
Abstract
Aim
This study evaluated the effect of a Roy Adaptation Model (RAM)-based educational intervention on A1C levels and adaptive behaviors in adolescents with type 1 diabetes, and its contribution to physiological, psychosocial, and behavioral adaptation within a holistic nursing framework.
Methods
This randomized controlled trial included 60 adolescents aged 11 to 18 years followed in a pediatric endocrinology clinic. Participants were randomly assigned to an intervention group receiving structured RAM-based education, individualized tasks, and follow-up support (n = 30), or a control group receiving an educational brochure (n = 30). Data were collected at baseline and three months postintervention using a Sociodemographic Form, the Diabetes Knowledge Assessment Form, and clinical A1C records.
Results
Compared with the control group, the intervention group showed significant improvements in diabetes knowledge, adaptive behaviors, and A1C levels (p < .05). Interventions targeting RAM's adaptive modes contributed to glycemic control by strengthening psychosocial adaptation.
Conclusion
RAM-based nursing interventions promote physiological, psychosocial, and behavioral adaptation in adolescents with type 1 diabetes. Structured education enhances self-care, glycemic control, and coping. Integrating holistic nursing approaches into pediatric diabetes care is essential for improving outcomes.
Keywords
Introduction
Type 1 diabetes mellitus (T1DM) is a chronic endocrine disorder characterized by insulin deficiency and hyperglycemia resulting from the destruction of pancreatic β-cells (Couper et al., 2018). According to current data, this disease affects millions of individuals worldwide and becomes particularly difficult to manage during adolescence, when physiological and psychosocial changes intensify the complexity of disease management (International Diabetes Federation, 2024; Henríquez-Tejo & Cartes-Velásquez, 2018). During this period, maintaining treatment adherence and achieving metabolic control require not only medical interventions but also a multidimensional approach that supports the individual comprehensively (Hanna et al., 2025; Missambou Mandilou et al., 2021). Glycated hemoglobin (A1c), one of the key indicators of glycemic control in diabetes management, is widely used to assess treatment adherence (American Diabetes Association, 2018). However, approaches based solely on biomedical indicators remain insufficient to explain adolescents’ experiences of living with the disease and the dynamics of adaptation. At this point, theoretical models that encompass not only the individual's physiological status but also their psychosocial characteristics are needed.
The Roy Adaptation Model (RAM) supports mind–body–spirit integrity by conceptualizing adaptation processes that develop through the individual's interaction with the environment in terms of meeting basic physiological needs, developing a positive self-concept, fulfilling social roles, and achieving a balance between dependence and independence (Alimohammadi et al., 2018; Alligood, 2017; Harris, 2021; Roy, 2009). RAM is a model widely used by nurses worldwide. It focuses on promoting adaptation to illness and improving health by enhancing individuals’ ability to cope with problems arising from their interaction with the environment (Harris, 2021; Silverstein et al., 2005; Tatoğlu & Ayyildiz, 2025). In this respect, RAM aligns with the philosophy of holistic nursing and contributes to adolescents’ ability to make sense of their illness experiences, develop emotional adaptation, and strengthen their social connections. Adolescence, which is one of the most challenging periods of childhood, is accompanied by various physiological, social, and emotional changes. During this period, in which risk-taking behaviors become more prominent due to increasing autonomy, adaptation to a chronic illness such as T1DM, which affects multiple body systems, requires a holistic nursing care approach (Güneş & Çetinkaya, 2026; Silverstein et al., 2005). The literature reports that adolescents experience difficulties in diabetes management, including metabolic control, diabetes burden, and concerns about the future. In addition, psychosocial factors such as anxiety, depression, and social isolation may adversely affect glycemic control and worsen HbA1c levels (Harazneh et al., 2024; Hood et al., 2006; Malkawi et al., 2025; Young-Hyman et al., 2016). In adolescents with T1DM, the fundamentals of disease management are closely related not only to glycemic control but also to the individual's emotional responses, self-perception, social relationships, and the meaning they attribute to their life (Hilliard et al., 2013; Spencer et al., 2010). In this context, approaches to diabetes management that focus solely on treatment adherence and knowledge level remain insufficient; individuals’ processes of meaning-making related to the disease, emotional awareness, and social support systems should also be considered (Delamater et al., 2014). In one study, adolescents diagnosed with T1DM were reported to experience challenging circumstances affecting their adaptation to the disease, and it was emphasized that health education programs are needed to improve their self-care management, adaptation, and coping skills (Harazneh et al., 2024).
In their study, Tatoğlu and Ayyıldız (2025) found that an education program developed based on RAM was effective in protecting and promoting the health of working adolescents, whom they characterized as a disadvantaged group. The RAM-based educational intervention implemented in the present study aims not only to increase knowledge levels and treatment adherence but also to support adolescents’ adaptation processes by enabling them to express their illness-related experiences, develop emotional awareness, strengthen their social support, and attribute meaning to their illness. This holistic approach is considered to play an important role in improving not only metabolic control but also the individual's overall wellbeing.
