
Abstract
Background
Bowel obstruction (BO) is a common surgical emergency often necessitating invasive intervention, including resection and potentially the creation of a stoma (Banerjee et al., 2023; Smith et al., Updated 2023, July 31). A stoma is a surgically created opening in the abdomen for waste elimination, which represents a significant alteration in bodily function and self-image. Beyond the significant physical trauma and long-term alterations in gastrointestinal function (Guillen & Atherton, Updated 2023, July 17; Ren et al., 2012), this diagnosis and its treatment represent a profound psychological stressor. The threat to bodily integrity, potential for a life-altering stoma, and fears about prognosis—particularly when related to an underlying malignancy—can trigger significant anxiety, stress, and depression (Ayaz-Alkaya, 2019; Hueso-Montoro et al., 2016). This psychological distress is not merely a secondary concern; it can directly impact recovery, quality of life, and a patient's capacity to engage in self-care.
Stress, anxiety, and depression represent distinct but interrelated psychological responses that frequently accompany major surgery (Loureiro et al., 2026; Tofthagen et al., 2026). Stress refers to the subjective experience of tension, irritability, and difficulty relaxing when demands exceed available coping resources (Tofthagen et al., 2026). Anxiety involves feelings of fear, apprehension, and physiological hyperarousal, often related to anticipation of future threats such as surgical complications or cancer diagnosis (Loureiro et al., 2026). Depression encompasses persistent low mood, loss of interest, feelings of hopelessness, and reduced energy that can impair motivation for self-care and recovery (Loureiro et al., 2026). Coping, as conceptualized by Lazarus and Folkman (1984), refers to the cognitive and behavioral efforts individuals employ to manage specific external and internal demands appraised as taxing or exceeding their resources (Biggs et al., 2017). For patients undergoing bowel obstruction surgery, these psychological states are particularly relevant given the sudden onset of symptoms requiring emergency intervention, the potential for life-altering stoma creation, the physiological stress of intestinal resection, and frequently, concerns about underlying malignancy as the cause of obstruction.
According to Lazarus and Folkman's (1984) Transactional Model of Stress and Coping, coping is a process-oriented endeavor where strategies evolve as an individual contends with a stressor (Ayaz-Alkaya, 2019; Lazarus & Folkman, 1984). For patients undergoing BO surgery, coping must address both practical, problem-focused challenges (e.g. learning ostomy care, managing nutrition) (Jeppesen & Fuglsang, 2018; Pironi, 2016) and profound emotion-focused challenges (e.g. managing fear, anxiety, and altered body image) (Schoenmakers et al., 2015; Torkzadeh et al., 2019). The literature suggests that the choice of coping strategies is intimately linked to prior experiences and the specific context of the illness (Hueso-Montoro et al., 2016; Torkzadeh et al., 2019), indicating a critical need for supportive, tailored interventions during this vulnerable period.
Holistic nursing is an approach that views the patient as a unified whole consisting of mind, body, spirit, and soul, functioning in dynamic interaction with the environment (Erickson, 2007; Frisch & Rabinowitsch, 2019). Within this framework, health represents balance and harmony among all dimensions, while illness reflects disequilibrium. The holistic nurse's role is to support patients in mobilizing their inherent healing capacities and self-care resources (Seager, 2018). This philosophical foundation distinguishes holistic nursing from conventional approaches that may focus predominantly on physical symptoms.
Nurses are uniquely positioned to use a holistic approach in helping patients modify their emotion-focused and meaning-focused coping processes. A human being, within a holistic framework, is seen as a unique whole comprising mind, body, spirit, and soul—an integrated system that cannot be reduced to its parts (Seager, 2018). Within this holistic framework, the human being exists in dynamic interaction with self, others, and the environment. When all dimensions—mind, body, spirit, and soul—are in balance and harmony, maximum well-being occurs (Erickson, 2007). The patient is viewed as a knowledgeable and capable individual who can focus their consciousness on accessing life goals and self-care resources. The individual consciously confronts the stressors present in their life and intentionally directs the changes caused by illness toward achieving healing. The primary purpose of holistic nursing is to intentionally assist patients in utilizing their potential abilities to enhance their self-care resources and adapt to the stressors and changes resulting from their disease process (Frisch & Rabinowitsch, 2019).
Presence as a Nursing Intervention
The concept of presence has been conceptualized in various ways within nursing literature, including caring presence, authentic presence, therapeutic presence, true presence, and intentional presence (Covington, 2003; Easter, 2000; McKivergin & Daubenmire, 1994). While these terms share common elements—such as being with the patient, attentiveness, and connection—they emphasize different aspects of the nurse–patient relationship. For this study, we focus on intentional presence, which refers to the nurse's conscious, purposeful, and authentic engagement with the patient that creates a healing connection (Aghebati et al., 2015).
The intentional presence of the nurse during a transpersonal caring relationship with the patient is considered one of the core interventions of holistic nursing (Gelogahi et al., 2018). In a concept analysis, intentionality was defined as a matrix of continuous known changes that may provide a structure giving meaning to experiences. Intentionality was conceptualized in two forms: intentionality as a capacity of a human being and intentionality as a capacity of transpersonal caring (Aghebati et al., 2015). When a person encounters disequilibrium that they do not know how to handle, they perceive the need to refer to a healthcare provider. Then, intentionality as a capacity for transpersonal caring becomes focused (Aghebati et al., 2015).
