
Abstract
The first cases of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) in the United States were reported in Washington State in January 2020. By March, Americans were made aware of the environmental threats and swiftly responded to the viral spread. For example, primarily in-person classes at the university abruptly became exclusively online by mid-March 2020. Beyond the classroom, the abrupt and dramatic shift caused disruptions and made a historical impact on many lives.
Concerns about whether these experiences elicited positive coronavirus disease 2019 (COVID-19) cases, healthy responses remained in question. At the outset of the pandemic, nurses expressed uncertainty and worry, never anticipating or experiencing the pandemic paths they were inevitably to take. One of these researchers was in the midst of preparing to offer a bachelor's level course for registered nurses (RNs) when the call went out by the university administration to teach via virtual instruction. When it became apparent that this new virus was creating a major public health crisis, with clear implications for nurses’ fight for lives, the course instructor assigned the RN students to record journal reflections as one of their course requirements. Clearly, history was in the making with what these RNs were to endure in the weeks ahead in their clinical practice and professional lives.
Nurse educators have long required students to engage in the act of journal writing to enrich clinical learning experiences. The skill of writing enables one to cope by processing their emotions of event(s) in a systematic way (Edwards et al., 2019). Research has shown reflective journaling promotes critical thinking, emotional growth, and effective coping skills which may shape individuals’ future professional practice (Edwards et al., 2019; Brown et al., 2022). Additionally, reflective journaling approaches may offer holistic health benefits to combat insomnia, stress, and pain both in the mental and physical sense. For example, a journaling method, coined as expressive writing, enables individuals to write about their stimulating lived experiences without giving much concern to proper grammar, punctuation, or style (Pennebaker, 2018). This therapeutic approach attempts to minimize judgment associated with standard writing conventions by promoting informal writing of one's thoughts about a particular situation that the individual is grappling with to reduce stress and anxiety (Pennebaker, 2018).
Study Purpose, Objectives, and Design
Researchers anticipated these reflective journals, completed by RNs working in the early days of the COVID-19 pandemic, would convey meaning in their effect on their personal and professional lives. The purpose of this qualitative descriptive study was to analyze and interpret experiences shared in journal reflections by RN-BSN students who were working at the bedside early in the COVID-19 pandemic. These journals illuminated nurses’ stories from a crucial “moment in time” for a profession facing an overwhelming crisis. A secondary outcome was for journals to serve as memoirs of nursing history as nurses shared first-hand experiences from early weeks of the pandemic. Insights gained from these journalized accounts may become profoundly important for the nursing profession.
The study design for this research was based upon Thorne's qualitative interpretive descriptive approach (Burdine et al., 2020; Thorne et al., 1997). Interpretive description is foundational for relating nursing knowledge with potential use among interdisciplinary qualitative approaches. In this study, the journals served as open-ended blank slates inviting participants to share themselves, including physical, emotional, mindful, and spiritual responses, and allowing others to view the world of pandemic nursing through their lens. Gathering data from different sources, such as journals, aligns with Thorne and is an acceptable qualitative research data source that may be used to generate practice knowledge in nursing. The researchers, guided by Thorne's iterative process, reviewed, coded, and then dwelled with the data for several weeks as thematic meanings and an overall interpretation emerged (Thorne et al., 1997).
Methods
Data Collection: Journal Assignment
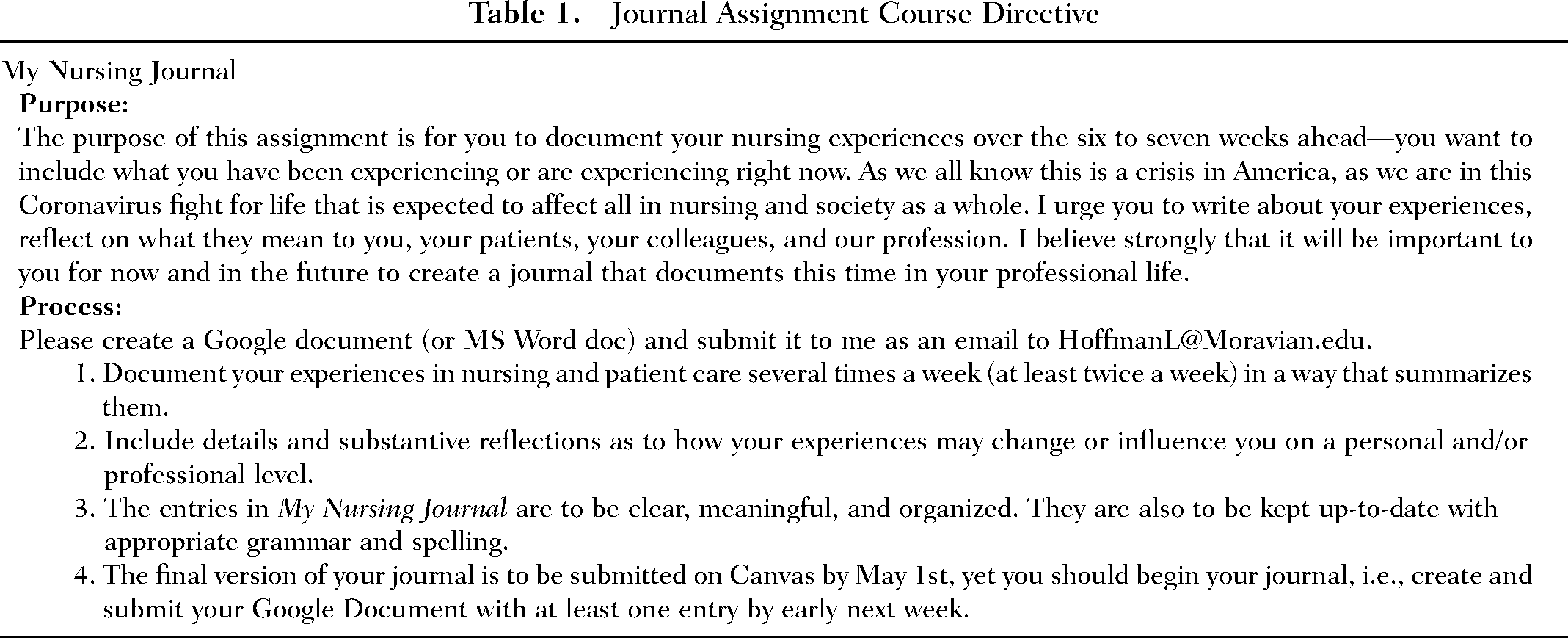
