
Abstract
Childbirth is a significant event that brings physical, psychological, and social changes to the mother, her partner, and other family members (Carpinelli & Savarese, 2022; Diaz-Rojas et al., 2021; Foster et al., 2021; Martin et al., 2022; Van Vulpen et al., 2021). The perinatal period refers to this transition, starting in pregnancy and continuing after the child is born (Antoniou et al., 2022; Kaya et al., 2022). Stricter time frames of this period focus on 22 completed weeks of gestation to 7 completed days after birth (World Health Organization, 2025), while others refer to the start of pregnancy to 12 months postpartum (Antoniou et al., 2022; Ngai & Lam, 2021). In this period, the utilization of health care services is high in both uncomplicated and complicated pregnancies (Bellerose et al., 2022; World Health Organization, 2025). The World Health Organization (2000, 2025) strongly advocates for perinatal care to be holistic, addressing the full spectrum of physical, emotional, and social needs of women, their newborns, and their families. This aligns with the broader emphasis of the American Holistic Nurses Association (AHNA, 2019), to focus on care for the whole person, including body, mind, and spirit within their social and cultural context.
However, there is a complex balance in obstetric care (i.e., care concentrated on pregnancy, childbirth, and the postpartum period). This care often focuses on reducing medical risks and treating conditions within a biomedical model, whereas childbirth is often experienced as a natural and fundamentally existential event, linked to one's personal worldview (Hansen et al., 2021; Najafi et al., 2017). Medicalization of childbirth is associated with diminishing women's confidence in natural childbirth, increased cesarean section rates, and the fostering of passive acceptance of medical authority, particularly when it limits the continuous presence of midwives during labor and/or restricts their capacity to offer holistic care (Najafi et al., 2017). Holistic care supports whole-person care, which includes emotional, psychosocial, and spiritual dimensions, and facilitates shared decision-making (not treating perinatal women as passive patients) (Davis, 2021).
In the broader field of healthcare, it is recognized that individuals turn to religion or spirituality as a source of strength and relief (Britt et al., 2025; Jawaid, 2014; Lavric, 2024). To clarify these concepts, religion refers to an organized set of beliefs, rituals, and practices that are often shared within a community and relate to a deity or higher power, such as Christianity, Islam, Hinduism, and Buddhism (Bradford, 2023; Murgia et al., 2022). Spirituality is a broader term that refers to the universal human search for meaning, purpose, transcendence, and connection (Bradford, 2023). Spirituality can be expressed through beliefs, values, and practices (Bradford, 2023; Murgia et al., 2022). While religion is inherently spiritual, spirituality can exist independently of religious affiliation or institutional structures. Neither religion nor spirituality is commonly considered as part of holistic obstetric care. This review addresses this gap. The aim is to provide a comprehensive narrative review of the literature regarding the spiritual and religious dimensions of holistic perinatal care, thereby identifying key themes and implications for clinical practice.
The Biopsychosocial Model and the Integration of Spirituality in Perinatal Care
From a holistic paradigm, the Biopsychosocial-Spiritual (BPSS) model (Van Denend et al., 2022) and the Holistic Biopsychosocial Perspective (HBP; Page et al., 2020) serve as the guiding theoretical frameworks for this review. These models build on Engel's (1977) well-known biopsychosocial model, which offered a corrective to biological reductionism by viewing health and illness as a dynamic interaction among biological, psychological, and social factors (Van Denend et al., 2022). Despite a trend of declining religiosity, particularly in Western countries, many people have spiritual needs (Bradford, 2023; Umberger & Wilson, 2024; Van Denend et al., 2022).
The addition of spirituality to the biopsychosocial model stems from the understanding that health is closely linked to meaning, purpose, and transcendence. As explained by Page et al. (2020), research has revealed that religious or spiritual engagement is associated with better mental health, less stress, and better birth-outcomes (e.g., higher birth-weight). As such, the HBP integrates spirituality in the psychological and social domains (Page et al., 2020). Paul and Kalir (2025) have especially emphasized integration of religiosity/spirituality, explaining that it encompasses behaviors and practices that promote physical well-being, such as prayer and meditation, which may reduce stress and improve immunity. Psychologically, spirituality offers purpose and meaning in life, and support during times of challenge (Paul & Kalir, 2025). Socially, spirituality reinforces interpersonal connection and support from one's community (Page et al., 2020; Paul & Kalir, 2025).
The BPSS model goes one step further and recognizes spirituality as a distinct, but interconnected, domain (Van Denend et al., 2022). The BPSS model describes a dynamic interaction between biological, psychological, social, and spiritual factors (Umberger & Wilson, 2024). This means that one's physical condition (biological), emotional and cognitive processes (psychological), social environment and relationships (social) and one's meaning, values and connection to the transcendent (spiritual) are all inextricably linked and contribute to one's overall experience and well-being (Bradford, 2023; Sulmasy, 2002; Umberger & Wilson, 2024; Van Denend et al., 2022). Both models emphasize the importance of spirituality for holistic nursing (Van Denend et al., 2022; Page et al., 2020). As such, spiritual care is advocated as a clinical necessity: without addressing the spirit, the biological and psychological healing of the perinatal woman remains incomplete (Sulmasy, 2002; Van Denend et al., 2022).
