
Abstract
Purpose
Guided by Watson's Caring Science, this study explored the humanistic care needs of hospitalized orthopedic patients and interpreted the lived meanings underlying these needs.
Design
A descriptive phenomenological design was used.
Methods
Purposive sampling was used to recruit 13 orthopedic inpatients from a tertiary hospital in Hebei Province, China. Data were collected through semistructured in-depth interviews and analyzed using Colaizzi's seven-step phenomenological method.
Findings
Nine themes were identified, covering pain management, safety and environmental needs, daily care, privacy and respect, psychological support, rehabilitation guidance, continuity of care, caring attention and support, and communication. Beyond these specific needs, the findings revealed a core lived experience of vulnerability, dependence, and threatened dignity during hospitalization. Patients sought not only symptom relief, but also humanistic care that helped them feel respected, understood, supported, and gradually move toward healing.
Conclusions
Orthopedic inpatients have multidimensional humanistic care needs that reflect a holistic caring experience of body, mind, and spirit. Integrating technical care, relational care, and continuity of care may strengthen holistic nursing practice in orthopedic settings.
Keywords
Introduction
Holistic nursing emphasizes care for the whole person by addressing physical, psychological, social, and spiritual needs. Grounded in the view that the person is an integrated whole, holistic nursing shifts the focus from task-oriented care to person-centered healing and is particularly relevant in clinical settings where patients present with complex and multidimensional care needs (American Nurses Association and American Holistic Nurses Association, 2019). Jean Watson's Caring Science provides an important theoretical foundation for this nursing paradigm. Watson conceptualizes caring as the essence of nursing, extending beyond technical procedures to an interpersonal and moral process that promotes harmony and unity of body, mind, and spirit (Watson, 1979). Watson's 10 Caritas Processes, including loving-kindness, sustaining faith and hope, authentic presence, and the creation of a healing environment, closely align with the principles of holistic nursing and humanistic care (Watson, 1988).
Orthopedic inpatients have specific vulnerabilities, necessitating comprehensive care and humanistic care. Fractures, joint replacements, and severe injuries frequently lead to acute pain, restricted mobility, functional impairment, extended recovery durations, and psychological distress, encompassing anxiety, sadness, and dread of dependency (Bandholm et al., 2018; van de Ree et al., 2020). These conditions may undermine patients’ sense of wholeness by affecting not only physical functioning, but also emotional resilience, social roles, and the search for meaning (Taylor et al., 2024). Although surgical techniques and rehabilitation practices have improved, routine orthopedic care often remains centered on disease-specific treatment, and the broader impact of illness on patients’ lived experiences and quality of life may receive insufficient attention (Gosens & den Oudsten, 2023).
Existing studies have highlighted the importance of holistic and humanistic care for orthopedic inpatients. Previous research suggests that patients’ needs for pain relief, emotional support, privacy protection, rehabilitation guidance, and family involvement are often insufficiently addressed, which may contribute to longer hospital stays and reduced satisfaction (van de Ree et al., 2020; Taylor et al., 2024; Reichman et al., 2023). Although Watson's Caring Science has been applied in various acute care settings such as neurosurgery and emergency care (Elahi et al., 2021), its application in orthopedic nursing remains limited. In addition, relatively few studies have explored orthopedic inpatients’ lived experiences from a holistic caring perspective (Elahi et al., 2021; Scott et al., 2024). This gap is particularly relevant in China, where population aging and the increasing number of orthopedic inpatients call for culturally sensitive and multidimensional nursing care (Yuan et al., 2025; Liu et al., 2024).
To fill this gap in research on humanistic care in orthopedics, this study uses Watson's Caring Science as its theoretical framework and epistemological stance. Using a descriptive phenomenological design, this study examines orthopedic inpatients’ lived experiences of illness, vulnerability, dependence, and the search for meaning, hope, and wholeness during hospitalization. This study aims to provide holistic nursing insights for orthopedic clinical practice, guided by care philosophy and informed by authentic patient voices, while also revealing patients’ multidimensional care needs across physical, psychological, social, and spiritual dimensions. By focusing on patients’ own accounts, this study may help inform orthopedic nursing practices that combine technical care with relational and holistic support.
Method
This study employed a descriptive phenomenological design. It is guided by Jean Watson's Caring Science and uses Colaizzi's seven-step phenomenological method to systematically explore and describe patients’ lived experiences of illness and vulnerability. The study explored both the care needs expressed by orthopedic inpatients and the lived meanings behind these needs, especially how pain, limited mobility, and dependence shaped their sense of vulnerability, dignity, and need for support. Specifically, it explores how patients, in the face of illness, pain, limited mobility, and dependence on others, experience vulnerability and anxiety, feel that their dignity is challenged, and express a desire to be understood, supported, and cared for as whole persons.
Descriptive phenomenology is appropriate for exploring participants’ lived experiences within a particular clinical context. In this study, it enabled an in-depth examination of orthopedic inpatients’ experiences of pain, limited mobility, dependence, dignity, emotional distress, and the need to be cared for as whole persons. This approach allowed the analysis to remain close to participants’ everyday language and descriptions while identifying the essential meanings underlying their physical, psychological, social, and spiritual humanistic care needs (Giorgi, 2009; Wirihana et al., 2018; Northall et al., 2020).
