
Abstract
Background
and Aim: The primary goal of care for transgender and gender diverse (TGD) individuals is to address their somatic, psychological, and social needs holistically while promoting well-being in a manner that affirms and respects their gender identity. Health care provisions should be grounded with respect to the patient and characterized by mutual trust, respect for autonomy, maintenance of confidentiality, and delivery of the highest standard of care. The aim of this study was to examine the perceptions of individuals with gender dysphoria and TGD individuals among professionally active nursing staff, as well as undergraduate nursing and midwifery students.
Methods
This study was conducted via the diagnostic survey method. The research instrument was a questionnaire comprising a sociodemographic section and items assessing knowledge of and perceptions of transgender identity and gender diversity.
Results
The level of knowledge regarding transgender identity and gender diversity was most frequently assessed by respondents as satisfactory (31%). More than half of the participants (65.1%) reported knowing a transgender or gender-diverse individual, and 37% declared having provided care to such a patient. According to the majority of respondents (82.9%), TGD individuals constitute a group at risk of discrimination and stigmatization, and 56.2% indicated that the Polish health care system does not adequately recognize or respond to their health-related needs. Most respondents (75.8%) reported perceiving TGD patients in the same way as all other patients did, with perceptions being primarily dependent on individual personality traits (82.6%). At the same time, respondents indicated that TGD individuals constitute a group with particular needs related to mental health care (89%) and gender-related health care (60.9%).
Conclusions
Perceptions of transgender and gender-diverse individuals among the surveyed nursing personnel were heterogeneous and dependent on sociodemographic variables and levels of knowledge. According to the respondents, TGD individuals experience discrimination and are subjected to prejudice and inappropriate treatment both by medical personnel and within the broader social context.
Introduction
Transgender people, gender diverse people, people with gender dysphoria, and people with gender incongruence have diverse and often complex health needs, including those related to gender identity. However, fears of stigmatization or mistreatment by healthcare professionals may cause this group to avoid or delay contact with the healthcare system, which can lead to a widening of existing health disparities compared with the cisgender population.
Gender dysphoria (GD, included in the Diagnostic and Statistical Manual of Mental Disorders Fifth Edition (DSM V) classification) and gender incongruence (GI, included in the International Classification of Disease 11th Revision (ICD-11) classification) refer to discomfort and a clear inconsistency between gender experience and expression and the biological sex assigned at birth based on the assessment of external genitalia (Byne et al., 2018; Diagnostic and Statistical Manual of Mental Disorders Fifth Edition; International Classification of Diseases 11th Revision The global standard for diagnostic health information; Robles et al., 2022). The term “transgender and gender diverse” (TGD) refers to individuals whose gender identity or expression (feelings) differ from or are inconsistent with culturally defined norms for the sex assigned to them at birth (Coyne et al., 2023; Jha & Bouman, 2023).
The gender incongruence described in the ICD-11 classification is included in the area of sexual health rather than mental health, which means that gender incongruence is not a mental disorder (International Classification of Diseases 11th Revision The global standard for diagnostic health information; Robles et al., 2022). However, the mere inclusion of issues related to transgenderness and gender diversity in diagnostic classifications may lead to pathologization and, thus, to the belief that medical assistance should be provided to people in this population, even if it is not based on their actual needs (Crawford et al., 2023; de Vries & Kathard, 2020). On the other hand, diagnostic classifications may be necessary to assess gender-affirming treatment (Crocq, 2022; de Freitas et al., 2020; de Vries & Kathard, 2020).
There has been an increase in the prevalence of gender dysphoria/gender incongruence (Defant, 2025; Mason et al., 2023; Ouliaris, 2022), and it is obvious that those who experience it are the subject of care both in the context of gender dysphoria and other general health needs. The complex needs of this group of patients require healthcare professionals to pay special attention, show empathy, and understand their life situation (Robles et al., 2022; The Commissioner for Human Rights: The legal situation of non-heterosexual and transgender people in Poland). Providing care in a manner that is adequate to meet the needs and expectations of patients requires staff to have the necessary knowledge and cultural competence (Coleman et al., 2022; Milionis & Koukkou, 2023; Tavares & Figueiredo, 2025; The Commissioner for Human Rights: The legal situation of non-heterosexual and transgender people in Poland; Ziegler et al., 2020). It is important to build universal awareness of the perception of gender expression as a continuum between males and females rather than relying solely on binary norms. This can facilitate understanding of the gender-diverse population and its holistic needs (Bayraktar, 2025; Coleman et al., 2022; Galupo et al., 2021; Garg et al., 2023).
Holistic care should be based on partnerships with TGD individuals to address their medical, mental, and social health needs and well-being holistically, taking into account their gender identity. Gender-affirming care refers to the recognition and respect of a person's gender identity in social, psychological, medical, and legal terms (Jha & Bouman, 2023). It should be provided as lifelong support for TGD individuals, including those who are unsure of their identity, those who identify clearly, those before and after gender-affirming treatment, and those who choose not to undergo such treatment (Coleman et al., 2022).
Transgender and gender diverse individuals face many barriers to receiving safe and accessible healthcare (Crawford et al., 2023; de Vries & Kathard, 2020; Milionis, 2025; Velasco et al., 2022). People with gender dysphoria/gender incongruence often face transphobia, stigmatization, discrimination, and hostility from medical personnel when they encounter the healthcare system (Click et al., 2020; Coleman et al., 2022; Coyne et al., 2023; Crawford et al., 2023; de Vries & Kathard, 2020; Dora et al., 2021; Dwyer & Greenspan, 2021; Milionis, 2025; Tavares & Figueiredo, 2025; Velasco et al., 2022), which contributes to difficulties in accessing and receiving appropriate care, thereby exacerbating health inequalities (de Vries & Kathard, 2020; Möck et al., 2025; Nowaskie & Patel, 2020). Negative experiences with medical professionals may discourage patients from seeking further help or from taking preventive measures for fear of discrimination (Benson et al., 2022).
Nursing staff are required to provide high-quality holistic nursing care to all patients on the basis of current medical knowledge and ethical principles, taking into account the psychosocial contexts of patients’ functioning; this also applies to diversity in the area of gender and sexuality (Act on the professions of nurse and midwife of 15 July 2011; Code of professional ethics for nurses and midwives of the Republic of Poland; Rosa et al., 2019; The Commissioner for Human Rights: The legal situation of non-heterosexual and transgender people in Poland; Velasco et al., 2022). Within a holistic care framework, health is conceptualized as the outcome of an individual's integrated functioning across multiple dimensions of human existence, including the physical, psychological, emotional, social, and spiritual domains (Jasemi et al., 2017). Holistic care should focus on creating an inclusive, safe, and supportive care environment that enables the provision of gender-affirming care, taking into account the diverse and unique health and social needs of TGD individuals (García-Acosta et al., 2024; Sundus et al., 2026).
The authors expect that the obtained results will contribute to the development of holistic care practices for TGD patients, particularly through enhancing knowledge of their needs and fostering the creation of an inclusive care environment.
Objective
The aim of this study was to investigate the perceptions of persons with TGD among nursing personnel and nursing students.
Materials and Methods
The study was conducted via the author's original survey questionnaire, which included a section on sociodemographic data and questions about the perceptions of patients with gender dysphoria and gender diversity, as well as personal experiences related to caring for such patients. The research instrument was developed with the involvement of practicing professional nurses and midwives possessing expertise in the care of TGD individuals. Prior to the commencement of the study, pilot testing was conducted to clarify any potential ambiguities in the interpretation of the questionnaire items and to assess their validity. The link and QR code were made available to potential study participants in the form of announcements posted on closed online forums dedicated to nursing staff and students.