This expanded understanding of religiosity and spirituality in the holistic approaches highlights the need for integrative care practices. Nurses and midwives can more effectively support their patients holistically by not only paying attention to physical and mental health, but also to spiritual well-being (Murgia et al., 2022). This strengthens respect for patients’ fundamental rights and beliefs and also harnesses the powerful, health-promoting aspects of spirituality and religiosity (Paul & Kalir, 2025). Research confirms that this also increases patient satisfaction (Rajabpour et al., 2019). However, while midwifery care is inherently grounded in a holistic philosophy, this care is provided in various settings (e.g., birthing centers or homes) and contexts, and midwives always need to operate within a specific professional scope of practice that balances clinical safety protocols with the support of the woman's emotional and spiritual autonomy (International Confederation of Midwives, 2021). Consequently, understanding how spirituality is integrated within these professional and environmental boundaries may inform improvements in person-centered perinatal care.
Implications for Knowledge, Research, and Practice
This critical narrative review aims to increase knowledge by providing an integration of what is currently known from the existing literature on the interface between religiosity/spirituality, and holistic perinatal care, as this domain is still often overlooked in mainstream obstetric discourse. A narrative literature review is a qualitative interpretive integration of findings from various sources to offer a comprehensive contextual understanding (Motevalli, 2025). This type of review was considered most appropriate for the present topic, given the multidimensionality of the topic and the identified need to provide a comprehensive overview and interpret but also critically evaluate the current state of knowledge (Ferrari, 2015; Siddaway et al., 2019). This work advances holistic nursing science by operationalizing the AHNA (2019) standards that call for care addressing body, mind, and spirit. For practice, the review provides guidance to nurses and midwives on how to incorporate spiritual assessment and support into their routines, thereby enhancing holistic care. This review can further clarify what empirical research is still needed to better inform practice and further validate theory. The following research questions were formulated to guide the literature review: What evidence is there about the inclusion of spiritual care on perinatal outcomes, such as psychological well-being, satisfaction with the birth experience, and stress reduction? What tools or methods are used to identify and support women's spiritual needs in perinatal care? How do nurses and midwives see their role in including the spiritual needs of their clients in care, and what strengths and barriers do they experience?
Method
A comprehensive and systematic literature search was conducted across several search engines, including PubMed, ScienceDirect, and Google Scholar. The latter (Google Scholar) was specifically included to ensure that doctoral dissertations could be included if relevant, besides peer-reviewed academic papers. The search terms included combinations of holistic care, spiritual care, religion, religiosity, spirituality, midwifery, perinatal care, pain management, biopsychosocial model, psychological coping, and perinatal mental