Setting and Participants
The study was carried out from March to April 2025 in the orthopedic ward of a Class III Grade A hospital in Hebei Province, China. To ensure diversity and adequate information, participants were selected using purposive sampling with a maximum variation strategy. During recruitment, the researchers intentionally included patients of different ages, genders, educational backgrounds, disease types, and lengths of hospital stay to reflect the diversity of humanistic care needs among orthopedic inpatients. Inclusion criteria were age ≥18 years, hospitalization duration ≥5 days, consciousness with clear communication ability, and voluntary participation. Exclusion criteria encompassed a history of mental illness or cognitive impairment, ambiguous verbal expression, or withdrawal from the study. Sample size was determined based on data saturation, ultimately enrolling 13 patients. No new significant information or themes emerged in the later interviews. The research team therefore concluded that data saturation had been reached and stopped recruiting new participants. In addition, the sample size was considered sufficient due to the richness and depth of participants’ narratives and the inclusion of patients with varied diagnoses, functional limitations, and hospitalization experiences, which allowed for a comprehensive understanding of diverse humanistic care needs. Participants’ demographic information is presented in Table 1.
General Participant Characteristics (N = 13).
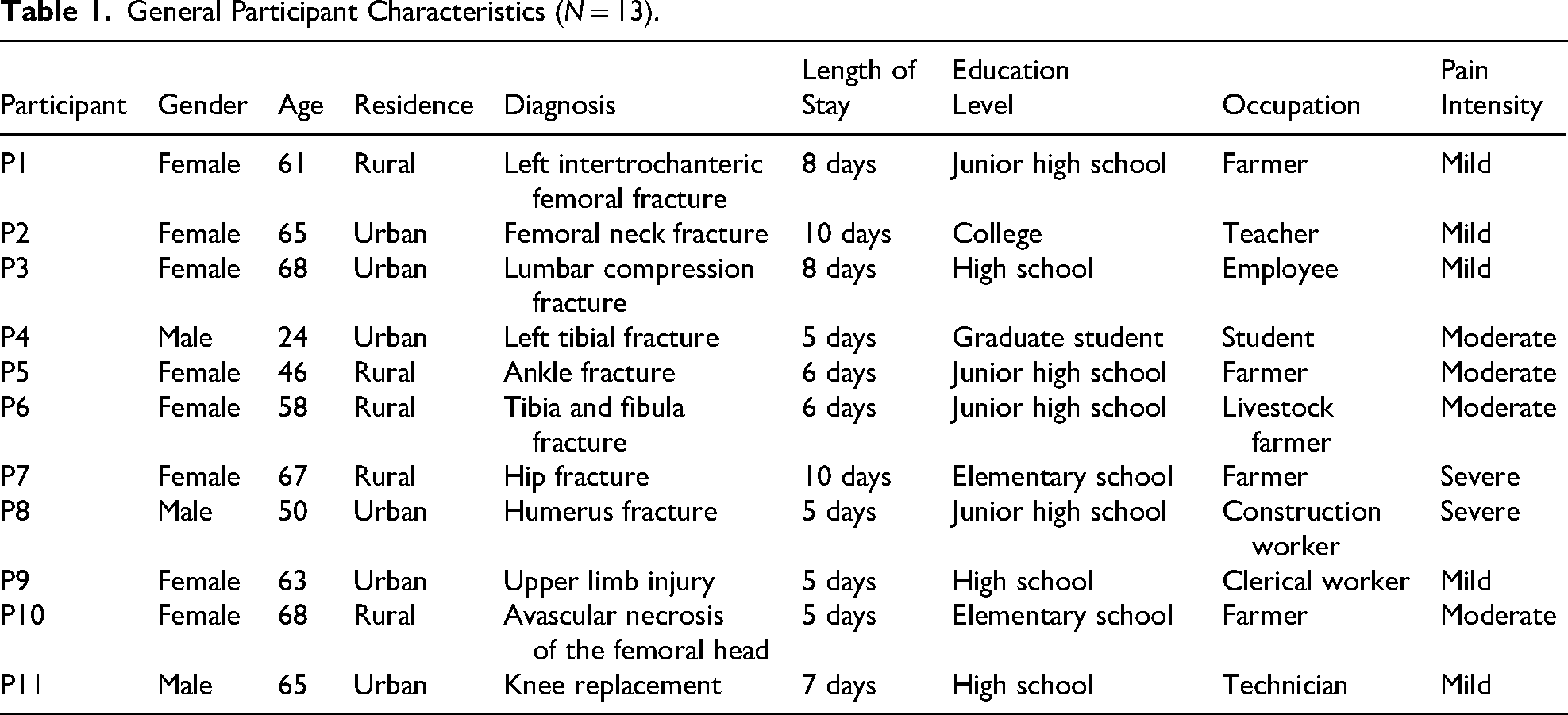

Note: Pain intensity was assessed using the Numeric Rating Scale (NRS), with scores of 1–3 indicating mild pain, 4–7 moderate pain, and 8–10 severe pain.
