
Abstract
Introduction
Spirituality, which has been studied by different professional groups in the literature since the mid-1990s, is a complex but very important concept. The word spirituality derives from the English word “spirit,” which means soul. The origin of “spirit” is the Latin word “spiritus,” which means “breath” (Thoresen & Harris, 2002a). The concept of spirituality, which emphasizes the psychological aspect of an individual as well as the physical aspect, is accepted as a part of the individual's holistic health (Lepherd, 2015; Weathers et al., 2016). Spirituality has a positive impact not only on physical and mental health but also on other positive health outcomes such as subjective well-being, health-related quality of life, coping skills, recovery from mental illness or less addiction or less suicidal behavior (Bożek et al., 2020; Gülnar et al., 2021; Panahi et al., 2019; Unterrainer et al., 2014). Spirituality can help individuals to overcome difficulties by adapting, accepting, and understanding suffering and sadness experienced during difficult life events such as diagnosis with a chronic disease and death (Boztilki & Ardıç, 2017; Weathers et al., 2016). Individuals who are suffering often receive support from what they believe in, such as God, a higher power, and consequently, this belief affects their psychological and physical health positively (Thoresen & Harris, 2002a).
Spirituality is a complex and multidimensional concept. Our review of the literature demonstrated that the concept of spirituality is defined in several ways such as “belief in a transcendent being and power,” “universal and human values,” “rituals such as praying and meditation,” “hope and optimism,” “search for meaning,” “a strong bond to the Creator,” “love, compassion and help given to other individuals,” “meaning of life,” and “harmonizing with nature and the universe” (de Meezenbroek et al., 2012; Hill et al., 2015; Lepherd, 2015; Myers et al., 2000; Puchalski et al., 2014; “WHO | Health Topics,” 2016). In a universal sense, transcendence, relationships, meaning, purpose, fulfillment, and connection are the key concepts among these concepts (McSherry, 2016, pp. 81–83; Weathers et al., 2016). The lack of a consensus regarding the definition of spirituality brings about several challenges and limitations for studies evaluating the concept. For example, various tools have been developed in various languages by different professionals since the mid-1980s to investigate spirituality from different aspects and levels (Monod et al., 2011). Today, there are several tools used to measure spirituality. The scales focus on many different aspects of spirituality including spiritual well-being (Ellison, 1983), support, spiritual care competence ((Daghan et al., 2019), spiritual caregiving (İpek Çoban et al., 2017), spiritual meaning (Şahin et al., 2017), spiritual experience (Kass et al., 2016), perception of spiritual support (Maton, 2017), and spiritual care needs (Hall & Edwards, 1996).
In recent years, various studies have been conducted on the importance, effect, and outcome of spirituality, including patients who receive palliative or intensive care (Choi et al., 2019; Damen et al., 2021), who are in the terminal period (Gryschek et al., 2020), or who suffer from cancer (Liu et al., 2022; Palmer Kelly et al., 2022). The number of studies conducted on the spirituality levels of individuals who have nonmalignant chronic diseases and have struggled with such diseases for many years is limited. The aim of the authors of the present study was to adapt the Spirituality Instrument-27 (SpI-27©) into Turkish language and to assess its reliability and validity in individuals with nonmalignant chronic diseases. The leading contribution of the present study is that the instrument developed in English will be administered to individuals in Turkey for the first time. It also builds on prior research where the instrument was used with individuals with nonmalignant chronic disease in Europe. This will make it possible to compare the findings of the original study with the findings of the present study. On the other hand, this measurement tool to be adapted into Turkish will enable researchers to plan and implement nursing interventions accurately and effectively by assessing the spiritual needs of individuals with nonmalignant chronic diseases.
Method
Sampling and Participants
Individuals hospitalized in the cardiology clinic of a medical faculty hospital with a diagnosis of chronic disease constituted the population of the study. A purposive sample of 267 over the age of 18, who were hospitalized in the cardiology service and diagnosed with chronic disease, who volunteered to participate in the study and had no psychiatric problems or communication barriers such as not being able to speak Turkish, being confused. To perform factor analysis, the sample size should be 5- or 10-fold the total number of items in the scale (Kline, 1994). The other way recommended to determine the sample size is to consider it as “moderate” if the number of participants is 200, as “good” if it is 300, as “very good” if it is 500, and as “excellent” if it is 1000 or more (Streiner & Kottner, 2014). In the present study, data were collected from 267 individuals using SPI-27©.
Data Collection Tools
Demographic questionnaire: The questionnaire consisted of items on the sociodemographic characteristics of individuals with a diagnosis of chronic disease including gender, age, education level, employment status, and marital status.
SpI-27©
Validity and Reliability Analysis
Three types of validity were assessed: language validity, content/context validity, and construct/concept validity using factor analysis (CFA and exploratory factor analysis [EFA]). To assess the reliability of the scale, internal consistency testing (item statistics; Cronbach's alpha coefficient and Guttman split-half) was conducted.
Language and Content Validity Studies of the Scale: Language and content validity studies of the scale were carried out by considering the methods and processes recommended by the World Health Organization for the translation and adaptation of instruments into other languages (Who, 2013). The SpI-27© whose original language is English was translated into Turkish by two linguists. The terms and applications in English were stated in Turkish in the most appropriate way. After revisions were made, the scale was back-translated by an American linguist living in Turkey, who had a good command of both Turkish and English. The items in the back-translated form were compared with those in the original form and the incomprehensible expressions were revised to make the form ready for expert opinion. Davis technique (1992) was used to calculate the content validity index (CVI) for the scale items, and the experts were asked to rate the items as follows: (a) “the item is appropriate,” (b) “the item should be slightly revised,” (c) “the item should be seriously revised,” and (d) “the item is not suitable” (Davis, 1992). According to the technique, the number of experts who rated the item as “the item is appropriate” and “the item should be slightly revised” was divided by the total number of experts to obtain the “content validity index” for the item. The scale was pilot tested on a group of 10 people not included in the sample and it was determined that no changes were needed. The data obtained from the pilot study were not included in the study data.