Eighteen (N = 18) RN students enrolled in a baccalaureate-level nursing course journaled on their personal and professional lives during the session. The journal assignment (see Table 1, p. 31), required students to write a minimum of two journal entries each week. Students were provided with a personalized online folder, accessible only to them and the course instructor, which contained dated journal entries and provided background information on the intention of capturing their nursing experiences of living and working during this time. Recognizing this would be an intense, stressful time for RN students working in healthcare while simultaneously attending class, grading was completion-based, meaning simply that their narrations be recorded in the online document. However, RN students were empowered to consider in the text of their journals, the meaning of the experience for what was certain, even then, to be historic times. Below is the instructor's introduction from the assignment directive which advised RNs of the importance of the journal assignment: As we all know this is a crisis in America, as we are in this Coronavirus fight for life that is expected to affect all in nursing and society as a whole. I [instructor] urge you to write about your experiences, reflect on what they mean to you, your patients, your colleagues, and our profession. I believe strongly that it will be important to you for now and in the future to create a journal that documents this time in your professional life.
Journal Assignment Course Directive
Ethical Considerations of the Study
Researchers obtained approval from the university's institutional review board (IRB) as an exempt study. Written consent was obtained to analyze the journal assignment entries after participants reviewed the consent form which outlined the study purpose, as well as associated benefits and risks to study participation. Procedures taken to uphold participants’ anonymity and confidentiality during study participation were described due to the potentially sensitive information disclosed in the journal. Consenting study participants were assured any identifying information associated with their journals would be redacted by the course instructor, and the two other researchers would not know journal authors. Three students from the original class of 18 did not reply to the email request, and these three students’ journals were not included in data analysis. Data were stored as per the approved IRB protocol.
Data Analysis
Interpretive description guided journal analysis. This approach varies from conventional methods in order to address the unique elements of nursing's epistemological approach in the fluidity of human experiences of health and illness (Thorne et al., 1997). One departure of interpretive description from tradition is the absence of bracketing, the process used in clearing from awareness one's biases, beliefs, or expectations about the topic under study. The research team experienced similar daily situations as the study participants. Therefore, Thorne's interpretive descriptive approach was used for the study. This approach permitted researchers to process their biases as they analyzed nurses’ journals during the plunge into the COVID-19 pandemic.
In following Thorne's process, the researchers began the analysis by carefully reading and absorbing journals in their entirety in order to gather the gestalt of the participants’ experiences. To maintain study rigor, the researchers engaged in reflexivity by reading and interpreting the first four journals separately. The meanings behind the written words were discussed among the research team. These discussions helped team members during analysis recognize similar or differing perspectives. Read and analyzed sequentially, the researchers individually analyzed the remaining 11 journals.
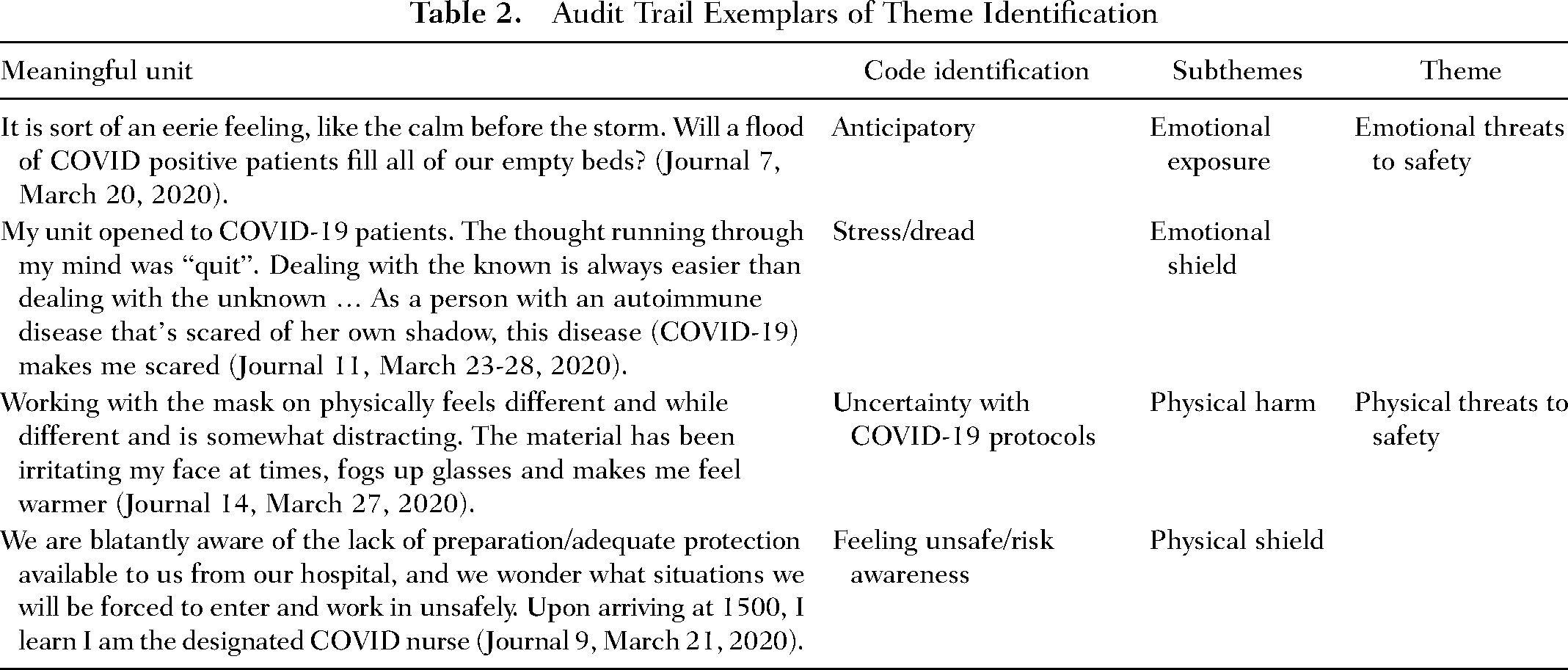
This process established congruence between study investigators which led to the beginning identification of codes. Significant statements were extracted from each journal and then reduced to meaningful units and codes. The researchers identified patterns within the codes to reveal emergent themes (see Table 2 for exemplar). Researchers placed these units of information on their transcript and then on the master codebook after researchers reached consensus. Triangulation of investigators was established to reach consensus through clarification and validation sessions. This was achieved by discussing the emergent codes and naming themes in accordance with interpretive descriptive design.
Audit Trail Exemplars of Theme Identification
Results