Research Hypotheses
Methods
Study Design
This study was a randomized controlled experimental study consisting of an intervention group and a control group. The CONSORT checklist was followed in the reporting of this study (Figure 1). The study was registered at ClinicalTrials.gov under the registration number “NCT05336929” (https://clinicaltrials.gov/study/NCT05336929).
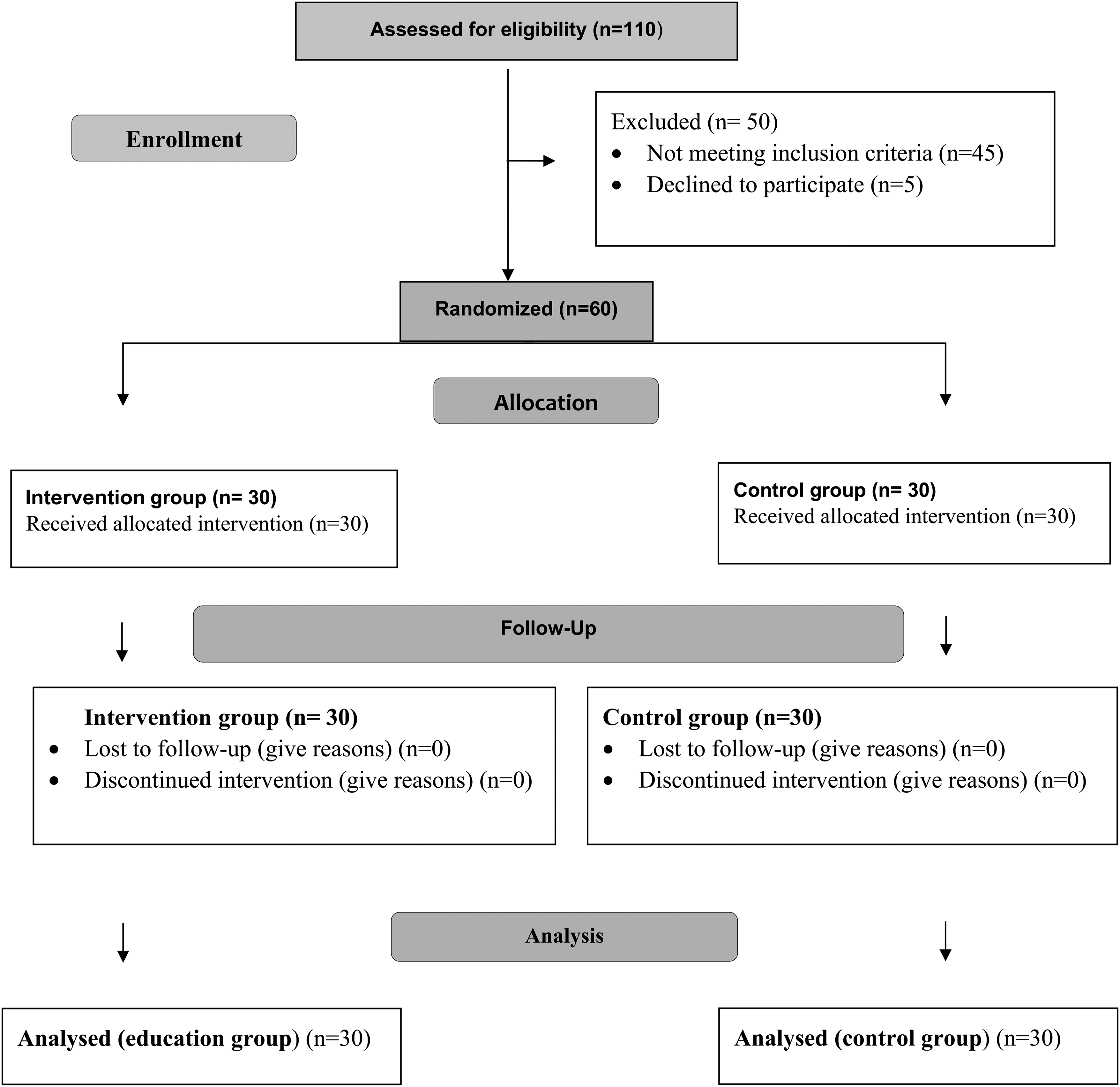
Consort flow diagram of this study.
Research Place and Time
The data were collected between January and June 2018 in the pediatric endocrinology outpatient clinic of a public hospital.
Research Population and Sample
The study population consisted of 110 children and adolescents aged 11–18 years who had been diagnosed with diabetes and were being regularly followed up in the diabetes outpatient clinic at the time the study began. Forty-five children/adolescents were not included in the study because they met the exclusion criteria. The mothers of five children/adolescents did not voluntarily agree to participate in the study. Consequently, the study was completed with a total of 60 adolescents.
Sample Size
Sample size was calculated using analysis of variance (ANOVA) in G*Power for repeated measures. The effect size was determined as 2.12, the significance level as α=0.05, and the test power as 1.00. The initial population consisted of 110 adolescents; 45 were excluded based on criteria, and five parents did not consent, resulting in a final sample of 60.
