes “care,” insurance companies and federal programs have been slower to fund the programs that contribute to a holistic environment. Furthermore, while appreciated at many levels in the health system, a consistent line item in the budget, which would help grow the program, has never been secure. Funding was secured initially through the foundation and at BMDACC through support from various departmental budgets within the system. Those have been enough to sustain the Caritas Coach nurse artist on a part-time level, allowing many departments and ultimately the team at BMDACC to experience what arts interventions can do to improve self-care, morale, and the patient experience. However, it has not allowed for expansion.
The program's success has been remarkable under budget constraints and demonstrates one person's power to make a difference using talent and passion. Mandarin Newsline writes “the program has blossomed into a Baptist Health-wide initiative that provides hundreds of patients with a creative healing space and sanctuary that is proven to boost physical and spiritual healing” (Ruffes, 2016, p. 1). Tillo (2020) interviewed PM in an article “Embrace your inner artist” in Juice Magazine an online newsletter published by Baptist Health in Jacksonville, Fl. Tillo affirms each month a new project was revealed in the BMDACC lobby before the COVID-19 pandemic. For example, PM's planned activity was the creation of gratitude cards for American Heart Association Month in February. The intention was to produce and distribute handmade cards to anyone the patient considered beneficial during cancer treatment. Tillo quotes PM “Art helps patients feel alive and whole, it demonstrates caring, and value as an individual, not just a person identified by their hospital number” (Tillo, 2020, p. 3). Painting rocks is also a favorite activity in the majestic and spacious lobby of BMDACC. Images and words of encouragement are painted on rocks with inspirational messages such as “Hope” or “Just Keep Swimming.” PM places the rocks among the flowers and shrubs throughout the center's atrium garden. If the message on the rock resonates with the patient, ownership is claimed. For example, a patient who was struggling with a new diagnosis of cancer was not able to talk about it, instead, she picked up a rock scribed BELIEVE. The rock was placed in her pocket and she walked out the door. Later reporting the rock had empowered her to fight, and the rock had traveled with her the last 2 weeks inside her pocket, so whenever insecurity and fear took over, she would place her hand in her pocket and hold on to her rock. Tillo quotes PM, “Implementing a creative process helps open the door into a patient's soul, it allows them to say, this is how I’m feeling right now, and this is who I am” (Tillo, 2020, p. 2).
Implications for Advancing Future Research and Practice
Recommendations for setting up an evaluation process require a structured design, a consistent process, and adequate funding. Focusing on a specific set of patients such as BMDACC infusion patients or surgical patients narrows the population. The future research could be structured so that patients are randomized into control (no caring arts participation) and experimental (participation in caring arts) groups. All patients could then receive a validated survey that measured their satisfaction numerically and allowed for qualitative measures and input. The two groups’ results could be compared to determine if there was a difference in the measurements between them. During the study timeframe (perhaps 6 months), funding would need to be available for a full-time caring arts coordinator to ensure randomized patients were seen in a timely fashion. The rigor of this type of design would allow results to be analyzed for statistical significance and would reinforce the impact of caring arts on patient outcomes.
Afterword
Alterations in a Pandemic
Potash et al. (2020) published the results of an invited report where they asked art therapists from around the world to share the practices they adopted during prior pandemics and in the current environment. Following the Center for Disease Control and the World Health Organization guidelines, therapists adapted their practices, knowing that supporting human caring and self-expression was more critical than ever. Practices they shared included the use of public and online art and posters to deliver instructional messages and messages of hope, creating virtual studios via telehealth where they could demonstrate the art and encourage communication, and developing instructions for family art projects to encourage the expression of anxiety and telephone counseling. While the practices varied, their goals were similar-helping people dealing with anxiety, understanding the pandemic's science and truth, maintaining family relationships, and amplifying hope (Potash et al., 2020).
The CAP at BMDACC is not art therapy but shares many of the same goals and practices. The Caritas Coach nurse artist has prepared a list of recommendations for healthcare leaders to consider as this, and other art-related programs, resume. These include:
Until the CDC guidelines relax, discontinue the communal experiences such as the Lobby Table Art and the art kits available in waiting rooms. The Caritas Coach nurse artist will follow health system precautions of face mask, face shield, and rigorous handwashing with each consult. Consults will be with individuals only and socially distanced for discussion. All materials used will be individually wrapped and kept by the family/patient/staff member or discarded after use. Offer virtual follow-up to existing patients to continue to encourage dialogue and expression. Partner with other caregiver support team members-social work and chaplains-to leverage self-care programs.
As all healthcare practitioners adapt to this new reality, they recognize the extreme stress levels experienced by patients and caregivers alike. While no one knows the downstream impact of this pandemic, offering programs and experiences that encourage self-care and the vital connection to our humanity and each other will become more critical, not less.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors were paid staff during the inception of this research. There is no additional financial support authorship and/or publication of this article.