
Abstract
Keywords
Multiple sclerosis (MS) is a chronic neuroinflammatory disease marked by relapses, remissions, and progressive disability that may profoundly interrupt daily life. In the United States, approximately one million adults were living with MS in 2019, with an estimated economic burden of $85.4 billion (Bebo et al., 2022). Often diagnosed in early adulthood, MS interrupts career development, family roles, and anticipated futures, magnifying its impact on identity and life direction (Ando et al., 2022). Although disease-modifying therapies have reduced relapse rates and slowed progression, they do not address the lived experiences that shape how individuals understand themselves and their lives with illness (Boeschoten et al., 2017).
A growing body of literature describes MS as a disruption to identity, autonomy, and future orientation (Andersen et al., 2021; Ando et al., 2022). Building on this work, existential disruption is defined as a disturbance in the continuity of self that confronts meaning, identity, and one's anticipated life trajectory. This disruption goes beyond physical changes, showing a shift in how individuals understand themselves and their place in the world over time (Emery et al., 2022).
Although related to constructs such as biographical disruption and identity reconstruction, existential disruption denotes a broader and continuing challenge to self-continuity. Biographical disruption emphasizes the interruption of expected life trajectories (Bury, 1982), while identity reconstruction focuses on processes of adaptation and integration. In contrast, existential disruption captures the persistent tension between past, present, and anticipated selves, shaped by uncertainty, loss of coherence, and difficulty sustaining a stable sense of identity across time (Nissen et al., 2022).
While depression and anxiety are common in MS and may negatively affect quality of life (Boeschoten et al., 2017; Hanna & Strober, 2020), they do not fully capture the deeper existential experiences patients describe. Emerging evidence suggests that existential disruption represents a distinct domain that may operate alongside, but not be reducible to, mood symptoms (Pellens et al., 2026; Wilski et al., 2024). Meaning-making and identity reconstruction are therefore understood not as equivalent constructs, but as processes through which individuals respond to and navigate existential disruption. This distinction helps explain why biomedical and symptom-focused psychological interventions may fail to address concerns rooted in disrupted identity and meaning (Andersen et al., 2021).
Holistic nursing emphasizes the integration and relationships between human experience, viewing individuals as whole beings whose health extends beyond physical symptoms (Frisch & Rabinowitsch, 2019). Within this theoretical perspective, existential disruption reflects a disturbance in personhood that encompasses identity, meaning, and lived experience as interrelated dimensions of health. From this lens, disruptions in self-continuity are not secondary concerns but central to the illness experience, unfolding across the disease trajectory and shaping how individuals engage with care and envision their future.
Unaddressed existential disruption carries significant consequences, including diminished quality of life, strained relationships, decreased engagement in care, and persistent isolation (Gülirmak Güler et al., 2024; Montesano et al., 2025). These experiences are rarely assessed or formally recognized in clinical encounters, leaving people to navigate distress without structured support (Nissen et al., 2022; Wilski et al., 2024). This integrative review synthesizes current evidence to clarify how existential disruption in MS is conceptualized and experienced, with particular attention to self-continuity implications regarding understanding and informing nursing care.
Method
This review followed the integrative methodology described by Whittemore and Knafl (2005), which supports synthesis across several designs to develop a comprehensive understanding of complex health phenomena. Their five-stage approach (problem identification, systematic search, data evaluation, analysis, and presentation) guided the process.
A systematic search of CINAHL, PubMed, MEDLINE, and PsycINFO identified studies published between January 2015 and June 2025. Search terms included “multiple sclerosis,” “existential,” “identity,” “purpose,” and “meaning in life,” combined with Boolean operators to capture literature linking MS with components of existential disruption. A PRISMA flow diagram (Figure 1) was utilized to ensure transparency in documenting the identification, screening, and inclusion of studies (Page et al., 2021).
