
Abstract
Purpose
This study examined the immediate holistic effects of a single-session Dhikr Istighfar intervention on anxiety among Indonesian patients undergoing percutaneous coronary intervention (PCI), guided by Kolcaba's Comfort Theory.
Design
A single-arm quasi-experimental pre–post study.
Method
Thirty-four adult Muslim patients scheduled for PCI participated in a 20-min, nurse-facilitated Dhikr Istighfar session, delivered at the bedside one hour before the procedure. Anxiety was measured using a validated scale. Paired t-tests and effect sizes assessed pre–post changes.
Findings
Anxiety scores decreased significantly from 22.3 ± 3.1 at baseline to 7.7 ± 2.1 after the intervention, indicating a large effect size (Cohen's d = 0.90). While reductions were substantial, causal inference is limited due to the absence of a control group. Ninety-one percent of participants transitioned to the “no anxiety” category, with improvements across all cognitive, somatic, and autonomic subdomains. Participants also reported enhanced psychospiritual comfort, consistent with the domains of relief, ease, and transcendence.
Conclusions
A brief, spiritually integrated nursing intervention using Dhikr Istighfar promotes immediate reductions in preprocedural anxiety and supports psychospiritual well-being, reflecting the holistic principles of mind–body–spirit care. Findings support incorporating culturally congruent spiritual practices within holistic nursing approaches for patients facing high-stress cardiac procedures.
Introduction
Anxiety is one of the most prevalent mental health conditions worldwide, affecting approximately 4.4% of the global population, or over 350 million individuals (Javaid et al., 2023; World Health Organization, 2023). Patients with cardiovascular diseases experience disproportionately high rates of anxiety, with studies reporting up to one-third of cardiac patients exhibiting clinically significant anxiety prior to invasive procedures such as percutaneous coronary intervention (PCI) (Saini et al., 2022; Smith, 2022). Preprocedural anxiety in this population is associated with increased sympathetic activation, higher perioperative complication rates, prolonged hospitalization, reduced adherence to medical recommendations, and diminished quality of life (Fernandez et al., 2021; Relawati et al., 2025; Usichenko et al., 2022). In Indonesia, a nation with a high burden of ischemic heart disease and a predominantly Muslim population, preprocedural anxiety remains a clinically significant concern often overlooked in routine cardiac care (Muharram et al., 2024; Qanitha et al., 2022).
Conventional pharmacological or psychological interventions, while effective in some settings, may not adequately address the unique cultural and spiritual needs of Indonesian patients (Cipta et al., 2024; Liem, 2019). Within holistic nursing, these cultural and spiritual dimensions are integral to understanding the person as a unified mind–body–spirit being, requiring approaches honoring patients’ beliefs, values, and sources of meaning (Enzman Hines & Gaughan, 2017; Frisch & Rabinowitsch, 2019).
In Muslim-majority contexts, spiritual practices such as Dhikr, the contemplative remembrance of God, are central to daily life and can serve as culturally congruent strategies to alleviate anxiety. Dhikr is believed to promote emotional calm, psychological resilience, and physiological relaxation through a combination of focused attention, rhythmic vocalization, and meditative breathing, aligning with the biopsychosocial-spiritual model of health (Abdurachman et al., 2025; Wahyuni et al., 2019). Such practices resonate strongly with holistic nursing principles, which recognize spiritual well-being as a vital aspect of healing.
This study draws on Kolcaba's Theory of Comfort, which defines comfort as a multidimensional experience encompassing physical, psychospiritual, social, and environmental dimensions (Smith & Parker, 2015). The psychospiritual dimension emphasizes the importance of spiritual well-being as a contributor to overall comfort, particularly in stressful healthcare contexts (Lin et al., 2023). From a holistic nursing perspective, Dhikr can be understood as an intervention promoting comfort by fostering inner peace, connection, and transcendence—core elements supporting healing in the midst of physiological vulnerability. Integrating such spiritual practices also reflects holistic nursing's emphasis on therapeutic presence, compassionate intention, and the creation of a healing environment.