Data Collection
All interviews were conducted by the first author, a registered nurse with clinical experience in orthopedic care and familiarity with Watson's Caring Science. To minimize the influence of prior assumptions, she maintained reflexive awareness throughout the research process and adopted an open, non-judgmental attitude during interviews. Prior to the interviews, the researcher explained the purpose of the study and introduced herself to the participants as the researcher. There was no therapeutic relationship between the researcher and the participants. Data collection employed semi-structured in-depth interviews. Watson's 10 Caritas Processes were used as a starting point to develop the interview guide (Watson, 1979; Watson, 1988), which was then updated based on a review of the literature and pre-interviews. A researcher-developed questionnaire with sociodemographic and clinical information was used to collect general participant data.
Interviews were conducted one-on-one in private settings (quiet ward demonstration rooms or bedside with privacy curtains), lasting 40–60 min each (mean duration: 48 min). This duration allowed sufficient time for participants to reflect on and articulate their experiences without fatigue or interruption.
All sessions were audio-recorded with nonverbal cues (e.g., facial expressions, tone of voice) documented. Bedside interviews were conducted for mobility-impaired patients. Informed consent forms explaining study objectives, confidentiality, and withdrawal rights were signed prior to interviews. After each interview, participants were thanked and asked if they wished to add supplementary information. Recordings were transcribed within 24 h, with two researchers independently verifying accuracy. Timely transcription and investigator cross-checking were undertaken to preserve experiential integrity and enhance data credibility. The semistructured interview guide consisted of the following open-ended questions designed to elicit participants’ lived experiences and humanistic care needs: (1) Please share your experiences with nursing care during your hospital stay regarding pain management, assistance with activities, or daily living. How would you most like nurses to support you? (2) Regarding ward safety (such as fall prevention and facility environment), what are your thoughts or experiences? What do you think could be improved? (3) When nurses perform care procedures or communicate treatment information, how do you feel respected or that your privacy is protected? Have you had any particular experiences? (4) During your hospitalization, when you felt anxious, worried, or down, what communication or support methods from nurses made you feel understood? (5) During functional exercises and rehabilitation guidance, how would you like nurses to assist you? What were your actual experiences? (6) What kind of ongoing help from staff or the hospital would you like to get after you leave the hospital for rehabilitation? (7) How would you like nurses to help you get in touch with family or neighborhood services that can help you get better? (8) Can you describe a time when you felt especially safe or cared for while receiving care? What effect did this experience have on your healing? (9) Throughout your hospital stay, are there any other care needs or expectations that have not been discussed? You are welcome to share your thoughts or experiences.
Data Analysis
Data analysis employed Colaizzi's seven-step phenomenological method, supplemented by NVivo 15.0 software for coding and management. Manual coding served as the primary analytical approach, while NVivo was used as a supportive tool for data organization and management (Vignato et al., 2022).
After transcription, all interview transcripts were imported into NVivo 15.0 for systematic storage and retrieval. Two researchers independently conducted line-by-line coding to identify meaningful statements relevant to the research aims. After initial coding, the researchers compared results, discussed discrepancies, and returned to the original data until consensus was reached.
The analysis followed Colaizzi's seven steps (Colaizzi, 1978): (1) reading all transcripts repeatedly to familiarize with the content; (2) extracting significant statements; (3) formulating meanings; (4) organizing meanings into theme clusters; (5) developing an exhaustive description; (6) identifying the fundamental structure of the experience; and (7) returning preliminary findings to participants for validation.
NVivo's node and clustering functions assisted in organizing codes and developing subthemes and broader themes. A descriptive phenomenological approach was adopted to examine the essential structure of humanistic care experiences among orthopedic inpatients. Throughout the process, the researchers maintained reflexive notes and engaged in iterative team discussions to minimize personal bias. Through the sixth and seventh steps of Colaizzi's method, this study distilled a core lived experience of vulnerability, dependence, and threatened dignity, through which patients sought security, respect, and healing during hospitalization.
Ethical Considerations
This study was approved by the Medical Ethics Committee of a tertiary Class A hospital in Hebei Province, China (Approval Number: HDFYLL-IIT-2025-033). Ethical principles of informed consent, voluntary participation, confidentiality, and non-maleficence were strictly followed. Written informed consent was obtained from all participants. All data were anonymized, and audio recordings and transcripts were used only for research purposes. Participants were free to withdraw at any time without affecting their care. Participants’ emotional well-being was monitored throughout the interview process, and interviews were paused or adjusted if signs of distress were observed.
Trustworthiness
Lincoln and Guba's (Lincoln & Guba, 1985) factors for establishing trustworthiness were used in this study. The following strategies were used to ensure credibility, transferability, dependability, and confirmability. (a) Credibility was established through in-depth interviews with patients, data analysis by two researchers who agreed on the results, and then sharing preliminary findings with a small group of patients to make sure they were in line with their real experiences; (b) transferability was supported by describing the study setting, participants’ characteristics (see Table 1), and the rationale for participant selection; (c) dependability was maintained by retaining complete audio recordings for cross-checking transcripts and analysis. These records were deleted after the completion of the study in accordance with ethical requirements. To keep track of the study process, transcripts and analysis notes were kept; and (d) during data collection and analysis, the researchers kept reflexive journals to document their assumptions, emotional responses, and possible preconceptions related to humanistic care and Watson's Caring Science. Coding results were discussed within the research team, and disagreements were resolved by constantly returning to participants’ original accounts, thereby enhancing confirmability.