health. Boolean operators (AND, OR) were used to truncate or expand the search (e.g., using spiritual OR religiosity to include papers that included either term). The inclusion criteria were (1) articles published between 2000 and 2025, that (2) addressed one or more of the following: the integration of spirituality or religiosity into perinatal or holistic care; the psychological impact of religiosity or spirituality on pain management during childbirth; the influence of spiritual beliefs on the childbirth experience; and the role of nurses and midwives in delivering holistic or spiritual care. The exclusion criteria were (1) topics different from perinatal care and spirituality; (2) the following formats: books, bachelor's/master's theses (conference) abstracts protocols; (3) resources only providing theory or protocols; (4) resources being too broad (mentioning spirituality and perinatal care, but focused on different topics).
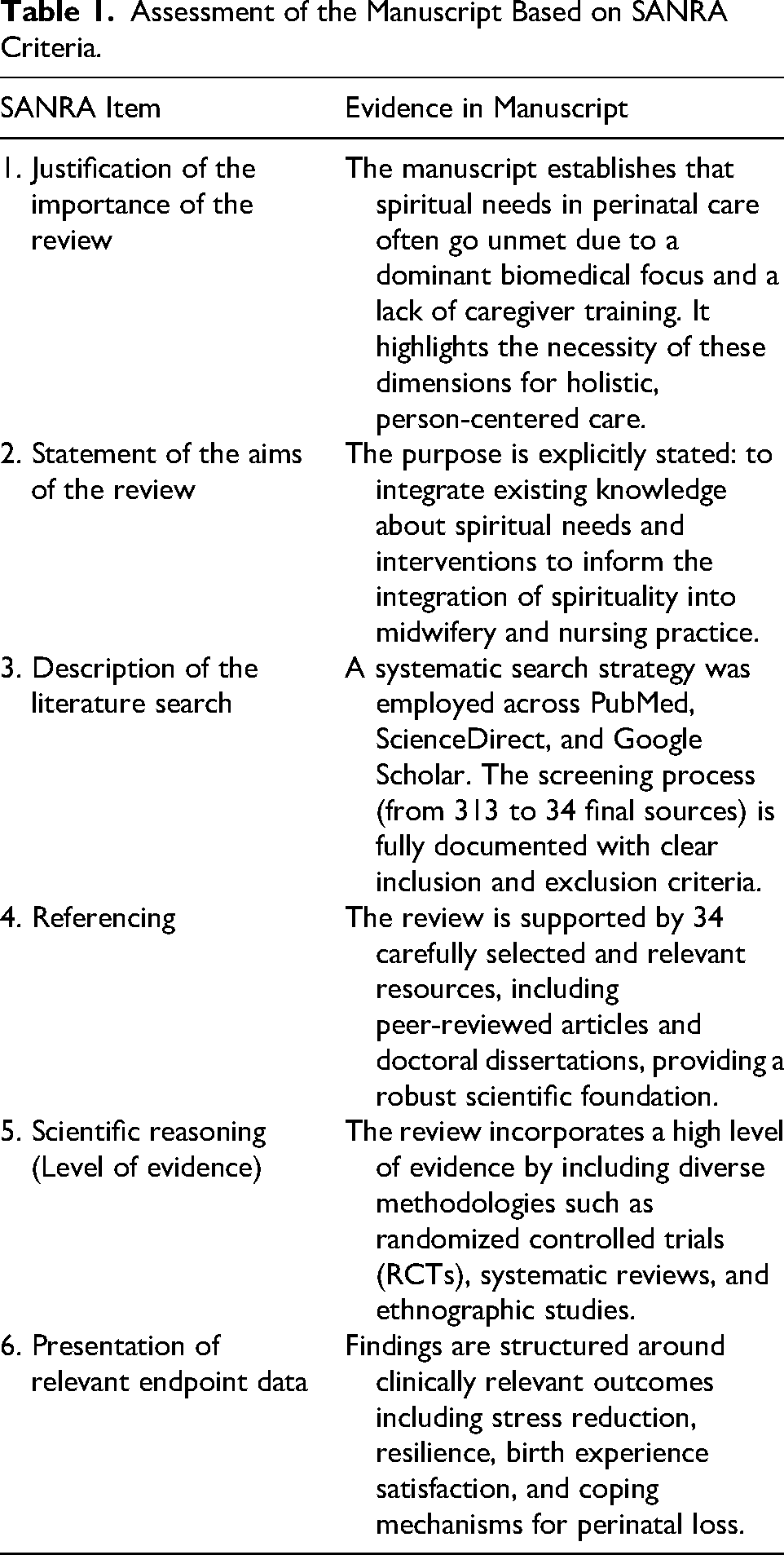
The findings of the selected references were synthesized using thematic analysis as described by Thomas and Harden (2008). The thematic synthesis was conducted by the first author and subsequently reviewed and confirmed by the second researcher. The researchers discussed the findings to ensure the themes accurately reflected the data, and a full consensus was reached on the final analytical framework. The process involved qualitative coding and creating descriptive and analytical themes to generate insights. To move beyond simple description, a higher-order framework was developed that addresses the holistic needs of parents, specifically focusing on resilience, clinical tools, and systemic barriers in hospital settings. To ensure scientific rigor and transparency, the review was prepared in accordance with the Scale for the Assessment of Narrative Review Articles (SANRA) criteria. SANRA is a validated six-item scale designed to assess the quality of non-systematic reviews, covering the importance and aims of the review, the literature search, referencing, and the presentation of evidence levels and endpoint data (see Table 1).
Assessment of the Manuscript Based on SANRA Criteria.
Ethical Considerations
This manuscript is based on a narrative review of published literature and did not involve human participants or primary data collection. Therefore, institutional review board approval and informed consent were not required.
Results
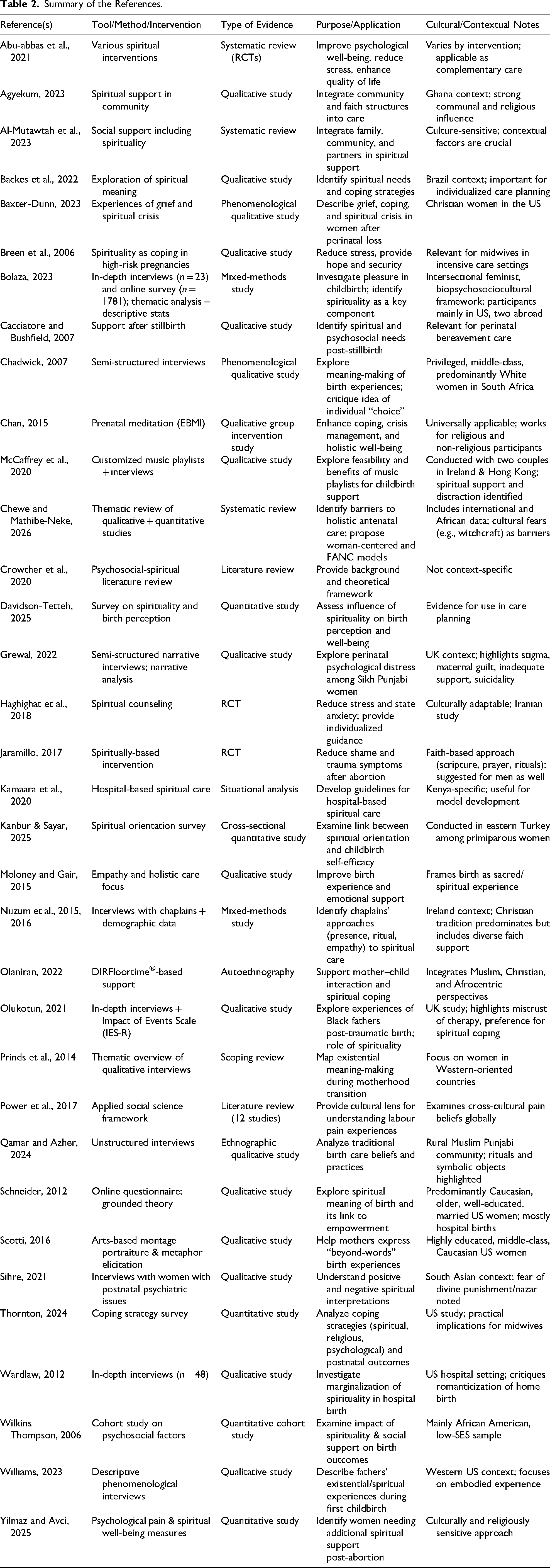
After deletion of duplicates (n = 12), there were 313 resources. Based on the titles, 139 of these resources were found to be irrelevant. All other resources were retrieved and further scanned (often abstract-based) to exclude sources based on their format and/or content, resulting in the deletion of 54 sources that were books, bachelor's/master's theses, or conference abstracts, and nine sources that were only theoretical or protocols. All other resources were read to make an adequate selection. A further 27 resources were found to be irrelevant as they did not provide information about the intersection of perinatal experiences with spirituality, and 50 were too broad, only mentioning this intersection as a sideline. It should be noted that some of the latter categories were books (e.g., on women's mental health) or conference abstracts and were missed in the earlier format screening. A final selection of 34 resources was used in the literature review. The references are summarized in Table 2.