McKivergin and Daubenmire (1994) conceptualized presence at three levels: physical (body to body), psychological (mind to mind), and therapeutic (spirit to spirit). Physical presence means the nurse is at the patient's bedside, establishing the foundation for any transpersonal relationship. Psychological presence commences when the patient notices the nurse's attention through active listening and engagement. Therapeutic presence begins when the patient discusses concerns and the nurse employs appropriate interventions, which may include auditory approaches (music therapy), visual methods (imagery), tactile methods (therapeutic touch), olfactory methods (aromatherapy), kinesthetic methods (relaxation movements), and cognitive methods (education) (McKivergin & Daubenmire, 1994). Intentional presence occurs when the nurse's heart connects with the patient's, evidenced by the patient's trust and willingness to express problems and needs (Aghebati et al., 2015).
According to a mid-range theory of nursing presence (McMahon & Christopher, 2011), five types of characteristics influence intentional presence: individual nurse characteristics, individual client characteristics, shared characteristics within the nurse–client relationship, an environment conducive to relational work, and the nurse's intentional decisions within the practice domain.
Linking Intentional Presence to Study Outcomes
Intentional presence is theorized to reduce stress, anxiety, and depression by creating a safe interpersonal space where patients feel heard, understood, and supported (Covington, 2003). Through this connection, patients can explore their fears, receive validation, and develop more effective coping strategies. The nurse's authentic engagement helps patients access their inner resources, identify meaning in their illness experience, and mobilize adaptive coping mechanisms (McMahon & Christopher, 2011). For patients undergoing BO surgery—who face multiple stressors including pain, altered body image, nutritional challenges, and potential cancer diagnosis—this supportive relationship may be particularly beneficial in facilitating psychological adaptation.
While several articles address the conceptualization of intentionality (Aghebati et al., 2015) and presence (Covington, 2003; Easter, 2000; McKivergin & Daubenmire, 1994), only one study has examined the effect of a nurse's intentional presence on anxiety, stress, and depression—in patients undergoing open-heart surgery (Gelogahi et al., 2018). Although the results indicated a positive effect, the researchers did not discuss methods used to verify the nurse's abilities as a key element in intentional presence, and recommended further studies to clarify the intervention process and “dosage” of nurse presence.
Patients undergoing BO surgery experience various disturbances in the absorption of food, water, and electrolytes due to the extent of surgery and intestinal resection (Guillen & Atherton, Updated 2023, July 17; Pironi, 2016). Additionally, because of complications associated with many problem-focused coping strategies after surgery, these patients face severe mental pressure manifesting as stress, anxiety, and depression. To date, no study has focused on improving coping processes based on problem-focused, emotion-focused, and meaning-focused coping simultaneously in patients undergoing BO surgery. Therefore, the present study aims to determine the effect of the nurse's intentional presence as a holistic intervention on stress, anxiety, depression, and coping strategies in patients undergoing bowel obstruction surgery.
Method
Study Design
This study was a randomized controlled trial with two parallel groups (intervention and control), conducted from March 2021 to October 2022.
Study Setting
The study was conducted at Qaem Hospital, Mashhad University of Medical Sciences, IR.MUMS.NURSE.REC.1399.033—a tertiary referral center for gastrointestinal surgery.
Ethical Considerations
The study protocol was approved by the Ethics Committee of Mashhad University of Medical Sciences and registered with the IR.MUMS.NURSE.REC.1399.033 All participants provided written informed consent. Participants were assured of questionnaire anonymity and data confidentiality.
Participants
Inclusion Criteria: Patients were eligible if they: (1) aged 20–70 years; (2) able to read and write; (3) underwent bowel obstruction surgery with intestinal resection length <120 cm; (4) no history of drug addiction; and (5) owned a smartphone to enable communication and delivery of educational materials (acknowledged as a limitation).
Exclusion Criteria: Potential participants were excluded if they: (1) were scheduled for long-term hospitalization (>1 month) for a comorbid condition; or (2) had a clinical prognosis suggesting high mortality risk within 1 month.
Withdrawal Criteria: Participants were withdrawn if they: (1) withdrew consent; (2) were hospitalized >1 month; (3) died during the study; (4) attended <3 of 5 in-person sessions; or (5) were unreachable for follow-up calls.
Sample Size Calculation
The sample size was calculated using PASS software, prioritizing the stress outcome as the primary variable of interest. Due to the absence of prior studies examining intentional presence in patients undergoing bowel obstruction surgery, we drew upon the most relevant available evidence. The primary basis for our calculation was Gelogahi et al. (2018), which examined the same intervention (intentional presence) in a different surgical population (coronary artery bypass surgery). This study reported a mean stress score of 10.23 ± 3.9 in the control group and 7.23 ± 3.1 in the intervention group postintervention, representing a clinically meaningful difference of 3 units. We selected the more conservative estimate (variance of 3.9) to ensure adequate power even if the effect size in our population proved smaller than that observed in cardiac surgery patients. While we acknowledge that effect sizes may vary across surgical populations, no published studies existed in bowel obstruction patients at the time of protocol development. The study by Guo et al. (2013) on growth hormone and intestinal adaptation was referenced only for methodological guidance on sample size calculation in gastrointestinal surgery populations, not for effect size estimation (Guo et al., 2013).
With a two-sided significance level of α = 0.05, power of 90% (β = 0.10), and assuming a detectable mean difference of 3 units in stress scores with a common standard deviation of 3.9 (effect size d = 0.77), the required sample size was calculated as 28 participants per group. To account for potential attrition (estimated at 10%), we increased this to 31 participants per group, yielding a total sample of 62 participants (Figure 1).
The CONSORT Diagram of Research.
