
Abstract
Purpose
To clarify and define self-management (SM) within cardiovascular-kidney-metabolic (CKM) syndrome through concept analysis, with implications for holistic nursing.
Design
Concept analysis using Walker and Avant's eight-step method.
Methods
Six databases were searched for peer-reviewed articles (2005–2025). Twenty-one studies met the inclusion criteria. Findings were interpreted through the Individual and Family Self-Management Theory and Neuman's Systems Model. Qualitative literature enriched interpretation of the holistic dimensions of each attribute.
Findings
Four defining attributes emerged: self-monitoring, personalized and precision care, collaborative care, and sustained engagement; each carrying behavioral and experiential significance. Five antecedents and six consequences were identified across biological, psychosocial, structural, and spiritual dimensions. Self-Management in CKM is distinct from self-care as traditionally conceptualized, due to pathophysiological interdependence, system-level coordination, and experiential complexity.
Conclusions
This analysis provides a holistic, theory-informed definition of Self-Management in CKM and a foundation for middle-range theory development. The framework supports nurse-led interventions addressing the whole person across interacting chronic conditions.
Keywords
Introduction
Cardiovascular-kidney-metabolic syndrome (CKM) is a progressive, multisystem disorder defined by the pathophysiological interplay among cardiovascular, kidney, and metabolic dysfunctions (Ndumele, Rangaswami et al., 2023). The American Heart Association and the European CaReMe Partnership characterize CKM as a shared pathophysiologic, epidemiologic, and prognostic continuum in which metabolic abnormalities, chronic kidney disease (CKD), and cardiovascular disease (CVD) interact to accelerate morbidity and mortality (Broseta et al., 2024; Ndumele, Neeland et al., 2023; Wu et al., 2024). Globally, more than 500 million people live with diabetes (Sun et al., 2022), 64 million with heart failure (Groenewegen et al., 2020), and 700 million with chronic kidney disease (Bikbov et al., 2020). This underscores the syndemic burden of CKM across regions and healthcare systems. In the United States, nearly 90% of adults meet criteria for CKM stage 1 or higher, with 15% at advanced stages (Aggarwal et al., 2024).
Unlike single-disease contexts in which self-management (SM) targets one condition, CKM presents a unique challenge. Its component diseases share bidirectional pathophysiological pathways that make the management of one condition inseparable from the others (Ndumele, Neeland et al., 2023; Vora et al., 2024). SM demands also vary across CKM stages (0–4): early stages emphasize prevention and lifestyle modification, while advanced stages require complex medication management and integrated specialist care (Ndumele, Neeland et al., 2023). This heterogeneity necessitates a reconceptualization of SM that accounts for the intertwined nature of these conditions rather than merely their coexistence.
SM is broadly defined as the ongoing process by which individuals monitor health indicators, adhere to treatment regimens, and address physical and psychosocial demands (Grady & Gough, 2014; M. E. Lawless et al., 2016; Salimu et al., 2025). It has emerged as a cornerstone of chronic disease care. However, the concept overlaps with related constructs such as self-care (Riegel et al., 2012). Its meaning within CKM remains theoretically inconsistent, complicated by overlapping comorbidities, behavioral challenges, and social barriers.
Nursing theories have long provided the conceptual architecture for chronic illness management, from the self-care deficit theory (Orem et al., 2001) to situation-specific theories of self-care (Riegel et al., 2012). Building on this tradition, the Individual and Family Self-Management Theory (IFSMT) conceptualizes SM through three interrelated domains: context, process, and outcomes (Ryan & Sawin, 2009). IFSMT's context domain encompasses biological, psychological, social, and environmental factors, providing an inherently holistic foundation for understanding SM. However, while IFSMT acknowledges contextual influences, its process and outcome domains center on the individual and family. Neuman's Systems Model (Neuman & Fawcett, 2011), on the other hand, offers a complementary systems-level perspective. It situates the person within lines of defense against intrapersonal, interpersonal, and extrapersonal stressors across five holistic variables: physiological, psychological, sociocultural, developmental, and spiritual. Together, these frameworks support the interpretation of SM that attends to both individual processes and the broader, system-level, and holistic dimensions of CKM.
Purpose
The purpose of this concept analysis is to clarify and define SM in CKM by identifying its defining attributes, antecedents, and consequences. Clarifying this concept strengthens the theoretical foundation for nursing interventions and advances research, education, and clinical practice related to CKM.
Methods
This concept analysis used Walker and Avant's (2021) eight-step method to clarify SM within the CKM context. The steps were as follows: (1) selecting the concept for its central yet inconsistently defined role in CKM; (2) determining the purpose; (3) identifying uses across disciplines; (4) determining defining attributes through thematic synthesis; (5) constructing a model case; (6) identifying borderline, related, and contrary cases; (7) outlining antecedents and consequences; and (8) defining empirical referents. The interpretation of synthesized findings was guided primarily by the IFSMT (Ryan & Sawin, 2009). Antecedents were mapped to IFSMT's context domain, defining attributes to the process domain, and consequences to the outcome domain. This alignment captured the theoretical mechanisms linking context, behavior, and outcomes in CKM. Additionally, Neuman's Systems Model (Neuman & Fawcett, 2011) presents a lens for interpreting how system-level stressors, including competing treatment demands, fragmented care, and structural barriers, interact with individual and family SM processes. Neuman's five holistic variables (physiological, psychological, sociocultural, developmental, and spiritual) and three levels of prevention (primary, secondary, tertiary) provided additional structure for situating SM within the broader systems context of CKM.
A comprehensive search was conducted in six databases: PubMed, CINAHL+, EMBASE, PsycINFO, Web of Science, and Scopus. The search covered peer-reviewed articles published in English between 2005 and 2025. MeSH terms and keyword combinations included “self-management,” “self-management behaviors,” “chronic kidney disease,” “type 2 diabetes,” “hypertension,” “cardiometabolic risk,” “obesity,” and “cardiorenal syndrome” (Table 1). MeSH terms applied in PubMed were adapted for other databases using equivalent subject headings and keyword fields. The search strategy used broad Boolean combinations across title, abstract, and subject heading fields. This approach captured studies addressing SM-related behaviors, including those framed as self-care, without restricting retrieval to a single term. The inclusion of studies employing self-care frameworks in the final sample confirms the breadth of this strategy.
Eligibility Criteria and Search Terms Used in the Review.