Summary of the References.
Effects of Including Spiritual Care on Perinatal Outcomes
Spirituality Increasing Resilience
From the literature, spirituality emerges as very important for maternal well-being and stress reduction (Backes et al., 2022; Crowther et al., 2020; Davidson-Tetteh, 2025; Haghighat et al., 2018; Moloney & Gair, 2015). In an earlier literature review conducted by Crowther et al. (2020), it became clear that this is at least partly explained by spirituality being an important coping strategy for mothers. Spirituality gives them inner strength, comfort, and stability (Crowther et al., 2020). This was also evident in a qualitative study by Backes et al. (2022), in which Brazilian mothers explained that spiritual care provides them with inner peace, emotional support, and comfort, thereby relieving stress and worry. Two more recent studies further supported this, showing a significant relationship between this internal spiritual orientation and less anxiety during and after pregnancy in the USA (Davidson-Tetteh, 2025) and childbirth self-efficacy among Turkish pregnant women (Kanbur & Sayar, 2025). An Australian interview study by Moloney and Gair (2015) clarified the role the midwife can play in this: through empathy and spiritual care, they can contribute to an improved birth experience. In the randomized controlled trial study of (2018), spiritual counseling provided by Iranian midwives was indeed found to reduce state anxiety in comparison to a control group.
A US study by Thornton (2024) found that spirituality was not predictive of overall quality of life but was associated with a lower risk of postpartum depression. This suggests that spirituality may primarily serve as a protective factor, increasing resilience. This was also believed by Olaniran (2022), who conducted an auto-ethnography. She describes the use of spirituality as an intervention to reduce stress, anxiety, and depression. More specifically, Olaniran suggests increasing spiritual intelligence through secular spiritual practices of gratitude, contentment, and mindfulness. Several other studies support this idea. A literature review by Breen et al. (2006) focused specifically on high-risk pregnancies and found that spirituality is a primary coping mechanism for mothers dealing with the immense stress, anxiety, and uncertainty that this situation brings. Spirituality helps them experience a sense of security and hope (Breen et al., 2006). Nevertheless, spirituality is also found to contribute to the experience of childbirth as pleasurable, something that was found among a majority of 76.9% of the women in a study carried out among mainly US participants (Bolaza, 2023). This latter finding is important as it indicates that spirituality may positively impact women also when they are not experiencing problems or excessive stress.
A systematic review by Al-Mutawtah et al. (2023) further supported that spirituality and specific religious practices, such as prayer, help reduce stress and pain. However, Al-Mutawtah et al. (2023) also pointed out that certain religious interpretations may increase stress among some women instead. The work of Sihre (2021) explains this well. This study focused on the experiences of South Asian women who struggled with post-natal psychiatric illnesses. The women reported various faith-based perceptions, including feeling empowered by God and helped by prayer, but also feeling punished by God or afraid of negative spiritual experiences, such as nazar (the evil eye or black magic). When filtered through such negative religious coping, spirituality can thus sometimes increase stress and confusion. Spirituality was also found to sometimes act as a barrier to access to prenatal care, for example, that birth is experienced as a natural process not to be interfered with (Chewe & Mathibe-Neke, 2026).
As such, it seems important to match care to women's individual perceptions. It appears that interventions, such as spiritual counseling or training that helps women to experience spirituality positively and find support in their beliefs, generally have a positive impact (Abu-abbas et al., 2021; Haghighat et al., 2018). For example, a study by Chan (2015) used prenatal meditation as a way to help pregnant women cope with physical discomfort, improve their crisis management, and strengthen their social relationships. This resulted in spiritual empowerment: feeling connected, believing in oneself, and feeling at rest and peace (Chan, 2015).
It should also be emphasized that spirituality is not just important for the pregnant woman or mother. A phenomenological study among five fathers in the USA involved in the birth of their firstborn child confirmed it as a spiritual experience. While in a highly medicalized setting, the fathers described how they felt it was a spiritual experience creating life, which was seen as something bigger than themselves. It increased their sense of responsibility and made them more aware of life and death, while they experienced positive feelings that included relief and awe (Williams, 2023).
Spirituality and Perinatal Loss
While most studies focus on pregnant or post-partum women, spirituality seems of especial importance in the case of miscarriage or stillbirth. Cacciatore and Bushfield (2007) showed with a qualitative study that stillbirth is an intensely emotional experience that often leads to long-term grief symptoms. Not only psychosocial, but also spiritual support from family, friends, and healthcare providers was considered important for women to find meaning in the face of such an existential crisis (Cacciatore & Bushfield, 2007). It should be considered that, also in the context of therapeutic and elective abortion, women often experience psychological pain, and this is stronger as they experience lower spiritual well-being (Yilmaz & Avci, 2025). Abortion can take place for a variety of reasons, including fetal anomaly or maternal health risks, and women can feel sadness, helplessness, guilt, and suffering, making the spiritual meaning-giving highly relevant (Yilmaz & Avci, 2025).
Further, in a phenomenological interview study among eight US Christian women who suffered from different forms of perinatal loss (including ectopic pregnancy, miscarriage, stillbirth, and neonatal death), it became clear that they felt confused and often lonely in their process of grief (Baxter-Dunn, 2023). This spiritual struggle was often expressed through their religious framework; most people temporarily felt angry at God and/or lost their motivation to pray or attend church. In a later stage, however, this crisis evolved into a process of growth and deepened faith (Baxter-Dunn, 2023). These findings indicate that for women who experience perinatal loss, longer-term guidance to use spirituality positively, within or outside a formal religious context, may be helpful.