Sensitivity Consideration: We acknowledge that if the true effect size in bowel obstruction patients is smaller than observed in cardiac surgery patients (e.g. d = 0.5), our study would have approximately 70% power to detect such a difference. This limitation is addressed in the Discussion section.
Sampling and Randomization
Patients were selected through convenience sampling from those meeting inclusion criteria. Random allocation used permuted blocks (block sizes of 4 and 6) generated by an independent statistician. Allocation sequences were concealed in sequentially numbered, opaque, sealed envelopes opened by a ward nurse not involved in the study.
Blinding
Due to the nature of the psychosocial intervention, blinding of participants and the nurse intervenor was not feasible. However, data analysis was performed by a statistician blinded to group allocation. Outcome data were collected via self-report questionnaires, minimizing assessor bias.
Intervention: Intentional Presence as a Holistic Nursing Framework
The intervention was delivered by a single trained researcher (the principal investigator) following a structured protocol while allowing individualization based on Holistic Needs Assessment (HNA) results. The intervention is conceptualized as a multi-level, relationship-based framework derived from holistic nursing theory rather than a single discrete component.
Phase 1: Professional Preparation of the Nurse
The researcher acquired specialized knowledge through: (1) review of relevant literature and clinical guidelines for bowel obstruction care; (2) supervised clinical practice in the abdominal surgery department to strengthen practical skills; and (3) completion of a short educational course on ostomy care.
Phase 2: Development of Comprehensive Holistic Care Plan
Based on a standard nursing care plan for abdominal surgery (Doenges et al., 2022), a comprehensive postoperative nursing care plan was developed specifically for patients undergoing bowel obstruction surgery. Table 1 presents the comprehensive postoperative nursing care plan developed for this study. This table is organized by nursing diagnosis (e.g. Ineffective Coping, Anxiety, Imbalanced Energy Field, Disturbed Body Image) and maps each diagnosis to: (1) expected outcomes using the Nursing Outcomes Classification (NOC); (2) standard nursing interventions using the Nursing Interventions Classification (NIC); and (3) the specific holistic nursing interventions derived from the intentional presence framework. As shown in the table, intentional presence is operationalized through diverse therapeutic modalities including active listening, educational video clips, relaxation techniques, heart-to-heart relationship building, unconditional acceptance, self-care enhancement training, and spiritual support. This table demonstrates that education, clinical care, and emotional support are not separate from intentional presence but rather constitute the therapeutic methods through which intentional presence is expressed and experienced by the patient.
Postoperative Nursing Care Plan of Patient Undergoing Bowel Obstruction Surgery
Phase 3: Development of Educational Materials
To support the cognitive therapeutic methods within the intentional presence framework, fourteen educational video clips were created covering the following topics: intestinal resection surgery methods, digestive system anatomy, ileostomy and colostomy care, techniques for changing a stoma bag, an introduction to different types of stoma bags, effective coughing techniques, active and passive exercises, and diaphragmatic breathing with relaxation methods. Additionally, three educational pamphlets were prepared, titled “Living with Colostomy,” “Nutrition for Patients with a Stoma,” and “Nutrition for Patients with Intestinal Obstruction.” These materials were introduced to intervention group participants within the context of the therapeutic relationship rather than as standalone information transfer.
Phase 4: The Nurse–Client Relationship in Intentional Presence
The nurse–client relationship unfolded through a structured sequence of interactions designed to progressively deepen the therapeutic connection across the three levels of presence—physical, psychological, and therapeutic—as conceptualized by McKivergin and Daubenmire (1994). Figure 2 illustrates this dynamic process and its outcomes.
The Process of Intentional Presence.
At the base of Figure 2, patients are shown entering the relationship in a state of distress characterized by anxiety related to surgical complications, unmet needs across multiple dimensions, ineffective coping strategies, stress, deficient knowledge about self-care, and imbalanced energy field. The central pathway demonstrates the progression of the nurse–patient relationship through three interconnected levels. Physical presence (body-to-body) begins when the nurse admits the patient with kindness and compassion, establishing physical proximity through clinical care. Psychological presence (mind-to-mind) develops as the nurse engages in active listening, counseling, and nonjudgmental acceptance, establishing a transpersonal caring relationship where the patient feels understood and safe. Therapeutic presence (spirit-to-spirit) emerges as trust develops, enabling the nurse to determine the appropriate “dose” of presence—tailoring the intensity and focus of engagement to the patient's unique needs identified through the Holistic Needs Assessment (HNA). This heart-to-heart connection allows the patient to share deeper concerns and engage more fully in the healing process. At the apex of Figure 2, the outcomes of intentional presence are realized, including enhanced coping strategies, fulfilled needs across holistic domains, reduced stress and anxiety, satisfaction with the caring process, and mutual growth in the experience of intentional presence for both patient and nurse.
This relational process was operationalized through five in-person sessions conducted during hospitalization, followed by telephone support for 1-month postdischarge. Table 2 presents the detailed structure, objectives, key activities, and intentional presence strategies for each session, demonstrating how the three levels of presence were progressively enacted throughout the intervention.
Intentional Presence Session Structure
The term “dose of presence” refers to the intensity and customization of the intervention within this standardized session structure. While the number of sessions (five in-person, eight or more telephone calls) was fixed to ensure consistency for the trial, the content and focus of each interaction were personalized based on HNA results. The HNA, administered during the initial sessions, identified specific patient concerns across physical, practical, social, emotional, and spiritual domains. The researcher used this assessment to prioritize topics, allocate time within sessions to the patient's most pressing needs, and tailor the guidance provided during both in-person and telephone interactions. Therefore, the dose of presence was defined by the combination of a standardized minimum number of contacts and a patient-centered, needs-based approach to the content of those contacts, as illustrated in Figure 2.
