
Abstract
Introduction
Nurses often work in contexts characterized by high levels of ethical, psychological, and physical demands, particularly during periods of widespread health crises. As frontline healthcare providers, they face burdensome workloads, moral distress, and personal risks, all of which influence job commitment and overall well-being (Bruyneel et al., 2021; Lin et al., 2025). Prolonged exposure to suffering and death has been associated with symptoms such as depression, anxiety, and sleep disturbances among nurses (Rourke et al., 2024). These stressors also contribute to increased turnover intention and fatigue (Özkan, 2022).
Spirituality is a significant resource for meaning-making, yet it can also give rise to religious and spiritual struggles (RSS) when personal beliefs conflict with clinical realities. Even in adversity, it enables nurses to maintain compassion, give meaning to suffering, and foster hope (De Diego-Cordero et al., 2022). Spirituality also provides an inner coping mechanism through which nurses can transcend current adversity and connect their practice to higher levels of personal and professional ideals (Sawyer & Bailey, 2022). Nurses may experience distress, burnout, or a diminished sense of purpose when these spiritual and moral dimensions are disrupted, for example, by moral injury or spiritual struggle. This weakens the caring relationship (Griffin et al., 2019; Taylor et al., 2024). On the other hand, spirituality can lead to positive transformation through post-traumatic growth and a renewed sense of fulfillment in one's career when it is fostered and articulated in a caring environment (Atashzadeh-Shoorideh et al., 2025).
The Philippines is one of the most religious countries in Asia, with more than 90% of the population identifying with an organized religion, predominantly Roman Catholicism, followed by Protestant Christianity and Islam (Philippine Statistics Authority, 2020). Religious faith is deeply embedded in Filipino cultural identity and often shapes moral reasoning, coping practices, and professional values (del Castillo & Alino, 2020; Labrague et al., 2016). For Filipino nurses, spirituality frequently serves as both a personal resource and a professional lens through which suffering, duty, and ethical conflict are interpreted (Labrague et al., 2016; Mangcucang, 2023). These cultural characteristics suggest that spirituality may interact with work stressors in ways that differ from findings reported in more secular contexts (Taylor et al., 2023).
Spirituality has consistently been shown to be related to positive work-related outcomes across multiple cultural contexts. For example, Chiang et al. (2016) found that nurses with higher levels of spirituality demonstrated a greater commitment to their work and a more optimistic attitude toward care. Similarly, Fradelos et al. (2022) found that spirituality and workplace spiritual support are associated with greater job satisfaction and caring behaviors among nurses in hospitals. Spirituality has been associated with lower levels of stress and burnout (Putri et al., 2022) and with greater post-traumatic growth and psychological well-being (Rogers et al., 2022), especially during periods of widespread health crises. Additionally, institutional policies that support nurses’ spiritual well-being help stabilize emotional states and foster long-term work commitment (Alquwez et al., 2022).
However, spirituality in nursing can sometimes manifest as struggle or distress, particularly when clinical realities conflict with the nurse's moral or religious convictions. This is known as moral injury, an intense psychological conflict that originates from acts or omissions that contradict one's moral convictions (Griffin et al., 2019; Mantri et al., 2020). Studies from various contexts have identified religious or spiritual struggles (RSS) and moral injury as powerful predictors of burnout and intention to leave among nurses (Taylor et al., 2023; Atashzadeh-Shoorideh et al., 2025; Gherman et al., 2025). Essentially, these studies highlight the complex role of spirituality in shaping both vulnerability and adaptive responses in nursing practice.
Faith and spirituality are commonly used as coping strategies and sources of purpose in work for Filipino nurses (Labrague et al., 2016). However, no empirical study has examined how spirituality within the Filipino context influences nurses’ work-related outcomes, such as burnout, moral injury, job satisfaction, and turnover intention. This gap hinders a comprehensive understanding of how spiritual well-being might be leveraged as both a protective factor and a resource for development among Filipino nurses.
Aims of the Study
This study aims to examine the relationships among dimensions of spirituality, specifically religious and spiritual struggle, moral injury, and post-traumatic growth and selected work-related outcomes, including burnout, job satisfaction, and turnover intention, among Filipino nurses. By analyzing these relationships, the study seeks to contribute to holistic nursing science by situating spirituality as a core dimension of nurses’ work experience.