Researchers collectively analyzed 161 passages (38,954 words) from the 15 journals. The journals, running commentaries written over a 6-to-7-week interval, coincided with the rapidly changing and uncertain schematic of both professional and personal lives of nurses working in health care during the early stage of the pandemic. The following emergent themes and sub-themes were Theme 1: Physical Threats to Safety: Physical harm and physical shield, Theme 2: Emotional Threats to Safety, Theme 3: Workplace Culture: Health care teamwork and accomplishment of work, Theme 4: Healing Energies, and Theme 5: Professional Identity: Questioning one's purpose in the moment and professional development.
These five themes along with their emergent sub-themes represented the crucial nature of the collective footprint nurses experienced in the early weeks of what became a global public health crisis. According to yogic philosophy, feet are a stable surface where energy arises. This life-force-energy known as the Pada Bandha promotes stability through the balancing of energies within internal body systems and organs (Ekhart, 2018; Iyengar, 1966). Researchers correlated nurses’ activity expenditures during the COVID-19 pandemic to this concept as they sought balance within their personal and professional lives. The footprint also symbolized ways nurses navigated their experiences and serves as a map to guide nurses’ future paths.
Theme 1: Physical Threats to Safety
The foundation of all journal narratives related to concepts of physical safety. As the numbers of COVID-19 positive cases increased, nurses became aware of their own risk of contracting the coronavirus. The availability and use of protective protocols and equipment were frequently changing at first, and their effectiveness was uncertain. The concept of masking for safety and protection from harm was uncovered. Although personal protective equipment was intended to shield them from the physical effects of the virus, masking led to possible physical harm and distress. The reflections below portray this theme of nurses’ concern about their physical safety from harm and shielding perspective.
Physical Harm
It is difficult to breathe in an N95 and 4 hours in full protection means 4 hours I am not breathing properly, without peeing, without drinking water, and without knowing what is going on outside of your one room. As an ER nurse who is aware of everything going on around you, it is isolating” (Journal 9, March 23, 2020). Working with the mask on physically feels different and while different and is somewhat distracting. The material has been irritating my face at times, fogs up glasses and makes me feel warmer (Journal 14, March 27, 2020). Working in a mask the entire day has become a challenge. It is hot and exhausting breathing through that thing while talking for most of the day! (Journal 2, April 3, 2020).
Physical Shields
I am not wearing an appropriate mask, will I contract the virus? What if I did and I’ll give [it] to my family? (Journal 15, April 11, 2020). I hate having to wear a mask and goggles all day, but I know it’s for my own protection. I also question this method of protection because of the way health care workers dress in other countries with a whole outfit on, but that’s besides the point (Journal 4, March 30, 2020). I wore the same N95 mask all shift, cleaned it with wipes, and got a facial rash from the cleaner. I took care of 20 + suspected COVIDs and each time wondered at which point I was most exposed. When home I stripped down on my porch, and leave those scrubs outside until I had to wash them—who knows how long the virus lives for sure? No one person if you consult the experts. I look forward to my 0330 shower to have every last germ washed off before getting into bed, where I’ll lay my head for five hours until I wake back up and face the world for another day. Today—my first-day shift! (Journal 9, March 21, 2020).
Theme 2: Emotional Threats to Safety
This theme permeates journals throughout the data collection weeks. Collective review of early journal entries revealed a pattern that researchers interpret as a protective dynamic against exposure to a threat, risk, or uncertainty. Nurses described COVID protocols, job status, pandemic patterns, and anticipation of or actual trauma or disaster in this domain. Two subthemes emerged and were best described holistically as emotional exposure and emotional shield. Emotional exposure captured risk awareness of the threats and the uncertainty of them. Emotional shielding referred to the unknown consequences of COVID and actions impacting self and others.
