
Abstract
Introduction
Emergency department (ED) nurses work in some of the most high-intensity, unpredictable, and emotionally demanding environments in health care. The cumulative exposure to trauma, rapid decision-making, and chronic staffing challenges contributes to burnout and emotional exhaustion. These stressors compromise not only the well-being of nurses but also the therapeutic presence essential to patient-centered care. Holistic nursing views the nurse as an instrument of healing and recognizes self-care as an ethical and professional responsibility. Grounded in the Integrative Nursing Framework (INF), which emphasizes whole-person care and the interconnectedness of body, mind, and spirit, this study evaluates a mindfulness-based mobile intervention as a strategy to support ED nurses’ well-being, enhance inner awareness, and strengthen holistic practice.
This study explores a mobile mindfulness intervention designed to support ED nurses’ self-care, emotional regulation, and resilience. Grounded in the INF, the study embraces a whole-person approach, addressing the interconnectedness of mind, body, and spirit within the clinical context. The intervention aligns with the values of holistic nursing by fostering inner awareness, honoring the nurse's healing capacity, and promoting sustainable caregiving practices. By evaluating a practical, evidence-informed strategy for supporting nurse well-being, this work contributes to the advancement of holistic nursing science and offers a scalable approach to creating healing environments—for both caregivers and the patients they serve.
Literature Review and Alignment With Holistic Nursing
Previous research has documented physical and mental health benefits from participating in mindfulness training and practice, particularly in healthcare settings. Such interventions hold great promise for nurses, especially those in high-stress environments like the ED (Carmody & Baer, 2008; Luken & Sammons, 2016; Pollard et al., 2023). Studies have shown that mindfulness-based stress reduction (MBSR) techniques are associated with decreased burnout, psychological distress, anxiety, and work-related stress (Beshai et al., 2016; Cohen-Katz et al., 2005; Duchemin et al., 2015; Geary & Rosenthal, 2011; Huang et al., 2015; Janssen et al., 2018; Klatt et al., 2009; Manotas et al., 2014; Roeser et al., 2013; Taylor et al., 2016; Wolever et al., 2012). These outcomes reflect key values of holistic nursing, which promotes self-awareness, self-care, and balance as necessary for delivering whole-person, compassionate care (Helming et al., 2020; Kreitzer, 2015).
The INF provides the theoretical foundation for this study. INF is grounded in the belief that human beings are whole systems inseparable from their environments, and that nurses have a professional responsibility to care for themselves as they care for others (AHNA, 2019; Kreitzer, 2015). In alignment with the American Holistic Nurses Association (AHNA), this framework guides the application of mindfulness as both a personal and professional healing practice (Kreitzer, 2015).
Although MBSR programs are effective, nurses often report barriers to participation—including time constraints, shift work, and lack of institutional support (Ameli et al., 2020; Cascales-Perez et al., 2021; Ireland et al., 2017; Janzarik et al., 2022; Kober & Chang, 2024; Lilly et al., 2019; Lin et al., 2019; McConachie et al., 2014; Watanabe et al., 2019). Mobile-based mindfulness interventions offer a flexible and accessible alternative. While technology-assisted mindfulness is not new, limited mixed-methods research has evaluated mobile apps for stress and burnout relief specifically among ED nurses. This study seeks to fill that gap.
Mindfulness Programs for Healthcare Workers
Numerous studies have demonstrated that nurses participating in mindfulness programs report reduced psychological distress and fewer self-reported medication errors (Daigle et al., 2018; dos Santos et al., 2016; Ghawadra et al., 2020; Janssen et al., 2018; Janzarik et al., 2022; Lilly et al., 2019; Lin et al., 2019; Mackenzie et al., 2006; Trygg Lycke et al., 2023; Watanabe et al., 2019). These findings are highly relevant for ED nurses, who frequently manage medication administration under pressure. By delivering mindfulness content in a mobile format, adherence may improve, making it easier to integrate holistic self-care into daily routines (Ghawadra et al., 2020; Keng et al., 2022; Mackenzie et al., 2006; Monfries et al., 2023; Watanabe et al., 2019; Xu et al., 2022; Yang et al., 2018).
Mindfulness, emotional regulation, and empathy have been linked to enhanced stress management skills in the ED setting (Ghawadra et al., 2020; Luken & Sammons, 2016; Monfries et al., 2023). Promoting self-care through mindfulness aligns with the holistic nursing perspective that self-care is not optional—it is an ethical imperative tied to both personal health and professional accountability (Luken & Sammons, 2016). Despite its potential, there is a lack of published mixed-methods research specifically examining mobile-based mindfulness interventions in ED nurses. This study directly addresses this limitation.
Mobile Mindfulness as a Holistic Strategy
Mobile mindfulness apps offer privacy, flexibility, and user-directed pacing—attributes well-suited to the needs of busy ED nurses. Prior studies show that these tools support better emotional processing, increased energy, improved decision-making, and greater self-awareness (dos Santos et al., 2016). These outcomes align with holistic nursing goals of fostering resilience, presence, and well-being (AHNA, 2019).
Comparative research between in-person and app-based mindfulness programs suggests similar outcomes in reducing stress and enhancing mindfulness across multiple nursing specialties (Ghawadra et al., 2020; Grabbe et al., 2020; Luken & Sammons, 2016; Mackenzie et al., 2006; Monfries et al., 2023; Pollard et al., 2023; Watanabe et al., 2019; Xu et al., 2022). However, few studies have focused specifically on the ED setting. The greater accessibility and autonomy afforded by mobile apps may increase frequency of practice and deepen engagement with holistic principles of healing.
Headspace as a Holistic Tool
Headspace is a widely used mobile mindfulness app designed to enhance mental well-being through guided meditations and stress-reduction tools (Bostock et al., 2019; Champion et al., 2018; DeSteno et al., 2018; Headspace, 2023; Lim et al., 2015; Wen et al., 2017; Wylde et al., 2017; Zollars et al., 2019). It supports principles of the INF by encouraging self-reflection, present-moment awareness, and compassionate self-care (Kreitzer & Koithan, 2018). Research with students, healthcare professionals, and the general public shows Headspace improves mindfulness, self-compassion, and emotional regulation—core outcomes relevant to holistic nursing practice(AHNA, 2019; Zollars et al., 2019).
Given its evidence base, usability, and alignment with the goals of this study, Headspace was selected as the intervention tool to explore that mobile mindfulness can be used to promote holistic well-being among ED nurses. By integrating this intervention within the INF, this study supports a growing body of evidence on the importance of accessible, meaningful, and holistic strategies for stress management and professional sustainability in nursing.
Theoretical Framework
The INF guided this study. As a holistic, evidence-informed model, the INF emphasizes whole-person care, self-care, and relationship-based practice, offering practical guidance for promoting health and well-being across clinical settings (Kreitzer, 2015; Kreitzer & Koithan, 2018). Its six principles informed the study's design, intervention, and qualitative inquiry.
The first principle—human beings as whole systems inseparable from their environments—supports using mindfulness to address mind–body–spirit dimensions of stress, burnout, and well-being. This guided the selection of outcomes and the whole-person focus of the intervention. The second principle asserts that individuals possess an innate capacity for health and well-being, informing the exploration of nurses’ intentions, motivations, and perceptions of mindfulness practice (Kreitzer & Koithan, 2018).
The third principle highlights nature's healing and restorative properties. Mindfulness practices such as breathwork and intentional awareness reflect this principle and shaped qualitative questions about stress and well-being. The fourth principle emphasizes person-centered and relationship-based care, underscoring how presence, reflection, and authentic connection influence both patient care and caregiver well-being (Kreitzer & Koithan, 2018).
The fifth principle encourages using a full range of therapeutic modalities, beginning with the least intensive and invasive. The mobile mindfulness intervention represents a low-intensity, non-pharmacologic strategy to support stress reduction among ED nurses. Quantitative surveys also align with minimally invasive methods. The sixth principle affirms the importance of caregiver well-being, directly aligning with this study's purpose (Kreitzer, 2015; Kreitzer & Koithan, 2018; Ilgaz & Gözüm, 2019).
The INF effectively supports research with ED nurses, who experience significant stress and cumulative exposure to trauma. A strength of the INF is its accessibility, requiring no specialized training to apply its principles. A potential challenge is varying familiarity with holistic approaches among nurses, reinforcing the need for ongoing research and education (Ilgaz & Gözüm, 2019).
In this study, the INF guided the intervention and the development of open-ended narrative questions for pre- and post-intervention surveys, as well as the semi-structured interview protocol. These qualitative components explored nurses’ experiences using a mindfulness app to manage stress and burnout. Findings grounded in the INF can inform future holistic interventions and reinforce the ethical responsibility of nurses to care for their own well-being (Faubion, 2024.)