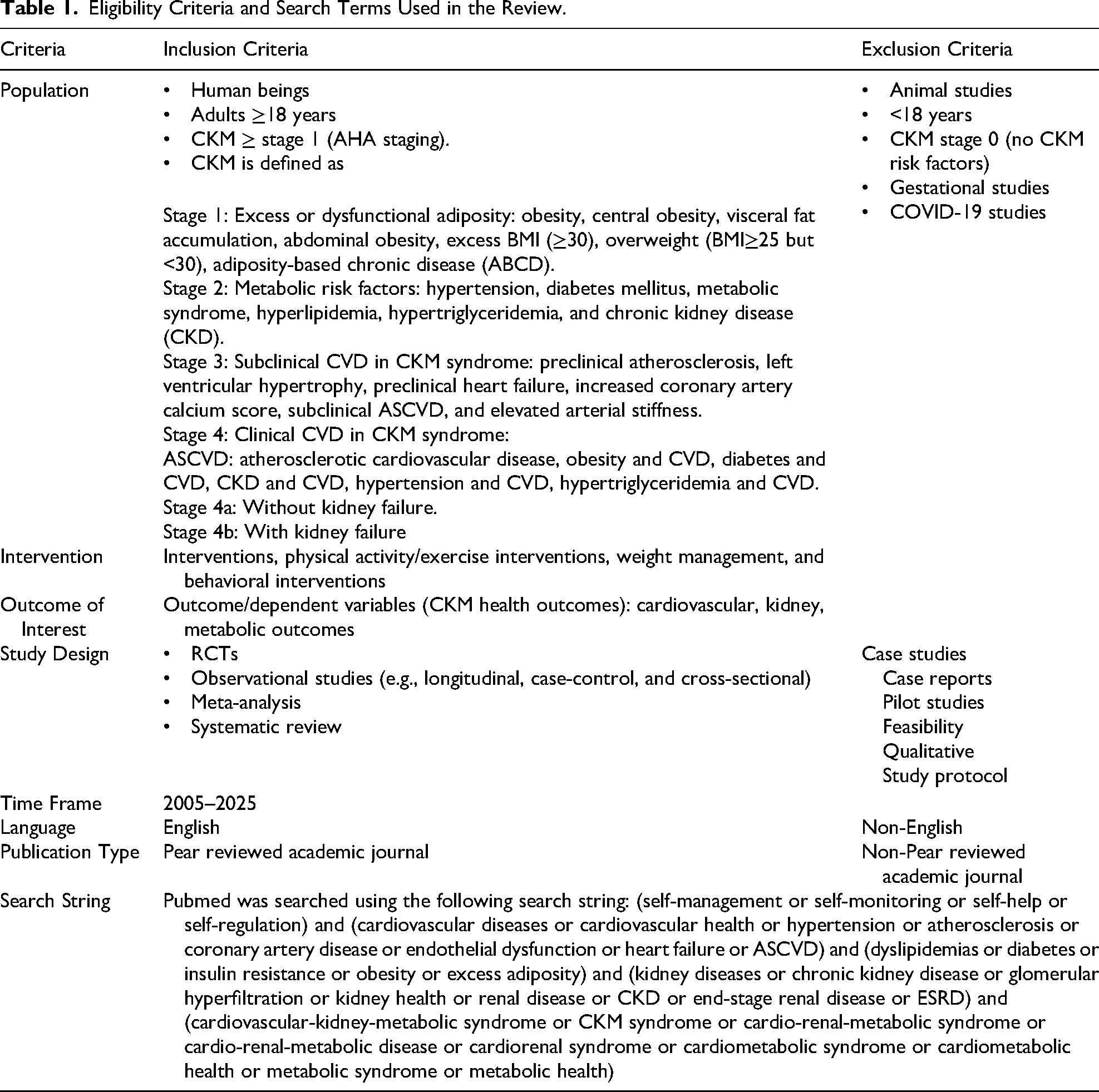
Studies were eligible if they examined SM behaviors or interventions linked to cardiovascular, kidney, or metabolic outcomes among adults aged 18 years or older. Because CKM is an emerging framework and few studies address all three component conditions simultaneously, studies addressing two or more CKM components were included. This reflects the continuum nature of CKM, in which shared pathophysiology connects conditions even when not all three are present. Randomized controlled trials, quasi-experimental studies, observational studies, systematic reviews, and meta-analyses were included. Studies were excluded if they did not explicitly address SM, focused solely on caregivers or pediatric populations, lacked CKM-relevant outcomes, or were protocols, feasibility studies, or pilot trials (Table 1). The focus on empirical studies was intentional: concept analysis requires observable evidence to identify measurable attributes and consequences. Qualitative and conceptual papers were not included but are recommended for future analyses.
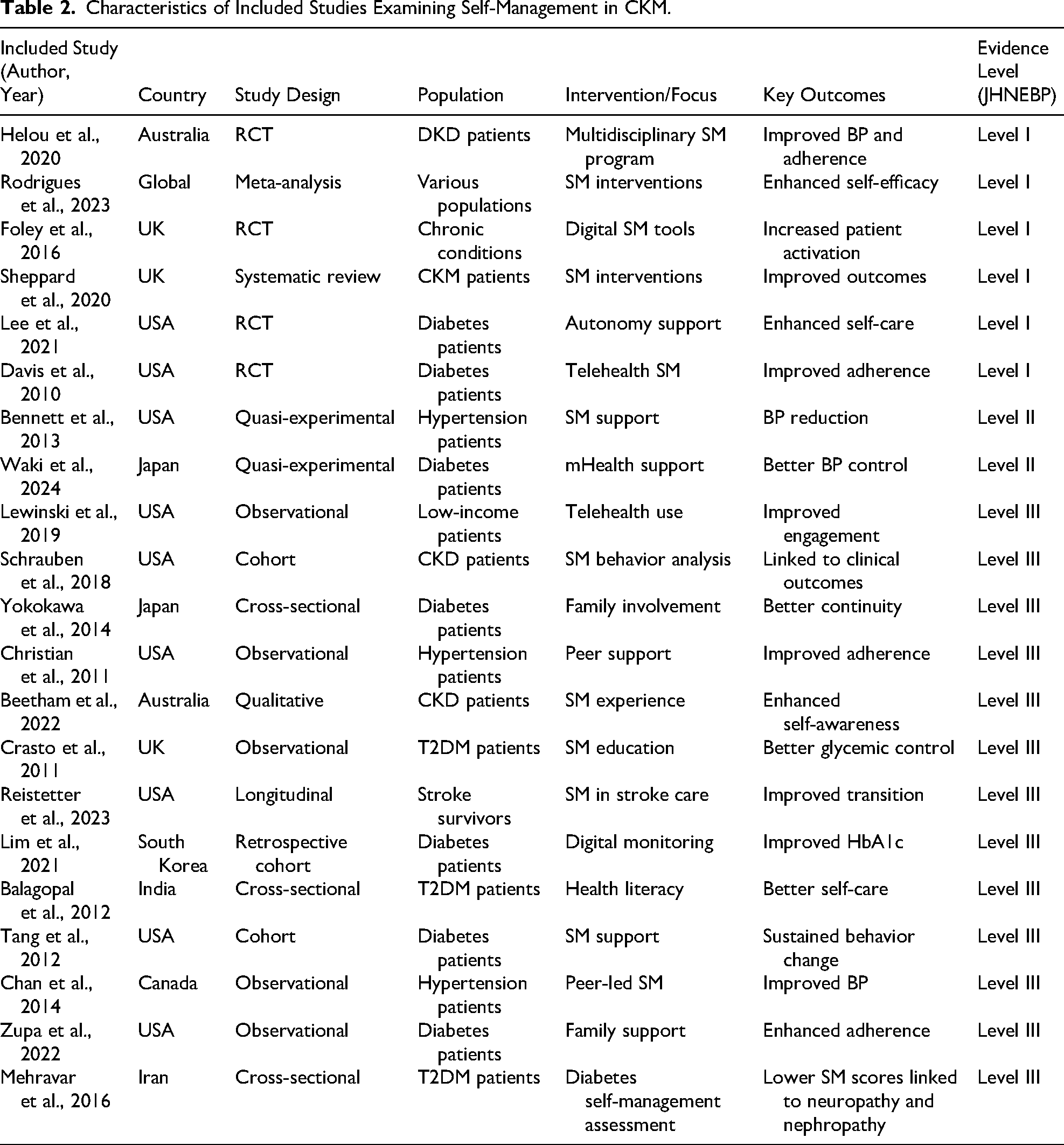
The search yielded 298 records. After removing 29 duplicates, 269 were screened by title and abstract. Fifty-two were assessed for full-text eligibility, and 21 met the inclusion criteria (Figure 1; Table 2). Study quality and level of evidence were appraised using the Johns Hopkins Nursing Evidence-Based Practice model (Dearholt & Dang, 2012). Two reviewers independently rated each study's design, methodological rigor, and relevance. Discrepancies were resolved through consensus discussion. The final sample included Level I, II, and III evidence across multiple disciplines and geographic regions (Table 2).