Emotional Exposure
It is sort of an eerie feeling, like the calm before the storm. Will a flood of COVID positive patients fill all of our empty beds? (Journal 7, March 20, 2020). I’m paranoid about being positive that I’ve been taking my temperature more than once a day. It’s been normal so far (Journal 11, March 28, 2020). I am seeing so many sad stories. I am living it enough at work. … but right now, I am going to work daily, fearing “what will go wrong today? (Journal 1, March 31, 2020).
Emotional Shields
Nurses struggling to deal with, and shield, their emotions of fear exemplifies the connection between mental awareness and emotional fear: My unit opened to COVID-19 patients. The thought running through my mind was “quit.” Dealing with the known is always easier than dealing with the unknown. Every corridor was chatter about safety. As a person with an autoimmune disease that’s scared of her own shadow, this disease (COVID-19) makes me scared (Journal 11, March 23–28, 2020).
When I pick the baby up after work, I’m petrified to hold her with my scrubs on and even worry about my shoes once I get home. I worried about carrying pathogens from work inside my home, but I never took it as seriously as now (Journal 2, March 27, 2020).
I became much better as a nurse advocating for my patients. Usually, I find my gut feeling to be right, this time I hope I am wrong … I received an email that room [number] is now rule out COVID. I feel angry, sad for him, scared for my family and coworkers, and uncertain of the future. We work at a hospital, and this is just the beginning, and I am already potentially exposed? (Journal 1, March 19, 2020).
A nurse showed compassion by assisting a patient to find closure in saying goodbyes to loved ones. … her anxiety was elevated that she called her children to say final goodbyes. I couldn’t imagine calling my children to say goodbye. I’m going to be dead by the time you see me. It broke my heart. I gave her a hug and asked her to do me a favor and write letters (Journal 11, March 22- 28, 2020).
Theme 3: Workplace Culture
As nurses faced a multiplicity of concerns and challenges during this time, they began to voice in their journal strength in shared work. Several codes represent this theme including healthcare teamwork and accomplishment of work. These ideas can be seen in the following participants’ comments, which represent two distinct sub-themes; healthcare teamwork and accomplishment of work.
Healthcare Teamwork
Nursing care teams demonstrated collaboration amongst each other to support patient care activities and each other as professionals. Coming together as a team, even during this time of social distancing is extremely important, making support available, educated, and aware is important for everyone to get through this together (Journal 14, March 23, 2020).
Maybe I was a little emotional because I just worked a 16 h shift the day before and I was going on 12 h, but to be chewed out instead of caring for our patient? After a good quick chat with my charge nurse, she gave me the courage to stand up to this doctor I felt was out of line (Journal 1, April 1, 2020).
We are cross training nurses for ICU, so there are some benefits to this pandemic. Everyone is excited for all this to be over soon, and we are receiving incredible support from our families and coworkers (Journal 8, April 1, 2020).
Although teamwork was highly valued, sometimes COVID impacted the workplace unfavorably in terms of staffing and interprofessional collaborations. The following examples highlight these lived concerns. So, at this time it was decided that PCAs are not allowed in the room leaving the RN responsible for all the work (Journal 4, March 26, 2020).
We will be working with a reduced number of staff. The reasoning is that there is a floor at (institution) designated to patients infected with COVID and taking from other floors will help with the increased demands of this pandemic. As a result, charge nurses will be working with full assignments … Working as a charge in full assignment (6 patients) is not only tedious, but also prevents me as a charge nurse from being a proper resource to my floor nurses (Journal 13, March 29, 2020).
The physician wasn’t worried at all. He was not worried that I told him our patient has not urinated since 9 am and was not himself. Instead, this doctor messaged me back “Why are you messaging me this? You need to inform [the hospitalist]. I am here for emergencies only. It is 2:21 am” (Journal 1, April 2, 2020).
Accomplishment of Work
Participants shared how they experienced recognition for the work they did during the COVID pandemic. These internal and external forms of acknowledgment and their processing of them strengthened their work ethic and commitment to patient care. There are a lot of horror stories but also a lot of encouraging happy stories. Also today, there was an appreciation parade at my hospital. Fire trucks, ambulances, and police cars from all over drove around the hospital flashing their lights and playing their sirens to show us support (Journal 4, April 14, 2020).
We arrived at the front entrance of the hospital and walked outside and he [security] said see, pointing and as I looked down there were sidewalk chalk drawings of praise and thanks for being healthcare heroes. I immediately took pictures and shared them with the leadership team. What a way to end the day (Journal 12, April 4, 2020).
I had my yearly eval this morning and it was something I needed to hear. During a time of stress and sadness, for my manager to tell me how important I was, made me feel like I am right where I belong. Through all the sadness, I wouldn’t change what I do for anything (Journal 1, April 21, 2020).
Theme 4: Healing Energies
Nurses shared how their experiences were an energizing catalyst that aided healing themselves and others throughout the pandemic. Connections with the community brought a sense of renewal. Nurses identified moments of hope as they celebrated patients’ health. This was apparent in the stories highlighting human acts of kindness. On a good note, our first extubated COVID-19-positive patient was discharged today! My supervisor was the one who wheeled him out. They took a video, and everyone was clapping and crying. It was really uplifting to think that there is hope for this virus and people can get better” (Journal 4, April 6, 2020).