Emerging international study supports the efficacy of spiritually integrated interventions in cardiovascular and acute care settings. Systematic reviews and meta-analyses have demonstrated prayer, mindfulness, and religious-based interventions can reduce anxiety, depression, and physiological stress indicators while improving coping and quality of life (Mousavizadeh & Jandaghian-Bidgoli, 2024; Sert et al., 2025; Zhang et al., 2024). Despite these encouraging findings, there is a paucity of studies evaluating Dhikr, particularly in the context of acute preprocedural anxiety for PCI patients. Existing studies often lack rigorous methodological designs, such as standardized assessment tools, or context-specific cultural frameworks, limiting their applicability (Piscesiana et al., 2021). Moreover, few studies explicitly situate Dhikr within the theoretical underpinnings of holistic nursing, leaving a gap in understanding how culturally rooted spiritual practices can be intentionally integrated into holistic care frameworks.
The present study addresses these gaps by exploring Dhikr Istighfar as a spiritually grounded, nurse-facilitated intervention designed to enhance psychospiritual comfort and reduce anxiety among adult Indonesian patients undergoing PCI. Dhikr Istighfar refers to the repeated recitation of “Astaghfirullahal-‘Azhiim,” meaning “I seek forgiveness from Allah the Almighty.” Within Islamic contemplative practice, dhikr functions as a structured form of spiritual mindfulness involving rhythmic verbal repetition, intentional breathing, and focused awareness of the divine. This practice is widely used to regulate emotional distress, promote inner calm, and facilitate spiritual connection.
Despite increasing interest in spiritual interventions, Quran-based practices often lack standardized protocols and theoretical grounding, limiting reproducibility and comparability (Nursyah & Apriliawati, 2025). This study aims to evaluate the immediate effect of Dhikr Istighfar on preprocedural anxiety (primary outcome), conceptualized as a psychospiritual response within Comfort Theory.
Methods
Study Design
This study employed a single-arm pre–post quasi-experimental design to evaluate the effect of a single-session Dhikr Istighfar intervention on anxiety levels among adults with acute coronary syndrome (ACS) scheduled for PCI. The single-arm design was chosen due to the acute, time-sensitive nature of preprocedural anxiety in PCI, where rapid intervention is needed and randomization may be ethically or practically challenging. The study followed Transparent Reporting of Evaluations with Nonrandomized Design reporting guidelines (Jarlais, 2014). Due to the single-group design, potential biases were addressed through standardized procedures; however, no protocol registration was performed.
Setting and Participants
The study was conducted in the Heart Critical Care Unit of a private tertiary-care hospital in Bandung, Indonesia, between April and June 2025. This hospital serves as a regional referral center for cardiovascular emergencies and provides a representative clinical context for investigating preprocedural anxiety in patients undergoing PCI. Eligible participants were adult Muslim patients (aged 34–60 years) with a confirmed diagnosis of ACS and scheduled for PCI. Standard preprocedural care included routine education, limited family visitation, and administration of mild sedation as indicated. “No comorbidities” refers to the absence of documented chronic conditions such as hypertension, diabetes, or obesity. Inclusion criteria required participants to be able to communicate verbally, have a stable hemodynamic status prior to the procedure, and provide informed consent. Patients with severe psychiatric disorders, impaired consciousness, or acute complications requiring immediate intervention were excluded.
A total of 34 eligible patients were consecutively recruited. The sample size was calculated a priori using G*Power version 3.1, based on paired t-test analysis with an assumed medium-to-large effect size (d = 0.70) derived from prior studies of spiritually integrated interventions, α = 0.05, and power (1–β) = 0.80, yielding a minimum sample requirement of 30 participants. To account for potential attrition, we recruited 34 patients, all of whom completed the study without dropout. This pragmatic approach is consistent with exploratory and pilot studies designed to evaluate the feasibility and preliminary effectiveness of culturally embedded spiritual interventions. The study population reflects the sociocultural and religious characteristics of Indonesian Muslim patients, enhancing ecological validity and supporting the translational relevance of the findings for similar Muslim-majority clinical settings worldwide.
Instruments
Participant characteristics were collected, including age, sex, education, lifestyle habits (smoking, high-salt diet, high-fat diet), and comorbidities (hypertension, diabetes mellitus, obesity). Anxiety was measured using the 14-item Indonesian version of Anxiety Rating Scale, with scores ranging from 0 (not present) to 4 (severe) for each item, yielding a total score between 0 and 56. Anxiety severity was categorized as: <14 (no anxiety), 14–20 (mild), 21–27 (moderate), 28–41 (severe), and 42–56 (very severe) (Erlina et al., 2022), administered as a structured clinician-rated instrument by a trained nurse. Internal consistency in this study was acceptable (Cronbach's α = 0.793). Although quantitative, the instrument captures both cognitive and somatic anxiety manifestations, aligning with holistic nursing's focus on the interconnectedness of psychological and physiological responses.