Research Criteria
Inclusion Criteria
Being between 11 and 18 years of age,
Having been diagnosed with T1DM by a pediatric endocrinologist,
Voluntary participation of both the parent and the child.
Exclusion Criteria
Having another chronic disease,
Having a cognitive or psychiatric disorder.
Randomization and Allocation
The sampling frame consisted of children and adolescents diagnosed with T1DM. After participants who met the eligibility criteria were identified, simple random sampling was applied. Group allocation was performed using a lottery method. To enhance allocation concealment, group assignments were conducted after the participant inclusion process had been completed and before data collection, using sealed envelopes prepared by an independent person. The researcher did not directly intervene in the group allocation process.
Blinding
Given that the study was an education-based intervention in which participants were necessarily aware of the intervention due to the nature of the study, participant blinding could not be implemented. Similarly, researcher blinding was not possible because the researcher was responsible for delivering the intervention. However, since the outcome assessments, namely A1C values, were obtained from routine clinical laboratory results, there was no subjective evaluation in the measurement process. Therefore, the risk of bias in outcome assessment was minimized.
Measurements
The study data were collected using the Sociodemographic Form, Diabetes Knowledge Assessment Form, and clinical records of A1C values.
Sociodemographic Data Form
This form was developed based on the literature. It contained 19 questions about adolescents’ demographic information, parental characteristics, and diabetes-related status. Content validity was ensured through expert review.
Diabetes Knowledge Assessment Form
The Diabetes Knowledge Assessment Form, developed by the researchers, was prepared based on the relevant literature and national/international diabetes education guidelines. Content validity was established by obtaining opinions from nursing and endocrinology experts in the field. To enhance the content validity of the form, the items were revised in accordance with expert evaluations. The form consists of 32 multiple-choice questions with a single correct answer, covering the definition, causes, and treatment of diabetes (National Juvenile Diabetes Group, 2018; Republic of Türkiye, Ministry of Health, General Directorate of Public Health, 2018b, 2018c; Turkish Diabetes Foundation, 2018). Each correct answer was scored as 1 point, while incorrect answers were scored as 0 points. Total scores range from 0 to 32, with higher post-intervention scores interpreted as an increase in diabetes knowledge. In addition, the form was found to have high internal consistency in a previous pilot implementation (Cronbach's alpha = 0.94). These characteristics support the usability and measurement reliability of the instrument in the present study.
Educational Materials
Nursing Education Handbook
Developed based on literature and expert input, this 55-page handbook included information on the four adaptive areas of the RAM and details related to diabetes management (Bakker et al., 2012; Guyton & Hall, 2013; International Diabetes Federation [IDF], 2017; International Diabetes Federation [IDF] & International Society for Pediatric and Adolescent Diabetes [ISPAD], 2011; Ministry of National Education, Turkey, 2017; Nahcivan & Tekin, 2012; Phelan et al., 2018; Republic of Turkey Ministry of Health, 2018b, 2018c,; Roy et al., 2009; Turkish Diabetes Foundation, 2018; Turkish Society of Endocrinology and Metabolism, 2016).
Education Brochure
Provided basic information about diabetes mellitus.
Educational Presentation
The content was developed based on the four principal modes of RAM (physiological, self-concept, role function, and interdependence). The educational program was delivered to adolescents during structured sessions (Nahcivan & Tekin, 2012; Roy et al., 2009). The presentation focused on T1DM and included visual aids and explanatory illustrations (International Diabetes Federation, 2017; National Juvenile Diabetes Group, 2018; Phelan et al., 2018; Republic of Türkiye, Ministry of Health, General Directorate of Public Health, 2018b, 2018c; Turkish Diabetes Foundation, 2018).