Construct/Concept Validity of the scale: CFA and EFA were used.
Reliability of the Scale: In the reliability analysis of the scale, internal consistency analysis was performed. Internal consistency was assessed with Cronbach's alpha, Spearman–Brown internal consistency coefficients, and item–total correlation.
Data Collection
Data were collected from individuals who were hospitalized in the aforementioned cardiology clinic between 1 July 2021 and 1 December 2021, and who met the inclusion criteria. Potential participants were informed about the study, and data were collected from those who wished to participate using the paper–pencil method. The researcher collected the data from illiterate individuals by asking questions one-to-one and writing down their responses.
Data Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS 22.0) and SPSS AMOS programs. Percentage and arithmetic mean were used for the descriptive statistics in the analysis of the data. Kolmogorov–Smirnov test was used to determine whether the quantitative data were normally distributed (p = .000). Kaiser–Meyer–Olkin (KMO) analysis was used to determine whether the sample size was suitable for the factor analysis. The EFA and confirmatory factor analysis (CFA) were used to examine the factor structure of the scale. The principal component analysis method and Oblimin rotation were used in the EFA. For internal consistency analysis, Cronbach's alpha value was calculated with Spearman–Brown internal consistency coefficients and item–total correlation.
Ethical Permissions
Before the study was conducted, ethical approval was obtained from the Noninvasive Clinical Research Ethics Committee. Institutional permission was obtained from the Medical Faculty Hospital to carry out the study. The individuals participating in the study were informed about the purpose of the study and their written consent was obtained. Permission to adapt and use the scale was obtained.
Results
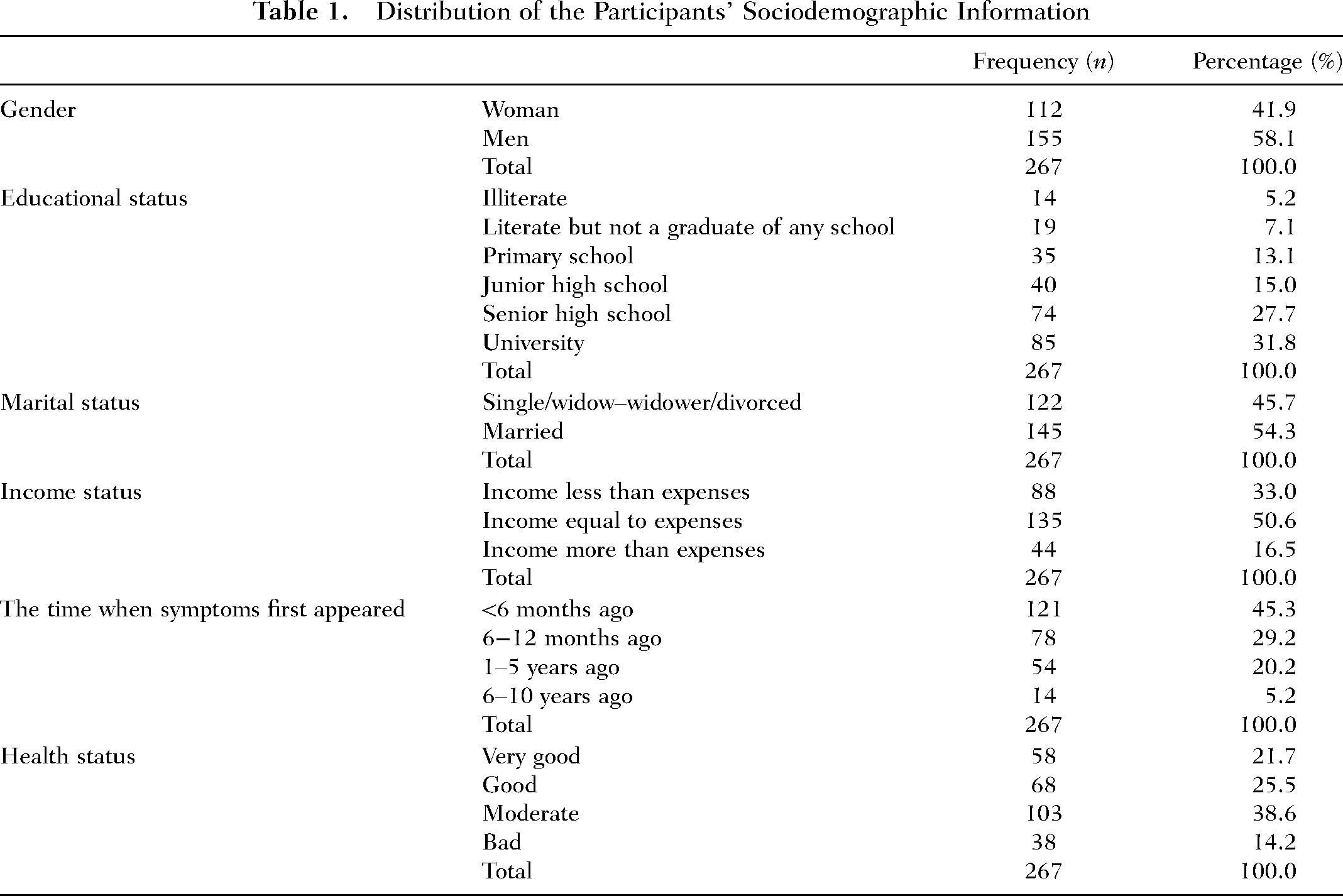
Of the participants, 58.1% were men, 54.3% were married, 68.2% had ≤12 years of education, 45.3% had a diagnosis for <6 months and 21.7% perceived their health status as very good, 38.6% as moderate, and 14.2% as bad (Table 1).
