
Abstract
Introduction
Chronic illnesses represent a major global health burden and require ongoing management to prevent complications and maintain well-being (Chan, 2021; World Health Organization, 2026). Effective self-care is a cornerstone of chronic illness management, encompassing activities such as symptom monitoring, medication adherence, and lifestyle modification (Lorig & Holman, 2003; Jonkman et al., 2016). Suboptimal self-care remains prevalent and contributes to impaired quality of life (Narasimhan et al., 2019; Gaspar & Domingos, 2017). Quality of life, encompassing physical, psychological, and social well-being, is recognized as a critical outcome in chronic illness care beyond clinical indicators (Chan, 2021; Koirala et al., 2023).
Despite the centrality of self-care and quality of life, interventions targeting self-care and quality of life have predominantly focused on individual patients, with limited consideration of relational contexts in which chronic illness is experienced and managed (Martire & Helgeson, 2017). Chronic illness management occurs within interpersonal environments shaped by significant others, including family members, partners, and caregivers, who contribute to decision-making, support provision, symptom monitoring, and treatment adherence (Chao et al., 2022; Lyons & Lee, 2018; Piette et al., 2015; Novais et al., 2023). Self-care behaviors and quality of life are therefore influenced by both individual and relational factors within dyadic interactions (Lyons & Lee, 2018; Martire & Helgeson, 2017).
Approaches involving significant others, including family-centered care and caregiver support interventions, demonstrate beneficial outcomes (Aliakbari et al., 2022; Asadollahi Hamedani et al., 2021; Payrovee et al., 2014). Existing approaches primarily emphasize unidirectional support, with limited attention to reciprocal engagement and shared responsibility in chronic illness management (Martire & Helgeson, 2017; Lyons & Lee, 2018). Dyadic empowerment (DE) has emerged as an approach that emphasizes mutual engagement, collaborative decision-making, and shared responsibility between individuals with chronic illness and significant others (Funnell et al., 1991; Anderson & Funnell, 2010).
Dyadic empowerment is defined as a relational process in which individuals with chronic illness and significant others jointly develop knowledge, skills, and shared responsibility to manage illness through mutual engagement and collaborative decision-making (Anderson & Funnell, 2010; Lyons & Lee, 2018). DE facilitates relational processes that enhance capacity for self-care and adaptation to chronic illness (Marzorati et al., 2018; De Maria et al., 2023). Alignment with holistic nursing principles is evident through integration of physical, psychological, social, and relational dimensions of care (Turkel et al., 2018; Cara, 2003). Holistic nursing conceptualizes caring as a relational process characterized by interconnectedness and mutual influence (Smith et al., 2012; Turkel et al., 2018). DE provides a mechanism to operationalize relationship-centered care, with potential to improve self-care and quality of life outcomes (Carr et al., 2019; Trump et al., 2018).
Evidence on dyadic or family-involved interventions in chronic illness is increasing; however, conceptualization of DE remains inconsistent across studies (Xiong et al., 2022; Ania-González et al., 2022). Variability exists in intervention components, delivery methods, duration, and theoretical foundations, with limited clarity regarding integration of empowerment processes within dyads (Hoffmann et al., 2014; Ania-González et al., 2022). Evidence related to self-care and quality of life outcomes is dispersed across conditions and intervention types, limiting identification of consistent patterns and mechanisms (De Maria et al., 2023; Xiong et al., 2022).
A comprehensive synthesis is required to clarify characteristics and outcomes of DE interventions. This scoping review aims to map and synthesize evidence on DE interventions for individuals with chronic illness and significant others, with emphasis on self-care and quality of life outcomes. Identification of key components, delivery approaches, and outcomes will contribute to conceptual refinement of dyadic empowerment and inform development of holistic, relationship-centered interventions in chronic illness care (Arksey & O’Malley, 2005; Peters et al., 2015; Pollock et al., 2021).
Conceptual Framework
This scoping review is guided by Jean Watson's Theory of Human Caring, which emphasizes caring relationships as a foundation for promoting healing, human dignity, and well-being (Smith & Turkel, 2012). Within this perspective, caring is conceptualized as a relational process characterized by interconnectedness and mutual influence. Caring relationships support emotional well-being, enhance self-efficacy, and contribute to improved quality of life, which are central outcomes in chronic illness care.