Data Collection and Intervention
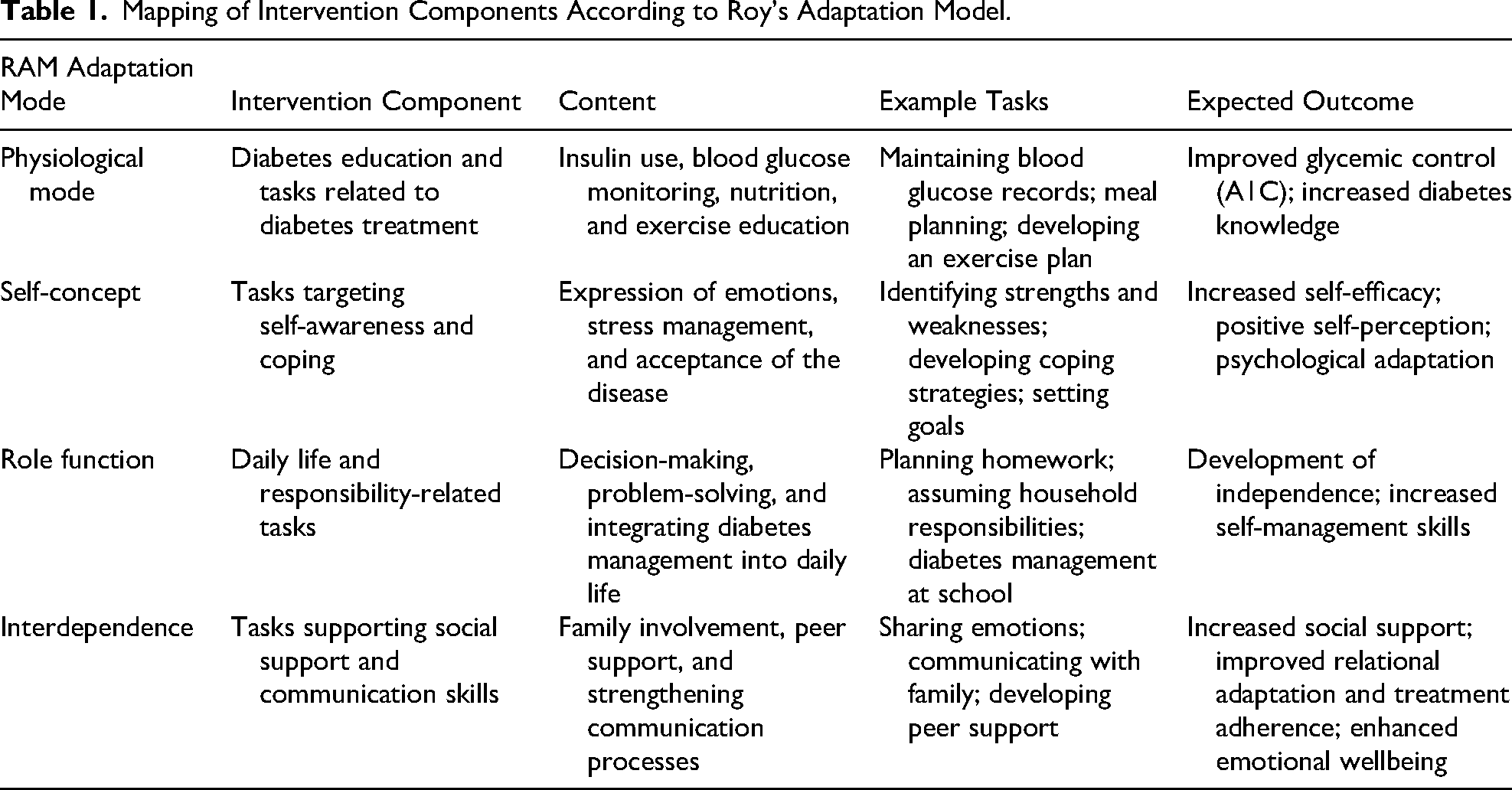
The intervention implemented in this study was not merely a procedure consisting of structured educational sessions, but rather a multidimensional nursing intervention grounded in the theoretical framework of RAM. Accordingly, the intervention components were systematically mapped onto the four adaptive modes: physiological, self-concept, role function, and interdependence.
Before the intervention, data were collected through face-to-face interviews conducted in a private setting. All adolescents completed the Sociodemographic Information Form and the Diabetes Knowledge Assessment Form, and their most recent A1C values were recorded. The intervention consisted of two individual education sessions conducted at 1-month intervals, each lasting approximately 45 to 60 min, followed by a 3-month follow-up process. The education sessions were delivered individually through interactive presentations supported by visual materials, and the content was structured to cover the four adaptive modes of RAM (Alimohammadi et al., 2018; Kacaroğlu Vicdan & Karabacak, 2014; Republic of Türkiye, General Directorate of Public Health, 2018a). Following the sessions, adolescents were provided with a comprehensive 55-page educational booklet that included RAM-based educational content and individualized tasks
During the follow-up process, adolescents were assigned individualized tasks included in the RAM-based educational booklet. Intervention fidelity was ensured through standardized educational content, structured educational materials, and the consistent delivery of the intervention by the same researcher. This structure reduced variability in intervention implementation and strengthened standardization. Intervention adherence was assessed through adolescents’ recording of task completion forms in the educational booklet and through follow-up interviews conducted with parents; it was operationalized based on the extent to which the assigned tasks were completed. Intervention intensity was defined in terms of the number of sessions, session duration, structured content, and continuity of the follow-up process. During follow-up interviews, the researcher reviewed these records and provided feedback, thereby supporting participation in and adherence to the intervention (Table 1).
RAM-Based Education and Tasks Were Structured as Follows
Development of Nursing Diagnoses
Potential maladaptive behaviors affecting diabetes management were identified through a literature review, and relevant nursing diagnoses were developed.
Goal Setting
Goals were established to support both medical and psychosocial adaptation, and an individualized care plan was developed based on focal, contextual, and residual stimuli in order to facilitate adaptation.
Educational Content According to RAM Domains
Physiological
Causes, signs and symptoms, treatment, long-term complications, and nutritional therapy of T1DM.