Methods
The study used an explanatory sequential mixed-methods approach, with the first step consisting of structured quantitative surveys to measure stress, burnout, mindfulness, and well-being. The surveys also included four open-ended narrative response questions in order to gather information about ED nurses’ attitudes and perceptions of stress and burnout in the workplace and how it is managed by themselves and/or the healthcare organization they work for (see Appendix B). The mobile app Headspace was administered to a sample of 11 ED nurses for a 4-week timeframe as an intervention to pilot test its effectiveness in managing ED nurses’ perceived stress and burnout. The study concluded with post-intervention surveys again measuring levels of stress, burnout, mindfulness, and well-being, along with an additional four open-ended narrative response questions (see Appendix C). This step also consisted of post-intervention semi-structured qualitative interviews with a sample of 7 ED nurses who have completed the intervention to examine their experiences with the app and intervention.
Population and Setting
Sample and Recruitment
This pilot study included registered nurses (RNs) employed in EDs in the Southern Tier, Central, and Western regions of New York State. Because this was an exploratory pilot, a power analysis was not required (LinkedIn, 2023). Convenience sampling was used among EDs that agreed to participate, and the intervention was completed remotely using participants’ personal smartphones.
Participants were recruited through IRB-approved emails distributed by ED management via departmental listservs, supplemented by posted flyers with QR codes linking to an interest form. Word-of-mouth and limited social media postings were also used. Interested nurses provided contact information through a secure form or by emailing the primary investigator (PI). Those who met eligibility criteria received an electronic consent form and subsequently completed the pre-intervention surveys.
Across all recruitment efforts, 26 ED nurses expressed interest, 23 completed screening, and 19 met eligibility criteria. Sixteen completed all pre-intervention measures and received instructions and access codes for the Headspace app. Eleven participants downloaded the app, engaged in the 4-week intervention, and completed post-intervention surveys; nine additionally completed qualitative interviews. Participant flow is depicted in Figure 1.
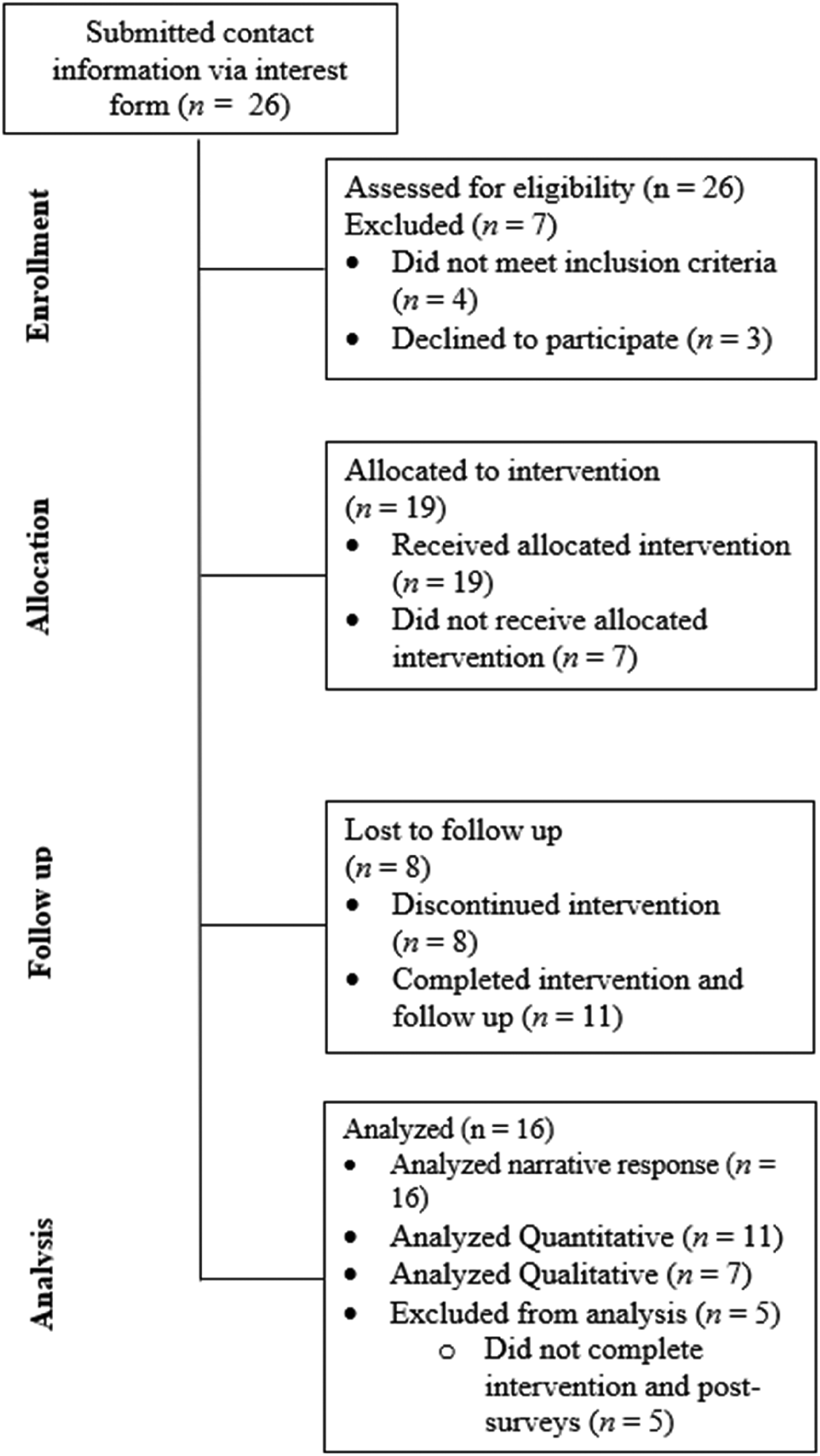
Participant flow diagram.
Inclusion and Exclusion Criteria
Eligible participants were required to hold RN or Licensed Practical Nurse (LPN) licensure, be able to read and speak English, and anticipate remaining employed in their ED for the duration of the four-week intervention. Individuals with an existing subscription to a mindfulness app or an established mindfulness/meditation practice were excluded. Screening included the Patient Health Questionnaire (PHQ-9) to assess mood symptoms; individuals with scores ≥15 or recent mental health hospitalization were excluded and provided referrals as appropriate (Kroenke et al., 2001). Additional exclusions included participants with extremely low baseline stress or burnout levels, and any individual reporting acute psychiatric symptoms or suicidal ideation, as the intervention was not intended to replace professional mental health care.
Measures
Quantitative and qualitative data were collected prior to the intervention starting, and again at its conclusion (see Appendices B and C and E–H). All data was collected electronically via RedCap surveys that were emailed to the participants. Semi-structured open-ended questions were presented at the end of the pre- and post-intervention surveys to assess participants’ subjective experiences with work-related stress and burnout and to provide them with the opportunity to share relevant information not included in the survey (see Appendices B and C). A personalized code was assigned to each of the participants to keep the data anonymous and was consistent across the use of the pre- and post-surveys, as well as the use of the intervention. Demographic information was collected at baseline (week 1), prior to the intervention. Information collected included nurses’ age, sex, race and ethnicity, role (RN or LPN) annual income, marital status, employment status (Full-Time, Part-Time, or Per Diem), years employed as a nurse, and shift worked (morning, midshift, or overnight). Each of the tools that were utilized to measure key outcomes of the proposed study have been previously validated (Al Mutair et al., 2020; American Psychological Association, 2020; Christopher et al., 2012; Chowdhury, 2019; Cohen-Katz et al., 2005; Kroenke et al., 2001; Leiter et al., 2016; Levenstein et al., 1993; Maslach & Jackson, 1981; Roberti et al., 2006; Warwick Medical School, 2006; World Health Organization, 2024). Data was collected by Headspace as to how the participants used the app, that is, how many minutes, how many days, what features, etc. This data was provided to the PI from Headspace upon request throughout the intervention time period in order to track fidelity and also was available upon completion of the study.
Instruments
Patient Health Questionnaire
The nine-item Patient Health Questionnaire (PHQ-9) is a self-administered tool which is commonly used as a screener for the constructs of depression and depressive symptoms (American Psychological Association, 2020). Higher scores on the PHQ-9 are more likely to be diagnosed with depression by a mental health professional, while lower scores are less likely to have depression (APA, 2020). A PHQ-9 score of 5 to 9 is indicative of minimal symptoms, a score of 10 to 14 indicates minor depressive symptoms, a score of 15 to 19 indicates major depression, moderately severe and >20 is considered major depression, severe. Internal consistency of this tool has shown to be high, and reliability and validity have indicated strong psychometric properties. Validity was tested against a sample of 580 individuals and reliability testing found the PHQ-9 to have a Cronbach's alpha ranging from .86 to .89 (American Psychological Association, 2020; Kroenke et al., 2001).