Theoretical Framework
This study is grounded in a holistic nursing perspective, which views individuals as integrated beings whose health arises from the interaction of physical, psychological, social, and spiritual dimensions (Dossey & Keegan, 2016). Within this perspective, spirituality is a core domain shaping how nurses interpret suffering, respond to ethical challenges, and sustain caring relationships. Guided by Watson's (2008) Theory of Human Caring, nursing is understood as a moral and relational practice grounded in the unity of mind, body, and spirit, where caring consciousness and meaning-making enable nurses to maintain compassion and purpose despite adversity.
From a holistic nursing perspective, spirituality is not merely a supportive resource or coping mechanism but a fundamental dimension of the nurse as a whole person, inseparable from the integration of mind, body, and spirit (Dossey & Keegan, 2016; Watson, 2008). Within this view, nurses’ experiences of practice, including burnout, job satisfaction, and intention to remain in the profession, are not simply occupational outcomes but expressions of the degree of coherence or disruption within this integrated wholeness. Experiences such as moral injury and religious or spiritual struggle may reflect fragmentation in meaning, values, and identity, whereas post-traumatic growth reflects processes of integration, renewal, and deeper engagement in caring-healing relationships (Taylor et al., 2024; Tedeschi & Calhoun, 1996). Framing spirituality in this way shifts the focus from examining isolated variables to understanding the nurse's lived experience as a unified, meaning-seeking being, thereby advancing holistic nursing knowledge.
Within this framework, moral injury, religious and spiritual struggle, and post-traumatic growth are understood as interrelated expressions of the nurse's spiritual experience. Moral injury reflects violations of deeply held moral values that disrupt ethical integrity, while spiritual struggle encompasses conflicts in meaning, belief, and connection with the transcendent (Griffin et al., 2019; Exline et al., 2014). In contrast, post-traumatic growth represents a process of meaning reconstruction and reintegration following adversity (Tedeschi & Calhoun, 1996). Together, these constructs provide a coherent basis for examining how spirituality shapes work-related outcomes, including burnout, job satisfaction, and turnover intention.
Methods
Design
This research utilized a quantitative, cross-sectional, observational design.
Participants and Setting
Convenience sampling was employed to recruit study participants. Participants were Registered Nurses providing direct patient care in public and private hospitals in Metro Manila, Philippines, who provided care for patients with COVID-19. Nurses in purely administrative roles or without direct patient contact were excluded. After securing official permission from the respective hospital nurse leaders, the researchers coordinated with unit heads to facilitate participant recruitment.
G*Power software, version 3.1, was used to perform an a priori power analysis. The calculation anticipated the use of regression analyses, achieving a medium effect size (d = 0.30), and an alpha of 0.05. The findings indicated that to achieve a power of 0.95, a sample size of 138 individuals was required.
Data Collection Procedure
Data were collected from May to July 2022 during the COVID pandemic. Data collection was conducted by distributing paper-and-pencil questionnaires directly to nurses who met the inclusion criteria and were willing to participate. No electronic recruitment methods (e.g., email or online surveys) were used. After obtaining written informed consent, participants were given 15 min to complete the questionnaires on the ward. Participants were instructed to return completed questionnaires directly to the researchers.
Research Instruments
The researchers used several psychometrically valid and reliable instruments to measure the study variables. In addition, some unvalidated items were used to collect personal and work-related information.
The
The
The
The
Copenhagen Burnout Inventory: Work-Related Burnout (CBI-WRB)
While the CBI comprises three distinct subscales for assessing burnout (personal, work-related, and client-related), this research used 6 items from the work-related burnout subscale (Kristensen et al., 2005). Response options include 5-point Likert scales (from 1 = always, to 5 = never). It is important to note that higher scores on the Copenhagen Burnout Inventory (CBI) indicate lower burnout, whereas lower scores indicate higher burnout. In this study, the Cronbach's alpha was 0.81.
The Turnover Intention Scale (TIS)
A three-item subscale from the TIS assessed the extent to which nurses consider leaving their profession. Response options ranged from 1 (strongly disagree) to 5 (strongly agree). Items were summed to create a total score; higher scores suggest a greater likelihood of leaving nursing (Cohen, 1999). In this study, the Cronbach's alpha was 0.86.
Demographic Profile Sheet
Demographic factors, including age, sex (male, female), religion (Roman Catholic/Christian), hospital type (private/public), frequency of providing care to patients presumed to have COVID-19, and years of nursing experience, were collected using questions developed by the researchers.