The study included professionally active nursing personnel and first-degree nursing students who agreed to participate in the study. Consent allowed respondents to proceed to the questions contained in the survey, whereas refusal to consent resulted in the survey form being closed. The exclusion criteria were refusal to participate in the study, not working as nursing personnel, and not studying nursing at the undergraduate level.
The study was conducted in southern Poland from September 19, 2024, to May 12, 2025, using an online survey questionnaire that allowed the results to be saved to an Excel spreadsheet.
Variables analyzed in the study. The dependent variable was the perception of TGD individuals. The independent variables included level of knowledge, level of preparation for providing care, personal acquaintance with a TGD individual, and professional contact with TGD individuals. Control variables: comprised age, length of professional experience or year of study, and place of employment.
Ethical Considerations
The respondents were informed about the purpose of the study, their anonymity, and the right to consent to participate in the study and to withdraw from it at any time. Consent confirmation allowed them to proceed to the survey questions. The respondents were also informed about the institutional affiliation of the study director and about the possibility of expressing any comments by e-mail (the e-mail address of the study director was provided). The study was approved by the Jagiellonian University Bioethics Committee, Cracow, Poland (Decision No.118.0043.1.242.2024, dated 02.08.2024).
The study was conducted as part of the statutory project of the Jagiellonian University, Cracow, Poland (N43/DBS/000332).
Data Management and Analysis
To answer the research questions and verify the hypotheses, statistical analyses were conducted via IBM SPSS Statistics version 29. The distributions were tested via the Kolmogorov‒Smirnov test. In addition, descriptive statistics were calculated. On the basis of the results, the ordinal nature of some of the other variables, and the numerical inequality of the groups included in the analysis, nonparametric tests were used. To investigate the relationship between age and the perception of people with TGD, a correlation analysis was conducted via Spearman's rho coefficient. To assess the relationship between the perception of people with TGD and their self-assessment of knowledge and preparation, along with its objective level, a correlation analysis was also conducted on the basis of Spearman's rho coefficient. Testing for differences in the perceptions of people with TGD depending on familiarity with a person with TGD and caring for them was based on the Mann‒Whitney U test. Statistical significance was accepted at the standard threshold of α = .05.
Characteristics of the Study Group
The study included a total of 281 participants, among whom 121 were working as nursing staff, whereas the remaining participants were nursing students who already had some clinical experience gained during their education. The majority of respondents identified as women (91.1%), followed by men (5.7%), nonbinary individuals (2.5%), and those identifying with another gender identity (0.7%). The respondents were aged between 18 and 61, with an overall average age of 27 (21 for students and 36 for working people). The majority of the respondents lived in urban areas (70.8%).
Results
Level of Knowledge and Education
The level of knowledge about issues related to transgenderness and gender diversity was most often assessed by respondents as satisfactory (31%), good (25.6), or not very high (25.3). A very good level of knowledge was indicated by 12.8%, a lack of knowledge was indicated by 2.1%, and 3.2% were unable to self-assess.
The vast majority of nurses (81.1%) stated that the issue of caring for transgender and gender-diverse patients had not been discussed during their education to date. Only 12.5% answered affirmatively, and 6.4% were unsure whether these topics had been covered. Most nurses recognized the need for education in caring for transgender and gender diverse individuals (definitely yes, 47.3%, rather yes, 33.1%).
Nursing staff provide care to all patients who need it; therefore, 34.2% of respondents admitted that they are not very well prepared to care for transgender and gender diverse patients, whereas another 21.7% described their level of preparation as satisfactory. Only 22.1% rated their preparation as good, and 10.7% rated their preparation as very good, whereas the rest (11.4%) were unable to assess it.
The vast majority of respondents (89.7%) were not familiar with the recommendations for the treatment of transgender and gender diverse individuals, which should be taken into account when providing care. Only 8.2% confirmed their knowledge of the Standards of Care for the Health of Transgender and Gender Diverse People Version 8 (SOC-8) recommendations, and 2.1% confirmed their knowledge of other guidelines in this area.
People With TGD in the Social Space
More than half of the respondents (65.1%) stated that they knew a diverse transgender or gender person (or persons), 24.9% indicated that they did not know any such person, and the rest were unsure of their answer (“I do not know”). The increase in the number of transgender and gender diverse people in Poland was confirmed by 85% of the respondents (an increase of 50.5%, definite increase of 34.5%), 12.1% had no opinion, and 2.9% denied an upward trend.
The visibility of transgender and gender diverse people in public spaces was also confirmed by the respondents: 44.8% were definitely yes, whereas 44.1% were rather yes. Only 3.2% denied an increase in the visibility of TGD people in public spaces, and 7.8% had no clear opinion. Similar results were obtained in response to the question of whether TGD people are more represented in public spaces—the majority of respondents agreed. The statement that transgender and gender diverse people are definitely more represented was agreed with by 42.3% and rather more represented by 42%; only 5.3% expressed the opposite opinion, and the rest (10.3%) answered “I do not know.”
Care for transgender and gender diverse patients was provided by a minority—10% provided it once, 15.3% several times, 11.7% were unsure, and the rest (63%) did not provide care to TGD patients.
Perception of TGD Patients
Although the majority of respondents expressed the opinion that the number of transgender and gender diverse people is growing and that they have become more visible and represented in Polish public space, the respondents noted that TGD people are exposed to discrimination, stigmatization, and prejudice. More than half (53%) strongly agreed with this statement, and 29.9% selected the answer “rather yes.”
The respondents were asked to indicate whether, in their opinion, transgender and gender diverse people have specific health needs (multiple answers were possible). The most frequently indicated needs were mental health (89%), sexual health (60.9%), and social health (58.7%). Less frequently indicated were somatic health needs (35.6%) and spiritual needs (70%), with only 14.6% of respondents indicating no special health needs. In the opinion of the respondents, the most common disorders (multiple answers were possible) that occurred more frequently in TGD individuals than in the general population were disorders of the endocrine system (66.5%), reproductive system (40.9%), and nervous system (33.8%). Disorders of the circulatory system (8.5%), digestive system (5.3%), and respiratory system (3.6%) were also indicated. Almost one in four respondents (24.6%) stated that disorders in the functioning of individual systems do not occur more frequently in TGD individuals than in the general population.
The respondents were also asked whether mental disorders/illnesses occurred more frequently in the TGD population than in the general population; multiple answers were possible. The most frequently indicated disorders were depressive disorders (77.9%), anxiety disorders (69.4%), personality disorders (61.6%), adjustment disorders (54.1%), and self-harming disorders (32.7%). Less frequently indicated mental disorders included addictions (32.7%), eating disorders (28.8%), autism spectrum disorders (15.3%), psychotic disorders (11.4%), and manic disorders (9.3%). Only 5% of the respondents indicated that mental health disorders are less common among the TGD group than among the general population.
In terms of social functioning, transgender and gender diverse individuals most often experience social stigmatization (86.5%), according to the nursing staff surveyed (Table 1).
The Most Important Problems Faced by Transgender and Gender-Diverse People in the Area of Social Functioning.