Cultural Differences in Experiences
The positive impact of spirituality is found cross-culturally, yet seems to be more recognized in non-Western studies and particularly in studies carried out among African diaspora populations. For example, Agyekum (2023) found that pregnant women in Ghana experience religious resources, such as faith, prayer, and the support of the church, as a powerful defense against severe mental symptoms (such as suicidal and infanticidal thoughts). This seemed even more important because urbanization decreased traditional social support (Agyekum, 2023). Further, Kamaara et al. (2020) found that most (about 80%) of Kenyan mothers of neonates felt a strong religious reliance, being dependent on God for power to deal with problems they faced. Wilkins Thompson (2006) found in a cohort study of 163 predominantly low-income African American women that higher spirituality was associated with greater social support during pregnancy, and that social support predicted higher infant birth weight. Similarly, a study carried out among Black fathers in the UK found that they relied mostly on their faith to process traumatic childbirth experiences, and this was strengthened by them feeling stereotyped and faced with culturally insensitive mental health support systems (Olukotun, 2021). While across different cultures, spirituality may act as a pathway to strengthen social connectedness, which in turn can positively affect birth outcomes, this may be specifically emphasized in African diaspora cultures. Afrocentrism tends to focus on communality and spirituality, often expressed through religious affiliation. This contrasts with more individualistic and secular visions that seem to prevail in many Eurocentric and Western studies (Power et al., 2017; Schneider, 2012). A review of Western studies shows that the transition to motherhood is often considered an existential and spiritual experience that makes women reflect on the meaning of life (Prinds et al., 2014). This indicates that while the form of expression (religious versus secular) varies by culture, the need for spirituality and spiritual guidance may be universal.
A culturally comparative literature review of previous qualitative studies focused on childbirth revealed that, in comparison to other cultures, for women in African cultures, pain during childbirth was experienced as part of a natural process, and women relied more on self-knowledge of their bodies (Power et al., 2017). In Asian cultures, too, religious practices, and especially prayer, are used to cope with pain during labor (Power et al., 2017). Power et al. (2017), however, also explained that a lack of pain education could make childbirth an experience where Asian women felt out of control. An ethnographic study in Pakistan (Punjab) found women used specific religious rituals, such as reciting prayers from the Quran (especially Surah Maryam), giving charity, and using sacred objects as a way to connect with the divine and reinforce spiritual hope for a safe and easy delivery (Qamar & Azher, 2024).
In European studies, trust in the body was often present, and women felt well-prepared (Power et al., 2017). However, spirituality was not mentioned explicitly, and while women felt pain could strengthen the bond with their baby, they were also reassured by the possibility of pain relief when necessary. More medicalized were the experiences reported by women in the US and South America. American women felt they had been prepared with an unrealistic, overly idealized picture of giving birth, and many chose an epidural, while in South America, instead, pain was emphasized and expected, and this often formed a reason for the medicalization of childbirth (Power et al., 2017).
From the cross-cultural comparisons, it appears that it is not so much having different spiritual and religious backgrounds that determines the extent to which parents can rely on spirituality during the perinatal period, but rather the cultural customs and focus. This was perhaps most clearly described by Chadwick (2007), who conducted a phenomenological study among privileged, middle-class White women in South Africa. These women, embracing a subculture of individualism and feminism, seemed to be so strongly shaped by the biomedical model that even among those who chose home delivery for a natural birth, their narratives still followed it (Chadwick, 2007). Their stories followed a clockwork script of centimeters and minutes, explicitly negating spirituality when asked about this. This suggests that the dominance of the biomedical model can overshadow spiritual meaning-making regardless of the birthing setting (hospital or home). In conclusion, the strongest positive feelings about spirituality seem to be shaped by a combination of considering childbirth as a natural process, being well-prepared, and cultural acknowledgment of spirituality.
These findings reinforce the holistic nursing principle that health encompasses body, mind, and spirit (AHNA, 2019). Nurses can integrate spiritual assessment and interventions into perinatal care plans to enhance resilience and reduce stress, thereby operationalizing holistic nursing standards.
Tools and Methods for Nurses and Midwives to Identify and Support Women's Spiritual Needs
Within this second theme, the tools and methods are addressed. The literature identifies several approaches to identifying and supporting women's spiritual needs, often in the form of integrative care practices, but also some structured interventions have been tested. Holistic nursing emphasizes presence, compassion, and spiritual support, including during times of profound grief (AHNA, 2019). These foundational nursing skills are applicable across all birthing environments (be it a hospital, birth center, or home) as they address the universal human search for meaning during the perinatal transition. In light of this, and the findings described supporting the importance of spirituality when faced with perinatal loss, a separate sub-section will describe the literature for this event.
Integrative Care Practices
In general, the literature demonstrates the importance of nurses and especially midwives’ empathy and attention to spiritual dimensions (Backes et al., 2022; Moloney & Gair, 2015). Several studies highlight the importance of leveraging community and organized religious support structures (Agyekum, 2023; Al-Mutawtah et al., 2023; Kamaara et al., 2020). Further, effective integration of spiritual care requires sensitivity to cultural, religious, and individual differences (Sihre, 2021; Yilmaz & Avci, 2025). According to Power et al. (2017), it is important for nurses and midwives to develop cultural competence. This means that they learn generalizations of preferences that are more common among women from different cultural backgrounds, yet prevent the development of stereotypes. The generalizations should only be used to inform what questions may be relevant and guide the interpretation of pain signals. For instance, understanding a woman's religious background can help a nurse identify specific rituals that provide spiritual comfort. Communication and an individualized approach are necessary to increase the control felt by women and reduce their fears. This seems to be especially relevant when seeing ethnic minority women, who may struggle with cultural barriers and can feel misunderstood (Grewal, 2022).