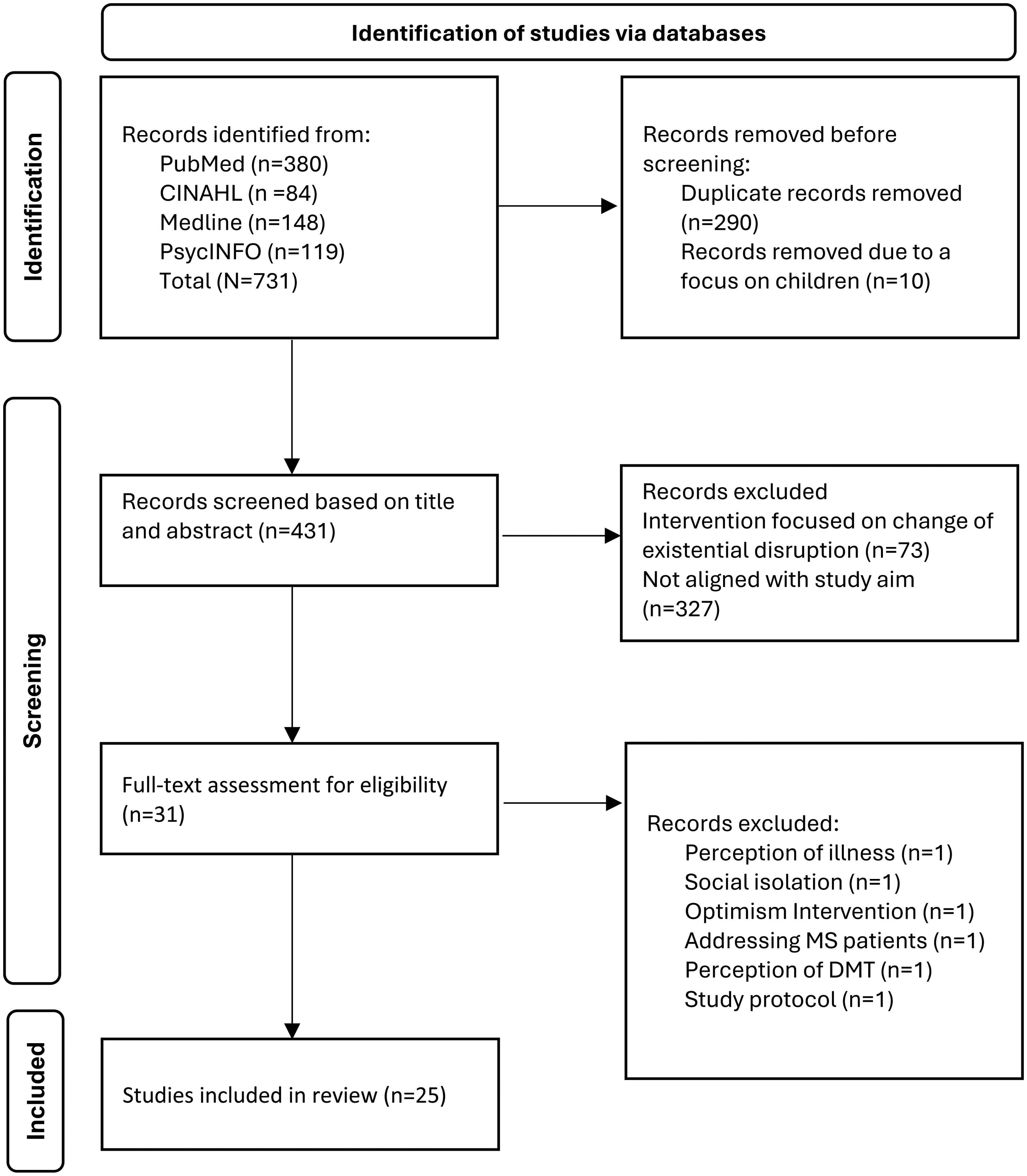
PRISMA flow diagram.
Eligible studies were peer-reviewed, written in English, and addressed experiences of MS relevant to identity, meaning, or purpose. All MS phenotypes were included, and qualitative, quantitative, and review designs were eligible; review articles were included for contextual purposes only. Intervention-focused studies were excluded to maintain conceptual focus. The initial literature search identified 731 articles; after screening, 25 remained for data synthesis and evaluation.
Study characteristics were extracted by the first author (LK), including country, design, sample, data collection methods, key findings, existential and meaning-related insights, and appraisal ratings (Table 1). Quality appraisal was conducted using the Johns Hopkins Evidence-Based Practice Model (Dang et al., 2021), with each study assigned a Level (I–III) and Quality grade (A–C). No studies were excluded based on appraisal, and the second author (CS) was available to address questions or uncertainties during the rating process.