Study Intervention: Dhikr Istighfar
Dhikr Istighfar is a form of Islamic contemplative practice involving repetitive recitation of “Astaghfirullahal-‘Azhiim” (I seek forgiveness from Allah the Almighty). Conceptually, Dhikr integrates psychological, physiological, and spiritual mechanisms: it directs attention, modulates emotional states, and activates relaxation responses, while fostering a sense of transcendence and meaning. Preprocedural anxiety in PCI patients is often associated with elevated sympathetic activity, ruminative thoughts, and anticipatory distress, which can negatively affect cardiovascular outcomes. A spiritually grounded intervention like Dhikr may reduce anxiety through attentional regulation, emotional reframing, and parasympathetic activation, providing a culturally congruent, low-cost, and ethically acceptable strategy for preoperative care.
Participants were guided using a standardized script: they were instructed to sit or lie comfortably, regulate breathing, and recite Astaghfirullahal-‘Azhiim at a steady rhythm (∼5 s per repetition) for 100 repetitions. A digital counter was used to ensure adherence. No audio recordings were used. Fidelity was monitored using a checklist completed by the facilitator. In accordance with holistic nursing practice, the nurse facilitating the intervention provided therapeutic presence, gentle guidance, and an intentionally calming environment to support mind–body–spirit integration during the Dhikr session.
Procedures
Following eligibility screening and informed consent, participants completed the sociodemographic and clinical questionnaire and a baseline anxiety assessment. The Dhikr Istighfar session was delivered individually, immediately followed by postintervention anxiety assessment to capture short-term changes in anxiety. No participants were lost to follow-up, and all data were complete. The procedural flow intentionally incorporated elements of holistic