Distribution of the Participants’ Sociodemographic Information
Validity Analysis
Content Validity: For content validity, the opinions of 10 experts working in public health nursing, mental health and diseases nursing, internal medicine nursing, nursing principles, and psychology departments were obtained. After expert opinions were obtained, the CVI value was calculated as 1.00. Only two items were altered according to experts' opinions during translation. These were; Item 14 (I am free to choose how I respond to any situation in life) was revised as “I am free to choose how I would react to any situation in life.”
Item 25 (I feel a connection to nature) was revised as “I feel that I have a connection with nature.”
Construct Validity: KMO value was 0.848 and Bartlett's test of sphericity value was p = .000 (df = 153).
Results of the CFA: Fit statistics and modification values (see Table 2) of the SpI-27© were obtained through the CFA (χ2/standard deviation [SD] ratio: 1.92, root mean square error of approximation value: 0.05, standardized root mean square of residual [SRMR]: 0.04, goodness-of-fit index: 0.92, adjusted goodness-of-fit index: 0.87, comparative fit index [CFI]: 0.90). Unlike the original scale, which had a five-factor structure, the scale showed a four-factor structure in the path diagram (see Figure 1). Items 23, 24 and 25, and items 26 and 27, which constitute two separate factors in the original scale, were grouped under a single factor.
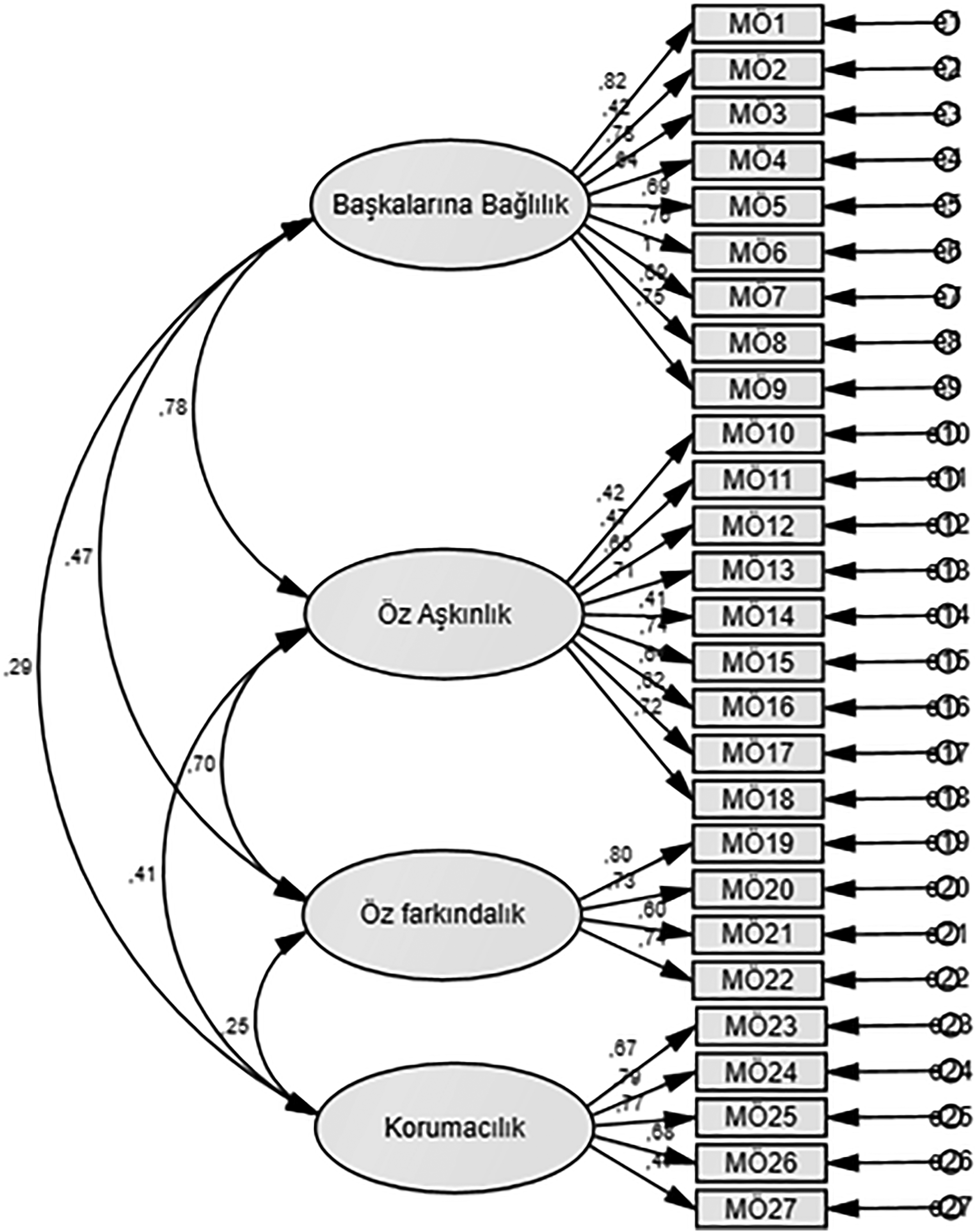
First-level path diagram of the confirmatory factor analysis (CFA) model. (Factor 1 = connectedness with others; Factor 2 = self-transcendence; Factor 3 = self-cognizance; Factor 4 = conservationism and belief).