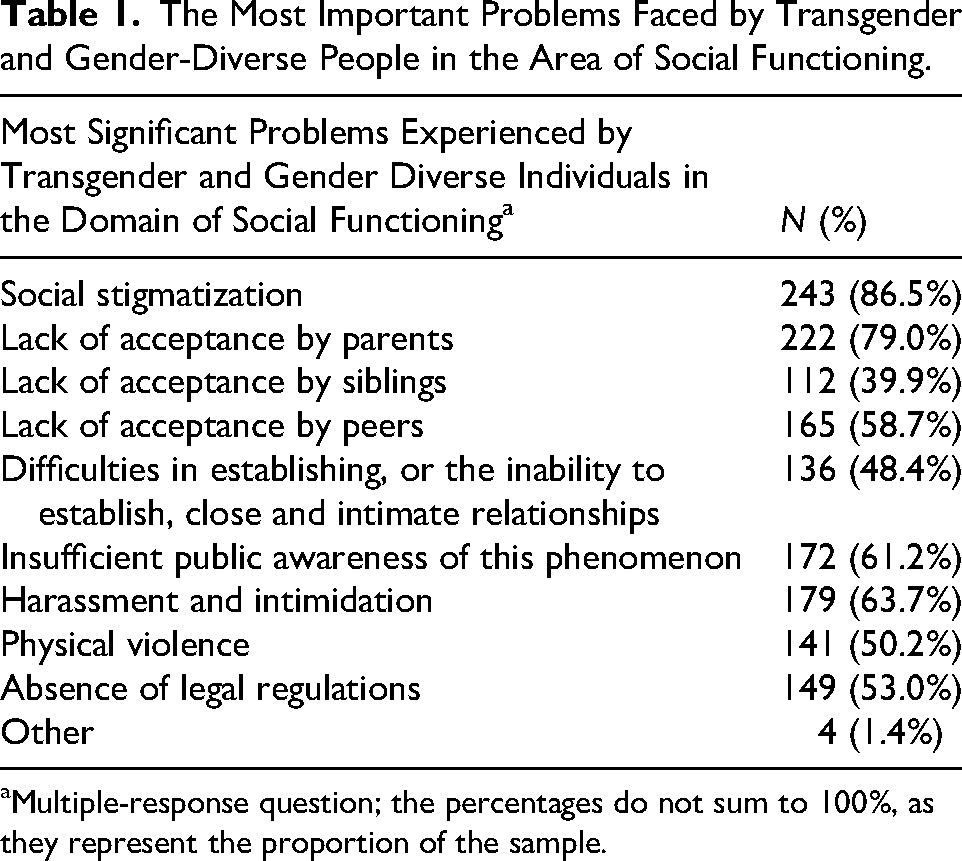
Multiple-response question; the percentages do not sum to 100%, as they represent the proportion of the sample.
Holistic Care for Patients With TGD
In addition to the substantive context of holistic medical care, the quality and sense of security of its recipients are equally important. According to the respondents, to ensure high-quality care and a sense of security, providing psychological care (77.6%), understanding individual health needs (75.4%), staff knowledge (65.8%), using pronouns and personal details consistent with the patient's gender identity (63%), providing sexological care (53.4%), providing psychiatric care (48.4%), understanding patients’ social situations (45.2%), the cultural competence of staff (41.3%), and gender affirmation (21%) are necessary.
Gender-affirming care, which was least frequently indicated as a factor influencing the quality of care and patient safety, was used mainly by the respondents to address patients in their preferred manner (86.5%) and show empathy (63.7%). The remaining results are presented in Table 2.
Gender-Affirming Care.
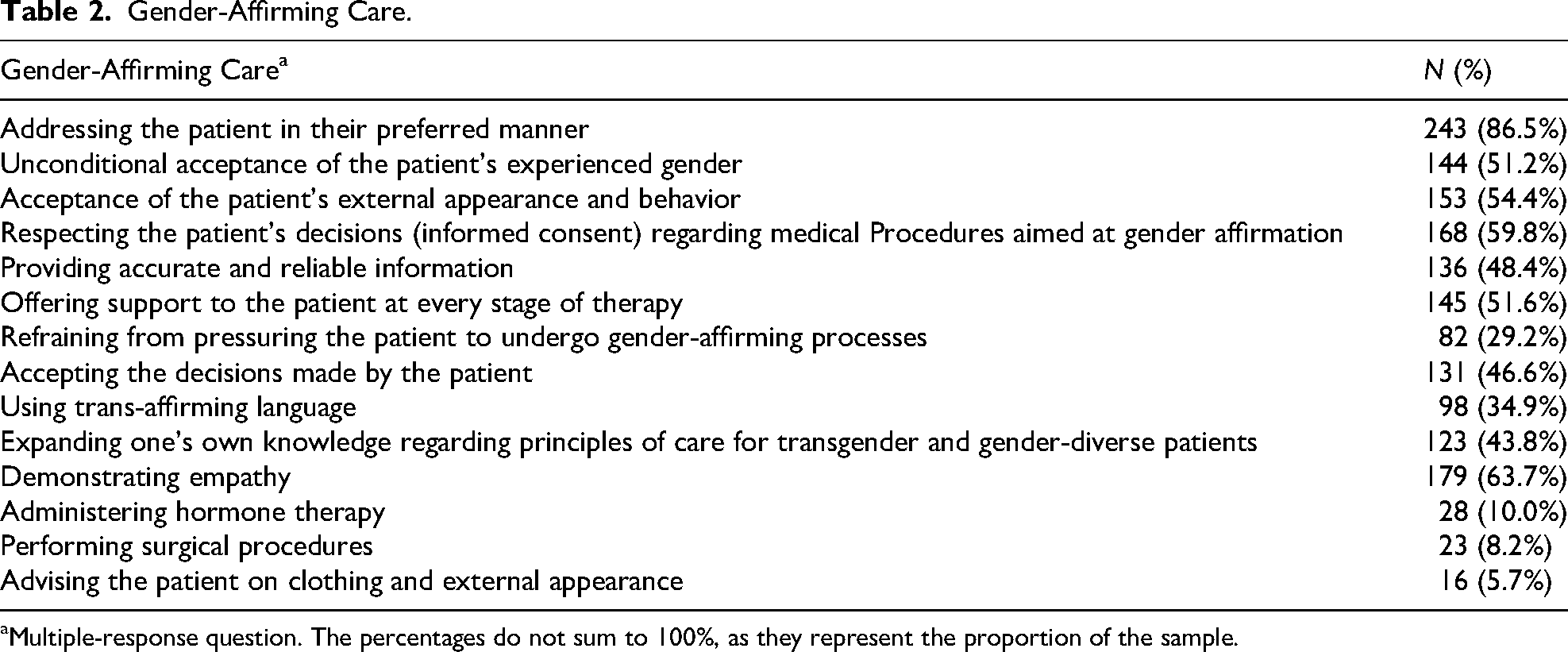
Multiple-response question. The percentages do not sum to 100%, as they represent the proportion of the sample.
In response to a question regarding how to address transgender and gender diverse patients, the majority of respondents (72.3%) believed that it should be done according to the patient's preferences (name, pronouns, etc.). Some of the respondents (16.7%) believed that it is possible to use personal details and pronouns in communication that are consistent with both the patient's identity and their documents, 10% maintained that only the names contained in the patient's documents should be used, and only two respondents (0.7%) indicated that it was appropriate to address patients in an impersonal manner.
In the respondents’ opinion on the use of personal details and pronouns of transgender and gender diverse patients in medical records, the prevailing approach was that this should be done in accordance with the patients’ wishes (49.1%). A slightly smaller percentage (38.4%) believed that they should be consistent with the patient's legal gender, whereas 3.9% believed that the use of personal pronouns interchangeably was acceptable, and 2.5% believed that it did not matter which personal details and pronouns were used. A larger group of respondents than in the case of direct conversation with the patient considered the use of impersonal forms to be appropriate—6%.
According to the nursing staff surveyed, when talking to and caring for transgender and gender diverse patients, they should behave as with other patients; 84.3% agreed with this statement. Significantly fewer responses concerned paying special attention to nonverbal expression (5.7%) and paying special attention to the relationships of TGD patients with other patients (3.9%), whereas other possibilities were indicated by individual respondents.