To strengthen the relational perspective, this review is further informed by dyadic illness management concepts, which conceptualize individuals with chronic illness and significant others as an interdependent unit engaged in shared illness management (Lyons & Lee, 2018). Within a dyadic context, self-care is shaped through collaborative processes, including shared appraisal of illness, mutual engagement, and joint decision-making.
Dyadic empowerment is positioned within this framework as a relational process in which individuals with chronic illness and significant others jointly develop knowledge, skills, and shared responsibility to manage illness through mutual engagement and collaborative decision-making (Anderson & Funnell, 2010; Lyons & Lee, 2018). Dyadic empowerment extends beyond unidirectional support by emphasizing reciprocal participation and shared responsibility in illness management.
This framework guides the synthesis by focusing on how interventions incorporate relational processes, including mutual engagement, shared responsibility, and collaborative decision-making, and how these elements contribute to self-care and quality of life outcomes. Analysis is directed toward identifying intervention components and delivery approaches that reflect dyadic interaction and relationship-centered care within chronic illness management.
Methods
Research Design
This study followed the five-stage framework for scoping reviews: identifying the research question, identifying relevant studies, selecting studies, charting the data, and collating, summarizing, and reporting the results (Arksey & O’Malley, 2005). Reporting adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guidelines.
Identify the Research Question
The research question guiding this scoping review was: What are the characteristics and outcomes of dyadic empowerment interventions for individuals with chronic illness and their significant others, particularly in relation to self-care and quality of life?
Identifying Relevant Studies
Relevant studies were identified through a comprehensive search of four electronic databases: EMBASE, Ovid MEDLINE, Cochrane Library, and CINAHL. These databases were selected for broad coverage of medical, nursing, and allied health literature. The search was conducted from database inception to March 2024.
The search strategy combined controlled vocabulary and free-text terms and was developed in consultation with an academic librarian to enhance methodological rigor. Search terms included concepts related to chronic illness, dyadic relationships, empowerment, self-care, and quality of life.
Using EMBASE as an example, the search combined controlled terms such as “chronic disease”/exp and “empowerment”/exp with free-text terms including (dyad* OR partner* OR couple* OR “significant other*” OR caregiver*) AND empowerment*, along with terms related to self-care and quality of life. Search syntax and indexing terms were adapted for each database to account for variations in terminology and indexing systems.
Additional studies were identified through citation tracking of included articles. The full search strategy is presented in Supplementary Table 1.
Study Selection
All retrieved records were imported into EndNote for duplicate removal and manually verified. Study selection was conducted in two stages. First, titles and abstracts were independently screened by two reviewers, DS and SAA, using predefined inclusion and exclusion criteria. Second, full-text articles were assessed for eligibility. Discrepancies were resolved through discussion, with involvement of a third reviewer when necessary.
Eligibility criteria were guided by the PCC framework (Population, Concept, Context). The population included individuals with chronic illness and their significant others. The concept focused on dyadic empowerment interventions, defined as interventions that actively engage both individuals within the dyad in collaborative processes such as shared learning, mutual engagement, joint decision-making, and coordinated self-management. The context included healthcare and community settings addressing chronic illness management.
Studies were included if they examined dyadic empowerment interventions and reported outcomes related to self-care and/or quality of life. Non-empirical publications, including editorials, books, and protocols, were excluded.
Charting the Data
Data charting was conducted using a structured extraction form developed by the research team to systematically capture relevant information from included studies. The extraction form was piloted on a subset of studies and refined iteratively to ensure consistency and alignment with the review objectives.
Extracted data included bibliographic information (author, year, and country), study characteristics (design, population, and type of chronic illness), and intervention characteristics. Intervention details were charted using the TIDieR-Lite framework, including components, delivery mode, setting, duration, intensity, and frequency (Hoffmann et al., 2014). Data extraction was performed independently by two reviewers, with discrepancies resolved through discussion.