The literature also provides several methods to assess the individual women's spiritual needs. Structured assessment tools and interview guides can help midwives systematically identify spiritual needs regardless of the clinical setting. Examples include semi-structured interviews used in meditation programs (Chan, 2015) or questionnaires integrated into prenatal visits (Davidson-Tetteh, 2025; Thornton, 2024). Questions may explore beliefs, values, coping mechanisms, and preferred sources of spiritual support, providing a foundation for individualized care plans. Of interest to midwives may also be the spirituality self-report scale developed by Bennington (2010) that explicitly measures spirituality free from specific religious background and was found to positively associate with birth experience and maternal infant bonding among US mothers of babies (<1 year old). Scotti (2016) further demonstrated the merit of using montage portraiture and metaphor elicitation in a group of urban, highly educated women in the USA who had recently given birth to their first child. It seems that these more creative forms of expression helped them access the emotions and spirituality surrounding their experiences, which may be less easily captured by traditional conversation techniques.
(Complementary) Intervention
Where intervention studies have been carried out (including randomized controlled trials and qualitative studies), spiritual counseling is mostly used to reduce stress and state anxiety during pregnancy (Abu-abbas et al., 2021; Haghighat et al., 2018). Counseling sessions typically involve guided discussions on personal beliefs, values, and coping strategies, and can be delivered individually or in small groups. These interventions may enable women to identify sources of spiritual strength, practice mindfulness, and increase spiritual intelligence, supporting emotional resilience (Olaniran, 2022). It should be stressed that these strategies should be used in addition to education. For example, even while faith was an important coping strategy in the study by Agyekum (2023), education on mental health problems seemed necessary as well for women who seemed to suffer from problems such as depression (Agyekum, 2023). Similarly, education about childbirth and pain experiences seemed to be of importance for women cross-culturally to be prepared (Power et al., 2017).
Further, some complementary interventions are described. Prenatal meditation programs, such as the Eastern-Based Meditative Intervention (EBMI) developed by Chan (2015), offer structured methods for integrating spirituality into daily routines. The aim of using mindfulness is to increase coping with physical discomfort, strengthen social connections, and foster a sense of spiritual empowerment. More specifically, mindful breathing, body scans, self-affirmation, and reflective exercises on bio-psycho-social-spiritual aspects of pregnancy are strategies. Midwives can incorporate these practices into prenatal education or support groups. A small-scale study among two couples in Ireland and Hong Kong found that a customized music playlist helped find spiritual support (in this case, Christian music) around childbirth, although the use of music was encountered with resistance by medical staff (Cheung & McCaffrey, 2022).
Support for Perinatal Loss
An interview study among clergy in Ireland focused on the approach to spiritual care concerning stillbirth (Nuzum et al., 2015, 2016). It revealed the importance of being there, creating safe spaces for mourning, and the use of ritual acts (e.g., lighting candles, blessing ceremonies) to honor the loss. Although the study took place in a predominantly Christian context, the clergy adapted their care for families of different faiths. These strategies could also be used by midwives to support perinatal loss. From the phenomenological study by Baxter-Dunn (2023), it appears that midwives may no longer be involved once doctors and nurses are taking over the care, while they could be helpful in providing support. The women appeared to feel lonely and misunderstood, resulting in a long process of grief and sometimes the need for psychotherapy. What helped them, and may be supported by midwives, is knowing their grief and emotions are normal, including feeling angry at God; being able to let go of the question why it happened and replace it with a focus on what they can learn from the experience, and finding purpose, trust in a higher plan, even if it is difficult to understand. More concrete ways of coping were the use of rituals that were also mentioned in the study by Nuzum et al., and hope for an afterlife with the belief that they would see their babies again one day (Baxter-Dunn, 2023).
Further, it should be taken into consideration that spiritually based intervention may be effective in helping women after abortion. In a study by Jaramillo (2017), many women experience trauma and shame after abortion, and the elements used in the specific Rachel's Vineyard program that was investigated may be applicable more broadly. Women found that a supportive and confidential setting, sharing their stories and hearing other women's stories, learning from scripture of God's love, mercy, and forgiveness, praying, and grief exercises were most helpful. The latter included writing letters to their babies, naming them, and having a memorial service (Jaramillo, 2017).
These strategies reflect holistic nursing principles of caring and advocacy (AHNA, 2019). Nurses and midwives can support families through rituals, empathetic listening, and grief counseling, ensuring spiritual needs are met alongside physical and emotional care.
Experiences and Challenges in Addressing Spiritual Needs
Many midwives acknowledge the importance of spirituality for maternal well-being and coping (Backes et al., 2022; Crowther et al., 2020). They recognize that supporting women's spiritual needs can enhance emotional resilience, reduce stress, and improve the overall birthing experience (Moloney & Gair, 2015). Midwives report an empathetic approach, strong interpersonal skills, and the ability to create a safe, respectful environment, which facilitates spiritual care, are helpful in supporting perinatal women (Backes et al., 2022; Moloney & Gair, 2015). Access to structured programs, such as prenatal meditation or spiritual counseling initiatives, further strengthens their capacity to support women holistically (Chan, 2015; Haghighat et al., 2018).