nursing, such as presence, attentiveness, and creation of a peaceful setting, to support participants emotionally and spiritually throughout data collection. The same researcher conducted assessments and intervention delivery, which may introduce observer bias; future studies should separate these roles or use blinded assessors.
Statistical Analysis
Data were analyzed using SPSS version 26.0. Descriptive statistics summarized participant characteristics. Paired t-tests compared pre- and immediate postintervention anxiety scores for total and subscale domains. Effect size for paired samples was calculated using Cohen's d_z, with 95% confidence intervals reported. Assumptions were checked using difference score normality. A p-value <.05 was considered statistically significant.
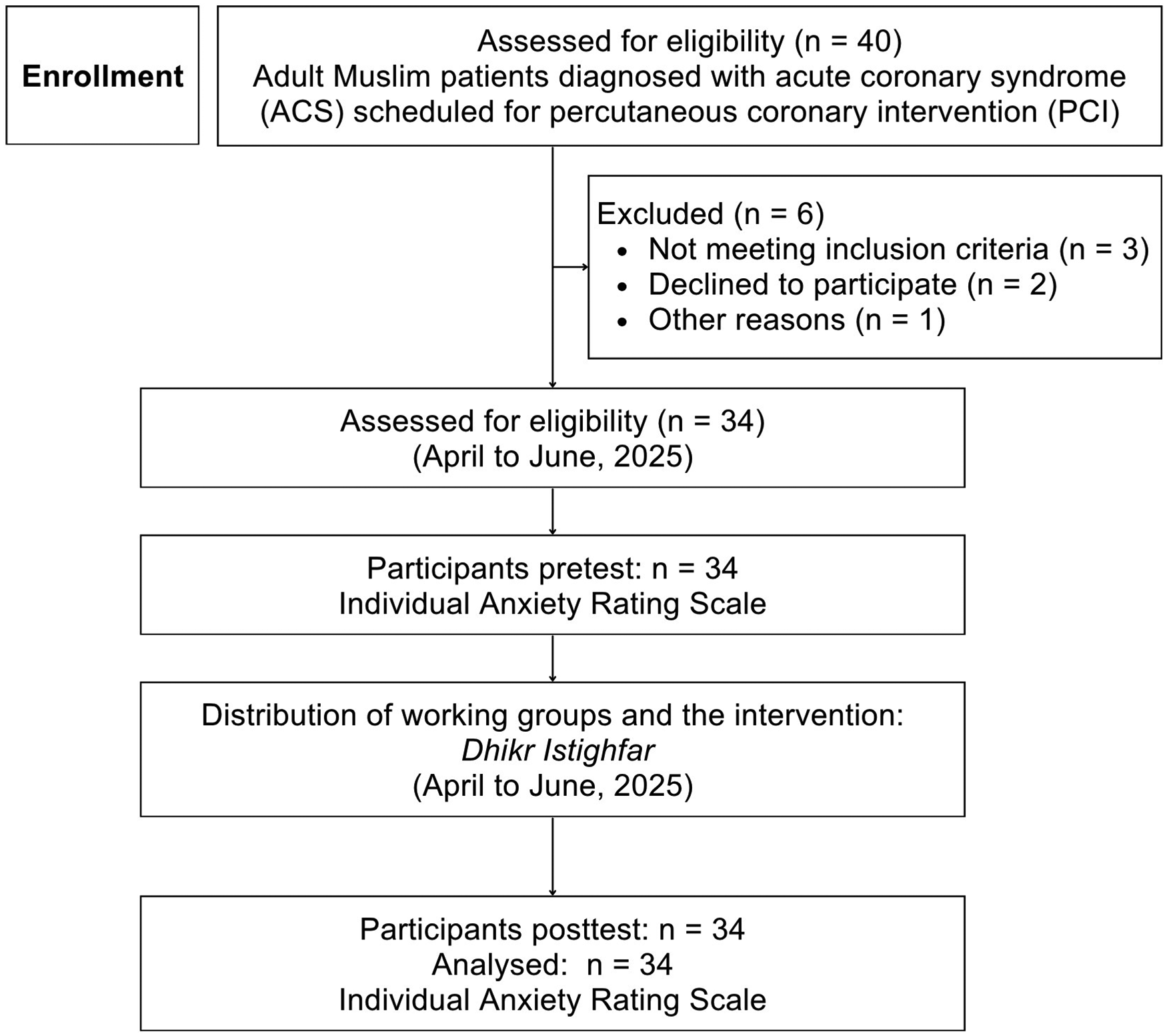
Flow of the participants and the periods of recruitment.
Ethics Approval
Ethics approval was obtained from the Research Ethics Committee of Al Islam Hospital, Bandung (Approval No. 011/KEPK-RSAI/04/2025). All participants provided written informed consent. The study complied with the Declaration of Helsinki and national study ethics guidelines. Participants were assured the intervention honored their cultural and spiritual values, reflecting holistic nursing's commitment to dignity, respect, and person-centered care.
Result
Participant Characteristics
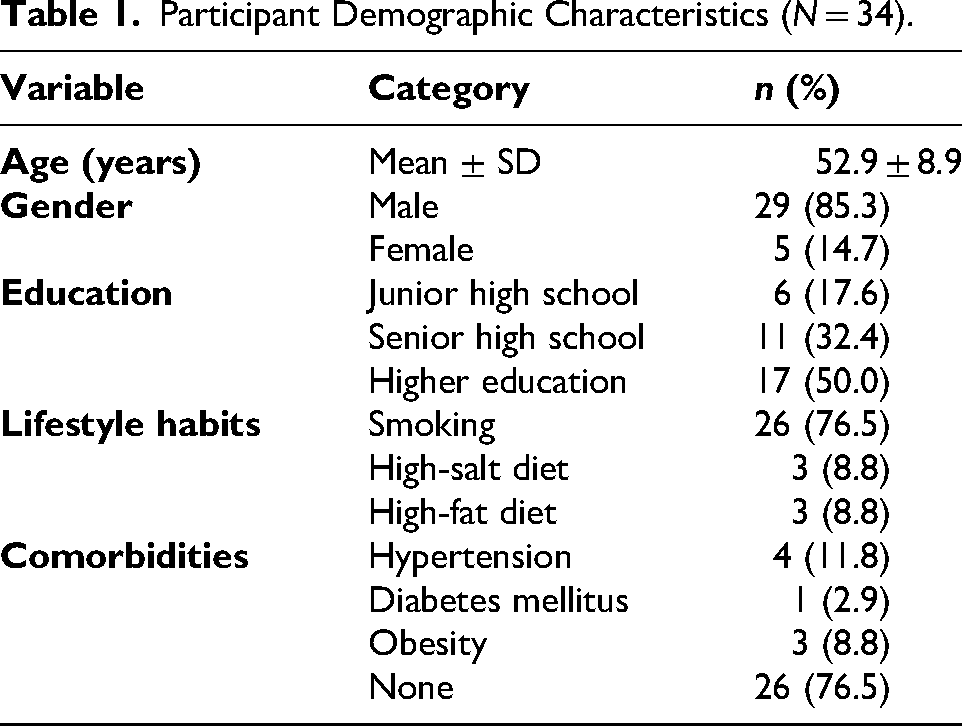
A total of 34 patients with ACS scheduled for PCI were enrolled and completed the study (Figure 1). No participants were lost to follow-up, and no missing data occurred. Participants had a mean age of 52.9 ± 8.9 years, with the majority being male (85.3%). Approximately half of the participants had attained higher education, and most reported current smoking. Comorbidities were relatively uncommon, with 76.5% of participants reporting no chronic illness. Sociodemographic and clinical characteristics are summarized in Table 1.