Fit Indices of the Model
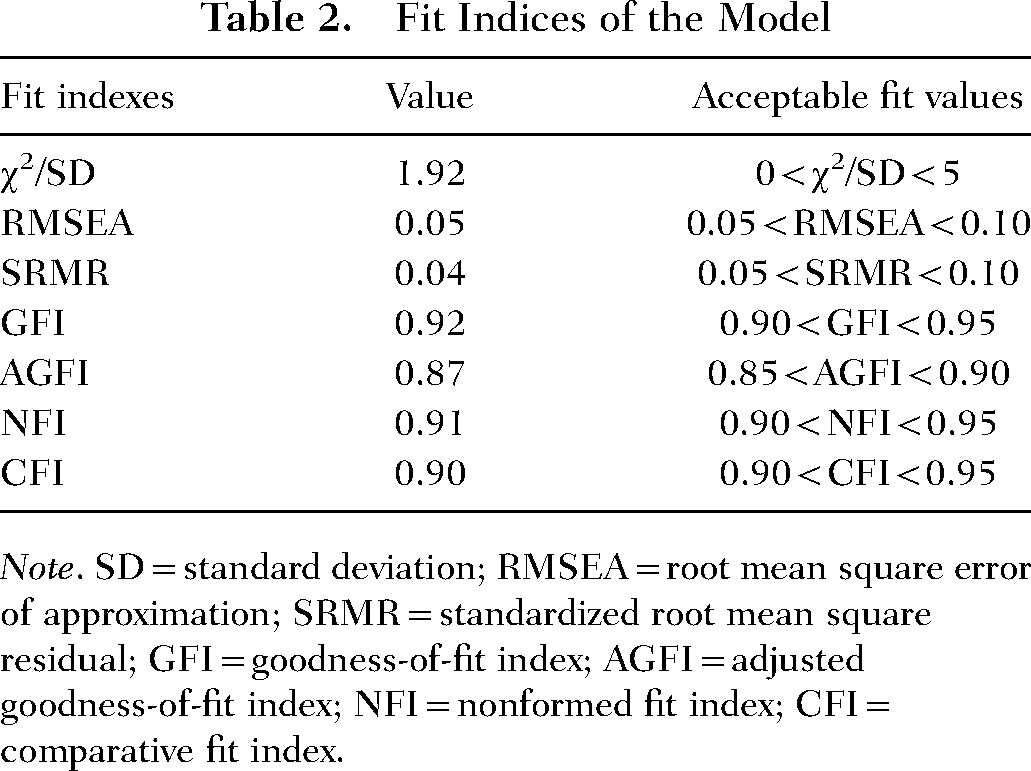
Note. SD = standard deviation; RMSEA = root mean square error of approximation; SRMR = standardized root mean square residual; GFI = goodness-of-fit index; AGFI = adjusted goodness-of-fit index; NFI = nonformed fit index; CFI = comparative fit index.