Data Analysis
Data were entered into Microsoft Excel prior to analysis. Then, JAMOVI version 2.4.14 (https://www.jamovi.org/) was used to analyze the data. Responses with missing data were excluded prior to analysis; therefore, the final dataset contained no incomplete cases, and no data imputation was required.
The Shapiro-Wilk and Kolmogorov-Smirnov tests were used to assess normality, and the results indicated that all variables were normally distributed (ps > .05). First, to understand each variable and characterize the sample, a variety of descriptive statistics were used, including frequencies, means, and standard deviations. Then, Pearson's correlation was used to assess relationships among the continuous variables, and multiple regression was used to determine their associations.
Ethical Consideration
Ethical approval was obtained from the San Beda University Research Ethics Board (SBU-REB No. 2021-021) prior to data collection. Participation in the study was entirely voluntary, and no form of coercion was used. Eligible participants were provided with a detailed explanation of the study's purpose, procedures, potential risks, and benefits before participation. Written informed consent was obtained from all participants. Participants were informed of their right to withdraw from the study at any point without penalty. Given the sensitive nature of topics such as moral injury and spiritual struggle, safeguards were implemented to ensure psychological safety, including conducting data collection in a non-threatening environment and informing participants that they could skip any questions that caused discomfort. Confidentiality and anonymity were strictly maintained throughout the study. No identifying information was collected, and completed questionnaires were coded to ensure participant anonymity. All data were securely stored and accessible only to the research team.
Results
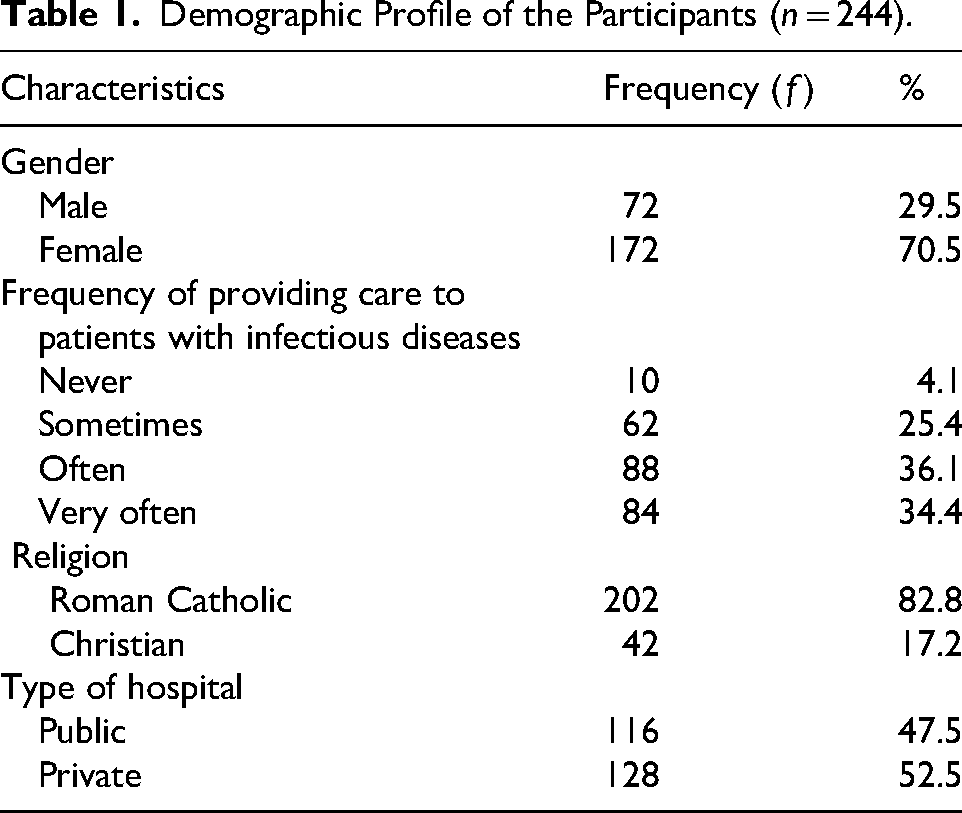
Table 1 summarizes the demographic and work-related characteristics of the study participants. The sample consisted of female nurses (70.5%), fairly young (M = 34.2 years ± 7.68), yet with considerable work experience (M = 8.02 years ± 6.45). All self-identified as Christian, mostly Roman Catholic.
Demographic Profile of the Participants (n = 244).