Control Group
Participants in the control group received routine hospital care, including vital sign monitoring, dressing changes, intravenous therapy, medication administration, and stoma care as ordered by the physician. They completed the same questionnaires at the same time points as the intervention group (baseline, 1 week, and 1 month). At discharge, they received the same educational pamphlets provided to the intervention group. However, they did not receive any intentional presence sessions, individualized holistic assessment, educational video clips, or telephone follow-up. This design allowed comparison between standard care plus educational materials and the same educational materials embedded within the intentional presence framework.
Data Collection
Data were collected at three points: baseline (preintervention), 1-week postintervention, and 1-month postintervention. Questionnaires were administered electronically to minimize assessment bias.
Instruments
Demographic information and a disease characteristics questionnaire were completed by the research participants.
Depression, Anxiety, and Stress were measured using the Depression, Anxiety and Stress Scale-21 (DASS-21). The DASS-21 is a widely used self-report instrument comprising three 7-item subscales designed to measure the emotional states of depression, anxiety, and stress over the past week. Participants rate the extent to which they experienced each state on a 4-point Likert scale ranging from 0 (“Did not apply to me at all”) to 3 (“Applied to me very much, or most of the time”).
Scores for each subscale are calculated by summing the scores for the relevant items and multiplying by 2 to maintain comparability with the full 42-item DASS, with higher scores indicating greater severity. The validity and reliability of the DASS-21 are well-established in both clinical and nonclinical populations across various cultures (Lovibond & Lovibond, 1995). In the present study, the Persian version of the scale was used. The Persian DASS-21 has demonstrated strong psychometric properties, with reported Cronbach's alpha coefficients of 0.85 for the Depression subscale, 0.82 for the Anxiety subscale, and 0.78 for the Stress subscale (Asghari et al., 2008). In this study, the Cronbach's alpha for the total scale was (0.86).
The Filipino Coping Strategies Scale (FCSS) (Rilveria, 2018) was administered before the intervention, 1 week later, and 1 month later. This scale consists of 37 questions with Likert-type responses ranging from 1 to 4, where 1 indicates the least coping, and 4 indicates the most coping. It includes nine coping strategies: cognitive reappraisal, social support, problem-solving, religiosity, tolerance, emotional release, overactivity, relaxation/recreation, and substance use. In this study, the forward-backward translation method was employed. The scale's reliability was measured using Cronbach's alpha coefficient (α = 0.7).
The Holistic Needs Assessment Checklist (Snowden & Fleming, 2015) was another tool used in the present study. It was employed in the intervention group to assess the patient's holistic needs, estimate the patient's situation, identify stressors, determine the appropriate dose of the nurse's intentional presence, and develop an individualized care plan. The Holistic Needs Assessment (HNA) comprises 48 items categorized into five domains: physical, practical, social, emotional, and spiritual. Each item is scored from zero (no problem) to 10 (maximum concern).
Data Analysis
Data were analyzed using SPSS Version 27. Descriptive statistics (frequencies, means, SD) described participant characteristics. Normality was assessed using Shapiro-Wilk tests. Between-group comparisons used independent t-tests (normal distribution), Mann-Whitney U tests (non-normal distribution), and chi-square/Fisher's exact tests (categorical variables). Within-group changes over time were analyzed using Friedman tests. Quantile regression models adjusted for baseline scores and relevant covariates, with 95% confidence intervals reported. Statistical significance was set at P < 0.05.
Results
Participant Flow
Of 138 patients assessed for eligibility, 62 met inclusion criteria and were randomized (31 per group). All 62 completed the 1-month follow-up (Figure 1).
Baseline Characteristics
The intervention and control groups were homogeneous regarding age (50.74 ± 10.68 vs. 54.42 ± 16.30 years, P = 0.14), gender (P = 0.61), education (P = 0.73), stoma presence (45.2% vs. 54.8%, P = 0.44), and other demographic/disease variables (P > 0.05) (Table 3).