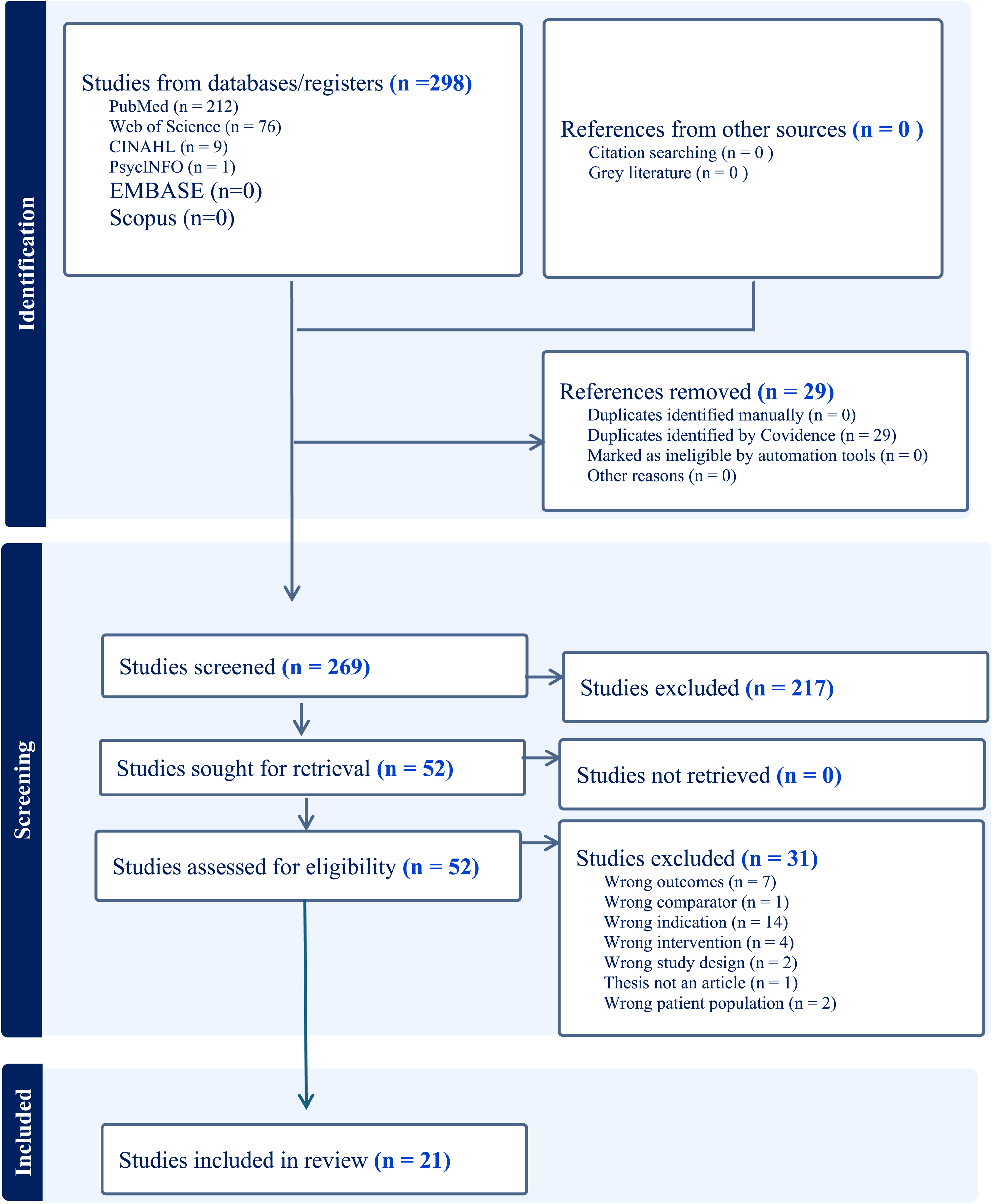
PRISMA flow diagram showing identification, screening, and inclusion of studies.
Characteristics of Included Studies Examining Self-Management in CKM.
Results
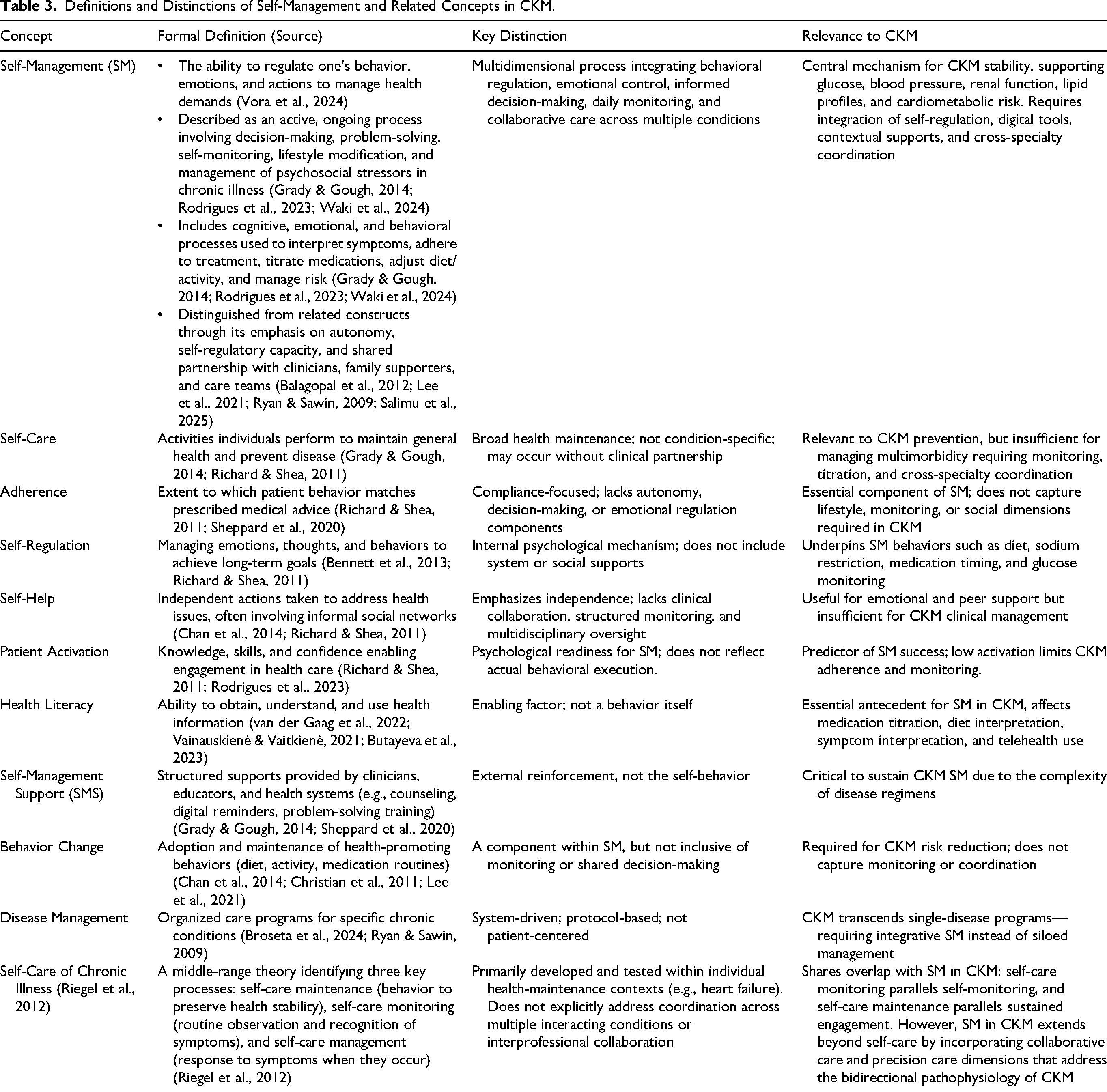
This concept analysis examined how SM is defined, applied, and measured in CKM literature. The results clarify SM as a multidimensional process encompassing contextual antecedents, behavioral attributes, and measurable outcomes. Table 3 summarizes common definitions of SM and related concepts.