Spirituality and Work-Related Outcomes
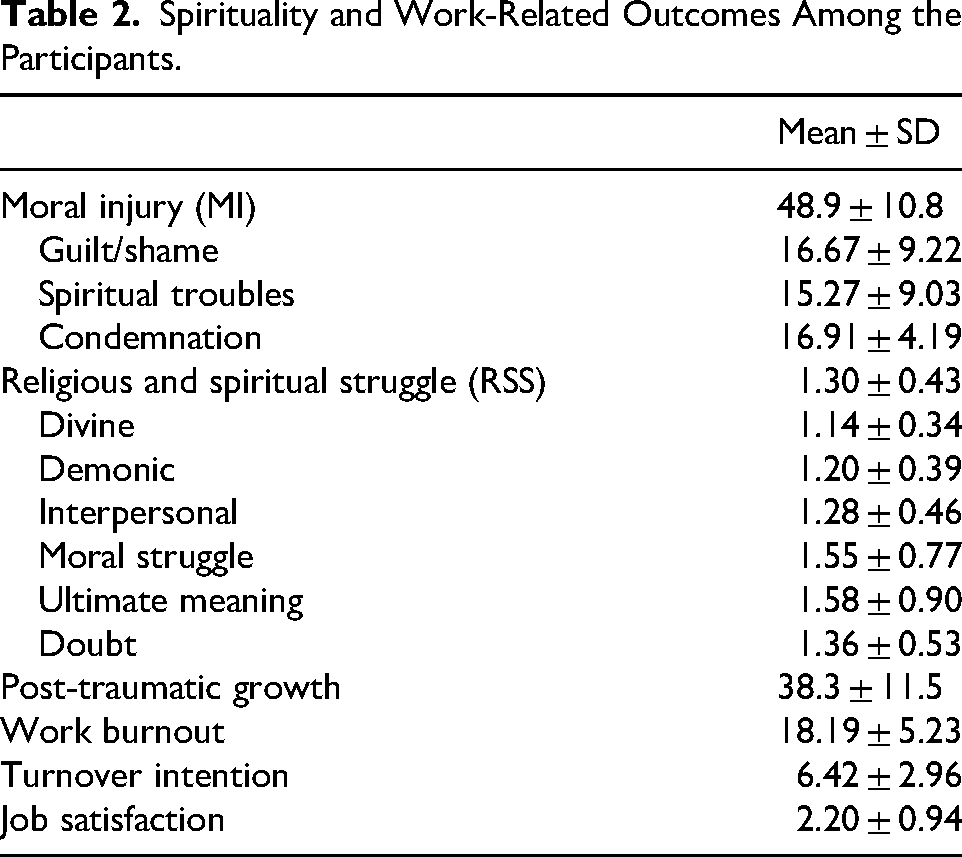
Table 2 presents the descriptive statistics for spirituality-related variables and work-related outcomes. Participants demonstrated clinically significant levels of moral injury, with mean scores exceeding the established cutoff as well as moderate to high post-traumatic growth. Although overall religious and spiritual struggles were low, struggles related to moral concerns and meaning-making were the most frequent. Work-related outcomes indicated that this sample reported moderate burnout and turnover intention, as well as moderate job dissatisfaction.
Spirituality and Work-Related Outcomes Among the Participants.
The Relationships Among Work Outcomes
Table 3 presents the key relationships among spirituality-related variables and work outcomes. Moral injury and spiritual struggle were positively associated with turnover intention and job satisfaction. However, both variables demonstrated significant negative correlations with burnout scores (r = −.278 and r = −.246, respectively). Because higher scores on the Copenhagen Burnout Inventory reflect lower burnout, the negative correlations indicate that higher moral injury and spiritual struggle are associated with higher levels of burnout. On the other hand, post-traumatic growth was negatively associated with job satisfaction and turnover intention and was not significantly associated with burnout.
Relationships Among the Work Outcomes.