Transgender and gender diverse individuals are perceived by respondents primarily in terms of their individual personality traits—perception depends on a person's personality (82.6%). They are also perceived as individuals who expect special treatment (21%), are demanding (7.5%), pretentious (6.4%), have a good opinion of themselves (4.6%), and are dependent on others (2.5%). Multiple answers to this question were possible.
The perception of transgender and gender diverse individuals as patients (multiple answers were possible) does not differ from the perception of other patients in the opinion of the surveyed staff; 75.8% perceive TGD patients in the same way as any other patient does. Significantly less often, they were perceived as persons requiring special care in terms of psychological support (32.4%), psychiatric and psychological care (23.5%), as persons whose care poses an organizational difficulty (13.5%), as persons who have difficulty accessing medical care (11%), and as persons who require special care in terms of somatic care (5.7%).
Knowledge of patients’ gender identity did not evoke any emotions in one-third of the nursing staff surveyed (29.5%). The feelings indicated by the respondents in relation to the care of transgender and gender diverse patients were concerned mainly with remembering how to address the patient (correct name, pronouns) (44.1%), difficulty asking which pronouns should be used so as not to offend the patient (30.2%), feelings of curiosity (23.1%), unexplainable uncertainty and fear (19.2%), focusing mainly on performing instrumental/procedural activities (19.7%), feeling discomfort (15.3%), and avoiding individual contact with the patient (2.1%).
The respondents were asked questions about issues related to the organization of care for TGD patients in hospital settings. According to 34.5%, during hospitalization, patients decide for themselves which gender they want to share a room with. A similar percentage of respondents (28.5%) believed that TGD patients should always be placed in a single room. On the other hand, 19.2% believed that it should be a room with patients consistent with the perceived gender identity of the TGD person, and 17.8% maintained that the room should be adapted to the registered gender. The respondents were also asked about access to separate toilets, bathrooms, cloakrooms, and changing rooms in public places for transgender and gender diverse individuals. The provision of areas specifically designated for TGD patients was supported by 30.6%, whereas 43.8% did not see such a need (15.3% were in favor of coeducational facilities everywhere), and 18.1% had no opinion.
More than half of the surveyed staff (56.2%) believed that the Polish healthcare system does not take into account and does not adequately respond to the health needs of transgender and gender diverse people. Only 12.1% had a different opinion, and the rest (31.3%) had no opinion. Access to medical care appropriate for their needs was also identified as a difficulty for transgender and gender diverse patients;—more than half of the respondents (53.8%) believed this to be the case, whereas 19.2% indicated that there were no difficulties in accessing care.
A small majority of respondents (51.3%) believed that transgender and gender diverse individuals are vulnerable to discrimination and become victims of prejudice or mistreatment by medical personnel. While 29.2% had no opinion on this issue, only 19.5% believed that TGD individuals were not exposed to negative attitudes and actions on the part of medical personnel.
Relationships Between Sociodemographic and Professional Variables and the Perceptions of Transgender and Gender Diverse People
To answer the research question of how sociodemographic and occupational variables are related to the perception of people with TGD, correlation analyses with Spearman's rho coefficient and difference analyses using the Kruskal–Wallis test were conducted to compare people working in different places in terms of how they perceive people with TGD. In the first step, age, education, and work experience (only for working individuals, n = 121) were included in the analysis. Table 3 summarizes the results of the analysis.
Results of Spearman's Rho Correlation Analysis Between Sociodemographic and Professional Variables and the Perceptions of Transgender and Gender Diverse (TGD) Individuals.
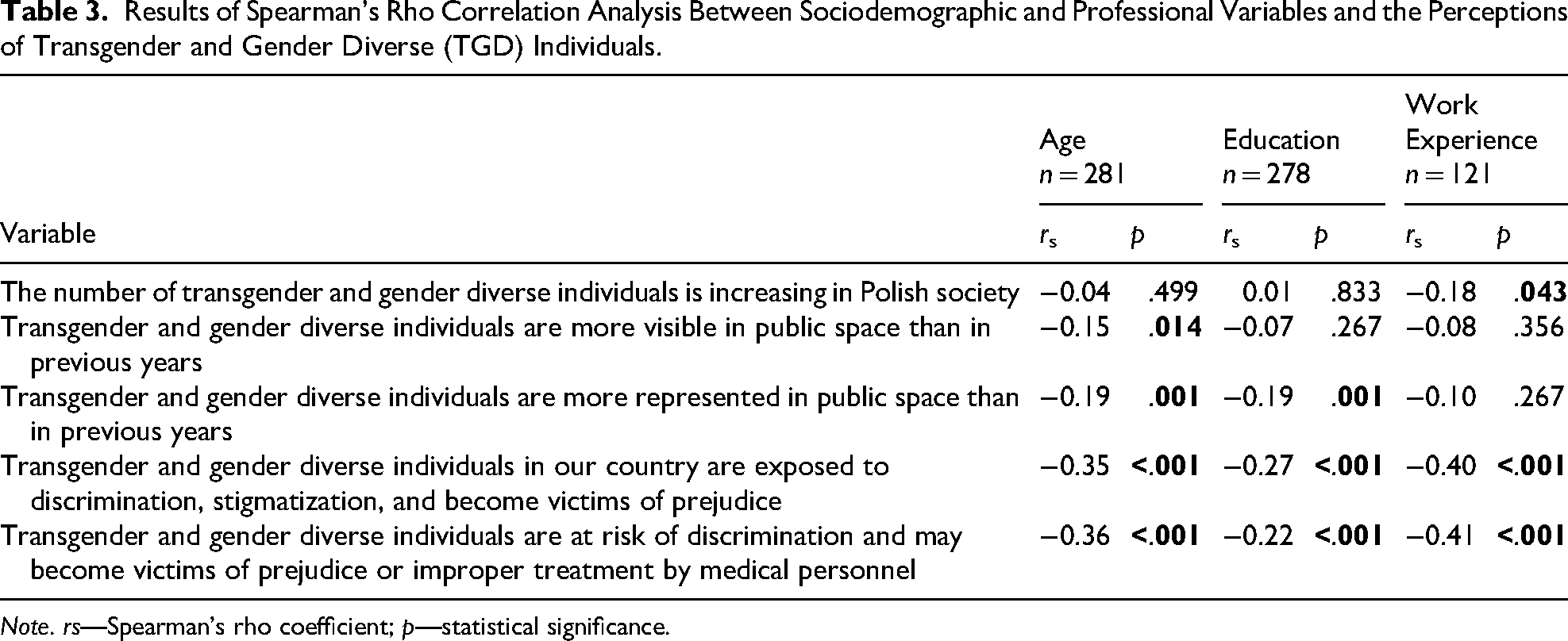
Note. rs—Spearman's rho coefficient; p—statistical significance.
The results of the analysis revealed that the participants’ age was related to their perception of people with TGD. No significant correlation was found between the assessment of the increase in the number of people with TGD, but the other correlations were statistically significant and negative. In the case of greater visibility and representation in public space than in previous years, these relationships are weak, whereas for exposure to discrimination, stigmatization, and being victims of prejudices—in general and on the part of medical personnel—these relationships are moderate. It follows that with age, agreement with the aforementioned attitudes decreases. At the same time, education is correlated with greater acceptance of the representation of people with TGD and exposure to discrimination in general, as well as from medical personnel (weak and negative correlations). With higher education, agreement with the presented aspects of the perception of people with TGD is weaker. A relationship was also found between work experience and the assessment of the increase in diversity of TGD individuals in Polish society (weak correlation) and exposure to discrimination in public and from medical personnel (moderate correlations). The longer the work experience of the respondents is, the less they agree with the increase in the representation of people with TGD in Polish society, and the less they agree with the statement that people with TGD are exposed to discrimination and stigmatization and become victims of prejudice or mistreatment by medical personnel.