Summary of Findings and Key Existential Messages From Included Studies.
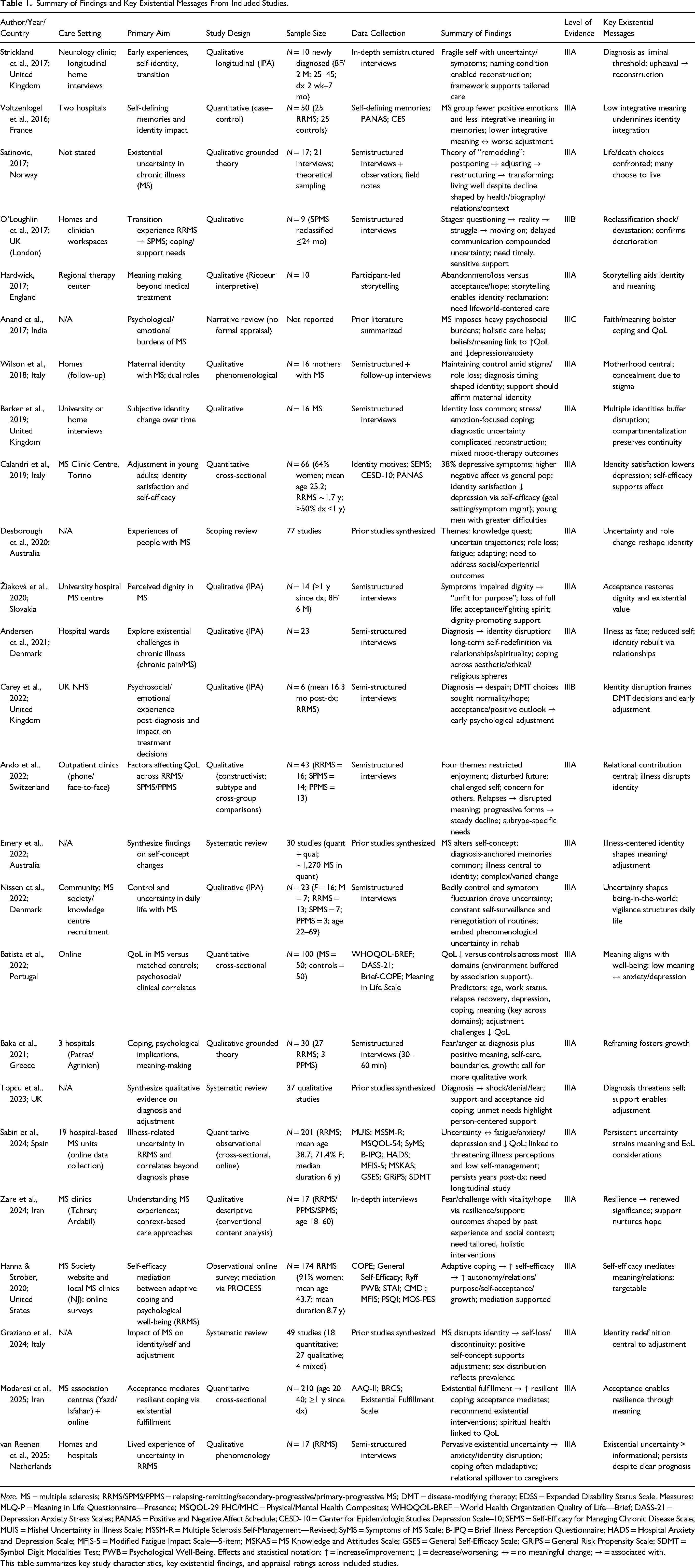
Note. MS = multiple sclerosis; RRMS/SPMS/PPMS = relapsing-remitting/secondary-progressive/primary-progressive MS; DMT = disease-modifying therapy; EDSS = Expanded Disability Status Scale. Measures: MLQ-P = Meaning in Life Questionnaire—Presence; MSQOL-29 PHC/MHC = Physical/Mental Health Composites; WHOQOL-BREF = World Health Organization Quality of Life—Brief; DASS-21 = Depression Anxiety Stress Scales; PANAS = Positive and Negative Affect Schedule; CESD-10 = Center for Epidemiologic Studies Depression Scale–10; SEMS = Self-Efficacy for Managing Chronic Disease Scale; MUIS = Mishel Uncertainty in Illness Scale; MSSM-R = Multiple Sclerosis Self-Management—Revised; SyMS = Symptoms of MS Scale; B-IPQ = Brief Illness Perception Questionnaire; HADS = Hospital Anxiety and Depression Scale; MFIS-5 = Modified Fatigue Impact Scale—5-item; MSKAS = MS Knowledge and Attitudes Scale; GSES = General Self-Efficacy Scale; GRiPS = General Risk Propensity Scale; SDMT = Symbol Digit Modalities Test; PWB = Psychological Well-Being. Effects and statistical notation: ↑ = increase/improvement; ↓ = decrease/worsening; ↔ = no meaningful change; → = associated with.