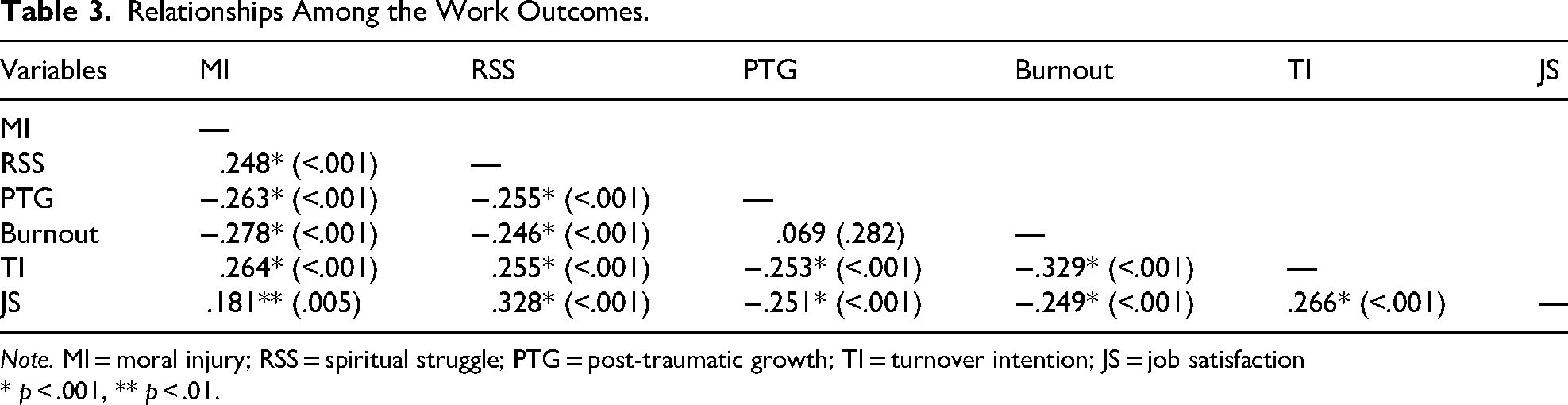
Note. MI = moral injury; RSS = spiritual struggle; PTG = post-traumatic growth; TI = turnover intention; JS = job satisfaction
* p < .001, ** p < .01.
Multivariate Analysis
The multivariate linear regression determined how job satisfaction (JSS), moral injury (MISS-HP), spiritual struggle (RSS 14), post-traumatic growth (PTGI), and burnout (CBI-WRB) were predicted by demographic and work-related outcomes, including age, gender, religion, hospital type (private/public and faith/non-faith based), primary work setting, area of assignment, working hours per week, and years of experience (Table 4). The overall model (M1) significantly improved the intercept-only model (M0) across all outcomes, including PTGI (F = 1.896, p = .047), CBI-WRB (F = 2.144, p = .022), RSS 14 (F = 4.154, p < .001), MISS-HP (F = 1.983, p = .036), and JSS (F = 2.352, p = .012). These findings suggest that variations in spiritual responses and work outcomes are partly associated with demographic and workplace characteristics
Multivariate Analysis of Work-Related Outcomes With the Profile of the Participants.
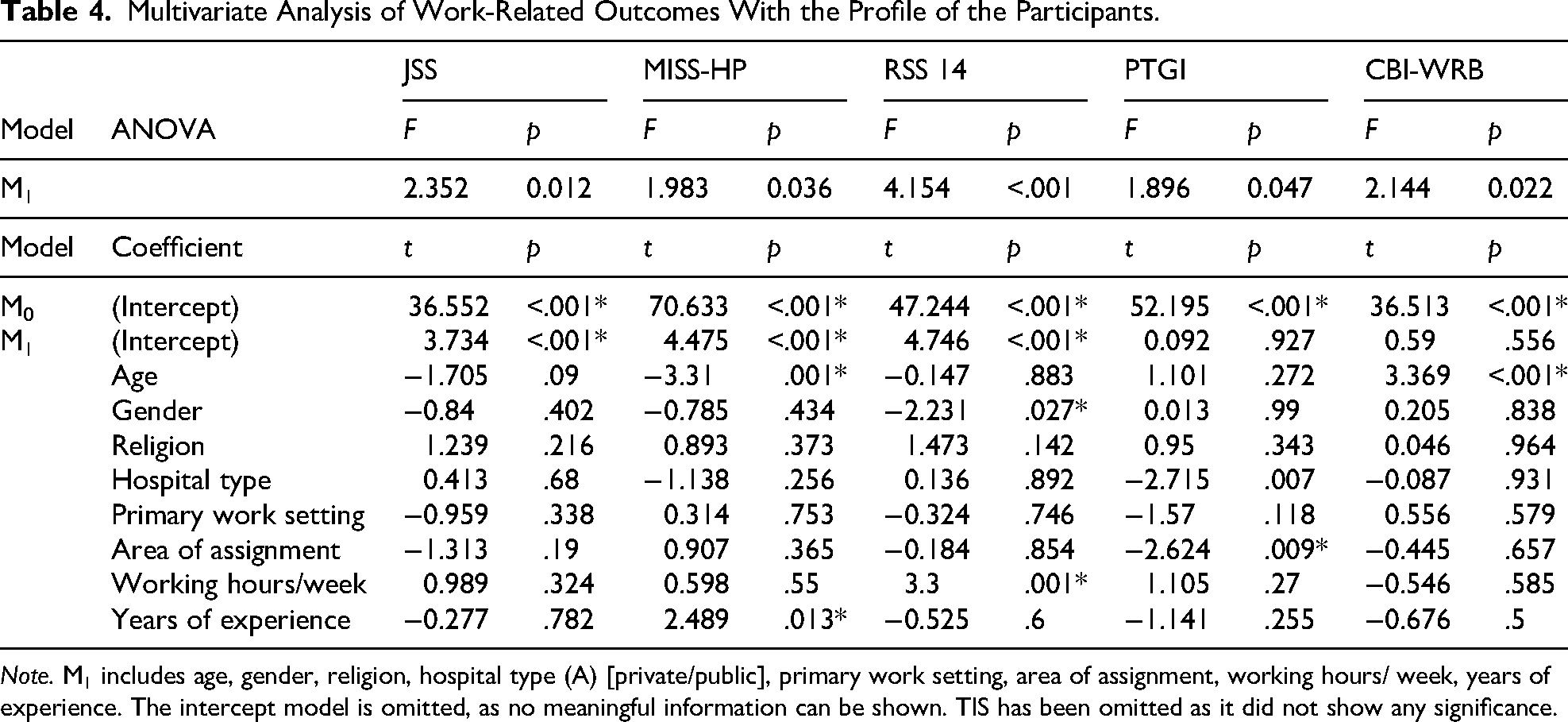
Note. M1 includes age, gender, religion, hospital type (A) [private/public], primary work setting, area of assignment, working hours/ week, years of experience. The intercept model is omitted, as no meaningful information can be shown. TIS has been omitted as it did not show any significance.
Older nurses tended to report lower levels of moral injury, suggesting that life experience may contribute to the development of moral resilience over time. Nurses working longer hours reported higher levels of spiritual struggle, indicating that sustained exposure to demanding work conditions may intensify existential or meaning-related concerns. Nurses in public hospitals demonstrated higher levels of post-traumatic growth compared to those in private settings, suggesting that contextual or organizational factors may influence opportunities for meaning-making and adaptation. Burnout was higher among older nurses, indicating that prolonged exposure to occupational demands may accumulate over time and affect well-being.