Relationships Between Knowledge About TGD Individuals and Their Perceptions
The relationships between the subjective and objective knowledge of TGD individuals and their perceptions were investigated. For this purpose, correlation analyses were conducted via Spearman's rho coefficient. Table 4 summarizes the results of the analysis.
Results of Spearman's Rho Correlation Analysis Between Knowledge About TGD Individuals and Perceptions of TGD Individuals.
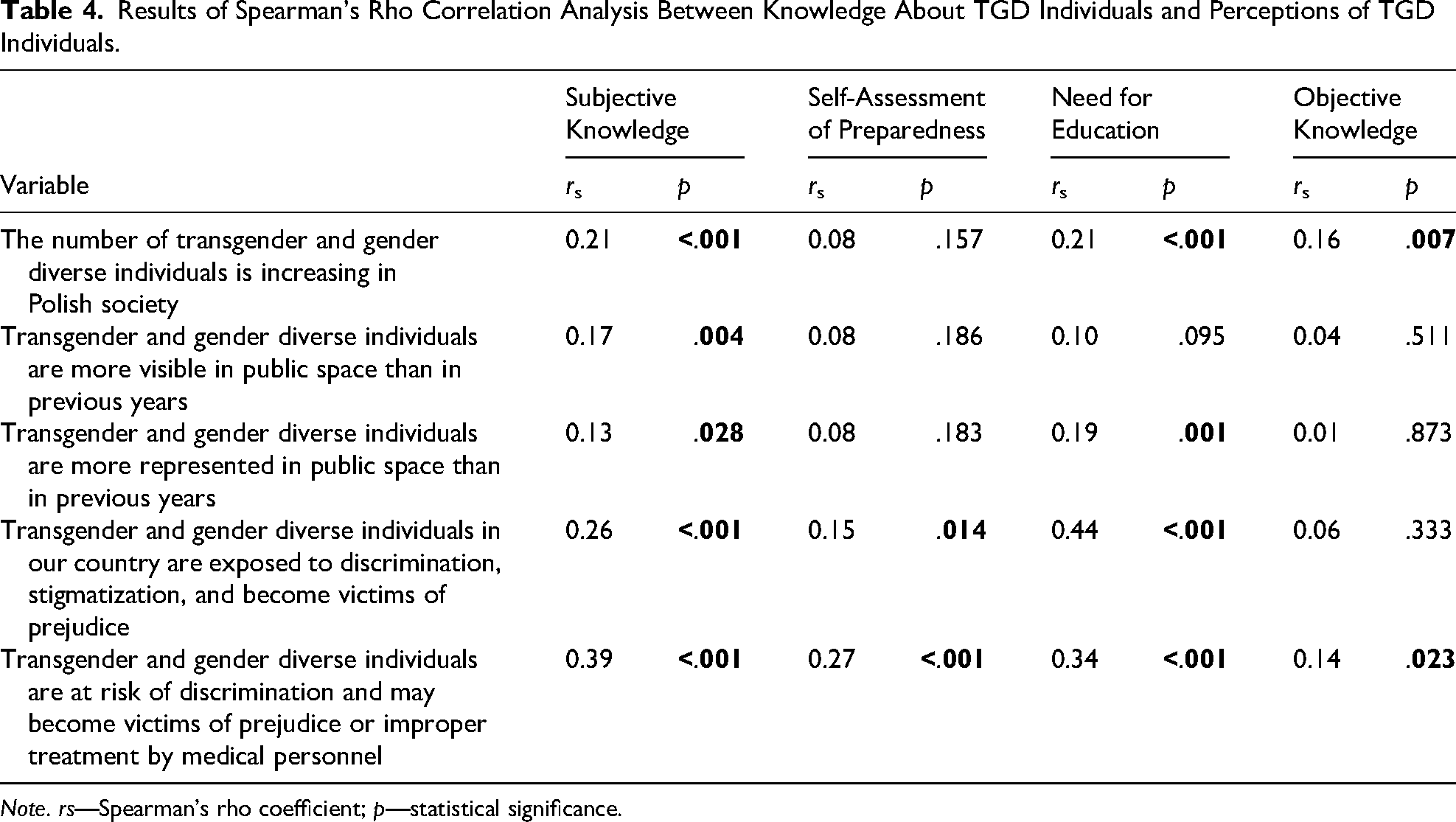
Note. rs—Spearman's rho coefficient; p—statistical significance.
There are statistically significant correlations between the subjective knowledge of the respondents and all areas of perception of people with TGD. The better the respondents rated their own knowledge about people with TGD, the more they agreed that the number of people with TGD is increasing, that they are more visible and represented, and that they are exposed to discrimination and stigmatization, including from medical personnel. The assessment of preparedness to address people with the TGD occurs only with the assessment of the exposure of people with the TGD to discrimination (in general and from medical personnel). With a better self-assessment of their own preparedness, the respondents were more aware of the danger of discrimination and stigmatization against people with TGD.
A relationship was also noted between the need for education and each of the attitudes toward people with TGD (apart from an increase in the perception of people with TGD in public spaces). The more strongly the respondents perceived the presence of people with TGD in Polish society and their increased representation, the more strongly they declared the need for further education on caring for these people. Furthermore, the more strongly the respondents perceived the danger of discrimination and stigmatization against people with TGD, the more strongly they expressed their need for further education on caring for people with TGD.
Moreover, objective knowledge was correlated only with the increase in the number of people with TGDs in Polish society and with the exposure of people with TGDs to discrimination, becoming victims of prejudice or mistreatment by medical personnel (weak and positive correlations). This shows that the greater the level of objective knowledge of the respondents regarding the care of people with TGD, the more strongly they perceived an increase in the number of people with TGD in Polish society and the better they perceived the exposure of people with TGD to mistreatment by medical personnel.
Differences in the Perception of TGD People Depending on Personal Acquaintance With a TGD Person
In further analyses, differences between people who know someone with TGD and those who do not know such people in terms of how they perceive people with TGD were investigated. People who chose the answer “I do not know” (n = 27) were excluded from the analysis because of their low number and lack of substantive value in comparisons. Differences in the size of the compared groups were noted: χ2(1) = 50.47; p < .001. Owing to the skewed distribution and problems with group size, a nonparametric test was conducted—the Mann‒Whitney U test (Table 5).
Results of the Mann–Whitney U Test for the Perception of TGD Individuals Depending on Acquaintance With a TGD Person.