Results
Nine main themes emerged from in-depth interviews with 13 orthopedic inpatients. These themes covered a wide range of care needs, including physical, psychological, social, and spiritual dimensions. Overall, they reflected patients’ expectations for humanistic care throughout hospitalization (see Table 2). This care was reflected not only in the attitudes and relationships between nurses and patients, but also in specific nursing practices such as pain management, safety assurance, rehabilitation guidance, and ongoing support.
Humanistic Care Needs of Hospitalized Orthopedic Patients: Main Themes, Subthemes, and Illustrative Alignment With Watson's 10 Caritas Processes.
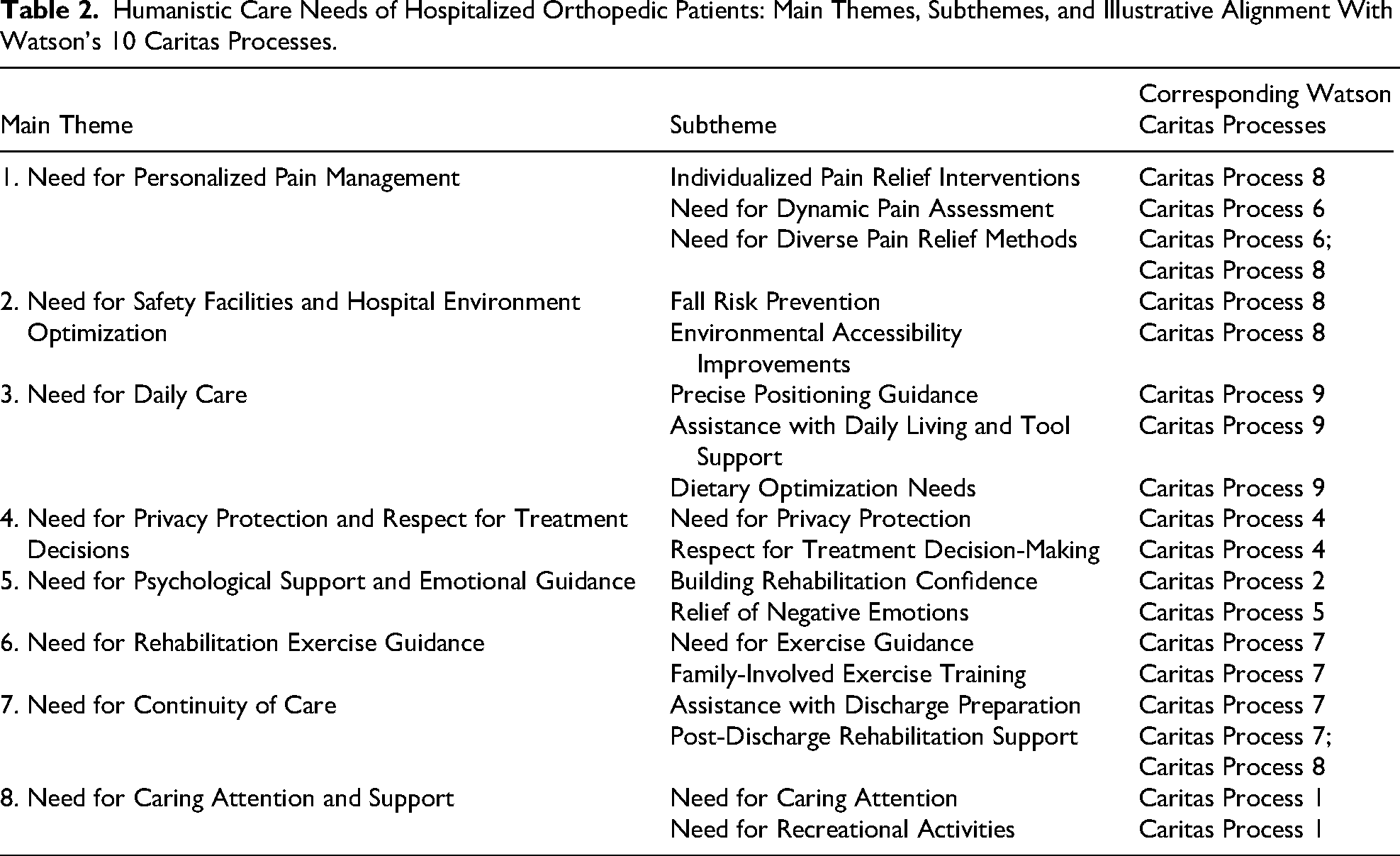
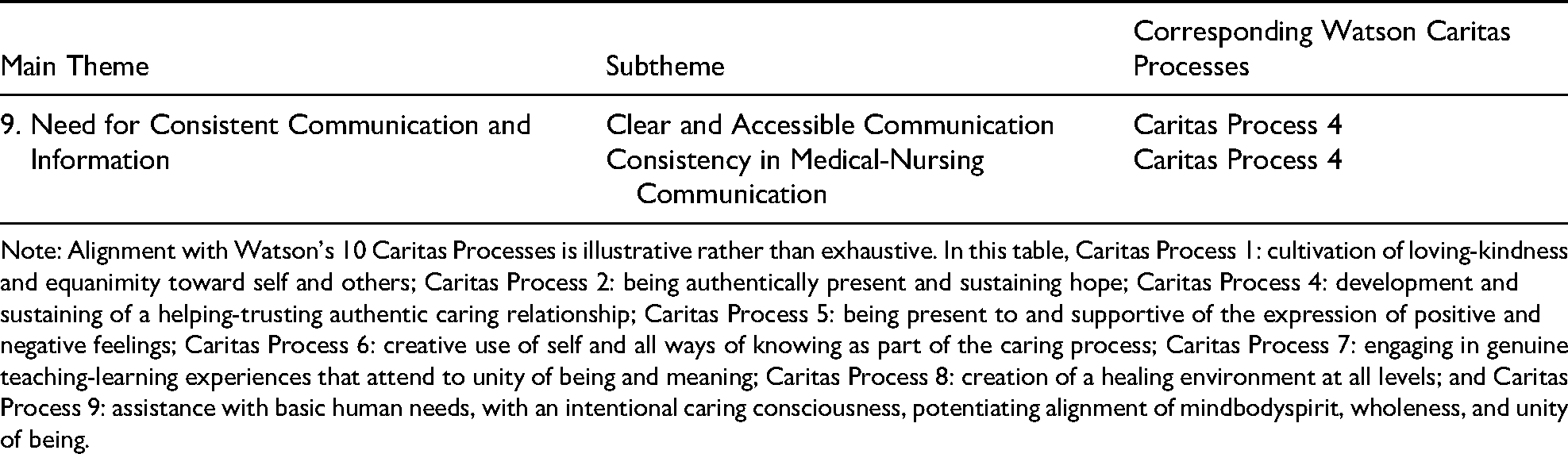
Note: Alignment with Watson's 10 Caritas Processes is illustrative rather than exhaustive. In this table, Caritas Process 1: cultivation of loving-kindness and equanimity toward self and others; Caritas Process 2: being authentically present and sustaining hope; Caritas Process 4: development and sustaining of a helping-trusting authentic caring relationship; Caritas Process 5: being present to and supportive of the expression of positive and negative feelings; Caritas Process 6: creative use of self and all ways of knowing as part of the caring process; Caritas Process 7: engaging in genuine teaching-learning experiences that attend to unity of being and meaning; Caritas Process 8: creation of a healing environment at all levels; and Caritas Process 9: assistance with basic human needs, with an intentional caring consciousness, potentiating alignment of mindbodyspirit, wholeness, and unity of being.
In summary, these themes reflected a core lived experience: for orthopedic inpatients, hospitalization was not merely a matter of receiving treatment, but also an ongoing process of vulnerability and dependence amid pain, limited mobility, and changes in social roles. Throughout this process, patients were concerned not only with symptom relief, but also with whether they were treated with respect, understanding, and compassion. For them, humanistic care was not an additional aspect of care, but a vital component in helping them rebuild a sense of security, dignity, and hope. In this sense, humanistic care was not only about comfort and being cared for, but also about whether patients could maintain their dignity, reduce their sense of helplessness, and gradually move toward healing during hospitalization.
Theme 1: Need for Personalized Pain Management
Patients described pain as a persistent and multifaceted experience that affected their sleep, mobility, emotional state, and sense of control. They desired timely, individualized pain assessment and relief strategies from nurses. The nurse taught me some pain relief methods—applying ice packs and practicing relaxation breathing. It worked fairly well, so I don't have to take painkillers every time. (P2) The postoperative wound hurt badly, especially during dressing changes and rehabilitation exercises. I wish they could have warned me beforehand that it might hurt a bit so I could have been mentally prepared. (P4) When the pain is severe, I wish nurses would promptly administer pain medication instead of making me endure it. (P6)
Theme 2: Need for Safety Facilities and Hospital Environment Optimization
Due to limited mobility and fear of falling, patients were particularly attentive to environmental safety and accessibility in the ward. They hoped the hospital environment could minimize risks and support safe movement. I’m especially afraid of slipping when walking with crutches, particularly in the wet bathroom. (P1) The ward toilet has no grab bars, and I fear falling every time I stand up. (P5) The bedside lamp is too dim at night; I can't see the path clearly when going to the bathroom. (P9)