Discussion
Two key findings emerged: nurses reported high levels of moral injury alongside moderate post-traumatic growth, and spirituality-related variables were associated with burnout, job satisfaction, and turnover intention. These findings position spirituality as an integral dimension of nurses’ experiences, reflecting processes of fragmentation and integration.
The Spirituality and Work-Related Outcomes Among the Participants
This study found that Filipino nurses reported high levels of moral injury alongside moderate post-traumatic growth (PTG), reflecting patterns also observed in international contexts (Atashzadeh-Shoorideh et al., 2025). Moral injury, arising from violations of moral beliefs and professional values, is often linked to ethically challenging work conditions such as resource scarcity and frequent exposure to suffering (Griffin et al., 2019; Taylor et al., 2024). At the same time, the presence of PTG indicates that nurses may experience positive psychological and spiritual transformation despite moral distress (Tedeschi & Calhoun, 1996; Wang et al., 2024). Together, these findings suggest that distress and growth can coexist within nurses’ experiences.
This dual pattern reflects the inherently paradoxical nature of spirituality, which encompasses both struggle and transformation. When deeply held beliefs and meaning systems are challenged, distress may arise, yet such disruption can also catalyze growth and meaning reconstruction (Hart et al., 2020; Tedeschi & Calhoun, 1996). Moral injury and spiritual struggle reflect disruptions, whereas post-traumatic growth reflects processes of reintegration, enabling nurses to restore meaning, sustain caring relationships, and re-engage in practice with renewed purpose (Watson, 2008; Mantri et al., 2020; Taylor et al., 2024).