Collating, Summarizing, and Reporting the Results
Data from included studies were synthesized using descriptive and qualitative approaches. Descriptive analysis was used to summarize study characteristics and intervention features. A narrative synthesis was conducted to organize findings related to intervention components, delivery approaches, relational processes, and outcomes.
The synthesis focused on identifying patterns in how dyadic empowerment was operationalized across studies and how intervention characteristics were associated with self-care and quality of life outcomes. Variability in intervention design, duration, and reporting was also examined to highlight gaps in the existing evidence base.
Results
Selection of Sources of Evidence
A total of 1,366 records were identified through database searching. After removing duplicates, records were screened based on their titles and abstracts. Twenty articles were assessed for full-text eligibility. Fifteen studies were excluded during full-text review due to the absence of self-care and/or quality of life outcomes (n = 9) or non-empirical design (n = 6). Five studies met the inclusion criteria from database searches. Citation tracking identified three additional studies, bringing the total to eight included in the final analysis (Figure 1).
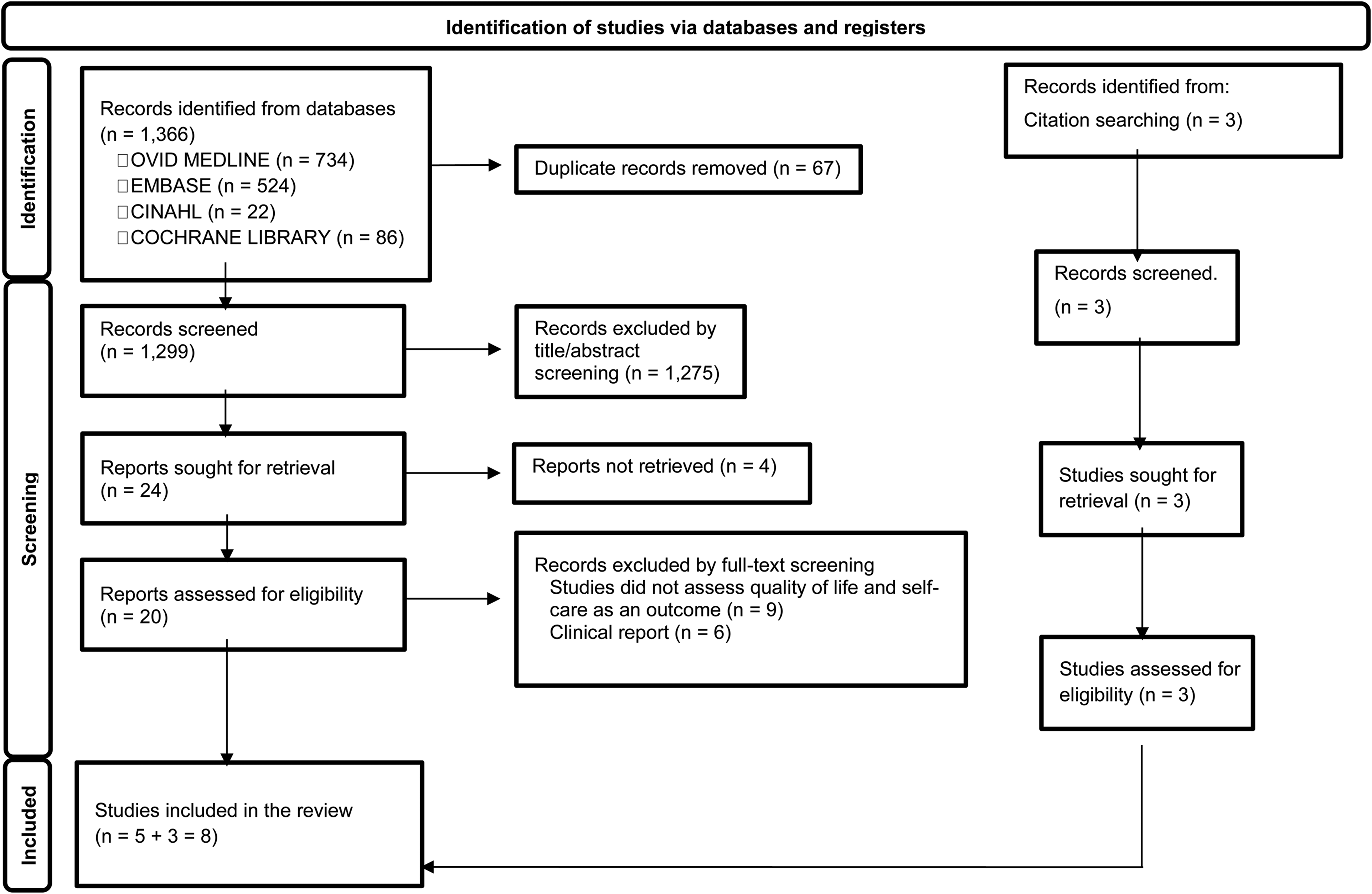
PRISMA flow diagram of the study selection process.