Theme 3: Need for Daily Care
Mobility limitations made patients highly dependent on nurses for maintaining body position, daily living assistance, and dietary management. They sought more meticulous, personalized care to enhance comfort and rehabilitation support. Teach family members how to support the waist and legs during repositioning so it's easier at home. (P2) Using the restroom and personal hygiene are the most troublesome; I hope nurses can lend a hand more often. (P5) My arm was injured, making dressing and undressing difficult. When I asked nurses to help change my clothes, they were exceptionally gentle—I'm truly grateful. (P9)
Theme 4: Need for Privacy Protection and Respect for Treatment Decisions
Patients desire privacy protection and respect for autonomy during nursing procedures and treatment decisions, viewing these as essential for building trust. Small gestures like drawing curtains or closing doors during procedures make me feel respected. (P2) Explain treatment risks and offer me choices instead of just recommending options. (P7) Please allow us sufficient time to review informed consent forms after providing a brief explanation. (P13)
Theme 5: Need for Psychological Support and Emotional Guidance
Patients frequently expressed feelings of anxiety, helplessness, and role disruption during hospitalization. They valued nurses’ empathetic listening, encouragement, and genuine presence, which helped them feel emotionally supported. When the nurse sat down to talk and said, “Don’t worry,” I felt much more at ease. (P3) That morning during shift handover, I overheard nurses saying Bed 27's auntie was being overly dramatic … Hearing that made me feel even more pressured, more distressed, and less inclined to turn over. (P10) My whole family depends on me for their livelihood. I’m the pillar of our household. Now I’m just lying here, spending so much money, feeling like a useless person. (P12)
Theme 6: Need for Rehabilitation Exercise Guidance
Patients require clear, actionable, personalized guidance, and family involvement in training. Questions about the purpose and correctness of exercises highlight the importance of information interpretation. Only when someone teaches me the movements step-by-step and corrects my mistakes do I dare to keep practicing. (P2) The rehab manual they gave me has tiny print and blurry pictures. It would be best if someone could guide me while I do the exercises to ensure my form is correct. (P11) They asked me to do foot flexing to prevent blood clots. I’m not that old—how could I get a blood clot? I would rather not do it, and I can’t remember the instructions. (P13)
Theme 7: Need for Continuity of Care
Patients expressed considerable uncertainty and anxiety about continuing rehabilitation after discharge. They desired clearer discharge preparation, follow-up support, and reliable communication channels. After discharge, I feel that no one will manage my care. I hope for phone follow-ups or WeChat group guidance. (P1) I dare not think about what happens after going home … What if an emergency arises at home? There won’t be any professionals to guide me. (P7) just hope I can still do farm work after discharge without any issues, like leg pain on cloudy or rainy days. (P8)
Theme 8: Need for Caring Attention and Support
Patients appreciated small acts of caring attention from nurses, such as remembering personal preferences or adjusting their position for comfort. Some also hoped for simple activities to reduce feelings of loneliness during long hospital stays. The nurse remembered my preferences and even helped resolve a dispute in the middle of the night—it felt like family. (P1) My primary nurse often adjusted my pillow height and the cushion behind my waist, worried I might be uncomfortable. It made me feel she truly cared for me like her family. (P2) Being hospitalized for so long is stifling. Could you organize some activities so we can chat and pass the time? (P2)