The Relationships Among Work Outcomes
These relationships can be understood within a conceptual continuum in which moral injury and spiritual struggle represent forms of disruption, while post-traumatic growth reflects processes of reintegration and transformation. Rather than linear associations between discrete variables, the findings reflect patterns. Although several associations were statistically significant, their small to moderate magnitudes suggest they should be interpreted as meaningful tendencies within complex clinical realities rather than as deterministic effects.
Moral injury and spiritual struggle signify disruptions in meaning, connection, and moral coherence, reflected in patterns of disengagement such as increased turnover intention, with more complex relationships observed for burnout (Dean et al., 2019; Taylor et al., 2024). In contrast, post-traumatic growth reflects the restoration of meaning and spiritual alignment, manifested in renewed engagement and sustained commitment to nursing (Tedeschi & Calhoun, 1996; Wang et al., 2024).
Caring-healing relationships are sustained not only through technical competence but through the nurse's spiritual integration. When this integration is disrupted, authentic engagement may be diminished; conversely, spiritual coherence enables sustained transpersonal caring relationships (Dossey & Keegan, 2016).
Some findings were counterintuitive, particularly the positive associations between spiritual struggle and job satisfaction. This may reflect spiritual struggle as a meaning-making process rather than solely a form of distress (Exline et al., 2014; Taylor et al., 2024). Additionally, the negative association between post-traumatic growth and job satisfaction should be interpreted with caution, given potential contextual influences and the use of a single-item measure.
Within the Filipino context, spirituality is deeply embedded in cultural identity and may shape how nurses interpret adversity. Experiences of moral injury and spiritual struggle may therefore reflect ongoing moral discernment, while also enabling the coexistence of distress and purpose. This cultural lens may help explain how nurses sustain meaning and engagement despite challenging conditions.
Overall, the findings highlight that (1) spiritual distress is associated with disengagement outcomes, (2) post-traumatic growth is associated with professional engagement, and (3) distress and growth may coexist within the nurse's experience.
Association of Work-Related Outcomes and the Demographic Profile
Results from this study demonstrate that work-related and demographic factors collectively shape nurses’ psychological well-being and professional outcomes. Age, sex, years of experience, working hours, and institutional type were associated with job satisfaction, moral injury, spiritual struggle, post-traumatic growth, and burnout, supporting prior findings that nurses’ experiences are embedded within organizational and structural contexts rather than solely individual factors (Khatatbeh et al., 2022).
The inverse relationship between age and moral injury suggests that older nurses may develop moral resilience through experience and reflection, while the positive association with years of experience indicates the cumulative impact of chronic moral stressors (Dean et al., 2019; Rabin et al., 2023). Similarly, longer working hours were associated with higher levels of spiritual struggle, highlighting how sustained exposure to demanding conditions may intensify meaning-related concerns, particularly in the absence of adequate recovery and support systems.
Institutional context also influenced adaptation. Nurses in public hospitals reported higher post-traumatic growth, possibly reflecting greater opportunities for peer support, collaboration, and collective meaning-making in resource-constrained environments (Azoulay et al., 2025). At the same time, higher burnout among older nurses aligns with evidence that prolonged exposure to occupational demands can accumulate and affect well-being over time (Hatch et al., 2018).
From a holistic nursing perspective, these findings underscore that nurses’ spiritual and professional experiences emerge from the dynamic interplay of personal, relational, and organizational factors. Spirituality, therefore, is not a static attribute but a context-dependent process shaped by workplace conditions, reinforcing the need for environments that support reflection, connection, and meaning-making.
Limitations of the Study
Although this study provides informative evidence on the impact of spirituality on work-related outcomes among Filipino nurses, several limitations should be considered. Firstly, the cross-sectional design of the study limits the extent to which causality inferences can be drawn. Longitudinal or experimental research is required to ascertain whether spirituality has a direct or interactive effect over time on these work outcomes.
Second, the results may not be as broadly applicable as they appear, given the convenience sample from Metro Manila hospitals. Nurses who work in rural or specialized care settings, or in private vs. public institutions, may have different experiences with moral injury, religious and spiritual struggle, and post-traumatic growth. To account for regional, institutional, and cultural variances, future studies should use a more varied national sample.
Third, the study used only self-report measures, which are susceptible to biases such as self-perception bias, acquiescence, and social desirability. Despite the use of established and standardized questionnaires, it is possible that participants underreported sensitive experiences such as moral injury or spiritual struggles. Future studies could deepen their understanding of the lived experiences by conducting qualitative interviews or focus groups.