Definitions and Distinctions of Self-Management and Related Concepts in CKM.
Uses of the Concept Across Disciplines
SM is used across nursing, behavioral medicine, public health, digital health, diabetes care, nephrology, cardiology, and primary care. In nursing, it emphasizes symptom monitoring, medication management, decision-making, and collaborative partnerships (Helou et al., 2020; Zupa et al., 2022). In medicine, it refers to adherence, lifestyle modification, and self-monitoring of clinical parameters (Lewinski et al., 2019; Mehravar et al., 2016; Sheppard et al., 2020). Behavioral sciences frame it as a self-regulatory process involving goal setting, motivation, and emotional regulation (Bennett et al., 2013; Lee et al., 2021). Digital health literature describes technology-supported behaviors such as telemonitoring, app-based tracking, and automated feedback (Davis et al., 2010; Rodrigues et al., 2023; Waki et al., 2024). Notably, SM overlaps with self-care as described in Riegel et al.'s (2012) theory, which identifies self-care maintenance, monitoring, and management as core processes (Riegel et al., 2012).
Defining Attributes
Attributes are the characteristics that distinguish a concept from related ones (Walker & Avant, 2021). For this analysis, four attributes emerged: self-monitoring, personalized and precision care, collaborative care, and sustained health engagement. Together, they describe an adaptive process through which individuals regulate health behaviors and physiological parameters across CKM conditions. While the empirical literature emphasizes their behavioral and clinical dimensions, each attribute also carries experiential and relational significance that reflects the holistic dimensions of living with multimorbidity, as explored in the Discussion.
Self-Monitoring
Self-monitoring is the consistent observation and interpretation of symptoms, vital signs, and treatment responses. It guides timely behavioral adjustments. Across studies, self-monitoring included tracking blood pressure, glucose, body weight, diet, and medication adherence, encompassing both prescribed regimen tracking and dose timing (Crasto et al., 2011; Davis et al., 2010; Helou et al., 2020; Lewinski et al., 2019; Lim et al., 2021; Sheppard et al., 2020). Both traditional methods and digital tools were employed (Balagopal et al., 2012; Rodrigues et al., 2023; Waki et al., 2024). However, human support remained critical. Interventions combining digital monitoring with counselling or peer coaching showed stronger medication adherence and long-term disease control (Lim et al., 2021; Tang et al., 2012; Waki et al., 2024). This attribute aligns with self-regulation theory, which posits that individuals adjust behavior through feedback loops comparing current status to desired goals (Bandura, 1991). In CKM, the complexity of simultaneous monitoring across multiple parameters distinguishes this attribute from single-disease self-monitoring.
Personalized and Precision Care
Personalized care involves tailoring SM strategies to individual values, cultural context, and lifestyle. Precision care applies data-driven approaches, such as biomarkers, comorbidity profiles, and predictive analytics, to optimize interventions (Christian et al., 2011; Helou et al., 2020; Lee et al., 2021; Reistetter et al., 2023). Studies described individualized goal-setting, motivational interviewing, and culturally tailored education as key components (Beetham et al., 2022; Foley et al., 2016; Helou et al., 2020; Lewinski et al., 2019; Lim et al., 2021). Multidisciplinary precision models and culturally tailored interventions improved adherence, glycemic control, and quality of life (Balagopal et al., 2012; Lim et al., 2021; Rodrigues et al., 2023). This attribute reflects IFSMT's process domain, in which individual knowledge, beliefs, and self-regulation skills shape SM behaviors within specific contexts (Ryan & Sawin, 2009).
Collaborative Care
Collaborative care involves coordinated partnerships among patients, families, and interprofessional teams. It includes reciprocal communication, shared decision-making, and mutual accountability (Beetham et al., 2022; Lee et al., 2021; Reistetter et al., 2023; Tang et al., 2012; Zupa et al., 2022). Multidisciplinary collaboration was associated with improved blood pressure control, medication adherence, and care continuity (Chan et al., 2014; Crasto et al., 2011; Davis et al., 2010; Lewinski et al., 2019; Helou et al., 2020). Family and community networks further strengthened these processes (Beetham et al., 2022; Helou et al., 2020; Lee et al., 2021; Reistetter et al., 2023; Zupa et al., 2022). This attribute aligns with Orem et al.'s (2001) concept of dependent-care agency, in which supportive others contribute to the individual's self-care capacity.
Sustained Health Engagement
Sustained engagement refers to ongoing, proactive participation in health-promoting behaviors over time; it encompasses the capacity to remain motivated and resilient despite challenges (Beetham et al., 2022; Bennett et al., 2013; Lee et al., 2021; Waki et al., 2024). Self-efficacy, social support, stress management, and perceived benefits of care influence this attribute (Balagopal et al., 2012; Foley et al., 2016; Helou et al., 2020; Waki et al., 2024). Digital reminders, peer support, and structured follow-up helped patients maintain adherence to both treatment regimens and intervention programs (Davis et al., 2010; Lee et al., 2021; Lewinski et al., 2019; Tang et al., 2012). Sustained engagement integrates the other three attributes into a continuous behavioral cycle. It parallels self-care maintenance in Riegel et al.'s (2012) theory, the behaviors used to maintain health stability over time.
Together, these four attributes characterize SM in CKM as an interactive, adaptive, and multidimensional process. Contextual factors shape behavioral processes that produce improved outcomes, consistent with the IFSMT framework (Ryan & Sawin, 2009). The experiential and relational dimensions of these attributes are explored in the Discussion
Antecedents
Antecedents are the prerequisites for SM. They precede engagement and create readiness, opportunity, and capacity for participation (Walker & Avant, 2021). Five antecedents emerged.
Chronic Illness Diagnosis and Disease Burden
Diagnosis catalyzes SM engagement. Disease awareness and symptom severity prompt individuals to take an active role in care (Beetham et al., 2022; Mehravar et al., 2016; Schrauben et al., 2018). Greater disease severity and perceived risk increase motivation for self-monitoring, medication adherence, and lifestyle change (Davis et al., 2010; Foley et al., 2016; Lee et al., 2021; Yokokawa et al., 2014). Low perceived burden reduces engagement (Balagopal et al., 2012; Lewinski et al., 2019; Schrauben et al., 2018).