Participant Demographic Characteristics (N = 34).
Anxiety Scores Before and After the Intervention
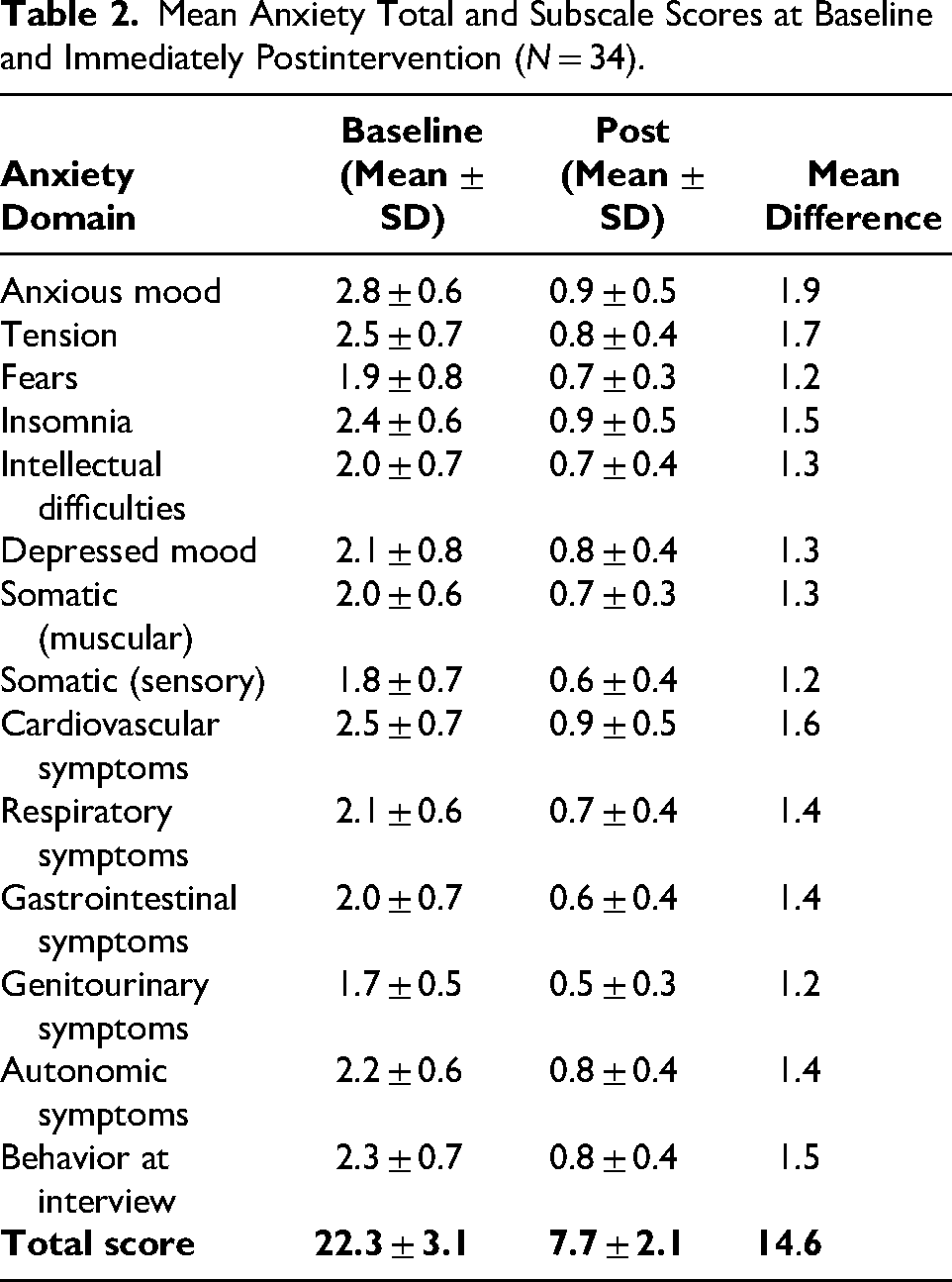
The scale was administered at baseline and immediately after the intervention. As shown in Table 2, mean scores for all subdomains decreased substantially postintervention. The total anxiety score declined from 22.3 ± 3.1 at baseline to 7.7 ± 2.1 immediately postintervention, indicating a marked reduction in anxiety levels. Holistically, this decline reflects not only cognitive and somatic relief but also a shift toward greater inner ease and calm, aligning with the psychospiritual domain of Comfort Theory.