Comparison of the Frequency/Mean Scores of Demographic and Disease Information of Patients in Intervention and Control Groups
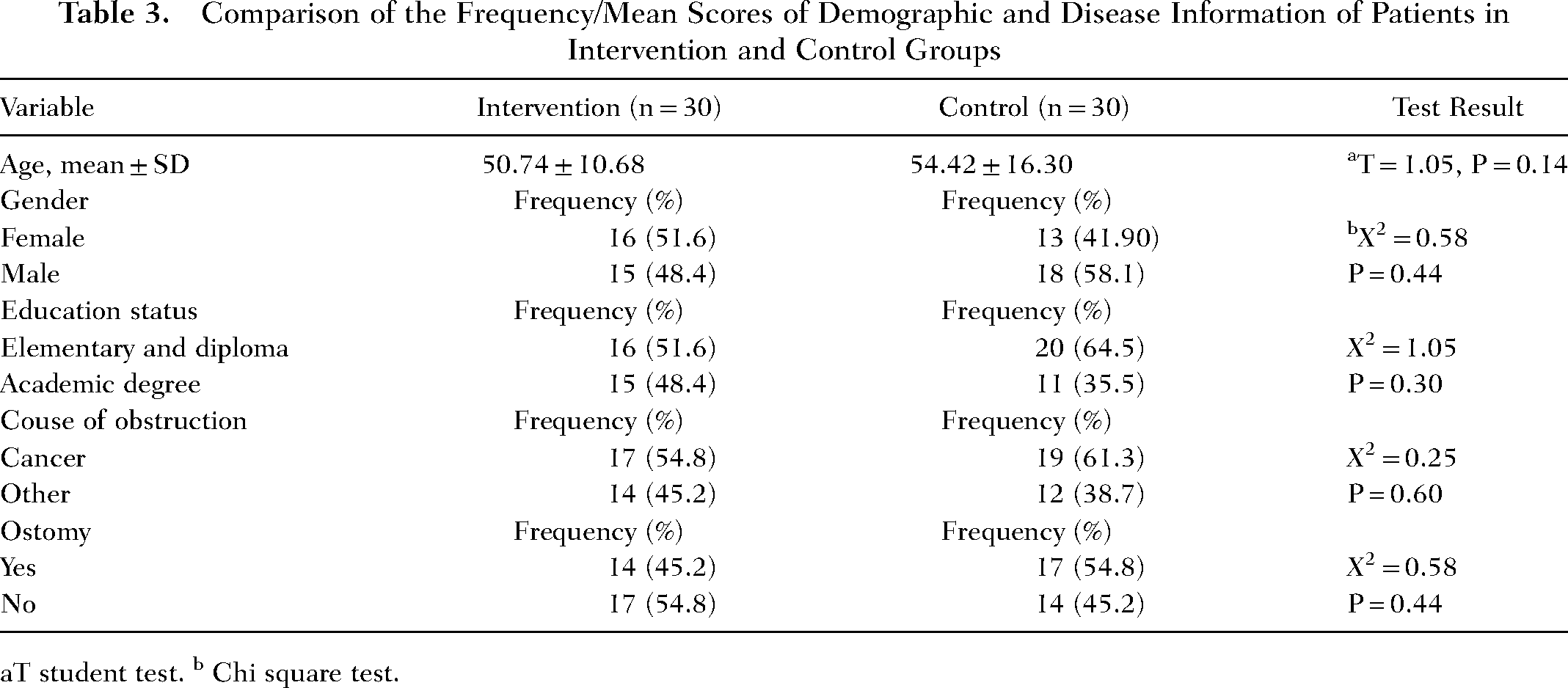
T student test. b Chi square test.
Coping Strategies
The Mann-Whitney test showed no significant difference in FCSS scores between groups at baseline (P = 0.40) or 1 week (P = 0.96). However, at 4 weeks, the intervention group had significantly higher FCSS scores (indicating better coping/adaptation) compared to the control group (P = 0.04). Friedman tests revealed that FCSS scores decreased over time in both groups (P < 0.001), indicating reduced use of maladaptive coping strategies (Table 4).
Comparison of the Mean and Standard Deviation of Patients’ Coping, Stress, Anxiety, and Depression in Intervention and Control Groups
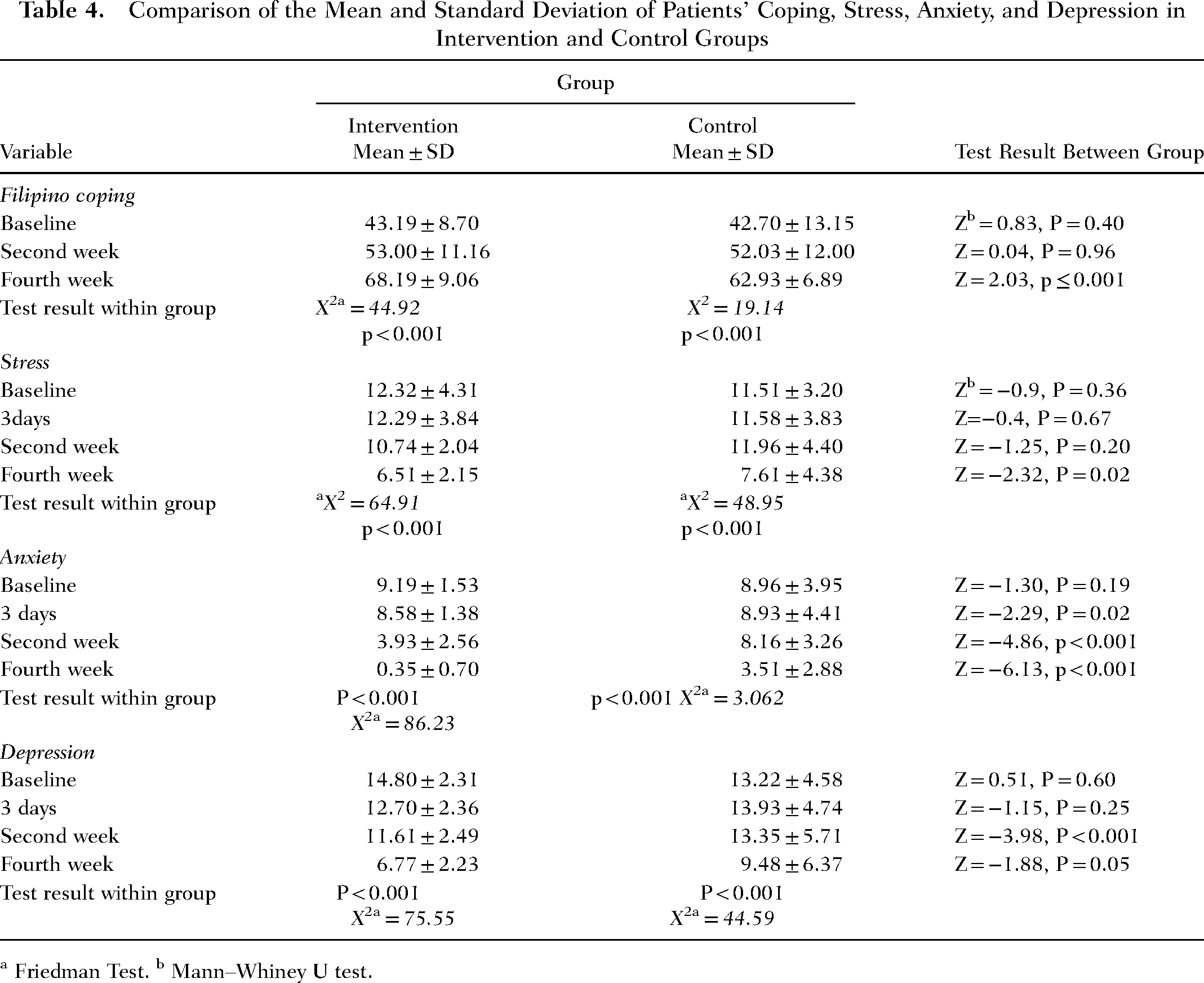
a Friedman Test. b Mann–Whiney U test.