The greatest barrier in providing spiritual support is the marginalization of spirituality and a holistic approach in hospitals (Wardlaw, 2012). Spirituality seems to be almost exclusively seen as possible in home births. In hospitals, the focus is on visible, decontextualized facts, creating a false dichotomy in which spiritual and medical care are seen as mutually exclusive (Cheung & McCaffrey, 2022; Moloney & Gair, 2015; Olaniran, 2022; Wardlaw, 2012). In several countries, hospital births have become normalized. For example, in the USA, a majority of more than 70% of young mothers had had a hospital birth, while they experienced it as a sacred event, and used prayer and faith (Schneider, 2012). This emphasizes a gap in needs and services as the prevailing biomedical environment often fails to align with the spiritual needs of perinatal women.
Further, cultural and religious diversity can make nurses and midwives uncertain about how to address spiritual needs appropriately (Sihre, 2021; Yilmaz & Avci, 2025). Associated with this is a lack of formal training in spiritual assessment and intervention (Al-Mutawtah et al., 2023; Crowther et al., 2020). Strategies to overcome these barriers include formal education on spiritual care, integration of semi-structured spiritual assessments into prenatal visits, interprofessional collaboration with religious resources, such as chaplains or faith leaders, and culturally sensitive guidelines for practice (Agyekum, 2023; Davidson-Tetteh, 2025; Olaniran, 2022).
Barriers to spiritual care highlight systemic gaps in implementing holistic nursing standards (AHNA, 2019). Nurses can advocate for institutional policies that integrate spiritual care, pursue continuing education, and collaborate across disciplines to ensure holistic perinatal support
Discussion
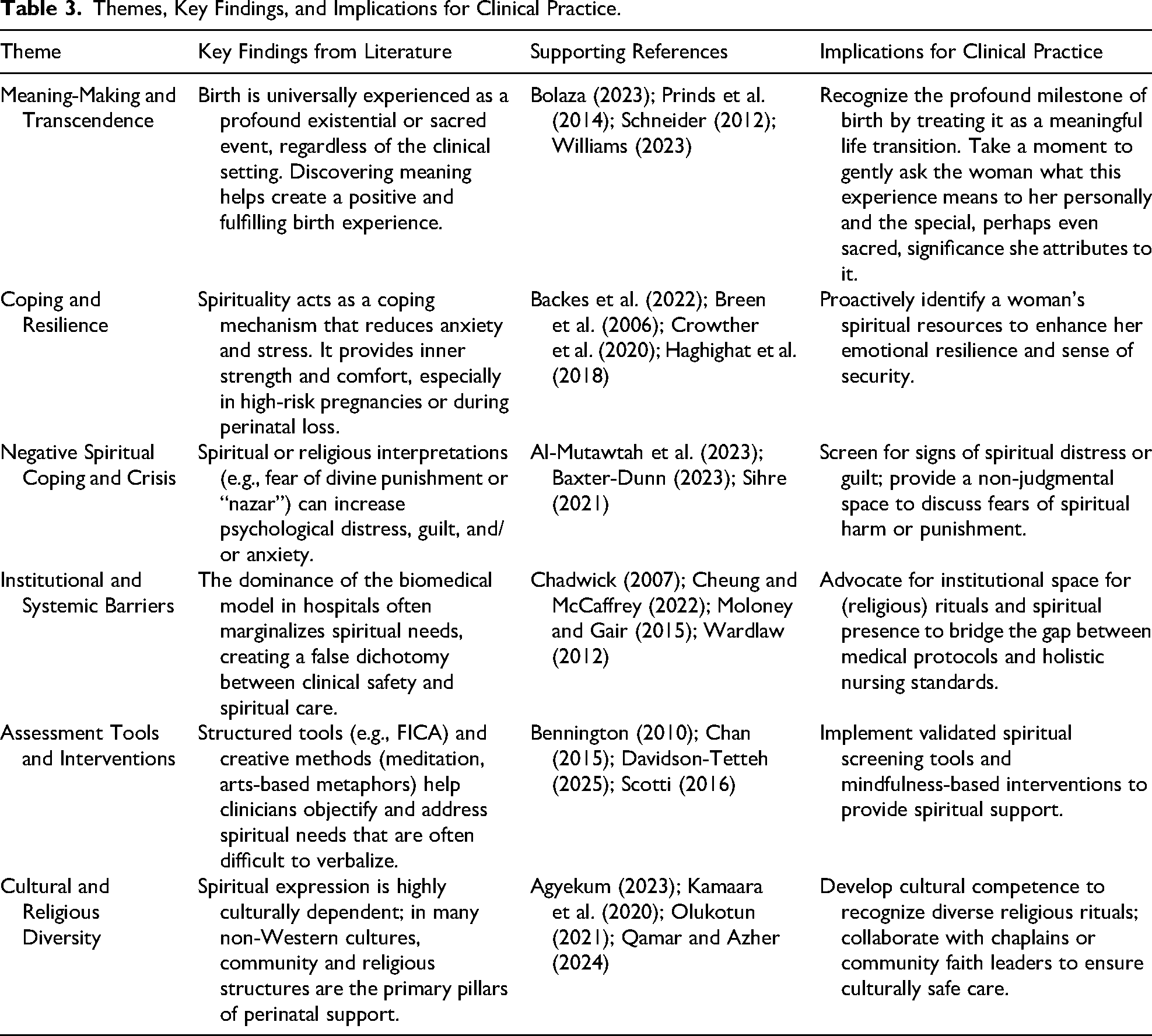
This critical, narrative literature was focused on holistic perinatal care and specifically how spirituality can be integrated. Table 3 summarizes the key findings of each theme, along with associated implications for clinical practice. A core finding of this review is that women seek more than the absence of complications; they seek a transformative experience. According to Moloney and Gair (2015) and Prinds et al. (2014), women pursue a sense of agency, connection (to the infant, partner, or a higher power), and the recognition of their transition into motherhood as a significant spiritual milestone. As such, providing spiritual care should not be considered as an optional, additional service but as a direct response to these needs. Research has demonstrated that the positive experience of spirituality in the perinatal period associates with better psychological health, less stress, and a higher quality of life (Abu-abbas et al., 2021; Haghighat et al., 2018). It offers women/mothers as well as their partners strength, hope, and a framework to make meaning of their experiences (Backes et al., 2022; Moloney & Gair, 2015; Williams, 2023). The importance of positive spiritual guidance was stressed by the finding that sometimes, certain religious interpretations can be stress-increasing (e.g., when women see their situation as a punishment from God or fear spiritual harm, such as nazar) or an overly exclusive emphasis on the natural or spiritual process leads to postponement of medical care (Qamar & Azher, 2024; Sihre, 2021). As such, the literature confirms the importance of spirituality was also theoretically emphasized by the BPSS model (Van Denend et al., 2022) and the HBP (Page et al., 2020).