Burnout
Burnout is operationalized as a psychological syndrome which emerges as a prolonged response to chronic interpersonal stressors on the job, with the three key dimensions of this response being emotional exhaustion (EE), depersonalization (DP), and lack of personal accomplishment (PA) (Maslach & Jackson, 1981). Burnout is a concept that can be measured using the Maslach Burnout Inventory for Health Services Survey for Medical Professionals (MBI-HSS MP), see Appendix E). This is a 22-item Likert scale from 0 to 6 (0 being never and 6 being every day), which measures the amount of burnout being experienced by an individual while also helping to identify the attitudes of healthcare workers toward their work and their patients (Al Mutair et al., 2020). It includes subscales of the three key dimensions of burnout: EE, DP, and PA, with higher levels of EE and DP indicating higher burnout, and lower levels of PA indicating higher burnout. Validity of this tool was tested against a sample of 888 healthcare workers, and Cronbach's alpha was used to determine reliability of the total and subscale correlations which yielded the estimates of the entire measurement scale as .87; .85 for EE, .80 for DP, and .75 for PA (Al Mutair et al., 2020).
Stress
Stress can be defined operationally in several ways. Conceptually, stress is a state of worry or mental tension caused by situations which are difficult (World Health Organization, 2024). Stress was measured with the Perceived Stress Scale (PSS) (see Appendix F), which is a classic stress assessment tool which helps us to understand how different situations affect our feelings and our perceived stress within the last month (Levenstein et al., 1993; Roberti et al., 2006). The PSS is a 10-item Likert scale from 0 to 4 (0 being never, and 4 being very often; Levenstein et al., 1993). The PSS was validated against a sample of 285 undergraduate college students and found to have a Cronbach's alpha ranging from .82 to .85 (Levenstein et al., 1993; Roberti et al., 2006).
Mindfulness
There are many ways to conceptualize mindfulness. One way to define it is a state in which one is paying full attention to the present moment and experience with openness and non-judgmental acceptance (Bostock et al., 2019; Christopher et al., 2012). Measurement of mindfulness was done with the Five Facet Mindfulness Questionnaire (FFMQ-15), see Appendix G) (Chowdhury, 2019). The FFMQ-15 is a tool which includes 15 items on a 1 to 5 Likert scale (1 being never, and 5 being always true), and measures the facets of observing, describing, acting with awareness, nonreactivity, and non-judging (Christopher et al., 2012; Chowdhury, 2019). The validity of the five factors measured with this tool was against a sample of 349 individuals and were assessed with Cronbach's alphas ranging from .75 to .91 (Christopher et al., 2012).
Well-Being
Well-being is operationally defined by using several constructs, including positive functioning, positive affect, negative affect, happy traits, life satisfaction, and perceived health (Warwick Medical School, 2006). This concept is measured in various ways. One common tool which has been chosen to use for this research is the Warwick-Edinburg Mental Wellbeing Scale (WEMWBS) (see Appendix H) (Warwick Medical School, 2006). This is a 14-item measurement tool which uses a 1 to 5 Likert scale (1 being none of the time, and 5 being all of the time), which helps to measure well-being in the general population and the evaluation of programs aimed at improving mental well-being. Validation of the WEMWBS was performed in the United Kingdom with students aged 16 and above at the Universities of Warwick and Edinburg in 2006. It was also included in two national surveys in Scotland, allowing validation using population data. Internal consistency was measured with this tool against a sample of 348 individuals and assessed with a Cronbach's alpha of .89. Test-retest reliability score was .83 after 1 week in a sample of 124 individuals, suggesting that “the transient fluctuations that a person may experience from one day to the next are not reflected in the scores, and these scores remain robust over a short period of time” (Warwick Medical School, 2006).
Procedure
This pilot study used a one-group, pre-test/post-test quasi-experimental design to evaluate the feasibility and effectiveness of the Headspace mobile mindfulness app for reducing perceived stress and burnout among ED nurses. Participants received a free 1-year subscription funded through a grant.
Interested nurses accessed a QR code linking to a secure interest form and were contacted by the primary investigator for eligibility screening. Eligible participants received an email with informed consent information and a link to complete the pre-intervention REDCap survey, which included standardized measures and four open-ended narrative questions. Each participant was assigned a unique four-character linkage code used to match pre- and post-intervention surveys, qualitative interviews, and app-usage data while maintaining anonymity.
Enrollment occurred on a rolling basis from June through October 2024. After completing the pre-survey, participants were instructed via email and text message to download the Headspace app and redeem their individualized access code. All participants were directed to use the “Today's Meditation” feature once daily in a setting conducive to focused practice. Daily sessions varied from approximately 3 to 20 minutes. Headspace provided de-identified usage data to the PI to monitor intervention fidelity.
At the end of the 4-week intervention period, participants received email and text reminders to complete the post-intervention REDCap survey, which included the same standardized measures and four additional narrative questions. Participants used their linkage code to submit post-intervention data.
Following survey completion, participants were invited to take part in an optional post-intervention qualitative interview conducted via password-protected Zoom. Although the initial plan was to interview at least five participants, all individuals who completed the intervention were invited due to the small sample size. Nine of the 11 participants who used the app completed an interview. The semi-structured interview protocol explored participants’ experiences using the mindfulness app and their perceptions of its impact on stress, burnout, and well-being.
Data Collection
The sample consisted of 16 ED nurses who completed the pre-intervention survey and received the Headspace app. The goal was to have the participants fill out their pre-intervention surveys and complete the four narrative response questions within 72 hours of meeting inclusion criteria, with a follow-up email being sent as a reminder after 24 hours. All participants had their surveys filled out relatively within this time frame, or soon after with a text message reminder being sent. The total time for the questionnaires to be completed was estimated to be 30 minutes. Because of initial difficulty recruiting participants to meet the original planned minimum number of 30 nurses for the study, the backup plan to reach out to other EDs for participation was initiated with an approved IRB modification.
At the end of the intervention (week 6–7) for each individual participant, the same survey questions were asked as a post-measure. Post-intervention interviews were conducted with a volunteer sample (n = 9) from the same group who completed the intervention, using the interview guide found in Appendix I. A password-protected Zoom interview was offered for the interview portion of the study. Participant interviews lasted anywhere from 15 to 30 minutes. The topics of the interview included open-ended questions regarding work-related stress and burnout. All participants were de-identified with an anonymous linkage code.
Interviews were scheduled via email at the convenience of the participants’ schedules. The goal of the interviews was to gain an understanding of how the nurses used the mindfulness app, and what barriers and facilitators they experienced while using it, as well as data related to how they feel the app was able to help them, or not help them, in regard to their levels of stress and burnout experienced in the workplace.
Ethical Considerations
This study received approval from the Institutional Review Board (IRB) at both University at Buffalo and United Health Services. All participants completed electronic informed consent via REDCap after reviewing the study purpose, procedures, risks, benefits, confidentiality protections, and voluntary participation. Participants could skip questions or withdraw at any time.
Each participant was assigned a unique, anonymous linkage code to match survey responses, interview data, and app-usage information. Identifiable data were stored separately in a password-protected file accessible only to the PI. Deidentified data were shared only with the research team.
Qualitative interviews were conducted via password-protected Zoom. Automated transcripts were cleaned and de-identified by the PI before analysis. Audio recordings were deleted within 30 days, and deidentified transcripts were stored securely per IRB protocol. All future publications will use deidentified data, and interview excerpts are reported using participant numbers.
In alignment with holistic nursing ethics, the research process emphasized respect, dignity, and participant autonomy. The intervention was self-directed, allowing nurses to engage in ways meaningful to their personal values and well-being. These procedures reflect the Standards of Holistic Nursing Practice, particularly those related to self-care, therapeutic presence, and creating environments that support healing (AHNA, 2019).
Data Analysis
Quantitative and qualitative data were used to provide a more in-depth explanation of the constructs of burnout, stress, mindfulness, and well-being. The analysis process was a team approach among the research team which consisted of a master's prepared nurse/Ph.D. candidate, a Ph.D. prepared nurse, and two Ph.D. prepared psychologists. Statistical Package for Social Sciences (SPSS) 29.0 software was used for the quantitative analysis portion of this project and the Wilcoxon Signed Rank Test was used for analysis. Given the small sample size and exploratory nature of the study, a non-parametric approach was used. This test was used to compare the pre- and post-intervention means of the study variables for a single group. The outcomes to be compared were the mean scores of stress, burnout, mindfulness, and well-being from the pre-test measures to the mean scores from the post-test measures. Results from the semi-structured open-ended questions in the pre- and post-intervention surveys were analyzed using qualitative content analysis, with themes reported holistically with the post-intervention interview themes (Castro et al., 2022).