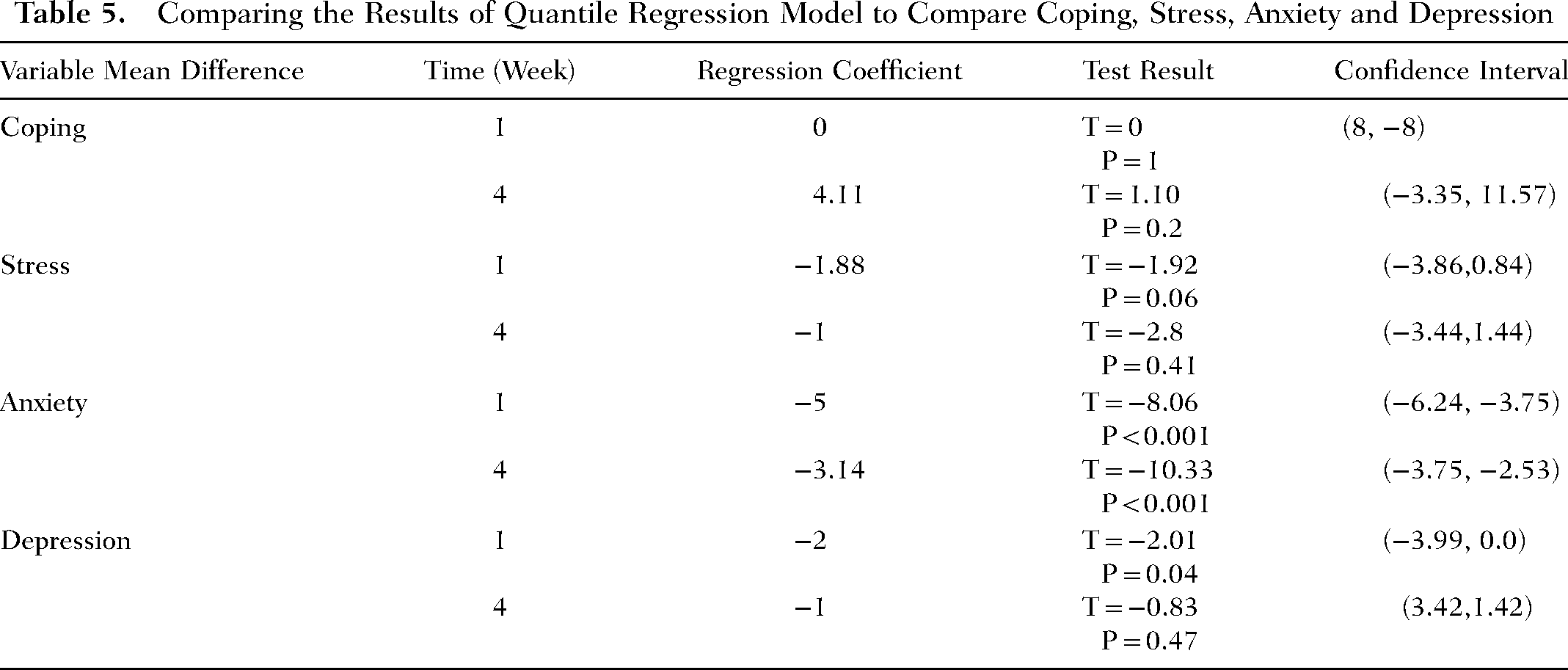
However, quantile regression adjusting for baseline scores showed that the intervention group had significantly greater improvement at 4 weeks (RC = 4.11, 95% CI [1.87, 6.35]), indicating better adaptive coping (Table 5).
Comparing the Results of Quantile Regression Model to Compare Coping, Stress, Anxiety and Depression
Stress
No significant between-group differences in stress scores at baseline (P = 0.67) or 1 week (P = 0.20). At 4 weeks, the intervention group had significantly lower stress (P = 0.02). Friedman tests showed decreased stress over time in both groups (P < 0.001) (Table 4).
Quantile regression confirmed significant intervention effects at 1 week (RC = −1.88, 95% CI [−3.28, −0.48]) and 4 weeks (RC = −1.00, 95% CI [−1.96, −0.04]) (Table 5).