Self-Concept
Self-concept and self-esteem, characteristics of individuals with high self-esteem, stress recognition and coping strategies, and methods for enhancing self-esteem.
Role Function
Age-appropriate household responsibilities, problem-solving, decision-making, social skills, goal setting, and planning for the future.
Interdependence
Establishing and maintaining support systems and effective communication with support networks.
After the sessions, adolescents received the RAM guide, which included tasks for each adaptive domain. Adolescents recorded their task completion status in the booklet, and parents monitored adherence. Follow-up and evaluation were conducted to assess the completion of tasks and goals (Bakker et al., 2012; Kacaroğlu Vicdan & Karabacak, 2014; Turkish Diabetes Foundation, 2018).
Examples of Tasks According to Adaptive Modes
Physiological
Creating a diabetes identification card, recording blood glucose levels, and preparing meal and exercise plans.
Self-Concept
Listing personal strengths and weaknesses, identifying sources of stress, implementing coping strategies, such as breathing exercises, and planning future goals.
Role Function
Helping with household chores, completing homework, planning personal care, budgeting, and monitoring blood glucose at school.
Interdependence
Making a friend with diabetes, sharing problems and joys with family members, planning weekly activities, and reflecting on social interactions.
Three months after the intervention, both groups completed the Diabetes Knowledge Assessment Form again, and A1C levels were remeasured. The control group received only an informational brochure, and no further intervention was provided (American Diabetes Association, 2018; Kacaroğlu Vicdan & Karabacak, 2014; Republic of Türkiye, General Directorate of Public Health, 2018a).
Data Analysis
Pre- and post-test data of the intervention and control groups were compared. The study data were entered into the statistical software by an independent statistician who was not involved in data collection or the intervention. Each adolescent was assigned a numerical code; the intervention group was coded as “1” and the control group as “2.”
Data analysis was performed using IBM SPSS Version 23. Descriptive statistics were presented as frequency (n) and percentage (%) for categorical variables, and as mean ± standard deviation for continuous variables. Normality was assessed using the Shapiro–Wilk test. Parametric tests were applied when the assumptions of normality were met; otherwise, nonparametric tests were used. For comparisons between the two groups, the Mann–Whitney U test and independent samples t-test were applied as appropriate. One-way ANOVA or the Kruskal–Wallis H test was used for comparisons involving multiple independent groups, while chi-square analysis was used for categorical variables. A p-value of < .05 was considered statistically significant.
When the effect size of the study was examined, within-group analyses showed a strong pre–post relationship in the intervention group (r = 0.87), whereas no significant change was observed in the control group (r = 0.03). Between groups, the baseline difference was small to moderate (d = 0.42), while the post-test difference was very large (d = 4.54). For nonparametric analyses, Wilcoxon effect size (r) and effect sizes for the t-test/Mann–Whitney U test were also calculated where appropriate.
The large between-group effect size was attributable to the substantial differences observed in both knowledge levels and A1C levels. In particular, the marked reduction in A1C levels and the increase in knowledge levels in the intervention group contributed to the high effect size. In addition, the randomized controlled design of the study and the baseline homogeneity of the groups support the reliability of the effect size. Despite the small sample size, this value indicates the strong effect of the intervention.
Ethical and Legal Considerations
Ethical approval was obtained from an institutional ethics committee before the study. Before the interviews started, the purpose of the study was explained to the participants, and their consent to participate in the study and to audio recording was obtained. The anonymity of participants and the confidentiality of the information provided were maintained throughout the study and in subsequent public presentations of results.