Healthcare Access and Social Determinants of Health
Healthcare access defines the structural capacity to initiate and maintain SM. This includes insurance coverage, service availability, and continuity of care (Bennett et al., 2013; Davis et al., 2010; Lewinski et al., 2019). Beyond traditional access barriers, broader social determinants of health shape SM capacity. Food insecurity limits the ability to follow dietary recommendations, particularly in low-income and rural communities (Balagopal et al., 2012; Bennett et al., 2013). Transportation barriers restrict attendance at clinical appointments. Davis et al. (2010) found that one-third of rural participants required study-provided transportation. Medication affordability is a persistent challenge. Nearly 30% of participants in Lewinski et al. (2019) were uninsured, and half in Foley et al. (2016) lacked health insurance. These structural factors interact with individual-level antecedents to create cumulative barriers. Financially subsidized, community-based, and culturally tailored programs partially offset these barriers (Balagopal et al., 2012; Lewinski et al., 2019).
Motivation and Lifestyle Behavior
Motivation predicts initiation and maintenance of SM behaviors such as healthy eating, physical activity, and medication adherence (Beetham et al., 2022; Christian et al., 2011; Mehravar et al., 2016). Autonomy-supporting environments, peer encouragement, and digital feedback tools enhance motivation (Lee et al., 2021; Lim et al., 2021; Lewinski et al., 2019; Tang et al., 2012). However, financial stress, limited social support, and low digital literacy weaken engagement (Balagopal et al., 2012; Schrauben et al., 2018).
Provider Involvement and Social Facilitation
Consistent provider engagement through education, reinforcement, and shared decision-making strengthens self-efficacy and adherence (Beetham et al., 2022; Christian et al., 2011; Helou et al., 2020). Multidisciplinary teams provide integrated guidance supporting continuity of care (Beetham et al., 2022; Helou et al., 2020). Family participation, peer mentoring, and community-based education enhance accountability and persistence (Balagopal et al., 2012; Chan et al., 2014; Lee et al., 2021; Zupa et al., 2022). In these studies, family involvement reflected supportive participation rather than formal caregiving.
Health Literacy, Cognitive, and Physical Functioning
Health literacy is the capacity to obtain, process, and use health information (Balagopal et al., 2012; Helou et al., 2020). It forms the knowledge base for interpreting instructions, monitoring parameters, and making informed decisions. Lower educational attainment limits access to health information and constrains SM engagement (Balagopal et al., 2012; Bennett et al., 2013; Schrauben et al., 2018). Tailored educational interventions improve comprehension and adherence (Balagopal et al., 2012; Lewinski et al., 2019). Beyond literacy, SM capacity is also influenced by cognitive and physical functioning. Cognitive impairments, including CKD-related cognitive changes, can compromise the ability to self-monitor symptoms and self-manage complex medication regimens. Moreover, physical limitations, such as reduced mobility or fatigue, may restrict exercise and clinic attendance. These functional dimensions are critical determinants of SM capacity in CKM populations.
Consequences
Consequences are the outcomes resulting from effective SM in CKM. Six emerged in this analysis: improved CKM health, greater autonomy, sustained lifestyle and behavioral change, reduced hospitalizations and healthcare costs, enhanced care coordination, and strengthened relational support.
Improved CKM Health
Improved CKM health encompasses measurable gains in glycemic control, blood pressure, renal function, and lipid management (Crasto et al., 2011; Helou et al., 2020; Lim et al., 2021; Waki et al., 2024). The Diabetes mHealth program demonstrated HbA1c reductions and a 28.8% decrease in albuminuria (Waki et al., 2024). Multidisciplinary approaches preserved renal function and slowed disease progression (Helou et al., 2020; Beetham et al., 2022).
Greater Autonomy
Greater autonomy reflects the self-efficacy and independence that develop through active disease management. Autonomy-supportive communication from clinicians and family strengthens activation and long-term engagement (Lewinski et al., 2019; Lee et al., 2021; Zupa et al., 2022). Culturally tailored education further builds confidence (Balagopal et al., 2012; Tang et al., 2012).
Sustained Lifestyle Changes
Sustained lifestyle change involves transforming health-promoting behaviors into habitual routines. Long-term adherence reduces cardiovascular and metabolic risks (Balagopal et al., 2012; Foley et al., 2016; Helou et al., 2020; Tang et al., 2012). Behavioral coaching, goal-setting, and digital interventions reinforce these changes over time (Lewinski et al., 2019; Lim et al., 2021; Waki et al., 2024).
Enhanced Care Coordination
Enhanced care coordination emerges when SM is integrated into healthcare delivery. Nurse-led and pharmacist-supported models reduce fragmentation and strengthen continuity (Beetham et al., 2022; Chan et al., 2014; Crasto et al., 2011; Helou et al., 2020). Reduced hospitalizations and costs result from consistent SM engagement (Foley et al., 2016; Lewinski et al., 2019; Sheppard et al., 2020). Strengthened relational support through family involvement, peer mentorship, and nurse-led follow-up sustains long-term SM (Balagopal et al., 2012; Chan et al., 2014; Tang et al., 2012; Zupa et al., 2022).
These consequences demonstrate multilevel benefits (biological, behavioral, psychosocial, and systemic), aligning with IFSMT's outcome domain (Ryan & Sawin, 2009).
Proposed Definition of SM in CKM
Self-management in CKM is a holistic, multidimensional, and adaptive process in which individuals navigate interacting chronic conditions through self-monitoring, personalized and precision care, collaborative care, and sustained engagement. Grounded in the IFSMT (Ryan & Sawin, 2009) and informed by Neuman's Systems Model (Neuman & Fawcett, 2011), SM in CKM integrates behavioral, technological, and relational strategies to support coordinated decision-making, long-term engagement, and whole-person well-being. This definition encompasses both behavioral regulation of health parameters and the experiential dimensions of living with multimorbidity within complex healthcare systems.
Illustrative Cases
Model Case: Mrs. A., a 58-year-old woman with type 2 diabetes, stage 3 CKD, and hypertension, enrolls in a nurse-led SM program. She tracks glucose, blood pressure, and activity via a digital app (self-monitoring). Her nurse helps her prioritize and tailor culturally appropriate goals (personalized care). She attends her regularly scheduled visits with her nephrologist and dietitian, and consults with her pharmacist about her medication regimen and changes (collaborative care). Family encouragement and positive reinforcement via weekly virtual sessions maintain her motivation (sustained engagement). Over 6 months, her HbA1c drops from 8.5% to 6.9%, her blood pressure stabilizes, and her albuminuria decreases by 25%. Mrs. A. also reports feeling more in control of her health and more connected to her care team.
Contrary Case: Mr. B., with the same diagnoses, declines to participate in SM. He misses appointments, skips medication, and avoids monitoring. He avoids conversations about his health with family and friends, and reports feeling overwhelmed and hopeless about managing multiple conditions. Without support, his HbA1c rises, his blood pressure remains uncontrolled, and emergency visits increase.
Borderline Case: Ms. C. takes medications and attends visits. However, she inconsistently monitors her glucose and rarely uses telehealth. Cultural barriers and limited motivation impede full engagement. She has limited social support from family or friends. Her labs show modest improvement but persistent risk.