Fourth, data were collected during a later stage of the COVID-19 pandemic marked by both adaptation and residual uncertainty (i.e., May to July 2022). As a result, the observed associations might reflect organizational and psychological factors unique to the pandemic. The stability of these correlations over time might be ascertained by repeating the regression study in non-crisis circumstances.
In addition, responses with missing data were excluded prior to analysis, resulting in a complete-case dataset. Although this approach ensures analytic clarity, it may introduce bias if the excluded responses systematically differed from those included. Furthermore, job satisfaction was measured using a single-item scale, which, while commonly used in large-scale nursing studies for its efficiency and face validity, may not capture the multidimensional nature of job satisfaction as comprehensively as multi-item instruments. Future research may benefit from using more robust measures and exploring potential differences between complete and incomplete cases.
Implications for Holistic Nursing Practice and Research
Findings show that nurses’ professional experiences are shaped not only by psychological and organizational factors but also by the processes of spiritual distress and growth.
To begin to address nurse moral injury and spiritual struggle, nurses may be supported to complete a validated spiritual assessment such as the RSS (Exline et al., 2014) or clinical acronym FICA (i.e., whether there is Faith, degree of Importance of spirituality, faith Community, desire to Address spiritual needs) (Puchalski et al., 2014) to enable early identification of spiritual struggle and moral distress. Interventions such as reflective debriefing, narrative reflection, and ethics rounds may support nurses in processing morally challenging experiences and restoring alignment between values and practice (Dean et al., 2019; Rabin et al., 2023). Access to spiritual support services and peer support may further sustain nurses’ spiritual integrity (Sawyer & Bailey, 2022).
To foster post-traumatic growth, meaning-centered strategies such as reflective journaling, mentorship, and resilience-building initiatives can help nurses transform adversity into opportunities for personal and professional development (Tedeschi & Calhoun, 1996; Rogers et al., 2022). At the organizational level, nurse leaders play a critical role in creating environments that support reflection, openness, and holistic well-being through supportive policies and staff development initiatives (Lee & Yu, 2023).
Overall, these findings highlight the importance of supporting the whole nurse—mind, body, and spirit—as a foundation for sustaining a resilient, compassionate, and engaged nursing workforce.
Conclusion
This study contributes to holistic nursing by demonstrating that spirituality is not merely a coping resource or a predictor of work-related outcomes, but a fundamental dimension of the nurse's being that shapes the experience of professional practice. The coexistence of moral injury, spiritual struggle, and post-traumatic growth reflects the dynamic processes of fragmentation and integration within the nurse as a whole person.
These findings suggest that outcomes such as burnout, job satisfaction, and turnover intention are not solely occupational indicators but expressions of the nurse's level of coherence, meaning, and connectedness. Supporting nurses, therefore, requires attention not only to external work conditions but also to the inner processes that sustain caring-healing relationships and authentic engagement in practice. By positioning spirituality at the center of the nurse's professional experience, this study advances a more integrative understanding of nursing as a relational, human, and deeply meaningful practice.
Footnotes
Acknowledgements
The authors would like to thank all the Filipino nurses who participated in this survey.
Ethical Approval and Informed Consent Statements
An ethical approval was obtained from the San Beda University-Research Ethics Board (SBU-REB) with Protocol No. SBU-REB No. 2021-021.
Author Contributions
Conceptualization: Gil P. Soriano, Elizabeth Johnston Taylor, and Kathyrine A. Calong Calong. Methodology: Gil P. Soriano, Brian A. Vasquez, Elizabeth Johnston Taylor, and Kathyrine A. Calong Calong. Software: Gil P. Soriano and Brian A. Vasquez. Formal analysis: Gil P. Soriano, Feni Betriana, Mars Ian A. Silud, Brian A. Vasquez, and Rheajane A. Rosales. Writing–original draft preparation: Gil P. Soriano, Mars Ian A. Silud, Rheajane A. Rosales, Feni Betriana, Kathyrine A. Calong Calong, and Elizabeth Johnston Taylor. Writing–review and editing: Gil P. Soriano, Brian A. Vasquez, Mars Ian A. Silud, Rheajane A. Rosales, Feni Betriana, Kathyrine A. Calong Calong, and Elizabeth Johnston Taylor. Project administration: Gil P. Soriano. All authors reviewed the manuscript.
Consent for Publication
Written informed consent for publication was obtained from all participants involved in the study.
Consent to Participate
Written informed consent to participate in the study was obtained from all participants involved in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy and ethical restrictions.