Results
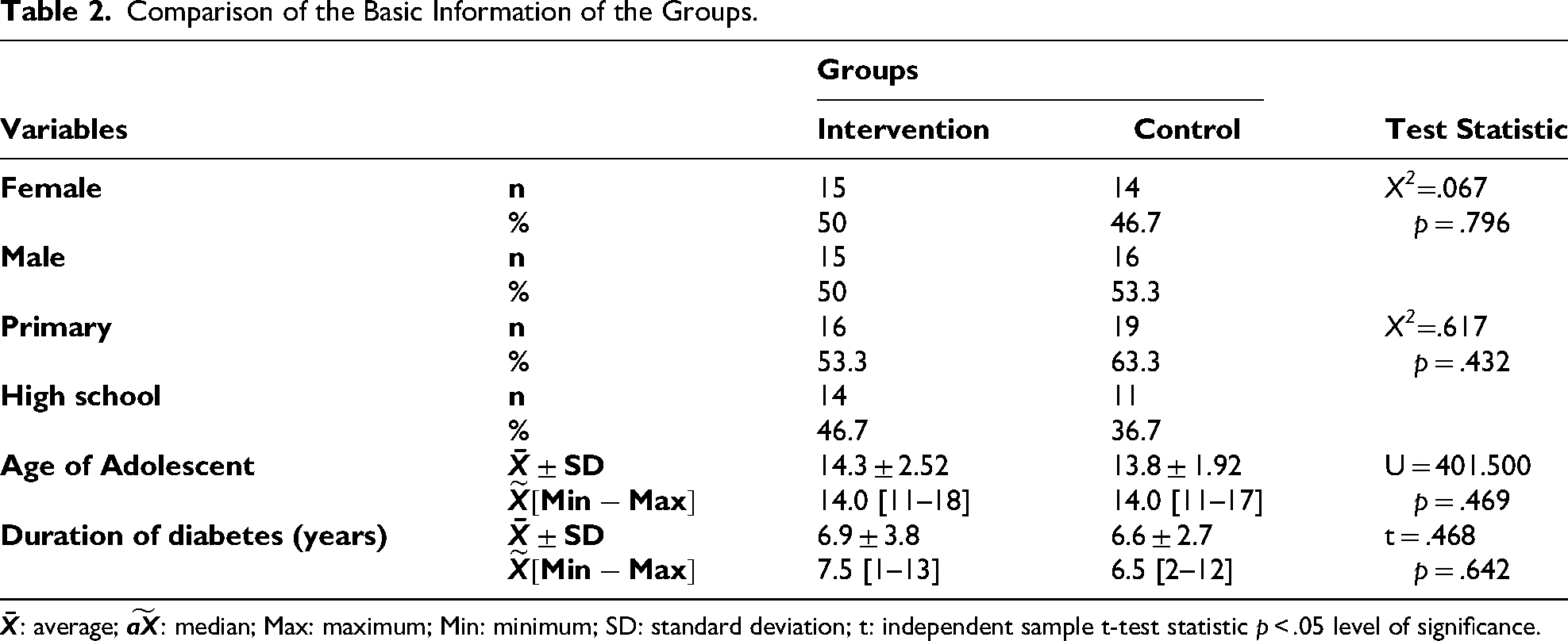
When comparing the sociodemographic characteristics of the intervention (n = 30) and control (n = 30) groups, the groups were similar in terms of gender, age, education level, and duration of diabetes (p > .05), indicating that the groups were homogenous at baseline (Table 2).
Mapping of Intervention Components According to Roy's Adaptation Model.
Comparison of the Basic Information of the Groups.
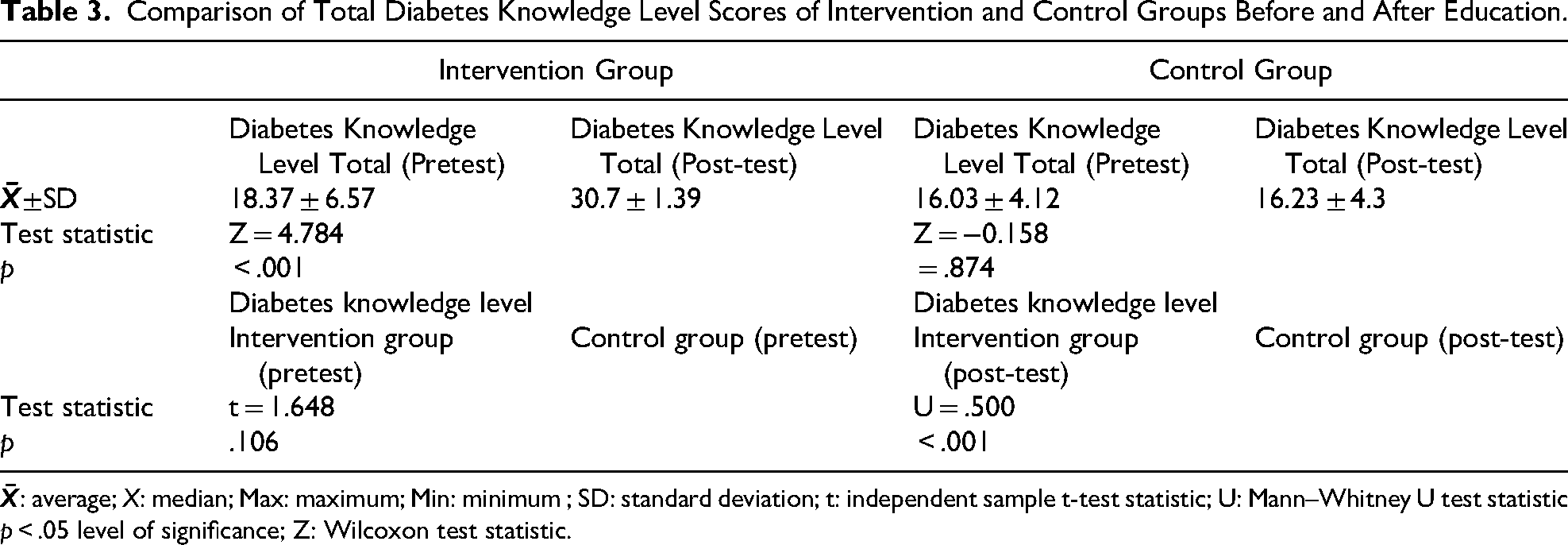
Regarding Diabetes Knowledge scores, the intervention group showed a significant increase from 18.37 ± 6.57 pre-intervention to 30.7 ± 1.39 post-intervention (Wilcoxon test, p < .001), whereas the control group's scores remained almost unchanged (16.03 ± 4.12 pretest vs. 16.23 ± 4.3 post-test, p = .874). Between-group comparison showed no significant difference in pretest scores (p = .106), but the post-test scores were significantly higher in the intervention group compared to the control group (p < .001). The between-group post-test Cohen's d was 4.53, indicating a very large effect size, and the within-group pre/post Cohen's d for the intervention group was 2.59, also indicating a very large effect (Table 3).