Related Case: Mr. D. follows treatment plans only with extensive family assistance. Though clinically stable, his SM lacks autonomy, highlighting dependence on external supports rather than intrinsic engagement.
These cases illustrate the spectrum of SM engagement and demonstrate how context, resources, and support shape outcomes. Through an IFSMT lens, variations in context alter SM processes and health outcomes.
Empirical Referents
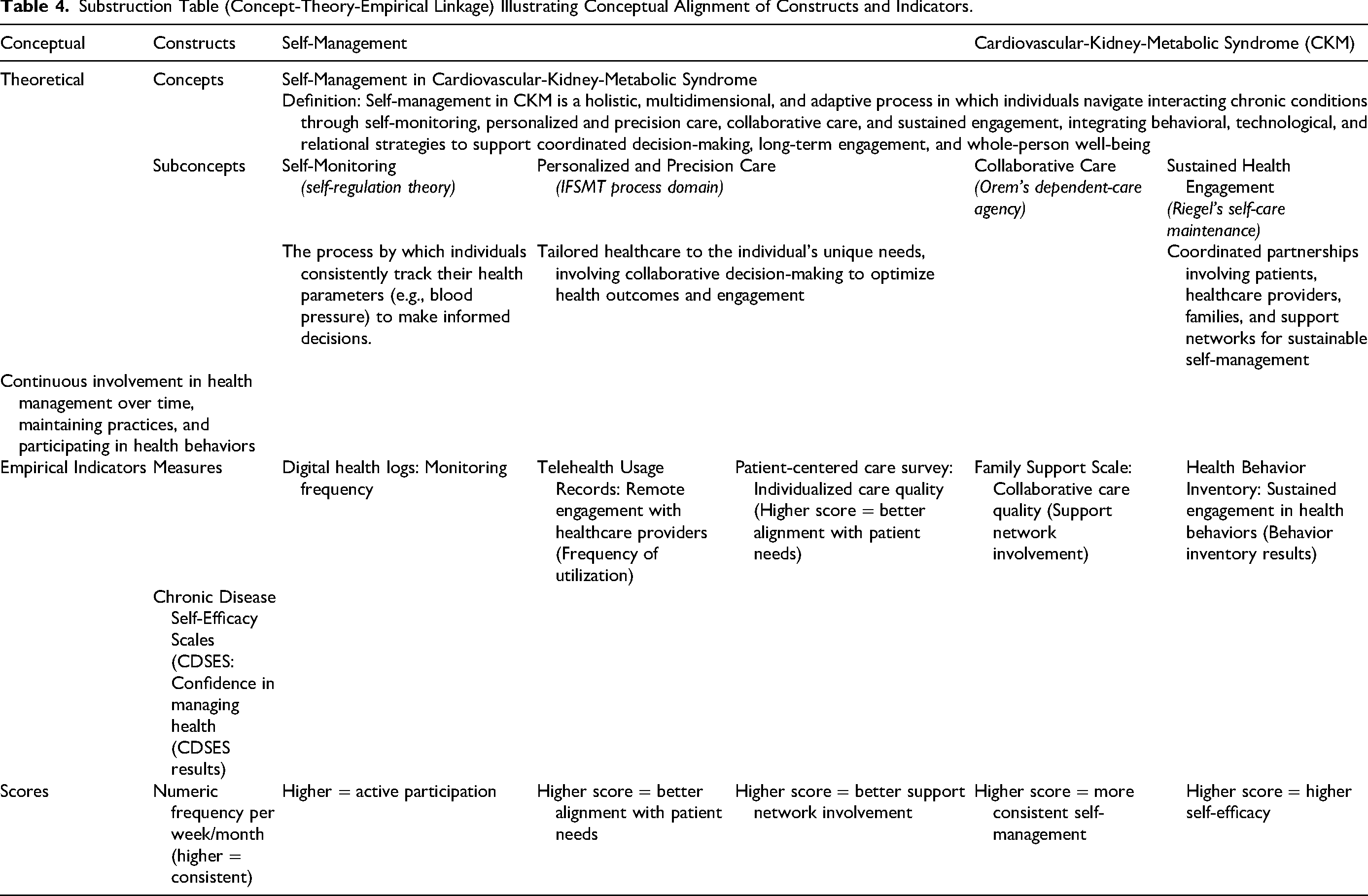
Empirical referents are the observable indicators used to measure the presence of a concept (Walker & Avant, 2021). CKM syndrome involves biological, behavioral, and digital referents. Biological referents include HbA1c, blood pressure, eGFR, serum creatinine, and urinary albumin-to-creatinine ratio. Behavioral referents encompass self-monitoring frequency, medication adherence, dietary modification, and physical activity. Digital health metrics include app usage, telehealth attendance, and care coordination logs. Patient-reported outcomes, including self-efficacy, quality of life, and adherence confidence, are measured using validated scales such as the Self-Care of Hypertension Inventory, EQ-5D, and chronic-disease self-efficacy instruments. Health-system indicators, including emergency visits and hospitalizations, quantify the durability of SM impact. Table 4 provides the full conceptual-theoretical-empirical linkage.
Substruction Table (Concept-Theory-Empirical Linkage) Illustrating Conceptual Alignment of Constructs and Indicators.
Discussion
Scope and Definition of SM in CKM
This concept analysis confirms that SM in CKM is a complex, multidimensional process integrating medication adherence, dietary regulation, symptom monitoring, psychosocial adjustment, and partnership with providers and families (Grady & Gough, 2014; van der Gaag et al., 2022). Definitions of SM often overlap with self-care, self-efficacy, and patient activation (Table 3), creating conceptual ambiguity (Richard & Shea, 2011; M. T. Lawless et al., 2021). In CKM, these stressors manifest as intrapersonal physiological and psychological burden, interpersonal tensions among patients, families, and providers, and extrapersonal barriers such as fragmented care and structural inequities (Neuman & Fawcett, 2011).
The relationship between SM and self-care warrants particular attention. Riegel et al.'s (2012) middle-range theory identifies self-care maintenance, monitoring, and management as core processes. Our findings align with elements of this framework: symptom tracking mirrors self-care monitoring, and sustained engagement mirrors self-care maintenance. However, SM in CKM is not simply an extension of self-care, but represents a distinct construct for three reasons.
First, pathophysiological interdependence. Self-care theories have primarily been developed in single-condition contexts and assume a relatively stable relationship between actions and responses. CKM operates across interdependent disease systems where interactions create unpredictable effects. For instance, intensifying glycemic control may compromise renal function, diuretic therapy may destabilize electrolyte balance, and renal-protective diets may conflict with diabetes nutrition. The person is not managing conditions in parallel; they are navigating competing demands.
Second, system-level coordination. Unlike self-care, which is conceptualized primarily at the individual or dyadic level, SM in CKM requires integration across multiple providers, specialties, and healthcare systems. Collaborative care and personalized/precision care (two defining attributes identified in this analysis) require coordination beyond the individual or dyadic level. This reflects what Neuman describes as the extrapersonal environment (Neuman & Fawcett, 2011). Third, experiential complexity. SM in CKM extends beyond competing regimens to encompass the existential weight of progressive, interacting conditions threatening multiple organ systems. Qualitative accounts describe this as a biographical disruption involving identity reconstruction and meaning-making (de la Cuesta-Benjumea et al., 2023; Frandsen et al., 2024). These three distinctions position SM in CKM as a concept that builds on but is not reducible to self-care.