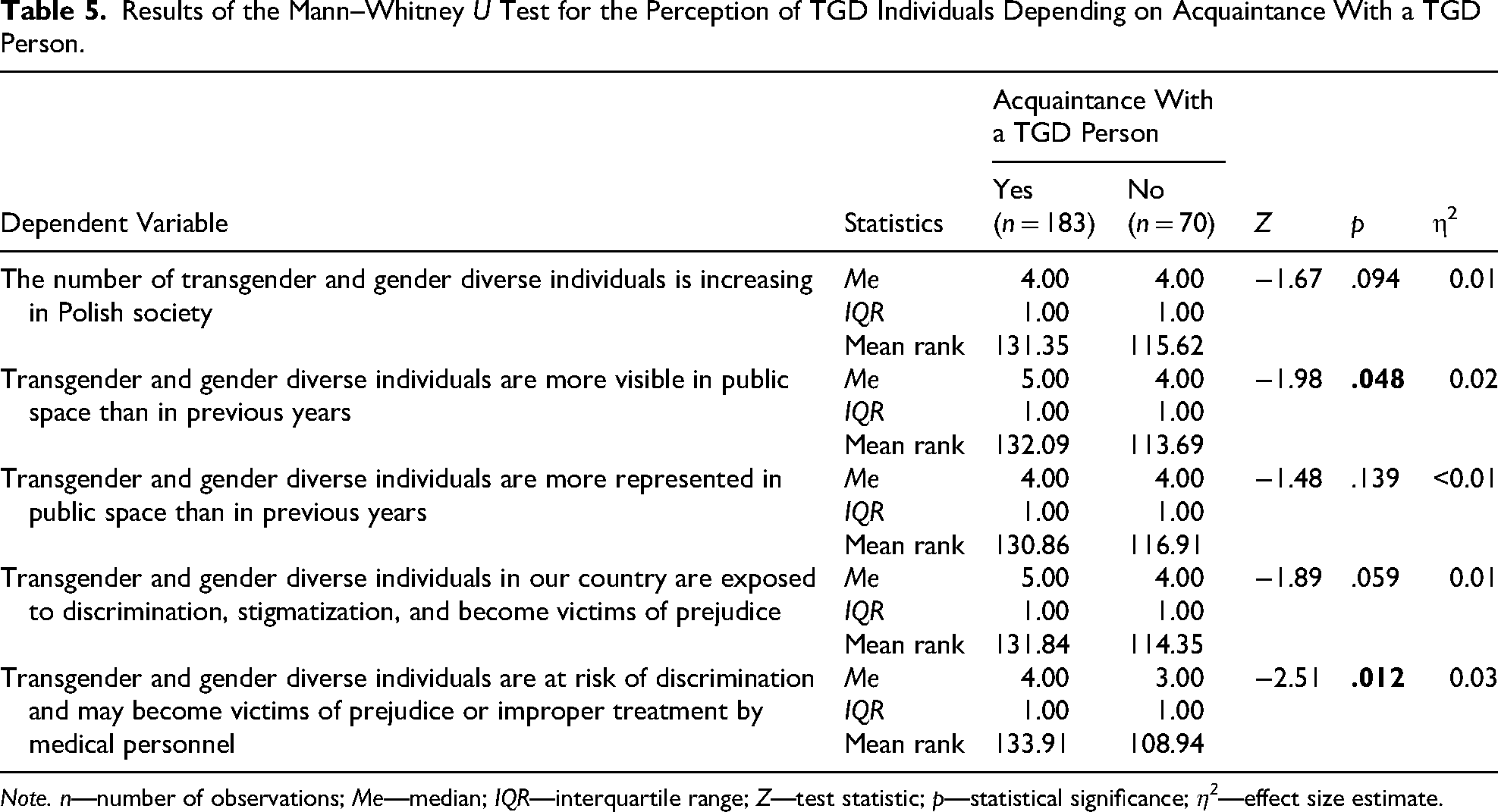
Note. n—number of observations; Me—median; IQR—interquartile range; Z—test statistic; p—statistical significance; η2—effect size estimate.
The analysis revealed that compared with previous years and exposure to discrimination and mistreatment by medical personnel, knowing someone with the TGD differentiates the visibility of people with the TGD in public spaces. In both comparisons, weak effects were observed (η2 < 0.06). The analysis of mean ranks and medians indicates that respondents who knew persons with TGD agreed more strongly with the increase in the visibility of persons with TGD in public spaces than did those in previous years and perceived the danger of discrimination and mistreatment by medical personnel more strongly than did respondents who did not know persons with TGD. For the remaining statements, no statistically significant differences were found between the compared groups.
Differences in the Perception of TGD People Depending on Previous Contact With a TGD Person
The final stage of the analysis sought to determine whether previous contact with people with the TGD differentiated the perceptions of people with the TGD. Contact with people with TGD was divided into two groups: individuals who had ever cared for people with TGD (answers: only once, more than once, and not sure) and individuals who had never cared for people with TGD. A numerical disproportion between the groups was noted: χ2(1) = 18.96; p < .001. The results of the Mann–Whitney U test for the perceptions of people with TGD are presented in Table 6.
Results of the Mann–Whitney U Test for the Perception of TGD Individuals Depending on Prior Professional Contact With TGD Individuals.
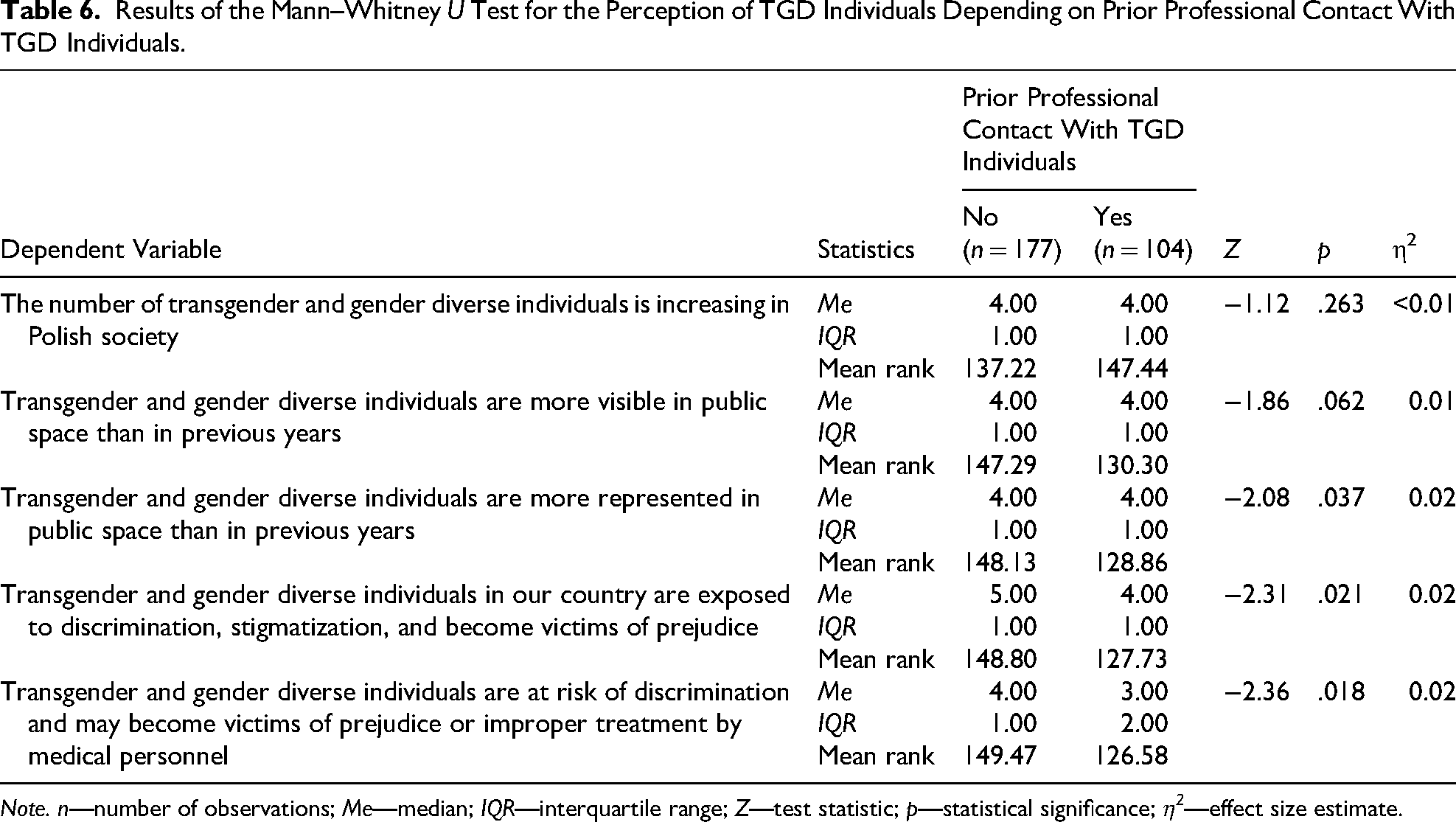
Note. n—number of observations; Me—median; IQR—interquartile range; Z—test statistic; p—statistical significance; η2—effect size estimate.