Comparison of Total Diabetes Knowledge Level Scores of Intervention and Control Groups Before and After Education.
Regarding A1C levels, the intervention group showed a significant decrease from 9.80 ± 1.99 pre-intervention to 8.46 ± 1.25 post-intervention (paired t-test, p < .001), whereas the control group showed no significant change (9.70 ± 1.03 pretest vs. 9.88 ± 1.02 post-test, p = .652). Between-group comparison of post-test A1C levels showed significantly lower values in the intervention group (p < .001). The between-group post-test Cohen's d was 1.25, indicating a large effect, while the within-group pre/post Cohen's d was 0.81 for the intervention group and 0.18 for the control group (Table 4).
Comparison of A1C Values of the Groups.

p: Mean p < .05; SD: standard deviation significance level; t: dependent sample test statistics.
Discussion
When the findings of this study are evaluated within the framework of RAM, the observed improvements appear to reflect a multidimensional and dynamic adaptation process. In particular, within the physiological mode, the significant reduction in A1C levels observed in the intervention group demonstrates the direct effect of increased knowledge and skills related to disease management on metabolic control (Table 3). This finding indicates that physiological adaptation is not limited solely to biological processes, but develops in interaction with learning, behavioral change, and cognitive processes (Table 4). Indeed, the literature also emphasizes that structured and multidimensional interventions are effective in reducing A1C levels (Edraki et al., 2020; Zhao et al., 2021; Elamin et al., 2024).
When evaluated in terms of the self-concept mode, it is thought that the self-awareness, self-expression, and coping strategies included in the intervention strengthened adolescents’ perceptions of the illness and their self-efficacy. The literature indicates that psychological adjustment and self-perception are key determinants in diabetes management, and that improvements in these domains enhance treatment adherence (Delamater et al., 2014; Hilliard et al., 2012). Furthermore, studies demonstrating the relationship between self-efficacy and glycemic control support the importance of individuals taking an active role in disease management (Hood et al., 2014; Iannotti et al., 2006).
In addition, structured education and support programs have been reported to contribute to adolescents’ ability to make sense of their illness experiences (Vaillancourt et al., 2023; Katsarou et al., 2017). This suggests that changes in the self-concept mode are not limited merely to an increase in knowledge, but rather indicate a deeper psychosocial adaptation that transforms the individual's meaning-based relationship with the illness.
Within the role function mode, supporting adolescents in fulfilling daily life responsibilities and developing decision-making and problem-solving skills may have contributed to their ability to integrate diabetes management as a natural part of everyday life. This finding reflects an adaptation process consistent with the development of independence during adolescence. The literature indicates that increased self-management skills are closely associated with diabetes management and treatment adherence (Schilling et al., 2009; Anderson et al., 2002). In addition, the development of problem-solving and decision-making skills has been reported to positively affect metabolic control (Grey et al., 2000; Wiebe et al., 2005). Similarly, structured interventions have been shown to improve adolescents’ adaptation to daily life activities and enhance their self-care skills (Gulcu et al., 2020; Doğan & Çam, 2020).
The interdependence mode, on the other hand, highlights the importance of social support and relational dimensions. Strengthening family involvement, peer support, and effective communication processes may have positively influenced adolescents’ coping processes with the illness. The literature emphasizes that family support and parental involvement are key determinants of glycemic control and treatment adherence (Anderson et al., 2002; Wiebe et al., 2005). Furthermore, strengthened peer relationships enhance psychosocial adjustment and improve illness-related coping skills (Helgeson et al., 2014 ). It has also been reported that strengthening social support mechanisms facilitates adaptation and improves disease management in this process (Tuohy et al., 2025; Altundağ, 2018). This suggests that the interdependence mode is associated not only with receiving support but also with establishing and maintaining meaningful social bonds.
When these four modes are evaluated together, it is evident that the most prominent effects of the study emerged in the physiological mode, as reflected by the reduction in A1C levels, and in the self-concept mode, through increased self-awareness and knowledge. The role function and interdependence modes, meanwhile, appeared to play a supportive role in this process. These findings indicate that adaptation is not a unidimensional process, but rather occurs through multiple interacting systems. Moreover, the literature also shows that RAM-based interventions similarly support multidimensional adaptation in different chronic diseases (Alimohammadi et al., 2018; Yeh, 2002; Sadeghnezhad Forotaghe et al., 2011).