Braun and Clarke's (2022) six-phased reflexive thematic analysis method was used to analyze interview data. This method utilizes an inductive or bottom-up approach to data analysis with use of semantic or direct explicit codes which are easily mapped back to the dataset. Additionally, throughout the data analysis process and writing the final report, reflexivity was practiced by the entire research team. According to Braun and Clarke (2022), a reflexive process involves the researcher having awareness and insight regarding how their personal and professional experiences, pre-existing knowledge, and their position in society may influence the data collection and analysis process. Within the reflexive process, the researcher and their team are invited to explore, understand, and bring forth their own beliefs, ideas, and values about the world, and consider how these may influence their interpretation of the research. The following described the six data analysis phases in detail.
The Six Phases of Thematic Analysis
In phase one of Braun and Clarke's (2022) reflexive thematic analysis method, familiarization of the data takes place. This requires the researcher to shift their focus from data generation to analysis, while becoming immersed in the data and connecting it in different ways. This phase entailed reading and re-reading each transcript while listening to the Zoom interview recording to ensure transcription quality and accuracy and removing any participant identifiers while taking initial notes of interesting data features. The notes are shaped by the research question, as well as broader questions revealed by the data. This process helps to gain a better initial insight into the data by sharing each other's perspectives as the team works together.
Phase two of Braun and Clarke's (2022) thematic analysis is where initial codes are first generated independently by the research team before meeting together. The initial coding phase focuses attention on making sense of the data in a systematic and rigorous way. With the identification of initial codes, the research team begins to organize data around similar meanings and reduce it into smaller bits of text. Codes attach labels to these bits of data and help organize the data into meaning-patterns.
In phase three of Braun and Clarke's (2022) reflexive thematic analysis method, candidate themes (or prototypes) are developed from work completed in the earlier data analysis phases and then brought back to the research question and overall dataset to determine if they are telling the participant's story. It is important to note that good themes are those which “tell a coherent, insightful story about the data in relation to the research question” (Braun & Clarke, 2022).
Phases four and five of the process include revising and further defining themes. In this phase, some prototype themes may be either merged with other themes or eliminated altogether to create a richer dataset story from without risking an overlap in the themes (Braun & Clarke, 2022). This phase entails clarifying the essence and scope of each theme by “delineating the theme's boundaries and central organizing concept” (Braun & Clarke, 2022). A key step within this phase is compiling all coded data for each of the candidate themes from the previous phase, reviewing them for relation to a central concept, and then checking them against the whole dataset. It is in this step that the creation of a Thematic Map may be useful to visualize how all of the themes fit together and tell the whole story without overlapping.
The final phase of Braun and Clarke's (2022) reflexive thematic analysis method involves connecting data analysis findings to the existing literature and producing the final report and thematic map. The research team revisits the research question and data analysis notes, codes and themes to ensure the final themes remain close to the data and reflect the voice of the participants. The thematic map provides the reader with a visual illustration of how the themes fit together and tells the overall dataset story.
Interviews were conducted by the PI from a volunteer sample of participants in the study, via a password protected Zoom session, and were recorded and transcribed. For data verification, all transcripts were reviewed and compared by the PI, line by line and paragraph by paragraph while listening to the audio recording, to ensure all data was correct and there was nothing missing. Participant names were removed and replaced with their anonymous linkage codes provided prior to them taking their pre-surveys. Patterns were identified in the data and codes were generated according to the topics addressed in the interviews. Various codes were compared based on differences and similarities, and then sorted into categories, and then into themes, which were used in the creation of a thematic map as seen in Figure 2.
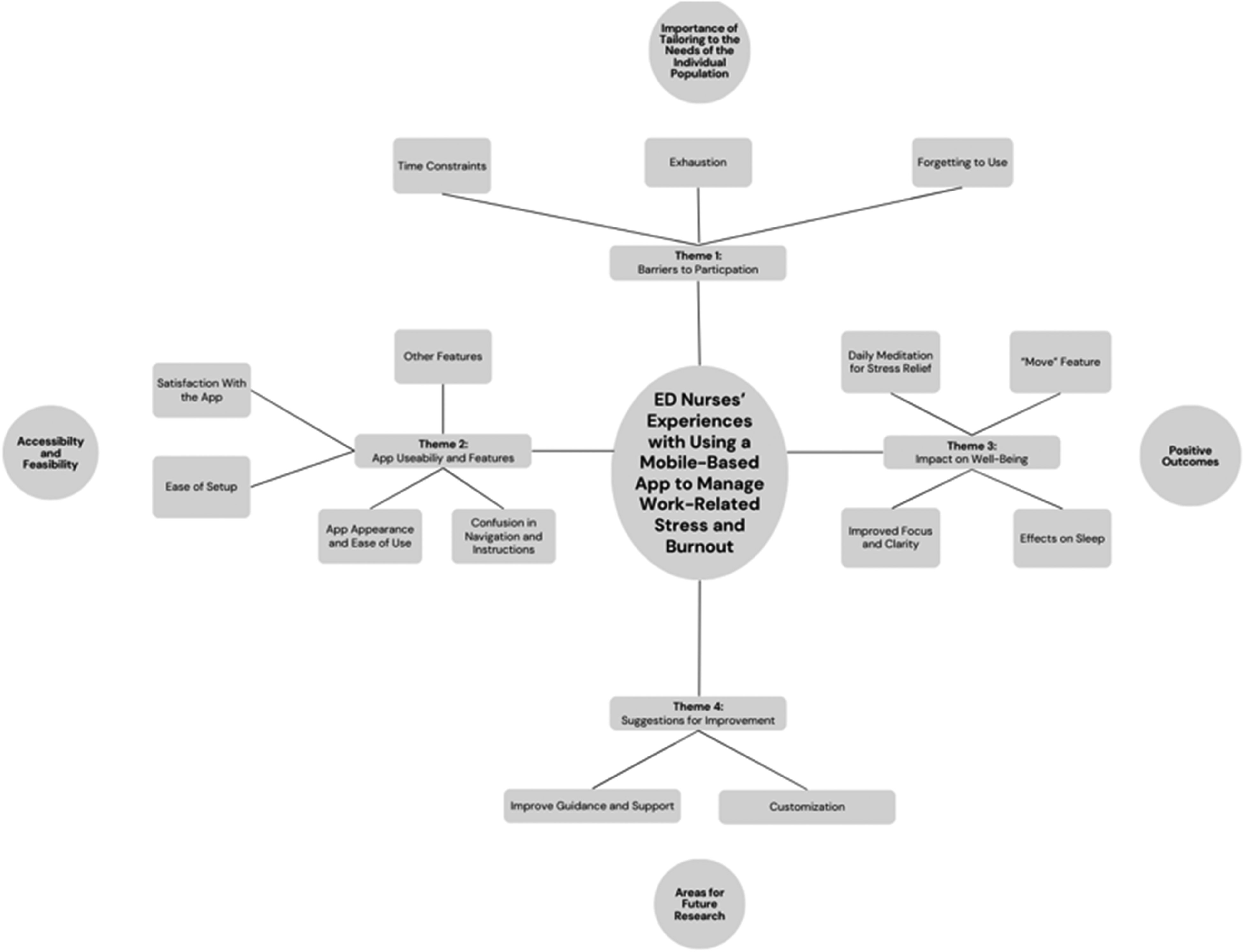
Thematic map.
To assess the validity of the themes, reflexivity was practiced by the researchers through iteration and reflection, by continuously revisiting the codes and themes in order to ensure they were grounded in data and not by any underlying personal assumptions of the researchers (Braun et al., 2006, 2019). Additionally, the researchers engaged in peer debriefing by discussing codes and themes with the other members of the research team in order to challenge any biases and examine additional emerging themes (Braun et al., 2006, 2019). Another member of the team also analyzed a subsample of the transcripts in order to assess reliability.