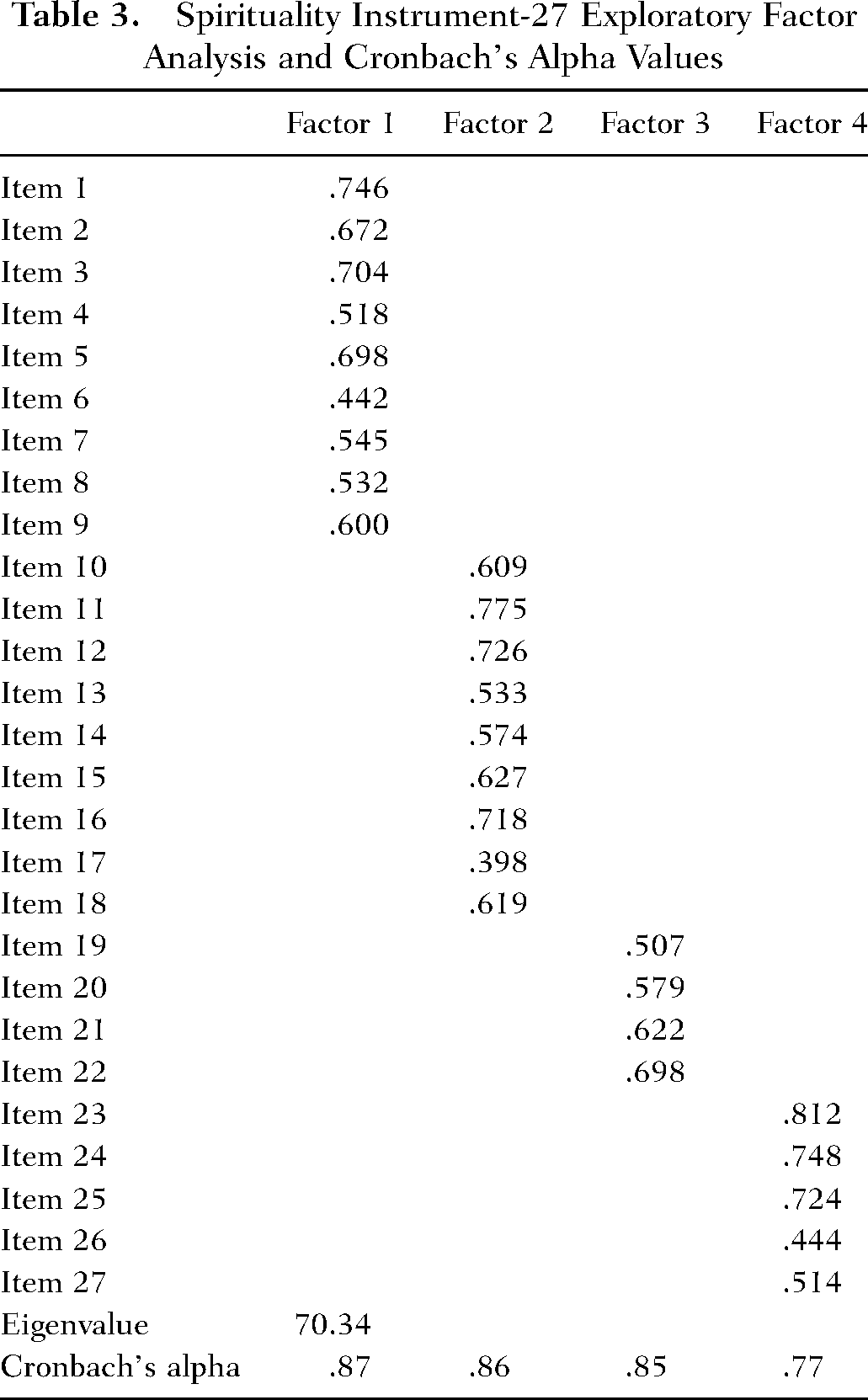
EFA Results: After the analysis, 27 items of the scale were included in the four subfactors with an eigenvalue above 1 (Scree plot; Figure 2).
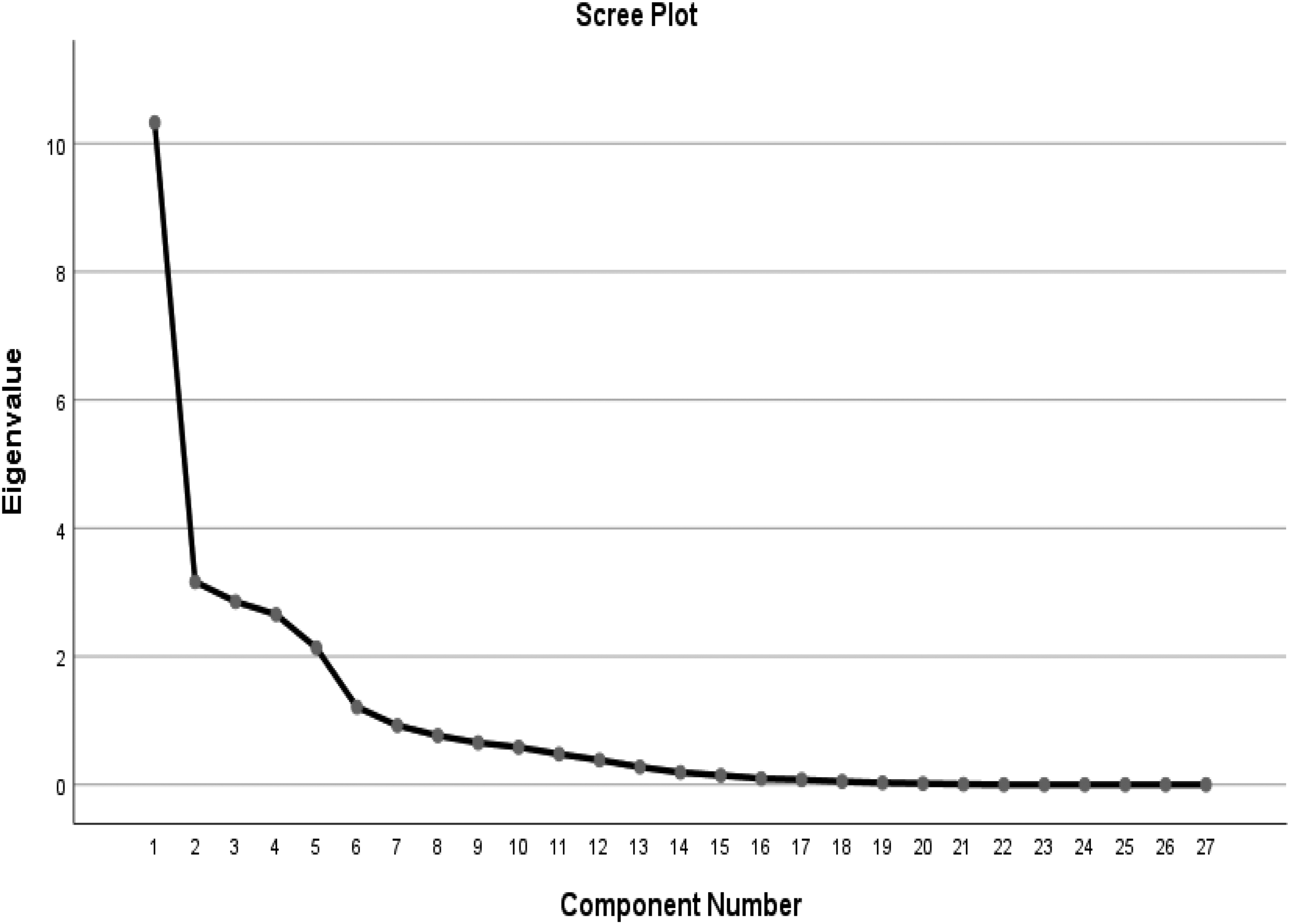
Scree plot of the Spirituality Instrument-27.