This table summarizes key study characteristics, key existential findings, and appraisal ratings across included studies.
Data analysis followed an iterative process consistent with integrative review methodology (Whittemore & Knafl, 2005). Extracted data were reviewed iteratively to identify patterns related to identity, meaning, and existential disruption across studies. An initial open coding approach was used to label key concepts, which were then grouped into broader categories through constant comparison across studies. These categories were refined through comparison of similarities and differences across studies, allowing for the development of higher-order themes that reflected shared existential experiences while preserving contextual variation.
To address heterogeneity in study design, findings were interpreted conceptually rather than aggregated statistically, with emphasis placed on convergence of meaning across methodologies. Review articles were used to support contextual interpretation rather than contribute primary data, reducing the risk of duplication while allowing for broader conceptual framing. Quality appraisal further informed synthesis by guiding the weighting of findings during interpretation, with higher-quality studies prioritized in thematic development and lower-quality studies interpreted with greater caution.
Potential bias in study selection is acknowledged, as screening and data extraction were conducted by a single reviewer. To mitigate this risk, uncertainties were discussed with a second author (CS). Additionally, the inclusion of primary and review studies may introduce interpretive overlap; however, this approach was intentionally used to support a comprehensive understanding of existential disruption while maintaining clear distinctions in how each source type contributed to the synthesis.
Results
Of the 25 studies included in this review, five were reviews, six were quantitative studies, and 14 were qualitative studies. The research was conducted across multiple continents, with the majority of studies from Europe (n = 19), alongside studies from North America (n = 1), Australia (n = 2), and Asia (n = 3). Findings are organized into five interrelated themes: biographical disruption and identity loss; meaning, identity disruption, and adaptation; uncertainty and liminality; stigma and social context; and patterns of existential disruption across the disease course. Across studies, these themes did not occur in isolation but interacted, shaping the experience of self, relationships, and future orientation over time.
Biographical Disruption and Identity Loss
Across reviewed studies, diagnosis was described as a disruptive event that altered anticipated life trajectories and required reevaluation of identity, roles, and future expectations (Emery et al., 2022; Graziano et al., 2024; Strickland et al., 2017). Participants reported loss across a range of domains central to selfhood, including work, family roles, bodily reliability, and social participation (Baka et al., 2021; Calandri et al., 2019; O'Loughlin et al., 2017). These disruptions were associated with losses in coherence and dignity as individuals worked to reconcile prior self-concepts with emerging limitations (Nissen et al., 2022; Žiaková et al., 2020).
Identity reconstruction was rarely linear and unfolded in shifting and overlapping ways. Individuals described grieving a lost past self, resisting integration through concealment, or gradually incorporating MS into a more coherent sense of self over time (Barker et al., 2019; Strickland et al., 2017). Young adults reported that a recent diagnosis struck at the core of identity, with identity satisfaction linked to improved adjustment and affect through MS-specific self-efficacy (Calandri et al., 2019; Desborough et al., 2020). One qualitative study framed existential disarray as a patterned response to interrupted life projects rather than an emotional reaction alone, emphasizing disruption to narrative continuity rather than symptom burden (Hardwick, 2017).