Results
Quantitative Analysis of Outcomes
Demographic Data
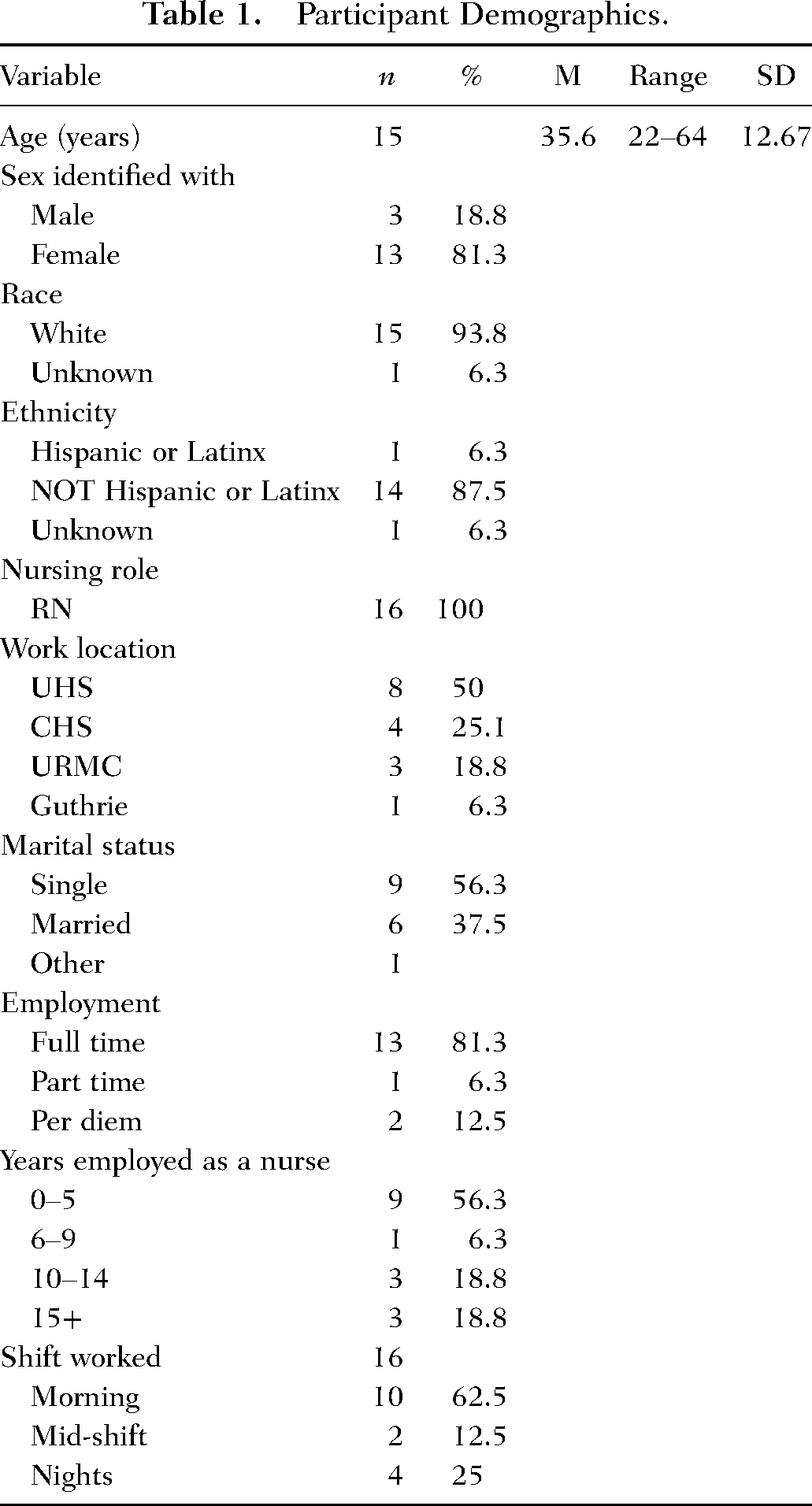
A total of 16 participants filled out pre-intervention demographic data. The demographic characteristics of this sample are summarized in Table 1. The sample consisted of 81% female (n = 13) and 23% male (n = 3). Ages ranged from 22 years to 64 years with a standard deviation of 12.68. Race was reported as white (n = 15), and unknown (n = 1). Ethnicity of the respondents was Hispanic/Latino \(n = 1,) non-Hispanic/Latino (n = 14), unknown (n = 1), and no answer (n = 1). 100% of participants worked as a Registered Nurse (n = 16), and location of work was reported as United Health Services (n = 8), Catholic Health (n = 4), Guthrie Cortland Medical Center (n = 1), and University of Rochester Medical Center (n = 3). Marital status was reported as single (n = 9), married (n = 6) and other (n = 1). Employment status was reported as full time (36.5 hours/week) (n = 13), part time (n = 1), per diem (n = 2). Years employed as a nurse ranged from 0 to 5 years (n = 9), 6 to 9 years (n = 1), 10 to 14 years (n = 3), and 15+ years (n = 1). Shift worked was reported based on whatever a majority of the participants’ work hours fell within and were reported as morning (0700–1900) (n = 10), mid shift (1100–2300) (n = 2), and night shift (1900–0700) (n = 4).
Participant Demographics.
Post-intervention demographic data was collected from n = 11 participants who completed the study. There were no differences in the characteristics of those who completed or did not complete the intervention.
Note: Work location, United Health Services Hospitals (UHS), Catholic Health Systems (CHS), University of Rochester Medical Center (UMRC).
Descriptive Analysis of App Use
The participants (n = 11) used the app for various amounts of time over the 4-week intervention period. The average number of days the app was used was 10.27, with a standard deviation of 9.84 days and a range of 1 to 28 days. The average number of minutes the app was used per day was 7.11 minutes with a standard deviation of 10.3 minutes and a range from 1 to 90 minutes per day.
Statistical Analysis
A Wilcoxon signed-rank test was used to compare nurses’ pre- and post-intervention scores on burnout, perceived stress, mindfulness, and well-being. Results indicated there was no significant difference between the nurses’ levels of burnout (EE, DP, PA) at baseline and after using a mobile mindfulness app for 4 weeks (see Table 2), although r = .36, .38, and .28 in each of the subscales respectively, suggesting medium effect sizes. Of the 11 participants, 6 reported higher EE, 5 reported lower EE, 6 reported higher DP, 5 reported lower DP, 4 reported lower PA, and 7 reported higher PA, all following the 4-week intervention
Pre- and Post-Intervention Outcomes.
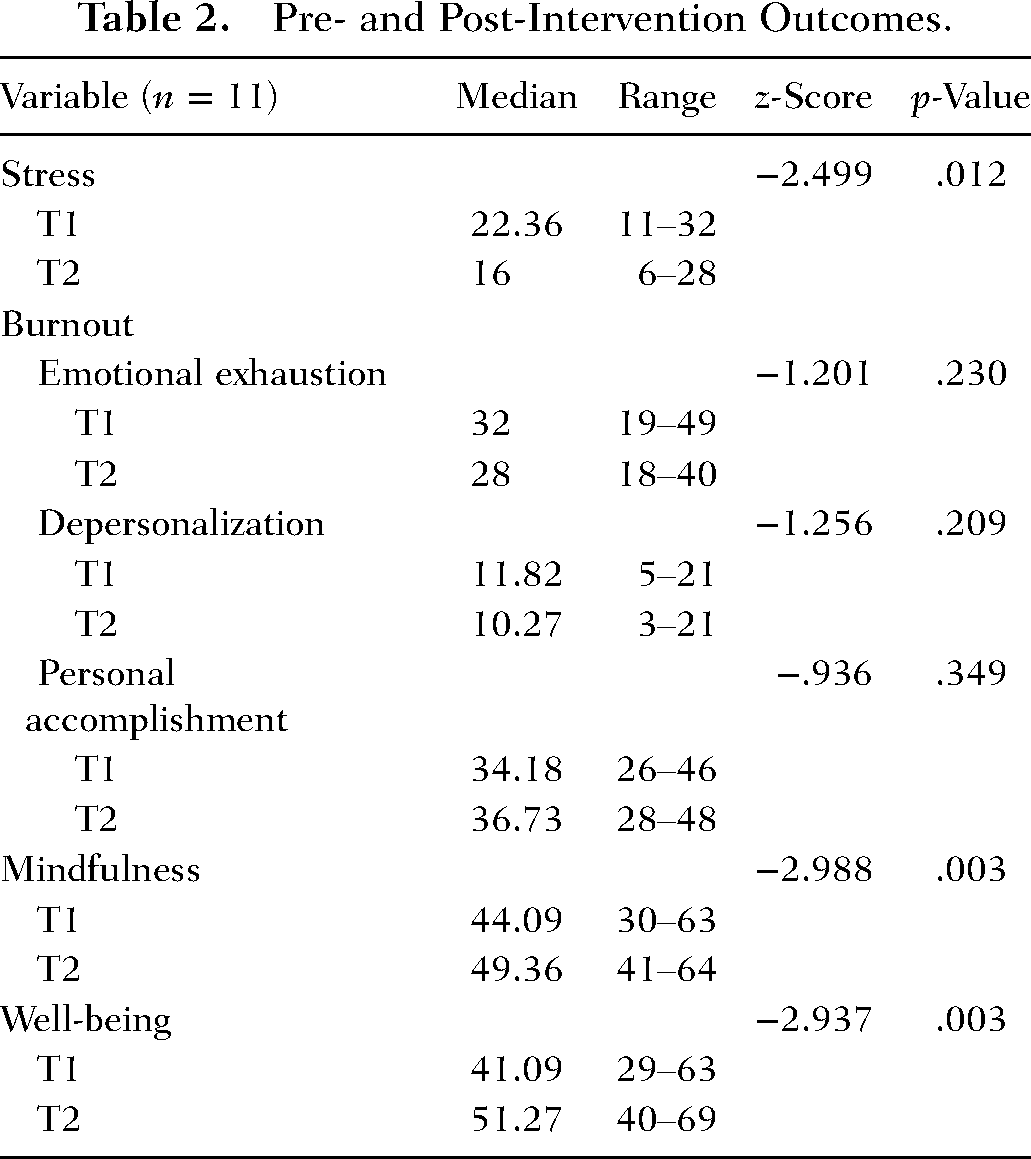
Of the 11 participants, eight reported less stress, two reported higher stress, and one reported the same amount of stress on the post-intervention measure compared with the pre-intervention assessment. Overall, the nurses’ median levels of perceived stress were significantly lower after 4 weeks (Mdn = 16) than at baseline (Mdn = 24), z = -2.499, p = .012, r = .75, suggesting a large effect size. Of the 11 participants, all reported higher mindfulness on the post-intervention measure compared with the pre-intervention assessment. The median levels of mindfulness of the nurses were significantly higher after using the mobile mindfulness app for 4 weeks (Mdn = 49) compared to mindfulness scores at baseline (Mdn = 42), z = -2.99, p = .003, r = .90, suggesting a large effect size. Of the 11 participants, all reported higher well-being on the post-intervention measure compared with the pre-intervention assessment. Nurses’ median levels of well-being were significantly higher after using the mobile mindfulness app for 4 weeks (Mdn = 53) compared to well-being scores at baseline (Mdn = 41), z = -2.94, p = .003, r = .89, suggesting a large effect size.