Theme 9: Need for Consistent Communication and Information
Ambiguous or inconsistent information causes patient confusion and distrust. Patients expect clear, accessible, and unified communication. Explain the purpose of medications and injections before administering them, especially for newly added ones. (P6) Different nurses provide conflicting information, which confuses me. (P9) Occasionally I don’t know whether to follow the doctor's instructions or the nurse's … It's all so confusing. (P9)
Overall, these themes reveal the holistic nature of humanistic care needs among orthopedic inpatients, extending from physical comfort to psychological support, social connection, and the restoration of meaning, hope, and a sense of being valued. Patients described genuine empathy, respect for their experiences, and sustained care as central to feeling secure, valued, and more confident during recovery.
Discussion
Core Lived Experience of Humanistic Care Among Orthopedic Inpatients
From a descriptive phenomenological perspective, this study revealed the core lived experience underlying orthopedic inpatients’ humanistic care needs. The findings indicate that hospitalization was experienced not only as a process of receiving treatment, but also as a period of vulnerability, dependence, and threatened dignity. Patients wanted more than fragmented care tasks; they wanted a holistic caring experience in which they felt seen, understood, respected, and continuously supported. In this sense, humanistic care not only relieved physical discomfort, but also supported patients in rebuilding a sense of security, hope, and wholeness of body, mind, and spirit during illness and hospitalization. These findings support Watson's view that caring promotes the unity of body, mind, and spirit and suggest that, in orthopedic inpatient care, this unity can be supported through concrete practices such as pain management, dignity preservation, relational support, and rehabilitation support (Watson, 1979; Watson, 1988). In the context of orthopedic inpatient care, these findings extend Watson's Caring Science by suggesting that caring is expressed not only through emotional presence, but also through technical care, dignity-preserving communication, and continued support during rehabilitation (Allsop et al., 2026).
Vulnerability, Dignity, and Healing in Orthopedic Care
Research findings indicate that orthopedic inpatients’ care needs are closely tied to vulnerability, dignity, and healing. Pain management needs were highly individualized, and patients’ concerns regarding dynamic assessment, non-pharmacological interventions, and medication side effects reflect the complexity of pain experiences among orthopedic inpatients (Mezey et al., 2022; Shi et al., 2021). Pain was described not only as a physical sensation, but also as an experience intertwined with fear, uncertainty, and vulnerability (Villar-Alises et al., 2024). Likewise, functional limitations heightened dependence on others and increased the need for safety facilities, daily care, and environmental improvement. Previous research has shown that external hazards can intensify feelings of insecurity among fracture patients (Allsop et al., 2026), while studies on orthopedic nursing services in China suggest that patients may also have context-specific needs related to ward environment, accessibility, and service quality (Cao et al., 2025). Together, these findings indicate that pain management and environmental support are meaningful not only because they reduce symptoms and risk, but also because they help patients regain security within the caring relationship and the healing environment (Watson, 1988).