She [charge nurse] went on to say how grateful she is for my help on the weekends and explained she just told her boss she didn’t think she would be as good at being in charge without my support. I thanked her by telling her this warmed my heart. It’s nice to be appreciated (Journal 12, April 18, 2020).
Despite emotional turmoil, nurses found meaning and a space of balance as they continued to care for patients who were struggling with life and death. The amount of death I have seen, doesn’t compare to the amount of people I have been able to help by advocating for them, finding issues before they became rapid, and being there during the scariest times of these patients’ lives (Journal 1, April 21, 2020).
While I wish I saw less dying in the hospital, I find myself requesting these patients. It means a lot to be able to care for them in their final moments, in hopes they feel a little more at peace with someone by their side (Journal 1, April 27, 2020).
To be honest, I don’t really believe in a “higher power,” but I felt like I was meant to take care of those two patients that day (Journal 4, March 23, 2020).
One nurse in a personal battle with COVID shared the experience of finding meaning in the complex survival seesaw through an internal supportive community.
[My partner] refused to allow me to accept it and asked me to keep fighting … I didn't want him [partner] giving up on me but here I was giving up on myself. Some days I wondered … should I start writing letters to my family and friends. It made me depressed and even more so when my daughter suggested that I start writing letters. It was as if they knew something I refused to see (Journal 11, March 31, 2020).
Theme 5: Professional Identity
Professional identity resonated with nurses, and its importance was apparent in many journal entries throughout the time of the reflective writing assignment. Aspects of identity were inclusive of roles of advocate, practitioner, collaborator, and leader. These roles were layered upon each other, blending into a mosaic of characteristics, such as being purposeful, selfless, responsible, along with fatigue, powerlessness, and uncertainty.
Participants wrote in their journals about self-doubt or uncertainty in reference to their patient care, despite many years as practitioners. Their comments depict a mixture of emotions regarding growth in their professional identity. Two subthemes, questioning one's purpose in the moment and professional development, were apparent.
Questioning One's Purpose in the Moment
Nurses shared a newfound perspective on professional identity and how their role changed during the early weeks of the pandemic. I was able to spend a day in the ER with a nurse … The experience, although scary, was also very insightful. I was walked through the part of the department that was transitioned for the COVID screenings and we were given our roles in detail. I am very proud to be helping on the front lines and I am hoping that I can take away something very valuable from this experience (Journal 6, April 5, 2020).
Nurses held professional expectations for themselves that sometimes presented a conflict. One nurse discussed the role of being an advocate but felt defeated and had advocacy fatigue as the process left an experience of powerlessness. I am nervous about what training they will have us do to start taking vented patients … The patients who are in the ICU aren’t getting better, and when they try to put them in the supine position, they desat instantly ….How am I supposed to take care of patients on these machines without proper training? (Journal 4, March 30, 2020).
Another nurse's conflict centered on the love of nursing being overshadowed by the current distress of caring for patients with COVID-19. We float one nurse each shift to take care of surgical patients we normally see on our floor. It was a breath of fresh air. I did have a patient on comfort care who [I] thought was going to pass but she made it through the night. I genuinely love nursing, but I can’t say I enjoy being a COVID nurse right now. I actually really hate it … I’m struggling (Journal 1, April 12, 2020).
Professional Development
Nurses were troubled by the lack of proper preparation and necessary training to care for patients. They often showed allegiance to helping where needed and being able to educate and lead others in the path they had walked. We were also informed that all of the OR nurses would be receiving clindoc training to be able to float to the floors if needed. This terrifies me. The OR is so highly specialized, and I fear that my skill set is of little use to med surg … I am longing for the predictable days of comfort that will eventually come to me. But for now, I will have to put that on hold and be an RN where I am needed most. I look forward to sharing my experience with others in the future when all of this has passed (Journal 6, March 22, 2020).
I have to get stronger, mentally and emotionally. I should prepare myself, mentally, emotionally, and physically to beat this war (Journal 15, March 22, 2020).
I am constantly learning and gaining more experience which makes “listening to my gut reaction” feel like a natural response. As I continue with my career, I know I will continue to improve my self-confidence and my ability as a nurse (Journal 14, April 14, 2020).
I do believe this experience [heightened] my desire to work in hospice. While I wish I saw less dying in the hospital, I find myself requesting these patients. It means a lot to be able to care for them in their final moments, in hopes they feel a little more at peace with someone by their side (Journal 1, April 21, 2020).
As journal narratives were analyzed and codes assigned, the researchers interpreted that some codes overlapped and then collapsed them into mutually understandable themes. For example, two codes shown in Table 2 were understood to represent the theme of perceived threats.
Discussion
The intent of this study was to analyze and interpret experiences shared in journal reflections by RN-BSN students who were working at the bedside early in the COVID-19 pandemic. The resulting qualitative views from nurses provide unique insights about how each nurse's holistic well-being was affected. Significant statements from the qualitative data were clustered together, and researchers identified patterns of meaning with Physical Threats to Safety, Emotional Threats to Safety, Workplace Culture, Healing Energies, and Professional Identity.
Although study results are similar to previously published literature, this study uniquely obtained data during a university shutdown while RN students were immersed in coronavirus concerns and uncertainties as well as academic studies. This study, from one geographic area in the Northeastern United States, yielded data from nurses who were simultaneously attending classes and working in a variety of clinical settings. The journals as a source of nurses’ thinking and feeling processes at this pivotal experiential time was a distinguishing methodology and data source among early studies reviewed on COVID-19 experiences.