Characteristics of Included Studies
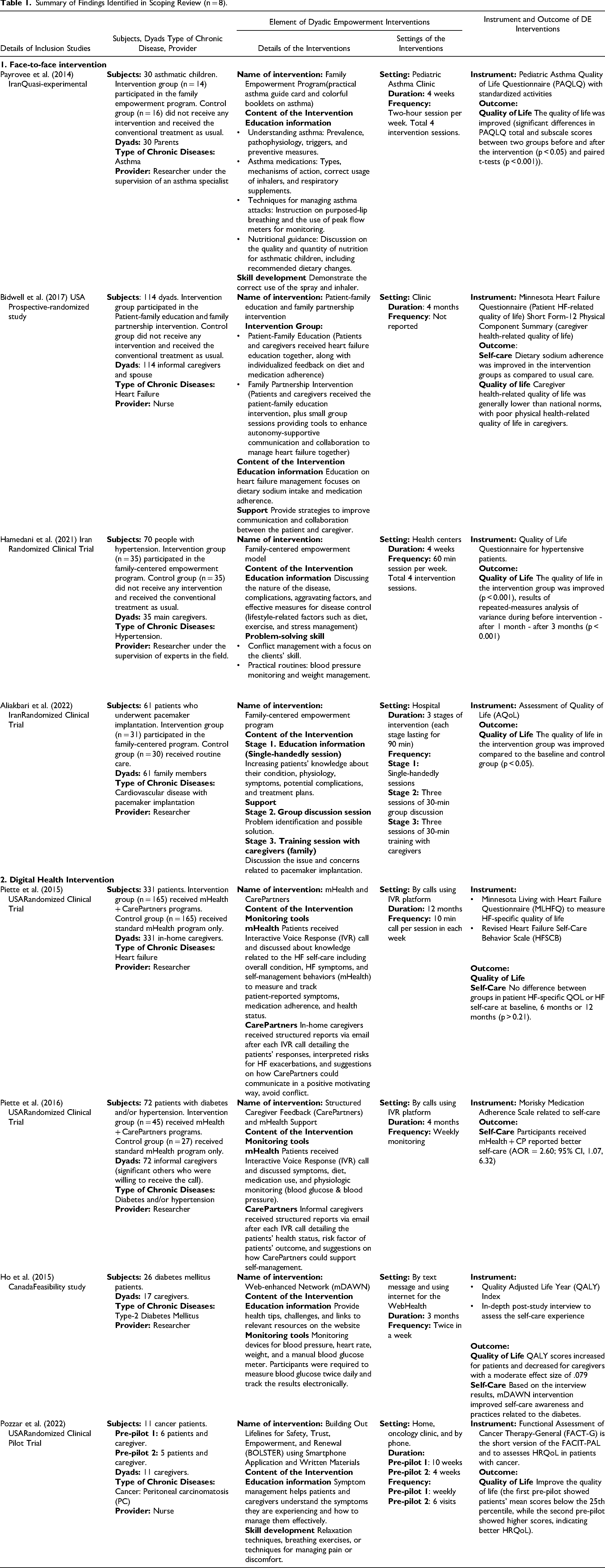
Eight studies published between 2014 and 2022 were included. Study designs comprised randomized controlled trials (n = 5), quasi-experimental design (n = 1), prospective randomized study (n = 1), and feasibility study (n = 1). Studies were conducted in the United States (n = 4), Iran (n = 3), and Canada (n = 1).