Contradictory and Competing Findings
The literature revealed several tensions. Chan et al. (2014) found that telephone-based peer support did not improve cardiometabolic outcomes beyond integrated care alone, suggesting additional social support may have a ceiling effect when structured care is already in place. Several digital interventions improved biomarkers, such as HbA1c, but did not produce changes in body weight (Bennett et al., 2013; Davis et al., 2010). This indicates that SM effectiveness may be condition-specific rather than uniformly beneficial across all CKM domains.
CKM heterogeneity also creates competing SM demands. Exercise prescriptions benefiting cardiovascular fitness must be modified for advanced CKD or heart failure. Medications optimizing one condition may exacerbate another, requiring ongoing reconciliation across prescribers. Communicating the rationale for these trade-offs helps patients understand why their treatment plans require tailoring and why active SM is essential.
Holistic Dimensions of Self-Management in CKM
Beyond their behavioral and clinical dimensions, each attribute carries holistic significance rooted in the lived experience of managing interacting chronic conditions.
Self-monitoring involves more than routine tracking. For persons living with CKM, it demands ongoing vigilance and the cognitive burden of interpreting conflicting signals from interacting diseases. Brown et al. (2025) found that individuals with diabetes and cardiovascular disease perceived their conditions as “disconnected,” while Liddy et al. (2014) identified conflicting knowledge and communication difficulties with providers as pervasive themes across multiple chronic conditions. These experiences represent intrapersonal stressors that penetrate the person's lines of defense, generating psychological distress alongside the clinical task of monitoring (Neuman & Fawcett, 2011).
Sustained engagement carries deep existential significance. de la Cuesta-Benjumea et al. (2023) described advanced CKD as a “biographical disruption” in which patients continuously reconstruct their sense of self. Frandsen et al. (2024) found that CKD altered family roles and identities, generating sadness, loss, and a desire to preserve ordinary life. Sustained engagement is thus not simply a behavioral outcome but an ongoing process of identity negotiation and meaning-making, reflecting the developmental and spiritual variables in Neuman's model.
Collaborative care extends beyond clinical partnerships to encompass relational connectedness. Patients, caregivers, and providers often share similar goals but prioritize different aspects of multimorbidity management, creating interpersonal stressors that can strengthen or undermine SM (Peeler et al., 2024). Individuals with CKD have also turned to online peer communities for emotional support and shared understanding (Du et al., 2022), reflecting the extrapersonal dimensions of collaboration within Neuman's framework.
The antecedents and consequences identified in this analysis also carry holistic dimensions beyond their structural and clinical descriptions. Chronic illness diagnosis is experienced as a profound disruption to identity and life trajectory (de la Cuesta-Benjumea et al., 2023), while emotional distress and existential uncertainty are pervasive across CKM conditions (Brown et al., 2025; Liddy et al., 2014). Among the consequences, improved health extends beyond clinical stability to encompass personal transformation (resilience, renewed purpose, and strengthened relationships), reflecting reconstitution toward a new normal line of defense (Neuman & Fawcett, 2011). These holistic dimensions do not diminish the behavioral and clinical components of SM; they situate them within the fuller context of living with CKM.
Health Literacy and Empowerment as Mediating Mechanisms
Health literacy and empowerment function as mediating mechanisms rather than independent antecedents. Structural factors such as healthcare access and social determinants create the conditions for self-management. However, they influence outcomes through health literacy and empowerment, which enable communication, navigation, shared decision-making, and resilient engagement (Billany et al., 2023; Vainauskienė & Vaitkienė, 2021). This proposed pathway, in which structural antecedents shape mediating mechanisms that activate SM attributes and produce consequences, is consistent with IFSMT's conceptualization of context influencing processes and outcomes (Ryan & Sawin, 2009) and is illustrated in Figure 2.
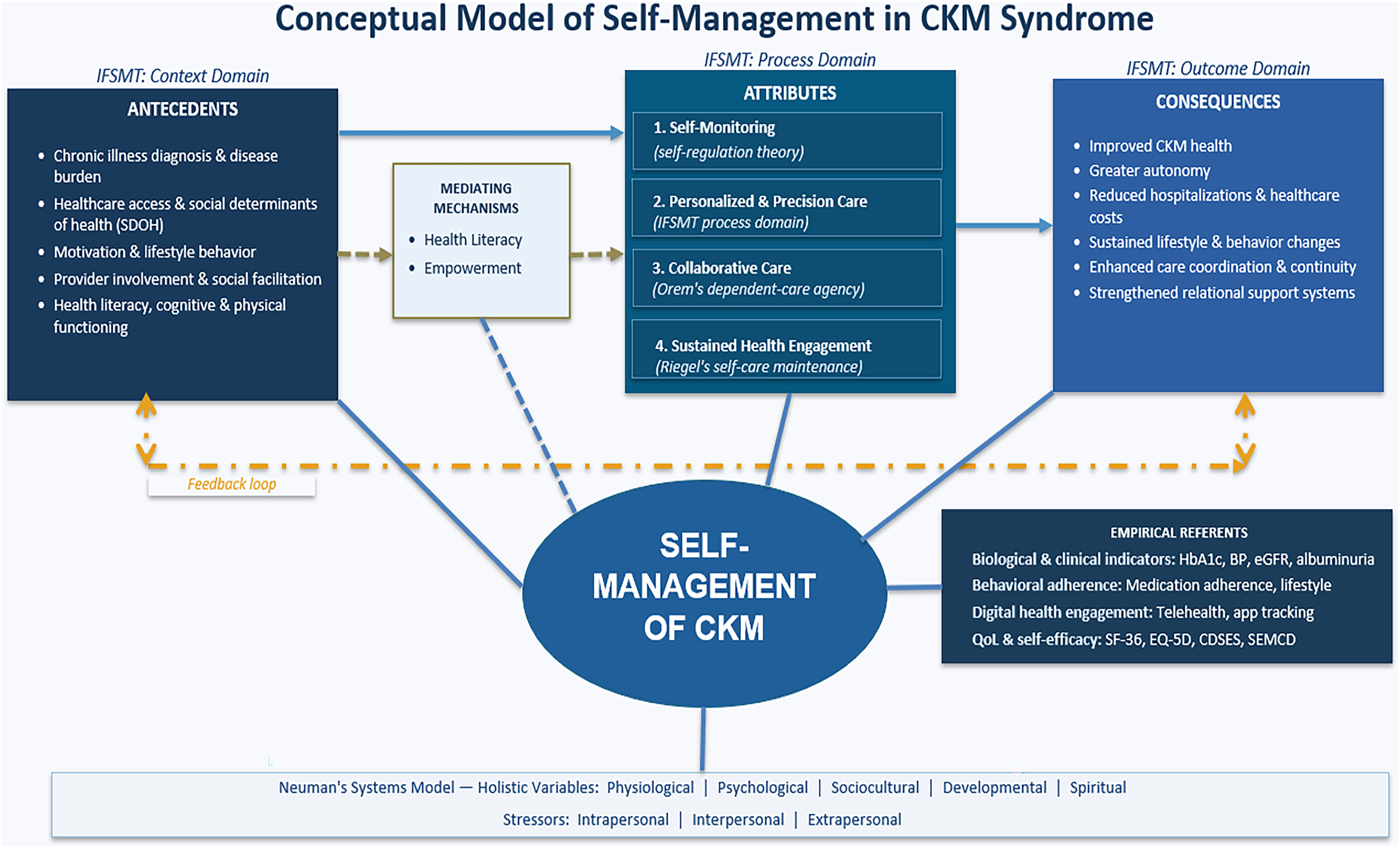
Conceptual model of self-management in cardiovascular-kidney-metabolic syndrome. Antecedents operate through mediating mechanisms (Health Literacy and Empowerment) to activate four defining attributes, producing six consequences. Arrows indicate directional influence; the dashed line reflects the cyclical feedback loop. The model integrates the IFSMT framework (Ryan & Sawin, 2009) with Neuman's holistic variables and stressor types (Neuman & Fawcett, 2011). Empirical referents identify observable indicators used to measure the concept.