Meaning, Identity Disruption, and Adaptation
Meaning-making processes were consistently described as central to adaptation. Participants reported reinterpreting experiences to preserve a sense of authorship over their life narratives and to integrate MS into identity without allowing illness to dominate the self-concept (Voltzenlogel et al., 2016). These processes were associated with greater perceived coherence and dignity, even in the presence of functional limitations (Stepleman et al., 2017; O'Loughlin et al., 2017). Experiences at diagnosis were further described as emotional upheaval, with disruptions to self-concept, narrative continuity, and future orientation that constrained early sense-making and adjustment (Topcu et al., 2023). Meaning-making processes were closely tied to identity reconstruction, shaping how individuals sustained a sense of self amid continued change.
Several studies described deliberate adaptations, such as remodeling the life course, involving adjustments in activities, priorities, and expectations to maintain agency despite ongoing loss (Graziano et al., 2024; Satinovic, 2017). Quantitative evidence demonstrated that existential fulfillment and acceptance were associated with more resilient coping, with acceptance mediating the relationship between meaning and adaptive functioning (Modaresi et al., 2025). Across qualitative work, meaning-making supported continued engagement with valued roles and facilitated identity continuity throughout disease progression rather than signaling resolution alone (Ando et al., 2022).
Uncertainty and Liminality
Uncertainty emerged as a pervasive feature of living with MS, shaping daily experience, identity stability, and future orientation (Hanna & Strober, 2020; Topcu et al., 2023). Participants described persistent vigilance toward bodily changes, fluctuating symptoms, and unpredictable disease progression, contributing to a sustained sense of suspension between past and future selves (Strickland et al., 2017).
Several qualitative studies characterized uncertainty as a liminal state marked by ambiguity, loss of temporal confidence, and difficulty planning for the future (Anand et al., 2017; O'Loughlin et al., 2017; van Reenen et al., 2025). Transitions such as diagnosis, reclassification, relapse, or treatment change intensified this instability, prompting renewed questioning of identity, roles, and expectations (Carey et al., 2022).
Quantitative studies demonstrated that illness-related unpredictability was associated with poorer quality of life and increased psychological burden, including fatigue, anxiety, and distress, even years after diagnosis (Batista et al., 2022; Sabin et al., 2024). This uncertainty persisted across MS phenotypes and was not limited to early disease stages. Participants described uncertainty not only as a source of strain but as a driver of ongoing adjustment, requiring repeated renegotiation of routines, relationships, and expectations in response to changing conditions (Nissen et al., 2022; Zare et al., 2024).
Stigma and Social Context
Stigma was described as a contributor to identity disruption in MS, shaping how individuals perceived themselves and were perceived by others (Graziano et al., 2024; O'Loughlin et al., 2017; Wilson et al., 2018). Participants reported internalized stigma and experiences of misrecognition, particularly regarding invisible symptoms, which contributed to feelings of illegitimacy and identity fragmentation (Žiaková et al., 2020).
Several qualitative studies described how stigma constrained identity options by narrowing social roles and discouraging disclosure or help-seeking (O'Loughlin et al., 2017; Wilson et al., 2018). Participants reported concealing symptoms or diagnosis to preserve valued identities, particularly in work and caregiving roles, though concealment often intensified strain over time.
Conversely, studies described how social validation and supportive contexts mitigated the effects of stigma. Recognition by clinicians, family members, or peers supported dignity, self-continuity, and identity coherence (Nissen et al., 2022; Žiaková et al., 2020). These relational dynamics highlight how identity is shaped not only internally but through ongoing interpersonal interactions within care and social environments.
Patterns of Existential Disruption Across the Disease Course
Existential disruption was described as unfolding in patterned but nonlinear ways across the MS disease course. Several qualitative and mixed-methods studies identified recurring phases, including acute upheaval, periods of transitional liminality, and later orientations toward identity integration, rejection, or accommodation (Emery et al., 2022; Graziano et al., 2024; Strickland et al., 2017).
Subsequent transitions reactivated uncertainty and identity fragmentation rather than resolving it (O'Loughlin et al., 2017; van Reenen et al., 2025). Later experiences reflected variability rather than resolution, with some individuals describing greater coherence over time and others reporting ongoing instability shaped by cumulative loss or persistent uncertainty (Nissen et al., 2022; Zare et al., 2024). Quantitative findings similarly demonstrated that insecurity and meaning-related concerns appeared over time (Batista et al., 2022; Zare et al., 2024). Existential disruption was therefore not confined to a single disease stage but recurred across the illness trajectory in response to ongoing clinical and experiential changes.