Chronic conditions included cardiovascular disease (n = 3), diabetes mellitus and hypertension (n = 3), asthma (n = 1), and cancer (n = 1). Dyads consisted of individuals with chronic illness and significant others, including parents (n = 3), spouses, and informal caregivers (n = 5). Detailed characteristics of included studies are presented in Table 1.
Summary of Findings Identified in Scoping Review (n = 8).
Characteristics of Dyadic Empowerment Interventions
Components of DE Interventions
Dyadic empowerment interventions incorporated multiple components. Educational content was the most frequently reported component (n = 6), addressing disease knowledge, symptom management, treatment adherence, and lifestyle modification (Payrovee et al., 2014; Asadollahi Hamedani et al., 2021; Aliakbari et al., 2022). Monitoring components (n = 4) included use of devices such as blood pressure monitors, glucometers, and symptom tracking systems (Piette et al., 2015; Piette et al., 2016; Ho et al., 2015).
Skill development (n = 2) focused on practical competencies such as inhaler use, relaxation techniques, and symptom management (Payrovee et al., 2014; Pozzar et al., 2022). Support components (n = 2) included communication strategies and emotional support between dyad members (Bidwell et al., 2017; Aliakbari et al., 2022). Problem-solving strategies (n = 1) addressed conflict management and daily routine adaptation (Asadollahi Hamedani et al., 2021).
Mode of Delivery, Settings, and Relational Features
Interventions were delivered through digital approaches (n = 4), including mHealth platforms, smartphone applications, and Interactive Voice Response systems (Piette et al., 2015; Piette et al., 2016; Ho et al., 2015; Pozzar et al., 2022), and face-to-face approaches (n = 4), including family empowerment programs and patient-family education sessions (Payrovee et al., 2014; Bidwell et al., 2017; Asadollahi Hamedani et al., 2021; Aliakbari et al., 2022).
Intervention settings included outpatient clinics and hospitals (n = 4), home-based or technology-mediated environments (n = 3), and combined settings (n = 1). Interventions demonstrated varying levels of dyadic engagement. Several interventions involved shared education and joint participation in disease management activities (Bidwell et al., 2017; Asadollahi Hamedani et al., 2021). Some interventions incorporated structured communication strategies to support collaboration between individuals with chronic illness and significant others (Bidwell et al., 2017).
Digital interventions facilitated indirect dyadic interaction through feedback systems, in which caregivers received patient data and guidance to support self-management (Piette et al., 2015; Piette et al., 2016). The degree of mutual engagement and shared decision-making varied across studies.
Intervention Dosage and Delivery Personnel
Intervention dosage and delivery personnel were variably reported across the included studies. Seven studies provided information on duration and frequency, with intervention duration ranging from 4 weeks to 12 months and session frequency ranging from weekly to several sessions per week (Payrovee et al., 2014; Piette et al., 2015). When reported, session length ranged from 30 to 120 min.
Interventions were delivered by healthcare professionals in two studies, including nurse-led programs, and by researchers in six studies (Bidwell et al., 2017). Variation was observed in the roles and involvement of intervention providers across studies. Reporting of provider training, qualifications, and intervention delivery procedures was limited. Inconsistent reporting of intervention dosage and delivery characteristics reduced comparability across studies.
Outcomes of Dyadic Empowerment Interventions
Three studies reported improvements in self-care behaviors, including medication adherence, dietary management, and symptom monitoring (Piette et al., 2016; Ho et al., 2015). Improvements were observed within three months and sustained up to 12 months in some studies (Piette et al., 2016). One study reported enhanced self-care awareness based on qualitative findings (Ho et al., 2015).
Five studies reported improvements in quality of life across chronic conditions (Payrovee et al., 2014; Asadollahi Hamedani et al., 2021; Aliakbari et al., 2022; Pozzar et al., 2022). Improvements were observed across short-term and longer follow-up periods. One randomized study reported no significant difference in quality-of-life outcomes despite improvements in self-care behaviors (Piette et al., 2015).