Mean Anxiety Total and Subscale Scores at Baseline and Immediately Postintervention (N = 34).
Categorical Changes in Anxiety and Statistical Comparison
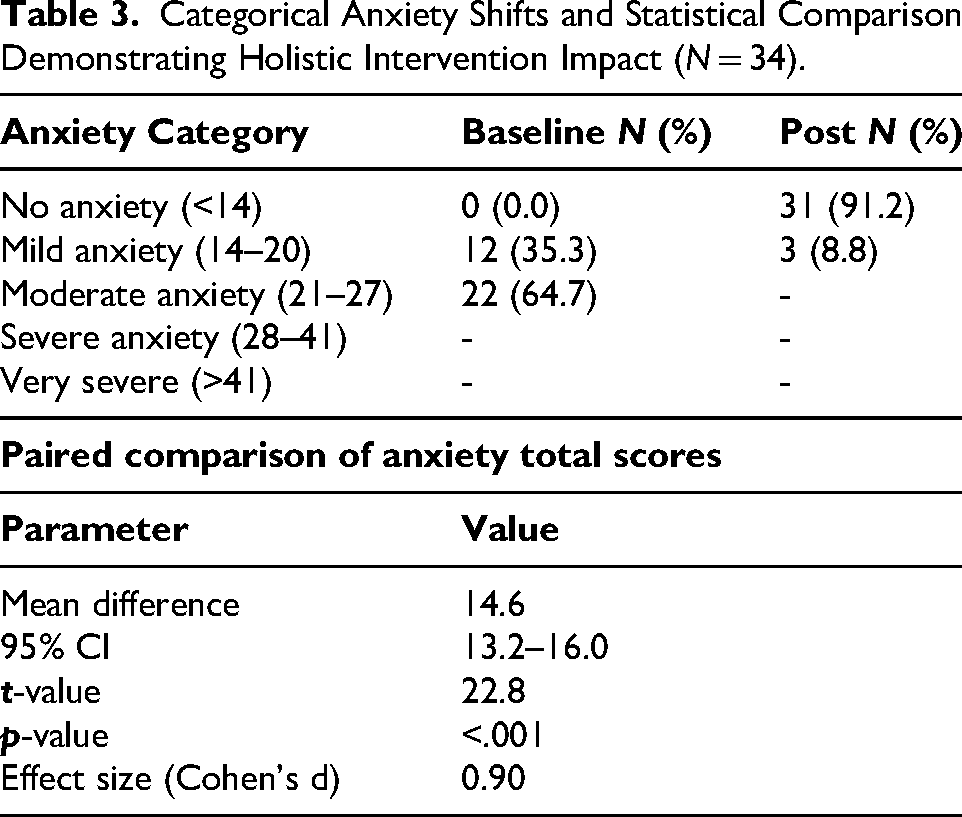
Following the intervention, the majority of participants transitioned from moderate anxiety to no or mild anxiety. Statistical analysis revealed a significant reduction in anxiety total scores (mean difference = 14.6, 95% CI [13.2–16.0], t = 22.8, p < .001; Table 3). Notably, 91.2% of participants moved into the “no anxiety” category. Although the reduction was substantial, the magnitude should be interpreted cautiously given the absence of a control group and potential contextual influences.
Categorical Anxiety Shifts and Statistical Comparison Demonstrating Holistic Intervention Impact (N = 34).