Implications for CKM-Specific Interventions
CKM-specific SM interventions should differ from single-disease programs by addressing competing management goals. Rather than delivering condition-specific education in isolation, interventions should help patients and providers navigate the trade-offs inherent in multimorbidity. Shared digital platforms that allow care teams to track interconnected clinical parameters within a single system may support integration. Nurse-led multidisciplinary coordination bridging relevant specialties is essential. For example, an intervention for a patient with diabetic kidney disease and hypertension might simultaneously address glycemic control, blood pressure management, and nephroprotection through a shared care plan that acknowledges competing priorities. Nurses are uniquely positioned to lead this coordination given their training in patient-centered care and their established roles in chronic disease management and self-management support.
Toward a Middle-Range Theory: Challenges and Future Directions
The proposed definition, together with the identified antecedents and consequences, constitutes the foundation for a middle-range explanatory theory of SM in CKM. The attributes describe the process; the antecedents describe the conditions under which it occurs; and the consequences describe the expected outcomes. This structure (conditions, processes, outcomes) is testable and falsifiable, meeting the criteria for a middle-range theory (Walker & Avant, 2021). This conceptualization advances the IFSMT by specifying how contextual antecedents interact with process attributes to produce outcomes, incorporating digital engagement, social determinants, and the unique pathophysiological interactions of CKM as contextual drivers.
However, several challenges warrant attention. At the patient level, competing SM demands, low health literacy, cognitive decline, physical limitations, and psychosocial barriers such as depression and diabetes distress can undermine engagement. Digital divides further disadvantage older adults and those in low-resource settings. At the system level, cardiovascular, kidney, and metabolic conditions are frequently treated in silos, with limited cross-specialty communication (Lee et al., 2021; Zupa et al., 2022). Workforce constraints, time-limited encounters, and the absence of standardized CKM-specific SM protocols hinder implementation.
Limitations
Several limitations should be noted. “Self-care” was not included as a MeSH heading or explicit search keyword. As discussed earlier, SM and self-care are related but distinct constructs:
Self-care has been primarily developed and tested within individual health-maintenance contexts, whereas SM in CKM encompasses collaborative, precision, and system-level coordination across interacting diseases. The search was therefore designed around SM as the target concept. Nevertheless, the broad Boolean strategy captured studies employing self-care frameworks, as confirmed by the final sample. Future concept analysis examining the intersection of SM and self-care in CKM should include “self-care” as an explicit term to ensure comprehensive retrieval.
Qualitative and conceptual papers were excluded from the formal concept analysis sample. While this decision maintained focus on empirical evidence with measurable outcomes, it limited the analysis's capacity to capture the experiential, relational, and spiritual dimensions of SM. These dimensions are central to holistic nursing. The exclusion may have biased the findings toward behavioral and clinical constructs at the expense of meaning-making, identity, suffering, and other aspects of the lived experience of managing CKM. To partially address this limitation, qualitative research was incorporated narratively in the Discussion to enrich the interpretation of the attributes, antecedents, and consequences. Future concept analyses of SM in CKM should include qualitative literature in the formal sample to ensure that the full scope of the human response to multimorbidity is represented. Additionally, pilot and feasibility studies were excluded, which may have limited the evidence base in this emerging area where larger trials remain scarce. Most included studies focused on CKM dyads rather than the full triad, reflecting the framework's emerging nature. Moreover, most evidence was cross-sectional or short-term. Longitudinal studies are needed to clarify causal pathways. Finally, cognitive and physical functioning were identified as influences on SM capacity but were not systematically measured across studies.
Implications for Holistic Nursing
Practice. Nurses are uniquely positioned to lead SM support for persons with CKM because of their training in whole-person assessment, care coordination, and patient education. This analysis identifies four attributes that should guide nursing practice. Self-monitoring support should attend to both data accuracy and the person's emotional experience of vigilance. Care plans should be personalized to honor the person's values, cultural context, and family roles. Collaborative relationships should be grounded in trust and authentic presence. Sustained engagement requires recognizing the existential demands of living with progressive multimorbidity. Moreover, screening for social determinants and integrating culturally responsive communication should be standard components of CKM care. Digital health tools should complement, not replace, the relational dimensions of nursing care.
Education. Nursing curricula should prepare students to care for persons with multimorbidity as a holistic challenge, not as the sum of disease-specific protocols. Education on CKM should integrate pathophysiological knowledge with skills in relational care and shared decision-making. Attention to the psychological, sociocultural, developmental, and spiritual dimensions of chronic illness management is essential. The IFSMT and Neuman's Systems Model offer complementary frameworks for teaching students to assess both individual SM processes and the system-level stressors that shape them.
Research. This analysis provides a foundation for a middle-range explanatory theory of SM in CKM. Future research should test the proposed relationships among antecedents, attributes, and consequences using longitudinal and hybrid effectiveness-implementation designs. CKM-specific SM outcome measures are needed that capture biomarkers, adherence, and experiential outcomes (including meaning-making, identity adaptation, relational connectedness, and spiritual well-being). Qualitative research on the lived experience of managing CKM is critically needed to deepen understanding of the holistic dimensions identified in this analysis. This analysis identifies measurable constructs (monitoring frequency, digital engagement, empowerment indicators, and psychosocial mediators) to guide instrument development and intervention evaluation.
Leadership and Policy. Nurse leaders should advocate for integrated CKM care models that bridge cardiology, nephrology, endocrinology, and primary care. Reducing fragmentation is critical, as patients experience it as a major barrier to SM. Policy efforts should address the structural determinants identified as antecedents in this analysis: insurance coverage, medication affordability, transportation access, and food security.
Conclusion
This concept analysis clarifies SM in CKM as a holistic, multidimensional, and adaptive process characterized by four defining attributes: self-monitoring, personalized and precision care, collaborative care, and sustained engagement. When effectively enacted, SM produces multilevel benefits including improved clinical outcomes, greater autonomy, sustained behavioral change, reduced healthcare utilization, and personal transformation. Nurse-led, multidisciplinary, digitally integrated SM programs attending to the whole person represent a promising approach to equitable CKM care across diverse populations and healthcare contexts.
Footnotes
Acknowledgments
None.
Ethical Considerations
Not applicable. This concept analysis synthesized published literature and did not involve human participants, human data, or human tissue. Institutional review board approval was not required.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
Margaret A. Ayorinde: conceptualization, methodology, writing—original draft. Lakeshia Cousin: methodology, writing—review and editing. Staja Q. Booker: supervision, methodology, writing—review and editing. Jennifer R. Dungan: methodology, writing—review and editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data supporting this concept analysis were derived from published sources. No new datasets were created or analyzed.