Conceptual Synthesis of Dyadic Empowerment Interventions
The findings of this review indicate that dyadic empowerment interventions consist of interconnected components and relational processes. Across the included studies, core intervention components included education, health monitoring, support, skill development, and problem-solving. These components provided knowledge, resources, and practical skills for individuals with chronic illness and their significant others.
In addition to these components, several dyadic processes were identified, including shared understanding, communication, mutual support, shared decision-making, and collaborative self-care. These processes were consistently described in relation to how individuals with chronic illness and their significant others engaged in joint illness management.
This synthesis reflects recurring patterns identified across the included studies, highlighting how intervention components are operationalized through relational processes within the dyad. Figure 2 presents a synthesized model illustrating the relationships between intervention components, dyadic processes, and outcomes, including self-care behaviors and quality of life.
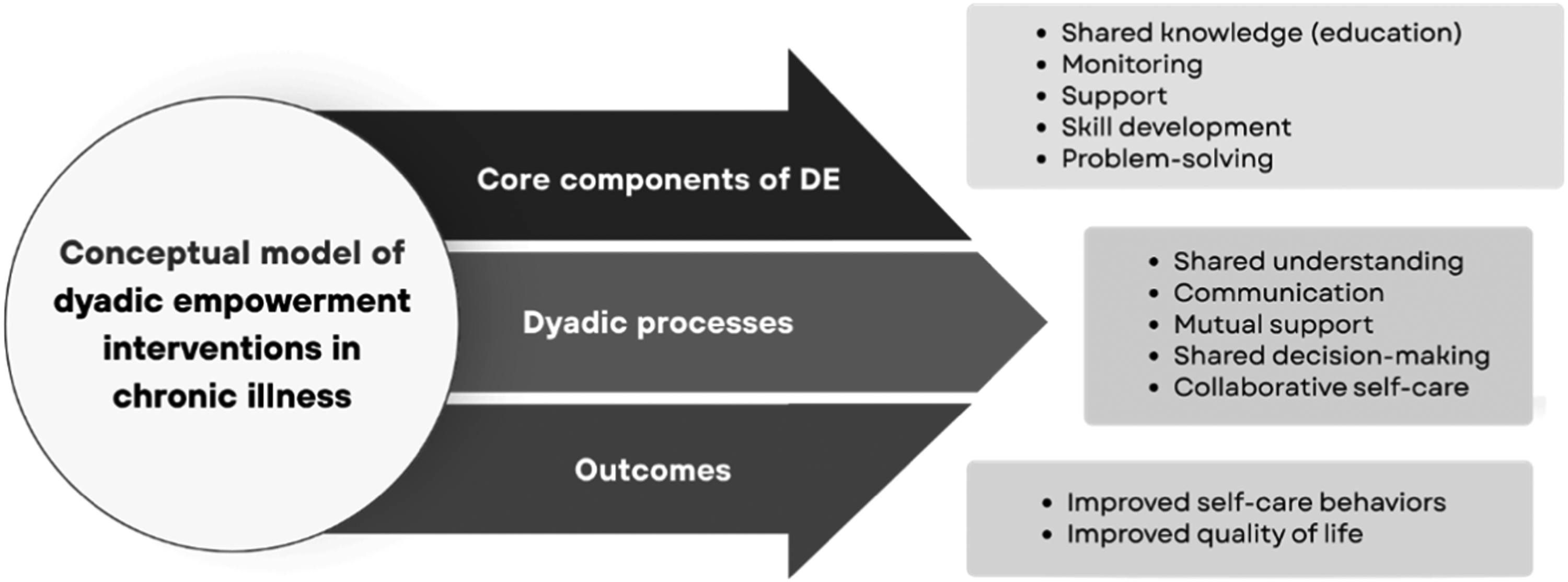
Synthesized model of dyadic empowerment interventions in chronic illness.
Variability and Gaps in Evidence
Substantial variability was observed across studies in intervention components, delivery modes, duration, and reporting of intervention characteristics. Definitions and operationalization of dyadic empowerment were inconsistent. Reporting of intervention dosage, provider roles, and relational processes was limited in several studies, constraining comparability across interventions.