Qualitative Analysis
Qualitative findings from the pre-intervention surveys (n = 16), post-intervention surveys (n = 11), and semi-structured interviews (n = 9) were combined into a unified thematic analysis. Four overarching themes emerged: Motivations and Barriers to Participation, App Use and Usability, Impact on Well-Being, and Recommendations for Improvement. Presenting the themes holistically allowed pre- and post-intervention perspectives to be interpreted together.
Theme 1: Motivations and Barriers to Participation
Across data sources, participants described a mix of personal and professional motivations for engaging with the intervention. Before beginning the program, many nurses expressed a desire for mental health support, increased self-awareness, and opportunities to contribute to nursing research. Some also hoped the intervention might alleviate unresolved workplace stressors and restore a sense of purpose in their ED practice.
However, these motivations were consistently challenged by substantial barriers revealed in both pre- and post-intervention data and explored further in interviews. Time constraints were the most pervasive barrier, with demanding 12-hour shifts, unpredictable workloads, and competing responsibilities reducing nurses’ capacity to integrate daily meditation. Nurses frequently forgot to use the app or lacked the cognitive energy to engage after emotionally taxing shifts. Many described “survival-oriented” coping—pushing through exhaustion or disengaging emotionally—rather than sustainable wellness-focused strategies. “We do work 12 and a half hour shifts. Then I came home, and I would have to take care of my son and then eat some food and get changed and ready for bed, and then I was pretty exhausted. So, the thought of going on the app and doing the meditation was a little bit tougher. Most of the days that I missed were days that I was actively working.” (p4) “I think the temptation was really strong whether it was early in the morning or late at night, after a shift, just to, you know, doom scroll on social media instead of using the app just because it felt easier.” (p1) “My schedule as a night shifter is rather volatile. And by the time I was done with a shift, I wanted to come home, do my daily rituals and pass out. Adding something onto that, or getting up early for it [meditating] was…just kind of on a back burner for me, cause I’m exhausted all the time….I’d just kind of give up. I’m tired. I’m going to bed. This is too much brain power for me…” (p2)
Theme 2: App Use and Usability
Across the post-intervention survey and interviews, most participants reported using the mindfulness app regularly, though with significant variation based on schedule, energy, and memory. Over half of the sample used the app daily or almost daily, while others engaged sporadically due to workload or forgetting. The app's onboarding process and overall design were perceived as simple and accessible, with participants noting that setup was straightforward. Aesthetics and the organization of the “Today” home screen helped support ease of use by offering day-part–specific suggestions (“Start your day,” “Your afternoon lift,” “At night”). Many nurses also explored additional app features beyond the prescribed daily meditation, noting the breadth of content allowed them to tailor their practice to their emotional state in the moment. “There was one day I was feeling just super overwhelmed with everything. I looked up ‘overwhelmed’ in the app, and a bunch of stuff came up. Just a ton of helpful mindfulness activities that had to do with overwhelmed feelings or that kind of stuff. That was really helpful.” (p6)
Theme 3: Impact on Well-Being
Participants consistently described meaningful psychological and emotional benefits from the app when they were able to engage with it. The “Daily Meditation” was perceived as the most impactful feature, offering moments of calm, grounding, and emotional release after demanding shifts. Nurses repeatedly described these sessions as a mental “reset,” helping them decompress and transition out of high-intensity clinical environments. “I definitely say it did have a positive impact…especially after having a rough shift. You kind of look forward and look towards something that will kind of help you come down off of that either high stress moment or that adrenaline high that you were going through. (p4) “…the ‘move’ section of the app, the stretches, the morning movement classes, I think really helped me to get moving before a shift, and then being able to stretch and release some of the tension after a shift.” (p1) “I think overall, it just kind of helped to calm me down, probably relax my heart, rate, my respiratory rate. Overall kind of provide some good mental health and good clarity.” (p8) “Yes, definitely, I did notice a difference when I use the app. How much easier it was to calm down before bed, and how much easier it was to fall asleep.” (p1) “I think it was a good thing that it helped with sleep, because the last couple of the nights that I didn't put it on, I didn't sleep well at night…there was a couple of nights that I used it consecutively and I slept through the night. And then then the nights that I get busy and forget to turn it on. I'm awake at like 3 o'clock in the morning.” (p9)
Theme 4: Recommendations for Improvement
Participants offered thoughtful suggestions to enhance the intervention's usability and alignment with clinical realities. Many recommended providing a short onboarding tutorial or more structured guidance at the start of the study to help users understand how to navigate the app and incorporate mindfulness into their daily flow. Visual cues such as home-screen widgets or personalized prompts were suggested to support memory, reduce cognitive load, and reinforce routine practice.
Customization of content to better reflect the emotional challenges and stressors unique to emergency nursing was also recommended. Nurses expressed interest in meditations addressing situational stressors, emotional fatigue, high acuity environments, and workplace trauma. These suggestions align with holistic nursing values emphasizing individualized care and the need for tailored, context-responsive interventions. “What is it that you need today? How do you feel on a scale, you know, what's your mood like? And then here's a recommendation. It can be helpful to just kind of be told what to do in an app like that.” (p5)
Discussion
Mindfulness enhances the nurse's ability to be fully present, grounded, and attentive—qualities essential to fostering authentic nurse-patient connections (Bostock et al., 2019; Kreitzer, 2015; Mani et al., 2015). Through regular mindfulness practice, nurses cultivate deeper self-awareness and emotional regulation, which helps reduce reactive behaviors and improve compassionate communication (Brooke, 2021). This presence creates a healing environment where patients feel seen, heard, and valued as whole persons, not just as medical conditions. In holistic nursing, this intentional presence is a core component of therapeutic healing relationships and is foundational to delivering care honoring the mind, body, and spirit of both patient and nurse (AHNA, 2019; Helming et al., 2020).
Implications for Holistic Nursing Practice
The findings of this study have several important implications for the advancement of holistic nursing practice. First, the use of a mobile mindfulness intervention reinforces the role of self-care as a cornerstone of holistic nursing and aligns with the American Holistic Nurses Association's (AHNA) Scope and Standards of Practice, which calls for nurses to engage in self-reflection and self-care as ethical and professional responsibilities (AHNA, 2019). These standards emphasize the importance of creating healing environments—not only for patients, but also for caregivers themselves (AHNA, 2019; Helming et al., 2020; Kreitzer, 2015; Kreitzer & Koithan, 2018).
Second, by promoting improved stress management, mindfulness, and well-being, the intervention supports nurses in delivering more present, compassionate care. These outcomes are consistent with the INF, which emphasizes the interconnectedness of caregiver and patient well-being (Kreitzer, 2015; Kreitzer & Koithan, 2018.) Finally, this study highlights the need for organizations to integrate holistic strategies into nursing support structures and education, thereby creating sustainable models for workforce wellness.
Key Findings
This mixed-methods pilot study explored the use of the mobile app, Headspace, as a holistic intervention to manage stress and burnout among ED nurses. The four-week intervention yielded statistically significant improvements in participants’ stress, mindfulness, and overall well-being. The findings support the feasibility and potential of such an intervention and reinforce the core principles of the INF, which guided the study. By integrating quantitative and qualitative data, several thematic insights emerged, each aligned with INF's core concepts of whole-person care, innate healing, and relationship-centered practice (Kreitzer, 2015; Kreitzer & Koithan, 2018.).
Participants noted improvements in their ability to self-regulate, feel present, and manage emotional distress. While statistical significance in burnout reduction was not achieved, likely due to the small sample and short intervention timeframe, qualitative responses suggested meaningful shifts in perception. These observations align with the INF principle that individuals possess an innate capacity for health and well-being (Kreitzer, 2015; Kreitzer & Koithan, 2018). Nurses described feeling more centered, calmer during shifts, and empowered to pause and reflect, indicating the app's role in activating this intrinsic healing potential.