Study results resonated with those in the previously published literature that used survey and interview data in the conduct of qualitative research. Two studies of nurses during the early months of COVID [Gast et al. (2022) and Guttormson et al. (2022)] showed results similar to the themes of this current study. These studies used open-ended questions, gathering data from national surveys with large samples of RNs working in critical care settings. Two themes described by Gast et al. (2022) are sheltering patients when I don't have enough and protecting those I love when I am a vector. Congruence was seen between Gast and colleagues’ two themes and the identified themes of physical and emotional shielding in the current study.
Themes emerged in the Guttormson et al. (2022) study similar to the current study themes of Physical and Emotional Threats to Safety. The national study by Guttormson and colleagues (2022) also described nurses’ physical and emotional suffering as well as fears of inadequate protection from viral spread to self and others. The resultant themes of Workplace Culture, Health Energies, and Professional Identity, were similar to the theme of positive experiences and outcomes with its subthemes, “finding strength in teamwork” and “personal and professional transformation” (Guttormson, 2022, p. 99). Results from the current study differed in that nurses described experiences of professional identity in which they saw themselves as learning and progressing as nurses even through the challenges of COVID-19. Some nurses in the Guttormson et al. (2022) study explained their regret at becoming nurses.
Nurses’ statements captured their overall rendering of the essence of the interpretive description as “pandemic footprints of nursing professionals, processing early experiences.” Furthermore, the researchers’ interpretation of the overall reflections of these nurses has suggested a framework for how to present meaningful perspectives as “Therapeutic Journaling,” “Nurse as Patient,” and “Professional Identity.”
Therapeutic Journaling
While the reflective practice of journaling was not evaluated in this study, the act of therapeutic journaling was recognized as a secondary study outcome. Participant journals disclosed the processing of sensitive matters such as abusive relationships (Journal 14) and pandemic victimization (Journal 11). One participant (Journal 15) even wrote in their journal “This journal has definitely helped my mental health.” The nature of data collection for this study—a reflective journaling assignment—appeared to help nurse participants cope during stressful times.
Therapeutic or expressive journaling is typically a private experience. The act of writing to support processing of emotional experiences in a systematic way has been demonstrated (Brown et al., 2022; Edwards et al., 2019). Therapeutic journaling has evolved through the emergence and popularity of social media networks. Engagement in such applications provides an outlet for disclosure while welcoming the factor of human interaction (Ruini & Mortara, 2022). Sharing experiences with others through written posts, pictures or videos adds the complex factor of judgment. During the COVID-19 lockdown, a variety of interventions were trialed formally and informally on the web to treat mental health and assist with human distress as they navigated a stressful experience (Ruini & Mortara, 2022).
This form of journaling was observed in social media venues during the pandemic as cyber community members posted about their pandemic living during quarantine through commentary, pictures, and memes. These informal methods of communicating may have helped individuals process pain in both mental and physical senses as raw accounts were expressed without care to standard writing conventions. As alluded through the work of Pennebaker (2018, 1997), people feel better after disclosing their emotional upheaval with others. Postings that resonated with others in a similar experience may have provided solace to combat mental and emotional turmoil as seen in the amount of “likes” given to it. Although writing on social media venues may enable judgment to what is posted, it remains informal and enables the creator of the posting to monitor what is seen.
Nurse as Patient
This study uncovered a glimpse of the “nurse as patient.” Enmeshed in their caregiver roles, nurses flexed with having one metaphorical footprint rooted in patient care and the other grounded in the preservation of self-care and protection of others. Within the themes of Physical Threats to Safety, Emotional Threats to Safety, Workplace Culture, Healing Energies, and Professional Identity. Nurses appeared to experience liminal spaces as more fluid. This space demarcation permitted nurses to make stronger connections with patients in a time of crisis and recovery as they recognized the similarities through shared pandemic experiences. Thus, these experiences depict the deepest level of empathy reached by nurses in this study.
In the face of intense, manifest emotions, nurses have seen death to an extent not before seen in their professional careers. In their mixed-method study of nurses’ experiences during COVID-19, Gray et al. (2021) conceptualized, “mortality sadness,” a sub-theme related to watching patients die, and die alone. Of those surveyed, 82% of them identified that their worry over patients’ families’ reactions affected as major stressors (Gray et al., 2021, p. 4). The literature is rife in the recognition that the effect of caring for seriously ill and dying patients with the coronavirus has left nurses with subsequent mental health challenges. To provide self-care and mental health resources for healthcare providers is a persistent refrain in these pandemic times (Busch et al., 2021; Wu et al., 2020).
Busch et al.'s. (2021) systematic review suggested adverse situations, such as those during COVID-19, impact a nurse similarly to what has been described as a “second victim.” The “second victim” phenomenon, previously described by Wu (2000) in the context of a provider's erroneous action, resulted in patient death or disability, and subsequently, other devastating consequences. In a more recent publication, Wu, Connors, and Everly Jr. (2020) encouraged institutions to provide support for nurses and other providers at high risk for exposure with resources like those given to “second victims.” Those engaged in caring for caregivers at Johns Hopkins Hospitals’ Resilience in Stressful Events (RISE) program recommended three strategic approaches inclusive of leadership/crisis work in developing resilience, communication, and continued staff/peer support.
Professional Identity
Nurses’ professional identity emerged in this study as a powerful anchor beckoning them to learn more, work to their highest potential, and use the best evidence to provide high-quality care while also attending to their own health. Their situation was not without challenge, as they described times of feeling the paradox of pride and frustration in their ability to maintain professional identity.