Anxiety
No significant baseline difference (P = 0.60). Significant differences emerged at 3 days (P = 0.02), 1 week (P < 0.001), and 4 weeks (P < 0.001) (Table 4). Quantile regression confirmed significant effects at 1 week (RC = −5.00, 95% CI [−6.67, −3.33]) and 4 weeks (RC = −3.14, 95% CI [−4.89, −1.39]) (Table 5).
Depression
No significant baseline difference (P = 0.67). Significant differences emerged at 1 week (P < 0.001) and 4 weeks (P = 0.05) (Table 4). Quantile regression confirmed significant effects at 1 week (RC = −2.00, 95% CI [−3.17, −0.83]) and 4 weeks (RC = −1.00, 95% CI [−1.98, −0.02]) (Table 5).
Discussion
The results of this study, aimed at determining the impact of the intentional presence of a holistic nurse on the levels of stress, anxiety, depression, and coping strategies of patients undergoing intestinal obstruction surgery, showed that intentional presence emphasizing the establishment of a purposeful and heartfelt interpersonal connection between the nurse and the patient resulted in a significant reduction in anxiety, stress, and depression scores of patients 1 week and 4 weeks after the intervention. Given that the pivotal point of intentional presence with a holistic approach is gaining the patient's trust and focusing on the patient's unique needs, the results indicate an improvement in the overall adaptation score of patients 4 weeks after the intervention.
Based on the results of a thematic analysis (Tuominen et al., 2020), the expectations of patients with colorectal cancer were categorized into three areas: first, receiving sufficient information about the disease, its complications, and self-management; second, receiving support from the healthcare team with a humane, compassionate, and hopeful approach; and third, receiving professional care based on a systematic evaluation. In this study, an effort was made to consider the daily program in line with patients’ expectations mentioned in the thematic analysis study so that the common needs of these patients in the process of holistic care are considered both in-person and through telephone follow-ups. Considering that in the holistic approach, gaining the patient's trust is achieved through compassionate, hopeful, and humane care, the results of this study demonstrated the effectiveness of this program on patients’ levels of anxiety, stress, depression, and adaptation.
In line with the results of the present study, Gelogahi et al. (2018) also concluded that the intentional presence of a holistic nurse reduces anxiety and stress levels in patients undergoing open-heart surgery (Gelogahi et al., 2018). However, while Gelogahi et al. studied hospitalized heart surgery patients and focused their intervention on hospital-related stressors, the present study extended follow-up to 1-month postdischarge and addressed the unique, long-term self-care needs of bowel obstruction patients (including ostomy management and nutritional challenges). This may explain why we observed significant effects on depression, whereas Gelogahi et al. did not.
Considering that more than half of the patients in the present study were diagnosed with cancerous masses as the cause of their intestinal obstruction and the researcher attempted to provide emotional support to patients through phone follow-ups and help them meet their unique needs, the results of this study are comparable to those of White et al. (2012). They placed colorectal cancer patients in two intervention and control groups over a 9-month period and examined anxiety, depression, and supportive care needs every 3 months through phone follow-ups and emotional support in the intervention group. Their study results indicated reduced patient anxiety but no change in depression status. Although in the present study, anxiety, stress, and depression levels decreased over time, it also showed that as time progressed, the levels of reduced depression and anxiety compared to the first week were less. One possible reason for this reduction might be patients’ fear of the temporary nature of their recovery. However, based on the results from quantile regression, the coefficient of reduction in anxiety and depression levels with the use of a holistic nurse's presence and compassionate follow-up showed a higher number compared to White et al.'s study.
The significant improvement in coping strategies observed in the intervention group reflects enhanced adaptation to the psychological and practical challenges of bowel obstruction surgery, confirming that intentional presence facilitates not only symptom reduction but also positive behavioral adjustment.
Accordingly, the results of this study can also be compared with Aghakhani et al.'s study (Aghakhani et al., 2019). They used an adaptation model to improve anxiety and stress levels in colorectal cancer patients through phone follow-ups after hospital discharge. Patients in Aghakhani's study showed significant improvement in their stress and anxiety levels. However, compared to Aghakhani's study, this study shows that employing intentional presence with a holistic approach and focusing on patients’ unique needs with gaining their trust and using active listening techniques has a greater effect on reducing anxiety and stress levels in patients, where regression coefficients showed an improvement in anxiety (RC = −3.14) and stress (RC = −1) after 4 weeks, which is higher than the effectiveness of the adaptation model used by Aghakhani et al.
In this regard, the results of the present study can be compared with the results of Zhang et al. (Zhang et al., 2013). They also concluded in their study that a nurse's phone contact 2–3 times during this period increases adaptation to the ostomy in patients. Comparing the present study with Zhang et al.'s study reveals that employing a deliberate presence approach—where the patient is met in person at the hospital and followed up by phone at home based on their unique needs—has a more significant impact on patients’ adaptation levels postbowel obstruction surgery than phone contact alone after discharge (Zhang et al., 2013). The regression coefficient findings indicate that the level of patient adaptation 1 month after discharge is RC = 4.11, whereas Zhang et al.'s study estimated a 10% increase in adaptation with an ostomy. These figures suggest that the present study shows greater improvement in adaptation.