Participants shared that using the app allowed them to approach patient care with more empathy and attentiveness. These reflections speak directly to INF's emphasis on person-centered and relationship-based care, reinforcing the link between caregiver well-being and compassionate care delivery (Kreitzer, 2015; Kreitzer & Koithan, 2018.). This echoes Brooke (2021), who emphasized mindfulness as a pathway to spiritual grounding and deeper presence in chaotic healthcare environments.
Logistical barriers such as time constraints, lack of organizational support, and inconsistent app use were echoed in both the current study and prior literature (Aghamohammadi et al., 2022; Ameli et al., 2020; Cascales-Perez et al., 2021; Fong et al., 2022; Ireland et al., 2017; Janzarik et al., 2022; Kober & Chang, 2024; Ksiksou et al., 2023; Lei et al., 2023; Lilly et al., 2019; Lin et al., 2019; McConachie et al., 2014; Wang et al., 2024; Watanabe et al., 2019; Yıldırım & Yıldız, 2022). These challenges reflect INF's recognition that human beings are inseparable from their environments (Kreitzer, 2015; Kreitzer & Koithan, 2018.). Participants often cited workplace culture and workload as deterrents to regular mindfulness practice, indicating that broader systemic changes are needed to foster healing environments. Despite barriers, the app's convenience and self-paced nature were appreciated, especially among those with demanding shift schedules. This supports INF's principle of using the least invasive, most effective intervention appropriate to the situation (Kreitzer, 2015; Kreitzer & Koithan, 2018.). Mobile delivery allowed for flexibility, supporting nurses’ varying needs and schedules, which is an important consideration for scalable workplace wellness initiatives.
The narrative that “nurses must care for themselves as they care for others” was prevalent throughout the responses, resonating with the current ANA Code of Ethics (Faubion, 2024). The INF's prioritization of caregiver health was operationalized in this study by offering an accessible and innovative tool to foster psychological and emotional well-being. Nurses not only recognized self-care as necessary but framed it as ethical; a responsibility rather than a luxury.
Participants reported improved ability to decompress after work, better focus, improved sleep, and a sense of emotional regulation from engaging with the app. Many found the app convenient and helpful, despite some usability issues. These findings align with current literature on MBIs and their benefits for psychological health among healthcare workers (Aghamohammadi et al., 2022; Ameli et al., 2020; Fong et al., 2022; Keng et al., 2022; Ksiksou et al., 2023; Lei et al., 2023; Lin et al., 2019; Monfries et al., 2023; Trygg Lycke et al., 2023; Wang et al., 2024; Watanabe et al., 2019; Xu et al., 2022; Yang et al., 2018).
Additionally, narrative responses and interviews highlighted existing strategies ED nurses use to manage stress, such as seeking social support, detaching from work outside of hours, and using informal mindfulness practices. However, a notable portion of participants expressed a lack of effective coping strategies, reinforcing the need for accessible and supportive interventions like the one piloted in this study. When asked about employer support, many participants expressed dissatisfaction with current organizational efforts to address burnout and stress. Themes emerged around systemic barriers including staffing shortages, inadequate mental health resources, and a general lack of institutional prioritization of well-being.
All of the participants in this study expressed satisfaction with using the app for the intervention time frame and they would continue using it for the remaining time they have available in their subscriptions they received for participating. This aligns with the existing literature published on Headspace's useability, which supports it scoring highly in user engagement, functionality, appearance and overall quality as an app (Lim et al., 2015).
The ED nurses who participated in this study also shared suggestions for improvement with the app, and with future research of this kind. As previously mentioned as a barrier, it was additionally suggested by participants that improving guidance at the beginning of the intervention could help the users with effectively adding the use of the app into their daily routine and optimizing the experience. Some users suggested changes to the Headspace platform, such as adding more customizable notifications to maximize engagement, adding toggle on-and-off features to limit “clutter” or distractions on the app, or the inclusion of routines and features specifically designed for healthcare workers like nurses. These suggestions are all valuable insights to bring forward in future research opportunities of this kind. These main themes indicate the app offers clear benefits in supporting stress reduction, mindfulness, and emotional well-being—key aspects of holistic self-care—however, barriers such as time constraints, physical exhaustion, and usability challenges can hinder consistent engagement. Addressing these concerns through more personalized, accessible, and user-centered features may enhance the app's effectiveness as a holistic intervention and strengthen its role in fostering sustainable healing practices for nurses.
Despite growing awareness of workplace burnout among healthcare professionals, findings from this study suggest that organizational and state-level policies continue to fall short in adequately supporting ED nurses. While some institutions offer wellness programs, flexible schedules, or mental health services, access and utilization remain inconsistent, many participants described these resources as poorly communicated or under-promoted, which aligns with previous research (Kober & Chang, 2024). Several ED nurses reported a lack of meaningful engagement from leadership and upper management and perceived that organizational support was superficial or insufficient in addressing the severity of their work-related stress. Moreover, participants highlighted that leadership was often disconnected from the realities of bedside care, especially in high-intensity environments like the ED. Notably, one participant suggested the responsibility to address mental health and burnout should extend beyond the organization to include community and governmental involvement, which frames the issue as a broader public health crisis rather than just an employer obligation (Kober & Chang, 2024). These sentiments align with national reports suggesting only 5% of nurses feel their organization effectively supports them with burnout, despite nearly 16% reporting symptoms of burnout (The Joint Commission, 2019).
Overall, while some organizational efforts are promising, meaningful and sustained change requires a holistic systems approach—one including compassionate leadership engagement, routine assessment of emotional and spiritual well-being, stigma reduction around mental health, and equitable access to integrative, evidence-informed interventions specifically designed to support the unique needs of nurses in high-stress roles like the ED. These efforts must foster a culture of caring, prioritizing the well-being of the whole nurse—mind, body, and spirit (Brooke, 2021; Kober & Chang, 2024)
Finally, by examining the use of a mobile-based mindfulness app to reduce stress and burnout in ED nurses, this study addresses a critical gap in the availability of holistic self-care modalities tailored to high-acuity nursing environments. Mobile mindfulness interventions offer a practical and accessible way to support emotional regulation, resilience, and mind-body-spirit balance amid the unpredictable demands of emergency care. In holistic nursing, self-care is not a luxury but a professional responsibility—essential to sustaining presence, therapeutic relationships, and safe, whole-person care. Yet, self-care among nurses is often neglected due to systemic barriers and cultural norms undervaluing the well-being of the caregiver (Nkabinde-Thamae et al., 2022). Many nurses report persistent workplace stress compromises their physical and emotional health, ultimately affecting the quality and safety of patient care (Nkabinde-Thamae et al., 2022). To truly embody the values of holistic nursing, practitioners must be supported in cultivating self-awareness, empathy, and self-compassion—capacities which mindfulness practices have been shown to enhance. Integrating such interventions into the professional culture of nursing can help restore the caregiver's capacity to heal, promote sustainability in practice, and uphold the integrity of holistic care delivery (Trygg Lycke et al., 2023).
The study's findings strongly align with the INF, which emphasizes person-centered, relationship-based care grounded in whole-person healing and well-being (Kreitzer, 2015; Kreitzer & Koithan, 2018). The use of a mobile mindfulness app, as demonstrated in this study, embodies the core principle that all people, patients and caregivers alike, have innate healing capacities that can be supported through holistic, evidence-informed practices. By integrating mindfulness into daily routines, ED nurses were empowered to care for themselves in a way that respects their unique needs, rhythms, and challenges. This intervention reflects the framework's emphasis on creating healing environments and leveraging simple, accessible modalities to promote resilience, self-awareness, and healing. Ultimately, supporting nurses through integrative practices not only enhances their own well-being but also enables them to deliver more compassionate, connected care to others.
Implications for Future Practice and Research
Health Education
Healthcare professions such as nursing are inherently high-stress fields, with many stressors emerging as early as the academic setting (Barrett & Eschiti, 2020). Multiple studies have shown that nursing students report higher levels of stress compared to peers in other healthcare disciplines, with younger or less experienced individuals often exhibiting underdeveloped coping mechanisms, placing them at increased risk for burnout (Barrett & Eschiti, 2020; Pollard et al., 2023). Elevated stress during training can impair students’ ability to manage challenges effectively, diminish academic performance, and negatively affect the retention of critical knowledge (Barrett & Eschiti, 2020; Kinyon, 2021). Integrating mindfulness education into pre-licensure nursing curricula may serve as a proactive strategy to enhance the mental fitness and emotional resilience of future nurses.