Discussion
The present review synthesized evidence from eight studies examining dyadic empowerment interventions across multiple chronic conditions. Despite heterogeneity in populations and intervention formats, consistent patterns emerged regarding intervention components, relational processes, and outcomes. The relatively small number of included studies reflects the limited of research on dyadic empowerment, particularly in relation to self-care and quality of life outcomes. Although dyadic and family-involved interventions are increasingly recognized, many studies do not explicitly address these outcomes within a dyadic empowerment framework.
Across studies, dyadic empowerment interventions demonstrated convergence in core components, particularly education, monitoring, and supportive interaction. However, the recurrence of similar components suggests that intervention outcomes are unlikely to be explained by content alone. Instead, the relational context in which these components are delivered appears to function as a key mechanism. The conceptual synthesis presented in Figure 2 highlights that dyadic empowerment interventions operate through the integration of intervention components and relational processes within the dyad. Interventions that incorporated shared participation, communication, and collaborative engagement between individuals with chronic illness and their significant others demonstrated more consistent improvements in self-care behaviors and quality of life (Bidwell et al., 2017; Asadollahi Hamedani et al., 2021; Aliakbari et al., 2022; Piette et al., 2016).
The dyadic processes identified across studies, including shared understanding, communication, mutual support, shared decision-making, and collaborative self-care, represent the mechanisms through which these interventions operate. These processes facilitate alignment in illness perceptions, coordination of care activities, and joint responsibility for disease management, thereby strengthening adherence and behavioral change (Martire & Helgeson, 2017; Orsulic-Jeras et al., 2020; Xiong et al., 2022). Empirical evidence further supports the role of relational processes in influencing health behaviors. Helping relationships have been shown to improve health-promoting lifestyles among patients with chronic kidney disease (Chao et al., 2022), while caregiver involvement and dyadic engagement are associated with improved adherence and self-care outcomes (Piette et al., 2015; Piette et al., 2016; De Maria et al., 2023). Together, these findings suggest that dyadic empowerment is inherently relational and that interventions focusing solely on individual behavior change may be insufficient without addressing interpersonal dynamics.
Recent studies published after the search period further reinforce the importance of relational mechanisms in dyadic approaches to chronic illness management. Dyadic observational studies demonstrate that dyadic coping, mutuality, and family resilience exert both actor and partner effects on self-care and illness management outcomes, highlighting the interdependent nature of patient–caregiver relationships (Li et al., 2025; Meng et al., 2025). Qualitative evidence similarly indicates that chronic illness management is negotiated within dyads, with collaborative patterns associated with more adaptive self-care and better relational balance (Baldan et al., 2026). Emerging intervention studies also suggest that dyadic approaches may support improvements in self-care and quality of life, particularly when interventions actively engage both patients and caregivers through digital platforms or structured psychoeducational programs (Son et al., 2025; Zhang et al., 2025).
Differences in delivery modality also appear to influence how relational processes are operationalized. Face-to-face interventions may facilitate deeper relational engagement through direct interaction, shared learning, and immediate feedback (Aliakbari et al., 2022; Bidwell et al., 2017). In contrast, digital interventions enhance accessibility and continuity of support, particularly through monitoring systems and caregiver feedback mechanisms (Piette et al., 2015; Piette et al., 2016; Pozzar et al., 2022). However, several digital approaches rely on indirect or asynchronous interaction, which may limit relational depth. Delivery mode should therefore be considered an active component of intervention design, as it shapes both the quality and intensity of dyadic interaction (Haleem et al., 2021; Gjellebæk et al., 2020).
Outcome patterns indicated that improvements in self-care were more consistently reported than improvements in quality of life. Self-care behaviors may respond more rapidly to structured support, monitoring, and reinforcement, whereas quality of life reflects broader physical, psychological, and social dimensions that may require longer follow-up to demonstrate meaningful change (Gaspar & Domingos, 2017; Koirala et al., 2023). The absence of significant improvements in quality of life in some studies (e.g., Piette et al., 2015) further indicates that behavioral change does not automatically translate into improved perceived well-being.
From a holistic nursing perspective, dyadic empowerment can be understood as an application of relationship-centered care. Holistic nursing emphasizes interconnectedness, caring relationships, and the integration of physical, psychological, social, and relational dimensions of health (Cara, 2003; Smith et al., 2012; Turkel et al., 2018). Dyadic empowerment reflects these principles by positioning both individuals in the dyad as active participants in care, rather than placing responsibility solely on the patient.