The findings also showed that dignity was central to patients’ experiences of care. Demands for privacy protection, respect for treatment decisions, and consistent information reflected patients’ desire to be treated as persons with autonomy and worth (Fuseini et al., 2023). Research by Sadh et al. (2025) suggests that inconsistent information can undermine nurse–patient trust. In the present study, being respected, informed, and taken seriously helped patients feel safe and supported. This enriches the understanding of “building genuine trust” within Watson's theory and suggests that, in orthopedic inpatient care, dignity is sustained through concrete experiences of explanation, respect, and acknowledgment; maintaining dignity is itself an important part of healing (Watson, 1988).
The need for psychological support, emotional guidance, and caring attention further highlighted the importance of emotional and spiritual care. Prior studies have shown that individuals with hip fractures often experience social role disruption, reduced participation, emotional isolation, and psychological distress during recovery (Zare et al., 2024; Scott et al., 2024). Similarly, participants in this study described feelings of helplessness, loss of worth, and disrupted wholeness. Expressions such as “like a useless person” or “the pillar of the family has fallen” reflect how illness and dependency can threaten identity and meaning. In this context, empathetic listening, encouragement, and genuine nurse–patient connection were not minor interpersonal details, but essential aspects of the caring–healing process. Healing, therefore, involved not only physical recovery, but also the rebuilding of self-worth, hope, and a sense of being needed (Watson, 2008; Babaii et al., 2021).
Continuity of Care and Implications for Holistic Nursing
Beyond patients’ in-hospital experiences of vulnerability, dignity, and healing, the findings also showed that their care needs extended into the transition from hospital to home. Needs for rehabilitation guidance and continuity of care reflected patients’ anxiety during the transition from hospital to home. Participants worried about being unsupported after discharge and expressed clear needs for consistent guidance, family involvement, and post-discharge support. These findings reinforce the importance of relational continuity across hospital–community boundaries and provide patient-centered evidence for strengthening transitional care models (Li et al., 2020). They also broaden the understanding of “teaching-learning experience” and “meeting basic needs” within Watson's theory, suggesting that humanistic care should not end with the inpatient phase, but should extend to discharge planning, family involvement, and ongoing rehabilitation support (Watson, 1988).
In summary, this study extends the understanding of holistic nursing in orthopedic care. Unlike previous studies, which have primarily focused on pain management, psychological distress, nurse–patient communication, or rehabilitation exercises, this study draws on patients’ lived experiences and shows how these specific needs together form a holistic caring experience shaped by vulnerability, dignity, and recovery (Mezey et al., 2022; Scott et al., 2024; Sadh et al., 2025; Li et al., 2020). In orthopedic nursing, holistic nursing is not limited to emotional support, but also emphasizes the integration of technical care, relational care, and continuous care to promote patients’ physical, psychological, and spiritual recovery (Watson, 1979; Watson, 1988).
These findings suggest that Watson's Caring Science can also help explain humanistic care needs in orthopedic inpatient care, especially those related to pain, functional limitation, dependence on others, and the transition from hospital to home (Elahi et al., 2021). Against the backdrop of China's accelerating population aging, these findings further underscore the importance of culturally sensitive holistic nursing in orthopedic care (Yuan et al., 2025). Consequently, this study not only provides a patient-experience-based foundation for holistic nursing practice in orthopedics, but also offers new empirical support for the application of holistic nursing knowledge in highly technical specialties.
Limitations
This study has several limitations. First, the sample was drawn from the orthopedic ward of a single Grade A tertiary hospital in Hebei Province and included only 13 participants. Although rich data were obtained, the findings may have limited transferability to other healthcare settings or regions because of the small sample size and single-site design (Kim et al., 2017). Second, this study focused only on patients’ perspectives and did not include those of nurses or family caregivers. Future research incorporating multiple perspectives may provide a more comprehensive understanding of humanistic care needs (Zhang et al., 2024). In addition, the interviews relied on participants’ retrospective accounts, which may have introduced recall bias (Shelton & Goodwin, 2022).
Implications
Implications for Nursing Practice
The findings of this study provide practical guidance for holistic nursing in orthopedic settings. Guided by Watson's Caring Science, orthopedic nursing should address patients’ physical, psychological, social, and spiritual needs within a person-centered model of care (Vujanić et al., 2022). In clinical practice, nurses should implement individualized and regularly evaluated pain management plans that combine pharmacological and nonpharmacological strategies to address complex and persistent pain (Goel et al., 2023; Duan, 2021). Environmental safety should also be strengthened by improving fall-prevention facilities and optimizing ward conditions such as lighting and temperature, thereby enhancing patients’ sense of security and comfort (Sivanathan & Rabes, 2023). In addition, because orthopedic inpatients often depend on others for daily activities, nurses should provide more individualized assistance in daily care and pay closer attention to privacy protection, clear communication, and information consistency, all of which are important for maintaining patients’ dignity and trust (Guo et al., 2022; Reddy et al., 2023; Seittu et al., 2024).
Emotional support should also be integrated into routine orthopedic nursing care. Nurses should use empathetic listening, encouragement, and timely responses to patients’ emotional distress in order to strengthen hope and psychological resilience (Campbell et al., 2020). At the same time, rehabilitation guidance and discharge preparation should be improved through clearer exercise instruction, stronger family involvement, individualized discharge planning, and ongoing follow-up support to reduce patients’ anxiety during the transition from hospital to home (Allsop et al., 2026).