Themes, Key Findings, and Implications for Clinical Practice.
These models align with holistic nursing principles and AHNA (2019) standards that call for care addressing body, mind, and spirit, regardless of the birthing environment. From the literature, practice to operationalize these standards and ensure person-centered, culturally sensitive care appeared as well. It became clear that it is important for midwives and nurses to develop cultural competence, delving into differences between cultural or religious groups, but keeping this only as a guide to delving into each individual (Grewal, 2022; Power et al., 2017). This can be done through questionnaires, interviews, but also possibly through more creative expressions, perhaps especially when women, from their cultural background, are less accustomed to making spirituality central and put into words (Chan, 2015; Scotti, 2016). In addition to integrating spirituality, more targeted interventions are possible in the form of mindfulness and other spiritual reflection exercises, including through rituals (Chan, 2015; Nuzum et al., 2015, 2016). This can strengthen coping strategies and resilience and make for a more pleasant perinatal experience (Abu-abbas et al., 2021; Haghighat et al., 2018; Olaniran, 2022).
What this study contributes to the literature is its emphasis on the perinatal experience as existential; It brings focus to life, especially to perinatal loss, an experience where spirituality is often seen as supportive (Baxter-Dunn, 2023; Cacciatore & Bushfield, 2007; Prinds et al., 2014). This validates the role of spirituality in making care more holistic rather than adopting the biomedical model (Hansen et al., 2021; Najafi et al., 2017; Wardlaw, 2012). In fact, the biomedical focus was the biggest barrier to providing holistic care identified in this study (Cheung & McCaffrey, 2022; Moloney & Gair, 2015). Nurses may lead a transformation by incorporating spiritual assessment tools, collaborating with faith leaders, and advocating for institutional policies that support holistic care. By doing so, holistic nursing would fulfill its commitment to promoting well-being and meaning during one of life's most profound transitions.
A second contribution is that where much previous research has focused on one culture or the comparison of a few, a more integrated comparison was possible. This made it clear that while spirituality can be part of perinatal care regardless of religion, there is already more room for it within some cultures than others (Kamaara et al., 2020; Olukotun, 2021; Power et al., 2017; Qamar & Azher, 2024). Moreover, it became evident that a one-sided focus on spirituality also brings possible negative effects (Al-Mutawtah et al., 2023; Sihre, 2021). It should be adapted to the individual, and accompanied by proper preparation and education (Agyekum, 2023; Power et al., 2017). In other words, holistic perinatal nursing requires actively tailoring spiritual care to individual needs and cultural contexts. Nurses and midwives need to balance respect for beliefs with evidence-based education to ensure safety and empowerment during the perinatal period.
The limitations of this literature review are the reliance on many qualitative studies that were carried out among small samples. This limits the generalizability of the results. Further, the use of English search keys may have resulted in overlooking studies in more cultures. It should also be noted that only a few studies have focused on interventions to increase focus on spirituality in perinatal care, and even fewer have focused on the experiences of midwives and nurses when trying to offer spiritual support. As such, future studies may include more quantitative methods, such as using surveys that address the findings of the present review to examine the extent to which they are recognized by individuals in different cultures. Moreover, future research may focus on the development of more interventions and their effects. Researchers may opt for the inclusion of more healthcare professionals, including midwives and nurses, but also doctors and gynecologists, who could potentially thwart spiritual support.
Finally, it is acknowledged that most studies focused on the hospital-based birthing model. As such, less is known about experiences in birth centers and home births, although Chadwick (2007) demonstrated the biomedical script can influence a woman's narrative even in the case of the latter (i.e., home birth settings). This limited focus does not seem accidental but rather reflects the biomedical model. In some cultures, medicalization extends further to the normalization of cesarean sections, where clinical efficiency may overshadow the spiritual transition of birth (Najafi et al., 2017). Comparative studies between physiological births and highly medicalized interventions may provide further insight into how different models of care either facilitate or hinder a woman's ability to find meaning and transcendence in the perinatal period.
Conclusion
Spirituality represents an often underexposed aspect of holistic perinatal care. It can serve as a source of strength, hope, and meaning, but requires a nuanced and culturally sensitive approach. An important implication for practice is that spiritual care competencies should be integrated into training and continuing education since midwives and nurses feel inadequately trained to provide spiritual care and are afraid of crossing boundaries or offending clients (Nuzum et al., 2015, 2016). Possibly, collaboration with spiritual caregivers and the use of spiritual screening tools could also help them offer more holistic care (Kamaara et al., 2020). Recognizing and supporting the spiritual dimension can contribute to better outcomes, greater satisfaction, and a more meaningful experience of pregnancy and birth. In conclusion, this review supports the integration of spiritual nursing care into holistic perinatal care, enabling nurses and midwives to go beyond biomedical care and fully support women and their partners in this life transition.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.