Overall, dyadic empowerment represents a relational approach to chronic illness management in which intervention components are operationalized through interpersonal processes within the dyad, rather than as a purely content-driven intervention.
Implications for Holistic Nursing Practice, Education, and Research
Dyadic empowerment interventions can be integrated into holistic nursing care by extending the focus from individuals to include their significant others, such as family members, caregivers, or partners. In clinical practice, nurses can involve significant others in patient education, symptom monitoring, and self-care planning to support collaborative illness management. Through shared engagement and communication, these approaches may enhance adherence to self-care, strengthen coping, and support overall well-being, consistent with holistic nursing principles that address interconnected dimensions of health.
In nursing education, curricula should incorporate competencies related to dyadic care, including dyadic communication, shared decision-making, and empowerment strategies that actively engage both individuals within the dyad. Simulation and case-based learning involving patient–significant other scenarios may help prepare nursing students to deliver relationship-centered care in chronic illness management. Continuing professional education should also emphasize the application of dyadic empowerment approaches across diverse clinical and cultural contexts.
Future research should focus on developing and evaluating more standardized dyadic empowerment interventions, particularly regarding intervention components, duration, frequency, and modes of delivery. Longitudinal studies are needed to examine sustained effects on self-care, quality of life, and caregiver-related outcomes. Further exploration of theoretical frameworks, including dyadic illness management and caring science, may also help clarify the relational mechanisms underlying these interventions.
Strengths and Limitations
This scoping review provides a structured synthesis of dyadic empowerment interventions and their reported outcomes related to self-care and quality of life. By mapping intervention components, delivery approaches, and outcomes across studies, the review offers an overview of how dyadic processes are incorporated into chronic illness care.
However, several limitations should be considered. The number of included studies was limited, and the interventions were heterogeneous in terms of design, duration, and reporting, which restricts comparability across studies. Inconsistent reporting of intervention characteristics, particularly duration and frequency, limits the ability to assess replicability. In addition, no formal quality appraisal was conducted, as is consistent with scoping review methodology, but this limits conclusions regarding the methodological rigor of the included studies. The included studies also focused on a limited range of chronic conditions, which may affect the generalizability of the findings.
Conclusion
This scoping review mapped the characteristics and outcomes of dyadic empowerment interventions for individuals living with chronic illness and their significant others. Across the included studies, these interventions commonly involved education, monitoring, and relational support delivered through face-to-face, digital, or hybrid approaches. Most studies reported improvements in self-care and quality of life, although the evidence was heterogeneous in terms of intervention components, delivery, and outcome reporting. The findings suggest that dyadic empowerment may support chronic illness care by strengthening shared engagement and mutual support within the dyad, which is consistent with the relational perspective of holistic nursing.
Supplemental Material
sj-docx-1-jhn-10.1177_08980101261458844 - Supplemental material for Dyadic Empowerment Intervention on Self Care and Quality of Life for People with Chronic Illness: A Scoping Review
Supplemental material, sj-docx-1-jhn-10.1177_08980101261458844 for Dyadic Empowerment Intervention on Self Care and Quality of Life for People with Chronic Illness: A Scoping Review by Deborah Siregar, Chun-Yi Ho, Shannastaniar Aisya Adif, Ching-Chu Liao, Huan-Fang Lee and Miaofen Yen in Journal of Holistic Nursing
Footnotes
Acknowledgment
The authors acknowledge the librarians at the National Cheng Kung University Medical Library for their valuable guidance on the search strategy.
AI Acknowledgment
The authors used an artificial intelligence-based language tool (ChatGPT, OpenAI) to assist with language refinement and improvement of clarity in the manuscript. All content, interpretation, and conclusions were developed by the authors, who take full responsibility for the integrity and accuracy of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
This study was a scoping review of published literature and did not involve human participants. Therefore, ethical approval and informed consent were not required.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
This scoping review is based on previously published studies. All data supporting the findings of this review are available within the included articles and cited in the references.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.