The last two subscales in the original five-factor structure scale were collected in a single factor (fourth subfactor) in the present study. Factors and their eigenvalues were as follows: 38.244 for Factor 1 (connectedness with others), 11.713 for Factor 2 (self-transcendence), 10.565 for Factor 3 (self-cognizance), and 9.827 for Factor 4 (conservationism and connectedness with a higher power). The four factors accounted for 70.34% of the total variance (Figure 2). The first factor included nine items (1st–9th items), the second factor included nine items (10th−18th items), the third factor included four items (19th−22nd items), and the fourth factor included five items (23rd–27th items). The highest and lowest item factor loadings of the scale were 0.812 and 0.398, respectively.
The correlation analysis was performed to determine whether there was a significant relationship between the overall SpI-27© and its subfactors. According to the result of Pearson correlation analysis, there was a significant positive correlation between all the subdimensions of the scale (p = .000).
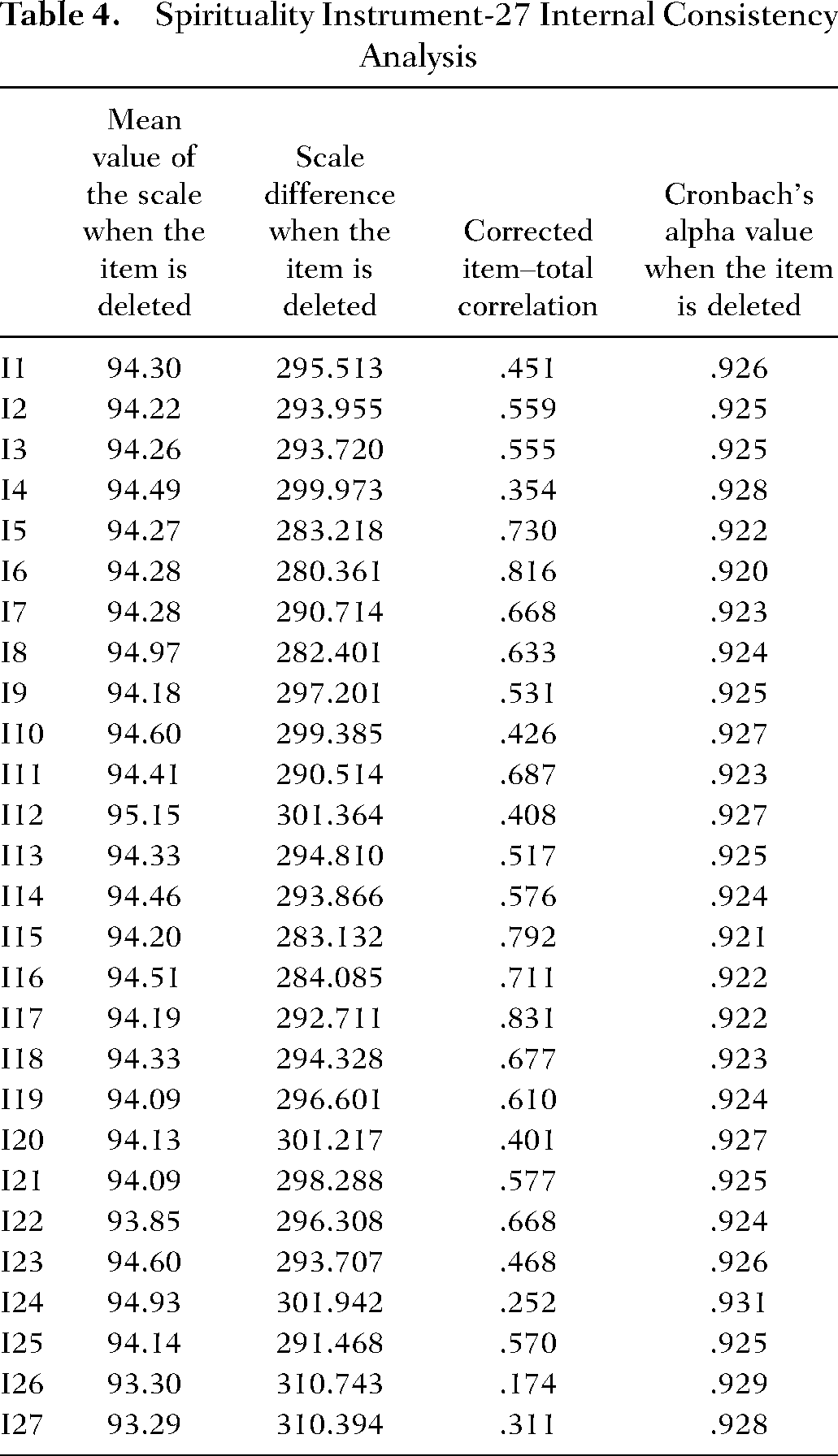
In the item total correlation analysis performed to confirm internal consistency, item–total correlation scores of the scale ranged between 0.174 and 0.831. The item with the lowest item–total correlation was the 26th item. In the CFA performed by including this item, it was left in the scale because the goodness-of-fit index values was good, factor loading was 0.444, and Cronbach's Alpha value of the scale (0.929) did not change when the item was deleted.