Discussion
This study demonstrates a brief, single-session Dhikr Istighfar administered immediately before PCI can produce significant reductions in anxiety and improvements in both psychological and spiritual well-being among adults in an Indonesian Muslim community. The immediate postintervention reduction in anxiety scores, along with the shift of most participants from moderate anxiety to no anxiety, highlights the clinical relevance and practical significance of this spiritually grounded intervention in high-stress clinical settings. These findings also illustrate how integrating culturally meaningful spiritual practices into nursing care can foster holistic healing by supporting patients’ mind–body–spirit balance during vulnerable moments (Nilsson, 2022). From a holistic nursing standpoint, the intervention's effect reflects the therapeutic potential of spiritual practices to enhance perceived comfort, inner peace, and readiness for invasive procedures.
These findings suggest an association rather than causation. Potential mechanisms include cognitive reorientation and meaning-making processes (Manurung, 2025), which require further validation using objective physiological measures. The mechanisms underlying the effectiveness of Dhikr are multidimensional, spanning psychological, physiological, and spiritual domains. Psychologically, the focused attention and repetitive recitation inherent in Dhikr facilitate cognitive regulation by redirecting focus from anxious thoughts toward a sense of divine presence (Achour et al., 2015; Wahyuni et al., 2019). This attentional shift promotes emotional stability by fostering trust, surrender, and acceptance, which buffer anticipatory stress prior to invasive procedures. Physiologically, the rhythmic recitation and controlled breathing patterns characteristic of Dhikr engage the parasympathetic nervous system, reducing sympathetic arousal and alleviating somatic manifestations of anxiety such as cardiovascular, respiratory, and muscular tension (Amjadian et al., 2020). Spiritually, Dhikr Istighfar nurtures a sense of connectedness, meaning, and transcendence—qualities holistic nursing recognizes as vital to promoting resilience, comfort, and healing. This multidimensional effect reflects the holistic unity of mind, body, and spirit, supporting nursing interventions honoring the whole person rather than isolated symptoms.
The spiritual dimension of Dhikr Istighfar further contributes to resilience and adaptive coping. Engagement in contemplative worship fosters a sense of meaning, purpose, and transcendence, strengthening psychological resources and promoting physiological stability, aligning with studies indicating spiritual involvement positively influences both mental and physical health (Gautam et al., 2024; Karori, 2024). Holistic nursing emphasizes the value of meaning-making and spiritual engagement as pathways to healing, particularly in contexts where illness threatens physical and emotional equilibrium (Lalani, 2020).
By combining attentional regulation, emotional modulation, and physiological relaxation within a spiritually meaningful framework, Dhikr exemplifies the creative partnership between psychology and religion, demonstrating spiritual practices can serve as active, evidence-informed contributors to health outcomes (Aggarwal et al., 2023; Wüthrich-Grossenbacher et al., 2023). These findings underscore the importance of spiritual care within nursing practice, affirming spiritual interventions can enhance human wholeness and strengthen patients’ capacity to cope with acute medical stress.
Compared to secular interventions such as mindfulness or relaxation exercises, Dhikr Istighfar offers the added advantage of cultural and religious relevance, enhancing receptivity, engagement, and adherence. The immediate reductions in preprocedural anxiety observed in this study illustrate that spiritually congruent interventions can provide rapid, meaningful benefits even in brief applications. This relevance is consistent with holistic nursing principles, which emphasize individualized, culturally sensitive, person-centered care reflecting patients’ beliefs and lived experiences.
Integrating spiritually informed practices into conventional healthcare highlights that religion and spirituality are not peripheral to care but central to holistic health promotion (Khalajinia et al., 2021; Najafi et al., 2022). Within the framework of Comfort Theory, Dhikr Istighfar appears to promote relief (reduced distress), ease (emotional soothing), and transcendence (a sense of connection beyond the immediate situation), supporting holistic comfort in the mid of medical uncertainty.
Overall, these findings contribute to a growing recognition that health-care interventions can be most effective when they incorporate patients’ cultural and spiritual frameworks. Dhikr Istighfar demonstrates that the creative partnership between psychological principles and religious practices can produce measurable improvements in mental, physical, and spiritual well-being, offering a model for culturally congruent, holistic care in clinical practice. For holistic nursing, this study reinforces the importance of therapeutic presence, intentionality, and spiritual sensitivity, affirming the nurse's role in facilitating healing environments nurturing the whole person.