At the practical level, orthopedic nurses can translate humanistic care into concrete measures across the entire hospitalization process. For example, in pain management, they can strengthen dynamic assessment and individualized interventions (Xie et al., 2025); in daily care, they can prioritize privacy protection, information consistency, and clear communication (Ambushe et al., 2023); in emotional support, they can increase active listening, encouragement, and attention to patients’ experiences of role frustration (Ambushe et al., 2023; Song et al., 2025); and in discharge planning, they can provide clearer rehabilitation guidance, family-involvement training, and arrangements for ongoing follow-up (Song et al., 2025). By making humanistic care more concrete and actionable, these measures can help integrate holistic nursing into the daily care of orthopedic patients.
Implications for Nursing Education and Institutional Support
These findings also have implications for nursing education and institutional support. In nursing education, orthopedic nursing training should not be limited to technical skills and disease knowledge, but should also emphasize communication skills, emotional recognition, empathetic responses, privacy protection, and support for discharge transition. The humanistic care needs identified in this study can be incorporated into case-based teaching, scenario simulation, and continuing education programs to help nurses and students better understand patients’ lived experiences of pain, dependence, role change, and uncertainty during recovery, thereby enhancing holistic nursing competence (Sigedar et al., 2026; Dai et al., 2025; Cao et al., 2025).
From a holistic nursing perspective, these findings also support interdisciplinary collaboration in meeting patients’ multifaceted needs (Kwame & Petrucka, 2021; Campbell et al., 2020). Even in resource-constrained clinical settings, attention to humanistic details such as communication, emotional responsiveness, and privacy protection can significantly influence patients’ sense of security, trust, and confidence in recovery (Liu et al., 2016; Reddy et al., 2023). In addition, digital health tools, such as follow-up platforms or mobile applications, may help extend holistic care across settings and improve continuity of support (Bulto, 2024; Charalambous et al., 2024; Schultz, 2023).
At the management and systems level, hospital and nursing leadership teams should strengthen institutional support for holistic nursing in orthopedics. This may include incorporating person-centered care indicators into nursing quality assessment, optimizing ward environments and safety facilities, refining discharge-planning and transition-of-care processes, and promoting information consistency and collaboration among clinical teams. With the support of policies, processes, and resources, holistic nursing can be translated into a stable and sustainable clinical practice (Lv et al., 2025; Li et al., 2020).
Conclusion
This study employed a descriptive phenomenological qualitative design and identified nine themes from the lived experiences of 13 orthopedic inpatients. These themes included pain management, a safe environment, daily care, privacy and respect, psychological support, rehabilitation guidance, continuity of care, caring attention and support, and clear communication. The findings suggest that orthopedic inpatients have multidimensional humanistic care needs related to pain, limited mobility, prolonged recovery, and dependence on others. These needs highlight that, in orthopedic nursing, holistic care is not merely a supplement to technical interventions, but an important pathway for supporting healing of body, mind, and spirit (Watson, 1979; Watson, 1988).
By focusing on patients’ own experiences, this study adds qualitative evidence on humanistic care needs in orthopedic nursing and highlights the importance of culturally sensitive holistic care in the context of population aging in China (Yuan et al., 2025). Future research may include multicenter studies, incorporate multiple perspectives such as those of nurses and family caregivers, and develop intervention programs based on the themes identified in this study to examine their effects on patient outcomes. Overall, this study supports the further application of holistic nursing in orthopedic care and provides patient-centered evidence for promoting more human-centered, integrated, and sustainable nursing practice.
Supplemental Material
sj-pdf-1-jhn-10.1177_08980101261456468 - Supplemental material for Humanistic Care Needs of Hospitalized Orthopedic Patients: A Qualitative Study Guided by Watson's Caring Science
Supplemental material, sj-pdf-1-jhn-10.1177_08980101261456468 for Humanistic Care Needs of Hospitalized Orthopedic Patients: A Qualitative Study Guided by Watson's Caring Science by Haitong Wu, Binglin Wu, Shanshan Chu and Haijing Ren in Journal of Holistic Nursing
Footnotes
Acknowledgments
We thank the participants in this study.
Ethical Considerations
This study was approved by the Medical Ethics Committee of Hebei University Affiliated Hospital. Written informed consent was obtained from all participants prior to interviews, explaining the study objectives, confidentiality measures, voluntary participation, and right to withdraw at any time without affecting their care. Anonymity and confidentiality were maintained throughout the study.
Consent to Participate
Written informed consent was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declarations of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The data presented in this study are available from the corresponding author upon reasonable request, due to privacy and ethical restrictions on sharing raw interview transcripts. All authors have read and agreed to the published version of the manuscript.
Declaration on the Use of Artificial Intelligence
This manuscript was written by the authors. Artificial intelligence tools (such as Chat GPT) were used solely for language translation, grammar checking, and polishing of the English text. No AI-generated content was used to create original ideas, analyses, or interpretations. All intellectual contributions, including conceptualization, data analysis, and conclusions, are those of the authors. The raw data (interview transcripts and audio recordings) generated and analyzed during the current study are not publicly available due to ethical restrictions and the need to protect participant confidentiality and anonymity as per the approval of the Medical Ethics Committee of a tertiary Class A hospital in Hebei Province. Deidentified excerpts or summaries of the data may be made available from the corresponding author upon reasonable request, subject to approval by the ethics committee and in compliance with applicable data protection regulations.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.