Taken together, these findings suggest a pattern in which existential disruption in MS unfolds as a dynamic and recurring process shaped by the interaction of identity disruption, uncertainty, stigma, and meaning-making over time. Across studies, these dimensions did not operate independently but influenced how individuals interpreted illness, reconstructed identity, and navigated future possibilities. Uncertainty and stigma often intensified disruptions in identity, while meaning-making processes supported efforts to maintain continuity of self. This pattern appears to reflect a nonlinear trajectory, in which periods of disruption, adaptation, and reorientation recur across the disease course rather than progressing toward resolution, with existential disruption emerging as an ongoing negotiation of self-continuity in the context of changing conditions.
Discussion
This integrative review synthesizes existing evidence on existential disruption in MS, demonstrating how identity, meaning, and future orientation are shaped alongside neurological symptoms. Across studies, existential disruption was not experienced as a single event but as an ongoing process involving identity disruption, uncertainty, stigma, and evolving patterns of adaptation over time.
This synthesis expands existing literature by moving beyond descriptive accounts of psychosocial adjustment to more clearly conceptualize existential disruption as a dynamic, relational, and recurring process. While prior studies have identified components such as identity loss, uncertainty, and meaning-making, this review unites these elements to demonstrate how they interact across the illness trajectory, shaping continuity of self over time. In doing so, this review offers a more cohesive conceptualization of existential disruption in MS that has not been previously articulated in a unified manner.
Rather than occurring as discrete themes, these dimensions appear to interact in ways that shape the continuity of self. Disruptions in identity were often intensified by uncertainty, while experiences of stigma influenced how individuals understood and expressed changes in self. Meaning-making processes emerged as a central mechanism through which individuals navigated these disruptions, supporting efforts to maintain coherence across past, present, and anticipated selves. These findings illustrate how existential disruption unfolds through the ongoing interplay of identity, meaning, and context across the illness experience.
Findings from this review strengthen the conceptual distinction between existential disruption and affective symptoms such as depression and anxiety. Although mood-related distress was frequently reported, the literature consistently described disruptions in meaning, identity coherence, and narrative continuity that extend beyond emotional symptomatology. These findings position existential disruption as a distinct domain of experience, one that may coexist with psychological symptoms but is not reducible to them.
The reviewed literature also highlights the recursive nature of existential disruption across the MS disease course. While initial diagnosis was often associated with acute disruption, subsequent transitions frequently reactivated uncertainty and identity fragmentation. Meaning-making in this context reflects not only adaptation but ongoing efforts to restore coherence and purpose in the face of disruption, aligning with broader existential frameworks that emphasize the centrality of meaning in navigating suffering and life disruption (Roikjaer et al., 2025). These findings indicate that existential disruption is not resolved following initial adjustment but is revisited over time in response to ongoing clinical and experiential changes. As such, existential disruption in MS is best understood as a dynamic and recurring disturbance in self-continuity, characterized by ongoing negotiation of identity, meaning, and future orientation across the illness trajectory.
Within holistic nursing frameworks, existential disruption is best understood as a disturbance in personhood that reflects disruption in meaning, identity, and lived experiences as interconnected dimensions of health (Frisch & Rabinowitsch, 2019). This review extends holistic nursing perspectives by demonstrating how existential disruption is recognized in practice. From this lens, disruptions in self-continuity are not peripheral concerns but core components of the illness experience, shaping how individuals interpret their condition, engage in care, and envision their future.
In practice, disruptions in identity may present as shifts in roles, loss of future orientation, or difficulty integrating illness into a coherent sense of self. Uncertainty and stigma may influence how individuals communicate their experiences, while meaning-related concerns may emerge through expressions of loss, disconnection, or questioning of purpose. Attending to these dimensions requires approaches that prioritize relational engagement rather than solely symptom management.
These findings also highlight the need for assessment approaches that move beyond functional status to include identity, meaning, and future orientation. Holistic nursing care is strengthened by incorporating questions that explore changes in self-perception, anticipated life trajectory, and sources of meaning. Such approaches support care that is responsive to the full scope of the illness experience and reinforce nursing's role in addressing visible and nonvisible dimensions of health.