The calculations show that previous contact with individuals has been a differentiating factor in the perception of people with the TGD, concerning the greater than previous representation of people with the TGD in public spaces and exposure to discrimination, including from medical personnel. According to the chi-square test, each recorded effect is weak. At the same time, a comparison of the mean ranks shows that people who have not had contact with people with the TGD agree more strongly that people with the TGD are more represented in public spaces than in previous years are people who have not had contact with people with the TGD. In addition, people who do not care for people with TGD perceived a greater risk of discrimination and stigmatization of people with TGD and mistreatment.
Discussion
Holistic and individualized nursing care should be oriented toward addressing patients’ health, social, and emotional needs, as well as their individual characteristics, rather than being exclusively focused on their gender identity (García-Acosta et al., 2024; Sundus et al., 2026). Furthermore, care should be grounded in a partnership-based approach within therapeutic relationships and in the attainment of health-related needs (Jasemi et al., 2017).
In recent years, the population of transgender and gender-diverse people has increased (Coleman et al., 2022; Defant, 2025; Mason et al., 2023; Milionis, 2025; Ouliaris, 2022). Our own research confirms this trend; respondents observe an increase in the number of TGD individuals in Polish society and similarly assess their visibility and representation in public spaces.
Despite healthcare being based on equality and nondiscrimination, transgender and gender diverse people are more likely than the general population to experience marginalization and discrimination in access to healthcare and mistreatment by medical personnel (Leal et al., 2024; Medina-Martínez et al., 2021; Milionis, 2025; Tavares & Figueiredo, 2025). Among the general LGBTQIA+ population living in Poland, transgender people are the most vulnerable to prejudice and discrimination (Polish Sexological Society). This is confirmed by the opinions of the surveyed respondents, most of whom believe that TGD people are vulnerable to discrimination, stigmatization, and numerous prejudices. Transgender and gender diverse people use medical care both for general health needs and for specific issues related to their gender identity. However, more than half of the respondents (63.0%) admitted that they had never provided nursing care to TGD patients. Despite their lack of experience in providing such care, the participants indicate that the TGD population has specific health needs, especially in areas related to mental health and sexual health.
One of the tools helpful in providing care to TGD patients is the SOC-8, which includes clinical recommendations based on reliable scientific evidence that promotes medical personnel practices enabling safe and effective interventions to help patients achieve lasting personal comfort with their gender identity and optimize their physical and mental health (Coleman et al., 2022).
The vast majority (89.7%) of the respondents were unfamiliar with recommendations (SOC-8 or others) regarding the care of transgender and gender diverse individuals. Our own research results indicate a lack of knowledge and preparation among staff to provide holistic care to TGD patients, taking into account their specific needs and expectations. This lack of knowledge and preparation has also been confirmed by studies of nursing staff conducted in other countries (Carabez et al., 2016; Kimmel et al., 2024; Padilha et al., 2022). There are also generational differences in attitudes toward TGD individuals, with older people often showing less sensitivity and knowledge than younger people do (Basile et al., 2025; Carlström et al., 2021). The results of our own research also revealed certain generational differences: the younger the respondents were, the less acceptance of negative behaviors toward TGD individuals. This may be due to general changes (including social, political, and cultural changes) and greater openness to diversity and respect for the rights of others among younger members of society (including in the area of gender identity).
The lack of knowledge and preparation of medical personnel is also evident in the opinions of TGD patients (Basile et al., 2025; Dasso et al., 2025; Leal et al., 2024; Mikovits, 2022; Skrzypczak et al., 2022). The lack of knowledge of guidelines for the holistic care of TGD patients has also been confirmed in the results of studies conducted by other authors (Dasso et al., 2025; Leal et al., 2024; Tavares & Figueiredo, 2025).
Notably, these issues were not addressed in the standard of professional education for nurses and midwives in force in Poland until September 2025 (Regulation of the Minister of Science and Higher Education of 26 July 2019 on the standards of education preparing for the profession of a physician, dentist, pharmacist, nurse, midwife, laboratory diagnostician, physiotherapist and paramedic; Regulation of the Minister of Science of 10 October 2024 amending the regulation on the standards of education preparing for the profession of a physician, dentist, pharmacist, nurse, midwife, laboratory diagnostician, physiotherapist and paramedic). To provide the highest possible quality of holistic healthcare to all individuals, with full respect for their sexual orientation and gender identity, it is necessary to implement educational programs for healthcare professionals and to monitor and evaluate the quality of healthcare services provided (García-Acosta et al., 2024; Martinez-Sabater et al., 2025; Padilha et al., 2022; The Commissioner for Human Rights: The legal situation of non-heterosexual and transgender people in Poland; Ussher et al., 2022; Velasco et al., 2022). The respondents in this study declare the need for education in the care of TGD patients, which should be provided at the level of basic professional education (a bachelor's degree). The inclusion of content related to the care of TGD patients in the curriculum significantly contributes to improving nursing care for this population (Álvarez-Muñoz & Barrios-Casas, 2024) and should be mandatory for healthcare professionals (Ussher et al., 2022). Participation in LGBTQIA+ health education programs is positively correlated with knowledge and confidence in meeting the health needs of TGD patients (Huang et al., 2025; Medina-Martínez et al., 2021). Independent efforts by nursing staff to deepen their knowledge of the needs and principles of caring for TGD patients also contribute to a better understanding of the needs of this patient group (Blus-Kadosh & Hartal, 2025; García-Acosta et al., 2024; Santiago et al., 2024).
An effective approach to overcoming inequalities in healthcare access and quality of care for TGD individuals is to provide gender-affirming care. This refers to culturally safe and engaged care based on respect for the identity and uniqueness of TGD individuals (Crawford et al., 2023; Milionis & Koukkou, 2023). It also means creating an inclusive care environment (Martinez-Sabater et al., 2025; Milionis, 2025; Rosa et al., 2019; The Commissioner for Human Rights: The legal situation of non-heterosexual and transgender people in Poland; Velasco et al., 2022) that focuses on depathologizing TGD individuals (Crawford et al., 2023). It should be grounded in the recognition and respect for patient autonomy, the empowerment of shared decision-making, and the application of person-centered communication (Sundus et al., 2026). Gender-affirming care further entails the delivery of professional roles and responsibilities in a manner that is free from bias and prejudice toward patients (Rivera et al., 2022). Nurses must be prepared to provide evidence-based and gender-affirming care. Providing empathetic and culturally sensitive nursing care is a key element in ensuring positive patient experiences (Kimmel et al., 2024). Unfortunately, in our own research, gender-affirming care was the least frequently indicated element influencing the quality and safety of care provided to TGD patients. Gender-affirming care was most often identified by addressing patients in their preferred manner, showing empathy, and respecting patients’ decisions regarding medical procedures aimed at gender confirmation.