By nurturing self-awareness, emotional regulation, and presence, these practices support the development of a strong foundation for holistic, person-centered care (Benzo et al., 2017). Future research is essential to explore the impact and feasibility of incorporating routine mental health screening and mindfulness-based self-care practices into nursing education. Doing so may help student nurses establish baseline strategies for managing stress and promoting well-being before they enter the clinical workforce, thereby reducing their vulnerability to burnout and supporting long-term professional sustainability.
Health Policy
A growing body of research highlights the strong association between workplace stress and self-reported declines in both mental and physical health. Workplace stress is estimated to account for 5–8% of annual healthcare costs in the United States (Chaudhry et al., 2022). Over the past two decades, dissatisfaction among hospital staff—particularly those in inpatient and acute care settings—has steadily increased, culminating in what many describe as a crisis during the COVID-19 pandemic (Bogue & Bogue, 2020; Laskowski-Jones L, 2019; McCauley & Irwin, 2006; Stimpfel et al., 2012). The Joint Commission recognized this escalating concern in its 2019 Quick Safety Advisory on “Developing Resilience to Combat Nurse Burnout,” identifying widespread workforce challenges and organizational gaps in supporting nurses (The Joint Commission, 2019). At that time, 15.6% of nurses reported experiencing burnout, while only 5% felt their organizations were adequately addressing it (Laskowski-Jones L, 2019; Yıldırım & Yıldız, 2022).
Given the well-documented consequences of workplace stress and burnout—both for the well-being of nurses and the quality of patient care—it is critical to identify sustainable, evidence-based strategies for prevention and support. Holistic nursing frameworks call for the creation of healing environments nurturing the whole person—mind, body, and spirit—and emphasize the importance of resilience, presence, and self-care as professional responsibilities (AHNA, 2019; Faubion, 2024; Helming et al., 2020; Kreitzer, 2015; Kreitzer & Koithan, 2018). Nurse researchers and leaders are uniquely positioned to influence policy by advocating for system-level changes to enhance job satisfaction, improve retention, and foster conditions supporting safe, compassionate, and high-quality care.
Mindfulness-based interventions (MBIs), particularly those delivered via mobile platforms, offer a promising, accessible avenue for stress reduction. These interventions empower nurses to engage in self-guided mind-body practices supporting emotional regulation, self-awareness, and psychological well-being—core tenets of holistic nursing (AHNA, 2019; Helming et al., 2020). However, to inform meaningful implementation and policy change, further research is needed to evaluate long-term outcomes across diverse settings and populations. Without robust evidence demonstrating their effectiveness and cost-benefit potential, healthcare institutions may be hesitant to adopt or fund such programs. Expanding the evidence base will be essential for advancing policies recognizing the value of integrative, nurse-centered wellness initiatives as both a workforce and patient care imperative.
Future Research
There remains a significant gap in mixed methods research critically examining how ED nurses navigate the persistent stress and emotional demands of their high-intensity clinical environments. This study addresses that gap by integrating qualitative narratives and interview data with quantitative measures of stress, burnout, mindfulness, and well-being. The findings offer meaningful insight into how ED nurses perceive and experience workplace stress, how they engage with mobile-based mindfulness interventions as a tool for self-care, and how a lack of organizational support often compounds their challenges.
By exploring these lived experiences through a holistic lens, this study contributes to a deeper understanding of the emotional and spiritual toll of frontline nursing and highlights the potential of mind-body interventions to support whole-person healing. The results inform practical recommendations for developing scalable, integrative strategies to reduce burnout and cultivate presence, resilience, and self-compassion among nurses.
Future research with larger, more diverse samples is needed to further evaluate the effectiveness and long-term impact of mobile mindfulness tools across varied healthcare settings. Such efforts will be essential for advancing policy, education, and practice initiatives prioritizing the holistic well-being of nurses. Centering the voices and needs of nurses in these initiatives can help promote sustainable self-care practices, enhance job satisfaction, reduce turnover, and ultimately contribute to the creation of more healing, human-centered healthcare systems and communities.
Limitations
This study had an attrition rate of 42%. Although specific reasons were not always known, qualitative feedback suggested two primary barriers: the demanding nature of ED work, which limits time and energy for optional activities, and limited awareness or understanding of mindfulness as a meaningful self-care practice. These insights indicate that engagement challenges may stem from both time constraints and knowledge gaps about holistic modalities. Future research should explore recruitment and retention strategies that incorporate education, organizational support, and more personalized engagement.
As a small pilot study without a control group, generalizability is limited. Larger samples, multiple settings, and controlled designs are needed to strengthen external validity (Polit & Beck, 2010). Although the mixed-methods approach allowed for triangulation, the four-week intervention period may have been too brief to detect changes in burnout, a construct that shifts gradually. Longitudinal research is recommended.
Recruitment challenges also impacted the sample size. All recruitment occurred virtually, which may have reduced connection and engagement; more direct or face-to-face strategies may be beneficial in future studies. Intervention fidelity varied, and inconsistent app use may have influenced outcomes, highlighting the need for strategies to support adherence.
Participants also expressed a desire for clearer onboarding support. Although written instructions were provided, several felt that a brief instructional video would have enhanced clarity and confidence. Future interventions should incorporate multimodal instructional materials to better support diverse learning preferences.
Selection bias remains a limitation, as individuals already interested in mindfulness may be more likely to participate. This was partially addressed by excluding individuals with a current mindfulness practice or recent use of a mindfulness app. Continued refinement of recruitment strategies is warranted to reduce volunteer bias (Polit & Beck, 2010).
Conclusion
This study examined the complex and multidimensional experience of stress and burnout among ED nurses through a holistic nursing lens, centering the lived experiences of clinicians working in one of the most demanding areas of healthcare. Grounded in the core values of holistic nursing—which emphasize whole-person care, self-awareness, presence, and the interconnection of mind, body, and spirit—this mixed-methods study explored both the measurable and narrative impacts of a mobile-based mindfulness intervention on stress, burnout, mindfulness, and overall well-being.
Quantitative results revealed statistically significant improvements in participants’ perceived stress, mindfulness, and well-being after the 4-week intervention. While reductions in burnout, as measured by the MBI-HSS, did not reach statistical significance, downward trends were observed, and qualitative interviews further contextualized these findings. Participants described experiencing meaningful relief from emotional exhaustion and stress-related symptoms, and valued the accessibility, flexibility, and supportive nature of the mindfulness app. At the same time, barriers such as time constraints, emotional fatigue, and usability challenges highlighted ongoing obstacles to fully integrating self-care into the daily routines of ED nurses.
This study affirms the critical need for healthcare systems to implement sustainable, integrative, and evidence-based strategies promoting clinician well-being—not as optional wellness offerings, but as essential components of professional practice and organizational responsibility. To advance a culture of whole-person care, healthcare organizations and academic institutions are encouraged to integrate accessible, evidence-informed holistic interventions into policies, workflows, and curricula prioritizing nurse self-care and emotional resilience. Mindfulness, particularly when delivered through mobile platforms, emerges as a practical and scalable intervention aligning with the principles of holistic nursing by empowering nurses to cultivate presence, resilience, and self-compassion in the midst of high-pressure environments.
Future research and policy initiatives should prioritize the integration of holistic, person-centered care models recognizing the well-being of nurses as foundational to quality patient outcomes and a sustainable healthcare workforce. By tailoring interventions to meet the unique needs of ED nurses—while also advocating for systemic changes reducing institutional sources of stress—this research contributes to a growing movement toward healing-centered work environments. In doing so, it reinforces the professional mandate within holistic nursing to not only care for others, but also to care for oneself as an ethical and healing practice.
Supplemental Material
sj-docx-1-jhn-10.1177_08980101261424557 - Supplemental material for Calm in the Chaos: A Mixed-Methods Pilot Study Using a Mobile Mindfulness App to Manage Stress and Burnout Among Emergency Department Nurses
Supplemental material, sj-docx-1-jhn-10.1177_08980101261424557 for Calm in the Chaos: A Mixed-Methods Pilot Study Using a Mobile Mindfulness App to Manage Stress and Burnout Among Emergency Department Nurses by Michelle Kober, PhD, RN, AHN-BC, Jennifer A. Livingston, PhD, Christopher Barrick, PhD, and Yu-Ping Chang, PhD, RN, FGSA, FAAN, FIAAN in Journal of Holistic Nursing
Footnotes
Author Contributions
Michelle Kober did conceptualization, methodology, formal analysis, investigation, writing—original draft preparation, review and editing.
Jennifer A. Livingston, Yu-Ping Chang, and Christopher Barrick did conceptualization, writing—review and editing.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request. To protect the confidentiality of the study participants, de-identified data may be shared with qualified researchers for academic or scholarly purposes, pending approval from the relevant Institutional Review Board and in accordance with ethical research guidelines.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was reviewed and approved by the Institutional Review Board at University at Buffalo (Protocol #FWA00008824).
Informed Consent
Informed consent was obtained from all individual participants involved in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Shirley DeVoe Nursing Research Support Fund.
Supplemental Material
Supplemental material for this article is available online.