From a holistic nursing perspective, the findings should be interpreted not merely as biomedical improvements, but as the development of holistic adaptation at the levels of the individual's mind, body, and social relationships. Considering the adverse effects of psychosocial factors, such as anxiety and depression, on glycemic control, strengthening these domains plays a critical role in improving metabolic outcomes (Missambou Mandilou et al., 2021; Harvey, 2015; Santos et al., 2013). In this context, it can be argued that the holistic nursing approach has not only a supportive function but also a transformative impact on clinical outcomes.
This study makes an important contribution by demonstrating that RAM can be used not only as a tool for intervention design, but also as a holistic theoretical framework for explaining and interpreting clinical outcomes. The findings reveal that the physiological, psychological, and social dimensions of adaptation are not independent of one another; rather, they operate as dynamic processes in mutual interaction. In particular, the reflection of improvements observed in psychosocial adaptation domains on metabolic outcomes empirically supports the holistic adaptation approach proposed by RAM. In this respect, the study demonstrates that, beyond approaches focusing on behavioral adaptation in the management of chronic illness among adolescents, theory-based nursing interventions grounded in mind–body–social integrity play a transformative role in clinical outcomes (Table 4). These findings indicate that the research hypothesis was supported. Therefore, by extending the theoretical scope of RAM, this study shows that the model offers not only an explanatory framework but also a powerful structure that guides clinical practice and enables outcomes to be interpreted holistically.
Limitations and Strengths of the Research
This study has several limitations. The single-center design and the relatively short 3-month follow-up period limit the generalizability of the findings and the evaluation of long-term effects. The voluntary nature of participation may have introduced potential selection bias, while the absence of blinding procedures may have led to measurement bias. In addition, the limited sample size and the focus solely on the adolescent population further restrict the generalizability of the results. Therefore, future studies with multicenter designs, larger samples, and longitudinal follow up are recommended. Nevertheless, the randomized controlled design of the study, the use of a standardized intervention protocol, and the reliance on clinical measurement data are considered important factors that enhance its methodological strength.
Implications for Holistic Nursing Practice
The structured and holistic intervention based on RAM was found to be effective in increasing knowledge levels and improving HbA1c levels among adolescents with T1DM. This finding highlights the importance of low-cost and feasible nursing interventions in pediatric diabetes care. Accordingly, nurses should conduct multidimensional assessments that address not only adolescents’ physiological status but also the domains of self-concept, role function, and interdependence, and should develop individualized care plans based on these assessments.
In clinical practice, RAM-based interventions can be implemented through structured educational sessions, individualized goal setting, support for self-care skills, and planned regular follow-up processes. In this process, nurses should not only improve adolescents’ knowledge levels but also provide counseling aimed at supporting their emotional adaptation.
In school settings, nurses should provide education focusing on role function and social adaptation to help adolescents integrate diabetes management into daily life, encourage peer support, and maintain follow-up processes in collaboration with teachers. In community-based care, the adaptation of both the adolescent and the family system should be supported through family education programs, home follow up, and counseling services.
In this process, the role of nurses is not limited to providing care; it also includes coordinating care, facilitating interdisciplinary communication, and managing all care needs of the individual through a holistic approach. Increasing family involvement and strengthening social support systems positively affect clinical outcomes by enhancing adolescents’ adaptation to the illness and adherence to treatment.
Finally, it is clear that focusing solely on biomedical approaches in diabetes management is insufficient and that holistic care encompassing emotional and social dimensions is necessary. Therefore, the inclusion of theoretical models such as RAM in nursing education programs and their integration into clinical practice will strengthen nurses’ critical thinking, clinical decision making, and holistic care deliver skills.
Conclusion
In summary, the RAM-based intervention significantly improved diabetes knowledge and glycemic control (A1C levels) in adolescents with T1DM, while no notable changes were observed in the control group. These findings indicate that structured, theory-based interventions can effectively enhance disease management and adherence in adolescents. Therefore, interventions based on the RAM should be implemented to strengthen self-efficacy and disease management in individuals with chronic conditions. Given that the model offers low-cost, nonpharmacological, and easily applicable strategies, it can be integrated into clinical practice. In addition, individualized training programs and parental counseling based on the model can be developed, and psychosocial support strategies can be incorporated into diabetes care guidelines. Future large-scale, long-term studies are recommended to evaluate the sustainability of adaptation from adolescence to adulthood.
Footnotes
Acknowledgments
We would like to thank the hospital staff who supported the study, all the mothers who agreed to participate in the study, and Assoc. Prof. Dr. Su Özgür who analyzed the study data.
Ethical Statement
Necessary ethical approval and institutional permission for this study were obtained.
Consent to Participate
Written “İnformed Consent” was obtained from the mothers participating in the study. During the preparation of this study, the authors used
Author Contributions
Funding
This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of Conflicting Interest
The authors declare that they have no conflict of interest regarding the publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the authors. Data could not be shared because the data belonged to adolescents aged 11 to 18.