Nursing and other medical personnel should, as part of their practice, use the name and pronouns preferred by patients, use gender-neutral language (e.g., patient) (Crawford et al., 2023; Dasso et al., 2025; Jha & Bouman, 2023; McLaughlin et al., 2025; Skrzypczak et al., 2022), or the language used by patients to describe their own identity (Polish Sexological Society). The results of our own research indicate that the vast majority of the surveyed staff correctly follow the communication recommendations they believe that patients should be addressed using names and pronouns in accordance with their expectations. However, with respect to the use of personal details and pronouns in medical records, less than half of the respondents believed that this should be done in accordance with the patient's wishes; this may be due to the applicable legal standards and the functionality of IT systems, which make it impossible to indicate the preferred name (they are based only on personal details consistent with the ID card).
According to the respondents, the perception of TGD patients depends primarily on their individual personality traits, and nurses’ perceptions of this group of patients do not differ from their perceptions of other patients. The feelings associated with caring for TGD patients were most often concern about remembering how to address patients and what pronouns to use when referring to them. Issues related to the organization of care for TGD patients can be a source of negative feelings in the form of discomfort resulting from the frustration or confusion experienced by nurses in relation to which pronouns and which bathrooms and patient rooms should be assigned to transgender patients (Carabez et al., 2016; Sundus et al., 2026).
Nursing staff play a significant role in the holistic care of transgender and gender diverse patients. The concept of patient-centered care allows individuals’ needs to be met, taking into account their individuality, and gender identity issues should also be considered in its implementation, as this has a positive impact on their overall well-being.
Nurses provide culturally appropriate, competent, and safe care on the basis of the assessment of needs and problems and the joint determination of care goals with the patient, based on scientific evidence and with respect to ethical values and patient rights (Crawford et al., 2023; Zimmerman et al., 2020). Within the framework of inclusive practices, nursing personnel should also engage in advocacy on behalf of TGD individuals as a form of support (Sundus et al., 2026).
Nursing professionals are often the first point of contact for individuals within the healthcare system; consequently, the quality of subsequent patient engagement, as well as patients’ overall perception of the care provided, is largely influenced by nurses’ competencies, knowledge, attitudes, and skills (García-Acosta et al., 2024; Santiago et al., 2024). In performing their professional role, nursing staff should strive to implement and promote inclusive practices on the basis of critical reflection on the perception of medical care in hetero and cisnormative terms.
Limitations of This Study
The study is subject to several limitations. First, the relatively small sample size (n = 281) limits the generalizability of the findings; therefore, the results should be considered preliminary. Future research should be conducted on larger samples and extended to include other professional groups. Another limitation is the inability to directly compare the present findings with those of other authors. To the best of our knowledge, this is the first study of its kind conducted in Poland among nursing personnel. Owing to sociocultural differences, comparisons with studies conducted in other countries may not always be appropriate. Participant recruitment was carried out by distributing survey links within closed online groups for practicing nurses and nursing students. No mechanism was implemented to prevent multiple survey submissions, as this would have required the collection of sensitive data (e.g., email addresses, professional license numbers, or student identification numbers).
Errors That May Affect Results
Missing data constitute a potential limitation, as the research instrument used may not have fully captured all aspects of the perception of TGD individuals considered relevant by respondents. To minimize this risk, a pilot study of the instrument was conducted prior to the main data collection. Additionally, in many items, respondents were provided with an “other” option allowing them to add open-ended comments. The participants were also given the opportunity to contact the principal investigator via email to submit any remarks; however, none of the respondents made use of this option.
Sampling bias represents another limitation, as participant selection may not be representative of the entire population of nurses and nursing students. Therefore, the findings should be interpreted as preliminary, and further research on larger and more diverse samples is warranted.
Recall bias may also have influenced the results, as respondents may not have accurately remembered their previous contacts with TGD individuals or patients and may have unconsciously distorted their recollections.
Key Findings and Implications for Future Research
Nursing personnel recognize the presence of TGD individuals in society and their utilization of health care services. However, respondents’ reported levels of knowledge and preparedness for providing holistic care to TGD patients are low, and perceptions of this group are heterogeneous. Continuous monitoring of changes in nurses’ perceptions of TGD individuals, as well as the provision of care aligned with patients’ needs and expectations, is essential.
Application in Holistic Nursing Practice
Implications for holistic nursing practice and nursing education. Given the increasing number of TGD individuals in society, the number of TGD patients receiving nursing care is also expected to rise. This trend requires nurses to possess adequate knowledge and skills, as well as to demonstrate attitudes grounded in understanding and sensitivity toward TGD individuals. It is essential to develop and implement content related to the holistic care of transgender and gender-diverse patients within both undergraduate and postgraduate nursing education curricula. Additionally, the development of evidence-based recommendations and guidelines for nursing care tailored to this patient population is warranted. The foundation of high-quality care is the individualized and holistic treatment of patients. Educational interventions are recommended, with an emphasis on a comprehensive understanding of patients’ needs, including aspects of sexuality and gender identity. However, the perception of TGD patients must not be reduced solely to issues related to their gender identity.
Conclusions
The perceptions of transgender and gender diverse people among respondents vary and depend on sociodemographic variables and knowledge. This determines the manner and extent to which they perceive the holistic needs of TGD individuals. In the opinion of the respondents, people with the TGD experienced discrimination and became victims of prejudice and mistreatment both by medical personnel and in social spaces. There is a need to educate medical students and practicing healthcare professionals in effective communication with TGD patients and to implement local guidelines that take into account their social needs, in order to prepare them to provide holistic, gender-affirming care. Developed guidelines and educational as well as clinical care recommendations should take into account the social and cultural context.
It is essential to strengthen both undergraduate and postgraduate education in the provision of care for TGD patients. Emphasizing the development of an inclusive care environment and the application of holistic care principles is expected to enhance the quality of care and increase patient satisfaction.
Supplemental Material
sj-spv-1-jhn-10.1177_08980101261456429 - Supplemental material for Perceptions of Transgender and Gender Diverse Patients by Nursing Personnel
Supplemental material, sj-spv-1-jhn-10.1177_08980101261456429 for Perceptions of Transgender and Gender Diverse Patients by Nursing Personnel by Patrycja Zurzycka, Patrycja Ostrogórska-Gonszewska, Grażyna Puto, Iwona Repka, Katarzyna Czyżowicz and Katarzyna Wojtas in Journal of Holistic Nursing
Supplemental Material
sj-docx-2-jhn-10.1177_08980101261456429 - Supplemental material for Perceptions of Transgender and Gender Diverse Patients by Nursing Personnel
Supplemental material, sj-docx-2-jhn-10.1177_08980101261456429 for Perceptions of Transgender and Gender Diverse Patients by Nursing Personnel by Patrycja Zurzycka, Patrycja Ostrogórska-Gonszewska, Grażyna Puto, Iwona Repka, Katarzyna Czyżowicz and Katarzyna Wojtas in Journal of Holistic Nursing
Footnotes
Acknowledgments
Not applicable.
Ethical Approval and Informed Consent Statements
The study was approved by the Jagiellonian University Bioethics Committee, Cracow, Poland (Decision No. 118.0043.1.242.2024, dated August 2, 2024. All study procedures adhered to the guidelines outlined in the Declaration of Helsinki. The respondents were informed about the purpose of the study, their anonymity, and the right to consent to participate in the study and to withdraw from it at any time. Consent confirmation allowed them to proceed to the survey questions.
Consent for Publication
Not applicable.
Authors Contributions
Research design: PZ, POG, KW, analysis and writing article: PZ, POG, KW, critical evaluation: PZ, POG, KW, KC, statistical analysis: PZ, KW, IR, GP, literature research: PZ, POG, KW, IR, GP.
Funding
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The study was financed as part of the statutory project of the Jagiellonian University, Cracow, Poland (N43/DBS/000332).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data supporting the results of this study are available in the attached file.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.