Internal Consistency: Given the reliability coefficients of the subdimensions of the scale, the fourth subfactor had the lowest Cronbach's alpha coefficient (α=.773), whereas the first subfactor had the highest Cronbach's alpha coefficient (α=.877). Cronbach's alpha coefficient for the overall scale was α=.927 (Table 3). The results of the internal consistency analysis according to the items are shown in Table 4. If an item is deleted from the scale, Cronbach's alpha coefficient varies between 0.92 and 0.93.
Spirituality Instrument-27 Exploratory Factor Analysis and Cronbach's Alpha Values
Spirituality Instrument-27 Internal Consistency Analysis
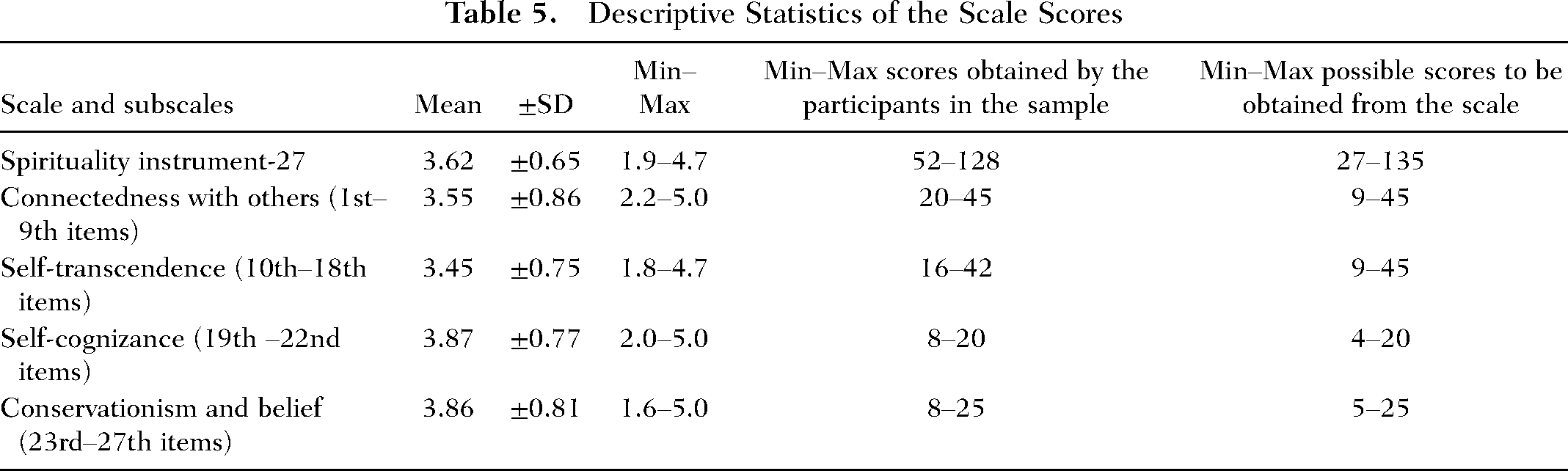
The Distribution of Findings Regarding the SpI-27© and Its Subscales: The mean scores obtained from the overall scale and its subscales were as follows: 97.91 ± 17.79 (overall scale), 32.00 ± 7.81 (connectedness with others subscale), 31.06 ± 6.76 (self-transcendence subscale) 15.50 ± 3.09 (self-cognizance subscale), and 19.33 ± 4.09 (conservationism and connectedness with a higher power subscale; Table 5).
Descriptive Statistics of the Scale Scores
The results of Hotelling's T2 analysis indicated that the mean scores were different (Hotelling's T2 = 63.80; p = .001), that the participants displayed different approaches while answering the items, and that their responses were reliable. The t value for the differences between the item scores of the 27% lower and upper groups determined according to the total scores was −64.335 (p = .000; SD = 88).
Discussion
The aim of this study was to adapt the “Spirituality Instrument-27,” developed to assess the spiritual state of individuals with chronic diseases, to the Turkish language and culture, and to evaluate its validity and reliability. Most of the participants were men, high school or university graduates, married, had an income equal to their expenses, were diagnosed with heart diseases less than a year ago, and perceived their health as good.
To determine whether the items in the measurement tool constituted a sample group representing the feature to be measured, expert opinions were obtained. Expert opinions were analyzed using the CVI (Zamanzadeh et al., 2015). After the opinions of 10 experts were obtained, the CVI value was calculated as 1.00. The experts agreed on all the items.
KMO analysis was used to determine the adequacy of the sample size for factor analysis. For a sufficient sample size, the KMO value is expected to be more than 0.80 and close to 1 (Sencan, 2005). The KMO value was 0.884 in the original study and 0.84 in the present study, which indicates that the sample size was very good.
The fit statistics and modification values obtained through the CFA indicated that the model was acceptable. As stated in the literature, if the goodness-of-fit values obtained through the CFA is ≥0.95, it indicates a perfect fit, and if it is between 0.90 and <0.95, it indicates a good fit (Harrington, 2009). According to the values obtained in the present study, the fit of the scale was at a good level. These values also indicated that the four-factor structure of the connection diagram was also suitable.