Implications for Practice
The study provides important guidance for clinical practice. A brief, single-session Dhikr Istighfar can serve as a practical, low-cost, and culturally sensitive intervention to reduce preprocedural anxiety in adults undergoing PCI. Nurses, counselors, and other healthcare providers can integrate guided Dhikr Istighfar into preoperative preparation to support psychological and spiritual well-being, emphasizing the interconnectedness of mental, physical, and spiritual health. For holistic nurses, this intervention offers an opportunity to apply therapeutic presence, respect spiritual diversity, and foster healing environments promoting comfort in the moments preceding invasive procedures.
Aligned with the American Holistic Nurses Association Scope and Standards of Practice, this intervention reflects core competencies in spiritual care, therapeutic presence, and culturally congruent practice. Dhikr Istighfar may be operationalized as a structured preprocedural intervention delivered 30–60 min before PCI by trained nurses, using a standardized script and patient-centered approach. Recognizing religious and spiritual practices as evidence-informed tools encourages a holistic, person-centered approach to care. Collaboration between healthcare professionals and religious leaders may further enhance patient engagement, adherence, and the overall effectiveness of spiritually integrated interventions. By integrating Dhikr into routine preprocedural nursing care, clinicians can strengthen the nurse–patient connection, reduce distress, and support readiness for procedures through culturally congruent spiritual support.
Holistic Significance
This study offers meaningful contributions to holistic nursing by demonstrating how a culturally grounded spiritual practice can enhance psychospiritual comfort and reduce acute anxiety during a high-stress cardiac procedure. Rooted in the mind–body–spirit paradigm, Dhikr Istighfar exemplifies an integrative healing modality aligned with nursing values of presence, compassion, and culturally sensitive care. Guided by Kolcaba's Comfort Theory, the intervention illustrates how nurses can cultivate relief, ease, and transcendence within moments of vulnerability, supporting the patient's whole-person experience. By honoring patients’ spiritual traditions, nurses strengthen therapeutic relationships, reinforce personal meaning, and create conditions fostering inner peace and resilience.
The findings underscore the essential role of spiritual care as a component of holistic nursing practice and highlight the importance of integrating culturally relevant interventions into acute cardiovascular care. Ultimately, this study expands the evidence base for spiritual nursing interventions and affirms that cultivating comfort is both a clinical and holistic act promoting healing, wholeness, and person-centered well-being.
Limitations
This study has several limitations. The absence of a control group in a single-arm pre–post design limits causal inference, as anxiety reductions may be influenced by expectancy effects or uncontrolled cointerventions such as sedation and routine education. Potential assessor bias is also present, given that the same researcher delivered the intervention and assessed outcomes. The small sample size and single-center setting restrict generalizability, particularly across different cultural or religious contexts. Additionally, reliance on self-report measures introduces the risk of response bias. Outcomes were assessed only immediately postintervention, providing no evidence on the durability of effects or impact on postoperative recovery. Future studies should use randomized controlled designs with blinded assessment, standardized cointerventions, and objective physiological measures.
Conclusions
A single-session Dhikr Istighfar administered immediately before PCI was effective in reducing anxiety and enhancing psychological and spiritual well-being among adult Muslim patients. By integrating attentional focus, emotional regulation, and spiritual meaning, the intervention reflects the mind–body–spirit approach central to holistic nursing. Guided by Kolcaba's Comfort Theory, Dhikr promoted relief, ease, and transcendence, demonstrating its potential as a culturally congruent strategy for cultivating comfort during high-stress cardiac procedures.
These findings underscore the importance of incorporating spiritual and culturally grounded practices into holistic nursing care, particularly in settings where faith plays a central role in patients’ lives. Dhikr Istighfar may support psychospiritual readiness, strengthen nurse–patient connection, and enhance person-centered care. Future research using randomized designs and exploring patients’ lived experiences can further clarify the role of spiritually integrated interventions in promoting comfort, healing, and whole-person well-being.
Footnotes
Acknowledgments
We want to express our gratitude to all who participated in this research. We would also like to thank Universitas ‘Aisyiyah Bandung and Al Islam Bandung Hospital for supporting this study.
Ethical Approval
This study received ethical approval from the Research Ethics Committee of Al Islam Hospital, Bandung (Approval No. 011/KEPK-RSAI/04/2025). All participants provided written informed consent. The study complied with the Declaration of Helsinki and national study ethics guidelines.
Consent to Participate
Written informed consent was obtained from all individual participants involved in the study after providing them with verbal and written explanations regarding the purpose, procedures, and ethical safeguards of the research.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available, but are available from the corresponding author on reasonable request.