Researchers identified themes that aligned closely with Sister Callista Roy's Adaptation Model, embracing a holistic perspective on the individual's modes of adaptation to physical/physiologic, self-concept, role performance, and interdependent aspects of self (Roy & Andrews, 2009). During times of extreme stress, adaptation to internal and external environmental stressors freed participants to sustain, and even enrich their professional identity and life balance. As nurses promote patients’ adaptation in the face of illness and injury, nurses’ own adaptive coping remained crucial in the throes of extreme challenges such as were experienced during the COVID-19 pandemic.
Gray et al. (2021) studied several factors that influenced nursing during the pandemic. They found nurses felt motivated by an ethical duty to care for patients. Nurses in the current study reported a different energy in regard to motivation for patient care, feeling buoyed by the opportunity to extract something very valuable from the experience of caring for patients in the COVID-19 environment.
This unique phenomenon amidst the COVID-19 nursing literature challenges a rigid mindset about nursing roles, inviting a more fluid perspective on nurses within a health care system ripe for change. Implications include a growth mindset for nursing leadership, urging investment in re-envisioning nurses’ professional identity. This phenomenon was also noted by Zipf et al. (2022) in their qualitative meta-synthesis of nurse experiences during the COVID-19 pandemic, represented by a theme of “Growth: A renewed sense of professional identity and calling” (p. 101). Data from the current study support a similar expansion of the lens of professional identity, recognizing deeper nuances and complexities through which nurses are challenged to continually survive, thrive, and grow.
The nurses in this study described experiences of feeling uplifted by bringing a positive impact to a patient or family and feeling grateful acknowledgment from co-workers or community members. This finding contrasts sharply with post-pandemic nursing challenges summarized by Kurtzman et al. (2022), who describe the “Great Resignation” (p. 49), burnout, and adverse effects on nurses’ psychological health. Clearly, there is no afterglow to sustain nurses. Yet, implications from the assault on nursing conjure up the sense of hope suggested by Kurtzman; negatives perhaps can be turned around to enhance growth and accentuate the wisdom of nurses who have witnessed and lived the unspeakable in a worldwide crisis. Health care leaders must pursue best practices for how to support nurses. As current study results indicate, physical and emotional safety are mainstays of nursing practice, not only for patients but nurses also. At a minimum, nurses need access to mental health services in a timely manner, at the point of care, when fear and uncertainty can consume the resources of even the hardiest of caregivers.
Implications
The five emergent study themes captured the essence of the pandemic footprints of the nursing profession. Study results may influence nursing future practice and education or shape further research and policy development. At a minimum, these journals may be distinctive in their contribution to nursing history, providing important insights into nurses’ response to social conditions and highlighting how nurses continued to remain a vital constituent in healthcare. Regardless of the nurses’ work environment the impact of the emerging pandemic on nurses remained similar. Nurses’ impressions were captured in real-time with therapeutic journaling. This study demonstrates the use of journaling and its potential effect on coping and healing. Journals reflected holistic concerns by nurses, including physical, emotional, healing, and professional identity through “in the moment” first-hand experiences rather than stimulating recollection of memories post-event.
The themes from this study have implications for holistic nursing practice as all core values are exemplified. Study themes provided a grounding from which nurses may draw inspiration when faced with similar challenges of mind, body, and spirit. Core value, one of the Holistic Nursing Model is holistic ethics, theories, and research (American Holistic Nurses Credentialing Corporation, 2017). Within this value nurses apply all ways of knowing and utilize theories of healing for the whole person. In this study, knowledge was gathered, and interventions were employed through application of the science and art of nursing. Researchers recognized relevant theories such as Maslow's hierarchy of needs (Maslow, 1943) and Peplau's nurse–patient relationship (Peplau, 1991) as journal passages were analyzed. These theories were shown through nurses’ voices of their needs for professional safety and security, as well as in the values represented in caring relationships, healing energies, and self and professional growth. The art of nursing was apparent in the care of patients, families, and self that was inclusive of letters, journals, or conversations that could convey the deepest feelings and perhaps open further dialogue on the most sensitive experiences at a critical juncture. Recognizing journaling, letter writing, or conversations as healing strategies in a time of turmoil speaks volumes about holistic nursing.
Nurses’ journals were inclusive of caring processes (Holistic Core Value Two) as illustrated in the themes of healing energies and workplace culture, voicing concern not only for themselves, but for their patients and others. The salience of holistic communication, a therapeutic environment and respect of cultural differences (Holistic Core Value Three)–were apparent in study themes of physical threats to safety, emotional threats to safety and the subtheme of healthcare teamwork. The nurses in this study, all pursuing further education, were guided by the core value of education and research (Holistic Core Value Four). This was illustrated through their commitment to professional identity with their willing participation in qualitative analyses of their experiences. The nurses also strived to quickly assimilate new knowledge and skills for care of patients and families facing novel and complex health disturbances not previously experienced. The theme of healing energies displayed during frantic days, weeks, and months of caring for others, communicating, creating therapeutic milieu, learning, and educating, generated moments for nurses’ self-care (Holistic Core Value Five). Nursing history will add a new chapter, still evolving and in a formative stage, on the unequivocal requirement for provision of emotional and mental wellness for nurses and those in their care.
While institutions have made efforts to provide mental health and well-being, resources nurse leaders are encouraged to recognize and continue supporting these experiences through creative programming. Program offerings should blend physical, psychological, and interpersonal approaches so nurses can grow as experts with confidence and professionalism as being recognized for the significance of their role in society appears important. Continuation of these efforts may serve useful in helping nurses unpack their unresolved emotions from the experience and may impact nurses’ development in resilience, communication, and peer support as they continue caregiver responsibilities.