Strengths and Limitations
This review is strengthened by integrating qualitative, quantitative, and review studies across diverse MS populations and disease phenotypes, enabling the synthesis of existential disruption across illness stages and care contexts. The inclusion of studies employing in-depth qualitative methods enriched the understanding of identity loss, meaning-making, uncertainty, and adaptation, while quantitative findings supported distinctions between existential disruption and affective symptoms. Together, this mixed-methods evidence base enabled a comprehensive synthesis of existential experiences in MS that would not be possible through a single methodological lens.
Several limitations should be noted. Included studies varied widely in design and measurement. Tools assessing meaning, identity, acceptance, or engulfment were not standardized, and few measures were developed specifically for MS. This variability limits cross-study comparison and highlights the need for methodological refinement. In addition, most studies were cross-sectional, constraining insight into how existential experiences change over time.
Implications for Holistic Nursing Practice, Education, and Research
These findings extend holistic nursing practice by highlighting the need for assessment and care approaches that explicitly address disruptions in identity, meaning, and self-continuity across the illness trajectory. Although patients frequently describe changes in identity and meaning, these experiences remain inconsistently captured in routine assessment and documentation, limiting opportunities for timely recognition. Nurses’ sustained presence across disease transitions positions them to recognize shifts in self-understanding as they emerge.
Routine assessment can be enhanced through brief, relational questions that explore changes in self-concept, roles, and future orientation. Individuals may express existential disruption through statements reflecting loss of identity, uncertainty about the future, or difficulty integrating illness into a coherent sense of self. Nurses can use these expressions as clinical entry points to explore meaning and support earlier recognition of distress.
Nurses can support narrative reconstruction by validating identity loss, acknowledging personal history, and facilitating recognition of emerging values or strengths (Tarbi et al., 2023). During periods of transition nurses, can support adaptive coping by helping patients recalibrate expectations and maintain a sense of continuity. Because relational contexts shape adaptation, incorporating family perspectives into assessment may further support dignity and continuity of self (Walbaum et al., 2024).
Preparing nurses to recognize and respond to existential disruption requires greater emphasis on relational assessment, narrative competence, and meaning-centered care within nursing education. Training that focuses on listening for disruptions in identity and self-understanding, rather than only symptom reporting, may strengthen nurses’ ability to identify existential distress in practice. Educational efforts may also benefit from integrating frameworks that support communication around meaning, loss, and uncertainty. Developing these skills may enhance nurses’ confidence in addressing complex, nonvisible dimensions of illness that are often left unspoken in clinical encounters, consistent with holistic nursing perspectives that emphasize whole-person care and the integration of meaning into healing processes (Shea & Frisch, 2016).
Sustained or severe existential distress highlights the importance of continued research in this area. Advancing this work will require approaches that more intentionally integrate meaning and self-continuity into care processes, consistent with evolving perspectives on holistic nursing and healing (Shea & Frisch, 2016). Future studies may prioritize longitudinal designs to better understand how existential disruption evolves over time. There is also a need for MS-specific assessment approaches that capture changes in identity and self-continuity with greater precision.
Further development and testing of nurse-led interventions that support meaning, identity, and adaptation across the disease course are warranted. Although this review focuses on MS, similar patterns have been described across chronic illnesses marked by uncertainty and life disruption. Future research should examine how these patterns translate across conditions to inform more generalizable approaches to supporting patients in long-term illness.
Conclusion
Existential disruption represents an important and underrecognized dimension of living with MS, shaping identity, meaning, and future orientation across the disease course. This review demonstrates that these experiences are not peripheral to illness but central to how individuals understand themselves and navigate ongoing uncertainty, stigma, and adaptation. These findings suggest that attending to disruptions in identity and meaning is essential to supporting individuals living with MS, particularly as these encounters evolve across transitions in the disease trajectory. Nurses are well-positioned to recognize and respond to these shifts through relational, person-centered care that supports the continuity of self over time. Advancing this work will require developing approaches that more consistently assess existential experiences and interventions that support meaning-making and identity reconstruction as part of holistic care.
Footnotes
Ethical Considerations
Not applicable. This article does not involve primary research involving human participants, data, or tissue.
Funding Statement
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.