The scree plot graph and eigenvalue values indicated that the scale items were gathered in four subfactors. Unlike the original scale (Weathers et al., 2020), which had a five-factor structure, the scale showed a four-factor structure in the present study, and items 23, 24, and 25 and items 26 and 27, which constituted two separate factors in the original scale, were gathered under a single factor in the present study. In the English version, the scale had 27 items and five subscales. Although the Turkish version of the scale has 27 items, it consists of four subdimensions. The first three subdimensions are the same as in the English version (connectedness with others, self-transcendence, and self-cognizance), and the fourth and fifth subdimensions are gathered in one subdimension (conservationism and connectedness with a higher power). The fact that the study sample consisted of individuals in a country most of whom have a strong belief in God may reflect the combination of conservationism and belief in God. According to the results of the EFA, the four-factor structure explained 70.34% of the total variance of the scale. The higher the variance rates obtained through the EFA (50% or more) are, the stronger the factor structure of the scale is (Hair et al., 2008). In Weather's et al study (2020), the five-factor structure accounted for 60.63% of the variance. The fact that the variance rate was ≥50% in the present study showed that the factor structure of the scale was strong and it was as high as that in the original study.
According to the principal component analysis method used in the EFA, in the four-factor structure scale, the first factor included nine items (1st–9th items), the second factor included nine items (10th–18th items), the third factor included four items (19th–22nd items), and the fourth factor included five items (23rd–27th items). The highest and the lowest item factor loadings of the scale were 0.812 and 0.398, respectively. In the original study (Weathers et al., 2020), factor loadings in the five-factor structure ranged from 0.453 to 0.953. Factor loadings of ≥0.40 indicate that the scale has a single-factor structure. In this context, it can be said that the scale items together measure the individual's spirituality level as a whole. Pearson correlation analysis of the SpI-27© and its subfactors showed that there was a correlation between the scale and its subscales, varying between 0.56 and 0.88, and that each item was associated with measuring spirituality (Hair et al., 2008).
In the present study, item–total correlation scores of the scale ranged between 0.174 and 0.831. In item–total–score correlations, values ≥0.40 indicate very good discrimination, values between 0.30 and 0.39 indicate good discrimination, and values between 0.20 and 0.29 indicate that the item needs revision (Tavsancil, 2019). In the present study, item 26 had the lowest item–total correlation. According to the results of the CFA, the goodness-of-fit index values were good, factor loading was 0.444 and the Cronbach's alpha value of the scale was .929; therefore, the item was not deleted. It is recommended that this item should be handled with care in future studies.
In scale adaptation studies, it is assumed that the higher the Cronbach's alpha coefficient is, the more consistent the items in the scale are and that the factor is comprised of the items of the same feature. Thus, the alpha coefficient is expected to be as close to one as possible (Sencan, 2005). In our sample group, Cronbach's alpha value of the scale was .927 indicating that the scale is highly reliable. In the original study (Weathers et al., 2020), Cronbach's alpha coefficients of the scale ranged between 0.823 and 0.911. The Spearman–Brown test also indicated that the level of internal consistency was high. The Turkish version of the scale had high internal consistency as did the original scale.
The results of Hotelling’s T2 analysis indicated that the mean scores for the items were different, that the participants displayed different approaches while answering the items, and that the responses were reliable. The difference between the item scores of the 27% lower and upper groups, in which the discriminant validity of the overall scale and its subdimensions was tested, also indicated that the scale had discriminant validity.
The mean score obtained from the overall SpI-27© was 97.91 ± 17.79 in the present study and 101.84 ± 15.70 in the original study (Weathers et al., 2020), which indicates that the participants’ spiritual levels were high in both studies.
Limitations of the Research
The present study was carried out with individuals who were hospitalized in the aforementioned cardiology clinic, and because the patients were hospitalized in the clinic for 2–5 days, it was not possible to collect data from the same individuals again, so we could not perform the test–retest analysis. It is recommended that in future studies including individuals with different nonmalignant chronic diseases, the stability of the scale over time should be tested. The spirituality measurement tools available in the literature are either specific to a field (cancer, HIV, palliative, etc.) or measure the need for spiritual care, or generally measure health professionals’ opinions/perceptions of spirituality. Therefore, we could not compare the results of the EFA and CFA analysis of our study with the results of other tools measuring spirituality in the literature. Because the study was conducted in a country where the rate of the Muslim population is 89.5%, the participants’ characteristics such as religion, ethnicity, etc., were not questioned. Therefore, it should be taken into account that the answers may vary if a study includes individuals of different religions and ethnic and cultural characteristics. In the future, it is recommended that the validity and reliability of the scale should be tested in studies including individuals with different ethnic, cultural, and religious characteristics and different chronic diseases and that it should be used as a measurement tool in studies conducted on spirituality.
Conclusion
The results of the present study demonstrated that the SpI-27© was statistically valid and reliable in determining the level of spirituality in individuals hospitalized in the cardiology clinic. This study demonstrated the importance of diagnosing spirituality, determining spirituality needs in different cultures and ethnic groups, and testing the reliability and validity of cultural-specific measurement tools in future studies. The scale can be used as a valid tool to determine the level of spirituality in patients with a chronic disease.
Whether they are religious or nonreligious, spirituality is extremely important for individuals and is even more prominent in cases of deviation from health. Rapid identification of problems related to spirituality, to which various meanings are attributed in different cultures and religions, and provision of immediate help will increase the effectiveness of healthcare services. In addition, determination of the spirituality level in individuals with chronic diseases will be beneficial for nurses and other healthcare professionals if they are to provide holistic health care.
Directions for Future Research
Future research may be conducted to test the SpI-27© in individuals diagnosed with chronic diseases of different languages, ethnicities, and cultures. In addition, the SpI-27© can be used in religious and nonreligious populations to explore the relationship between spirituality and health-related variables such as quality of life, coping with stress, adjustment to chronic illness, and satisfaction with care. The conceptual framework that guided the SpI-27© can be used to enhance healthcare professionals’ understanding of spirituality and its key dimensions.