Nurse educators have demonstrated that storytelling is an effective teaching method and studies such as this may help share accurate portrayals of the COVID-19 pandemic and the character of nurses who lived the event. Through storytelling from this journal analysis, nursing students may discern essential nursing characteristics from past professionals and develop their own professional nurse identity. Since some participants stated journaling as therapeutic, it may also behoove nurse educators to engage students in assignments that promote reflective practices such as expressive journaling as these activities teach how to process experiences thereby supporting development of healthy coping habits. This learned skill may then be used by professional nurses as healthy coping mechanisms throughout their professional practice.
Further research may extend the lens to focus on nurses’ professional identity as nurses emerge from a complex, traumatic event, taking stock of what has occurred and what lies ahead. Nurses who lived through the pandemic experience remain forever affected by that personally and professionally. Their changing professional footprint has yet to be elucidated, perhaps examined further through a combination of longitudinal and correlational studies. An abiding question for exploration might be framed: What have nurses learned from these times to use in the future regarding human crises and disasters impacting health and well-being?
The aforementioned study implications from practice, education, and research perspectives are supported by nursing program accreditation bodies such as the American Association of Colleges of Nursing (AACN). The AACN Essentials (2021) guides the development of nursing professionals in academic programming. The first domain (Knowledge for Practice) in AACN Essentials (2021) acknowledges that knowing nursing's collective history is important in advancing the impact of nursing on health and health care. The realization that the nursing profession may learn from this documented history of past experiences to avoid professional pitfalls and potentially advance the impact of nursing in healthcare is important. Nursing programs and institutions are particularly aware of mental health status and self-care efforts. Furthermore, the AACN essentials (2021) now requires accredited nursing programs to become more mindfully aware of the mental health status of caregivers and their patients by encouraging self-care efforts to be explored and embraced throughout their academic study (Domain 10: Personal, Professional and Leadership Development & Domain 2: Person-Centered Care). The emphasis placed on the development and employment of self-care principles shows how these strategies may impact health and well-being for patient recovery as well as professional development as leaders in the nursing profession. This emphasis encourages nursing leadership to support and effectively employ well-being initiatives in the nursing profession. In addition to the emphasis on self-care, Domain 10 of AACN Essentials (2021) references nurses’ own development as leaders in the profession. This links to study findings in Theme 5: Professional Identity as strategic competencies include a commitment to personal health and well-being, contributions to an environment that promotes self-care, personal health and well-being, and evaluation of the workplace environment to determine levels of health and well-being. Accomplishment of these wellness initiatives seems most tenable through the development of a policy by healthcare institutions and other accrediting agencies that will proclaim the importance of valuing nurses’ health front and center, both physically and mentally.
Limitations and Study Strengths
While rigor and trustworthiness were upheld, researchers recognize the study had limitations. The purposive sample originated from a group of nursing professionals enrolled in an RN-BSN nursing course at one university. Although the journal assignment was graded only for completion, it is possible participants’ may not have written a true reflection on their lived experiences as they knew another person (in this case, a faculty member) would be reading about it. Since this study was course-based versus hospital-based, a broad range of clinical areas were represented. Participants worked in varied in-patient and outpatient settings throughout a regional health network along with their demographics and specific nursing roles.
Study investigators did not collect data on the nurses’ years of experience. It is possible the level of experience and a broad range of clinical areas may have impacted responses as nursing expertise and exposure to different clinical settings may have exposed nurses’ to different challenges. The results from the study may only be transferable to RNs in similar COVID-19 health care situations. It is for the reader to determine if the experiences “ring true” to their own experiences during pandemic nursing.
Another study limitation pertains to the study design. Participant journals were not analyzed in real-time by the research team. This study was conceived by the course faculty member after journals were reviewed and the course officially ended for the term. The course faculty member remained on the research team, obtained participant consent, de-identified journals, and engaged with the research team in the analysis of journal passages. It is possible that not analyzing the journals in real time may have limited clarifying concepts or reduced the importance of the recorded event.
While the physical timing of the study analysis was not ideal, a strength of this study was the implementation of rigorous qualitative research processes. Meaningful units were identified and coded through iterative review of journal transcripts and triangulation by three researchers’ consensus of data during the coding of the first four journals. This, along with thick, rich, descriptive quotes from journals supported data credibility and dependability. All three researchers reviewed and agreed on themes in the final analysis of all journals; data saturation was achieved since no new codes or themes had emerged. Confirmability is shown by the audit trail, as described above, that documents the researchers’ process of checking and rechecking the steps of data analysis (Sandelowski, 2000).
Conclusion
The essence of the thematic coding and interpretation was elucidated in the crucial nature of pandemic “footprints” of nursing professionals. Study investigators’ conceptualization of nurses created “footprints in time,” a metaphorical presence, navigating their paths through heretofore unknown territory. It was apparent as these journal reflections were processed that journaling was therapeutic and led to holistic self-reflection as mentioned by one nurse (student): Since this pandemic, I’ve been journaling my thoughts a lot and I’ll be honest this journaling definitely helps my mental health … I definitely need to relax, take care of my mind, body and soul … I’ve been talking to my friends and family more often and writing down all my goals once this pandemic is over.
The researchers interpreted that nurses’ journal entries brought forth a meaningful template for empathy, understanding, and connectedness. Nurses’ fight for lives and living, seen in their reflections were honest and insightful, and can inspire others’ walks through personal and professional challenges. It is suggested to keep reflective practices, such as journaling, if and when nurses face critical circumstances again such as what they confronted in the early weeks of COVID-19.