Theoretical Considerations in Evaluating Holistic Interventions
The choice of a randomized controlled trial design to evaluate a complex relational intervention such as intentional presence reflects the tension between methodological rigor and philosophical fidelity in holistic nursing research. While RCTs are designed to isolate specific variables, holistic interventions are inherently multi-dimensional, targeting the whole person through integrated therapeutic modalities. As such, the multi-component nature of our intervention is not a methodological weakness but a faithful operationalization of holistic nursing principles. The significant differences observed between groups, despite both receiving the same educational materials, suggest that the intentional presence framework—the quality of the therapeutic relationship and the integration of multiple caring modalities—produces clinically meaningful benefits beyond information provision alone. Future research should continue to develop and refine methodologies that respect the holistic nature of nursing interventions while maintaining scientific rigor, potentially including mixed-methods designs that capture both quantitative outcomes and the qualitative experience of the nurse–patient relationship
Limitations
This study has several limitations that should be considered when interpreting the findings:
Blinding limitations: Due to the nature of the psychosocial intervention, participants and the nurse intervenor could not be blinded, introducing potential performance and detection bias.
Selection bias: The inclusion criterion requiring smartphone ownership may have excluded lower socioeconomic individuals, limiting generalizability.
Sample size assumptions: The sample size calculation used effect size estimates from a different surgical population (cardiac surgery), which may not accurately reflect the true effect in bowel obstruction patients.
Short follow-up: One-month follow-up may not capture longer-term outcomes or sustained intervention effects.
COVID-19 impact: Conducted during the pandemic, resulting in shorter hospital stays and restricted bedside access. Some intervention elements were necessarily delivered via telephone postdischarge, potentially diminishing the nonverbal cues central to holistic, in-person communication.
Single intervenor: The intervention was delivered by a single trained researcher, which enhanced consistency and fidelity but limits generalizability to other nurses with different interpersonal styles and levels of training in holistic nursing. Future research should examine whether similar outcomes can be achieved when the intervention is delivered by multiple nurses in routine clinical practice.
Intervention complexity: While the multi-component nature of the intervention—integrating in-person sessions, telephone follow-up, educational videos, and pamphlets—reflects the comprehensive approach of holistic nursing care, this design does not permit identification of which specific elements contributed most to the observed outcomes. However, it is important to note that this question addresses a different research purpose. Within holistic nursing theory, intentional presence is conceptualized as an integrative framework wherein multiple therapeutic modalities work synergistically, not as a single component that can or should be isolated from other caring practices (Aghebati et al., 2015; McKivergin & Daubenmire, 1994). The control group design, in which both groups received the same educational pamphlets and routine care, allows attribution of between-group differences to the intentional presence framework as a whole. Future studies employing factorial or dismantling designs could further elucidate the relative contributions of specific elements within this framework, such as in-person versus telephone contact or relational support versus educational content.
Lack of qualitative data: The RCT design, while providing robust quantitative evidence, does not capture the rich, subjective experience of the nurse–patient relationship. The qualitative sufficiency of the “dose of presence” and patient satisfaction with the intervention were not measured.
HNA used only in intervention group: The Holistic Needs Assessment guided personalized care only in the intervention group, which was intentional as part of the intervention but may have introduced assessment-related differences between groups.
Despite these limitations, the study has notable strengths, including the randomized design with concealed allocation, high retention rate (100%), use of validated instruments, extended follow-up beyond hospitalization, and theoretically grounded intervention with detailed protocol documentation. Future research should employ multi-center designs with longer follow-up periods, include diverse patient populations without technology-based exclusion criteria, utilize mixed-methods approaches to capture the qualitative experience of the nurse–patient relationship, and conduct studies under nonpandemic conditions to evaluate the full in-person model of intentional presence.
Conclusion
The findings indicate that applying a holistic nursing theory with an intentional presence approach—aimed at establishing compassionate communication and building trust between the nurse and patient—significantly reduces anxiety, stress, and depression while enhancing coping and adaptation in patients undergoing bowel obstruction surgery. Within this framework of compassionate and humanitarian care, gaining the patient's trust and accepting them unconditionally as capable and knowledgeable partners in care amplifies the effectiveness of self-care education. The study demonstrates that when nurses identify and address patients’ unique needs across physical, emotional, social, and spiritual dimensions with kindness, openness, and authentic engagement, patients demonstrate improved self-care abilities and greater adaptation to illness-imposed limitations. Consequently, empowered patients experience lower levels of anxiety, stress, and depression during the vulnerable postoperative period. These findings affirm the central role of the nurse–patient relationship in promoting holistic healing and support the integration of intentional presence into routine surgical nursing practice.
Footnotes
Acknowledgments
This research is part of a master's thesis in critical nursing, conducted with the approval of the Ethics Committee of Mashhad University of Medical Sciences (Ethics Code: IR.MUMS.NURSE.REC.1399.033) and registered at the Iranian Clinical Trial Center (Code: IRCT20200811048368N1, registration date: 2020-10-11) in Qaem Hospital, Mashhad, Iran. The researchers express their gratitude to the esteemed officials of the Educational and Therapeutic Center of Qaem Hospital in Mashhad, and all the patients who participated in this research.
Authors’ Contributions
The first author participated to gathering the samples of the research and preparing the nursing care plans, videos and educational pamphlets. The corresponding author was the supervisor and critically reviewed all the steps of the research, and finally critically reviewed the final version of the article. The third author analyzed the data, and the last author helped the researchers to get access to the participants.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent for Publication
Not applicable in this section.
Ethics Approval and Consent to Participate
In accordance with the Declaration of Helsinki, the study protocol was approved by the Research Ethics Committee of Mashhad University of Medical Sciences, Mashhad, Iran, with Code: IR.MUMS.NURSE.REC.1399.033. Before the intervention, all the participants completed the informed consent form.
Funding
The article has been extracted from a Master's Thesis of Critical Care Nursing fulfilled at Nursing and Midwifery School of Mashhad University of Medical Sciences, Mashhad, Iran. The funder of this research was Mashhad University of Medical Sciences.